
Quo Vadis Advanced Prostate Cancer Therapy? Novel Treatment Perspectives and Possible Future Directions

 ,
,  and
and 
Abstract
1. Introduction
2. Prostate Cancer Treatment
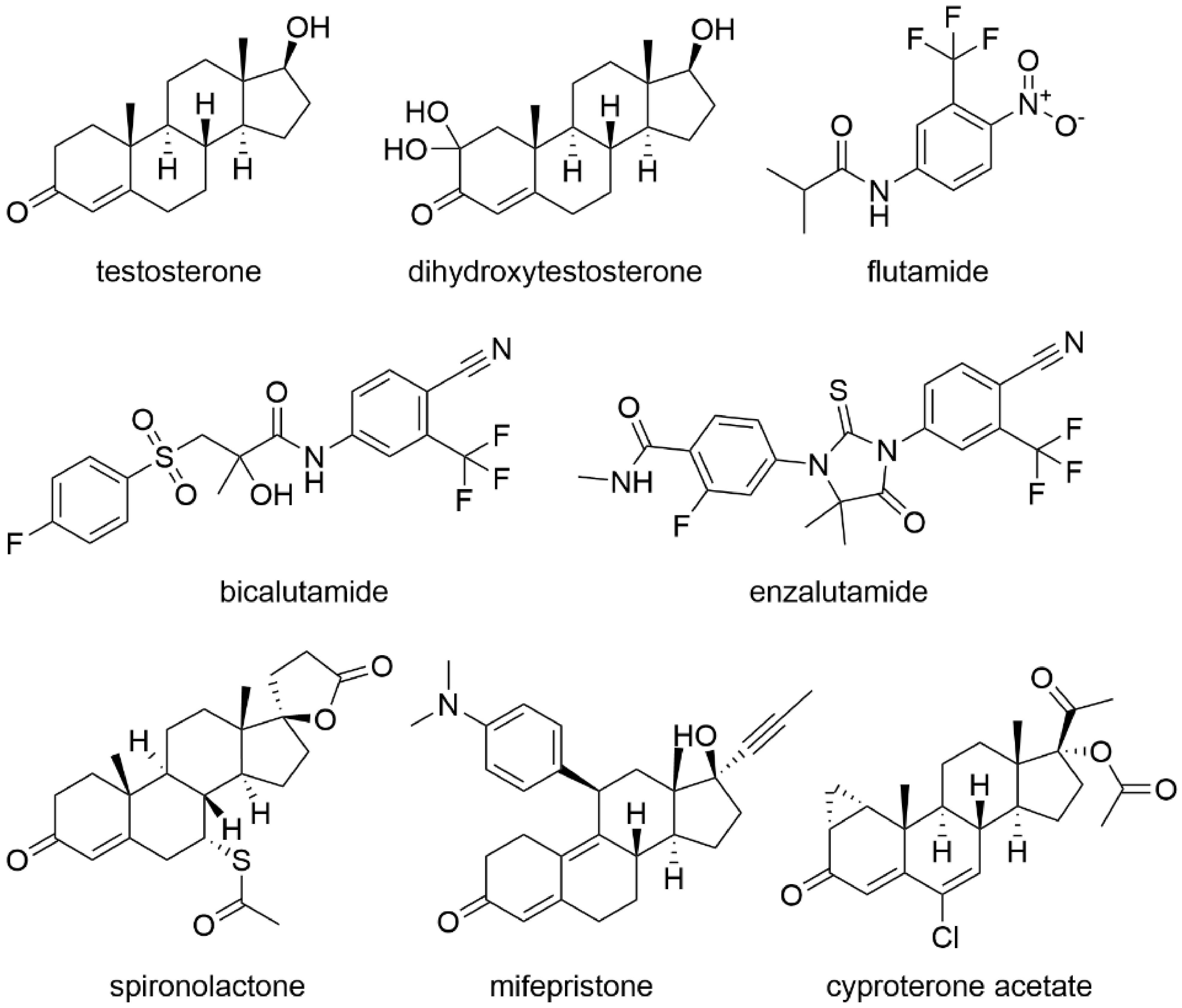
2.1. Treatment with Antiandrogens
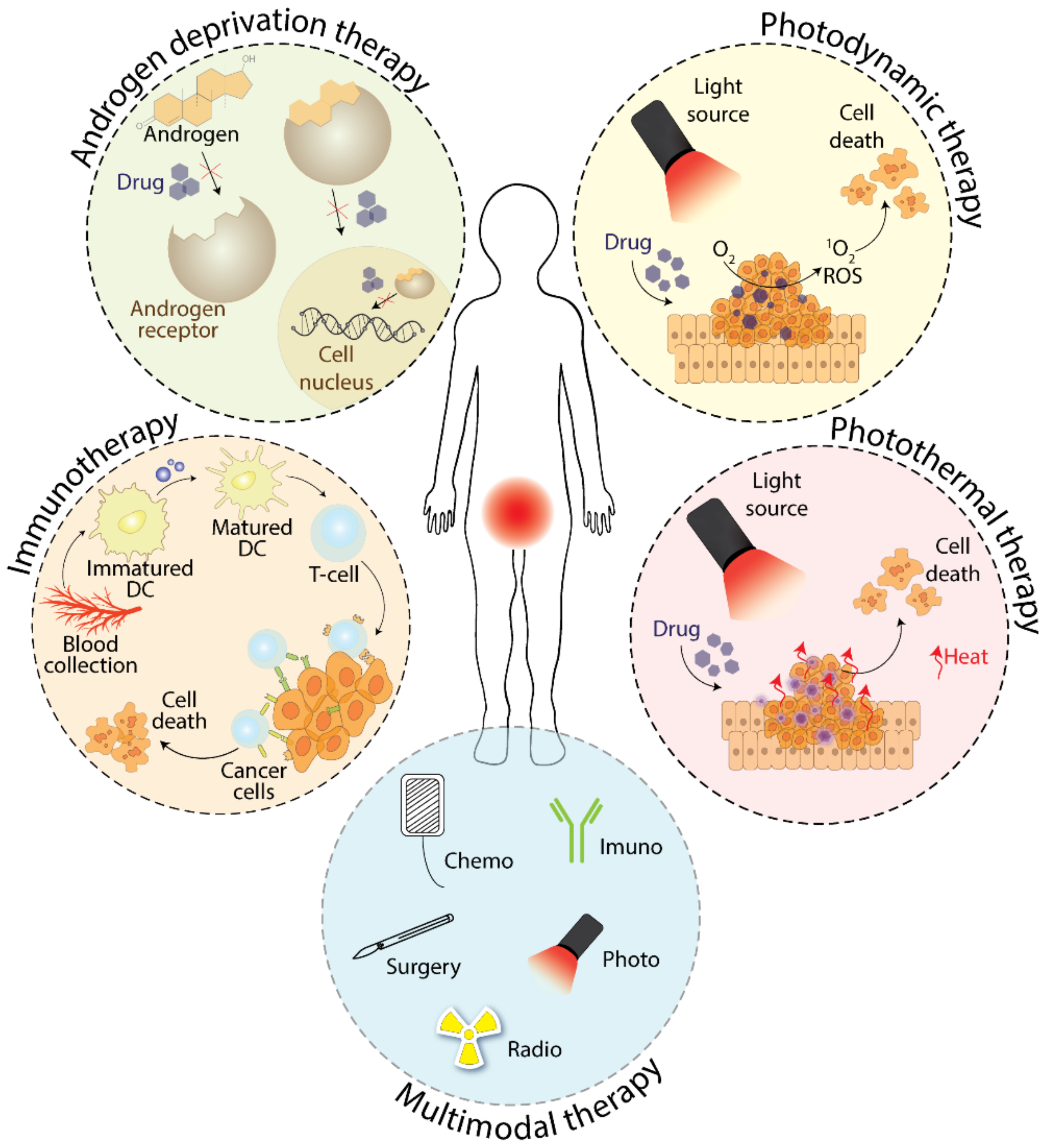
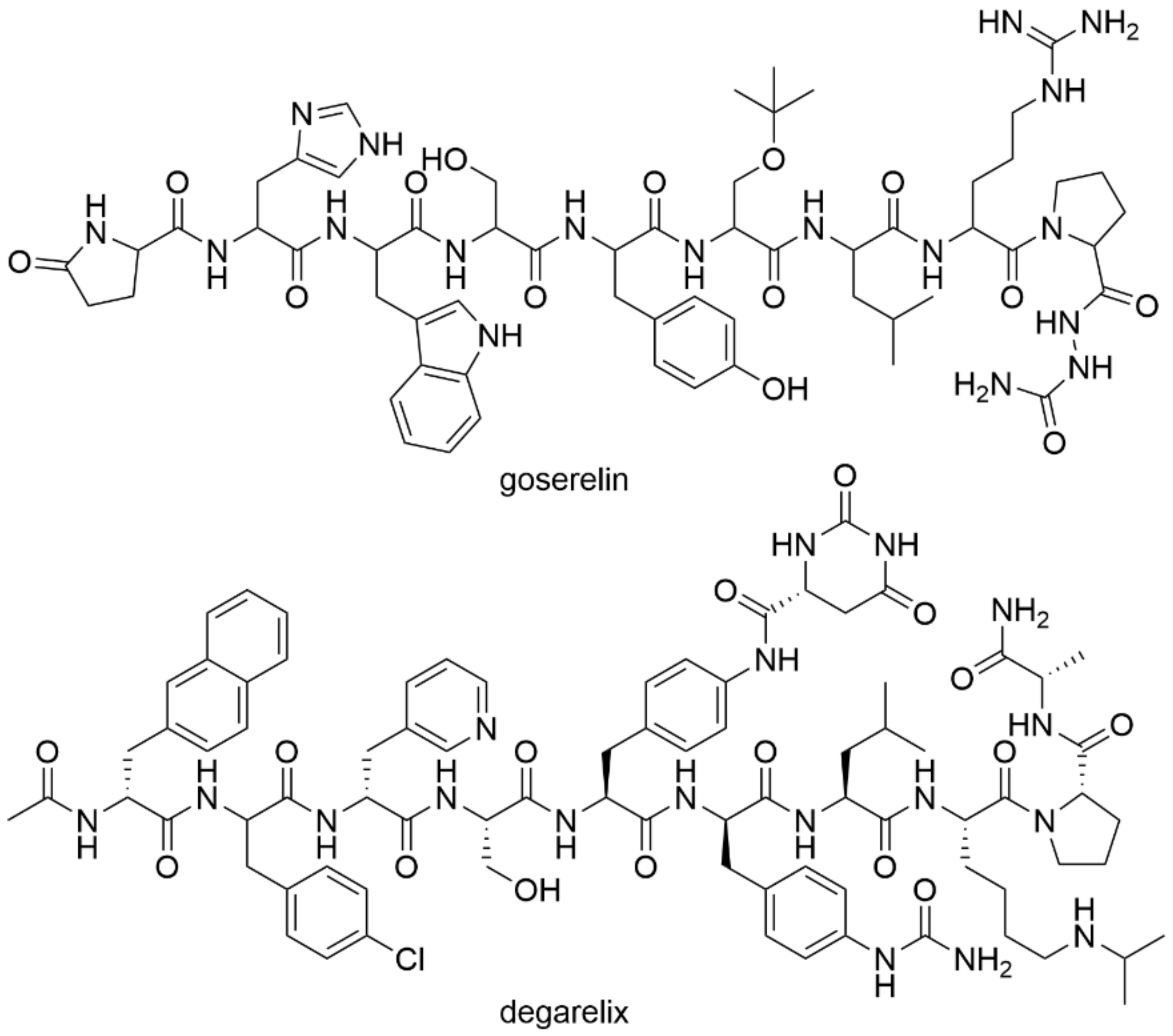
2.2. Treatment with Androgen Deprivation
3. Phototherapy as a Tool for Prostate Cancer Treatment
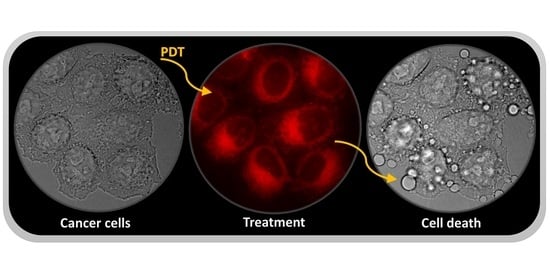
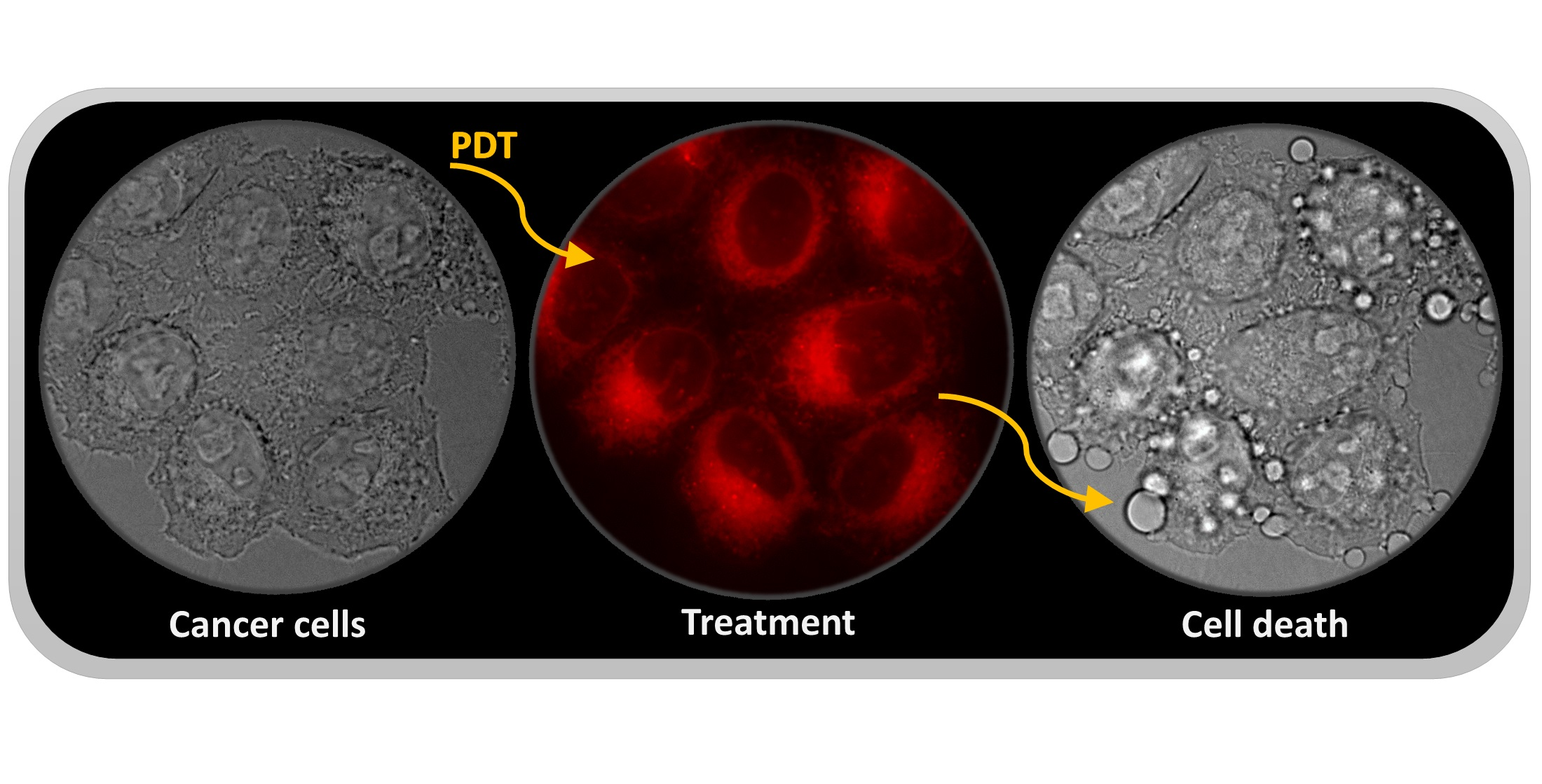
3.1. Photodynamic Therapy
3.2. Photothermal Therapy
4. Immunotherapy in the Therapy of Prostate Cancer
5. Multimodal Therapy of Prostate Cancer
6. Poly(ADP-Ribose) Polymerase Inhibitors
7. Akt Inhibitors
8. Cyclin-Dependent Kinase Inhibitors
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ADT | Androgen-deprivation therapy |
| Akt | Protein kinase B |
| AR | The androgen receptor |
| AuNC SiO2 | Silica-coated gold-nanoparticle clusters |
| CAR T | Chimeric antigen receptor T-cell therapy |
| CDK | Cyclin-dependent kinase |
| CPA | Cyproterone acetate |
| CRPC | Castration-resistant prostate cancer |
| CTLA-4 | Cytotoxic T-lymphocyte antigen 4 (CD152) |
| CYP17A1 | Cytochrome P450-17A1 |
| DC | Dendritic cells |
| DCVAC/PCa | Autologous active cellular immunotherapy based on activated dendritic cells |
| DHT | Dihydroxytestosterone |
| DU145 | Human cells from prostate carcinoma |
| EMA | European medicines agency |
| FDA | U.S. Food and Drug Administration |
| FSH | Follicle-stimulating hormone |
| GCPII | Glutamate carboxypeptidase II |
| GNPs | Gold nanoparticles |
| HER2/neu | Receptor tyrosine-protein kinase erbB-2 |
| LH | Luteinizing hormone |
| LHRH | Luteinizing hormone-releasing hormone |
| LNCaP | Human cells from prostate carcinoma |
| mCRPC | Metastatic CRPC |
| NNALADase I | N-acetyl-L-aspartyl-L-glutamate peptidase I |
| PAP | Prostatic acid phosphatase |
| PARP | Poly(ADP-ribose) polymerase |
| PARPi | Poly(ADP-ribose) polymerase inhibitors |
| PC-3 | Human cells from prostate carcinoma |
| PD-1 | Programmed cell death 1 receptor (CD279) |
| PD-L1 | Ligand 1 of programmed cell death receptor |
| PD-L2 | Ligand 2 of programmed cell death receptor |
| PDT | Photodynamic therapy |
| PIP3 | Phosphatidylinositol-3,4,5-trisphosphate |
| PS | Photosensitizer |
| PSA | Prostate-specific antigen |
| PSMA | Prostate-specific membrane antigen |
| PTEN | Phosphatase and tensin homologue |
| PTT | Photothermal therapy |
| ROS | Reactive oxygen species |
| SPECT | Single-photon emission computed tomography |
| VGFA | Vascular endothelial growth factor |
| VTP | Vascular-targeted photodynamic therapy |
References
- Lonergan, P.E.; Tindall, D.J. Androgen receptor signaling in prostate cancer development and progression. J. Carcinog. 2011, 10, 20. [Google Scholar] [CrossRef] [PubMed]
- Schaufele, F.; Carbonell, X.; Guerbadot, M.; Borngraeber, S.; Chapman, M.S.; Ma, A.A.; Miner, J.N.; Diamond, M.I. The structural basis of androgen receptor activation: Intramolecular and intermolecular amino-carboxy interactions. Proc. Natl. Acad. Sci. USA 2005, 102, 9802–9807. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J. The role of antiandrogen monotherapy in the treatment of prostate cancer. BJU Int. 2003, 91, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Potosky, A.L.; Knopf, K.; Clegg, L.X.; Albertsen, P.C.; Stanford, J.L.; Hamilton, A.S.; Gilliland, F.D.; Eley, J.W.; Stephenson, R.A.; Hoffman, R.M. Quality-of-life outcomes after primary androgen deprivation therapy: Results from the prostate cancer outcomes study. J. Clin. Oncol. 2001, 19, 3750–3757. [Google Scholar] [CrossRef]
- Harris, W.P.; Mostaghel, E.A.; Nelson, P.S.; Montgomery, B. Androgen deprivation therapy: Progress in understanding mechanisms of resistance and optimizing androgen depletion. Nat. Clin. Pract. Urol. 2009, 6, 76–85. [Google Scholar] [CrossRef]
- Iversen, P. Antiandrogen monotherapy: Indications and results. Urology 2002, 60, 64–71. [Google Scholar] [CrossRef]
- Singh, S.M.; Gauthier, S.; Labrie, F. Androgen receptor antagonists (antiandrogens): Structure-activity relationships. Curr. Med. Chem. 2000, 7, 211–247. [Google Scholar] [CrossRef]
- Rice, M.A.; Malhotra, S.V.; Stoyanova, T. Second-generation antiandrogens: From discovery to standard of care in castration resistant prostate cancer. Front Oncol. 2019, 9, 801. [Google Scholar] [CrossRef]
- Kenny, B.; Ballard, S.; Blagg, J.; Fox, D. Pharmacological options in the treatment of benign prostatic hyperplasia. J. Med. Chem. 1997, 40, 1293–1315. [Google Scholar] [CrossRef]
- Schellhammer, P.; Sharifi, R.; Block, N.; Soloway, M.; Venner, P.; Patterson, A.L.; Sarosdy, M.; Vogelzang, N.; Jones, J.; Kolvenbag, G. A controlled trial of bicalutamide versus flutamide, each in combination with luteinizing hormone-releasing hormone analogue therapy, in patients with advanced prostate cancer. Urology 1995, 45, 745–752. [Google Scholar] [CrossRef]
- Ito, Y.; Sadar, M.D. Enzalutamide and blocking androgen receptor in advanced prostate cancer: Lessons learnt from the history of drug development of antiandrogens. Res. Rep. Urol. 2018, 10, 23–32. [Google Scholar] [CrossRef]
- Rathkopf, D.; Scher, H.I. Androgen receptor antagonists in castration-resistant prostate cancer. Cancer, J. 2013, 19, 43–49. [Google Scholar] [CrossRef]
- Tan, P.S.; Haaland, B.; Montero, A.J.; Kyriakopoulos, C.E.; Lopes, G. Enzalutamide and abiraterone acetate in the treatment of metastatic castration-resistant prostate cancer (mCRPC) post-docetaxel-an indirect comparison. Clin. Med. Insights Oncol. 2014, 8, 29–36. [Google Scholar] [CrossRef]
- Tran, C.; Ouk, S.; Clegg, N.J.; Chen, Y.; Watson, P.A.; Arora, V.; Wongvipat, J.; Smith-Jones, P.M.; Yoo, D.; Kwon, A.; et al. Development of a second-generation antiandrogen for treatment of advanced prostate cancer. Science 2009, 324, 787–790. [Google Scholar] [CrossRef]
- FDA. Available online: http://www.fda.gov (accessed on 1 November 2019).
- Rathkopf, D.E.; Scher, H.I. Apalutamide for the treatment of prostate cancer. Expert Rev. Anticancer Ther. 2018, 18, 823–836. [Google Scholar] [CrossRef]
- Shore, N.D. Darolutamide (ODM-201) for the treatment of prostate cancer. Expert Opin. Pharmacother. 2017, 18, 945–952. [Google Scholar] [CrossRef]
- Attard, G.; Reid, A.H.; Yap, T.A.; Raynaud, F.; Dowsett, M.; Settatree, S.; Barrett, M.; Parker, C.; Martins, V.; Folkerd, E.; et al. Phase I clinical trial of a selective inhibitor of CYP17, abiraterone acetate, confirms that castration-resistant prostate cancer commonly remains hormone driven. J. Clin. Oncol. 2008, 26, 4563–4571. [Google Scholar] [CrossRef]
- Clegg, N.J.; Wongvipat, J.; Joseph, J.D.; Tran, C.; Ouk, S.; Dilhas, A.; Chen, Y.; Grillot, K.; Bischo, E.D.; Cail, L.; et al. ARN-509: A novel antiandrogen for prostate cancer treatment. Cancer Res. 2012, 72, 1494–1503. [Google Scholar] [CrossRef]
- Moilanen, A.M.; Riikonen, R.; Oksala, R.; Ravanti, L.; Aho, E.; Wohlfahrt, G.; Nykänen, P.S.; Törmäkangas, O.P.; Palvimo, J.J.; Kallioa, P.J. Discovery of ODM-201, a new-generation androgen receptor inhibitor targeting resistance mechanisms to androgen signaling-directed prostate cancer therapies. Sci. Rep. 2015, 5, 12007. [Google Scholar] [CrossRef]
- Chen, Y.; Clegg, N.J.; Scher, H.I. Anti-androgens and androgen-depleting therapies in prostate cancer: New agents for an established target. Lancet Oncol. 2009, 10, 981–991. [Google Scholar] [CrossRef]
- Hammerer, P.; Madersbacher, S. Landmarks in hormonal therapy for prostate cancer. BJU Int. 2012, 110, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Abraham, J.; Staffurth, J. Hormonal therapy for cancer. Medicine 2016, 44, 30–33. [Google Scholar] [CrossRef]
- Pullar, B.; Shah, N. Prostate cancer. Surgery 2016, 34, 505–511. [Google Scholar] [CrossRef]
- Omlin, A.; Pezaro, C.; Mukherji, D.; Cassidy, A.M.; Sandhu, S.; Bianchini, D.; Olmos, D.; Ferraldeschi, R.; Maier, G.; Thompson, E.; et al. Improved survival in a cohort of trial participants with metastatic castration-resistant prostate cancer demonstrates the need for updated prognostic nomograms. Eur. Urol. 2013, 64, 300–306. [Google Scholar] [CrossRef]
- Schally, A.V.; Block, N.L.; Rick, F.G. New therapies for relapsed castration-resistant prostate cancer based on peptide analogs of hypothalamic hormones. Asian, J. Androl. 2015, 17, 925–928. [Google Scholar] [CrossRef]
- Kotake, T.; Usami, M.; Akaza, H.; Koiso, K.; Homma, Y.; Kawabe, K.; Aso, Y.; Orikasa, S.; Shimazaki, J.; Isaka, S.; et al. Goserelin acetate with or without antiandrogen or estrogen in the treatment of patients with advanced prostate cancer: A multicenter, randomized, controlled trial in Japan. Jpn. J. Clin. Oncol. 1999, 29, 562–570. [Google Scholar] [CrossRef][Green Version]
- FDA. Available online: http://www.accessdata.fda.gov (accessed on 6 November 2019).
- Heidenreich, A.; Bellmunt, J.; Bolla, M.; Joniau, S.; Mason, M.; Matveev, V.; Mottet, N.; Schmid, H.P.; van der Kwast, T.; Wiegel, T.; et al. EAU guidelines on prostate cancer. Part 1: Screening, diagnosis, and treatment of clinically localised disease. Eur. Urol. 2011, 59, 61–71. [Google Scholar] [CrossRef]
- Klotz, L.; Miller, K.; Crawford, E.D.; Shore, N.; Tombal, B.; Karup, C.; Malmberg, A.; Persson, B.E. Disease control outcomes from analysis of pooled individual patient data from five comparative randomised clinical trials of degarelix versus luteinising hormone-releasing hormone agonists. Eur. Urol. 2014, 66, 1101–1108. [Google Scholar] [CrossRef]
- Stricker, H.J. Luteinizing hormone–releasing hormone antagonists in prostate cancer. Urology 2001, 58, 24–27. [Google Scholar] [CrossRef]
- EMA. Available online: http://www.ema.eu (accessed on 6 November 2019).
- Kiratli, B.J.; Srinivas, S.; Perkash, I.; Terris, M.K. Progressive decrease in bone density over 10 years of androgen deprivation therapy in patients with prostate cancer. Urology 2001, 57, 127–132. [Google Scholar] [CrossRef]
- Skolarus, T.A.; Caram, M.V.; Shahinian, V.B. Androgen-deprivation-associated bone disease. Curr. Opin. Urol. 2014, 24, 601–607. [Google Scholar] [CrossRef]
- Seidell, J.C.; Bjorntorp, P.; Sjostrom, L.; Kvist, H.; Sannerstedt, R. Visceral fat accumulation in men is positively associated with insulin, glucose, and C-peptide levels, but negatively with testosterone levels. Metabolism 1990, 39, 897–901. [Google Scholar] [CrossRef]
- Ferroni, C.; Del Rio, A.; Martini, C.; Manoni, E.; Varchi, G. Light-induced therapies for prostate cancer treatment. Front. Chem. 2019, 7, 719. [Google Scholar] [CrossRef]
- Lian, H.; Wu, J.; Hu, Y.; Guo, H. Self-assembled albumin nanoparticles for combination therapy in prostate cancer. Int. J. Nanomed. 2017, 12, 7777–7787. [Google Scholar] [CrossRef]
- Miller, J.D.; Baron, E.D.; Scull, H.; Hsia, A.; Berlin, J.C.; McCormick, T.; Colussi, V.; Kenney, M.E.; Cooper, K.D.; Oleinick, N.L. Photodynamic therapy with the phthalocyanine photosensitizer Pc 4: The case experience with preclinical mechanistic and early clinical-translational studies. Toxicol. Appl. Pharmacol. 2007, 224, 290–299. [Google Scholar] [CrossRef]
- Mokwena, M.G.; Kruger, C.A.; Ivan, M.T.; Heidi, A. A review of nanoparticle photosensitizer drug delivery uptake systems for photodynamic treatment of lung cancer. Photod. Photodyn. Ther. 2018, 22, 147–154. [Google Scholar] [CrossRef]
- Paszko, E.; Ehrhardt, C.; Senge, M.O.; Kelleher, D.P.; Reynolds, J.V. Nanodrug applications in photodynamic therapy. Photodiagnosis Photodyn. Ther. 2011, 8, 14–29. [Google Scholar] [CrossRef]
- Yoon, I.; Li, J.Z.; Shim, Y.K. Advance in photosensitizers and light delivery for photodynamic therapy. Clin. Endosc. 2013, 46, 7–23. [Google Scholar] [CrossRef]
- Darmostuk, M.; Rimpelova, S.; Gbelcova, H.; Ruml, T. Current approaches in SELEX: An update to aptamer selection technology. Biotechnol. Adv. 2015, 33, 1141–1161. [Google Scholar] [CrossRef]
- Pavlíčková, V.; Jurášek, M.; Rimpelová, S.; Záruba, K.; Sedlák, D.; Šimková, M.; Kodr, D.; Staňková, E.; Fähnrich, J.; Rottnerová, Z.; et al. Oxime-based 19-nortestosterone–pheophorbide a conjugate: Bimodal controlled release concept for PDT. J. Mater. Chem. B 2019, 7, 5465–5477. [Google Scholar] [CrossRef]
- Peterková, L.; Kmoníčková, E.; Ruml, T.; Rimpelová, S. Sarco/endoplasmic reticulum calcium ATPase inhibitors: Beyond anticancer perspective. J. Med. Chem. 2020, 63, 1937–1963. [Google Scholar] [CrossRef]
- Zimmermann, T.; Drašar, P.; Rimpelová, S.; Christensen, S.B.; Khripach, V.A.; Jurášek, M. Large scale conversion of trilobolide into the payload of mipsagargin: 8-O-(12-aminododecanoyl)-8-O-debutanoylthapsigargin. Biomolecules 2020, 10, 1640. [Google Scholar] [CrossRef]
- Tomanová, P.; Rimpelová, S.; Jurášek, M.; Buděšínský, M.; Vejvodová, L.; Ruml, T.; Kmoníčková, E.; Drašar, P.B. Trilobolide–porphyrin conjugates: On synthesis and biological effects evaluation. Steroids 2015, 97, 8–12. [Google Scholar] [CrossRef]
- Kozlowska, D.; Foran, P.; MacMahon, P.; Shelly, M.J.; Eustace, S.; O’Kennedy, R. Molecular and magnetic resonance imaging: The value of immunoliposomes. Adv. Drug Deliv. Rev. 2009, 61, 1402–1411. [Google Scholar] [CrossRef]
- Liu, T.; Wu, L.Y.; Choi, J.K.; Berkman, C.E. In vitro targeted photodynamic therapy with a pyropheophorbide-a conjugated inhibitor of prostate specific membrane antigen. Prostate 2009, 69, 585–594. [Google Scholar] [CrossRef]
- Wang, X.; Tsui, B.; Ramamurthy, G.; Zhang, P.; Meyers, J.; Kenney, M.E.; Kiechle, J.; Ponsky, L.; Basilion, J.P. Theranostic agents for photodynamic therapy of prostate cancer by targeting prostate-specific membrane antigen. Mol. Cancer Ther. 2016, 15, 1834–1844. [Google Scholar] [CrossRef] [PubMed]
- Torchilin, V.P. Targeted pharmaceutical nanocarriers for cancer therapy and imaging. AAPS J. 2007, 9, E128–E147. [Google Scholar] [CrossRef]
- Zhang, L.; Gu, F.X.; Chan, J.M.; Wang, A.Z.; Langer, R.S.; Farokhzad, O.C. Nanoparticles in medicine: Therapeutic applications and developments. Clin. Pharmacol. Ther. 2008, 83, 761–769. [Google Scholar] [CrossRef]
- Zhang, C.; Zhao, X.; Guo, S.; Lin, T.; Guo, H. Highly effective photothermal chemotherapy with pH-responsive polymer-coated drug-loaded melanin-like nanoparticles. Int. J. Nanomed. 2017, 12, 1827–1840. [Google Scholar] [CrossRef] [PubMed]
- Cai, Z.; Zhang, Y.; He, Z.; Jiang, L.P.; Zhu, J.J. NIR-triggered chemo-photothermal therapy by thermosensitive gold nanostarmesoporous silicaliposome-composited drug delivery systems. ACS Appl. Biomater. 2020, 3, 5322–5330. [Google Scholar] [CrossRef]
- Motlagh, N.S.J.; Parvin, P.; Mirzaie, Z.H.; Karimi, R.; Sanderson, J.H.; Atyabi, F. Synergistic performance of triggered drug release and photothermal therapy of MCF7 cells based on laser activated PEGylated GO + DOX. Biomed. Opt. Express 2020, 3783–3794. [Google Scholar] [CrossRef]
- Tran, V.A.; Vo, V.G.; Shim, K.; Lee, S.W.; An, S.S.A. Multimodal mesoporous silica nanocarriers for dual stimuli-responsive drug release and excellent photothermal ablation of cancer cells. Int. J. Nanomed. 2020, 15, 7667–7685. [Google Scholar] [CrossRef]
- Li, X.; Wang, X.; Hua, M.; Yu, H.; Wei, S.; Wang, A.; Zhou, J. Photothermal-triggered controlled drug release from mesoporous silica nanoparticles based on base-pairing rules. ACS Biomater. Sci. Eng. 2019, 5, 2399–2408. [Google Scholar] [CrossRef]
- Zhang, W.; Zheng, X.; Shen, S.; Wang, X. Doxorubicin-loaded magnetic nanoparticle clusters for chemo-photothermal treatment of the prostate cancer cell line PC3. Biochem. Biophys. Res. Commun. 2015, 466, 278–282. [Google Scholar] [CrossRef]
- Qiang, L.; Cai, Z.; Jiang, W.; Liu, J.; Tai, Z.; Li, G.; Gong, C.; Gao, S.; Gao, Y. A novel macrophage-mediated biomimetic delivery system with NIR-triggered release for prostate cancer therapy. J. Nanobiotechnol. 2019, 17, 83. [Google Scholar] [CrossRef]
- Doughty, A.C.; Hoover, A.R.; Layton, E.; Murray, C.K.; Howard, E.W.; Chen, W.R. Nanomaterial applications in photothermal therapy for cancer. Materials 2019, 12, 779. [Google Scholar] [CrossRef]
- Riley, R.S.; Day, E.S. Gold nanoparticle-mediated photothermal therapy: Applications and opportunities for multimodal cancer treatment. Wiley Interdiscip. Rev. Nanomed. 2017, 9, e1449. [Google Scholar] [CrossRef]
- Kim, J.; Chun, S.H.; Amornkitbamrung, L.; Song, C.; Yuk, J.S.; Ahn, S.Y.; Kim, B.W.; Lim, Y.T.; Oh, B.K.; Um, S.H. Gold nanoparticle clusters for the investigation of therapeutic efficiency against prostate cancer under near-infrared irradiation. Nano Converg. 2020, 7, 5. [Google Scholar] [CrossRef]
- Liu, Y.; Ashton, J.R.; Moding, E.J.; Yuan, H.; Register, J.K.; Fales, A.M.; Choi, J.; Whitley, M.J.; Zhao, X.; Qi, Y.; et al. A plasmonic gold nanostar theranostic probe for in vivo tumor imaging and photothermal therapy. Theranostics 2015, 5, 946–960. [Google Scholar] [CrossRef]
- Huang, L.; Xu, C.; Xu, P.; Qin, Y.; Chen, M.; Feng, Q.; Wen, X.; Wang, Y.; Shi, Y.; Cheng, Y. Intelligent photosensitive mesenchymal stem cells and cell-derived microvesicles for photothermal therapy of prostate cancer. Nanotheranostic 2019, 3, 41–53. [Google Scholar] [CrossRef]
- Stern, J.M.; Solomonov, V.V.K.; Sazykina, E.; Schwartz, J.A.; Gad, S.C.; Goodrich, G.P. Initial evaluation of the safety of nanoshell-directed photothermal therapy in the treatment of prostate disease. Int. J. Toxicol. 2016, 35, 38–46. [Google Scholar] [CrossRef]
- Gad, S.C.; Sharp, K.L.; Montgomery, C.; Payne, J.D.; Goodrich, G.P. Evaluation of the toxicity of intravenous delivery of auroshell particles (gold–silica nanoshells). Int. J. Toxicol. 2012, 31, 584–594. [Google Scholar] [CrossRef]
- Rastinehad, A.R.; Anastos, H.; Wajswol, E.; Winoker, J.S.; Sfakianos, J.P.; Doppalapudi, S.K.; Carrick, M.R.; Knauer, C.J.; Taouli, B.; Lewis, S.C.; et al. Gold nanoshell-localized photothermal ablation of prostate tumors in a clinical pilot device study. Proc. Natl. Acad. Sci. USA 2019, 116, 18590–18596. [Google Scholar] [CrossRef]
- Slovin, S. Chemotherapy and immunotherapy combination in advanced prostate cancer. Clin. Adv. Hematol. Oncol. 2012, 10, 90–100. [Google Scholar] [CrossRef]
- Cordes, L.M.; Gulley, J.L.; Madan, R.A. Perspectives on the clinical development of immunotherapy in prostate cancer. Asian J. Androl. 2018, 20, 253–259. [Google Scholar] [CrossRef]
- Dunn, G.P.; Old, L.J.; Schreiber, R.D. The three es of cancer immunoediting. Annu. Rev. Immunol. 2004, 22, 329–360. [Google Scholar] [CrossRef]
- Steinman, R.M. Lasker basic medical research award. Dendritic cells: Versatile controllers of the immune system. Nat. Med. 2007, 13, 1155–1159. [Google Scholar] [CrossRef]
- Handy, C.E.; Antonarakis, E.S. Sipuleucel-T for the treatment of prostate cancer: Novel insights and future directions. Future Oncol. 2017, 14, 907–917. [Google Scholar] [CrossRef] [PubMed]
- FDA. Available online: https://www.fda.gov/vaccines-blood-biologics/cellular-gene-therapy-products/provenge-sipuleucel-t (accessed on 9 January 2019).
- Podrazil, M.; Horvath, R.; Becht, E.; Rozkova, D.; Bilkova, P.; Sochorova, K.; Hromadkova, H.; Kayserova, J.; Vavrova, K.; Lastovicka, J.; et al. Phase I/II clinical trial of dendritic-cell based immunotherapy (DCVAC/PCa) combined with chemotherapy in patients with metastatic, castration-resistant prostate cancer. Oncotarget 2015, 6, 18192–18205. [Google Scholar] [CrossRef] [PubMed]
- Schepisi, G.; Cursano, M.C.; Casadei, C.; Menna, C.; Altavilla, A.; Lolli, C.; Cerchione, C.; Paganelli, G.; Santini, D.; Tonini, G.; et al. CAR-T cell therapy: A potential new strategy against prostate cancer. J. Immunother. Cancer 2019, 7, 258. [Google Scholar] [CrossRef] [PubMed]
- Schepisi, G.; Farolfi, A.; Conteduca, V.; Martignano, F.; De Lisi, D.; Ravaglia, G.; Rossi, L.; Menna, C.; Bellia, R.S.; Barone, D.; et al. Immunotherapy for prostate cancer: Where we are headed. Int. J. Mol. Sci. 2017, 18, 2627. [Google Scholar] [CrossRef]
- Hansen, A.R.; Massard, C.; Ott, P.A.; Haas, N.B.; Lopez, J.S.; Ejadi, S.; Wallmark, J.M.; Keam, B.; Delord, J.P.; Aggarwal, R.; et al. Pembrolizumab for advanced prostate adenocarcinoma: Findings of the KEYNOTE-028 study. Ann. Oncol. 2018, 29, 1807–1813. [Google Scholar] [CrossRef]
- Adam, M.; Tennstedt, P.; Lanwehr, D.; Tilki, D.; Steuber, T.; Beyer, B.; Thederan, I.; Heinzer, H.; Haese, A.; Salomon, G.; et al. Functional outcomes and quality of life after radical prostatectomy only versus a combination of prostatectomy with radiation and hormonal therapy. Eur. Urol. 2017, 71, 330–336. [Google Scholar] [CrossRef]
- Seisen, T.; Abdollah, F. Surgery-based multimodal management of high-risk prostate cancer patients: What is the functional price to pay for optimal disease control? Eur. Urol. 2017, 71, 337–339. [Google Scholar] [CrossRef]
- Zhang, X.Y.; Zhang, P.Y. Combinations in multimodality treatments and clinical outcomes during cancer. Oncol. Letters 2016, 12, 4301–4304. [Google Scholar] [CrossRef]
- Koupparis, A.; Gleave, M.E. Multimodal approaches to high-risk prostate cancer. Curr. Oncol. 2010, 17, S33–S37. [Google Scholar] [CrossRef]
- Lee, S.U.; Cho, K.H. Multimodal therapy for locally advanced prostate cancer: The roles of radiotherapy, androgen deprivation therapy, and their combination. Rad. Oncol. J. 2017, 35, 189–197. [Google Scholar] [CrossRef]
- Azzouzi, A.R.; Barret, E.; Moore, C.M.; Villers, A.; Allen, C.; Scherz, A.; Muir, G.; de Wildt, M.; Barber, N.J.; Lebdai, S.; et al. TOOKAD® Soluble vascular-targeted photodynamic (VTP) therapy: Determination of optimal treatment conditions and assessment of effects in patients with localised prostate cancer. BJU Int. 2013, 112, 766–774. [Google Scholar] [CrossRef]
- Borle, F.; Radu, A.; Fontolliet, C.; van den Bergh, H.; Monnier, P.; Wagnières, G. Selectivity of the photosensitiser TOOKAD® for photodynamic therapy evaluated in the Syrian golden hamster cheek pouch tumour model. Br. J. Cancer 2003, 89, 2320–2326. [Google Scholar] [CrossRef][Green Version]
- Koudinova, N.V.; Pinthus, J.H.; Brandis, A.; Brenner, O.; Bendel, P.; Ramon, J.; Eshhar, Z.; Scherz, A.; Salomon, Y. Photodynamic therapy with Pd-Bacteriopheophorbide (TOOKAD): Successful in vivo treatment of human prostatic small cell carcinoma xenografts. Int. J. Cancer 2003, 104, 782–789. [Google Scholar] [CrossRef]
- Azzouzi, A.R.; Lebdai, S.; Benzaghou, F.; Stief, C. Vascular-targeted photodynamic therapy with TOOKAD® Soluble in localized prostate cancer: Standardization of the procedure. World J. Urol. 2015, 33, 937–944. [Google Scholar] [CrossRef]
- Rapozzi, V.; Ragno, D.; Guerrini, A.; Ferroni, C.; della Pietra, E.; Cesselli, D.; Castoria, G.; Di Donato, M.; Saracino, E.; Benfenati, V.; et al. Androgen receptor targeted conjugate for bimodal photodynamic therapy of prostate cancer in vitro. Biocon. Chem. 2015, 26, 1662–1671. [Google Scholar] [CrossRef]
- Nagaya, T.; Nakamura, Y.; Okuyama, S.; Ogata, F.; Maruoka, Y.; Choyke, P.L.; Kobayashi, H. Near-infrared photoimmunotherapy targeting prostate cancer with prostate-specific membrane antigen (PSMA) antibody. Mol. Cancer Res. 2017, 15, 1153–1162. [Google Scholar] [CrossRef]
- Fucikova, J.; Moserova, I.; Truxova, I.; Hermanova, I.; Vancurova, I.; Partlova, S.; Fialova, A.; Sojka, L.; Cartron, P.F.; Houska, M.; et al. High hydrostatic pressure induces immunogenic cell death in human tumor cells. Int. J. Cancer 2014, 135, 1165–1177. [Google Scholar] [CrossRef]
- Melichar, B.; Študentova, H.; Kalábová, H.; Vitásková, D.; Čermáková, P.; Hormychová, H.; Ryška, A. Predictive and prognostic significance of tumor-infiltrating lymphocytes in patients with breast cancer treated with neoadjuvant systemic therapy. Anticancer Res. 2014, 34, 1115–1125. [Google Scholar]
- McDonnell, A.M.; Nowak, A.K.; Lake, R.A. Contribution of the immune system to the chemotherapeutic response. Semin. Immunopathol. 2011, 33, 353–367. [Google Scholar] [CrossRef]
- Škubník, J.; Jurášek, M.; Ruml, T.; Rimpelová, S. Mitotic poisons in research and medicine. Molecules 2020, 25, 4632. [Google Scholar] [CrossRef] [PubMed]
- Petrylak, D.P.; Vogelzang, N.J.; Chatta, G.S.; Fleming, M.T.; Smith, D.C.; Appleman, L.J.; Hussain, A.; Modiano, M.; Singh, P.; Tagawa, S.T.; et al. PSMA ADC monotherapy in patients with progressive metastatic castration-resistant prostate cancer following abiraterone and/or enzalutamide: Efficacy and safety in open-label single-arm phase 2 study. Prostate 2020, 80, 99–108. [Google Scholar] [CrossRef]
- Tekin, V.; Aweda, T.; Guldu, O.K.; Muftuler, Z.B.; Bartels, J.; Lapib, S.E.; Unak, P. A novel anti-angiogenic radio/photo sensitizer for prostate cancer imaging and therapy: 89Zr-Pt@TiO2-SPHINX, synthesis and in vitro evaluation. Nucl. Med. Biol. 2021, 94–95. [Google Scholar] [CrossRef]
- Bryant, H.E.; Schultz, N.; Thomas, H.D.; Parker, K.M.; Flower, D.; Lopez, E.; Kyle, S.; Meuth, M.; Curtin, N.J.; Helleday, T. Specific killing of BRCA2-deficient tumours with inhibitors of poly(ADP-ribose) polymerase. Nature 2005, 434, 913–917. [Google Scholar] [CrossRef]
- Patel, A.G.; Sarkaria, J.N.; Kaufmanna, S.H. Nonhomologous end joining drives poly(ADP-ribose) polymerase (PARP) inhibitor lethality in homologous recombination-deficient cells. Proc. Natl. Acad. Sci. USA 2011, 108, 3406–3411. [Google Scholar] [CrossRef] [PubMed]
- Beck, C.; Boehler, C.; Barbat, J.G.; Bonnet, M.E.; Illuzzi, G.; Ronde, P.; Gauthier, L.R.; Magroun, N.; Rajendran, A.; Lopez, B.S.; et al. PARP3 affects the relative contribution of homologous recombination and nonhomologous end-joining pathways. Nucleic Acids Res. 2014, 42, 5616–5632. [Google Scholar] [CrossRef] [PubMed]
- Lord, C.J.; Ashworth, A. PARP inhibitors: Synthetic lethality in the clinic. Science 2017, 355, 1152–1158. [Google Scholar] [CrossRef] [PubMed]
- Clinical Trials. Available online: https://clinicaltrials.gov/ct2/show/NCT02975934 (accessed on 15 February 2021).
- Smith, M.R.; Sandhu, S.K.; Kelly, W.K.; Scher, H.I.; Efstathiou, E.; Lara, P.N.; Yu, E.Y.; George, D.J.; Chi, K.N.; Saad, F.; et al. LBA50—Pre-specified interim analysis of GALAHAD: A phase II study of niraparib in patients (pts) with metastatic castration-resistant prostate cancer (mCRPC) and biallelic DNA-repair gene defects (DRD). Ann. Oncol. 2019, 30, v884–v885. [Google Scholar] [CrossRef]
- De Bono, J.S.; Mehra, N.; Higano, C.S.; Saad, F.; Buttigliero, C.; Mata, M.; Chen, H.C.; Healy, C.G.; Paccagnella, M.L.; Czibere, A.; et al. TALAPRO-1: A phase II study of talazoparib (TALA) in men with DNA damage repair mutations (DDRmut) and metastatic castration-resistant prostate cancer (mCRPC)—First interim analysis (IA). J. Clin. Oncol. 2020, 38, 119. [Google Scholar] [CrossRef]
- Clinical Trials. Available online: https://clinicaltrials.gov/ct2/show/NCT03395197 (accessed on 15 February 2021).
- Clinical Trials. Available online: https://clinicaltrials.gov/ct2/show/NCT01576172 (accessed on 15 February 2021).
- Clinical Trials. Available online: https://www.clinicaltrials.gov/ct2/show/NCT03712930?term=pamiparib&cond=prostate&draw=2&rank=1 (accessed on 15 February 2021).
- Chowdhury, S.; Mateo, J.; Gross, M.; Armstrong, A.J.; Cruz-Correa, M.; Piulats, J.M.; Blay, J.Y.; Li, M.; Rivas, D.; Quintero, L.; et al. Pamiparib, an investigational PARP inhibitor, in patients with metastatic castration-resistant prostate cancer (mCRPC) and a circulating tumor cell (CTC) homologous recombination deficiency (HRD) phenotype or BRCA defects: A trial in progress. J. Clin. Oncol. 2019, 37 (Suppl 15). [Google Scholar] [CrossRef]
- Clinical Trials. Available online: https://clinicaltrials.gov/ct2/show/NCT03572478 (accessed on 15 February 2021).
- Clinical Trials. Available online: https://clinicaltrials.gov/ct2/show/NCT03012321 (accessed on 15 February 2021).
- Clinical Trials. Available online: https://clinicaltrials.gov/ct2/show/NCT03732820 (accessed on 15 February 2021).
- Clinical Trials. Available online: https://clinicaltrials.gov/ct2/show/NCT03317392 (accessed on 15 February 2021).
- Nizialek, E.; Antonarakis, E.S. PARP inhibitors in metastatic prostate cancer: Evidence to date. Cancer Manag. Res. 2020, 12, 8105–8114. [Google Scholar] [CrossRef]
- Powers, E.; Karachaliou, G.S.; Kao, C.; Harrison, M.R.; Hoimes, C.J.; George, D.J.; Armstrong, A.J.; Zhang, T. Novel therapies are changing treatment paradigms in metastatic prostate cancer. J. Hematol. Oncol. 2020, 13, 144. [Google Scholar] [CrossRef]
- Pezaro, C. PARP inhibitor combinations in prostate cancer. Ther. Adv. Med. Oncol. 2020, 12, 1–10. [Google Scholar] [CrossRef]
- Clinical Trials. Available online: https://www.clinicaltrials.gov/ (accessed on 9 April 2021).
- Carver, B.S.; Chapinski, C.; Wongvipat, J.; Hieronymus, H.; Chen, Y.; Chandarlapaty, S.; Arora, V.K.; Le, C.; Koutcher, J.; Scher, H.; et al. Reciprocal feedback regulation of PI3K and androgen receptor signaling in PTEN-deficient prostate cancer. Cancer Cell 2011, 19, 575–586. [Google Scholar] [CrossRef]
- Braglia, L.; Zavatti, M.; Vinceti, M.; Martelli, A.M.; Marmiroli, S. Deregulated PTEN/PI3K/AKT/mTOR signaling in prostate cancer: Still a potential druggable target? Biochim. Biophys. Acta Mol. Cell Res. 2020, 1867, 118731. [Google Scholar] [CrossRef]
- Grünwald, V.; DeGraffenried, L.; Russel, D.; Friedrichs, W.E.; Ray, R.B.; Hidalgo, M. Inhibitors of mTOR reverse doxorubicin resistance conferred by PTEN status in prostate cancer cells. Cancer Res. 2002, 62, 6141–6145. [Google Scholar] [CrossRef]
- Skvortsova, I.; Skvortsov, S.; Stasyk, T.; Raju, U.; Popper, B.A.; Schiestl, B.; von Guggenber, E.; Neher, A.; Bonn, G.K.; Huber, L.K.; et al. Intracellular signaling pathways regulating radioresistance of human prostate carcinoma cells. Cell Biol. 2008, 8, 4521–4533. [Google Scholar] [CrossRef]
- De Bono, J.S.; De Giorgi, U.; Rodrigues, D.N.; Massard, C.; Bracarda, S.; Font, A.; Arija, J.A.A.; Shih, K.C.; Radavoi, G.D.; Xu, N.; et al. Randomized phase II study evaluating Akt blockade with ipatasertib, in combination with abiraterone, in patients with metastatic prostate cancer with and without PTEN loss. Clin. Cancer Res. 2019, 25, 2019. [Google Scholar] [CrossRef]
- Clinical Trials. Available online: https://clinicaltrials.gov/ct2/show/NCT03072238 (accessed on 16 February 2021).
- Clinical Trials. Available online: https://clinicaltrials.gov/ct2/show/NCT03673787 (accessed on 16 February 2021).
- Clinical Trials. Available online: https://clinicaltrials.gov/ct2/show/NCT04404140 (accessed on 16 February 2021).
- Clinical Trials. Available online: https://clinicaltrials.gov/ct2/show/NCT04493853 (accessed on 16 February 2021).
- Clinical Trials. Available online: https://www.clinicaltrials.gov/ct2/show/NCT04087174 (accessed on 16 February 2021).
- Clinical Trials. Available online: https://clinicaltrials.gov/ct2/show/NCT02121639 (accessed on 16 February 2021).
- Crabb, S.J.; Griffiths, G.; Marwood, E.; Dunkley, D.; Downs, N.; Martin, K.; Light, M.; Northey, J.; Wilding, S.; Whitehead, A.; et al. Pan-AKT Inhibitor Capivasertib With Docetaxel and Prednisolone in Metastatic Castration-Resistant Prostate Cancer: A Randomized, Placebo-Controlled Phase II Trial (ProCAID). J. Clin. Oncol. 2021, 39, 190–201. [Google Scholar] [CrossRef]
- Clinical Trials. Available online: https://repository.icr.ac.uk/bitstream/handle/internal/3528/jco.19.00368.pdf?sequence=2&isAllowed=y (accessed on 17 February 2021).
- Clinical Trials. Available online: https://clinicaltrials.gov/ct2/show/NCT02905318 (accessed on 17 February 2021).
- Clinical Trials. Available online: https://clinicaltrials.gov/ct2/show/NCT02059213 (accessed on 17 February 2021).
- Palmbos, P.L.; Tomlins, S.A.; Daignault, S.; Agarwal, N.; Twardowski, P.; Morgans, A.K.; Kelly, W.K.; Arora, V.; Antonarakis, E.S.; Siddiqui, J.; et al. Clinical outcomes and markers of treatment response in a randomized phase II study of androgen deprivation therapy with or without palbociclib in RB-intact metastatic hormone-sensitive prostate cancer (mHSPC). J. Clin. Oncol. 2020, 38, 5573. Available online: https://ascopubs.org/doi/abs/10.1200/JCO.2020.38.15_suppl.5573 (accessed on 17 February 2021). [CrossRef]
- Palmbos, P.L.; Tomlins, S.A.; Agarwal, N.; Twardowski, P.; Morgans, A.K.; Kelly, W.K.; Arora, V.; Antonarakis, E.S.; Siddiqui, J.; Daignault, S.; et al. Cotargeting AR signaling and cell cycle: A randomized phase II study of androgen deprivation therapy with or without palbociclib in RB-positive metastatic hormone sensitive prostate cancer (mHSPC). J. Clin. Oncol. 2018, 36, 251. Available online: https://ascopubs.org/doi/abs/10.1200/JCO.2018.36.6_suppl.251 (accessed on 17 February 2021). [CrossRef]
- Clinical Trials. Available online: https://clinicaltrials.gov/ct2/show/NCT02555189?term=Ribociclib&cond=prostate+cancer&draw=2&rank=1 (accessed on 17 February 2021).
- Clinical Trials. Available online: https://clinicaltrials.gov/ct2/show/NCT02494921 (accessed on 17 February 2021).
- Clinical Trials. Available online: https://clinicaltrials.gov/ct2/show/NCT04408924?term=Abemaciclib&cond=Prostate+Cancer&draw=2&rank=3 (accessed on 17 February 2021).
- Clinical Trials. Available online: https://clinicaltrials.gov/ct2/show/NCT04298983 (accessed on 17 February 2021).
- Clinical Trials. Available online: https://clinicaltrials.gov/ct2/show/NCT03706365 (accessed on 17 February 2021).
- Clinical Trials. Available online: https://clinicaltrials.gov/ct2/show/NCT04751929?term=Abemaciclib&cond=Prostate+Cancer&draw=2&rank=5 (accessed on 17 February 2021).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PARPi | Combination | Indication | Status | Phase | Clinical Trial Identifier |
|---|---|---|---|---|---|
| Olaparib | Monotherapy | mCRPC, a mutation in one of 15 genes involved in the HRR | n.r. | III | NTC02987543 |
| Monotherapy | Advanced CRPC | n.r. | II | NCT01682772 | |
| Monotherapy | mCRPC, after docetaxel treatment | n.r. | II | NCT03434158 | |
| Monotherapy | Non-mBRPC | Recruiting | II | NCT03047135 | |
| Prior to radical prostatectomy | localized PC | Terminated | II | NCT03570476 | |
| Prior to radical prostatectomy | Locally advanced PC with DNA repair defects | Recruiting | II | NCT03432897 | |
| Ceralasertib | mCRPC, with DNA repair-deficient | Recruiting | II | NCT03787680 | |
| Bromodomain and extraterminal inhibitor (AZD5153) | Malignant solid tumors | n.r. | I | NCT03205176 | |
| AA | mCRPC, prior chemotherapy containing docetaxel | n.r. | II | NCT01972217 | |
| AA, P | mCRPC, with DNA repair-deficient | Recruiting | II | NCT03012321 | |
| PLX2853, AA, P | mCRPC | Recruiting | Ib/IIa | NCT04556617 | |
| MEDI4736, cediranib | Advanced solid tumors | Recruiting | I/II | NCT02484404 | |
| AA | mCRPC, no prior chemotherapy or new hormonal agents | n.r. | III | NCT03732820 | |
| Testosterone | mCRPC | n.r. | II | NCT03516812 | |
| Degarelix, prior to radical prostatectomy | Intermediate/high risk PC | Completed | I | NCT02324998 | |
| Cediranib | mCRPC | n.r. | II | NCT02893917 | |
| Nanoparticle camptothecin | mCRPC, relapsed/refractory small cell lung cancer | Recruiting | I/II | NCT02769962 | |
| Carboplatin | mCRPC, tumors containing BRCA1, BRCA2 or PALB2 | Recruiting | II | NCT04038502 | |
| Carboplatin, cabazitaxel, P | Aggressive variant PC | n.r. | II | NCT03263650 | |
| Pembrolizumab | mCRPC, failed to respond to either AA or enzalutamide (but not both), and chemotherapy | Recruiting | III | NCT03834519 | |
| Radiation, ADT, AA, P | CSOmPC | n.y.r. | II | NCT04748042 | |
| Pembrolizumab | mCRPC | Recruiting | Ib/II | NCT02861573 | |
| Durvalumab | CSBR non-mPC, harboring mutations in DNA damage repair | Recruiting | II | NCT03810105 | |
| 177Lu-PSMA | mCRPC | Recruiting | I | NCT03874884 | |
| Ra-223 dichloride | mCRPC | Recruiting | I/II | NCT03317392 | |
| Rucaparib | Monotherapy | mCRPC, HRR gene deficiency | Recruiting | III | NCT02975934 |
| Monotherapy | mHSPC | Recruiting | II | NCT03413995 | |
| Monotherapy | Non-mHSPC | Recruiting | NCT03533946 | ||
| Monotherapy | mCRPC, ovarian, epithelial, peritoneal, fallopian tube cancer | n.y.r. | III | NCT04676334 | |
| Monotherapy | Solid tumors associated with deleterious mutations in HRR genes | Recruiting | II | NCT04171700 | |
| Monotherapy | mCRPC | n.r. | NCT02952534 | ||
| Nivolumab | mCRPC | n.r. | II | NCT03338790 | |
| Nivolumab | PC, endometrial cancer | Terminated | Ib/IIa | NCT03572478 | |
| Ipatasertib | Advanced BC, OC, PC | n.r. | I/II | NCT03840200 | |
| Enzalutamide, AA | mCRPC | n.r. | Ib | NCT04179396 | |
| Enzalutamide | mCRPC, resistant to testosterone-deprivation therapy | Suspended | III | NCT04455750 | |
| Docetaxel, carboplatin | mCRPC, HRR gene deficiency | Recruiting | II | NCT03442556 | |
| Copanlisib | mCRPC | Recruiting | Ib/II | NCT04253262 | |
| Niraparib | AA, P | mCRPC, HRR gene alteration | Recruiting | III | NCT03748641 |
| AA, P | mCSPC, deleterious germline or somatic HRR gene-mutated | Recruiting | III | NCT04497844 | |
| AA, P | mCRPC, with and without HRR gene alterations | Recruiting | I | NCT04577833 | |
| Cetrelimab, AA, P | mCRPC | Recruiting | I/II | NCT03431350 | |
| Monotherapy | Platinum sensitive CRPC | Recruiting | II | NCT04288687 | |
| Apalutamide, AA, P | mCRPC | Completed | I | NCT02924766 | |
| Monotherapy | mCRPC and DNA repair anomalies | n.r. | II | NCT02854436 | |
| Monotherapy | Advanced solid tumor or hematologic malignancies | Completed | I | NCT00749502 | |
| Prostatectomy | Non-metastatic high-risk PC | Recruiting | II | NCT04030559 | |
| Cabazitaxel, carboplatin, cetrelimab | Aggressive variant mPC | Recruiting | II | NCT04592237 | |
| Leuprolide, AA, P, radiotherapy | High risk and node-positive PC | Recruiting | I/II | NCT04194554 | |
| ATR inhibitor (BAY 1895344) | Advanced solid tumors, OC | Recruiting | Ib | NCT04267939 | |
| Radium 223 | mPC, hormone refractory PC, stage IV PC | n.r. | Ib | NCT03076203 | |
| Radiotherapy, antiandrogen therapy | high-risk PC | Recruiting | II | NCT04037254 | |
| Talazoparib | Monotherapy | mCRPC, previously received taxane-based chemotherapy and progressed on at least 1 novel hormonal agent | n.r. | II | NCT03148795 |
| Monotherapy | Advanced cancer, a mutation in DNA damage response genes | Recruiting | II | NCT04550494 | |
| Enzalutamide | mCRPC | Recruiting | III | NCT03395197 | |
| Enzalutamide | mHSPC | Recruiting | II | NCT04332744 | |
| Enzalutamide | mCSPC | n.y.r. | III | NCT04821622 | |
| Glutaminase inhibitor telaglenastat | mCRPC | n.y.r. | II | NCT04824937 | |
| Temozolomide | PC | Recruiting | Ib/II | NCT04019327 | |
| belinostat | mCRPC, mBC, OC | n.y.r. | I | NCT04703920 | |
| ADT | mCSPC | n.y.r. | II | NCT04734730 | |
| Avelumab, bempegaldesleukin | Advanced squamous cell carcinoma of the head and neck, mCRPC | Terminated | II | NCT04052204 | |
| Avelumab | Advanced or metastatic solid tumors | n.r. | Ib/II | NCT03330405 | |
| Monotherapy | Advanced or recurrent solid tumors | Completed | I | NCT01286987 | |
| Monotherapy | Metastatic solid tumors | Withdrawn | I | NCT02567396 | |
| Veliparib | AA, P | mCRPC | Completed | II | NCT01576172 |
| Temozolomide | mPC | Completed | I | NCT01085422 | |
| Monotherapy | Malignant solid tumors | Completed | I | NCT00892736 | |
| Pamiparib | Monotherapy | mCRPC | Terminated | II | NCT03712930 |
| Temozolomide | Locally advanced or metastatic solid tumors | Recruiting | I/II | NCT03150810 |
| Akt Inhibitor | Combination | Indication | Status | Phase | Clinical Trial Identifier |
|---|---|---|---|---|---|
| Ipatasertib | AA | mCRP | n.r. | III | NCT03072238 |
| AA | mCRP, previous treatment with docetaxel | n.r. | I/II | NCT01485861 | |
| Androgen deprivation therapy, darolutamide | Localized, high-risk PC | n.y.r. | I/II | NCT04737109 | |
| Atezolizumab | Advanced solid tumors, glioblastoma multiforme, PC | Recruiting | I/II | NCT03673787 | |
| Atezolizumab, docetaxel | mCRPC previously treated with second-generation AR targeted therapy | Recruiting | Ib | NCT04404140 | |
| Rucaparib | Advanced BC, OC, PC | n.r. | I/II | NCT03840200 | |
| Monotherapy | PC | Recruiting | II | NCT03385655 | |
| Monotherapy | Solid tumors, lymphomas, multiple myeloma | ||||
| Capivasertib | AA, P | mHSPC | Recruiting | III | NCT04493853 |
| AA, enzalutamide | mCRPC | n.r. | I | NCT04087174 | |
| Monotherapy | Solid tumors, lymphomas, multiple myeloma | Recruiting | II | NCT02465060 | |
| Docetaxel, P | mCRPC | n.r. | I/II | NCT02121639 | |
| Monotherapy | mCRPC | Completed | I | NCT01692262 | |
| Enzalutamid | mCRPC | Unknown | II | NCT02525068 | |
| Enzalutamide, fulVestrant | Advanced solid tumors (PC, BC) | n.r. | I | NCT03310541 | |
| Itraconazole | Healthy volunteers (intended indication: metastatic triple negative/HR+ BC, mHSPC) | n.r. | I | NCT04712396 |
| CDK Inhibitor | Combination | Indication | Status | Phase | Clinical Trial Indetifier |
|---|---|---|---|---|---|
| Palbociclib | Monotherapy | mCRPC | Recruiting | II | NCT02905318 |
| bicalutemide, zoladex, lupron depot | Retinoblastoma protein-positive mPC | Completed | II | NCT02059213 | |
| KAT6 inhibitor (PF-07248144) | Advanced or metastatic solid tumors (BC, PC, lung cancer) | Recruiting | I | NCT04606446 | |
| Monotherapy | Advanced refractory solid tumors, lymphomas, multiple myeloma | Recruiting | II | NCT02465060 | |
| Combinations of drug | Metastatic solid tumor or hematological malignancy | Recruiting | Ib | NCT03878524 | |
| Ribociclib | Enzalutamide | HRPC, mPC | Recruiting | Ib/II | NCT02555189 |
| Docetaxel, P | mCRPC | n.r. | II | NCT02494921 | |
| Abemaciclib | Monotherapy | mCRPC previously treated hormonally or with taxane chemotherapy | Recruiting | II | NCT04408924 |
| Androgen deprivation therapy, radiation therapy | Locally advanced PC | Recruiting | II | NCT04298983 | |
| Atezolizumab | mCRPC | Withdrawn | II | NCT04272645 | |
| AA, P | mCRPC | n.r. | II | NCT03706365 | |
| Atezolizumab | mCRPC | n.y.r. | II | NCT04751929 | |
| Combinations of drug | Metastatic solid tumor or hematological malignancy | Recruiting | Ib | NCT03878524 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kvízová, J.; Pavlíčková, V.; Kmoníčková, E.; Ruml, T.; Rimpelová, S. Quo Vadis Advanced Prostate Cancer Therapy? Novel Treatment Perspectives and Possible Future Directions. Molecules 2021, 26, 2228. https://doi.org/10.3390/molecules26082228
Kvízová J, Pavlíčková V, Kmoníčková E, Ruml T, Rimpelová S. Quo Vadis Advanced Prostate Cancer Therapy? Novel Treatment Perspectives and Possible Future Directions. Molecules. 2021; 26(8):2228. https://doi.org/10.3390/molecules26082228
Chicago/Turabian StyleKvízová, Jana, Vladimíra Pavlíčková, Eva Kmoníčková, Tomáš Ruml, and Silvie Rimpelová. 2021. "Quo Vadis Advanced Prostate Cancer Therapy? Novel Treatment Perspectives and Possible Future Directions" Molecules 26, no. 8: 2228. https://doi.org/10.3390/molecules26082228
APA StyleKvízová, J., Pavlíčková, V., Kmoníčková, E., Ruml, T., & Rimpelová, S. (2021). Quo Vadis Advanced Prostate Cancer Therapy? Novel Treatment Perspectives and Possible Future Directions. Molecules, 26(8), 2228. https://doi.org/10.3390/molecules26082228