
Consumption of Sinlek Rice Drink Improved Red Cell Indices in Anemic Elderly Subjects

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Subject Information
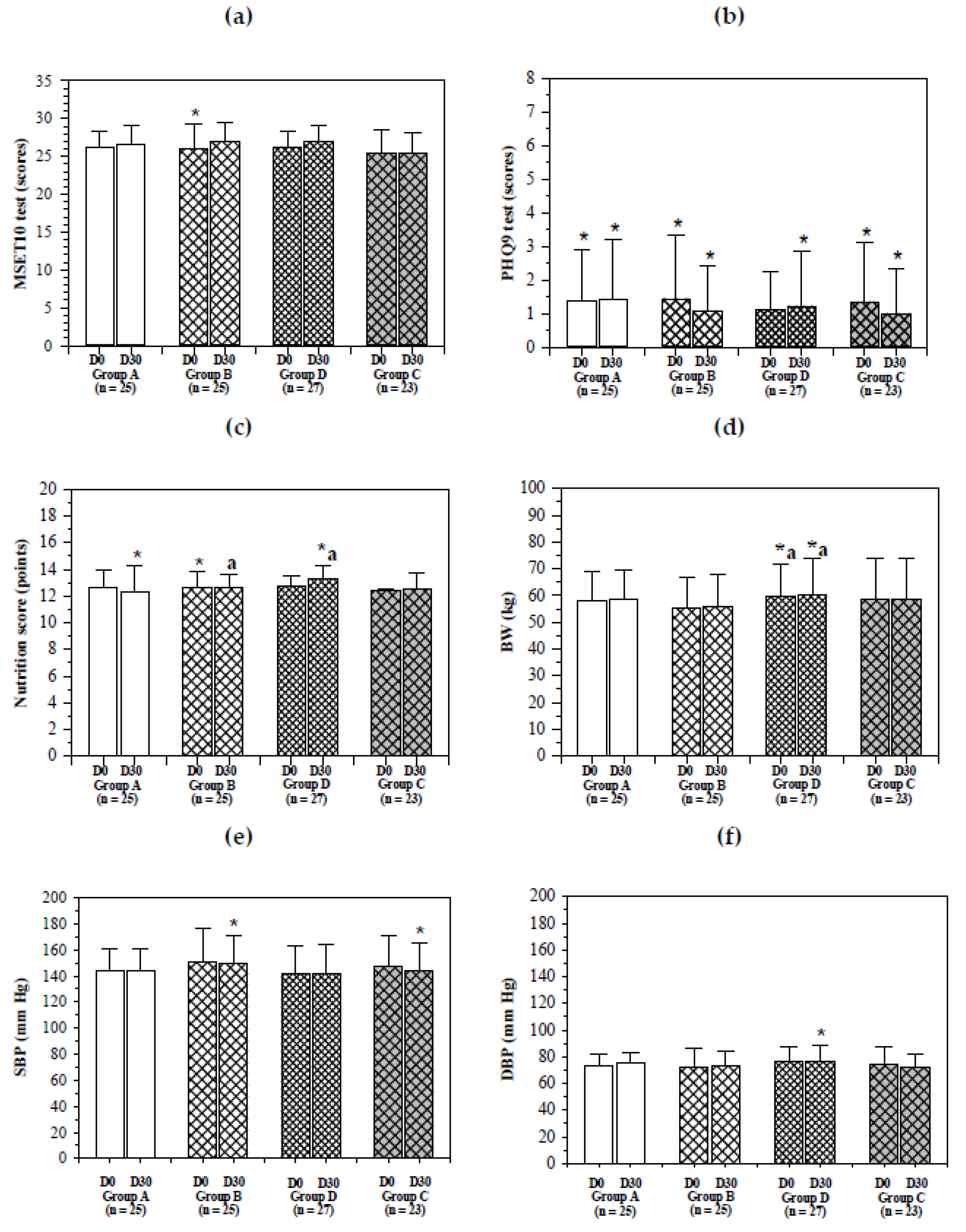
2.2. Health, Nutritional Scores and Neurological Function
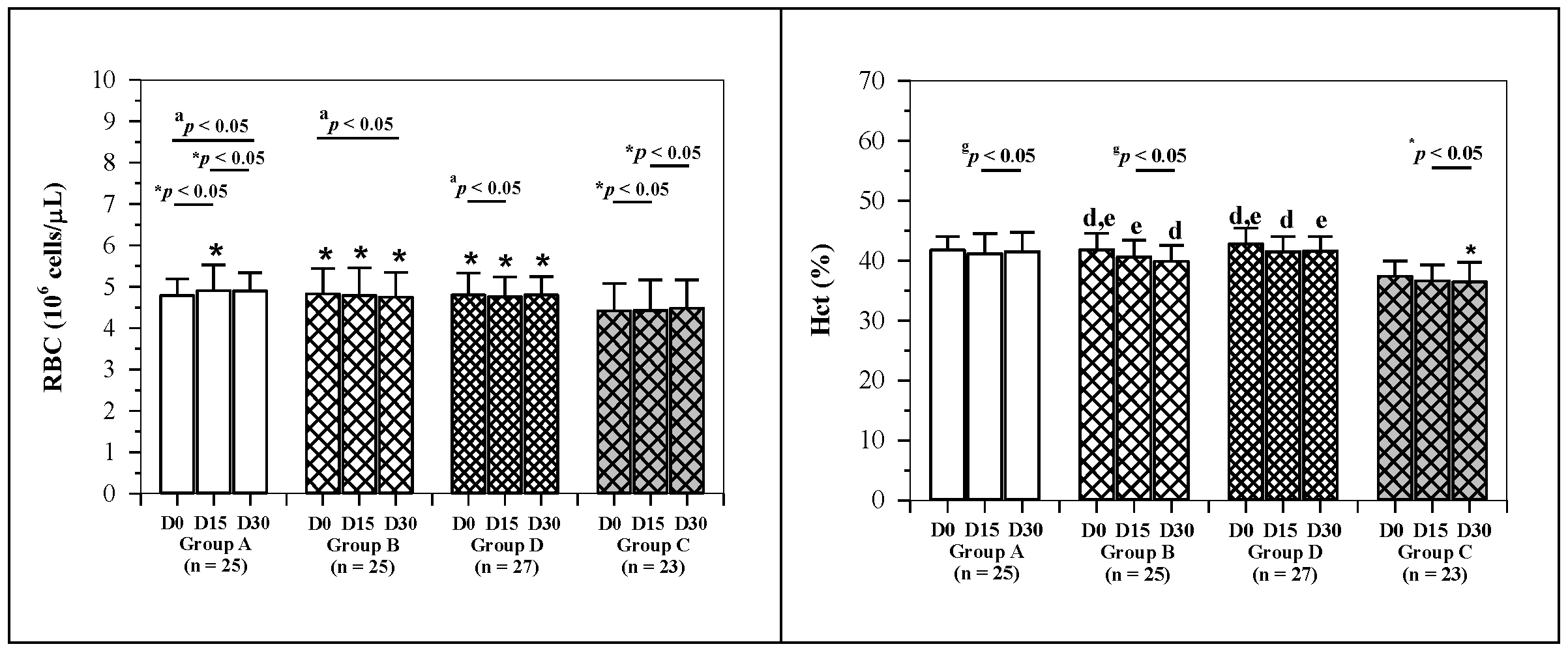
2.3. Hematopoietic Activity
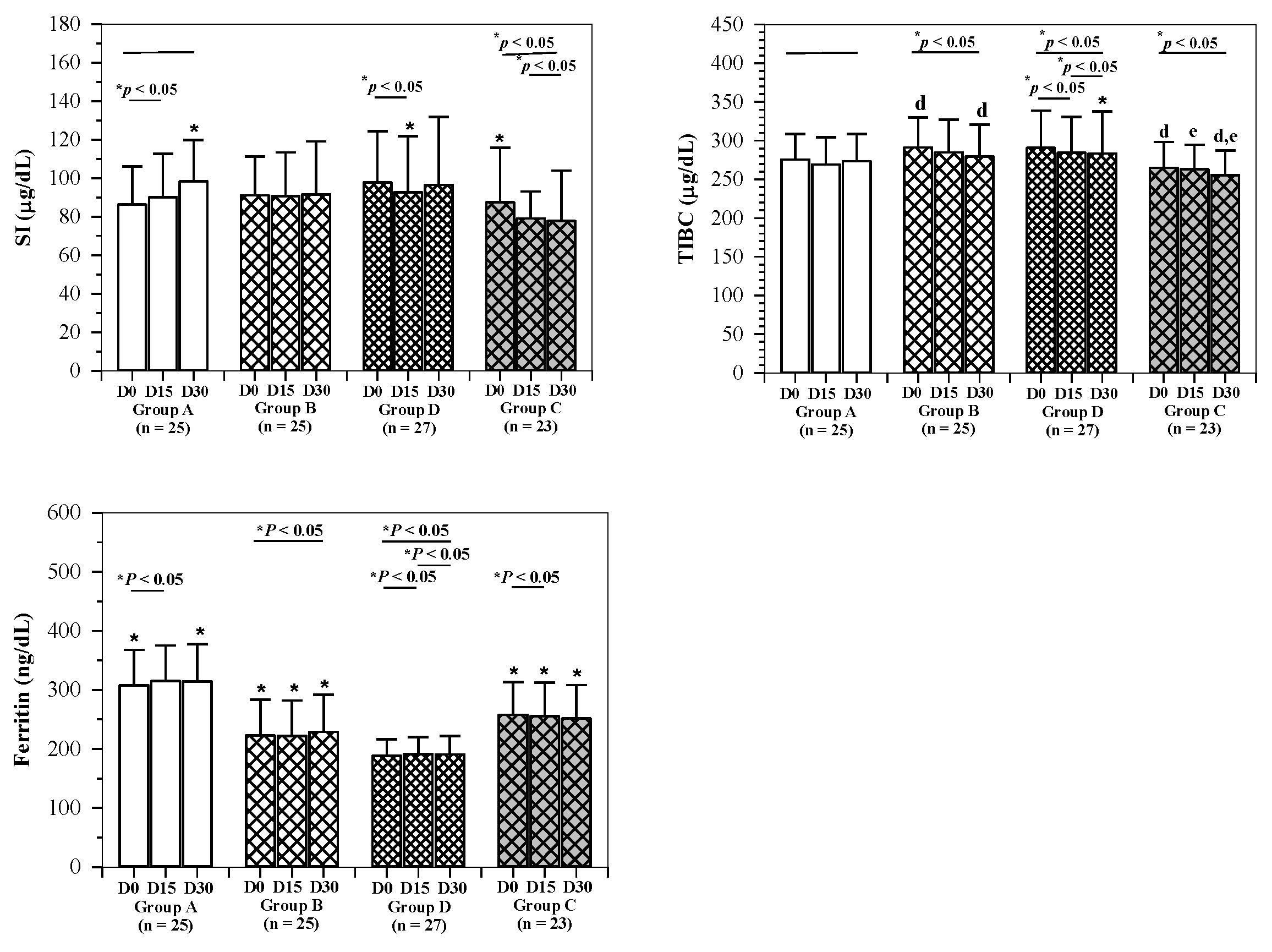
2.4. Iron Status
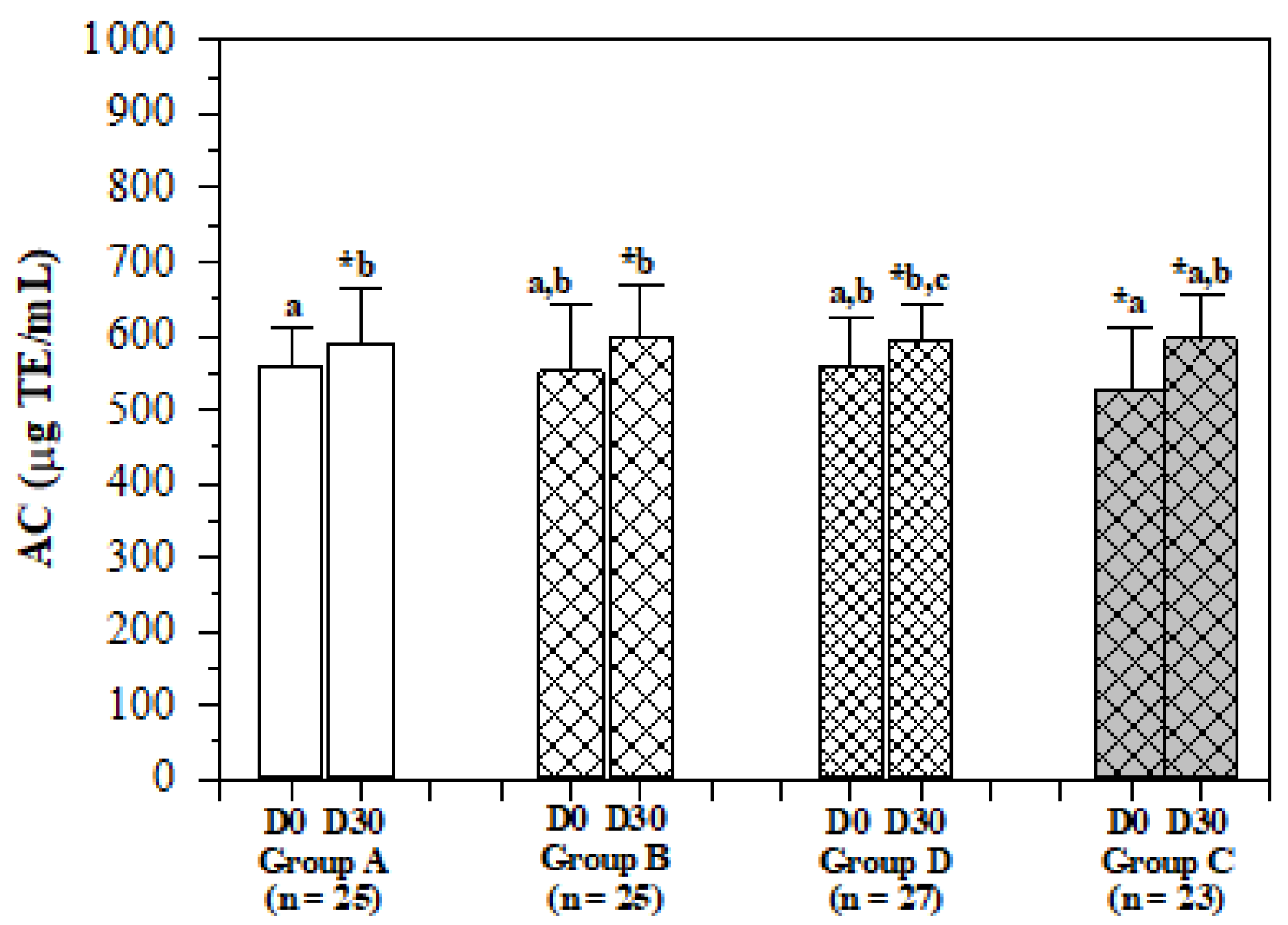
2.5. Serum Antioxidant Capacity
2.6. Blood Biochemical Parameters
3. Discussion
4. Materials and Methods
4.1. Materials
4.1.1. Chemicals and Reagents
4.1.2. Food Ingredients
4.2. Production of Rice Drink
4.3. Subject Recruitment
4.4. Administration of Rice Drinks
4.5. Physical Examination, Psychological and Nutrition Testing
4.6. Blood Analysis
4.7. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Sample Availability
Abbreviations
References
- Lopez, A.; Cacoub, P.; Macdougall, I.C.; Peyrin-Biroulet, L. Iron deficiency anaemia. Lancet 2016, 387, 907–916. [Google Scholar] [CrossRef]
- Galloway, R.; Dusch, E.; Elder, L.; Achadi, E.; Grajeda, R.; Hurtado, E.; Favin, M.; Kanani, S.; Marsaban, J.; Meda, N.; et al. Women’s perceptions of iron deficiency and anemia prevention and control in eight developing countries. Soc. Sci. Med. 2002, 55, 529–544. [Google Scholar] [CrossRef]
- Roger, S.D.; Tio, M.; Park, H.C.; Choong, H.L.; Goh, B.; Cushway, T.R.; Stevens, V.; Macdougall, I.C. Intravenous iron and erythropoiesis-stimulating agents in haemodialysis: A systematic review and meta-analysis. Nephrology (Carlton) 2016, 22, 969–976. [Google Scholar] [CrossRef] [Green Version]
- Wang, K.; Li, L.; Xu, X.; Lu, L.; Wang, J.; Wang, S.; Wang, Y.; Jin, Z.; Zhang, J.Z.; Jiang, Y. Fe3O4@ Astragalus polysaccharide core-shell nanoparticles for iron deficiency anemia therapy and magnetic resonance imaging in vivo. ACS Appl. Mater. Interfaces 2019, 11, 10452–10461. [Google Scholar] [CrossRef] [Green Version]
- Bianchi, V.E. Role of nutrition on anemia in elderly. Clin. Nutr. ESPEN 2016, 11, e1–e11. [Google Scholar] [CrossRef]
- Beard, J.L.; Richards, R.E.; Smiciklas-Wright, H.; Bernardo, V.; Kordish, S. Iron nutrition in rural home bound elderly persons. J. Nutr. Elder. 1996, 15, 3–19. [Google Scholar] [CrossRef]
- Meng, F.; Wei, Y.; Yang, X. Iron content and bioavailability in rice. J. Trace Elem. Med. Biol. 2005, 18, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Schaffer, S.; Pallauf, J.; Krawinkel, M.B. Impact of feeding high-iron rice on plasma iron, hemoglobin and red blood cell variables of early-weaned piglets. A Pilot Study. Ann. Nutr. Metab. 2004, 48, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Prom, U.T.C.; Rashid, A.; Ram, H.; Zou, C.; Guilherme, L.R.G.; Corguinha, A.P.B.; Guo, S.; Kaur, C.; Naeem, A.; Yamuangmorn, S.; et al. Simultaneous biofortification of rice with zinc, iodine, iron and selenium through foliar treatment of a micronutrient cocktail in five countries. Front. Plant. Sci. 2020, 11, 589835. [Google Scholar] [CrossRef] [PubMed]
- Bevilacqua, A.; Casanova, F.P.; Petruzzi, L.; Sinigaglia, M.; Corbo, M.R. Using physical approaches for the attenuation of lactic acid bacteria in an organic rice beverage. Food Microbiol. 2015, 53, 1–8. [Google Scholar] [CrossRef]
- Korcok, D.J.; Trsic-Milanovic, N.A.; Ivanovic, N.D.; Dordevic, B.I. Development of probiotic formulation for the treatment of iron deficiency anemia. Chem. Pharm. Bull. (Tokyo) 2018, 66, 347–352. [Google Scholar] [CrossRef] [Green Version]
- Watchararuji, K.; Goto, M.; Sasaki, M.; Shotipruk, A. Value-added subcritical water hydrolysate from rice bran and soybean meal. Bioresour. Technol. 2008, 99, 6207–6213. [Google Scholar] [CrossRef]
- Liabeuf, S.; Gras, V.; Moragny, J.; Laroche, M.L.; Andrejak, M. Ulceration of the oral mucosa following direct contact with ferrous sulfate in elderly patients: A case report and a review of the French National Pharmacovigilance Database. Clin. Interv. Aging 2014, 9, 737–740. [Google Scholar] [CrossRef] [Green Version]
- Bashir, K.; Takahashi, R.; Nakanishi, H.; Nishizawa, N.K. The road to micronutrient biofortification of rice: Progress and prospects. Front. Plant. Sci. 2013, 4, 15. [Google Scholar] [CrossRef] [Green Version]
- Finkelstein, J.L.; Fothergill, A.; Hackl, L.S.; Haas, J.D.; Mehta, S. Iron biofortification interventions to improve iron status and functional outcomes. Proc. Nutr. Soc. 2019, 78, 197–207. [Google Scholar] [CrossRef]
- Jeng, T.L.; Shih, Y.J.; Ho, P.T.; Lai, C.C.; Lin, Y.W.; Wang, C.S.; Sung, J.M. Gamma-Oryzanol, tocol and mineral compositions in different grain fractions of giant embryo rice mutants. J. Sci. Food Agric. 2011, 92, 1468–1474. [Google Scholar] [CrossRef]
- Min, B.; McClung, A.; Chen, M.H. Effects of hydrothermal processes on antioxidants in brown, purple and red bran whole grain rice (Oryza sativa L.). Food Chem. 2014, 159. [Google Scholar] [CrossRef] [PubMed]
- Sangani, R.G.; Ghio, A.J. Iron, human growth, and the global epidemic of obesity. Nutrients 2013, 5, 4231–4249. [Google Scholar] [CrossRef] [PubMed]
- Deng, Q.; Wang, Y.; Wang, X.; Wang, Q.; Yi, Z.; Xia, J.; Hu, Y.; Zhang, Y.; Wang, J.; Wang, L.; et al. Effects of dietary iron level on growth performance, hematological status, and intestinal function in growing-finishing pigs. J. Anim. Sci. 2021, 99. [Google Scholar] [CrossRef] [PubMed]
- Banach, W.; Nitschke, K.; Krajewska, N.; Mongiallo, W.; Matuszak, O.; Muszynski, J.; Skrypnik, D. The association between excess body mass and disturbances in somatic mineral levels. Int. J. Mol. Sci. 2020, 21, 7306. [Google Scholar] [CrossRef]
- de Pee, S. Proposing nutrients and nutrient levels for rice fortification. Ann. N. Y. Acad. Sci. 2014, 1324, 55–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hackl, L.S.; Abizari, A.R.; Speich, C.; Zungbey-Garti, H.; Cercamondi, C.I.; Zeder, C.; Zimmermann, M.B.; Moretti, D. Effects of dietary iron level on growth performance, hematological status, and intestinal function in growing-finishing pigs. Sci. Adv. 2016, 5, eaau0790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chitpan, M.; Chavasit, V.; Kongkachuichai, R. Development of fortified dried broken rice as a complementary food. Food Nutr. Bull. 2005, 26, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Bothwell, T.H.; MacPhail, A.P. The potential role of NaFeEDTA as an iron fortificant. Int. J. Vitam. Nutr. Res. 2004, 74, 421–434. [Google Scholar] [CrossRef] [PubMed]
- Hurrell, R.F. Iron fortification: Its efficacy and safety in relation to infections. Food Nutr. Bull. 2007, 28, S585–S594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nielsen, P.; Gabbe, E.E.; Fischer, R.; Heinrich, H.C. Bioavailability of iron from oral ferric polymaltose in humans. Arzneimittelforschung 1994, 44, 743–748. [Google Scholar] [PubMed]
- Sultana, T.; DeVita, M.V.; Michelis, M.F. Oral vitamin C supplementation reduces erythropoietin requirement in hemodialysis patients with functional iron deficiency. Int. Urol. Nephrol. 2016, 48, 1519–1524. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, M.J.; Ward, R.J.; Baum, H.; Peters, T.J. Iron release from haemosiderin and ferritin by therapeutic and physiological chelators. Biochem. J. 1989, 260, 903–907. [Google Scholar] [CrossRef] [Green Version]
- Martinez, R.; Brassard, P.; Mwanjewe, J.; Grover, A.K. Iron promotes cadmium binding to citrate. Mol. Cell Biochem. 2001, 225, 93–96. [Google Scholar] [CrossRef]
- Watanapaisantrakul, R.; Chavasit, V.; Kongkachuichai, R. Fortification of soy sauce using various iron sources: Sensory acceptability and shelf stability. Food Nutr. Bull. 2006, 27, 19–25. [Google Scholar] [CrossRef] [Green Version]
- Koonyosying, P.; Tantiworawit, A.; Hantrakool, S.; Utama-Ang, N.; Cresswell, M.; Fucharoen, S.; Porter, J.B.; Srichairatanakool, S. Consumption of a green tea extract-curcumin drink decreases blood urea nitrogen and redox iron in beta-thalassemia patients. Food Funct. 2020, 11, 932–943. [Google Scholar] [CrossRef] [PubMed]
- Pasricha, S.R.; Tye-Din, J.; Muckenthaler, M.U.; Swinkels, D.W. Iron deficiency. Lancet 2021, 397, 233–248. [Google Scholar] [CrossRef]
- Thankachan, P.; Rah, J.H.; Thomas, T.; Selvam, S.; Amalrajan, V.; Srinivasan, K.; Steiger, G.; Kurpad, A.V. Multiple micronutrient-fortified rice affects physical performance and plasma vitamin B-12 and homocysteine concentrations of Indian school children. J. Nutr. 2012, 142, 846–852. [Google Scholar] [CrossRef] [Green Version]
- Kuong, K.; Fiorentino, M.; Perignon, M.; Chamnan, C.; Berger, J.; Sinuon, M.; Molyden, V.; Burja, K.; Parker, M.; Ly, S.C.; et al. Cognitive performance and iron status are negatively associated with hookworm infection in cambodian schoolchildren. Am. J. Trop. Med. Hyg. 2016, 95, 856–863. [Google Scholar] [CrossRef]
- de Gier, B.; Campos Ponce, M.; Perignon, M.; Fiorentino, M.; Khov, K.; Chamnan, C.; de Boer, M.R.; Parker, M.E.; Burja, K.; Dijkhuizen, M.A.; et al. Micronutrient-fortified rice can increase hookworm infection risk: A cluster randomized trial. PLoS One 2016, 11, e0145351. [Google Scholar] [CrossRef]
- Mahapatra, S.; Parker, M.E.; Dave, N.; Zobrist, S.C.; Shajie Arul, D.; King, A.; Betigeri, A.; Sachdeva, R. Micronutrient-fortified rice improves haemoglobin, anaemia prevalence and cognitive performance among schoolchildren in Gujarat, India: A case-control study. Int. J. Food Sci. Nutr. 2021, 72, 690–703. [Google Scholar] [CrossRef]
- Sen, C.K.; Khanna, S.; Roy, S. Tocotrienol: The natural vitamin E to defend the nervous system? Ann. N. Y. Acad. Sci. 2004, 1031, 127–142. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T.; Nakaso, K.; Horikoshi, Y.; Hanaki, T.; Yamakawa, M.; Nakasone, M.; Kitagawa, Y.; Koike, T.; Matsura, T. Rice bran dietary supplementation improves neurological symptoms and loss of Purkinje cells in vitamin E-deficient mice. Yonago Acta Med. 2016, 59, 188–195. [Google Scholar]
- Um, M.Y.; Kim, S.; Jin, Y.H.; Yoon, M.; Yang, H.; Lee, J.; Jung, J.; Urade, Y.; Huang, Z.L.; Kwon, S.; et al. A novel neurological function of rice bran: A standardized rice bran supplement promotes non-rapid eye movement sleep in mice through histamine H1 receptors. Mol. Nutr. Food Res. 2017, 61. [Google Scholar] [CrossRef]
- Shi, Z.; El-Obeid, T.; Li, M.; Xu, X.; Liu, J. Iron-related dietary pattern increases the risk of poor cognition. Nutr. J. 2019, 18, 48. [Google Scholar] [CrossRef] [Green Version]
- Belaidi, A.A.; Bush, A.I. Iron neurochemistry in Alzheimer’s disease and Parkinson’s disease: Targets for therapeutics. J. Neurochem. 2016, 139 (Suppl. 1), 179–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agrawal, S.; Berggren, K.L.; Marks, E.; Fox, J.H. Impact of high iron intake on cognition and neurodegeneration in humans and in animal models: A systematic review. Nutr. Rev. 2017, 75, 456–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bao, W.; Rong, Y.; Rong, S.; Liu, L. Dietary iron intake, body iron stores, and the risk of type 2 diabetes: A systematic review and meta-analysis. BMC Med. 2012, 10, 119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Logroscino, G.; Gao, X.; Chen, H.; Wing, A.; Ascherio, A. Dietary iron intake and risk of Parkinson’s disease. Am. J. Epidemiol. 2008, 168, 1381–1388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nogueira Arcanjo, F.P.; Santos, P.R.; Arcanjo, C.P.; Amancio, O.M.; Braga, J.A. Use of iron-fortified rice reduces anemia in infants. J. Trop. Pediatr. 2012, 58, 475–480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moretti, D.; Zimmermann, M.B.; Muthayya, S.; Thankachan, P.; Lee, T.C.; Kurpad, A.V.; Hurrell, R.F. Extruded rice fortified with micronized ground ferric pyrophosphate reduces iron deficiency in Indian schoolchildren: A double-blind randomized controlled trial. Am. J. Clin. Nutr. 2006, 84, 822–829. [Google Scholar] [CrossRef] [Green Version]
- Schumann, K.; Longfils, P.; Monchy, D.; von Xylander, S.; Weinheimer, H.; Solomons, N.W. Efficacy and safety of twice-weekly administration of three RDAs of iron and folic acid with and without complement of 14 essential micronutrients at one or two RDAs: A placebo-controlled intervention trial in anemic Cambodian infants 6 to 24 months of age. Eur. J. Clin. Nutr. 2009, 63, 355–368. [Google Scholar] [CrossRef]
- Koonyosying, P.; Flemming, B.; Ekwattanakit, S.; Viprakasit, V.; Fucharoen, S.; Srichairatanakool, S. Optimal use of Thai Sinlek rice (IR) provides the nutraceutical effect on erythropoiesis in rats. Blood 2019, 134, S4808. [Google Scholar] [CrossRef]
- Moor, M.A.; Fraga, M.A.; Garfein, R.S.; Rashidi, H.H.; Alcaraz, J.; Kritz-Silverstein, D.; Elder, J.P.; Brodine, S.K. Individual and community factors contributing to anemia among women in rural Baja California, Mexico. PLoS One 2017, 12, e0188590. [Google Scholar] [CrossRef] [Green Version]
- Szymura, J.; Wiecek, M.; Maciejczyk, M.; Gradek, J.; Kantorowicz, M.; Szygula, Z. Unchanged erythrocyte profile after exposure to cryogenic temperatures in elder marathon runners. Front. Physiol. 2018, 9, 659. [Google Scholar] [CrossRef] [Green Version]
- Bousounis, P.; Bergo, V.; Trompouki, E. Inflammation, aging and hematopoiesis: A complex relationship. Cells 2021, 10, 1386. [Google Scholar] [CrossRef]
- Angeles-Agdeppa, I.; Capanzana, M.V.; Barba, C.V.; Florentino, R.F.; Takanashi, K. Efficacy of iron-fortified rice in reducing anemia among schoolchildren in the Philippines. Int. J. Vitam. Nutr. Res. 2008, 78, 74–86. [Google Scholar] [CrossRef]
- Bries, A.E.; Hurrell, R.F.; Reddy, M.B. Iron absorption from bouillon fortified with iron-enriched Aspergillus oryzae Is higher than that fortified with ferric pyrophosphate in young women. J. Nutr. 2020, 150, 1109–1115. [Google Scholar] [CrossRef]
- Cerven, D.; DeGeorge, G.; Bethell, D. 28-Day repeated dose oral toxicity of recombinant human apo-lactoferrin or recombinant human lysozyme in rats. Regul. Toxicol. Pharmacol. 2008, 51, 162–167. [Google Scholar] [CrossRef]
- Commenges, D.; Scotet, V.; Renaud, S.; Jacqmin-Gadda, H.; Barberger-Gateau, P.; Dartigues, J.F. Intake of flavonoids and risk of dementia. Eur. J. Epidemiol. 2000, 16, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Vauzour, D.; Vafeiadou, K.; Rodriguez-Mateos, A.; Rendeiro, C.; Spencer, J.P. The neuroprotective potential of flavonoids: A multiplicity of effects. Genes Nutr. 2008, 3, 115–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caldwell, K.; Charlton, K.E.; Roodenrys, S.; Jenner, A. Anthocyanin-rich cherry juice does not improve acute cognitive performance on RAVLT. Nutr. Neurosci. 2015, 19, 423–424. [Google Scholar] [CrossRef] [PubMed]
- McGrattan, A.M.; McGuinness, B.; McKinley, M.C.; Kee, F.; Passmore, P.; Woodside, J.V.; McEvoy, C.T. Diet and inflammation in cognitive ageing and Alzheimer’s disease. Curr. Nutr. Rep. 2019, 8, 53–65. [Google Scholar] [CrossRef] [Green Version]
- Inagawa, H.; Saika, T.; Nishiyama, N.; Nisizawa, T.; Kohchi, C.; Uenobe, M.; Soma, G.I. Dewaxed brown rice feed improves fatty liver in obese and diabetic model mice. Anticancer Res. 2018, 38, 4339–4345. [Google Scholar] [CrossRef]
- Hou, Z.; Qin, P.; Ren, G. Effect of anthocyanin-rich extract from black rice (Oryza sativa L. Japonica) on chronically alcohol-induced liver damage in rats. J. Agric. Food Chem. 2010, 58, 3191–3196. [Google Scholar] [CrossRef]
- Mohd Esa, N.; Abdul Kadir, K.K.; Amom, Z.; Azlan, A. Antioxidant activity of white rice, brown rice and germinated brown rice (in vivo and in vitro) and the effects on lipid peroxidation and liver enzymes in hyperlipidaemic rabbits. Food Chem. 2013, 141, 1306–1312. [Google Scholar] [CrossRef] [PubMed]
- Jung, E.H.; Kim, S.R.; Hwang, I.K.; Ha, T.Y. Hypoglycemic effects of a phenolic acid fraction of rice bran and ferulic acid in C57BL/KsJ-db/db mice. J. Agric. Food Chem. 2007, 55, 9800–9804. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Chen, L.; Zhang, H.; Zhang, Y.; Wang, L.; Qian, H.; Qi, X. In vitro and in vivo antioxidant activity of ethyl acetate extraction of purple rice. Cell Mol. Biol. (Noisy-le-grand) 2016, 62, 96–103. [Google Scholar]
- Cicero, A.F.G.; Fogacci, F.; Bove, M.; Veronesi, M.; Rizzo, M.; Giovannini, M.; Borghi, C. Short-term effects of a combined nutraceutical on lipid level, fatty liver biomarkers, hemodynamic parameters, and estimated cardiovascular disease risk: A double-blind, placebo-controlled randomized clinical trial. Adv. Ther. 2017, 34, 1966–1975. [Google Scholar] [CrossRef] [PubMed]
- Sartore, G.; Seraglia, R.; Burlina, S.; Bolis, A.; Marin, R.; Manzato, E.; Ragazzi, E.; Traldi, P.; Lapolla, A. High-density lipoprotein oxidation in type 2 diabetic patients and young patients with premature myocardial infarction. Nutr. Metab. Cardiovasc. Dis. 2014, 25, 418–425. [Google Scholar] [CrossRef]
- Nuttall, K.L.; Gordon, W.H.; Ash, K.O. Inductively coupled plasma mass spectrometry for trace element analysis in the clinical laboratory. Ann. Clin. Lab. Sci. 1995, 25, 264–271. [Google Scholar]
- Compendium of Methods for Food Analysis/cDepartment of Medical Sciences and National Bureau of Agriculture Commodity and Food Standards; Department of Medical Sciences and National Bureau of Agriculture Commodity and Food Standards, Ministry of Public Health: Nonthaburi, Thailand, 2003.
- Boonvisudhi, T.; Kuladee, S. Association between internet addiction and depression in Thai medical students at Faculty of Medicine, Ramathibodi Hospital. PLoS One 2017, 12, e0174209. [Google Scholar] [CrossRef]
- Senanarong, V.; Vannasaeng, S.; Poungvarin, N.; Ploybutr, S.; Udompunthurak, S.; Jamjumras, P.; Fairbanks, L.; Cummings, J.L. Endogenous estradiol in elderly individuals: Cognitive and noncognitive associations. Arch. Neurol. 2002, 59, 385–389. [Google Scholar] [CrossRef] [Green Version]
- Trongsakul, S.; Lambert, R.; Clark, A.; Wongpakaran, N.; Cross, J. Development of the Thai version of Mini-Cog, a brief cognitive screening test. Geriatr. Gerontol. Int. 2014, 15, 594–600. [Google Scholar] [CrossRef]
- Velasco-Rodriguez, R.; Perez-Hernandez, M.G.; Mora-Brambila, A.B.; Bazan-Arellano, D.A.; Vasquez, C. Serum ferritin and nutritional status in older adults at eldercare facilities. J. Nutr. Health Aging 2012, 16, 525–528. [Google Scholar] [CrossRef]
- Schlosnagle, D.C.; Hutton, P.S.; Conn, R.B. Ferrozine assay of serum iron and total iron-binding capacity adapted to the COBAS BIO centrifugal analyzer. Clin. Chem. 1982, 28, 1730–1732. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Number (Percentage) of Subjects | p-Value When All Groups Were Compared | ||||
|---|---|---|---|---|---|---|
| Non-Anemic | Anemic | |||||
| Group A | Group B | Group D | Group C | |||
| Gender | Male | 7 (28.00) | 4 (16.00) | 2 (7.41) | 12 (52.17) | p = 0.002 * |
| Female | 18 (72.00) | 21 (84.00) | 25 (92.59) | 11 (47.83) | ||
| Age (years) | 60–69 | 13 (52.00) | 10 (40.00) | 18 (66.67) | 5 (21.74) | p = 0.019 ** |
| 70–79 | 11 (44.00) | 11 (44.00) | 5 (18.52) | 12 (52.17) | ||
| ≥80 | 1 (4.00) | 4 (16.00) | 4 (14.81) | 6 (26.09) | ||
| Marital status | Single | 3 (12.00) | 3 (12.00) | 3 (11.11) | 3 (13.04) | p = 0.491 ** |
| Couple | 13 (52.00) | 11 (44.00) | 10 (37.04) | 8 (34.78) | ||
| Divorce/separate | 0 | 0 | 3 (11.11) | 4 (17.39) | ||
| Widow | 9 (36.00) | 11 (44.00) | 11 (40.74) | 8 (34.78) | ||
| Education | Primary school | 15 (60.00) | 18 (72.00) | 17 (62.96) | 13 (56.62) | p = 0.485 ** |
| Secondary school | 0 | 1 (4.00) | 0 | 2 (8.70) | ||
| High school | 6 (24.00) | 0 | 5 (18.52) | 3 (13.04) | ||
| Under graduate | 2 (8.00) | 3 (12.00) | 1 (3.70) | 2 (8.70) | ||
| Postgraduate | 0 | 1 (4.00) | 1 (3.70) | 1 (4.35) | ||
| Other | 2 (8.00) | 2 (8.00) | 3 (11.11) | 2 (8.70) | ||
| Profession | No | 16 (64.00) | 13 (52.00) | 18 (66.67) | 10 (43.48) | p = 0.704 ** |
| Agriculture | 0 | 1 (4.00) | 0 | 3 (13.04) | ||
| Worker | 0 | 2 (8.00) | 1 (3.70) | 3 (13.04) | ||
| Merchant | 3 (12.00) | 3 (12.00) | 2 (7.41) | 2 (8.70) | ||
| Pension | 2 (8.00) | 2 (8.00) | 3 (11.11) | 1 (4.35) | ||
| Other | 4 (16.00) | 4 (16.00) | 3 (11.11) | 4 (17.39) | ||
| Health Information | Number (Percentage) of Subjects | p-Value When All Groups Were Compared | ||||
|---|---|---|---|---|---|---|
| Non-Anemic | Anemic | |||||
| Group A | Group B | Group D | Group C | |||
| BMI (kg/m2) | <18.5 | 0 | 1 (4.00) | 0 | 1 (4.35) | p = 0.911 ** |
| 18.5–22.9 | 9 (36.00) | 10 (40.00) | 10 (37.04) | 7 (30.43) | ||
| ≥23 | 16 (64.00) | 14 (56.00) | 17 (62.96) | 15 (65.22) | ||
| Chronic diseases | 17/25 (68.00) | 12/25 (48.00) | 18/27 (66.67) | 19/23 (82.91) | p = 0.090 * | |
| Hypertension | 11/25 (44.00) | 9/25 (36.00) | 13/27 (48.15) | 12/23 (52.17) | p = 0.702 * | |
| Diabetic mellitus | 0/25 (0) | 3/25 (12.00) | 3/27 (11.11) | 3/23 (13.04) | p = 0.287 ** | |
| Hyperlipidemia | 9/25 (36.00) | 7/25 (28.00) | 12/27 (44.44) | 8/23 (34.78) | p = 0.672 * | |
| Osteoarthritis | 5/25 (20.00) | 4/25 (16.00) | 4/27 (14.81) | 7/23 (30.43) | p = 0.541 ** | |
| Smoking | 1/25 (4.00) | 0/25 (0) | 1/27 (3.70) | 2/23 (3.70) | p = 0.456 ** | |
| Alcohol drinking | 1/25 (4.00) | 0/25 (0) | 0/27 (0) | 2/23 (8.70) | p = 0.136 ** | |
| Exercise | 21/25 (84.00) | 19/25 (76.00) | 20/27 (74.07) | 16/23 (69.57) | p = 0.693 * | |
| Drug allergy | 4/25 (16.00) | 0/25 (0) | 5/27 (18.52) | 1/23 (4.35) | p = 0.063 ** | |
| Parameters | Time | Group A (n = 25) | Group B (n = 25) | Group D (n = 27) | Group C (n = 23) |
|---|---|---|---|---|---|
| FBS (mg/dL) | D0 (D0:D15) | 82.5 ± 13.2 (7.3 ± 3.4) | 79.0 ± 14.6 d,e (6.5 ± 2.5) | 81.0 ± 14.5 d (7.3 ± 3.1 *) | 84.4 ± 16.1 (1.8 ± 3.2) |
| D15 (D15:D30) | 88.8 ± 15.6 (4.5 ± 5.0 *) | 85.5 ± 17.7 d (−1.4 ± 1.8 *) | 87.9 ± 14.0 d (−3.8 ± 2.9 *) | 86.2 ± 16.4 (6.3 ± 3.3 *) | |
| D30 (D0:D30) | 93.2 ± 26.1 * (11.8 ± 6.1 *) | 84.1 ± 15.6 e (5.1 ± 2.1) | 85.3 ± 15.2 (3.5 ± 2.9) | 92.5 ± 21.9 (8.1 ± 4.6 *) | |
| TC (mg/dL) | D0 (D0:D15) | 210 ± 39 (−11 ± 4 *) | 209 ± 37 d (−8 ± 5) | 207 ± 36 (−1 ± 5) | 193 ± 30 (−4 ± 4) |
| D15 (D15:D30) | 203 ± 38 (7 ± 5) | 202 ± 32 (−4 ± 4) | 206 ± 39 (1 ± 3) | 188 ± 32 (4 ± 4) | |
| D30 (D0:D30) | 209 ± 37 (5 ± 12 *) | 198 ± 29 d (0 ± 8) | 207 ± 39 (11 ± 7) | 192 ± 35 (9 ± 13 *) | |
| TG (mg/dL) | D0 (D0:D15) | 120 ± 59 (−22 ± 13 *) | 117 ± 54 * (−6 ± 11) | 105 ± 36 (10 ± 10) | 110 ± 54 (5 ± 8) |
| D15 (D15:D30) | 98 ± 36 a (27 ± 9) | 111 ± 62 * (6 ± 12 *) | 113 ± 50 * (1 ± 7) | 115 ± 52 (4 ± 9) | |
| D30 (D0:D30) | 125 ± 48 *a (5 ± 12 *) | 117 ± 71 * (0 ± 8) | 114 ± 37 (11 ± 7) | 119 ± 61 * (9 ± 12 *) | |
| HDL-C (mg/dL) | D0 (D0:D15) | 53 ± 11 (−5 ± 2 *) | 54 ± 17 *a (−3 ± 1) | 55 ± 12 d (−3 ± 1 *) | 51 ± 14 d (−5 ± 1) |
| D15 (D15:D30) | 49 ± 13 *a (7 ± 2 *) | 51 ± 15 *a,b (4 ± 2) | 53 ± 12 d (3 ± 2 *) | 46 ± 13 d,e (4 ± 1) | |
| D30 (D0:D30) | 55 ± 12 a (2 ± 2) | 56 ± 17 *b (1 ± 1 *) | 56 ± 15 (0 ± 2) | 49 ± 14 e (−1 ± 1) | |
| LDL-C (mg/dL) | D0 (D0:D15) | 169 ± 45 (−20 ± 7 *) | 159 ± 45 *a,b (−12 ± 5) | 155 ± 41 (−7 ± 5) | 146 ± 36 d (−5 ± 1) |
| D15 (D15:D30) | 153 ± 48 (5 ± 6 *) | 147 ± 37 a (−4 ± 4 *) | 148 ± 48 *a (7 ± 4) | 134 ± 35 d,e (10 ± 4) | |
| D30 (D0:D30) | 157 ± 45 (−16 ± 8) | 143 ± 33 b (−16 ± 6) | 155 ± 46 *a (−1 ± 4) | 144 ± 42 e (−1 ± 6) |
| Parameters | Time | Group A (n = 25) | Group B (n = 25) | Group D (n = 27) | Group C (n = 23) |
|---|---|---|---|---|---|
| BUN (mg/dL) | D0 (D0:D15) | 13.2 ± 2.4 d (−1.7 ± 0.4) | 13.0 ± 3.5 (−0.9 ± 0.4) | 14.0 ± 3.8 (−1.1 ± 0.6) | 15.8 ± 6.9 * (−0.7 ± 0.8) |
| D15 (D15:D30) | 11.6 ± 2.1 d (0.5 ± 0.4) | 12.1 ± 2.9 * (0.8 ± 0.6) | 12.8 ± 2.8 (0.4 ± 0.6) | 15.1 ± 6.6 * (0.2 ± 0.6 *) | |
| D30 (D0:D30) | 12.2 ± 2.2 (−1.2 ± 0.6 *) | 12.9 ± 2.8 (−0.1 ± 0.7) | 13.0 ± 2.9 * (−0.7 ± 0.7) | 15.3 ± 5.2 * (−0.4 ± 1.0 *) | |
| CRE (mg/dL) | D0 (D0:D15) | 0.90 ± 0.14 (0.01 ± 0.03) | 0.87 ± 0.20 * (0.03 ± 0.03) | 0.87 ± 0.19 * (0 ± 0.04) | 1.21 ± 0.61 * (0.01 ± 0.04) |
| D15 (D15:D30) | 0.91 ± 0.16 (0 ± 0.04) | 0.90 ± 0.19 (0.05 ± 0.03) | 0.87 ± 0.17 * (0.03 ± 0.04) | 1.22 ± 0.62 * (0.03 ± 0.04) | |
| D30 (D0:D30) | 0.94 ± 0.29 (0.01 ± 0.06 *) | 0.95 ± 0.21 (0.08 ± 0.04 *) | 0.90 ± 0.16 (0.03 ± 0.05) | 1.25 ± 0.70 * (0.04 ± 0.05) | |
| UA (mg/dL) | D0 (D0:D15) | 6.75 ± 2.07 * (0.07 ± 0.41 *) | 7.35 ± 2.10 (−0.23 ± 0.21) | 6.24 ± 1.86 * (0.10 ± 0.46 *) | 7.63 ± 2.56 (0.43 ± 0.55 *) |
| D15 (D15:D30) | 6.85 ± 1.90 (0.17 ± 0.41) | 7.12 ± 1.71 * (0.31 ± 0.21) | 6.31 ± 1.36 (0.16 ± 0.27) | 8.06 ± 2.57 (−0.16 ± 0.37 *) | |
| D30 (D0:D30) | 7.03 ± 2.03 (0.25 ± 0.50 *) | 7.43 ± 1.69 (0.08 ± 0.25) | 6.43 ± 1.26 (0.26 ± 0.42 *) | 7.90 ± 1.75 (0.27 ± 0.45 *) | |
| Na+ (mmol/L) | D0 (D0:D15) | 142 ± 3 d,e (−1 ± 1) | 144 ± 3 *a,b (−3 ± 1) | 143 ± 2 (−2 ± 1 a) | 140 ± 3 (−1 ± 1 a) |
| D15 (D15:D30) | 140 ± 2 d (−0 ± 1) | 141 ± 3 *a,c (−1 ± 1) | 141 ± 2 (−2 ± 1) | 139 ± 2 (−0 ± 1) | |
| D30 (D0:D30) | 140 ± 3 e (−2 ± 1) | 139 ± 3 b,c (−4 ± 1) | 140 ± 2 (−3 ± 1 a) | 139 ± 3 (−1 ± 1 a) | |
| K+ (mmol/L) | D0 (D0:D15) | 3.80 ± 0.44 (0 ± 0.08) | 4.03 ± 0.35 d,e (−0.12 ± 0.05) | 4.09 ± 0.80 * (−0.24 ± 0.18 *) | 4.27 ± 0.51 a (−0.17 ± 0.19 *) |
| D15 (D15:D30) | 3.77 ± 0.51 (−0.05 ± 0.80) | 3.91 ± 0.36 e (−0.1 ± 0.05) | 3.92 ± 0.42 * (0.01 ± 0.11) | 4.03 ± 0.75 *a,b (0.05 ± 0.14 *) | |
| D30 (D0:D30) | 3.74 ± 0.44 (−0.04 ± 0.08) | 3.81 ± 0.31 d (−0.22 ± 0.06) | 3.95 ± 0.57 * (−0.15 ± 0.20 *) | 4.08 ± 0.46 b (−0.19 ± 0.10) |
| Parameters | Time | Group A (n = 25) | Group B (n = 25) | Group D (n = 27) | Group C (n = 23) |
|---|---|---|---|---|---|
| TP (g/dL) | D0 (D0:D15) | 8.00 ± 0.46 (−0.24 ± 0.09) | 8.14 ± 0.72 d,e (−0.11 ± 0.15) | 7.97 ± 0.40 (−0.00 ± 0.12) | 7.94 ± 0.35 d (−0.24 ± 0.09) |
| D15 (D15:D30) | 7.96 ± 0.42 * (−0.09 ± 0.07) | 7.90 ± 0.56 e (1.99 ± 0.09) | 7.90 ± 0.54 (−0.34 ± 0.12) | 7.94 ± 0.48 e (−0.09 ± 0.07) | |
| D30 (D0:D30) | 7.82 ± 0.46 (−0.33 ± 0.10) | 7.81 ± 0.52 d (−0.11 ± 0.14 *) | 7.83 ± 0.53 * (−0.34 ± 0.09) | 7.60 ± 0.47 d,e (−0.33 ± 0.10) | |
| Alb (g/dL) | D0 (D0:D15) | 4.50 ± 0.36 (−0.15 ± 0.08) | 4.55 ± 0.32 * (−0.09 ± 0.10) | 4.44 ± 0.43 d (0.00 ± 0.12 *) | 4.20 ± 0.64 d (−0.15 ± 0.08) |
| D15 (D15:D30) | 4.46 ± 0.51 (0.21 ± 0.05) | 4.40 ± 0.43 *a (0.37 ± 0.10) | 4.36 ± 0.52 e (0.51 ± 0.14) | 4.20 ± 0.60 e (0.21 ± 0.05) | |
| D30 (D0:D30) | 4.66 ± 0.37 (0.06 ± 0.08) | 4.62 ± 0.42 *a (0.27 ± 0.09) | 4.68 ± 0.38 d,e (0.51 ± 0.17 *) | 4.71 ± 0.48 d,e (0.06 ± 0.08) | |
| Glo(g/dL) | D0 (D0:D15) | 3.56 ± 0.72 e (−0.05 ± 0.10) | 3.57 ± 0.77 e (0.00 ± 0.16 *) | 3.53 ± 0.59 *a (−0.03 ± 0.14) | 3.74 ± 0.75 d (−0.05 ± 0.10) |
| D15 (D15:D30) | 3.48 ± 0.63 d (−0.32 ± 0.09 h) | 3.52 ± 0.80 d (−0.39 ± 0.13 i) | 3.57 ± 0.64 b (−0.83 ± 0.17 g,h,i) | 3.72 ± 0.84 e (−0.32 ± 0.09 h) | |
| D30 (D0:D30) | 3.16 ± 0.56 d,e (−0.38 ± 0.09) | 3.20 ± 0.71 d,e (−0.39 ± 0.15) | 3.15 ± 0.63 *a,b (−0.86 ± 0.16) | 2.89 ± 0.61 d,e (−0.38 ± 0.09) | |
| AST (U/L) | D0 (D0:D15) | 19 ± 6 (−1 ± 1) | 19 ± 4 (−1 ± 2 *) | 20 ± 10 * (−1 ± 1) | 18 ± 4 (−1 ± 1) |
| D15 (D15:D30) | 18 ± 4 (0 ± 1) | 18 ± 3 (−1 ± 1) | 20 ± 8 (−0 ± 1) | 18 ± 4 (0 ± 1) | |
| D30 (D0:D30) | 18 ± 5 (−1 ± 1) | 18 ± 4 (−2 ± 2 *) | 19 ± 7 * (−1 ± 1) | 17 ± 4 (−1 ± 1) | |
| ALT (U/L) | D0 (D0:D15) | 19 ± 9 *a,b (−4 ± 1) | 20 ± 5 d,e (−4 ± 1) | 21 ± 12 *a,b (−4 ± 1 *) | 19 ± 8 d,e (−4 ± 1) |
| D15 (D15:D30) | 15 ± 5 a (−0 ± 1) | 15 ± 3 e (−0 ± 1) | 17 ± 9 *a (−1 ± 1) | 15 ± 6 d (−0 ± 1) | |
| D30 (D0:D30) | 15 ± 4 b (−5 ± 1) | 15 ± 5 d (−4 ± 1) | 17 ± 10 *b (−5 ± 1 *) | 14 ± 5 e (−5 ± 1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lerttrakarnnon, P.; Kusirisin, W.; Koonyosying, P.; Flemming, B.; Utama-ang, N.; Fucharoen, S.; Srichairatanakool, S. Consumption of Sinlek Rice Drink Improved Red Cell Indices in Anemic Elderly Subjects. Molecules 2021, 26, 6285. https://doi.org/10.3390/molecules26206285
Lerttrakarnnon P, Kusirisin W, Koonyosying P, Flemming B, Utama-ang N, Fucharoen S, Srichairatanakool S. Consumption of Sinlek Rice Drink Improved Red Cell Indices in Anemic Elderly Subjects. Molecules. 2021; 26(20):6285. https://doi.org/10.3390/molecules26206285
Chicago/Turabian StyleLerttrakarnnon, Peerasak, Winthana Kusirisin, Pimpisid Koonyosying, Ben Flemming, Niramon Utama-ang, Suthat Fucharoen, and Somdet Srichairatanakool. 2021. "Consumption of Sinlek Rice Drink Improved Red Cell Indices in Anemic Elderly Subjects" Molecules 26, no. 20: 6285. https://doi.org/10.3390/molecules26206285
APA StyleLerttrakarnnon, P., Kusirisin, W., Koonyosying, P., Flemming, B., Utama-ang, N., Fucharoen, S., & Srichairatanakool, S. (2021). Consumption of Sinlek Rice Drink Improved Red Cell Indices in Anemic Elderly Subjects. Molecules, 26(20), 6285. https://doi.org/10.3390/molecules26206285