
The Development of New Methodology for Determination of Vincristine (VCR) in Human Serum Using LC-MS/MS-Based Method for Medical Diagnostics

 , , ,
, , ,  and
and 
Abstract

1. Introduction
2. Results and Discussion
2.1. LC–MS/MS Method Development
- -
- Kinetex, grain 2.6 um, C18 100 A. 50 × 2.1 mm;
- -
- Acquity BEH 1.7 μm, C18 50 × 2.1 mm
2.2. Assay Validation Results
- (I)
- Stored for 120 h in the autosampler;
- (II)
- Stored for a period of 120 h exposed to light at room temperature in the laboratory;
- (III)
- Subjected to freezing and thawing several times (five cycles).
2.3. Comparison of Our Method with the Methods of Other Authors
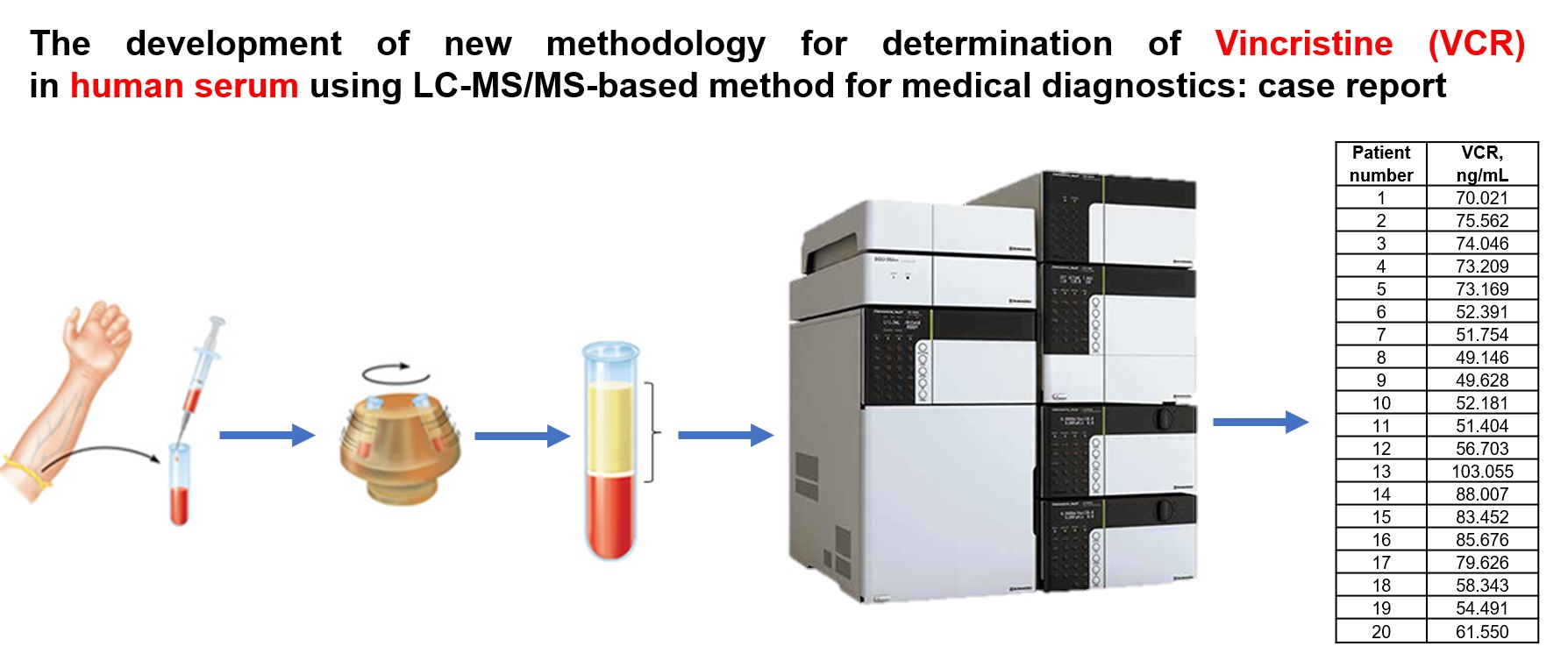
2.4. Application of the Validated Method to Analysis of Clinical Samples
3. Materials and Methods
3.1. Chemicals
3.2. Samples
3.3. LC-MS/MS Conditions
3.4. Calibration Strategy, Quality Control, and Statistical Analysis
- (1)
- The constancy of the retention times of vinblastine and the IS in test samples against calibration solutions;
- (2)
- The constancy of the ratio of fragmentation ion signals of both compounds in the tested samples in relation to the calibration solutions;
- (3)
- The ratio of the signals obtained during the retention of the analyte and the internal standard for blank samples (n = 5) versus the sample at the LLOQ level.
3.5. Sample Preparation
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Sample Availability
References
- Gill, P.S.; Wernz, J.; Scadden, D.T.; Cohen, P.; Mukwaya, G.M.; von Roenn, J.H.; Ross, M.E. Randomized phase III trial of liposomal daunorubicin versus doxorubicin, bleomycin, and vincristine in AIDS-related Kaposi’s sarcoma. J. Clin. Oncol. 1996, 14, 2353–2364. [Google Scholar] [CrossRef] [PubMed]
- Holland, J.F.; Scharlau, C.; Gailani, S.; Krant, M.J.; Olson, K.B.; Horton, J.; Shnider, B.I.; Lynch, J.J.; Owens, A.; Carbone, P.P.; et al. Vincristine treatment of advanced cancer: A cooperative study of 392 cases. Cancer Res. 1973, 33, 1258–1264. [Google Scholar] [PubMed]
- Steiner, R.; Stewart, J.F.; Cantwell, B.M.; Minton, M.J.; Knight, R.K.; Rubens, R.D. Adriamycin alone or combined with vincristine in the treatment of advanced breast cancer. Eur. J. Cancer Clin. Oncol. 1983, 19, 1553–1557. [Google Scholar] [CrossRef]
- Cairncross, J.G.; Wang, M.; Jenkins, R.B.; Shaw, E.G.; Giannini, C.; Brachman, D.G.; Buckner, J.C.; Fink, K.L.; Souhami, L.; Laperriere, N.J.; et al. Benefit from procarbazine, lomustine, and vincristine in oligodendroglial tumors is associated with mutation of IDH. J. Clin. Oncol. 2014, 32, 783–790. [Google Scholar] [CrossRef] [PubMed]
- Da Rocha, A.B.; Lopes, R.M.; Schwartsmann, G. Natural products in anticancer therapy. Curr. Opin. Pharmacol. 2001, 1, 364–369. [Google Scholar] [CrossRef]
- Ceppi, F.; Langlois-Pelletier, C.; Gagné, V.; Rousseau, J.; Ciolino, C.; De Lorenzo, S.; Kevin, K.M.; Cijov, D.; Sallan, S.E.; Silverman, L.B.; et al. Polymorphisms of the vincristine pathway and response to treatment in children with childhood acute lymphoblastic leukemia. Pharmacogenomics 2014, 15, 1105–1116. [Google Scholar] [CrossRef] [PubMed]
- Qaddoumi, I.; Billups, C.A.; Tagen, M.; Stewart, C.F.; Wu, J.; Helton, K.; McCarville, M.B.; Merchant, T.E.; Brennan, R.; Free, T.M.; et al. Topotecan and vincristine combination is effective against advanced bilateral intraocular retinoblastoma and has manageable toxicity. Cancer 2012, 118, 5663–5670. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, S.; Kaufman, S. Vincristine neurotoxicity. Ann. Intern. Med. 1974, 80, 733–737. [Google Scholar] [CrossRef] [PubMed]
- Verstappen, C.C.; Koeppen, S.; Heimans, J.J.; Huijgens, P.C.; Scheulen, M.E.; Strumberg, D.; Kiburg, B.; Postma, T.J. Dose-related vincristine-induced peripheral neuropathy with unexpected off-therapy worsening. Neurology 2005, 64, 1076–1077. [Google Scholar] [CrossRef] [PubMed]
- Moore, A.S.; Norris, R.; Price, G.; Nguyen, T.; Ni, M.; George, R.; van Breda, K.; Duley, J.; Charles, B.; Pinkerton, R. Vincristine pharmacodynamics and pharmacogenetics in children with cancer: A limited-sampling, population modelling approach. J. Paediatr. Child. Health. 2011, 47, 875–882. [Google Scholar] [CrossRef] [PubMed]
- Plasschaert, S.L.; Groninger, E.; Boezen, M.; Kema, I.; de Vries, E.G.; Uges, D.; Veerman, A.J.; Kamps, W.A.; Vellenga, E.; de Graaf, S.S.; et al. Influence of functional polymorphisms of the MDR1 gene on vincristine pharmacokinetics in childhood acute lymphoblastic leukemia. Clin. Pharmacol. Ther. 2004, 76, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Lavoie Smith, E.M.; Li, L.; Hutchinson, R.J.; Ho, R.; Burnette, W.B.; Wells, E.; Bridges, C.; Renbarger, J. Measuring vincristine-induced peripheral neuropathy in children with acute lymphoblastic leukemia. Cancer Nurs. 2013, 36, E49–E60. [Google Scholar] [CrossRef] [PubMed]
- Guo, P.; Wang, X.; Zhou, F.; Gallo, J.M. Determination of vincristine in mouse plasma and brain tissues by liquid chromatography–electrospray mass spectrometry. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2004, 809, 273–278. [Google Scholar] [CrossRef]
- Corona, G.; Casetta, B.; Sandron, S.; Vaccher, E.; Toffoli, G. Rapid and sensitive analysis of vincristine in human plasma using on-line extraction combined with liquid chromatography/tandem mass spectrometry. Rapid Commun. Mass Spectrom. 2008, 22, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Dennison, J.B.; Renbarger, J.L.; Walterhouse, D.O.; Jones, D.R.; Hall, S.D. Quantification of vincristine and its major metabolite in human plasma by high-performance liquid chromatography/tandem mass spectrometry. Ther. Drug Monit. 2008, 30, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Wang, H.; Hu, P.; Jiang, J. Validation of an UPLC-MS-MS Method for Quantitative Analysis of Vincristine in Human Urine After Intravenous Administration of Vincristine Sulfate Liposome Injection. J. Chromatogr. Sci. 2015, 53, 974–978. [Google Scholar] [CrossRef]
- Nabiabad, H.S.; Amini, M. Fabrication of an Impedimetric Immunosensor for Screening and Determination of Vincristine in Biological Samples. J. Anal. Chem. 2020, 75, 1094–1101. [Google Scholar] [CrossRef]
- Shah, V.P.; Midha, K.K.; Dighe, S.; McGilveray, I.J.; Skelly, J.P.; Yacobi, A.; Layloff, T.; Viswanathan, C.T.; Cook, C.E.; McDowall, R.D.; et al. Analytical methods validation: Bioavailability, bioequivalence, And Pharmacokinetic Studies. J. Pharm. Sci. 1992, 81, 309–312. [Google Scholar] [CrossRef]
- Yan, Z.; Zhu, Z.L.; Qian, Z.Z.; Hu, G.; Wang, H.Q.; Liu, W.H.; Cheng, G. Pharmacokinetic characteristics of vincristine sulfate liposomes in patients with advanced solid tumors. Acta Pharmacol. Sin. 2012, 33, 852–858. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Series | Level of DSP | Cexp [ng/mL] | SD [ng/mL] | CV |
|---|---|---|---|---|
| [ng/mL] | n = 5 | n = 5 | [%] | |
| 3.3 | 3.067 | 0.081 | 2.65 | |
| I | 50.17 | 44.301 | 1.208 | 2.74 |
| 167.23 | 173.805 | 5.438 | 3.14 | |
| 3.3 | 3.136 | 0.124 | 4.0 | |
| II | 50.17 | 44.72 | 0.49 | 1.10 |
| 167.23 | 172.559 | 5.937 | 3.41 |
| Patient Number | Concentration Level of VRC, ng/mL |
|---|---|
| 1 | 70.02 |
| 2 | 75.56 |
| 3 | 74.05 |
| 4 | 73.21 |
| 5 | 73.17 |
| 6 | 52.39 |
| 7 | 51.75 |
| 8 | 49.15 |
| 9 | 49.63 |
| 10 | 52.18 |
| 11 | 51.40 |
| 12 | 56.70 |
| 13 | 103.05 |
| 14 | 88.00 |
| 15 | 83.45 |
| 16 | 85.68 |
| 17 | 79.63 |
| 18 | 58.34 |
| 19 | 54.49 |
| 20 | 61.55 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jurowski, K.; Paprotny, Ł.; Zakrzewski, M.; Wianowska, D.; Kasprzyk-Pochopień, J.; Herman, M.; Madej, K.; Piekoszewski, W.; Kubrak, T. The Development of New Methodology for Determination of Vincristine (VCR) in Human Serum Using LC-MS/MS-Based Method for Medical Diagnostics. Molecules 2022, 27, 7945. https://doi.org/10.3390/molecules27227945
Jurowski K, Paprotny Ł, Zakrzewski M, Wianowska D, Kasprzyk-Pochopień J, Herman M, Madej K, Piekoszewski W, Kubrak T. The Development of New Methodology for Determination of Vincristine (VCR) in Human Serum Using LC-MS/MS-Based Method for Medical Diagnostics. Molecules. 2022; 27(22):7945. https://doi.org/10.3390/molecules27227945
Chicago/Turabian StyleJurowski, Kamil, Łukasz Paprotny, Marcin Zakrzewski, Dorota Wianowska, Joanna Kasprzyk-Pochopień, Małgorzata Herman, Katarzyna Madej, Wojciech Piekoszewski, and Tomasz Kubrak. 2022. "The Development of New Methodology for Determination of Vincristine (VCR) in Human Serum Using LC-MS/MS-Based Method for Medical Diagnostics" Molecules 27, no. 22: 7945. https://doi.org/10.3390/molecules27227945
APA StyleJurowski, K., Paprotny, Ł., Zakrzewski, M., Wianowska, D., Kasprzyk-Pochopień, J., Herman, M., Madej, K., Piekoszewski, W., & Kubrak, T. (2022). The Development of New Methodology for Determination of Vincristine (VCR) in Human Serum Using LC-MS/MS-Based Method for Medical Diagnostics. Molecules, 27(22), 7945. https://doi.org/10.3390/molecules27227945