
Pharmacological Approaches to the Treatment of Dementia in Down Syndrome: A Systematic Review of Randomized Clinical Studies


Abstract
:1. Introduction
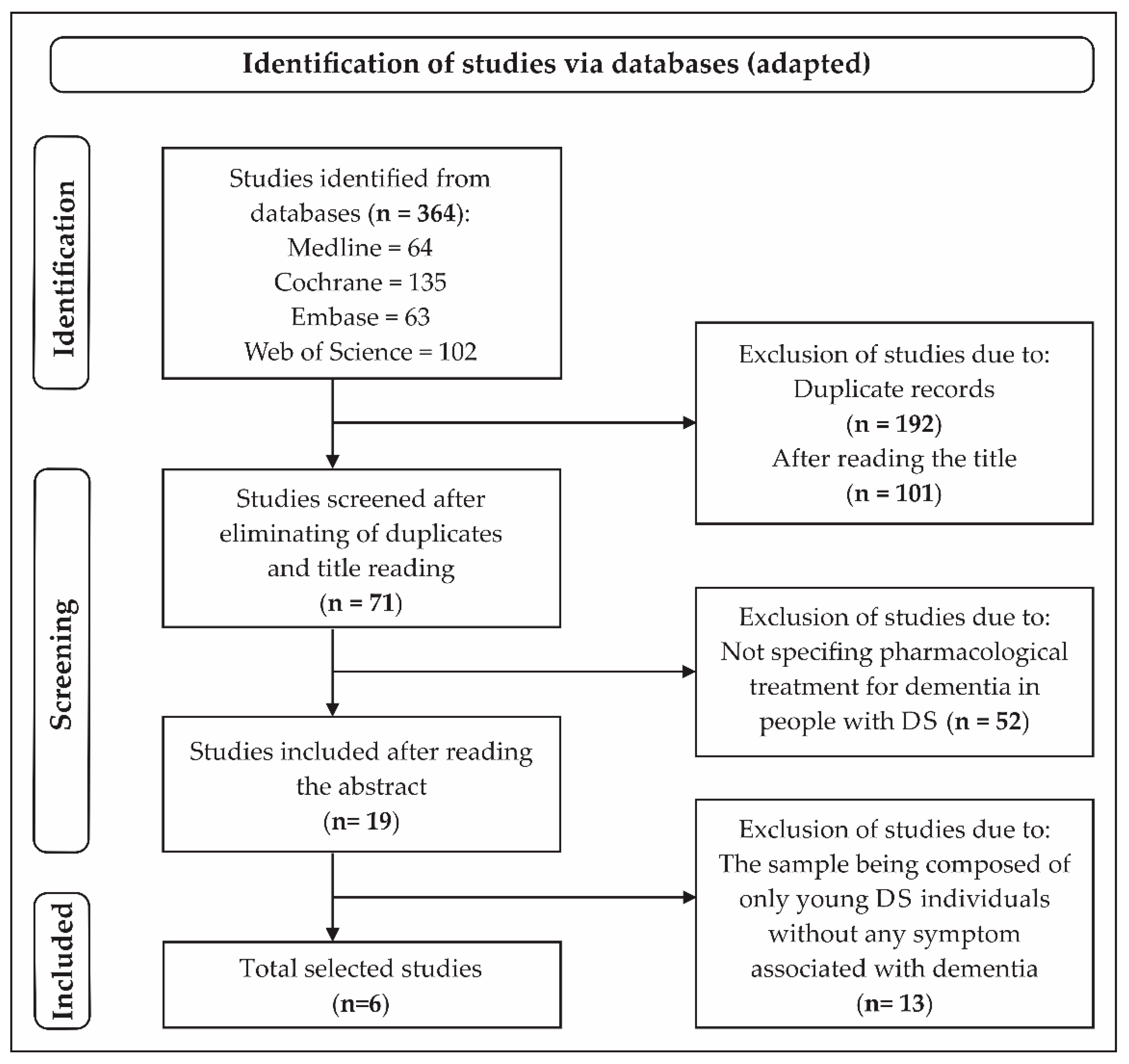
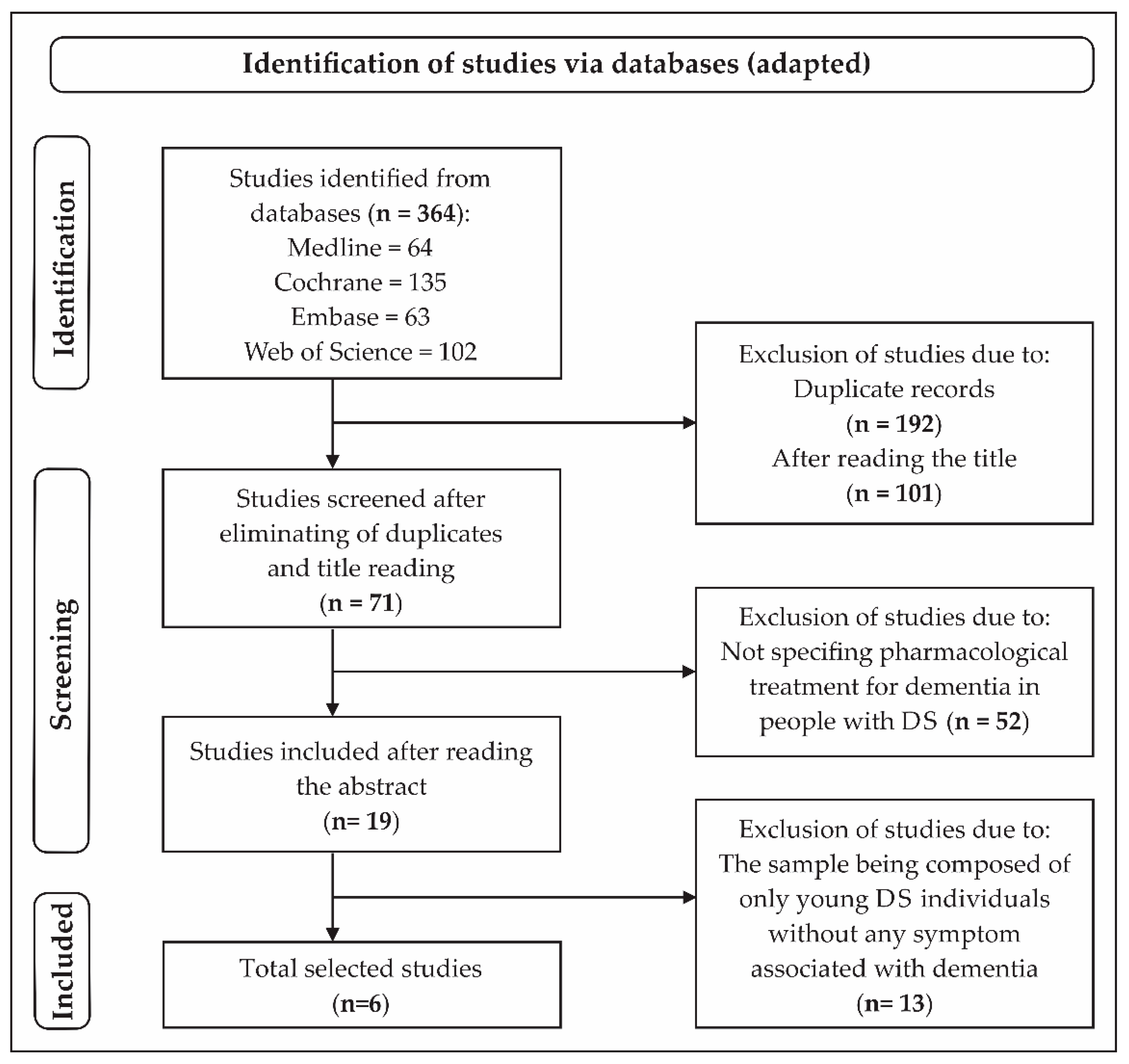
2. Materials and Methods
- -
- “Low risk of bias” = The trial is judged to be at a low risk of bias for all domains for this result.
- -
- “Unclear” = The trial is judged to raise some concerns in at least one domain for this result, but not to be at a high risk of bias for any domain.
- -
- “High risk of bias” = The trial is judged to be at a high risk of bias in at least one domain for this result.

{kind=link}
| Publication | Study Design | Participants | Pharmacological Treatment | Outcome | Main Conclusions | |||
|---|---|---|---|---|---|---|---|---|
| Age (Mean ± SD) | Sample Size (Participants with DS) | Drug | Dose | Duration | ||||
| Prasher et al. (2002) [27] | A randomized, double-blind, placebo-controlled study | 53 ± 8.03 | 30 | Donepezil | 5 mg per day during the first four weeks and then 10 mg per day thereafter | 24 weeks | ↓ NPI * (Improvement in the treated group although less significant than placebo group) | There is possible efficacy in the treatment of symptoms of mild to moderate AD with the use of donepezil in people with DS |
| Lott et a. (2011) [3] | A randomized, double-blind, placebo-controlled study | 50 ± 4.88 | 53 | Antioxidant supplementation | 900 IU Alpha tocopherol, 200 mg ascorbic acid followed by 600 mg alpha—lipoic acid. All participants received an associated acetylcholinesterase inhibitor | 2 years | DMR *, SIB *, DMR SOC *, BADLS *, and BPT * (No significant differences between groups) ↓ VABS * motor skills (Significant difference in the treated group in 2-year of treatment) | Antioxidant supplementation is safe, however, ineffective for the treatment of dementia in people with DS and dementia of the Alzheimer’s type |
| Kondoh et al. (2011) [28] | A randomized, double-blind, placebo-controlled clinical trial | 45 ** | 21 | Donepezil | 3 mg once daily throughout the trial | 24 weeks | ↑ ICF * (improvement only in the treated group) | Donepezil can help improve general functioning and severe cognitive impairment effectively and safely in people with DS |
| Hanney et al. (2012) [29] | A randomized, double-blind, placebo-controlled trial | 51 ± 7.3 | 173 | Memantine | The dose was escalated over 8 weeks from 5 mg per day to the optimal therapeutic dose of 10 mg per day with fixed titration | 52 weeks | DAMES *, ABS * Non-significant differences between the groups | Memantine is not an effective treatment for cognitive impairment and dementia in people older than 40 years with DS |
| Sano et al. (2016) [30] | A randomized, double-blind, controlled clinical trial | 54 ± 4.75 | 337 | Vitamin E | 1000 IU orally twice daily | 3 years | BPT * and memory tests (both verbal and visual), Vocabulary Test, Orientation Test, The Behavior & Function Questionnaire, and CGI-C * No differences between the groups | Vitamin E did not slow the progression of cognitive deterioration in DS |
| Rosenbloom et al. (2020) [4] | A single-center, single-dose, randomized, double-blind, placebo-controlled, crossover pilot study | 42 ± 1.7 | 12 | Intranasal insulin | A total of 0.20 mM of glulisine or placebo was administered using the POD® device to deliver 0.10 mL of agent in each nostril for a total of 20 IU | 8 weeks | ↑ RBMT * There was significant improvement in memory retention in the glulisine treated group and in immediate recall in the placebo group FOME * No significant impact in the groups | There was no significant impact of intranasal glulisine on learning, immediate recall, delayed recall, memory retention, recognition memory, and retention estimate |
| Random Sequence Generation | Allocation Concealment | Blinding of Participants and Personnel | Blinding of Outcome Assessment | Incomplete Outcome Data | Selective Reporting | Anything Else, Ideally Prespecified | |
|---|---|---|---|---|---|---|---|
| Prasher et al. (2002) [27] | Low | Low | Low | Low | Low | Low | Low |
| Lott et al. (2011) [3] | Low | Low | Low | Low | Low | Low | Low |
| Kondoh et al. (2011) [28] | Low | Low | Low | Low | Low | Low | Low |
| Hanney et al. (2012) [29] | Low | Low | Low | Low | Low | Low | Low |
| Sano et al. (2016) [30] | Low | Low | Low | Unclear | Low | Unclear | Low |
| Rosenbloom et al. (2020) [4] | Low | Low | Low | Unclear | Low | Low | Low |
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sinet, P.M.; Theopile, D.; Rahmani, Z.; Chettouch, Z.; Blovin, J.L.; Prier, M.; Noel, B.; Delabar, J.M. Mapping of Down syndrome phenotype on chromosome 21 at themolecular level. Biomed. Pharmacother. 1994, 48, 247–252. [Google Scholar] [CrossRef]
- Asim, A.; Kumar, A.; Muthuswamy, S.; Jain, S.; Agarwal, S. Down syndrome: An insight of the disease. J. Biomed.Sci. 2015, 22, 41–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lott, I.T.; Doran, E.; Nguyen, V.Q.; Tournay, A.; Head, E.; Gillen, D.L. Down syndrome and dementia: A randomized, controlled trial of antioxidant supplementation. Am. J. Med. Genet. Part A 2011, 155, 1939–1948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenbloom, M.; Barclay, T.; Johnsen, J.; Erickson, L.; Svitak, A.; Pyle, M.; Frey, W.; Hanson, L.R. Double-Blind Placebo-Controlled Pilot Investigation of the Safety of a Single Dose of Rapid-Acting Intranasal Insulin in Down Syndrome. Drugs RD 2020, 20, 11–15. [Google Scholar] [CrossRef] [Green Version]
- Parizot, E.; Dard, R.; Janel, N.; Vialard, F. Down syndrome and infertility: What support should we provide? J. Assist. Reprod. Genet. 2019, 36, 1063–1067. [Google Scholar] [CrossRef]
- Bittles, A.H.; Bower, C.; Hussain, R.; Glasson, E.J. The four ages of Down syndrome. Eur. J. Public Health 2007, 17, 221–225. [Google Scholar] [CrossRef]
- Rafii, M.S.; Santoro, S.L. Prevalence and Severity of Alzheimer Disease in Individuals with Down Syndrome. JAMA Neurol. 2019, 76, 142–143. [Google Scholar] [CrossRef]
- Rumble, B. Retallak, R. Amyloid A4 and its precursor in Down’s syndrome and Alzheimer’s disease. N. Engl. J. 1989, 320, 1446–1452. [Google Scholar] [CrossRef]
- Strydom, A.; Coppus, A.; Blesa, R.; Danek, A.; Fortea, J.; Hardy, J.; Levin, J.; Nuebling, G.; Rebillat, A.S.; Ritchie, C.; et al. Alzheimer’s disease in Down syndrome: An overlooked population for prevention trials. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2018, 4, 703–713. [Google Scholar] [CrossRef]
- Cody, K.A.; Piro-Gambetti, B.; Zammit, M.D.; Christian, B.T.; Handen, B.L.; Klunk, W.E.; Zaman, S.; Johnson, S.C.; Plante, D.T.; Hartley, S.L. Association of sleep with cognition and beta amyloid accumulation in adults with Down syndrome. Neurobiol. Aging 2020, 93, 44–51. [Google Scholar] [CrossRef]
- Startin, C.M.; Hamburg, S.; Hithersay, R.; Al-Janabi, T.; Mok, K.Y.; Hardy, J.; Strydom, A.; Fisher, E.; Nizetic, D.; Tybulewicz, V.; et al. Cognitive markers of preclinical and prodromal Alzheimer’s disease in Down syndrome. Alzheimers Dement. 2019, 15, 245–257. [Google Scholar] [CrossRef] [PubMed]
- Dekker, A.D.; Sacco, S.; Carfi, A.; Benejam, B.; Vermeiren, Y.; Beugelsdijk, G.; Schippers, M.; Hassefras, L.; Eleveld, J.; Grefelman, S.; et al. The Behavioral and Psychological Symptoms of Dementia in Down Syndrome (BPSD-DS) Scale: Comprehensive Assessment of Psychopathology in Down Syndrome. J. Alzheimer’s Dis. 2018, 63, 797–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiseman, K.; Al-Janabi, T.; Hardy, J.; Karmiloff-Smith, A.; Nizetic, D.; Tybulewicz, V.L.; Fisher, E.; Strydom, A. A genetic cause of Alzheimer disease: Mechanistic insights from Down syndrome. Nat. Rev. Neurosci. 2015, 16, 564–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiseman, F.K.; Pulford, L.J.; Barkus, C.; Liao, F.; Portelius, E.; Webb, R.; Chávez-Gutiérrez, L.; Cleverley, K.; Noy, S.; Sheppard, O.; et al. Trisomy of human chromosome 21 enhances amyloid-beta deposition independently of an extra copy of APP. Brain 2018, 141, 2457–2474. [Google Scholar] [CrossRef] [Green Version]
- Cacace, R.; Sleegers, K.; Van Broeckhoven, C. Molecular genetics of early-onset Alzheimer’s disease revisited. Alzheimers Dement. 2016, 12, 733–748. [Google Scholar] [CrossRef] [Green Version]
- Wisniewski, K.E.; Wisniewski, H.M.; Wen, G.Y. Occurrence of neuropathological changes and dementia of Alzheimer’s disease in Down’s syndrome. Ann. Neurol. 1985, 17, 278–282. [Google Scholar] [CrossRef]
- Davidson, Y.S.; Robinson, A.; Prasher, V.P.; Mann, D.M.A. The age of onset and evolution of Braak tangle stage and Thal amyloid pathology of Alzheimer’s disease in individuals with Down syndrome. Acta Neuropathol. Commun. 2018, 6, 56. [Google Scholar] [CrossRef]
- Mann, D.M. The pathological association between Down syndrome and Alzheimer disease. Mech. Ageing Dev. 1988, 43, 99–136. [Google Scholar] [CrossRef]
- Griffiths-Jones, S. The microRNA Registry. Nucleic Acids Res. 2004, 32, D109–D111. [Google Scholar] [CrossRef]
- Rachidi, M.; Lopes, C. Molecular and cellular mechanisms elucidating neurocognitive basis of functional impairments associated with intellectual disability in Down syndrome. Am. J. Intellect. Dev. Disabil. 2010, 115, 83–112. [Google Scholar] [CrossRef]
- Della Ragione, F.; Gagliardi, M.; D’Esposito, M.; Matarazzo, M.R. Non-coding RNAs in chromatin disease involving neurological defects. Front. Cell Neurosci. 2014, 8, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamlett, E.D.; Ledreux, A.; Potter, H.; Chial, H.J.; Patterson, D.; Espinosa, J.M.; Bettcher, B.M.; Granholm, A.C. Exosomal biomarkers in Down syndrome and Alzheimer’s disease. Free Radic. Biol. Med. 2018, 114, 110–121. [Google Scholar] [CrossRef] [PubMed]
- Matsuoka, Y.; Andrews, H.F.; Becker, A.G.; Gray, A.J.; Mehta, P.D.; Sano, M.C.; Dalton, A.J.; Aisen, P.S. The relationship of plasma Abeta levels to dementia in aging individuals with Down syndrome. Alzheimer Dis. Assoc. Disord. 2009, 23, 315–318. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; Cochrane: London, UK, 2021. Available online: www.training.cochrane.org/handbook (accessed on 24 February 2022).
- Prasher, V.P.; Huxley, A.; Haque, M.S.; Down Syndrome Ageing Study Group. A 24-week, double-blind, place-controlled trial of donepezil in patients with Down syndrome and Alzheimer’s disease—Pilot study. Int. J. Geriatr. Psychiatry 2002, 17, 270–278. [Google Scholar]
- Kondoh, T.; Kanno, A.; Itoh, H.; Nakashima, M.; Honda, R.; Kojima, M.; Noguchi, M.; Nakane, H.; Nozaki, H.; Sasaki, H.; et al. Donepezil significantly improves abilities in daily lives of female down syndrome patients with severe cognitive impairment: A 24-week randomized, double-blind, placebo-controlled trial. Int. J. Psychiatry Med. 2011, 41, 71–89. [Google Scholar] [CrossRef]
- Hanney, M.; Prasher, V.; Williams, N.; Jones, E.L.; Aarsland, D.; Corbett, A.; Lawrence, D.; Yu, L.M.; Tyrer, S.; Francis, P.T.; et al. Memantine for dementia in adults older than 40 years with Down’s syndrome (MEADOWS): A randomised, double-blind, placebo-controlled trial. Lancet 2012, 379, 528–536. [Google Scholar] [CrossRef]
- Sano, M.; Aisen, P.S.; Andrews, H.F.; Tsai, W.; Lai, F.; Dalton, A.J. Vitamin E in Aging Persons with Down Syndrome. Neurology 2016, 86, 2071–2076. Available online: https://clinicaltrials.gov/ct2/show/NCT00056329. (accessed on 3 November 2021). [CrossRef]
- Daly, B.; Watt, R.; Batchelor, P.; Treasure, E. Essential Dental Public Health; Oxford Press University: New York, NY, USA, 2002. [Google Scholar]
- Leavell, H.R. Planejamento para a Saúde Comunitária. In Medicina Preventiva; Leavell, H.R., Clark, E.G., Eds.; MacGrawHill: Sao Paolo, Brazil, 1976; pp. 666–677. [Google Scholar]
- Ellis, J.M.; Tan, H.K.; Gilbert, R.E.; Muller, D.P.R.; Henley, W.; Moy, R.; Pumphrey, R.; Ani, C.; Davies, S.; Edwards, V.; et al. Supplementation with antioxidants and folinic acid for children with Down’s syndrome: Randomised controlled trial. BMJ 2008, 336, 594–597. [Google Scholar] [CrossRef] [Green Version]
- Castro, P.; Zaman, S.; Holland, A. Alzheimer’s disease in people with Down’s syndrome: The prospects for and the challenges of developing preventative treatments. J. Neurol. 2017, 264, 804–813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brigelius-Flohe, R.; Traber, M.G. Vitamin E: Function and metabolism. FASEB J. 1999, 13, 1145–1155. [Google Scholar] [CrossRef] [PubMed]
- Reiter, E.; Jiang, Q.; Christen, S. Anti-inflammatory properties ofα- andγ-tocopherol. Mol. Asp. Med. 2007, 28, 668–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, Q. Natural forms of vitamin E: Metabolism, antioxidant, and anti-inflammatory activities and theirrole in disease prevention and therapy. Free Radic. Biol. Med. 2014, 72, 76–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, L.; Davis, T.A.; Porter, N.A. Rate constants for peroxidation of polyunsaturated fatty acids and sterols insolution and in liposomes. J. Am. Chem. Soc. 2009, 131, 13037–13044. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersen, R.C.; Thomas, R.G.; Grundman, M.; Bennett, D.; Doody, R.; Ferris, S.; Galasko, D.; Jin, S.; Kaye, J.; Levey, A.; et al. Vitamin E and donepezil for the treatment of mild cognitive impairment. N. Engl. J. Med. 2005, 352, 2379–2388. [Google Scholar] [CrossRef] [Green Version]
- Lu, S.; Nasrallah, H.A. The use of memantine in neuropsychiatric disorders: An overview. Ann. Clin. Psychiatry 2018, 30, 234–248. [Google Scholar]
- Kishi, T.; Matsunaga, S.; Oya, K.; Nomura, I.; Ikuta, T.; Iwata, N. Memantine for Alzheimer’s Disease: An Updated Systematic Review and Meta-analysis. J. Alzheimers Dis. 2017, 60, 401–425. [Google Scholar] [CrossRef]
- Lott, I.T.; Osann, K.; Doran, E.; Nelson, L. Down syndrome and Alzheimer’s disease: Response to donepezil. Arch. Neurol. 2002, 59, 1133–1136. [Google Scholar] [CrossRef]
- Boada, R.; Hutaff-Lee, C.; Schrader, A.; Weitzenkamp, D.; Benke, T.A.; Goldson, E.J.; Costa, A.C. Antagonism of NMDA receptors as a potential treatment for Down syndrome: A pilot randomized controlled trial. Transl Psychiatry 2012, 2, e141. [Google Scholar] [CrossRef] [Green Version]
- Costa, A.C.S.; Brandão, A.C.; Boada, R.; Barrionuevo, V.L.; Taylor, H.G.; Roth, E.; Stasko, M.R.; Johnson, M.W.; Assir, F.F.; Roberto, M.P.; et al. Safety, efficacy, and tolerability of memantine for cognitive and adaptive outcome measures in adolescents and young adults with Down syndrome: A randomised, double-blind, placebo-controlled phase 2 trial. Lancet Neurol. 2022, 21, 31–41. [Google Scholar] [CrossRef]
- Berlanga-Acosta, J.; Guillén-Nieto, G.; Rodríguez-Rodríguez, N.; Bringas-Vega, M.L.; García-del-Barco-Herrera, D.; Berlanga-Saez, J.O.; García-Ojalvo, A.; Valdés-Sosa, M.J.; Valdés-Sosa, P.A. Insulin Resistance at the Crossroad of Alzheimer Disease Pathology: A Review. Front. Endocrinol. 2020, 11, 560375. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Clinical Excellence. Donepezil, Galantamine, Riv-Astigmine (Review) and Memantine for the Treatment of Alzheimer’s Disease (Amended); NICE technology Appraisal Guidanc 111 (Amended); National Health Service: London, UK, 2007.
- Clegg, A.; Bryant, J.; Nicholson, T.; McIntyre, L.; De Broe, S.; Gerard, K.; Waugh, N. Clinical and cost-effectiveness of donepezil, rivastigmine, and galantamine for Alzheimer’s disease. A systematic review. Int. J. Technol. Assess. Health Care 2002, 18, 497–507. [Google Scholar] [CrossRef] [PubMed]
- Prasher, V.P. Review of donepezil, rivastigmine, galantamine and memantine for the treatment of dementia in Alzheimer’s disease in adults with Down syndrome: Implications for the intellectual disability population. Int. J. Geriatr. Pshychiatry 2004, 19, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Mohan, M.; Bennett, C.; Carpenter, P.K. Galantamine for dementia in people with Down syndrome. Cochrane Database Syst. Rev. 2009, CD007656. [Google Scholar] [CrossRef]
- Mohan, M.; Bennett, C.; Carpenter, P.K. Rivastigmine for dementia in people with Down syndrome. Cochrane Database Syst. Rev. 2009, CD007656. [Google Scholar] [CrossRef]
- Lee, Y.H.; Im, E.; Hyun, M.; Park, J.; Chung, K.C. Protein phosphatase PPM1B inhibits DYRK1A kinase through dephosphorylation of pS258 and reduces toxic tau aggregation. J. Biol. Chem. 2021, 296, 100245. [Google Scholar] [CrossRef]
- Nelly Pitteloud, Centre Hospitalier Universitaire Vaudois Clinical Trials Registry [Internet]: Nelly Pitteloud: Clinical Trials Centre, Universitaire Vaudois (Suiça). Identifier NCT04390646 History of Changes. GnRH Therapy on Cognition in Down Syndrome. 31 August 2020; Status: In Recruitment. Available online: https://clinicaltrials.gov/ct2/show/NCT04390646 (accessed on 22 April 2022).
- Rondal, J.A. Down syndrome: A curative prospect? AIMS Neurosci. 2020, 7, 168–193. [Google Scholar] [CrossRef]
- Park, J.; Song, W.J.; Chung, K.C. Function and regulation of Dyrk1A: Towards understanding Down syndrome. Cell Mol. Life Sci. 2009, 66, 3235–3240. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Oliveira, L.C.; de Paula Faria, D. Pharmacological Approaches to the Treatment of Dementia in Down Syndrome: A Systematic Review of Randomized Clinical Studies. Molecules 2022, 27, 3244. https://doi.org/10.3390/molecules27103244
de Oliveira LC, de Paula Faria D. Pharmacological Approaches to the Treatment of Dementia in Down Syndrome: A Systematic Review of Randomized Clinical Studies. Molecules. 2022; 27(10):3244. https://doi.org/10.3390/molecules27103244
Chicago/Turabian Stylede Oliveira, Laura Cavalcanti, and Daniele de Paula Faria. 2022. "Pharmacological Approaches to the Treatment of Dementia in Down Syndrome: A Systematic Review of Randomized Clinical Studies" Molecules 27, no. 10: 3244. https://doi.org/10.3390/molecules27103244
APA Stylede Oliveira, L. C., & de Paula Faria, D. (2022). Pharmacological Approaches to the Treatment of Dementia in Down Syndrome: A Systematic Review of Randomized Clinical Studies. Molecules, 27(10), 3244. https://doi.org/10.3390/molecules27103244