
Needle Trap Device-GC-MS for Characterization of Lung Diseases Based on Breath VOC Profiles


 ,
,  ,
, 
Abstract
1. Introduction
2. Results and Discussion
2.1. Calibration Method and Quantitation of Analytes
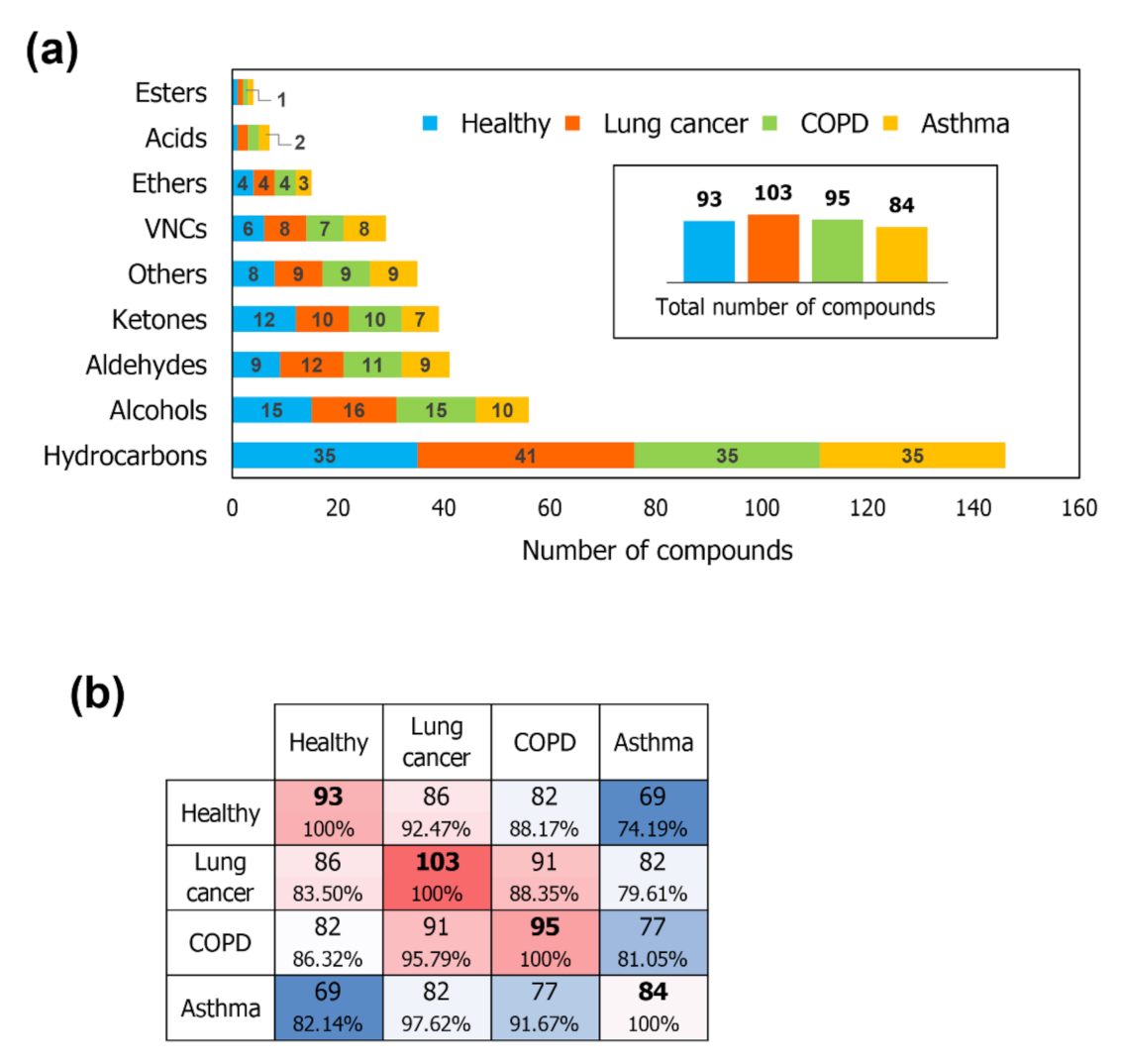
2.2. VOCs Detected in Breath
2.3. Differential Distribution of VOCs
2.4. Diagnosis Prediction–Global Profiles
2.5. Diagnosis Prediction–Target Analysis
3. Materials and Methods
3.1. Apparatus and Standards
3.2. Breath Collection
3.3. Selection of Targets
3.4. Calibration Procedure
3.5. Sample Extraction
3.6. Data Analysis and Chemometrics Approaches
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Sample Availability
References
- Varghese, C.; Troisi, G.; Schotte, K.; Prasad, V.M.; St Claire, S.M. World No Tobacco Day 2019 puts the spotlight on lung health. J. Thorac. Dis. 2019, 11, 2639–2642. [Google Scholar] [CrossRef] [PubMed]
- Van de Kant, K.D.; Van der Sande, L.J.; Jöbsis, Q.; Van Schayck, O.C.; Dompeling, E. Clinical use of exhaled volatile organic compounds in pulmonary diseases: A systematic review. Respir. Res. 2012, 13, 117. [Google Scholar] [CrossRef] [PubMed]
- Hashoul, D.; Haick, H. Sensors for detecting pulmonary diseases from exhaled breath. Eur. Respir. Rev. 2019, 28, 190011. [Google Scholar] [CrossRef]
- Sun, X.; Shao, K.; Wang, T. Detection of volatile organic compounds (VOCs) from exhaled breath as noninvasive methods for cancer diagnosis. Anal. Bioanal. Chem. 2016, 408, 2759–2780. [Google Scholar] [CrossRef] [PubMed]
- Monedeiro, F.; Dos Reis, R.B.; Peria, F.M.; Sares, C.T.G.; De Martinis, B.S. Investigation of sweat VOC profiles in assessment of cancer biomarkers using HS-GC-MS. J. Breath Res. 2020, 14, 026009. [Google Scholar] [CrossRef]
- Monedeiro, F.; Milanowski, M.; Ratiu, I.-A.; Zmysłowski, H.; Ligor, T.; Buszewski, B. VOC Profiles of Saliva in Assessment of Halitosis and Submandibular Abscesses Using HS-SPME-GC/MS Technique. Molecules 2019, 24, 2977. [Google Scholar] [CrossRef]
- Ratiu, I.-A.; Ligor, T.; Monedeiro, F.; Al-Suod, H.; Bocos-Bintintan, V.; Szeliga, J.; Jackowski, M.; Buszewski, B. “Features of infected versus uninfected chemical profiles released from human exudates ”. Stud. Univ. Babeș-Bolyai Chem. 2019, 64, 207–216. [Google Scholar] [CrossRef]
- Silva, C.L.; Passos, M.; Câmara, J.S. Investigation of urinary volatile organic metabolites as potential cancer biomarkers by solid-phase microextraction in combination with gas chromatography-mass spectrometry. Br. J. Cancer 2011, 105, 1894–1904. [Google Scholar] [CrossRef] [PubMed]
- Buszewski, B.; Kęsy, M.; Ligor, T.; Amann, A. Human exhaled air analytics: Biomarkers of diseases. Biomed. Chromatogr. 2007, 21, 553–566. [Google Scholar] [CrossRef]
- Filipiak, W.; Mochalski, P.; Filipiak, A.; Ager, C.; Cumeras, R.; E. Davis, C.; Agapiou, A.; Unterkofler, K.; Troppmair, J. A Compendium of Volatile Organic Compounds (VOCs) Released By Human Cell Lines. Curr. Med. Chem. 2016, 23, 2112–2131. [Google Scholar] [CrossRef]
- Amann, A.; Miekisch, W.; Schubert, J.; Buszewski, B.; Ligor, T.; Jezierski, T.; Pleil, J.; Risby, T. Analysis of Exhaled Breath for Disease Detection. Annu. Rev. Anal. Chem. 2014, 7, 455–482. [Google Scholar] [CrossRef]
- Ratiu, I.-A.; Bocos-Bintintan, V.; Monedeiro, F.; Milanowski, M.; Ligor, T.; Buszewski, B. An Optimistic Vision of Future: Diagnosis of Bacterial Infections by Sensing Their Associated Volatile Organic Compounds. Crit. Rev. Anal. Chem. 2019, 1–12. [Google Scholar] [CrossRef]
- Schmidt, K.; Podmore, I. Current Challenges in Volatile Organic Compounds Analysis as Potential Biomarkers of Cancer. J. Biomarkers 2015, 2015, 1–16. [Google Scholar] [CrossRef]
- Mazzone, P.J. Analysis of Volatile Organic Compounds in the Exhaled Breath for the Diagnosis of Lung Cancer. J. Thorac. Oncol. 2008, 3, 774–780. [Google Scholar] [CrossRef]
- Ratiu, I.-A.; Ligor, T.; Bocos-Bintintan, V.; Buszewski, B. Mass spectrometric techniques for the analysis of volatile organic compounds emitted from bacteria. Bioanalysis 2017, 9, 1069–1092. [Google Scholar] [CrossRef] [PubMed]
- Nardi-Agmon, I.; Peled, N. Exhaled breath analysis for the early detection of lung cancer: Recent developments and future prospects. Lung Cancer Targets Ther. 2017, 8, 31–38. [Google Scholar] [CrossRef]
- Miekisch, W.; Schubert, J.K.; Noeldge-Schomburg, G.F. Diagnostic potential of breath analysis—Focus on volatile organic compounds. Clin. Chim. Acta 2004, 347, 25–39. [Google Scholar] [CrossRef] [PubMed]
- Milanowski, M.; Monedeiro, F.; Złoch, M.; Ratiu, I.-A.; Pomastowski, P.; Ligor, T.; De Martinis, B.S.; Buszewski, B. Profiling of VOCs released from different salivary bacteria treated with non-lethal concentrations of silver nitrate. Anal. Biochem. 2019, 578, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Vishinkin, R.; Haick, H. Nanoscale Sensor Technologies for Disease Detection via Volatolomics. Small 2015, 11, 6142–6164. [Google Scholar] [CrossRef]
- Ratiu, I.A.; Bocos-Bintintan, V.; Patrut, A.; Moll, V.H.; Turner, M.; Thomas, C.L.P. Discrimination of bacteria by rapid sensing their metabolic volatiles using an aspiration-type ion mobility spectrometer (a-IMS) and gas chromatography-mass spectrometry GC-MS. Anal. Chim. Acta 2017, 982, 209–217. [Google Scholar] [CrossRef]
- Ratiu, I.-A.; Ligor, T.; Bocos-Bintintan, V.; Al-Suod, H.; Kowalkowski, T.; Rafińska, K.; Buszewski, B. The effect of growth medium on an Escherichia coli pathway mirrored into GC/MS profiles. J. Breath Res. 2017, 11, 036012. [Google Scholar] [CrossRef]
- Mametov, R.; Ratiu, I.-A.; Monedeiro, F.; Ligor, T.; Buszewski, B. Evolution and Evaluation of GC Columns. Crit. Rev. Anal. Chem. 2019, 1–24. [Google Scholar] [CrossRef]
- Dobrzyńska, E.; Buszewski, B. Needle-trap device for the sampling and determination of chlorinated volatile compounds. J. Sep. Sci. 2013, 36, 3372–3378. [Google Scholar] [CrossRef] [PubMed]
- Lord, H.L.; Zhan, W.; Pawliszyn, J. Fundamentals and applications of needle trap devices. Anal. Chim. Acta 2010, 677, 3–18. [Google Scholar] [CrossRef] [PubMed]
- Filipiak, W.; Filipiak, A.; Ager, C.; Wiesenhofer, H.; Amann, A. Optimization of sampling parameters for collection and preconcentration of alveolar air by needle traps. J. Breath Res. 2012, 6, 027107. [Google Scholar] [CrossRef]
- Frank Kneepkens, C.M.; Lepage, G.; Roy, C.C. The potential of the hydrocarbon breath test as a measure of lipid peroxidation. Free Radic. Biol. Med. 1994, 17, 127–160. [Google Scholar] [CrossRef]
- Fuchs, P.; Loeseken, C.; Schubert, J.K.; Miekisch, W. Breath gas aldehydes as biomarkers of lung cancer. Int. J. Cancer 2010, 126, 2663–2670. [Google Scholar] [CrossRef]
- Hakim, M.; Broza, Y.Y.; Barash, O.; Peled, N.; Phillips, M.; Amann, A.; Haick, H. Volatile Organic Compounds of Lung Cancer and Possible Biochemical Pathways. Chem. Rev. 2012, 112, 5949–5966. [Google Scholar] [CrossRef] [PubMed]
- Charles, S.M.; Batterman, S.A.; Jia, C. Composition and emissions of VOCs in main- and side-stream smoke of research cigarettes. Atmos. Environ. 2007, 41, 5371–5384. [Google Scholar] [CrossRef]
- Kischkel, S.; Miekisch, W.; Sawacki, A.; Straker, E.M.; Trefz, P.; Amann, A.; Schubert, J.K. Breath biomarkers for lung cancer detection and assessment of smoking related effects—Confounding variables, influence of normalization and statistical algorithms. Clin. Chim. Acta 2010, 411, 1637–1644. [Google Scholar] [CrossRef]
- Elfaki, I.; Mir, R.; Almutairi, F.M.; Abu Duhier, F.M. Cytochrome P450: Polymorphisms and roles in cancer, diabetes and atherosclerosis. Asian Pacific J. Cancer Prev. 2018, 19, 2057–2070. [Google Scholar] [CrossRef]
- Zamay, T.; Zamay, G.; Kolovskaya, O.; Zukov, R.; Petrova, M.; Gargaun, A.; Berezovski, M.; Kichkailo, A. Current and Prospective Protein Biomarkers of Lung Cancer. Cancers 2017, 9, 155. [Google Scholar] [CrossRef]
- Karachaliou, N.; Pilotto, S.; Lazzari, C.; Bria, E.; De Marinis, F.; Rosell, R. Cellular and molecular biology of small cell lung cancer: An overview. Transl. Lung Cancer Res. 2016, 5, 2–15. [Google Scholar] [CrossRef] [PubMed]
- Schaich, K.M.; Shahidi, F.; Zhong, Y.; Eskin, N.A.M. Lipid Oxidation. In Biochemistry of Foods; Eskin, N.A., Shahidi, F., Eds.; Elsevier: Cambridge, UK, 2013; pp. 419–478. ISBN 9780122423529. [Google Scholar]
- Altomare, D.F.; Di Lena, M.; Porcelli, F.; Trizio, L.; Travaglio, E.; Tutino, M.; Dragonieri, S.; Memeo, V.; De Gennaro, G. Exhaled volatile organic compounds identify patients with colorectal cancer. Br. J. Surg. 2013, 100, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Weinberg, R.A. Hallmarks of Cancer: The Next Generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [PubMed]
- Phillips, M.; Herrera, J.; Krishnan, S.; Zain, M.; Greenberg, J.; Cataneo, R.N. Variation in volatile organic compounds in the breath of normal humans. J. Chromatogr. B Biomed. Sci. Appl. 1999, 729, 75–88. [Google Scholar] [CrossRef]
- Mutti, A.; Falzoi, M.; Lucertini, S.; Arfini, G.; Zignani, M.; Lombardi, S.; Franchini, I. n-Hexane metabolism in occupationally exposed workers. Occup. Environ. Med. 1984, 41, 533–538. [Google Scholar] [CrossRef]
- Forney, F.W.; Markovetz, A.J. The biology of methyl ketones. J. Lipid Res. 1971, 12, 383–395. [Google Scholar] [CrossRef]
- Abaffy, T.; Duncan, R.; Riemer, D.D.; Tietje, O.; Elgart, G.; Milikowski, C.; DeFazio, R.A. Differential Volatile Signatures from Skin, Naevi and Melanoma: A Novel Approach to Detect a Pathological Process. PLoS ONE 2010, 5, e13813. [Google Scholar] [CrossRef]
- Phillips, M.; Cataneo, R.N.; Cummin, A.R.C.; Gagliardi, A.J.; Gleeson, K.; Greenberg, J.; Maxfield, R.A.; Rom, W.N. Detection of Lung Cancer With Volatile Markers in the Breatha. Chest 2003, 123, 2115–2123. [Google Scholar] [CrossRef]
- Bos, L.D.J.; Sterk, P.J.; Schultz, M.J. Volatile Metabolites of Pathogens: A Systematic Review. PLoS Pathog. 2013, 9, e1003311. [Google Scholar] [CrossRef]
- Egge, H.; Murawski, U.; Ryhage, R.; György, P.; Chatranon, W.; Zilliken, F. Minor constitutents of human milk IV: Analysis of the branched chain fatty acids. Chem. Phys. Lipids 1972, 8, 42–55. [Google Scholar] [CrossRef]
- Gosset, G. Production of aromatic compounds in bacteria. Curr. Opin. Biotechnol. 2009, 20, 651–658. [Google Scholar] [CrossRef] [PubMed]
- Xue, J.; Murrieta, C.M.; Rule, D.C.; Miller, K.W. Exogenous or l-Rhamnose-Derived 1,2-Propanediol Is Metabolized via a pduD-Dependent Pathway in Listeria innocua. Appl. Environ. Microbiol. 2008, 74, 7073–7079. [Google Scholar] [CrossRef] [PubMed]
- Ramachandriya, K.D.; Wilkins, M.R.; Delorme, M.J.M.; Zhu, X.; Kundiyana, D.K.; Atiyeh, H.K.; Huhnke, R.L. Reduction of acetone to isopropanol using producer gas fermenting microbes. Biotechnol. Bioeng. 2011, 108, 2330–2338. [Google Scholar] [CrossRef] [PubMed]
- Houten, S.M.; Violante, S.; Ventura, F.V.; Wanders, R.J.A. The Biochemistry and Physiology of Mitochondrial Fatty Acid β-Oxidation and Its Genetic Disorders. Annu. Rev. Physiol. 2016, 78, 23–44. [Google Scholar] [CrossRef]
- Ludwiczuk, A.; Skalicka-Woźniak, K.; Georgiev, M.I. Terpenoids. In Pharmacognosy; Badal, S., Delgoda, R., Eds.; Elsevier: London, UK, 2017; pp. 233–266. ISBN 9780128020999. [Google Scholar]
- Audrain, B.; Farag, M.A.; Ryu, C.M.; Ghigo, J.M. Role of bacterial volatile compounds in bacterial biology. FEMS Microbiol. Rev. 2015, 39, 222–233. [Google Scholar] [CrossRef]
- Friedman, M.I.; Preti, G.; Deems, R.O.; Friedman, L.S.; Munoz, S.J.; Maddrey, W.C. Limonene in expired lung air of patients with liver disease. Dig. Dis. Sci. 1994, 39, 1672–1676. [Google Scholar] [CrossRef]
- Mullen, P.J.; Yu, R.; Longo, J.; Archer, M.C.; Penn, L.Z. The interplay between cell signalling and the mevalonate pathway in cancer. Nat. Rev. Cancer 2016, 16, 718–731. [Google Scholar] [CrossRef] [PubMed]
- Johnson, W.; Bergfeld, W.F.; Belsito, D.V.; Hill, R.A.; Klaassen, C.D.; Liebler, D.; Marks, J.G.; Shank, R.C.; Slaga, T.J.; Snyder, P.W.; et al. Safety Assessment of Isoparaffins as Used in Cosmetics. Int. J. Toxicol. 2012, 31, 269S–295S. [Google Scholar] [CrossRef]
- Fujiwara, R.; Noda, S.; Tanaka, T.; Kondo, A. Styrene production from a biomass-derived carbon source using a coculture system of phenylalanine ammonia lyase and phenylacrylic acid decarboxylase-expressing Streptomyces lividans transformants. J. Biosci. Bioeng. 2016, 122, 730–735. [Google Scholar] [CrossRef] [PubMed]
- Wiggins, T.; Kumar, S.; Markar, S.R.; Antonowicz, S.; Hanna, G.B. Tyrosine, Phenylalanine, and Tryptophan in Gastroesophageal Malignancy: A Systematic Review. Cancer Epidemiol. Biomarkers Prev. 2015, 24, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Pal, M. Random forest classifier for remote sensing classification. Int. J. Remote Sens. 2005, 26, 217–222. [Google Scholar] [CrossRef]
- Steeghs, M.M.L.; Cristescu, S.M.; Harren, F.J.M. The suitability of Tedlar bags for breath sampling in medical diagnostic research. Physiol. Meas. 2007, 28, 73–84. [Google Scholar] [CrossRef]
- Bajtarevic, A.; Ager, C.; Pienz, M.; Klieber, M.; Schwarz, K.; Ligor, M.; Ligor, T.; Filipiak, W.; Denz, H.; Fiegl, M.; et al. Noninvasive detection of lung cancer by analysis of exhaled breath. BMC Cancer 2009, 9, 348. [Google Scholar] [CrossRef]
- Poli, D.; Carbognani, P.; Corradi, M.; Goldoni, M.; Acampa, O.; Balbi, B.; Bianchi, L.; Rusca, M.; Mutti, A. Exhaled volatile organic compounds in patients with non-small cell lung cancer: Cross sectional and nested short-term follow-up study. Respir. Res. 2005, 6, 71. [Google Scholar] [CrossRef]
- Fens, N.; Zwinderman, A.H.; Van der Schee, M.P.; De Nijs, S.B.; Dijkers, E.; Roldaan, A.C.; Cheung, D.; Bel, E.H.; Sterk, P.J. Exhaled Breath Profiling Enables Discrimination of Chronic Obstructive Pulmonary Disease and Asthma. Am. J. Respir. Crit. Care Med. 2009, 180, 1076–1082. [Google Scholar] [CrossRef]
- Ligor, M.; Ligor, T.; Bajtarevic, A.; Ager, C.; Pienz, M.; Klieber, M.; Denz, H.; Fiegl, M.; Hilbe, W.; Weiss, W.; et al. Determination of volatile organic compounds in exhaled breath of patients with lung cancer using solid phase microextraction and gas chromatography mass spectrometry. Clin. Chem. Lab. Med. 2009, 47, 550–560. [Google Scholar] [CrossRef] [PubMed]
- Ulanowska, A.; Kowalkowski, T.; Trawińska, E.; Buszewski, B. The application of statistical methods using VOCs to identify patients with lung cancer. J. Breath Res. 2011, 5, 046008. [Google Scholar] [CrossRef]
- Phillips, C.O.; Syed, Y.; Mac Parthaláin, N.; Zwiggelaar, R.; Claypole, T.C.; Lewis, K.E. Machine learning methods on exhaled volatile organic compounds for distinguishing COPD patients from healthy controls. J. Breath Res. 2012, 6, 036003. [Google Scholar] [CrossRef] [PubMed]
- Rudnicka, J.; Kowalkowski, T.; Ligor, T.; Buszewski, B. Determination of volatile organic compounds as biomarkers of lung cancer by SPME–GC–TOF/MS and chemometrics. J. Chromatogr. B 2011, 879, 3360–3366. [Google Scholar] [CrossRef]
- Fens, N.; Roldaan, A.C.; Van der Schee, M.P.; Boksem, R.J.; Zwinderman, A.H.; Bel, E.H.; Sterk, P.J. External validation of exhaled breath profiling using an electronic nose in the discrimination of asthma with fixed airways obstruction and chronic obstructive pulmonary disease. Clin. Exp. Allergy 2011, 41, 1371–1378. [Google Scholar] [CrossRef]
- Smolinska, A.; Klaassen, E.M.M.; Dallinga, J.W.; Van de Kant, K.D.G.; Jobsis, Q.; Moonen, E.J.C.; Van Schayck, O.C.P.; Dompeling, E.; van Schooten, F.J. Profiling of Volatile Organic Compounds in Exhaled Breath As a Strategy to Find Early Predictive Signatures of Asthma in Children. PLoS ONE 2014, 9, e95668. [Google Scholar] [CrossRef]
- Phillips, M.; Gleeson, K.; Hughes, J.M.B.; Greenberg, J.; Cataneo, R.N.; Baker, L.; McVay, W.P. Volatile organic compounds in breath as markers of lung cancer: A cross-sectional study. Lancet 1999, 353, 1930–1933. [Google Scholar] [CrossRef]
- Phillips, M.; Cataneo, R.N.; Ditkoff, B.A.; Fisher, P.; Greenberg, J.; Gunawardena, R.; Kwon, C.S.; Tietje, O.; Wong, C. Prediction of breast cancer using volatile biomarkers in the breath. Breast Cancer Res. Treat. 2006, 99, 19–21. [Google Scholar] [CrossRef]
- Gaspar, E.M.; Lucena, A.F.; Duro da Costa, J.; Chaves das Neves, H. Organic metabolites in exhaled human breath—A multivariate approach for identification of biomarkers in lung disorders. J. Chromatogr. A 2009, 1216, 2749–2756. [Google Scholar] [CrossRef] [PubMed]
- Gaida, A.; Holz, O.; Nell, C.; Schuchardt, S.; Lavae-Mokhtari, B.; Kruse, L.; Boas, U.; Langejuergen, J.; Allers, M.; Zimmermann, S.; et al. A dual center study to compare breath volatile organic compounds from smokers and non-smokers with and without COPD. J. Breath Res. 2016, 10, 026006. [Google Scholar] [CrossRef]
- Ibrahim, B.; Basanta, M.; Cadden, P.; Singh, D.; Douce, D.; Woodcock, A.; Fowler, S.J. Non-invasive phenotyping using exhaled volatile organic compounds in asthma. Thorax 2011, 66, 804–809. [Google Scholar] [CrossRef]
- Martinez-Lozano Sinues, P.; Meier, L.; Berchtold, C.; Ivanov, M.; Sievi, N.; Camen, G.; Kohler, M.; Zenobi, R. Breath Analysis in Real Time by Mass Spectrometry in Chronic Obstructive Pulmonary Disease. Respiration 2014, 87, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Song, G.; Qin, T.; Liu, H.; Xu, G.-B.; Pan, Y.-Y.; Xiong, F.-X.; Gu, K.-S.; Sun, G.-P.; Chen, Z.-D. Quantitative breath analysis of volatile organic compounds of lung cancer patients. Lung Cancer 2010, 67, 227–231. [Google Scholar] [CrossRef] [PubMed]
- Dragonieri, S.; Schot, R.; Mertens, B.J.A.; Le Cessie, S.; Gauw, S.A.; Spanevello, A.; Resta, O.; Willard, N.P.; Vink, T.J.; Rabe, K.F.; et al. An electronic nose in the discrimination of patients with asthma and controls. J. Allergy Clin. Immunol. 2007, 120, 856–862. [Google Scholar] [CrossRef]
- Oguma, T.; Nagaoka, T.; Kurahashi, M.; Kobayashi, N.; Yamamori, S.; Tsuji, C.; Takiguchi, H.; Niimi, K.; Tomomatsu, H.; Tomomatsu, K.; et al. Clinical contributions of exhaled volatile organic compounds in the diagnosis of lung cancer. PLoS ONE 2017, 12, e0174802. [Google Scholar] [CrossRef]
- Chen, X.; Xu, F.; Wang, Y.; Pan, Y.; Lu, D.; Wang, P.; Ying, K.; Chen, E.; Zhang, W. A study of the volatile organic compounds exhaled by lung cancer cells in vitro for breath diagnosis. Cancer 2007, 110, 835–844. [Google Scholar] [CrossRef]
- Cazzola, M.; Segreti, A.; Capuano, R.; Bergamini, A.; Martinelli, E.; Calzetta, L.; Rogliani, P.; Ciaprini, C.; Ora, J.; Paolesse, R.; et al. Analysis of exhaled breath fingerprints and volatile organic compounds in COPD. COPD Res. Pract. 2015, 1, 7. [Google Scholar] [CrossRef]
- Van de Kant, K.D.G.; Van Berkel, J.J.B.N.; Jobsis, Q.; Lima Passos, V.; Klaassen, E.M.M.; Van der Sande, L.; Van Schayck, O.C.P.; De Jongste, J.C.; Van Schooten, F.J.; Derks, E.; et al. Exhaled breath profiling in diagnosing wheezy preschool children. Eur. Respir. J. 2013, 41, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Van Berkel, J.J.B.N.; Dallinga, J.W.; Möller, G.M.; Godschalk, R.W.L.; Moonen, E.J.; Wouters, E.F.M.; Van Schooten, F.J. A profile of volatile organic compounds in breath discriminates COPD patients from controls. Respir. Med. 2010, 104, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Van Vliet, D.; Smolinska, A.; Jöbsis, Q.; Rosias, P.P.R.; Muris, J.W.M.; Dallinga, J.W.; Van Schooten, F.J.; Dompeling, E. Association between exhaled inflammatory markers and asthma control in children. J. Breath Res. 2016, 10, 016014. [Google Scholar] [CrossRef] [PubMed]
- Peng, G.; Hakim, M.; Broza, Y.Y.; Billan, S.; Abdah-Bortnyak, R.; Kuten, A.; Tisch, U.; Haick, H. Detection of lung, breast, colorectal, and prostate cancers from exhaled breath using a single array of nanosensors. Br. J. Cancer 2010, 103, 542–551. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Analyte | Average Concentration (ppbv) | Frequency in Samples (%) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| H (SD) | CA (SD) | COPD (SD) | AS (SD) | Total | H | CA | COPD | AS | |||||
| 2-Methylbutane | 1.52 | (1.32) | 3.73 | (6.15) | 1.63 | (0.50) | 1.72 | (1.85) | 37.5 | 25.0 | 50.0 | 33.3 | 50.0 |
| Pentane | 1.66 | (0.67) | 2.21 | (1.09) | 1.87 | (0.53) | 2.11 | (2.26) | 51.8 | 45.0 | 62.5 | 41.7 | 50.0 |
| Ethanol | 70.60 | (95.14) | 179.08 | (132.87) | 218.64 | (216.1) | 100.89 | (108.96) | 98.2 | 95.0 | 93.8 | 100.0 | 100.0 |
| Isoprene | 32.85 | (34.01) | 34.19 | (30.08) | 34.61 | (20.9) | 48.70 | (16.95) | 100.0 | 95.0 | 100.0 | 100.0 | 100.0 |
| 2-Propanol | 10.55 | (9.30) | 230.66 | (190.62) | 258.37 | (255.01) | 123.42 | (67.37) | 85.7 | 55.0 | 100.0 | 100.0 | 100.0 |
| 2-Methylpentane | 1.24 | (0.30) | 3.44 | (2.41) | 2.61 | (2.07) | 4.59 | (5.57) | 55.4 | 25.0 | 75.0 | 75.0 | 50.0 |
| 3-Methylpentane | 0.24 | (0.12) | 0.93 | (0.72) | 1.27 | (0.49) | 1.07 | (1.25) | 35.7 | 10.0 | 68.8 | 33.3 | 25.0 |
| 1-Propanol | 14.59 | (14.63) | 34.10 | (37.73) | 28.15 | (38.54) | 9.94 | (5.77) | 100.0 | 95.0 | 100.0 | 100.0 | 100.0 |
| Methylcyclopentane | 1.80 | (0.53) | 2.49 | (1.11) | 2.20 | (0.47) | 2.20 | (0.27) | 87.5 | 75.0 | 93.8 | 83.3 | 100.0 |
| 2-Butanone | 1.74 | (1.15) | 1.93 | (1.30) | 1.45 | (1.00) | 1.26 | (0.80) | 80.4 | 55.0 | 100.0 | 83.3 | 87.5 |
| Benzene | 1.13 | (0.83) | 0.29 | (−) | 0.57 | (−) | 0.60 | (0.09) | 16.1 | 25.0 | 6.3 | 8.3 | 25.0 |
| Acetoin | 44.02 | (19.8) | 60.39 | (51.63) | 55.22 | (28.95) | 41.72 | (17.93) | 53.6 | 45.0 | 56.3 | 50.0 | 75.0 |
| Toluene | 6.23 | (8.38) | 0.98 | (1.40) | 0.63 | (0.42) | 0.89 | (0.60) | 55.4 | 40.0 | 75.0 | 58.3 | 50.0 |
| Ethylbenzene | 0.650 | (0.65) | 2.73 | (2.50) | 0.34 | (0.36) | 1.41 | (−) | 17.9 | 5.0 | 25.0 | 33.3 | 12.5 |
| p-Xylene | 1.15 | (0.92) | 1.62 | (1.86) | 1.40 | (1.11) | 1.97 | (0.95) | 41.1 | 25.0 | 50.0 | 58.3 | 37.5 |
| Styrene | 0.27 | (0.26) | 3.78 | (6.26) | 1.61 | (1.30) | 0.73 | (0.59) | 53.6 | 5.0 | 81.3 | 75.0 | 87.5 |
| Decane | nd | (−) | nd | (−) | 0.23 | (−) | nd | (−) | 1.8 | 0.0 | 0.0 | 8.3 | 0.0 |
| 6-Methyl-2-heptanone | 1.65 | (−) | 4.42 | (2.85) | 1.72 | (−) | 6.46 | (−) | 12.5 | 5.0 | 25.0 | 8.3 | 12.5 |
| Isododecane | 0.69 | (0.49) | 1.59 | (1.57) | 0.98 | (0.48) | 0.52 | (0.35) | 76.8 | 45.0 | 93.8 | 83.3 | 100.0 |
| 1,2,4-Trimethylbenzene | 0.83 | (0.61) | 2.55 | (1.94) | 2.60 | (2.46) | 1.42 | (0.76) | 82.1 | 50.0 | 93.8 | 100.0 | 100.0 |
| (E)-Ocimene | 1.16 | (0.80) | 4.64 | (4.03) | 2.95 | (1.99) | 2.98 | (1.54) | 82.1 | 50.0 | 100.0 | 91.7 | 100.0 |
| Limonene | 1.57 | (1.20) | 1.87 | (1.80) | 1.71 | (1.75) | 5.05 | (2.15) | 89.3 | 75.0 | 93.8 | 91.7 | 100.0 |
| m-Cymene | 0.61 | (0.21) | 0.41 | (0.35) | 0.38 | (0.23) | 0.32 | (0.21) | 46.4 | 10.0 | 62.5 | 50.0 | 87.5 |
| Benzonitrile | 1.44 | (1.23) | 3.57 | (3.95) | 4.57 | (2.64) | 2.12 | (1.67) | 78.6 | 50.0 | 93.8 | 91.7 | 87.5 |
| Phenol | nd | (−) | 52.78 | (47.13) | 75.02 | (72.16) | nd | (−) | 16.1 | 0.0 | 37.5 | 25.0 | 0.0 |
| Undecane | 0.80 | (0.11) | 3.83 | (3.09) | 2.44 | (1.38) | 1.78 | (0.30) | 41.1 | 20.0 | 75.0 | 41.7 | 25.0 |
| Dodecane | 5.18 | (0.72) | 10.58 | (8.66) | 9.51 | (7.18) | 6.27 | (3.19) | 73.2 | 45.0 | 87.5 | 91.7 | 87.5 |
| Terpineol | 3.57 | (0.30) | 17.36 | (21.72) | 26.53 | (36.34) | 6.87 | (6.38) | 71.4 | 15.0 | 100.0 | 100.0 | 100.0 |
| Tridecane | 3.43 | (1.69) | 42.16 | (38.89) | 28.36 | (21.59) | 8.59 | (7.87) | 51.8 | 10.0 | 75.0 | 75.0 | 75.0 |
| Statistics by Class | Sensitivity | Specificity | AUC | Balanced Accuracy |
|---|---|---|---|---|
| Asthma | 75.0% | 100% | 0.872 | 87.5% |
| Lung cancer | 93.8% | 87.5% | 0.956 | 90.6% |
| COPD | 67.0% | 97.7% | 0.935 | 82.2% |
| Healthy | 95.0% | 94.5% | 0.994 | 94.7% |
| RF overall accuracy (95% CI) | 85.7% (73.7–93.6) | |||
| Condition | Coefficients | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Intercept | 2-Propanol | 3-Methyl-pentane | (E)-Ocimene | Limonene | m-Cymene | Benzonitrile | Undecane | Terpineol | Phenol | |
| AS | −557.79 | 0.56 | 17.03 | 50.39 | 100.40 | 212.50 | −22.69 | −88.94 | 32.33 | −12.95 |
| (SE) | (42.62) | (0.37) | (2.55) | (2.48) | (10.34) | (11.52) | (1.32) | (3.64) | (1.31) | (5.31) |
| CA | −127.12 | 0.61 | −129.32 | 32.92 | 32.33 | 31.11 | −96.07 | 26.50 | 32.81 | −1.89 |
| (SE) | (29.25) | (0.38) | (17.43) | (8.11) | (9.90) | (6.47) | (16.91) | (11.17) | (8.40) | (0.86) |
| COPD | −23.49 | 0.49 | −269.07 | −64.27 | 11.09 | −72.04 | −7.72 | −111.52 | 37.91 | 1.73 |
| (SE) | (3.35) | (0.83) | (6.92) | (8.57) | (3.39) | (0.66) | (1.29) | (4.22) | (8.18) | (0.65) |
| Statistics by Class | Sensitivity | Specificity | AUC | Balanced Accuracy |
|---|---|---|---|---|
| Asthma | 68.0% | 100% | 0.700 | 83.4% |
| Lung cancer | 83.4% | 93.4% | 0.950 | 88.4% |
| COPD | 100% | 94.1% | 0.971 | 97.1% |
| Healthy | 100% | 100% | 1.000 | 100% |
| MLR overall accuracy (95% CI) | 91.0% (70.0–99.0) | |||
| Group | Control | Positive | p | |||
|---|---|---|---|---|---|---|
| n | % | n | % | |||
| Total | 20 | 36 | 0.367 | |||
| Gender | Male | 13 | 65.0% | 27 | 75.0% | 0.325 |
| Female | 7 | 35.0% | 9 | 25.0% | 0.437 | |
| Age (SD) | 41.2 (10.1) | 66.8 (8.22) | 0.078 | |||
| Smoking status | Active smoker | 2 | 10.0% | 5 (2 COPD, 3 CA) | 13.9% | 0.287 |
| Ex-smoker | 2 | 10.0% | 22 (12 CA, 10 COPD) | 61.1% | 0.083 | |
| Non-smoker | 16 | 80.0% | 9 (1 CA, 8 AS) | 25.0% | 0.640 | |
| Condition | Lung cancer | − | 16 | 44.4% | ||
| COPD | − | 12 | 33.3% | − | ||
| Asthma | − | 8 | 22.2% | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Monedeiro, F.; Monedeiro-Milanowski, M.; Ratiu, I.-A.; Brożek, B.; Ligor, T.; Buszewski, B. Needle Trap Device-GC-MS for Characterization of Lung Diseases Based on Breath VOC Profiles. Molecules 2021, 26, 1789. https://doi.org/10.3390/molecules26061789
Monedeiro F, Monedeiro-Milanowski M, Ratiu I-A, Brożek B, Ligor T, Buszewski B. Needle Trap Device-GC-MS for Characterization of Lung Diseases Based on Breath VOC Profiles. Molecules. 2021; 26(6):1789. https://doi.org/10.3390/molecules26061789
Chicago/Turabian StyleMonedeiro, Fernanda, Maciej Monedeiro-Milanowski, Ileana-Andreea Ratiu, Beata Brożek, Tomasz Ligor, and Bogusław Buszewski. 2021. "Needle Trap Device-GC-MS for Characterization of Lung Diseases Based on Breath VOC Profiles" Molecules 26, no. 6: 1789. https://doi.org/10.3390/molecules26061789
APA StyleMonedeiro, F., Monedeiro-Milanowski, M., Ratiu, I.-A., Brożek, B., Ligor, T., & Buszewski, B. (2021). Needle Trap Device-GC-MS for Characterization of Lung Diseases Based on Breath VOC Profiles. Molecules, 26(6), 1789. https://doi.org/10.3390/molecules26061789