
VEGF Expression, Cellular Infiltration, and Intratumoral Collagen Levels after Electroporation-Based Treatment of Dogs with Cutaneous Squamous Cell Carcinoma

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
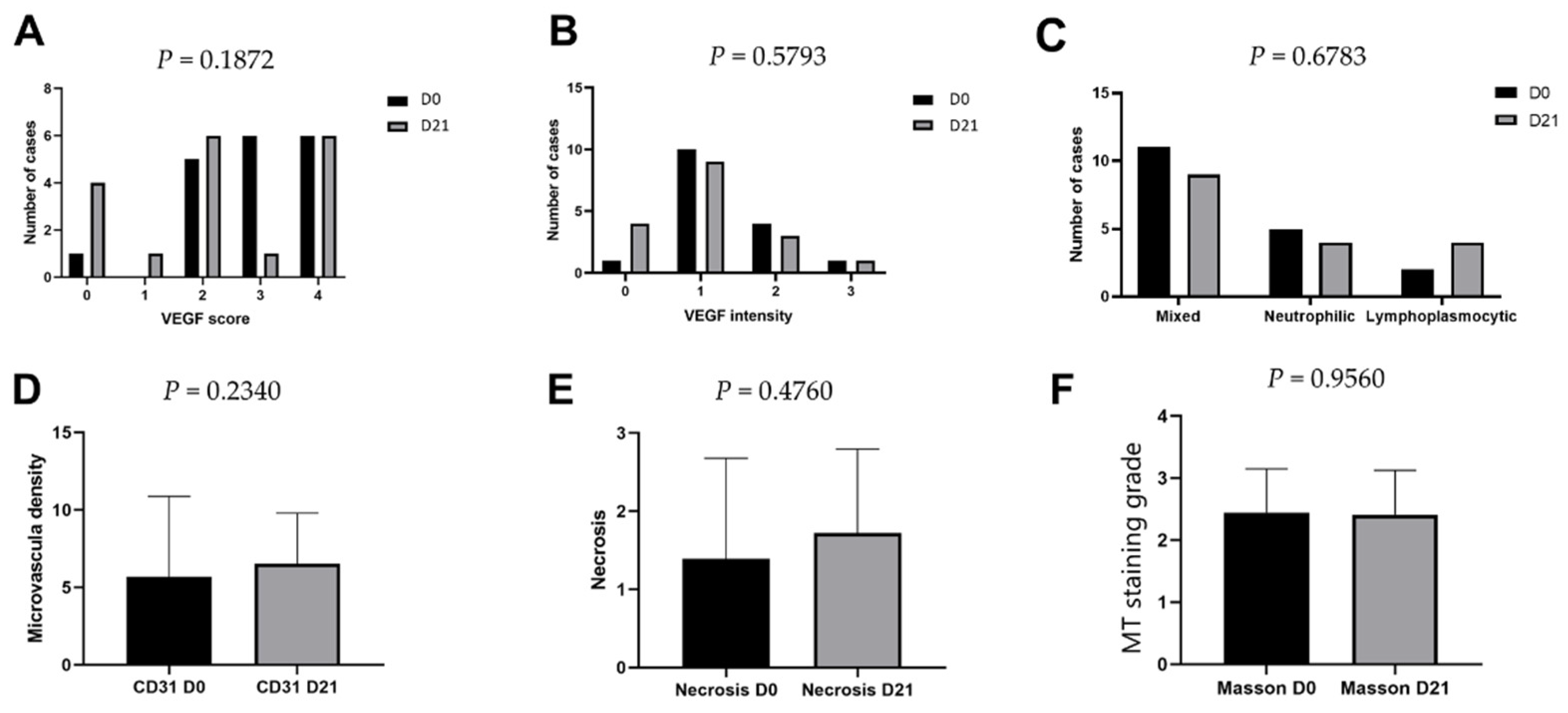
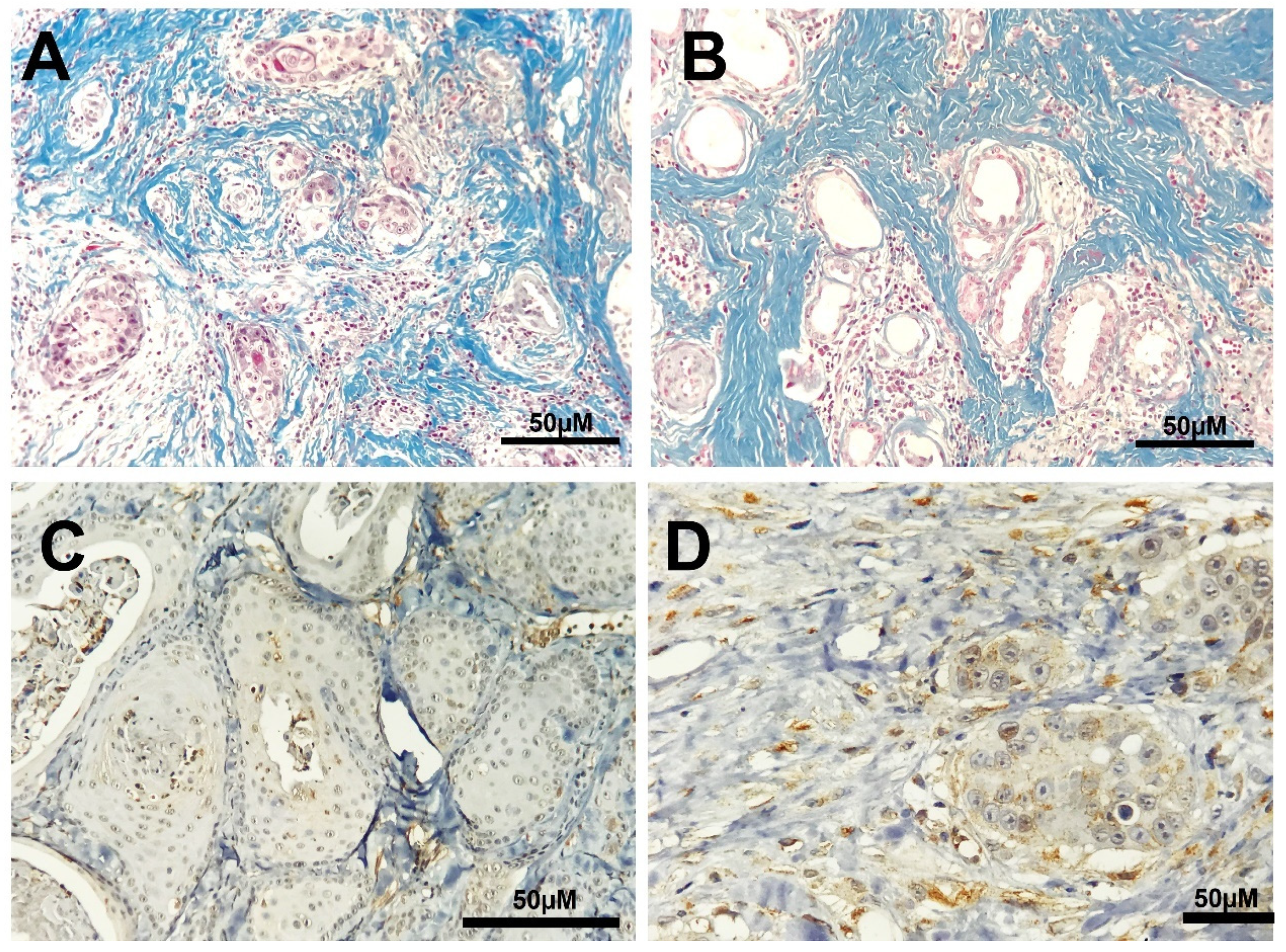
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goldschmidt, M.H.; Shofer, F.S. Squamous cell carcinoma. In Skin Tumors of the Dog and Cat, 2nd ed.; Goldschmidt, M.H., Shofer, F.S., Eds.; Reed Educational and Professional Publishing: Oxford, UK, 1998; pp. 37–49. [Google Scholar]
- Hauck, M.L.; Oblak, M. Tumors of the skin and subcutaneous tissues. In Withrow & MacEwen’s Small Animal Clinical Oncology, 6th ed.; Vail, D.M., Thamm, D.H., Liptak, J.M., Eds.; Elsevier: St. Louis, MO, USA, 2020; pp. 352–362. [Google Scholar]
- Goldschmidt, M.H. Basal and squamous-cell neoplasms of dogs and cats. Am. J. Dermatopathol. 1984, 6, 199–206. [Google Scholar] [CrossRef]
- Gross, T.; Ihrke, P.J.; Walder, E.J.; Affolter, V.K. Epidermal tumors. In Skin Diseases of the Dog and Cat. Clinical and Histopathologic Diagnosis; Blackwell Science Ltd.: Oxford, UK, 2005; pp. 581–585. [Google Scholar]
- Goldschmidt, M.H.; Goldschmidt, K.H. Epithelial and melanocytic tumors of the skin. In Tumors in Domestic Animals, 5th ed.; Meuten, D.J., Ed.; Iowa State Press: Ames, IA, USA, 2016; pp. 88–141. [Google Scholar]
- Buckman, S.Y.; Gresham, A.; Hale, P.; Hruza, G.; Anast, J.; Masferrer, J.; Pentland, A.P. COX-2 expression is induced by UVB exposure in human skin: Implications for the development of skin cancer. Carcinogenesis 1998, 19, 723–729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salashe, S. Epidemiology of actinic keratoses and squamous cell carcinoma. J. Am. Acad. Dermatol. 2000, 42, S4–S7. [Google Scholar] [CrossRef]
- Graf, R.; Gruntzig, K.; Boo, G.; Hassig, M.; Axhausen, K.W.; Fabrikant, S.; Welle, M.; Meier, D.; Guscetti, F.; Folkers, G.; et al. Swiss Feline Cancer Registry 1965–2008: The influence of sex, breed, and age on tumours types and tumours locations. J. Comp. Path. 2016, 154, 195–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muzic, J.G.; Schmitt, A.R.; Wright, A.C.; Alniemi, D.T.; Zubair, A.S.; Lourido, J.M.O.; Seda, I.M.S.S.; Weaver, A.L.; Baum, C.L. Incidence and trends of basal cell carcinoma and cutaneous squamous cell carcinoma, a population-based study in Osmsted County, Minnesota, 2000 to 2010. Mayo Clin. Proc. 2017, 92, 890–898. [Google Scholar] [CrossRef] [PubMed]
- Mittelbronn, M.A.; Mullins, D.L.; Ramos-Caro, F.A.; Flowers, F.P. Frequency of pre-existing actinic keratosis in cutaneous squamous cell carcinoma. Int. J. Dermatol. 1998, 37, 677–681. [Google Scholar] [CrossRef]
- Poggiani, S.S.C.; Hatayde, M.R.; Laufer-Amorim, R.; Werner, J. Expression of Cyclooxygenase-2 and Ki-67 in Actinic Keratosis and Cutaneous Squamous Cell Carcinoma in Dogs. Open J. Vet. Med. 2012, 2, 41–47. [Google Scholar] [CrossRef] [Green Version]
- Willcox, J.L.; Marks, S.L.; Ueda, Y.; Skorupski, K.A. Clinical features and outcome of dermal squamous cell carcinoma in 193 dogs (1987–2017). Vet. Comp. Oncol. 2019, 17, 130–138. [Google Scholar] [CrossRef]
- Dos Anjos, D.S.; Bueno, C.; Magalhaes, L.F.; Magalhaes, G.M.; Mattos-Junior, E.; Pinto, M.M.R.; De Nardi, A.B.; Brunner, C.H.M.; Leis-Filho, A.F.; Calazans, S.G.; et al. Electrochemotherapy induces tumor regression and decreases the proliferative index in canine cutaneous squamous cell carcinoma. Sci. Rep. 2019, 9, 15819. [Google Scholar] [CrossRef] [PubMed]
- Brougham, N.D.; Dennett, E.R.; Cameron, R.; Tan, S.T. The incidence of metastasis from cutaneous squamous cell carcinoma and the impact of its risk factors. J. Surg. Oncol. 2012, 106, 811–815. [Google Scholar] [CrossRef] [PubMed]
- Karia, P.S.; Jambusaria-Pahlajani, A.; Harrington, D.P.; Murphy, G.F.; Qureshi, A.A.; Schmults, C.D. Evaluation of American Joint Committee on Cancer, International Union Against Cancer, and Brigham and Women’s Hospital tumor staging for cutaneous squamous cell carcinoma. J. Clin. Oncol. 2014, 32, 327–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lana, S.E.; Ogilvie, G.K.; Withrow, S.J.; Straw, R.C.; Rogers, K.S. Feline cutaneous squamous cell carcinoma of the nasal planum and the pinnae: 61 cases. J. Am. Anim. Hosp. Assoc. 1997, 33, 329–332. [Google Scholar] [CrossRef]
- Dos Anjos, D.S.; Sierra, O.R.; Spugnini, E.P.; De Nardi, A.B.; Fonseca-Alves, C.E. Comparison of two different doses of bleomycin in electrochemotherapy protocols for feline cutaneous squamous cell carcinoma nonsegregated from ultraviolet light exposure. Sci. Rep. 2020, 10, 18362. [Google Scholar] [CrossRef]
- Lascelles, B.D.X.; Henderson, R.A.; Seguin, B.; Liptak, J.M.; Withrow, S.J. Bilateral rostral maxillectomy and nasal planectomy for large rostral maxillofacial neoplasms in six dogs and one cat. J. Am. Anim. Hosp. Assoc. 2004, 40, 137–146. [Google Scholar] [CrossRef] [PubMed]
- Que, S.K.T.; Zwald, F.O.; Schmults, C.D. Cutaneous squamous cell carcinoma: Management of advanced and high-stage tumors. J. Am. Acad. Dermatol. 2018, 78, 249–261. [Google Scholar] [CrossRef]
- Tay, S.S.; Roediger, B.; Tong, P.L.; Tikoo, S.; Weninger, W. The Skin-Resident Immune Network. Curr. Dermatol. Rep. 2014, 3, 13–22. [Google Scholar] [CrossRef] [Green Version]
- Iqbal, J.; Abbasi, B.A.; Ahmad, R.; Batool, R.; Mahmood, T.; Ali, B.; Khalil, A.T.; Kanwal, S.; Shah, S.A.; Alam, M.M.; et al. Potential phytochemicals in the fight against skin cancer: Current landscape and future perspectives. Biomed. Pharmacol. J. 2019, 109, 1381–1393. [Google Scholar] [CrossRef]
- Steward, W.P.; Brown, K. Cancer chemoprevention: A rapidly evolving field. Br. J. Cancer 2013, 109, 1. [Google Scholar] [CrossRef] [PubMed]
- Holcmann, M.; Sibiia, M. Mechanisms underlying skin disorders induced by EGFR inhibitors. Mol. Cell Oncol. 2015, 2, e1004969. [Google Scholar] [CrossRef] [Green Version]
- Paulson, K.G.; Lahman, M.C.; Chapuis, A.G.; Brownell, I. Immunotherapy for skin cancer. Int. Immunol. 2019, 31, 465–475. [Google Scholar] [CrossRef] [Green Version]
- Santana, C.H.; Moreira, P.R.R.; Rosolem, M.C.; Vasconcelos, R.O. Relationship between the inflammatory infiltrate and the degree o fdifferentiation of the canine cutaneous squamous cell carcinoma. Vet. Anim. Sci. 2016, 1, 4–8. [Google Scholar] [CrossRef] [Green Version]
- Estrela-Lima, A.; Araujo, M.S.S.; Costa-Neto, J.M.; Teixeira-Carvalho, A.; Barrouin-Melo, S.M.; Cardoso, S.V.; Martins-Filho, O.A.; Serakides, R.; Cassali, G.D. Immunophenotypic features of tumor infiltrating lymphocytes from mammary carcinomas in female dogs associated with prognostic factors and survival rates. BMC Cancer 2010, 10, 256. [Google Scholar] [CrossRef] [Green Version]
- Hanahan, W.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [Green Version]
- Giuliano, A.; dos Santos Horta, R.; Constantino-Casas, F.; Hoather, T.; Dobson, J. Expression of fibroblast activating protein and correlation with histological grade, mitotic index and Ki67 expression in canine mast cell tumours. J. Comp. Pathol. 2017, 156, 14–20. [Google Scholar] [CrossRef]
- Xu, S.; Xu, H.; Wang, W.; Li, S.; Li, H.; Li, T.; Zhang, W.; Yu, X.; Liu, L. The role of collagen in cancer: From bench to bedside. J. Transl. Med. 2019, 17, 309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonnans, C.; Chou, J.; Werb, Z. Remodelling the extracellular matrix in development and disease. Nat. Rev. Mol. Cell Biol. 2014, 15, 786–801. [Google Scholar] [CrossRef]
- Lu, P.; Weaver, V.M.; Werb, Z. The extracellular matrix: A dynamic niche in cancer progression. J. Cell Biol. 2012, 196, 395–406. [Google Scholar] [CrossRef]
- Daniel, J.; Barra, C.N.; Pulz, L.H.; Kleeb, S.R.; Xavier, J.G.; Catao-Dias, J.L.; Nishiya, A.T.; Fukumasu, H.; Strefezzi, R.F. Intratumoral collagen index predicts mortality and survival in canine cutaneous mast cell tumours. Vet. Dermatol. 2019, 30, 162. [Google Scholar] [CrossRef]
- Whalen, G.F.; Ingber, D.E. Inhibition of tumor-cell attachment to extracellular matrix as a method for preventing tumor recurrence in a surgical wound. Ann. Surg. 1989, 210, 758–764. [Google Scholar] [CrossRef] [PubMed]
- Garcia, A.P.V.; Reis, L.A.; Nunes, F.C.; Longford, F.G.J.; Frey, J.G.; De Paula, A.M.; Cassali, G.D. Canine mammary cancer tumour behaviour and patient survival time are associated with collagen fibre characteristics. Sci. Rep. 2021, 11, 5668. [Google Scholar] [CrossRef] [PubMed]
- Rosen, S.; Brisson, B.K.; Durham, A.C.; Munroe, C.M.; McNeill, C.J.; Stefanovski, D.; Sorenmo, K.U.; Volk, S.W. Intratumoral collagen signatures predict clinical outcomes in feline mammary carcinoma. PLoS ONE 2020, 15, e0236516. [Google Scholar] [CrossRef]
- Miklavcic, D.; Davalos, R.V. Electrochemotherapy (ECT) and irreversible electroporation (IRE) -advanced techniques for treating deep-seated tumors based on electroporation. Biomed. Eng. Online. 2015, 14 (Suppl. 3), I12015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heller, R.; Jaroszeski, M.J.; Reintgen, D.S.; Puleo, C.A.; DeConti, R.C.; Gilbert, R.A.; Glass, L.F. Treatment of cutaneous and subcutaneous tumors with electrochemotherapy using intralesional bleomycin. Cancer 1998, 83, 148–157. [Google Scholar] [CrossRef]
- De Virgilio, A.; Ralli, M.; Longo, L.; Mancini, P.; Attanasio, G.; Atturo, F.; De Vincentiis, M.; Greco, A. Electrochemotherapy in head and neck cancer: A review of an emerging cancer treatment (Review). Oncol. Lett. 2018, 16, 3415–3423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spugnini, E.P.; Baldi, A. Electrochemotherapy in veterinary oncology state-of-the-art and perspectives. Vet. Clin. Small Anim. 2019, 49, 967–979. [Google Scholar] [CrossRef]
- Spugnini, E.P.; Baldi, F.; Mellone, P.; Feroce, F.; D’Avino, A.; Bonetto, F.; Vincenzi, B.; Citro, G.; Baldi, A. Patterns of tumor response in canine and feline cancer patients treated with electrochemotherapy: Preclinical data for the standardization of this treatment in pets and humans. J. Transl. Med. 2007, 7, 48. [Google Scholar] [CrossRef] [Green Version]
- Gasljevic, G.; Edhemovic, I.; Cemazar, M.; Brecelj, E.; Gadzijev, E.M.; Music, M.M.; Sersa, G. Histopathological findings in colorectal liver metastases after electrochemotherapy. PLoS ONE 2017, 12, e0180709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sersa, G.; Cemazar, M.; Parkins, C.S.; Chaplin, D.J. Tumour blood flow changes induced by application of electric pulses. Eur. J. Cancer 1999, 35, 672–677. [Google Scholar] [CrossRef]
- Cemazar, M.; Parkins, C.S.; Holder, A.L.; Chaplin, D.J.; Tozer, G.M.; Sersa, G. Electroporation of human microvascular endothelial cells: Evidence for an anti-vascular mechanism of electrochemotherapy. Br. J. Cancer 2001, 84, 565–570. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Lyu, C.; Liu, Y.; Lv, Y.; Chang, T.T.; Rubinsky, B. Molecular and histological study on the effects of non-thermal irreversible electroporation on the liver. Biochem. Biophys. Res. Commun. 2018, 500, 665–670. [Google Scholar] [CrossRef]
- National Research Council. Guide for the Care and Use of Laboratory Animals, 8th ed.; National Academies Press: Washington, DC, USA, 2011.
- Campana, L.G.; Clover, A.J.P.; Valpione, S.; Quaglino, P.; Gehl, J.; Kunte, C.; Snoj, M.; Cemazar, M.; Rossi, C.R.; Miklavcic, D.; et al. Recommendations for improving the quality of reporting clinical electrochemotherapy studies based on qualitative systematic review. Radiol. Oncol. 2016, 50, 1–13. [Google Scholar] [CrossRef]
- Owen, L.N. TNM Classification of Tumor in Domestic Animals; World Health Organization: Geneva, Switzerland, 1980. [Google Scholar]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Prophet, E.B.; Mills, B.; Arrington, J.; Sobin, L. Métodos Histotecnologicos; Instituto de Patología de las Fuerzas Armadas de los Estados Unidos de America (AFIP): Washington, DC, USA, 1995; p. 280. [Google Scholar]
- Prado, M.C.M.; Macedo, S.A.L.; Guiraldelli, G.G.; de Faria Lainetti, P.; Leis-Filho, A.F.; Kobayashi, P.E.; Laufer-Amorim, R.; Fonseca-Alves, C.E. Investigation of the Prognostic Significance of Vasculogenic Mimicry and Its Inhibition by Sorafenib in Canine Mammary Gland Tumors. Front. Oncol. 2019, 19, 1445. [Google Scholar] [CrossRef] [Green Version]
- Al-Dissi, A.N.; Haines, D.M.; Singh, B.; Kidney, B.A. Immunohistochemical expression of vascular endothelial growth factor and vascular endothelial growth factor receptor-2 in canine simple mammary gland adenocarcinomas. Can. Vet. J. 2010, 51, 1109–1114. [Google Scholar] [PubMed]
- Dos Anjos, D.S.; Vital, A.F.; Lainetti, P.F.; Leis-Filho, A.F.; Dalmolin, F.; Elias, F.; Calazans, S.G.; Fonseca-Alves, C.E. Deregulation of VEGFR-2 and PDGFR Expression and Microvascular Density in a Triple-Negative Model of Canine Malignant Mammary Tumors with Lymph Node or Lung Metastasis. Vet. Sci. 2019, 9, 3. [Google Scholar] [CrossRef] [Green Version]
- Hanahan, D.; Folkman, J. Patterns and emerging mechanisms of the angiogenic switch during tumorigenesis. Cell 1996, 86, 353–364. [Google Scholar] [CrossRef] [Green Version]
- Kukreja, I.; Kapoor, P.; Deshmukh, R.; Kulkarni, V. VEGF and CD 34. A correlation between tumor angiogenesis and microvessel density-an immunohistochemical study. J. Oral. Maxill. Pathol. 2013, 17, 367–373. [Google Scholar]
- Maiolino, P.; De Vico, G.; Restucci, B. Expression of vascular endothelial growth factor in basal cell tumours and in squamous cell carcinomas of canine skin. J. Comp. Pathol. 2000, 123, 141–145. [Google Scholar] [CrossRef]
- Al-Dissi, A.N.; Haines, D.M.; Singh, B.; Kidney, B.A. Immunohistochemical Expression of Vascular Endothelial Growth Factor and Vascular Endothelial Growth Factor Receptor Associated with Tumor Cell Proliferation in Canine Cutaneous Squamous Cell Carcinomas and Trichoepitheliomas. Vet. Pathol. 2007, 44, 823–830. [Google Scholar] [CrossRef]
- Jarm, T.; Cemazar, M.; Miklavcic, D.; Sersa, G. Antivascular effects of electrochemotherapy: Implications in treatment of bleeding metastases. Exp. Rev. Anticancer Ther. 2010, 10, 729–746. [Google Scholar] [CrossRef] [PubMed]
- Sersa, G.; Jarm, T.; Kotnik, T.; Coer, A.; Podkrajsek, M.; Sentjurc, M.; Miklavcic, D.; Kadivec, M.; Kranjc, S.; Secerov, A.; et al. Vascular disrupting action of electroporation and electrochemotherapy with bleomycin in murine sarcoma. Br. J. Cancer 2008, 98, 388–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blancher, C.; Moore, J.W.; Talks, K.L.; Houlbrook, S.; Harris, A.L. Relationship of hypoxia-inducible factor (HIF)-1a and HIF-2a expression to vascular endothelial growth factor induction and hypoxia survival in human breast cancer cell lines. Cancer Res. 2000, 60, 7106–7113. [Google Scholar] [PubMed]
- Gehl, J.; Geertsen, P.F. Efficient palliation of haemorrhaging malignant melanoma skin metastases by electrochemotherapy. Melanoma Res. 2000, 10, 585–589. [Google Scholar] [CrossRef]
- Markelc, B.; Sersa, G.; Cemazar, M. Differential mechanisms associated with vascular disrupting action of electrochemotherapy: Intravital microscopy on the level of single normal and tumor blood vessels. PLoS ONE 2013, 8, e59557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bigi, L.; Galdo, G.; Cesinaro, A.M.; Vaschieri, C.; Marconi, A.; Pincelli, C.; Fantini, F. Electrochemotherapy induces apoptotic death in melanoma metastases: A histologic and immunohistochemical investigation. Clin. Cosmet. Investig. Dermatol. 2016, 9, 451–459. [Google Scholar] [CrossRef] [Green Version]
- Rice, C.; Huang, L.E. From antiangiogenesis to hypoxia: Current research and future directions. Cancer Man Res. 2011, 3, 9–16. [Google Scholar]
- Santos, M.; Mercante, A.M.; Louro, I.D.; Gonçalves, A.J.; De Carvalho, M.B.; Da Silva, E.H.T.; Da Silva, A.M.A. HIF1-alpha expression predicts survival of patients with squamous cell carcinoma of the oral cavity. PLoS ONE 2012, 7, e45228. [Google Scholar] [CrossRef] [Green Version]
- Tozon, N.; Kodre, V.; Sersa, G.; Cemazar, M. Effective treatment of perianal tumors in dogs with electrochemotherapy. Anticancer Res. 2005, 25, 839–846. [Google Scholar]
- Entin, I.; Plotnikov, A.; Korenstein, R.; Keisari, Y. Tumor growth retardation, cure, and induction of antitumor immunity in B16 melanoma-bearing mice by low electric field-enhanced chemotherapy. Clin. Cancer Res. 2003, 9, 3190–3197. [Google Scholar]
- Longo, F.; Perri, F.; Caponigro, F.; Scarpati, G.D.V.; Guida, A.; Pavone, E.; Aversa, C.; Muto, P.; Giuliano, M.; Ionna, F.; et al. Boosting the Immune Response with the Combination of Electrochemotherapy and Immunotherapy: A New Weapon for Squamous Cell Carcinoma of the Head and Neck? Cancers 2020, 12, 2781. [Google Scholar] [CrossRef]
- Satyam, A.; Singh, P.; Badjatia, N.; Seth, A.; Sharma, A. A disproportion of TH1/TH2 cytokines with predominance of TH2 in urothelial carcinoma of bladder. Urol. Oncol. 2011, 29, 58–65. [Google Scholar]
- Nzula, S.; Going, J.J.; Stott, D.I. The role of B lymphocytes in breast cancer: A review and current status. Cancer Therap. 2003, 1, 353–362. [Google Scholar]
- Enokida, T.; Tahara, M. Electrochemotherapy in the Treatment of Head and Neck Cancer: Current Conditions and Future Directions. Cancers 2021, 13, 1418. [Google Scholar] [CrossRef]
- Di monta, G.; Caraco, C.; Simeone, E.; Grimaldi, A.M.; Marone, U.; Di Marzo, M.; Vanella, V.; Festino, L.; Palla, M.; Mori, S.; et al. Electrochemotherapy efficacy evaluation for treatment of locally advanced stage III cutaneous squamous cell carcinoma: A 22-cases retrospective analysis. J. Trans. Med. 2017, 15, 82. [Google Scholar] [CrossRef] [PubMed]
- Gerlini, G.; Sestini, S.; Di Gennaro, P.; Urso, C.; Pimpinelli, N.; Borgognoni, L. Dendritic cells recruitment in melanoma metastasis treated by electrochemotherapy. Clin. Exp. Metastasis 2013, 30, 37–45. [Google Scholar] [CrossRef]
- Chandrashekaraiah, G.B.; Rao, S.; Munivenkatappa, B.S.; Mathur, K.Y. Canine Squamous Cell Carcinoma: A review of 17 cases. Braz. J. Vet. Pathol. 2011, 4, 79–86. [Google Scholar]
- Wu, J.P.; Huang, W.B.; Zhou, H.; Xu, L.W.; Zhao, J.H.; Zhu, J.G.; Su, J.H.; Sun, H.B. Intensity of stromal changes is associated with tumor relapse in clinically advanced prostate cancer after castration therapy. Asian J. Androl. 2014, 16, 710–714. [Google Scholar]
- Golberg, A.; Khan, S.; Belov, V.; Quinn, K.P.; Albadawi, H.; Broelsch, F.; Watkins, M.T.; Georgakoudi, I.; Papisov, M.; Mihm Jr, M.C.; et al. Skin Rejuvenation with Non-Invasive Pulsed Electric Fields. Sci. Rep. 2015, 5, 10187. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Intensity | Day 0 | Day 21 |
|---|---|---|
| Mild | 2 | 2 |
| Moderate | 6 | 6 |
| Accentuated | 10 | 9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dos Anjos, D.; Bueno, C.; Mattos-Junior, E.; De Nardi, A.B.; Fonseca-Alves, C.E. VEGF Expression, Cellular Infiltration, and Intratumoral Collagen Levels after Electroporation-Based Treatment of Dogs with Cutaneous Squamous Cell Carcinoma. Life 2021, 11, 1321. https://doi.org/10.3390/life11121321
Dos Anjos D, Bueno C, Mattos-Junior E, De Nardi AB, Fonseca-Alves CE. VEGF Expression, Cellular Infiltration, and Intratumoral Collagen Levels after Electroporation-Based Treatment of Dogs with Cutaneous Squamous Cell Carcinoma. Life. 2021; 11(12):1321. https://doi.org/10.3390/life11121321
Chicago/Turabian StyleDos Anjos, Denner, Cynthia Bueno, Ewaldo Mattos-Junior, Andrigo Barboza De Nardi, and Carlos Eduardo Fonseca-Alves. 2021. "VEGF Expression, Cellular Infiltration, and Intratumoral Collagen Levels after Electroporation-Based Treatment of Dogs with Cutaneous Squamous Cell Carcinoma" Life 11, no. 12: 1321. https://doi.org/10.3390/life11121321
APA StyleDos Anjos, D., Bueno, C., Mattos-Junior, E., De Nardi, A. B., & Fonseca-Alves, C. E. (2021). VEGF Expression, Cellular Infiltration, and Intratumoral Collagen Levels after Electroporation-Based Treatment of Dogs with Cutaneous Squamous Cell Carcinoma. Life, 11(12), 1321. https://doi.org/10.3390/life11121321