
Motor-Imagery EEG-Based BCIs in Wheelchair Movement and Control: A Systematic Literature Review



Abstract
:1. Introduction
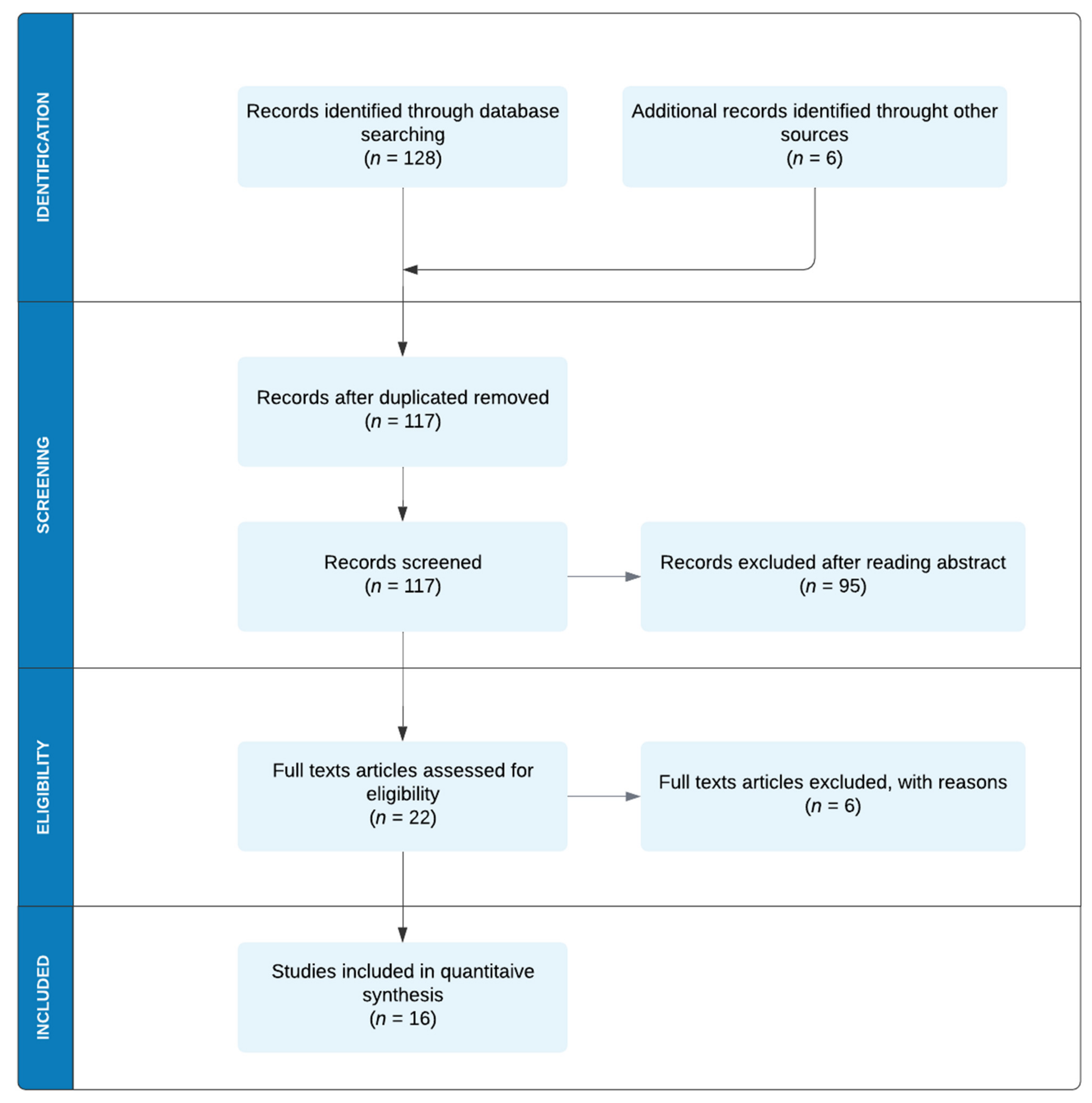
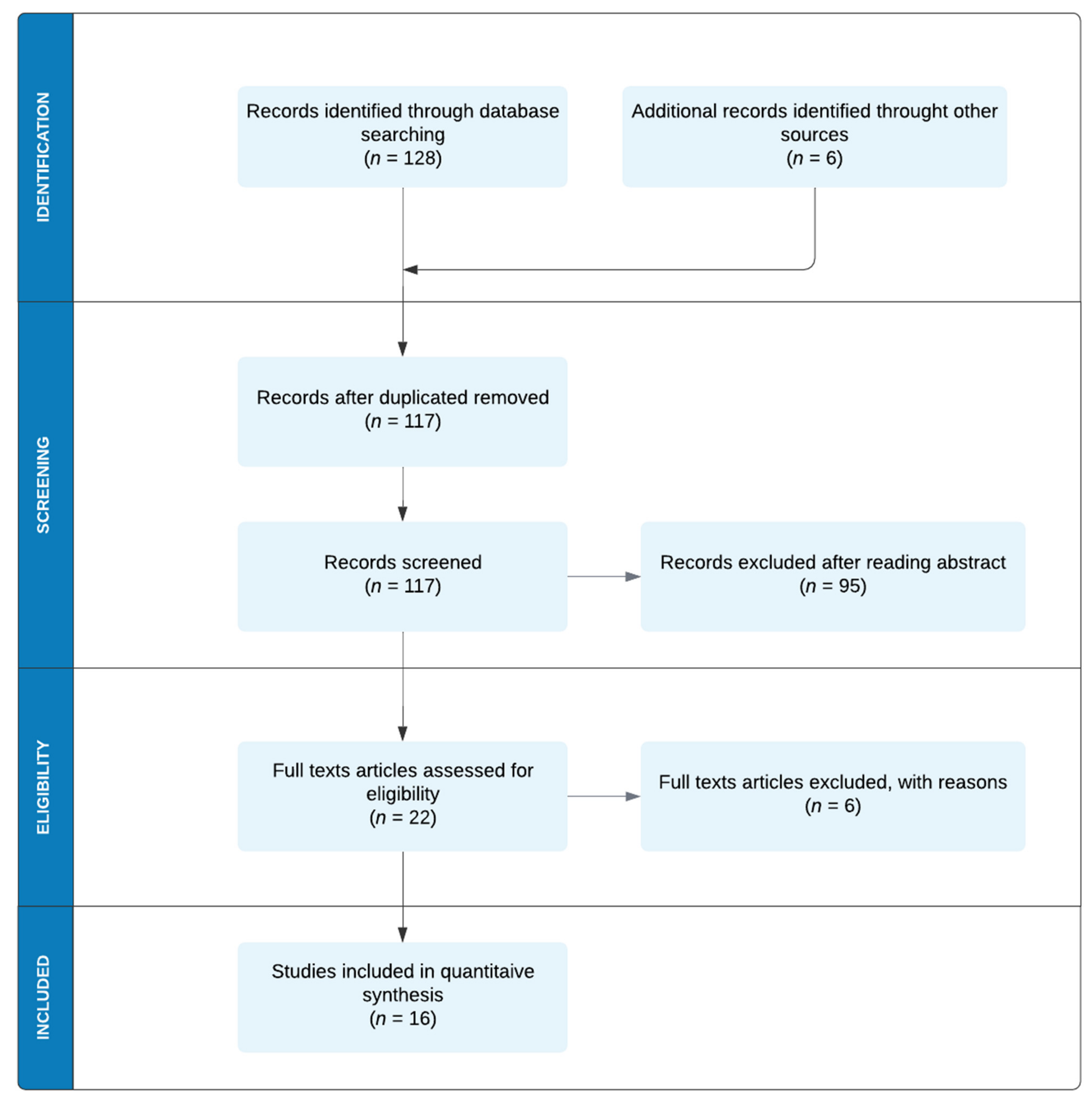
2. Methodology for This Review
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection
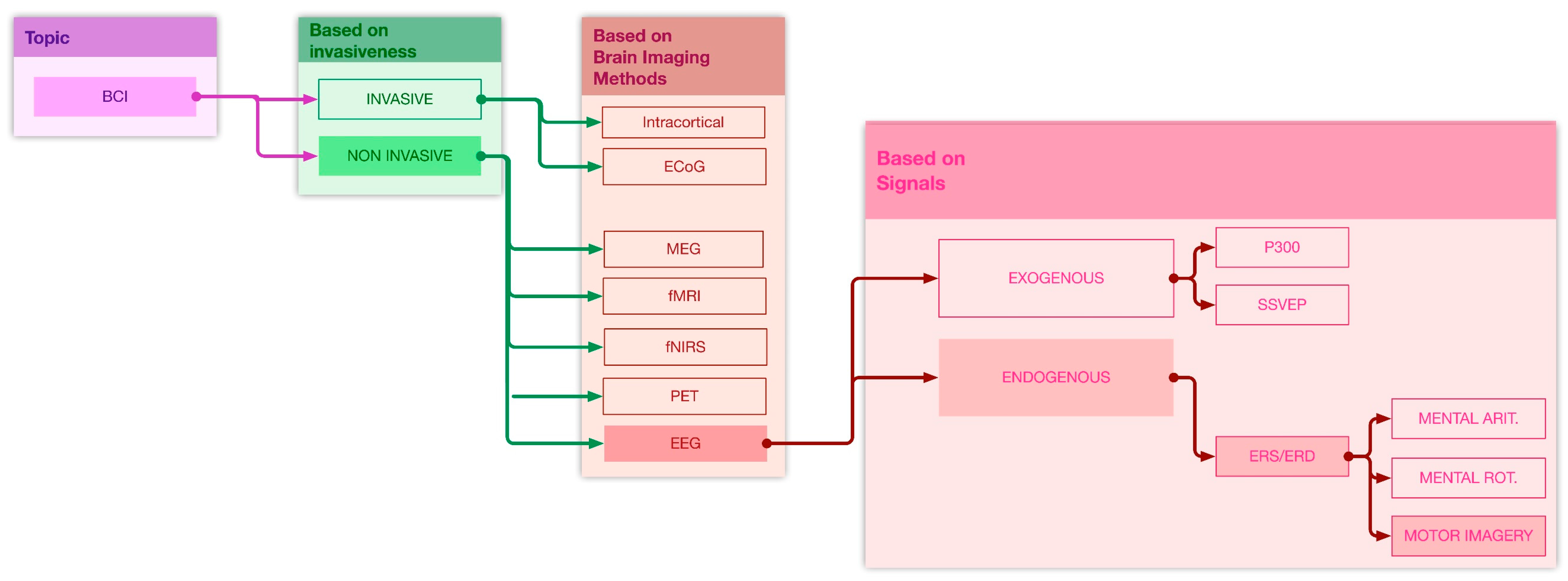
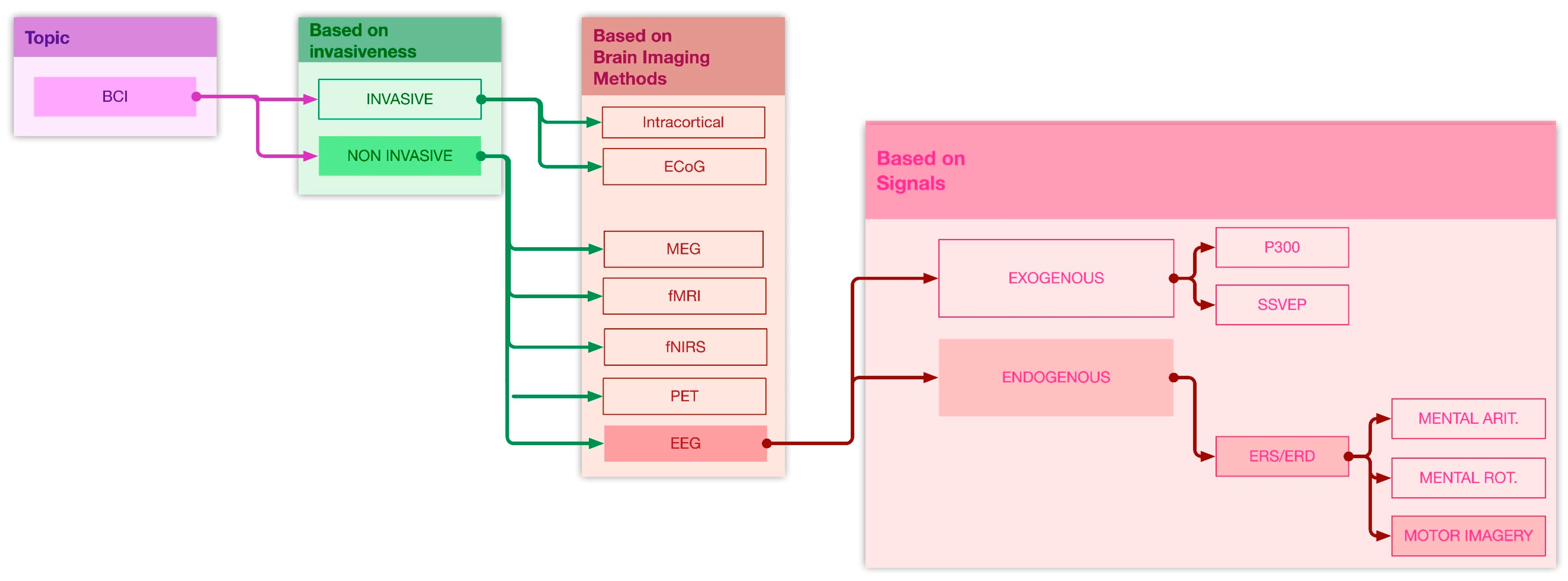
3. Brain–Computer Interfaces Classifications and Applications: A Synthetic Overview
4. MI EEG-Based BCIs in Wheelchair Movement and Control: Literature Results
Existing Applications of MI EEG BCW
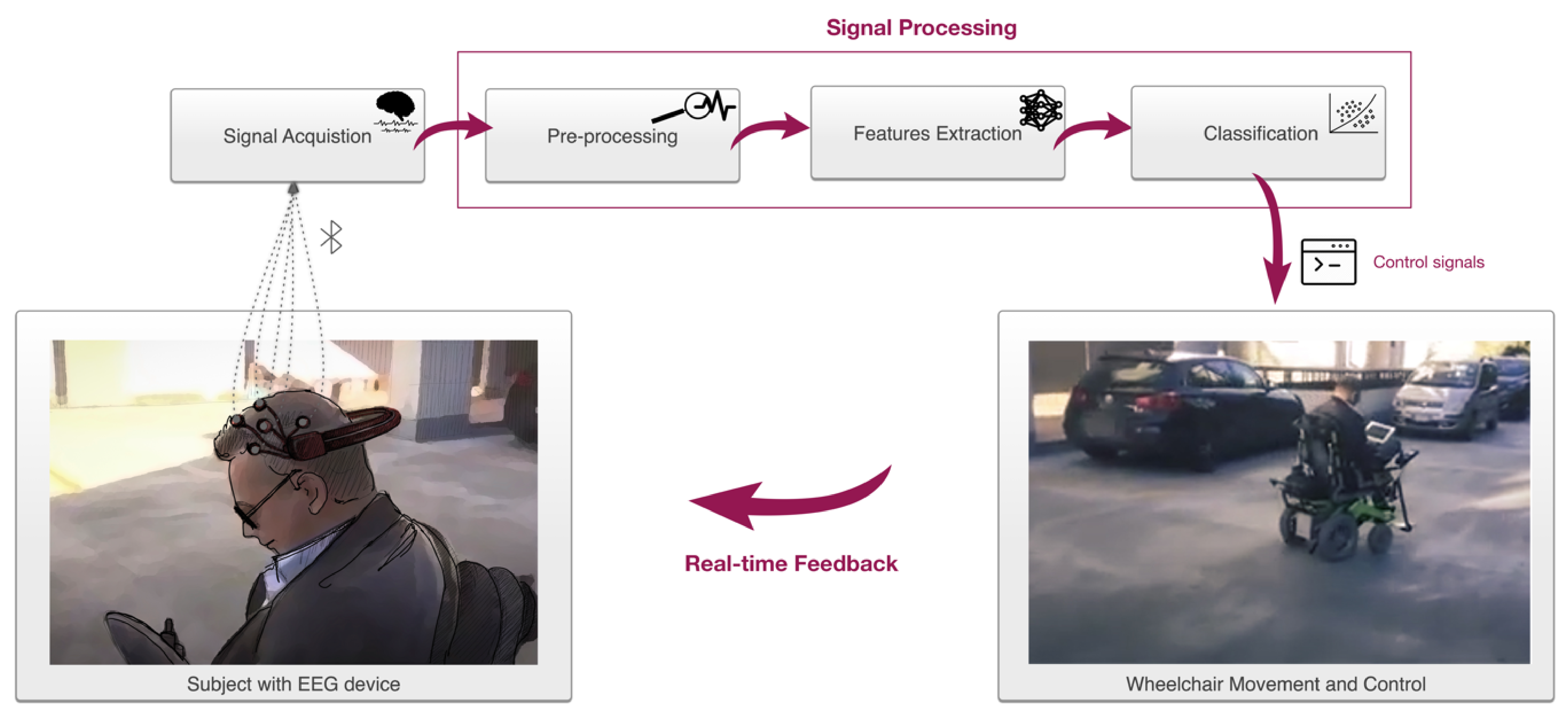
5. MI-Based BCW Elements
5.1. Signal Acquisition
5.2. Pre-Processing
5.3. Feature Extraction
5.4. Pattern Classification
5.5. Software Platforms
6. MI-BCWs Performance Evaluation
7. Conclusions
- -
- to define the sub-area of interest in BCI context, rather than proving a wide overview of brain–computer interface typologies and applications;
- -
- to present the state-of-the-art applications of EEG-based BCIs, particularly those using motor-imagery data, to wheelchair movement and control in a real environment;
- -
- to highlight the need for easy usability required for disabled people and to focus the attention on the applicability and feasibility of brain-controlled wheelchair in a real context;
- -
- to analyze MI EEG-based BCIs applied to wheelchair movement and control, not only in terms of algorithm analysis, features extraction, features selection, classification techniques, and software used, but also adding information about wheelchair type and components, obstacle avoidance systems, and wheelchair performances evaluation;
- -
- to make assumption and provide suggestions on potential improvements of these devices.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Smith, E.M.; Hernandez, M.L.T.; Ebuenyi, I.D.; Syurina, E.V.; Barbareschi, G.; Best, K.L.; Danemayer, J.; Oldfrey, B.; Ibrahim, N.; Holloway, C.; et al. Assistive Technology Use and Provision During COVID-19: Results From a Rapid Global Survey. Int. J. Health Policy Manag. 2020, 210, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Lazarou, I.; Nikolopoulos, S.; Petrantonakis, P.C.; Kompatsiaris, I.; Tsolaki, M. EEG-Based Brain–Computer Interfaces for Communication and Rehabilitation of People with Motor Impairment: A Novel Approach of the 21st Century. Front. Hum. Neurosci. 2018, 12, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaughan, T.M. Brain-computer interfaces for people with amyotrophic lateral sclerosis. Clin. Neurophysiol. Basis Tech. Asp. 2020, 168, 33–38. [Google Scholar] [CrossRef]
- De Marchi, F.; Sarnelli, M.F.; Serioli, M.; De Marchi, I.; Zani, E.; Bottone, N.; Ambrosini, S.; Garone, R.; Cantello, R.; Mazzini, L.; et al. Telehealth approach for amyotrophic lateral sclerosis patients: The experience during COVID-19 pandemic. Acta Neurol. Scand. 2021, 143, 489–496. [Google Scholar] [CrossRef]
- De Marchi, F.; Contaldi, E.; Magistrelli, L.; Cantello, R.; Comi, C.; Mazzini, L. Telehealth in Neurodegenerative Diseases: Opportunities and Challenges for Patients and Physicians. Brain Sci. 2021, 11, 237. [Google Scholar] [CrossRef]
- Palumbo, A.; Calabrese, B.; Ielpo, N.; Demeco, A.; Ammendolia, A.; Corchiola, D. Cloud-based biomedical system for remote monitoring of ALS patients. In Proceedings of the IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Seoul, Korea, 16–19 December 2020; pp. 1469–1476. [Google Scholar]
- Pinto, S.; Quintarelli, S.; Silani, V. New technologies and Amyotrophic Lateral Sclerosis—Which step forward rushed by the COVID-19 pandemic? J. Neurol. Sci. 2020, 418, 117081. [Google Scholar] [CrossRef]
- Xiong, M.; Brandenberger, A.; Bulger, M.; Chien, W.; Doyle, A.; Hao, W.; Jiang, J.; Kim, K.; Lahlou, S.; Leung, C.; et al. A Low-Cost, Semi-Autonomous Wheelchair Controlled by Motor Imagery and Jaw Muscle Activation. In Proceedings of the IEEE International Conference on Systems, Man and Cybernetics (SMC), Bari, Italy, 6–9 October 2019; pp. 2180–2185. [Google Scholar]
- Bi, L.; Fan, X.-A.; Liu, Y. EEG-Based Brain-Controlled Mobile Robots: A Survey. IEEE Trans. Hum.-Mach. Syst. 2013, 43, 161–176. [Google Scholar] [CrossRef]
- Krishnan, N.M.; Mariappan, M.; Muthukaruppan, K.; Hijazi, M.H.A.; Kitt, W.W. Electroencephalography (EEG) Based Control in Assistive Mobile Robots: A Review. In IOP Conference Series: Materials Science and Engineering; IOP Publishing: Bristol, UK, 2016; Volume 121, p. 012017. [Google Scholar]
- Fernández-Rodríguez, Á.; Velasco-Álvarez, F.; Ron-Angevin, R. Review of real brain-controlled wheelchairs. J. Neural Eng. 2016, 13, 61001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Qaysi, Z.; Zaidan, B.; Zaidan, A.; Suzani, M. A review of disability EEG based wheelchair control system: Coherent taxonomy, open challenges and recommendations. Comput. Methods Programs Biomed. 2018, 164, 221–237. [Google Scholar] [CrossRef]
- Leaman, J.; La, H.M. A Comprehensive Review of Smart Wheelchairs: Past, Present, and Future. IEEE Trans. Hum.-Mach. Syst. 2017, 47, 486–499. [Google Scholar] [CrossRef] [Green Version]
- Aljalal, M.; Ibrahim, S.; Djemal, R.; Ko, W. Comprehensive review on brain-controlled mobile robots and robotic arms based on electroencephalography signals. Intell. Serv. Robot. 2020, 13, 539–563. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Dev, A.; Rahman, A.; Mamun, N. Design of an EEG-Based Brain Controlled Wheelchair for Quadriplegic Patients. In Proceedings of the 3rd International Conference for Convergence in Technology (I2CT), Pune, India, 6–8 April 2018; pp. 1–5. [Google Scholar]
- Xin, L.; Gao, S.; Tang, J.; Xu, X. Design of a Brain Controlled Wheelchair. In Proceedings of the IEEE 4th International Conference on Control Science and Systems Engineering (ICCSSE), Wuhan, China, 24–26 August 2018; pp. 112–116. [Google Scholar]
- Abiyev, R.H.; Akkaya, N.; Aytac, E.; Günsel, I.; Çağman, A. Brain-Computer Interface for Control of Wheelchair Using Fuzzy Neural Networks. BioMed Res. Int. 2016, 2016, 9359868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Q.; Zhang, Z.; Yu, T.; He, S.; Li, Y. An EEG-/EOG-Based Hybrid Brain-Computer Interface: Application on Controlling an Integrated Wheelchair Robotic Arm System. Front. Neurosci. 2019, 13, 1243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, Y.; Zhou, Z.; Liu, Y.; Jiang, J.; Yin, E.; Zhang, N.; Wang, Z.; Liu, Y.; Wu, X.; Hu, D. Self-Paced Operation of a Wheelchair Based on a Hybrid Brain-Computer Interface Combining Motor Imagery and P300 Potential. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 2516–2526. [Google Scholar] [CrossRef]
- Long, J.; Li, Y.; Wang, H.; Yu, T.; Pan, J.; Li, F. A Hybrid Brain Computer Interface to Control the Direction and Speed of a Simulated or Real Wheelchair. IEEE Trans. Neural Syst. Rehabil. Eng. 2012, 20, 720–729. [Google Scholar] [CrossRef]
- Permana, K.; Wijaya, S.K.; Prajitno, P. Controlled wheelchair based on brain computer interface using Neurosky Mindwave Mobile 2. Proc. Int. Symp. Curr. Prog. Math. Sci. 2019, 2168, 020022. [Google Scholar] [CrossRef]
- Yu, Y.; Liu, Y.; Jiang, J.; Yin, E.; Zhou, Z.; Hu, D. An Asynchronous Control Paradigm Based on Sequential Motor Imagery and Its Application in Wheelchair Navigation. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 2367–2375. [Google Scholar] [CrossRef]
- Al-Turabi, H.; Al-Junaid, H. Brain Computer Interface for Wheelchair Control in Smart Environment. In Proceedings of the Smart Cities Symposium 2018, Bahrain, 22–23 April 2018; p. 23. [Google Scholar]
- Ron-Angevin, R.; Velasco-Álvarez, F.; Fernández-Rodríguez, Á.; Díaz-Estrella, A.; Blanca-Mena, M.J.; Vizcaíno-Martín, F.J. Brain-Computer Interface application: Auditory serial interface to control a two-class motor-imagery-based wheelchair. J. Neuroeng. Rehabil. 2017, 14, 49. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Li, Y.; Yan, Y.; Zhang, H.; Wu, S.; Yu, T.; Gu, Z. Control of a Wheelchair in an Indoor Environment Based on a Brain–Computer Interface and Automated Navigation. IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 24, 128–139. [Google Scholar] [CrossRef]
- Swee, S.K.; Kiang, K.D.T.; You, L.Z. EEG Controlled Wheelchair. In Proceedings of the MATEC Web of Conferences, Amsterdam, The Netherlands, 23–25 March 2016; Volume 51, p. 02011. [Google Scholar]
- Varona-Moya, S.; Velasco-Alvarez, F.; Sancha-Ros, S.; Fernández-Rodríguez, Á.; Blanca, M.J.; Angevin, R.R. Wheelchair navigation with an audio-cued, two-class motor imagery-based brain-computer interface system. In Proceedings of the 7th International IEEE/EMBS Conference on Neural Engineering (NER), Montpellier, France, 22–24 April 2015; pp. 174–177. [Google Scholar]
- Kim, K.-T.; Carlson, T.; Lee, S.-W. Design of a robotic wheelchair with a motor imagery based brain-computer interface. In Proceedings of the 2013 International Winter Workshop on Brain-Computer Interface (BCI), Pacific Grove, CA, USA, 3–7 June 2013; pp. 46–48. [Google Scholar] [CrossRef]
- Carlson, T.; Millan, J.D.R. Brain-Controlled Wheelchairs: A Robotic Architecture. IEEE Robot. Autom. Mag. 2013, 20, 65–73. [Google Scholar] [CrossRef] [Green Version]
- Reshmi, G.; Amal, A. Design of a BCI System for Piloting a Wheelchair Using Five Class MI Based EEG. In Proceedings of the Third International Conference on Advances in Computing and Communications, Kochi, India, 29–31 August 2013; pp. 25–28. [Google Scholar]
- Carra, M.; Balbinot, A. Evaluation of sensorimotor rhythms to control a wheelchair. In Proceedings of the 2013 ISSNIP Biosignals and Biorobotics Conference: Biosignals and Robotics for Better and Safer Living (BRC), Rio de Janeiro, Brazil, 18–20 February 2012; pp. 1–4. [Google Scholar]
- Li, J.; Liang, J.; Zhao, Q.; Li, J.; Hong, K.; Zhang, L. Design of assistive wheelchair system directly steered by human thoughts. Int. J. Neural Syst. 2013, 23, 1350013. [Google Scholar] [CrossRef] [Green Version]
- Choi, K. Control of a vehicle with EEG signals in real-time and system evaluation. Graefe Arch. Clin. Exp. Ophthalmol. 2011, 112, 755–766. [Google Scholar] [CrossRef] [PubMed]
- Carrino, F.; Dumoulin, J.; Mugellini, E.; Khaled, O.A.; Ingold, R. A self-paced BCI system to control an electric wheelchair: Evaluation of a commercial, low-cost EEG device. In Proceedings of the ISSNIP Biosignals and Biorobotics Conference: Biosignals and Robotics for Better and Safer Living (BRC), Rio de Janeiro, Brazil, 18–20 February 2012; pp. 1–6. [Google Scholar]
- Tsui, C.S.L.; Gan, J.; Hu, H. A Self-Paced Motor Imagery Based Brain-Computer Interface for Robotic Wheelchair Control. Clin. EEG Neurosci. 2011, 42, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Rashid, M.; Sulaiman, N.; Majeed, A.P.P.A.; Musa, R.M.; Nasir, A.F.A.; Bari, B.S.; Khatun, S. Current Status, Challenges, and Possible Solutions of EEG-Based Brain-Computer Interface: A Comprehensive Review. Front. Neurorobot. 2020, 14, 25. [Google Scholar] [CrossRef] [PubMed]
- Padfield, N.; Zabalza, J.; Zhao, H.; Masero, V.; Ren, J. EEG-Based Brain-Computer Interfaces Using Motor-Imagery: Techniques and Challenges. Sensors 2019, 19, 1423. [Google Scholar] [CrossRef] [Green Version]
- Steyrl, D.; Kobler, R.J.; Müller-Putz, G.R. On Similarities and Differences of Invasive and Non-Invasive Electrical Brain Signals in Brain-Computer Interfacing. J. Biomed. Sci. Eng. 2016, 9, 393–398. [Google Scholar] [CrossRef] [Green Version]
- Han, C.-H.; Kim, Y.-W.; Kim, D.Y.; Kim, S.H.; Nenadic, Z.; Im, C.-H. Electroencephalography-based endogenous brain–computer interface for online communication with a completely locked-in patient. J. Neuroeng. Rehabil. 2019, 16, 18. [Google Scholar] [CrossRef]
- Abiri, R.; Borhani, S.; Sellers, E.W.; Jiang, Y.; Zhao, X. A comprehensive review of EEG-based brain–computer interface paradigms. J. Neural Eng. 2018, 16, 011001. [Google Scholar] [CrossRef]
- Müller-Putz, G.R.; Scherer, R.; Brauneis, C.; Pfurtscheller, G. Steady-state visual evoked potential (SSVEP)-based communication: Impact of harmonic frequency components. J. Neural Eng. 2005, 2, 123–130. [Google Scholar] [CrossRef]
- Han, C.; Xu, G.; Xie, J.; Chen, C.; Zhang, S. Highly Interactive Brain–Computer Interface Based on Flicker-Free Steady-State Motion Visual Evoked Potential. Sci. Rep. 2018, 8, 5835. [Google Scholar] [CrossRef] [PubMed]
- Sellers, E.W.; Krusienski, D.J.; McFarland, D.J.; Vaughan, T.M.; Wolpaw, J.R. A P300 event-related potential brain–computer interface (BCI): The effects of matrix size and inter stimulus interval on performance. Biol. Psychol. 2006, 73, 242–252. [Google Scholar] [CrossRef]
- Xu, M.; Xiao, X.; Wang, Y.; Qi, H.; Jung, T.-P.; Ming, D. A Brain–Computer Interface Based on Miniature-Event-Related Potentials Induced by Very Small Lateral Visual Stimuli. IEEE Trans. Biomed. Eng. 2018, 65, 1166–1175. [Google Scholar] [CrossRef]
- Onose, G.; Grozea, C.; Anghelescu, A.; Daia, C.; Sinescu, C.J.; Ciurea, A.; Spircu, T.; Mirea, A.; Andone, I.; Spânu, A.; et al. On the feasibility of using motor imagery EEG-based brain–computer interface in chronic tetraplegics for assistive robotic arm control: A clinical test and long-term post-trial follow-up. Spinal Cord 2012, 50, 599–608. [Google Scholar] [CrossRef] [Green Version]
- Shin, J.; Kwon, J.; Im, C.-H. A Ternary Hybrid EEG-NIRS Brain-Computer Interface for the Classification of Brain Activation Patterns during Mental Arithmetic, Motor Imagery, and Idle State. Front. Aging Neurosci. 2018, 12, 5. [Google Scholar] [CrossRef]
- Wolpaw, J.R.; Birbaumer, N.; McFarland, D.J.; Pfurtscheller, G.; Vaughan, T.M. Brain–computer interfaces for communication and control. Clin. Neurophysiol. 2002, 113, 767–791. [Google Scholar] [CrossRef]
- Serby, H.; Yom-Tov, E.; Inbar, G. An improved P300-based brain-computer interface. IEEE Trans. Neural Syst. Rehabil. Eng. 2005, 13, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Middendorf, M.; McMillan, G.; Calhoun, G.; Jones, K. Brain-computer interfaces based on the steady-state visual-evoked response. IEEE Trans. Rehabil. Eng. 2000, 8, 211–214. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Wang, R.; Gao, X.; Hong, B.; Gao, S. A practical VEP-based brain-computer interface. IEEE Trans. Neural Syst. Rehabil. Eng. 2006, 14, 234–240. [Google Scholar] [CrossRef]
- Pichiorri, F.; Mattia, D. Brain-computer interfaces in neurologic rehabilitation practice. Brain-Comput. Interfaces 2020, 168, 101–116. [Google Scholar] [CrossRef]
- Cheng, N.; Phua, K.S.; Lai, H.S.; Tam, P.K.; Tang, K.Y.; Cheng, K.K.; Yeow, R.C.-H.; Ang, K.K.; Guan, C.; Lim, J.H. Brain-Computer Interface-Based Soft Robotic Glove Rehabilitation for Stroke. IEEE Trans. Biomed. Eng. 2020, 67, 3339–3351. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, U.; Mrachacz-Kersting, N.; Birbaumer, N. Neuropsychological and neurophysiological aspects of brain-computer-interface (BCI) control in paralysis. J. Physiol. 2021, 599, 2351–2359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pulliam, C.L.; Stanslaski, S.R.; Denison, T.J. Chapter 25—Industrial perspectives on brain-computer interface technology. In Handbook of Clinical Neurology; Ramsey, N.F., Millán, J.D.R., Eds.; Elsevier: Amsterdam, The Netherlands, 2020; Volume 168, pp. 341–352. [Google Scholar]
- Edelman, B.; Meng, J.; Suma, D.; Zurn, C.; Nagarajan, E.; Baxter, B.; Cline, C.C.; He, B.J.S.R. Noninvasive neuroimaging en-hances continuous neural tracking for robotic device control. Sci. Robot. 2019, 4, 31. [Google Scholar] [CrossRef]
- Elstob, D.; Secco, E.L. A Low Cost Eeg Based Bci Prosthetic Using Motor Imagery. Int. J. Inf. Technol. Converg. Serv. 2016, 6, 23–36. [Google Scholar] [CrossRef] [Green Version]
- Kruse, A.; Suica, Z.; Taeymans, J.; Schuster-Amft, C. Effect of brain-computer interface training based on non-invasive electroencephalography using motor imagery on functional recovery after stroke—A systematic review and meta-analysis. BMC Neurol. 2020, 20, 385. [Google Scholar] [CrossRef]
- Baniqued, P.D.E.; Stanyer, E.C.; Awais, M.; Alazmani, A.; Jackson, A.E.; Mon-Williams, M.A.; Mushtaq, F.; Holt, R.J. Brain–computer interface robotics for hand rehabilitation after stroke: A systematic review. J. Neuroeng. Rehabil. 2021, 18, 15. [Google Scholar] [CrossRef]
- Ramos-Murguialday, A.; Broetz, D.; Rea, M.; Läer, L.; Yilmaz, Ö.; Msc, F.L.B.; Liberati, G.; Curado, M.R.; Garcia-Cossio, E.; Vyziotis, A.; et al. Brain-machine interface in chronic stroke rehabilitation: A controlled study. Ann. Neurol. 2013, 74, 100–108. [Google Scholar] [CrossRef]
- Ang, K.K.; Guan, C.; Ephua, K.S.; Ewang, C.; Ezhou, L.; Etang, K.Y.; Joseph, G.J.E.; Ekuah, C.W.K.; Echua, K.S.G. Brain-computer interface-based robotic end effector system for wrist and hand rehabilitation: Results of a three-armed randomized controlled trial for chronic stroke. Front. Neuroeng. 2014, 7, 30. [Google Scholar] [CrossRef]
- Ono, T.; Eshindo, K.; Ekawashima, K.; Eota, N.; Eito, M.; Eota, T.; Emukaino, M.; Efujiwara, T.; Ekimura, A.; Eliu, M.; et al. Brain-computer interface with somatosensory feedback improves functional recovery from severe hemiplegia due to chronic stroke. Front. Neuroeng. 2014, 7, 19. [Google Scholar] [CrossRef]
- Frolov, A.A.; Mokienko, O.; Lyukmanov, R.; Biryukova, E.; Kotov, S.; Turbina, L.; Nadareyshvily, G.; Bushkova, Y. Post-stroke Rehabilitation Training with a Motor-Imagery-Based Brain-Computer Interface (BCI)-Controlled Hand Exoskeleton: A Randomized Controlled Multicenter Trial. Front. Neurosci. 2017, 11, 400. [Google Scholar] [CrossRef] [Green Version]
- Hiremath, S.; Chen, W.; Wang, W.; Foldes, S.; Yang, Y.; Tyler-Kabara, E.C.; Collinger, J.L.; Boninger, M.L. Brain computer interface learning for systems based on electrocorticography and intracortical microelectrode arrays. Front. Integr. Neurosci. 2015, 9, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merel, J.; Fox, R.; Jebara, T.; Paninski, L. A multi-agent control framework for co-adaptation in brain-computer interfaces. In Proceedings of the 26th International Conference on Neural Information Processing Systems, Lake Tahoe, NV, USA, 5–10 December 2013; pp. 2841–2849. [Google Scholar]
- Mladenović, J.; Mattout, J.; Lotte, F. A generic framework for adaptive EEG-based BCI training and operation. In Brain-Computer Interfaces Handbook: Technological and Theoretical Advances; Chang, S.N., Anton, N., Fabien, L., Eds.; CRC Press: Boca Raton, FL, USA, 2017; Volume 1. [Google Scholar]
- Millàn, J.D.R. Brain-Machine Interfaces: The Perception-Action Closed Loop: A Two-Learner System. IEEE Syst. Man Cybern. Magazine 2015, 1, 14. [Google Scholar] [CrossRef] [Green Version]
- Perdikis, S.; Tonin, L.; Saeedi, S.; Schneider, C.; Millán, J.D.R. The Cybathlon BCI race: Successful longitudinal mutual learning with two tetraplegic users. PLoS Biol. 2018, 16, e2003787. [Google Scholar] [CrossRef]
- Millán, J.D.R.; Renkens, F.; Mouriño, J.; Gerstner, W. Noninvasive Brain-Actuated Control of a Mobile Robot by Human EEG. IEEE Trans. Biomed. Eng. 2004, 51, 1026–1033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, K.; Matsunaga, K.; Wang, H. Electroencephalogram-based control of an electric wheelchair. IEEE Trans. Robot. 2005, 21, 762–766. [Google Scholar] [CrossRef]
- Tang, J.; Liu, Y.; Hu, D.; Zhou, Z. Towards BCI-actuated smart wheelchair system. Biomed. Eng. Online 2018, 17, 111. [Google Scholar] [CrossRef] [Green Version]
- Rebsamen, B.; Burdet, E.; Guan, C.; Teo, C.L.; Zeng, Q.; Ang, M.; Laugier, C. Controlling a wheelchair using a BCI with low information transfer rate. In Proceedings of the IEEE 10th International Conference on Rehabilitation Robotics, Noordwijk, The Netherlands, 13–15 June 2007; pp. 1003–1008. [Google Scholar]
- Iturrate, I.; Antelis, J.M.; Kubler, A.; Minguez, J. A Noninvasive Brain-Actuated Wheelchair Based on a P300 Neurophysiological Protocol and Automated Navigation. IEEE Trans. Robot. 2009, 25, 614–627. [Google Scholar] [CrossRef] [Green Version]
- Alqasemi, R.; Dubey, R. A 9-DoF Wheelchair-Mounted Robotic Arm System: Design, Control, Brain-Computer Interfacing, and Testing. In Advances in Robot Manipulators; InTech: London, UK, 2010. [Google Scholar]
- Shin, B.-G.; Kim, T.; Jo, S. Non-invasive brain signal interface for a wheelchair navigation. In Proceedings of the International Conference on Control, Automation, and Systems (ICCAS), Jeju, Korea, 27–30 October 2010; pp. 2257–2260. [Google Scholar]
- Lopes, A.; Pires, G.; Nunes, U.J.C. Assisted navigation for a brain-actuated intelligent wheelchair. Robot. Auton. Syst. 2013, 61, 245–258. [Google Scholar] [CrossRef]
- Mandel, C.; Luth, T.; Laue, T.; Rofer, T.; Graser, A.; Krieg-Bruckner, B. Navigating a smart wheelchair with a brain-computer interface interpreting steady-state visual evoked potentials. In Proceedings of the IEEE/RSJ International Conference on Intelligent Robots and Systems, St. Louis, MI, USA, 10–15 October 2009; pp. 1118–1125. [Google Scholar]
- Xu, Z.; Li, J.; Gu, R.; Xia, B. Steady-State Visually Evoked Potential (SSVEP)-Based Brain-Computer Interface (BCI): A Low-Delayed Asynchronous Wheelchair Control System. In Algorithms and Data Structures; Springer International Publishing: Berlin/Heidelberg, Germany, 2012; Volume 7663, pp. 305–314. [Google Scholar]
- Müller, S.M.T.; Bastos, T.F.; Filho, M.S. Proposal of a SSVEP-BCI to Command a Robotic Wheelchair. J. Control Autom. Electr. Syst. 2013, 24, 97–105. [Google Scholar] [CrossRef]
- Duan, J.; Li, Z.; Yang, C.; Xu, P. Shared control of a brain-actuated intelligent wheelchair. In Proceedings of the 11th World Congress on Intelligent Control and Automation, Shenyang, China, 29 June–4 July 2014; pp. 341–346. [Google Scholar]
- Li, Y.; Pan, J.; Wang, F.; Yu, Z. A Hybrid BCI System Combining P300 and SSVEP and Its Application to Wheelchair Control. IEEE Trans. Biomed. Eng. 2013, 60, 3156–3166. [Google Scholar] [CrossRef]
- Cao, L.; Li, J.; Ji, H.; Jiang, C. A hybrid brain computer interface system based on the neurophysiological protocol and brain-actuated switch for wheelchair control. J. Neurosci. Methods 2014, 229, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Trambaiolli, L.R.; Falk, T.H. Chapter 10 Hybrid brain–computer interfaces for wheelchair control: A review of existing solu-tions, their advantages and open challenges. In Smart Wheelchairs and Brain-Computer Interfaces; Academic Press: Cambridge, MA, USA, 2018; pp. 229–256. [Google Scholar]
- Pfurtscheller, G.; Allison, B.Z.; Bauernfeind, G.; Brunner, C.; Escalante, T.S.; Scherer, R.; Zander, T.O.; Mueller-Putz, G.; Neuper, C.; Birbaumer, N. The hybrid BCI. Front. Neurosci. 2010, 4, 30. [Google Scholar] [CrossRef]
- Allison, B.Z.; Neuper, C. Could Anyone Use a BCI? In Human–Computer Interaction Series; Springer Science and Business Media LLC.: Berlin/Heidelberg, Germany, 2010; pp. 35–54. [Google Scholar]
- Ing. Arrigo Palumbo, PhD Website and Publications. Available online: https://arrigopalumbo.com/pubblicazioni/ (accessed on 7 August 2021).
- SIMpLE Project. Available online: https://biomedical.arrigopalumbo.com/progetto-simple/ (accessed on 7 August 2021).
- Alessio Forlano Designer Website. Available online: http://www.alessioforlano.com/ (accessed on 7 August 2021).
- Soufineyestani, M.; Dowling, D.; Khan, A. Electroencephalography (EEG) Technology Applications and Available Devices. Appl. Sci. 2020, 10, 7453. [Google Scholar] [CrossRef]
- Gu, X.; Cao, Z.; Jolfaei, A.; Xu, P.; Wu, D.; Jung, T.-P.; Lin, C.-T. EEG-based Brain-Computer Interfaces (BCIs): A Survey of Recent Studies on Signal Sensing Technologies and Computational Intelligence Approaches and Their Applications. IEEE/ACM Trans. Comput. Biol. Bioinform. 2021. [Google Scholar] [CrossRef]
- Emotiv-Epoc. Available online: https://www.emotiv.com/epoc/ (accessed on 7 August 2021).
- Williams, N.S.; McArthur, G.M.; Badcock, N.A. 10 years of EPOC: A scoping review of Emotiv’s portable EEG device. BioRxiv 2020. [Google Scholar] [CrossRef]
- G.Tec-USBamp. Available online: https://www.gtec.at/product-configurator/g-usbamp/ (accessed on 7 August 2021).
- Brainproducts. Available online: https://www.brainproducts.com/products_by_apps.php?aid=5 (accessed on 7 August 2021).
- Jiang, X.; Bian, G.-B.; Tian, Z. Removal of Artifacts from EEG Signals: A Review. Sensors 2019, 19, 987. [Google Scholar] [CrossRef] [Green Version]
- Aggarwal, S.; Chugh, N. Signal processing techniques for motor imagery brain computer interface: A review. Array 2019, 1, 100003. [Google Scholar] [CrossRef]
- Singh, A.; Hussain, A.; Lal, S.; Guesgen, H. A Comprehensive Review on Critical Issues and Possible Solutions of Motor Imagery Based Electroencephalography Brain-Computer Interface. Sensors 2021, 21, 2173. [Google Scholar] [CrossRef] [PubMed]
- Ramoser, H.; Muller-Gerking, J.; Pfurtscheller, G. Optimal spatial filtering of single trial EEG during imagined hand movement. IEEE Trans. Rehabil. Eng. 2000, 8, 441–446. [Google Scholar] [CrossRef] [Green Version]
- Lotte, F.; Congedo, M.; Lécuyer, A.; Lamarche, F.; Arnaldi, B. A review of classification algorithms for EEG-based brain–computer interfaces. J. Neural Eng. 2007, 4, R1–R13. [Google Scholar] [CrossRef] [PubMed]
- Vapnik, V.N. The Nature of Statistical Learning Theory; Springer Inc.: New York, NY, USA, 1995. [Google Scholar]
- Tyagi, A.; Nehra, V. Classification of motor imagery EEG signals using SVM, k-NN and ANN. CSI Trans. ICT 2016, 4, 135–139. [Google Scholar] [CrossRef]
- Brunner, C.; Andreoni, G.; Bianchi, L.; Blankertz, B.; Breitwieser, C.; Kanoh, S.i.; Kothe, C.A.; Lécuyer, A.; Makeig, S.; Mellinger, J.; et al. BCI Software Platforms. In Towards Practical Brain-Computer Interfaces: Bridging the Gap from Research to Real-World Applications; Allison, B.Z., Dunne, S., Leeb, R., Del R. Millán, J., Nijholt, A., Eds.; Springer: Berlin/Heidelberg, Germany, 2013; pp. 303–331. [Google Scholar]
- Tayeb, Z.; Waniek, N.; Fedjaev, J.; Ghaboosi, N.; Rychly, L.; Widderich, C.; Richter, C.; Braun, J.; Saveriano, M.; Cheng, G.; et al. Gumpy: A Python toolbox suitable for hybrid brain–computer interfaces. J. Neural Eng. 2018, 15, 065003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The GNU General Public License v3.0. Available online: http://www.gnu.org/licenses/gpl-3.0.html (accessed on 8 September 2021).
- OpenVibe. Available online: http://openvibe.inria.fr/ (accessed on 7 August 2021).
- The OpenBCI Gui. Available online: https://docs.openbci.com/Software/OpenBCISoftware/GUIDocs/ (accessed on 7 August 2021).
- Matanga, Y.; Djouani, K.; Anish, K. A Matlab/Simulink framework for real time implementation of endogenous brain computer interfaces. In Proceedings of the 2017 IEEE AFRICON, Cape Town, South Africa, 18–20 September 2017; pp. 100–105. [Google Scholar]
- Venthur, B.; Dähne, S.; Höhne, J.; Heller, H.; Blankertz, B. Wyrm: A Brain-Computer Interface Toolbox in Python. Neuroinformatics 2015, 13, 471–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wyrm. Available online: https://github.com/bbci/wyrm (accessed on 7 August 2021).
- Schalk, G.; McFarland, D.J.; Hinterberger, T.; Birbaumer, N.; Wolpaw, J. BCI2000: A General-Purpose Brain-Computer Interface (BCI) System. IEEE Trans. Biomed. Eng. 2004, 51, 1034–1043. [Google Scholar] [CrossRef] [PubMed]
- BCI2000. Available online: https://www.bci2000.org/mediawiki/index.php/Main_Page (accessed on 7 August 2021).
- Kothe, C.A.; Makeig, S. BCILAB: A platform for brain–computer interface development. J. Neural Eng. 2013, 10, 056014. [Google Scholar] [CrossRef] [Green Version]
- BCILAB. Available online: https://www.nitrc.org/projects/bcilab/ (accessed on 7 August 2021).
- Gumpy. Available online: http://gumpy.org/ (accessed on 7 August 2021).
- Peterson, V.; Galván, C.; Hernández, H.; Spies, R. A feasibility study of a complete low-cost consumer-grade brain-computer interface system. Heliyon 2020, 6, e03425. [Google Scholar] [CrossRef]
- Sellers, E.W.; Vaughan, T.M.; Wolpaw, J. A brain-computer interface for long-term independent home use. Amyotroph. Lateral Scler. 2010, 11, 449–455. [Google Scholar] [CrossRef]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef]
- Hochreiter, S.; Schmidhuber, J. Long short-term memory. Neural Comput. 1997, 9, 1735–1780. [Google Scholar] [CrossRef] [PubMed]
- Palumbo, A.; Vizza, P.; Veltri, P.; Gambardella, A.; Pucci, F.; Sturniolo, M. Design of an electronic device for brain computer interface applications. In Proceedings of the 2009 IEEE International Workshop on Medical Measurements and Applications, Cetraro, Italy, 29–30 May 2009; pp. 99–103. [Google Scholar] [CrossRef]
- Palumbo, A. An Embedded System for EEG Acquisition and Processing for Brain Computer Interface Applications. In Wearable and Autonomous Biomedical Devices and Systems for Smart Environment: Issues and Characterization; Lay-Ekuakille, A., Mukhopadhyay, S.C., Eds.; Springer: Berlin/Heidelberg, Germany, 2010; pp. 137–154. [Google Scholar]
- Schettini, F.; Aloise, F.; Mecella, M.; Caruso, M.; Palumbo, A.; Pizzimenti, A.; Inghilleri, M.; Cincotti, F. From Keyboard to Brain-Computer Interface: The Brindisys Project; GNB2012: Rome, Italy, 2012; ISBN 978-88-555-3182-5. [Google Scholar]
- Schettini, F.; Riccio, A.; Simione, L.; Liberati, G.; Caruso, M.; Calabrese, B.; Ielpo, N.; Palumbo, A.; Frasca, V.; Mecella, M.; et al. The Brindisys Project: Brain-computer interface devices to support individual autonomy in locked-in individuals. In 3° Convegno Arisla: Nuove Prospettive di Ricerca per un Futuro Senza; SLA: Milano, Italy, 2012. [Google Scholar]
- Schettini, F. The Brindisys project: Brain Computer Interfaces as assistive technology for people with ALS. In Proceedings of the Fifth International Brain-Computer Interface Meeting, Pacific Grove, CA, USA, 3–7 June 2013. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Reference | MI Paradigm | Types of Control Command | EEG System | Additional Biosignals Acquisition | n° of EEG Electrodes | EEG Sample Frequency (Hz) | EEG Features Extraction | Classification Algorithm | Context and Duration of the Experimental Tests | n° of Users | Performance § | Wheelchair Type and Components | Obstacle Avoidance System | Software |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Xiong et al., 2019 [8] | LH RH Jaw Clench | Left Right Forward Stop | OpenBCI’s Cyton Biosensing 32-bit board (also used for EMG signal), (OpenBCI, New York, NY, USA) | EMG ECG US Location | 4: C1, C2, C3, C4 | 250 | PSD | Logistic Regression | INDOOR (Office/Laboratory) Average duration: 5 min (run) * 4–19 (n° of runs) = 20–95 min | 7 CTR | Mean subject accuracy: 60 ± 5% | Modified version of commercially available Orthofab Oasis 2008 wheelchair (Orthofab, Anjou, QC, Canada) with components: n° 2 commercial-grade 40A, 12 V PWM controllers connected to an Arduino Uno. Project: MILO: Mind Controlled Locomotive | n° 4 consumer-grade ultrasonic sensors | OpenBCI Graphical User Interface (GUI) Pyton Javascript |
| Permana et al., 2019 [22] | MI and eye motion -Think moving forward -Think moving backward -Think moving backward while continually move the eyes -Think moving forward while continually move the eyes -Default (motionless) | Move forward Move backward Turn left Turn right Default (motionless) | Neurosky Mindwave Mobile2 | NO | 1: Fp1 | 512 | For MI: eSense score For eyes-motion: high alpha | n.d. | INDOOR (Office/Laboratory) Average duration: 5 min | 5 CTR | Success rate range: 46, 67–82.22% | Modified version of JRWD 501 electric wheelchair | NO | Matlab |
| Yu et al., 2018 [23] | LH RH IDLE STATE | Move forward Turn left Turn right Accelerate Decelerating Stopping | BrainAmp DC, (Brain Products, GmbH, Germany) | NO | 31: F3, F1, Fz, F2, F4, FC5, FC3, FC1, FCz, FC2, FC4, FC6, C5, C3, C1, Cz, C2, C4, C6, CP5, CP3, CP1, CPz, CP2, CP4, CP6, P3, P1, Pz, P2, P4 | 250 | Multi CSP | LDA | INDOOR (Office/Laboratory) Average duration: Offline training: 8 s (trial) * 15 (n° of trials) = 2 min per mental task + 5 min (rest period) Online wheelchair navigation experiment (navigation time): 2106.4 s. | 7 CTR | Accuracy: >85% Success rate: 94.2% | Wheelchair prototype: a chair and an omnidirectional moving vehicle | NO | n.d. |
| Al-Turabi et al., 2018 [24] | Imagine visually moving a pen | Forward, Backward Right Left | Emotiv Epoc | NO | 14 (+2 ref): AF3; F7; F3; FC5; T7; P7; O1; O2; P8; T8; FC6; F4; F8; AF4 (+CMS and DRL) | 128 | PSD | SVM KNN ANN | INDOOR (Office/Laboratory) Average duration: n.d. | 1 CTR | Accuracy: 70.8–79.2% | Wheelchair prototype | Ultrasonic sensor | Matlab |
| Ron-Angevin et al., 2017 [25] | RH IDLE STATE | Move forward Move backward, Turn right Turn left | Acti-CHamp amplifier (Brain Products GmbH, Munich, Germany) | NO | 9: C3, F3, P3, T7, Cz, C4, F4, P4, T8. | 200 | Average signal power | LDA | INDOOR (Laboratory/University room) Average duration: Calibration session: 30 min Navigation session in a VE: 5–10 min Navigation session in a real environment with the BCW: 5–10 min. | 17 CTR | Medium accuracy: 83% | Customized Invacare Mistral3 electric wheelchair | -n° 11 ultrasonic rangefinders SRF08 -n° 2 magnetic rotary encoders AS5048 | Matlab |
| Zhang et al., 2016 * [26] | RH LH | Turn right Turn left Stop | EEG-cap (Compumedics, Neuroscan Inc., Abbotsford, Australia) EEG-amplified (NuAmps, Neuroscan) | NO | 15: FC3, FCz, FC4, C3, Cz, C4, CP3, CPz, CP4, P3, Pz, P4, O1, Oz, O2 | 250 | CSP | SVM | INDOOR (room/home environment) Average duration (time to complete a destination selection using the MI-based BCI): -24.3 s (Scenario A) -23.8 s (Scenario B) | 3 CTR (MI-based BCI experiment) | Success rate: 94.7 ± 2.3% | Mid-wheel drive model 888WNLL, Pihsiang Machinery MFG. Co. Ltd., Taiwan, with sensors: - n° 1 laser range finder (SICK LMS 111) - n° 2 encoders, which are attached to the central driving wheels | n° 2 webcams n° 3 ultrasonic sensors | GUI |
| Swee et al., 2016 [27] | PUSH, PULL, LEFT, RIGHT | Forward Backward Left Right | Emotiv Epoc | NO | 14 (+2 ref): AF3; F7; F3; FC5; T7; P7; O1; O2; P8; T8; FC6; F4; F8; AF4 (+CMS and DRL) | 128 | n.d. | n.d. | INDOOR (Office/Laboratory) | 5 CTR | Accuracy: <90% | Wheelchair Prototype with components: Scooter motors DC 24 V ATmega328P microcontroller Arduino Uno microcontroller board Bluetooth Hc-06 module | NO | Emotiv API Arduino IDE |
| Varona-Moya et al., 2015 [28] | RH RELAX | Move forward Turn right Move backward Turn left | actiCHamp amplifier (Brain Products GmbH, Munich, Germany) | NO | 9: F3, F4, T7, T8, C3, C4, P3, P4, Cz | 200 | PSD | LDA | INDOOR (Private room in the school) Average duration: Training schedule: 30 min (first phase) + 15 min (second phase) + 20 min (third phase) Robotic wheelchair navigation tasks (minimum time lapse): -4 min 38 s (for task 1) -5 min (for task 2) | 3 CTR | n.d. | Customized Invacare “Mistral3” electric wheelchair | n° 11 SRF08 ultrasonic range finders (i.e., sonars) allowed to create a real-time discrete grid map of the area surrounding the wheelchair. n° 2 AS5048 magnetic rotary encoders were attached to the wheelchair’s driving wheels to carry out the odometry and thus compute the wheelchair’s heading at every moment. | Matlab |
| Kim et al., 2013 [29] | LH RH F F-LH F-RH | Left Right Forward Left-diagonal Right- diagonal | g.tec system (an EEG cap and a gUSBamp amplifier) | NO | 16 | 256 | OVR CSP | LDA OVR LDA | INDOOR (Office) Average duration: n.d. | 1 CTR | n.d. | Electric wheelchair (K2 POWER model of WHEELOPIA), with components: n° 2 permanent magnet DC brushed motors (pMDC motors: 24 V at 320 W). n° 1 micro controller unit (MCV, Atmega128). | NO | Simulink Matlab |
| Carlson et al., 2013 [30] | RH LH F | Turn right Turn left Keep going straight | EEG device (model n.d.) | NO | 16: Fz, FC3, FC1, FCz, FC2, FC4, C3, C1, Cz, C2, C4, CP3, CP1, CPz, CP2, CP4 | 512 | PSD | Gaussian classifier | INDOOR (Office/Laboratory) Average duration: Online BCI session: 4–5 min Driving task: 15–30 min | 4 CTR | Average accuracy: 95% | Modified version of commercial mid-wheel drive model by Invacare Corporation (TDX SP2) | n° 10 close-range sonar sensors n° 2 webcams to provide environmental feedback to the controller. | n.d. |
| Reshmi, et al., 2013 [31] | LH RH RLH RLF RELAX | Move left Move right Go forward Go backward Stop | RMS EEG machine | NO | 3: C3,C4, Cz | 256 | PSD | SVM | INDOOR (Laboratory) Average duration: 2.30 min each run | 50 CTR | n.d. | Wheelchair Prototype with components ATMEGA 328 microcontroller L293 motor driving circuit | NO | Matlab |
| Carra et al., 2013 [32] | RH F | Forward Turn right | EEG device (model n.d.) | NO | 6: F3, P3, Fz, Pz, F4, P4 | 256 | BPM | LDA | INDOOR (Office/Laboratory) Average duration: 5 min (training test) + 3 sessions (7 positions each) | 1 CTR | Average hit rate: 65.7% | Motorized wheelchair (model n.d.) | NO | LabView 9.0 Matlab |
| Li et al., 2013 [33] | RH LH RLF | Turn right Turn left Go forward | g.tec amplifier (Guger Technologies, Austria) | NO | 14: C5, C3, C1, Cz, C2, C4, C6, CP5, CP3, CP1, CPz, CP2, CP4, CP6 | 256 | CSP | SVM | INDOOR (Office) Average duration: 4 s (trial) * 12 (n° of trials) * 4 (n° of sessions) | 3 CTR | Average trial accuracy: 82.56% | Wheelchair system (model n.d.) | NO | Provided GUI |
| Choi et al., 2012 [34] | LH (imagine clenching the left hand) RH (imagine squeezing the right hand) RLF STOP: EMG | Turns left Turns right Moves forward | g.tec system: an EEG cap and a gUSBamp amplifier (Guger Technologies, Schiedlberg, Austria) | EMG | 5: C3, C4, Cz, FC3, FC4 | 256 | CSFSD | SVM | INDOOR (Office) Average duration: Bar-controlling experiment: 5 s (trial) * 30 (n° of trials) * 7 (n° of sets) Obstacle avoidance experiment: 24–28 s (trial) * 10 (n° of trials) * 7 (n° of sets) | 3 CTR | Success rate: 90–95% | Rear-wheel drive type wheelchair: JW active model of Yamaha Motor Co | NO | Matlab |
| Carrino et al., 2012 [35] | RH LH | Turn right Turn left | Emotiv Epoc | NO | 14 (+2 ref): AF3; F7; F3; FC5; T7; P7; O1; O2; P8; T8; FC6; F4; F8; AF4 (+CMS and DRL) | 128 | n.d. | LDA | INDOOR (Office) Average duration: n.d. | 1 CTR | Classification rate: 67.5–91% on 2 gestures (left and right inputs) | Wheelchair prototype | NO | Developed application GERBIL. OpenVibe |
| Tsui, et al., 2011 [36] | RH LH IDLE STATE | Turn right Turn left | g. tec amplifier (Guger Technologies, Schiedlberg, Austria) | NO | 10 (5 bipolar EEG channels): C3 (FC3 vs. CP3), C1 (FC1 vs. CP1), Cz (FCz vs. CPz), C2 (FC2 vs. CP2), and C4 (FC4 vs. CP4) | 250 | Logarithmic Band Power | LDA | INDOOR (University of Essex’s robotic arena) Average duration: −108.75 s for subject 1–114.75 s for subject 2. | 2 CTR | n.d. | Electric-powered wheelchair (RoboChair) with components: An on-board DSP TMS320LF2407-based controller for motion control of 2 differentially-driven wheels; An on-board embedded PC connected to the DSP motion controller via a USB link A 24-volt battery providing power for the DSP controller, the PC and drive motors A local joystick controller connected to an A/D converter of the DSP-based controller | n° 6 ultrasonic range sensors for obstacle avoidance; n° 1 Hokuyo URG-04LX laser range finder to scan the environment. | n.d. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palumbo, A.; Gramigna, V.; Calabrese, B.; Ielpo, N. Motor-Imagery EEG-Based BCIs in Wheelchair Movement and Control: A Systematic Literature Review. Sensors 2021, 21, 6285. https://doi.org/10.3390/s21186285
Palumbo A, Gramigna V, Calabrese B, Ielpo N. Motor-Imagery EEG-Based BCIs in Wheelchair Movement and Control: A Systematic Literature Review. Sensors. 2021; 21(18):6285. https://doi.org/10.3390/s21186285
Chicago/Turabian StylePalumbo, Arrigo, Vera Gramigna, Barbara Calabrese, and Nicola Ielpo. 2021. "Motor-Imagery EEG-Based BCIs in Wheelchair Movement and Control: A Systematic Literature Review" Sensors 21, no. 18: 6285. https://doi.org/10.3390/s21186285
APA StylePalumbo, A., Gramigna, V., Calabrese, B., & Ielpo, N. (2021). Motor-Imagery EEG-Based BCIs in Wheelchair Movement and Control: A Systematic Literature Review. Sensors, 21(18), 6285. https://doi.org/10.3390/s21186285