
High PD-L1 Expression on Tumor Cells Indicates Worse Overall Survival in Advanced Oral Squamous Cell Carcinomas of the Tongue and the Floor of the Mouth but Not in Other Oral Compartments


 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Group
2.2. Specimen Preparation and Immunohistochemistry
2.3. Statistical Analysis
3. Results
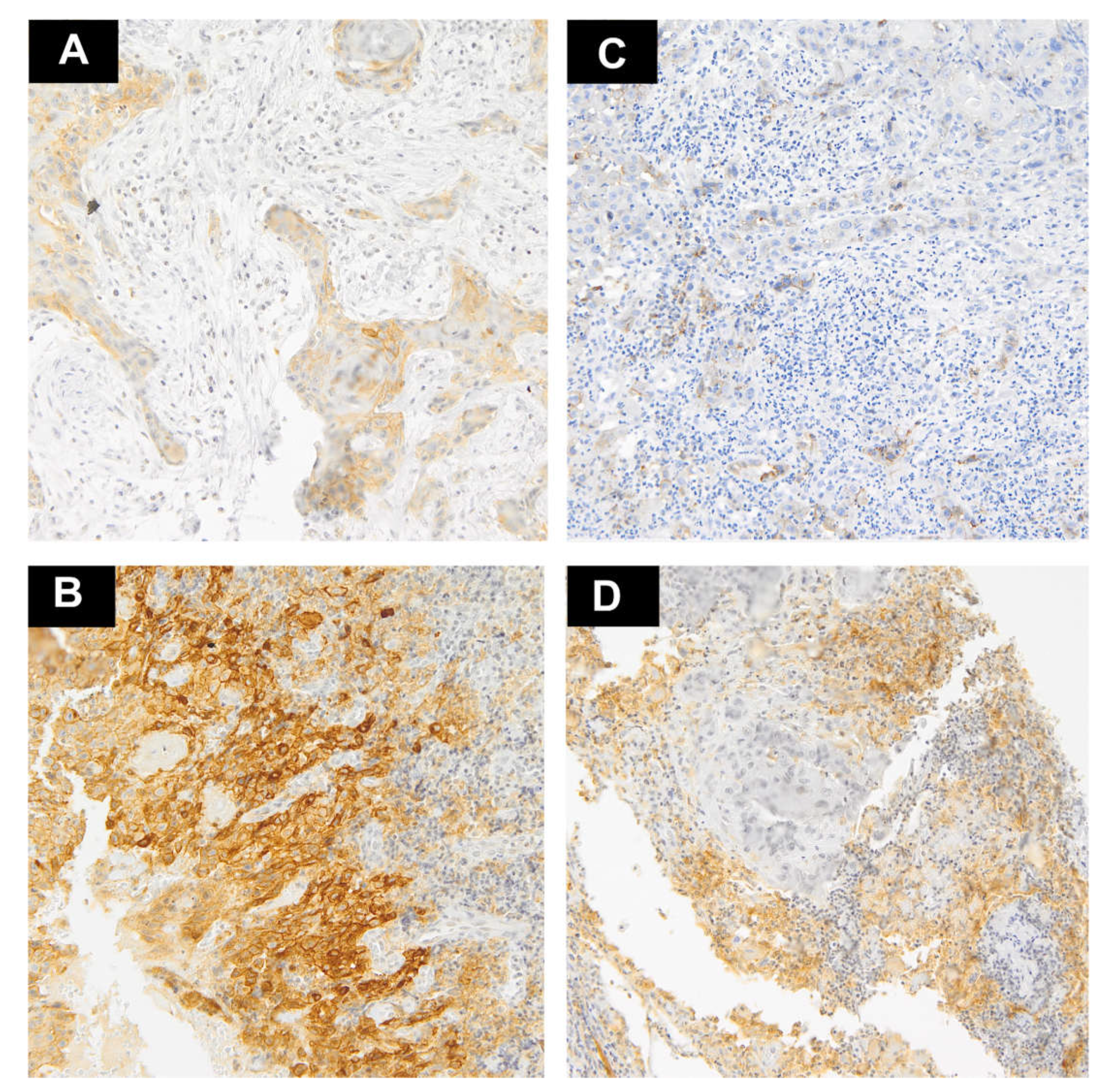
3.1. PD-L1 Expression
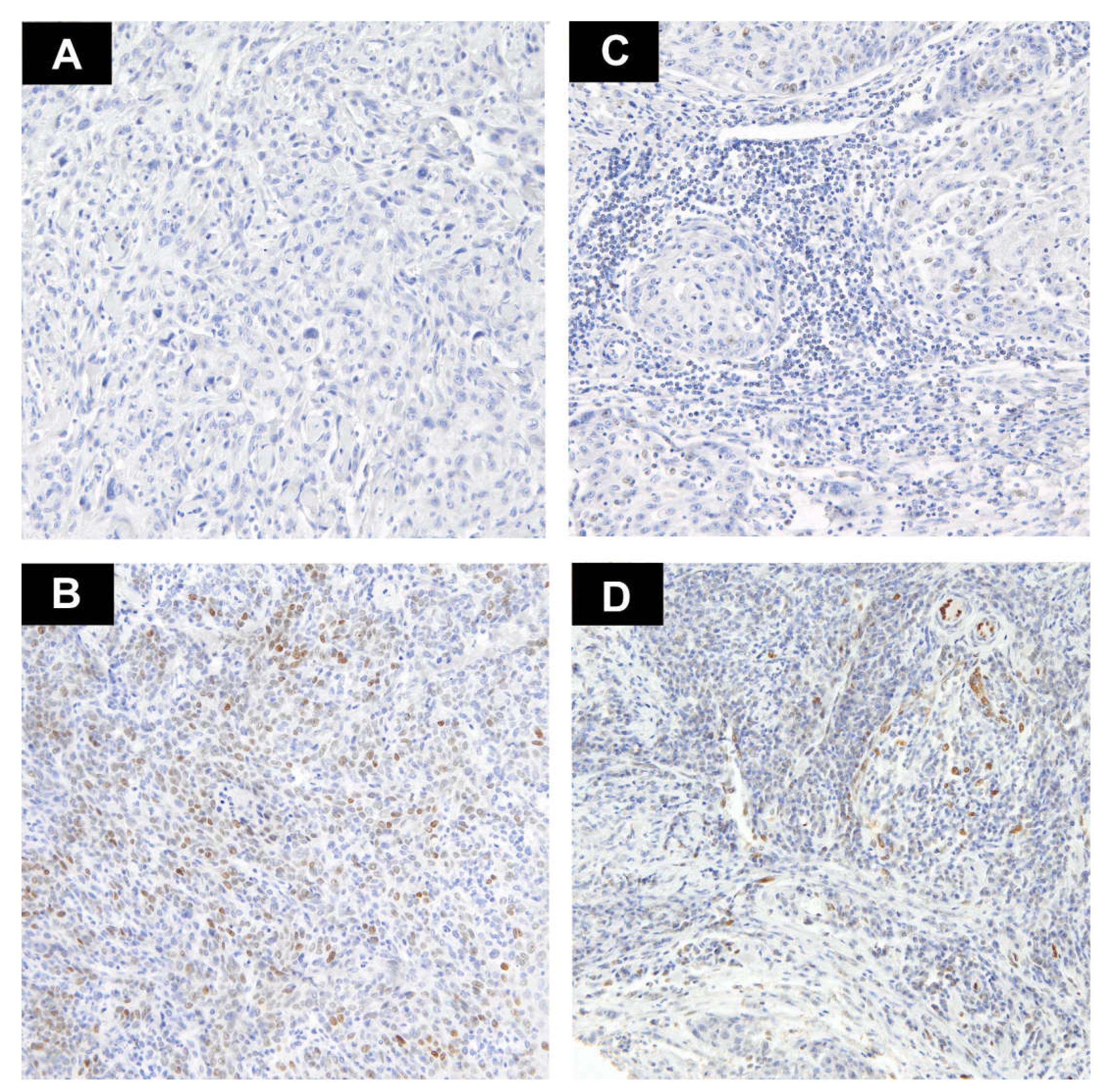
3.2. IL-33 Expression
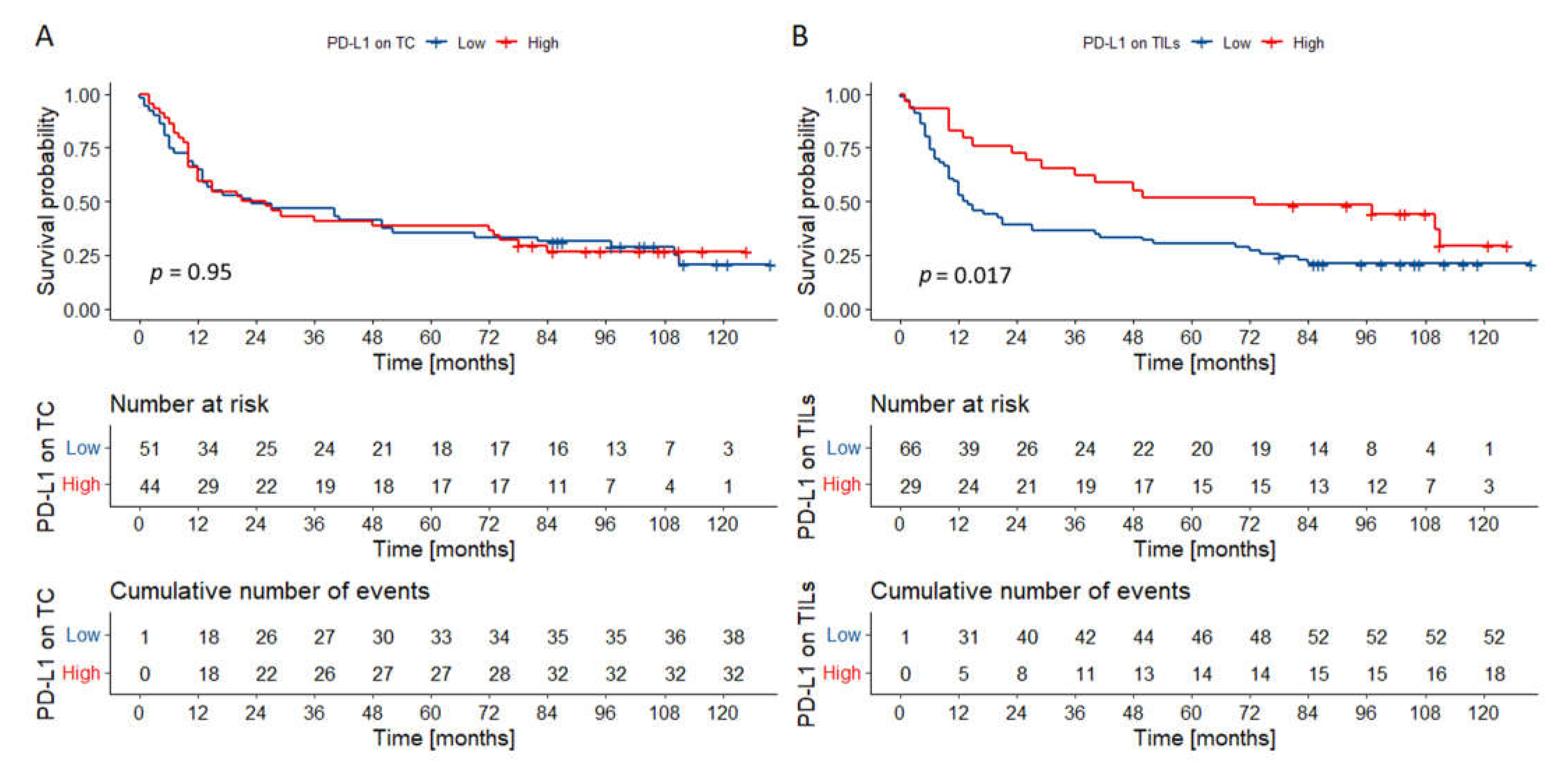
3.3. Survival Analysis
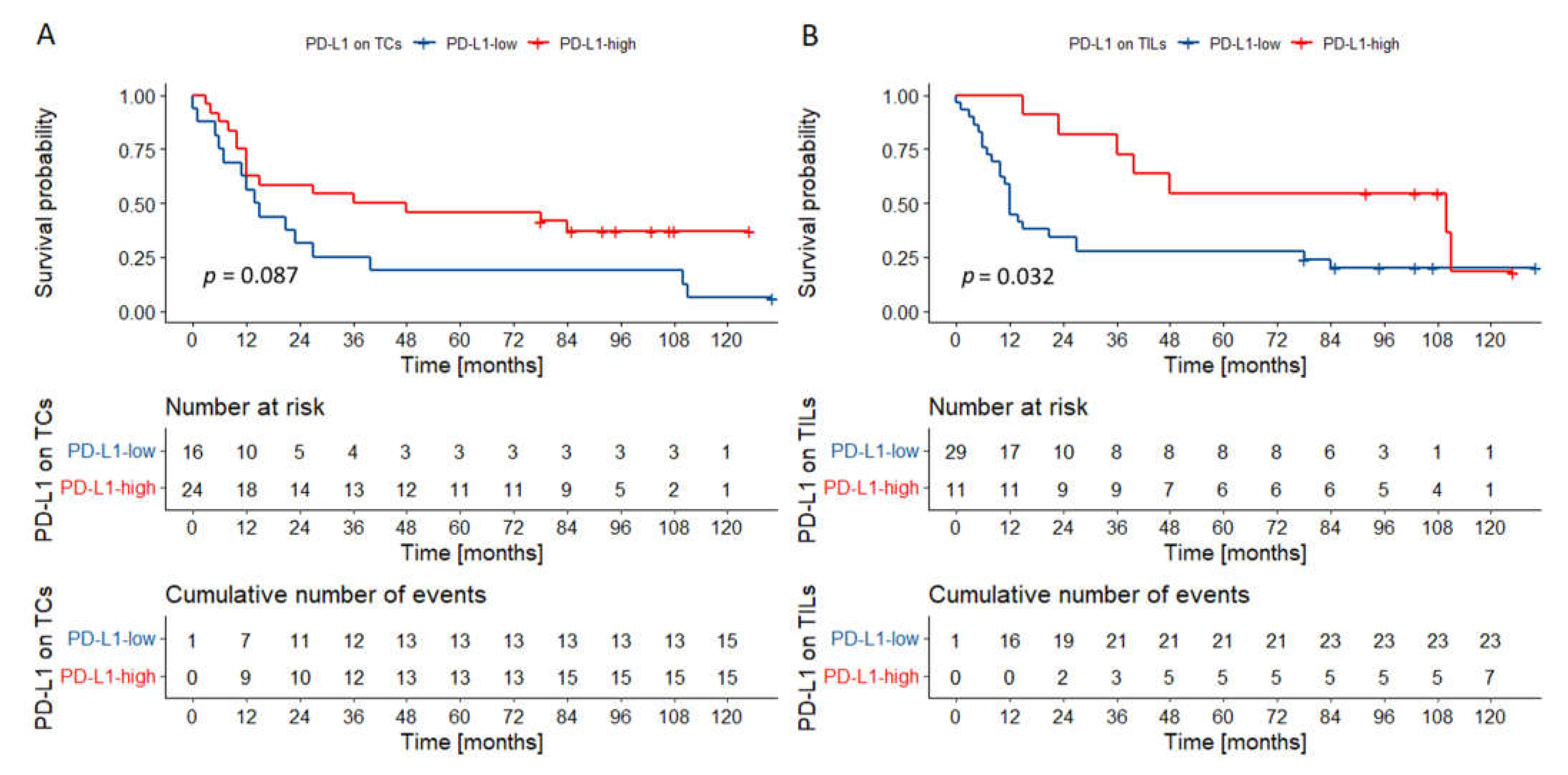
3.3.1. Whole Cohort
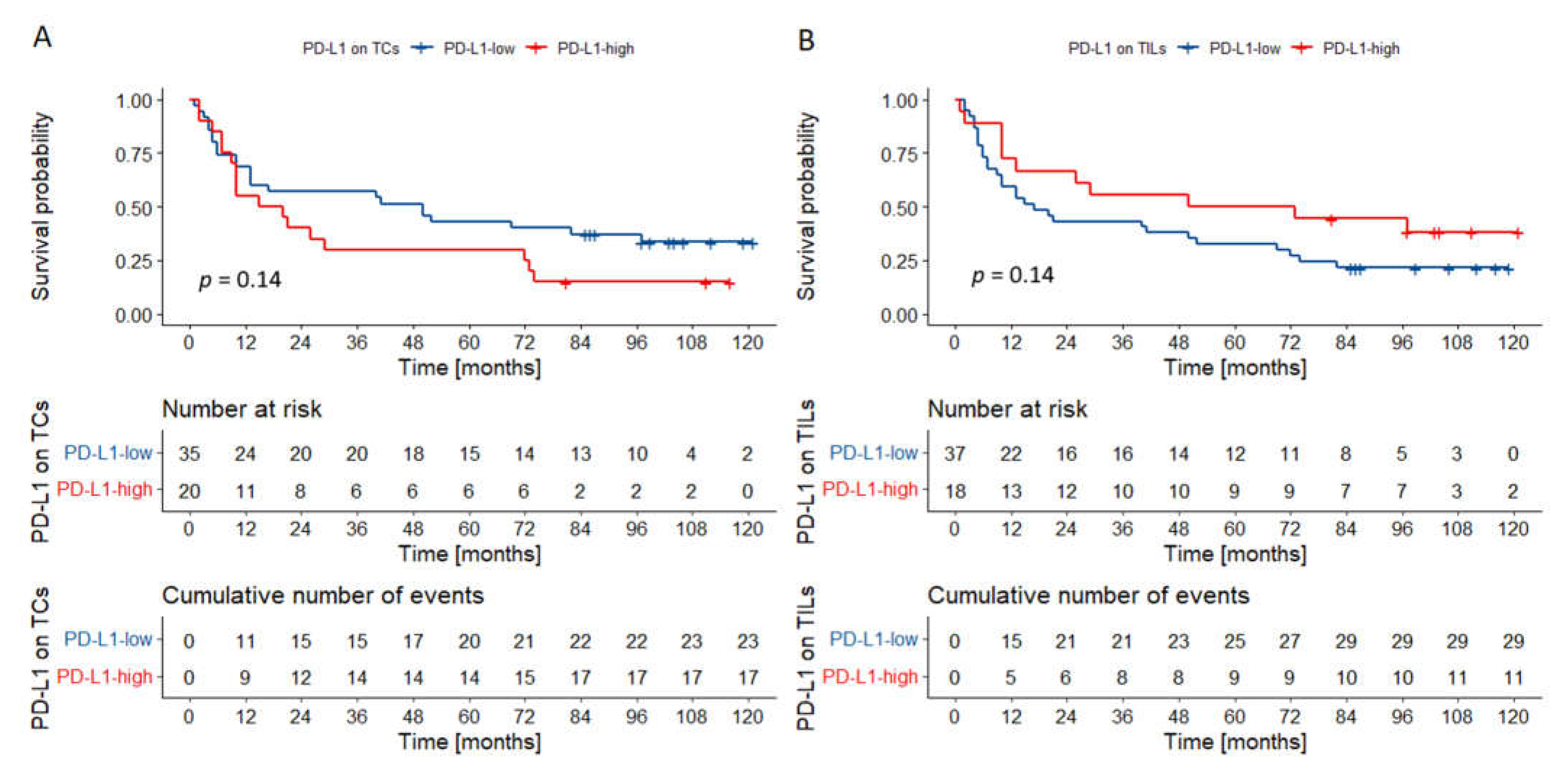
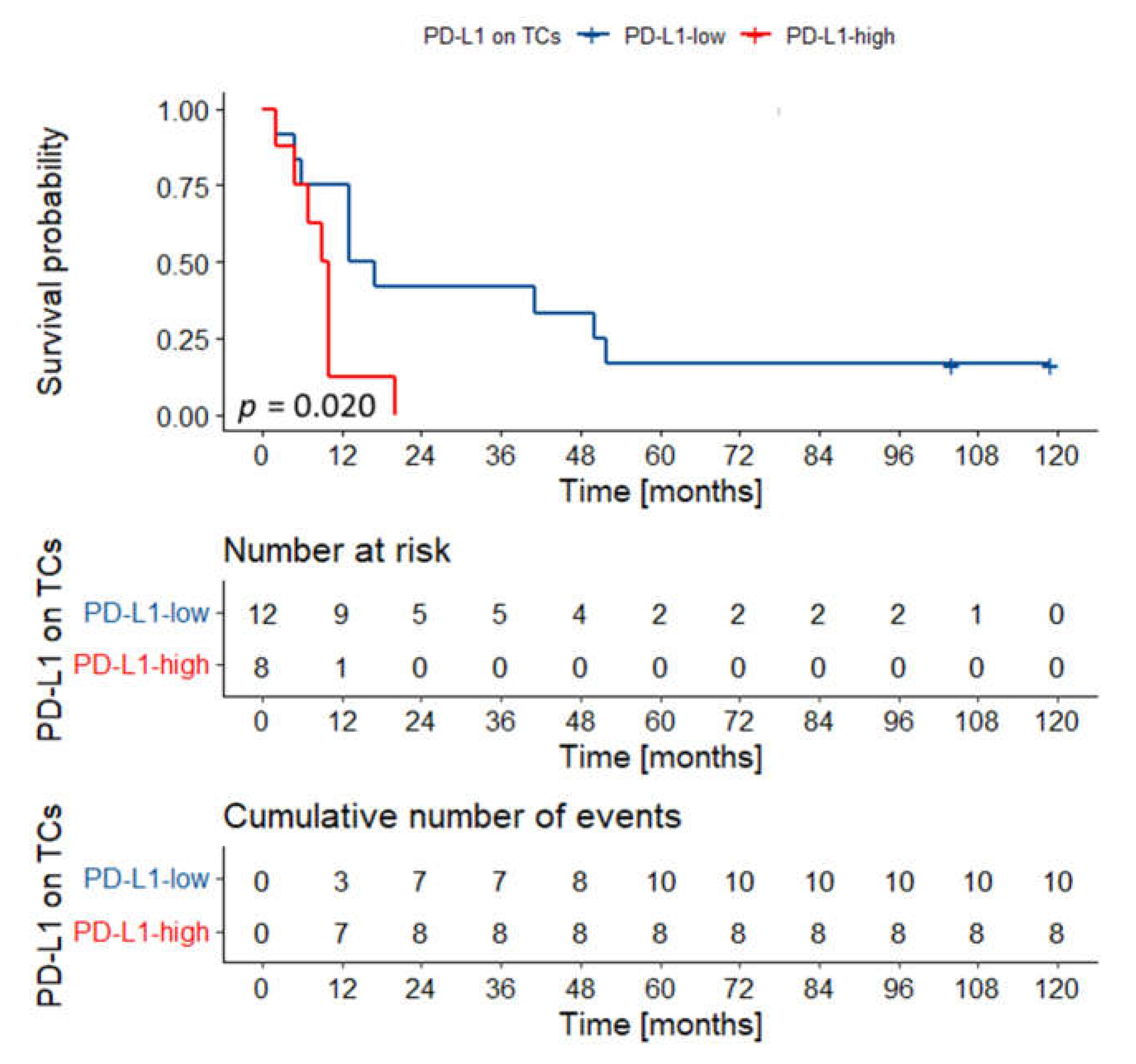
3.3.2. Prognostic Significance of PD-L1 and IL-33 Expression in Various Locations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AJCC | American Joint Committee on Cancer |
| CAFs | carcinoma-associated fibroblasts |
| CI | confidence interval |
| FFPE | formalin-fixed paraffin-embedded |
| HR | hazard ratio |
| IHC | immunohistochemistry |
| IL-33 | interleukin 33 |
| IFN-γ | interferon gamma |
| M | lymph nodes |
| N | metastasis |
| OS | overall survival |
| OSCC | oral squamous cell carcinoma |
| p | p value |
| PD-L1 | programmed cell death-ligand 1 |
| ST2 | membrane receptor soluble interleukin 1 receptor-like 1 |
| T | tumor |
| TCs | tumor cells |
| TILs | tumor infiltrating lymphocytes |
| TMA | tissue microarray |
| TME | tumor microenviroment |
| TNM | tumor, lymph nodes, metastasis—TNM Classification of Malignant Tumors |
References
- Feller, L.; Lemmer, J. Oral Squamous Cell Carcinoma: Epidemiology, Clinical Presentation and Treatment. J. Cancer Ther. 2012, 03, 263–268. [Google Scholar] [CrossRef] [Green Version]
- Starzyńska, A.; Sejda, A.; Adamski, Ł.; Adamska, P.; Pęksa, R.; Sakowicz-Burkiewicz, M.; Wychowański, P.; Jereczek-Fossa, B.A. The B7 family molecules in oral squamous cell carcinoma: A systematic review. Part I: B7-H1 (PD-L1) and B7-DC (PD-L2). Adv. Dermatol. Allergol. 2020, 37. [Google Scholar] [CrossRef]
- Starzyńska, A.; Sejda, A.; Adamski, Ł.; Adamska, P.; Pęksa, R.; Sakowicz-Burkiewicz, M.; Wychowański, P.; Jereczek-Fossa, B.A. The B7 family molecules in oral squamous cell carcinoma: A systematic review. Part II: B7-1, B7-2, B7-H2, B7-H3, B7-H4, B7-H5 (VISTA), B7-H6 and B7-H7. Adv. Dermatol. Allergol. 2020, 37. [Google Scholar] [CrossRef]
- Starzyńska, A.; Sejda, A.; Adamska, P.; Marvaso, G.; Sakowicz-Burkiewicz, M.; Adamski, Ł.; Jereczek-Fossa, B.A. Prognostic value of the PIK3CA, AKT, PTEN mutations in oral squamous cell carcinoma: Literature review. Arch. Med. Sci. 2021, 17, 207–217. [Google Scholar] [CrossRef]
- Binnewies, M.; Roberts, E.W.; Kersten, K.; Chan, V.; Fearon, D.F.; Merad, M.; Coussens, L.M.; Gabrilovich, D.I.; Ostrand-Rosenberg, S.; Hedrick, C.C.; et al. Understanding the tumor immune microenvironment (TIME) for effective therapy. Nat. Med. 2018, 24, 541–550. [Google Scholar] [CrossRef]
- Lacina, L.; Plzak, J.; Kodet, O.; Szabo, P.; Chovanec, M.; Dvorankova, B.; Smetana, K. Cancer Microenvironment: What Can We Learn from the Stem Cell Niche. Int. J. Mol. Sci. 2015, 16, 24094–24110. [Google Scholar] [CrossRef]
- Zitvogel, L.; Kroemer, G. Targeting PD-1/PD-L1 interactions for cancer immunotherapy. Oncoimmunology 2012, 1, 1223–1225. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Ahn, E.; Kissick, H.T.; Ahmed, R. Reinvigorating Exhausted T Cells by Blockade of the PD-1 Pathway. For. Immunopathol. Dis. Therap. 2015, 6, 7–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pęksa, R.; Kunc, M.; Popęda, M.; Piątek, M.; Bieńkowski, M.; Żok, J.; Starzyńska, A.; Perdyan, A.; Sowa, M.; Duchnowska, R.; et al. Combined Assessment of Immune Checkpoint Regulator VISTA on Tumor-Associated Immune Cells and Platelet-to-Lymphocyte Ratio Identifies Advanced Germ Cell Tumors with Higher Risk of Unfavorable Outcomes. Cancers 2021, 13, 1750. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.R.; Ha, S.J.; Hong, M.H.; Heo, S.J.; Koh, Y.W.; Choi, E.C.; Kim, E.K.; Pyo, K.H.; Jung, I.; Seo, D.; et al. PD-L1 expression on immune cells, but not on tumor cells, is a favorable prognostic factor for head and neck cancer patients. Sci. Rep. 2016, 6, 36956. [Google Scholar] [CrossRef] [Green Version]
- Carbone, D.P.; Reck, M.; Paz-Ares, L.; Creelan, B.; Horn, L.; Steins, M.; Felip, E.; van den Heuvel, M.M.; Ciuleanu, T.E.; Badin, F.; et al. First-Line Nivolumab in Stage IV or Recurrent Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 376, 2415–2426. [Google Scholar] [CrossRef]
- Lee, J.; Kefford, R.; Carlino, M. PD-1 and PD-L1 inhibitors in melanoma treatment: Past success, present application and future challenges. Immunotherapy 2016, 8, 733–746. [Google Scholar] [CrossRef] [PubMed]
- Ferris, R.L.; Blumenschein, G., Jr.; Fayette, J.; Guigay, J.; Colevas, A.D.; Licitra, L.; Harrington, K.J.; Kasper, S.; Vokes, E.E.; Even, C.; et al. Nivolumab vs investigator’s choice in recurrent or metastatic squamous cell carcinoma of the head and neck: 2-year long-term survival update of CheckMate 141 with analyses by tumor PD-L1 expression. Oral Oncol. 2018, 81, 45–51. [Google Scholar] [CrossRef]
- Xiong, Y.; Neskey, D.M.; Horton, J.D.; Paulos, C.M.; Knochelmann, H.M.; Armeson, K.E.; Young, M.R.I. Immunological effects of nivolumab immunotherapy in patients with oral cavity squamous cell carcinoma. BMC Cancer 2020, 20, 229. [Google Scholar] [CrossRef] [PubMed]
- Rousset-Rouviere, S.; Rochigneux, P.; Chrétien, A.-S.; Fattori, S.; Gorvel, L.; Provansal, M.; Lambaudie, E.; Olive, D.; Sabatier, R. Endometrial Carcinoma: Immune Microenvironment and Emerging Treatments in Immuno-Oncology. Biomedicines 2021, 9, 632. [Google Scholar] [CrossRef]
- Martin, M.U. Special aspects of interleukin-33 and the IL-33 receptor complex. Semin. Immunol. 2013, 25, 449–457. [Google Scholar] [CrossRef]
- Pisani, L.F.; Tontini, G.E.; Gentile, C.; Marinoni, B.; Teani, I.; Nandi, N.; Creo, P.; Asti, E.; Bonavina, L.; Vecchi, M.; et al. Proinflammatory Interleukin-33 Induces Dichotomic Effects on Cell Proliferation in Normal Gastric Epithelium and Gastric Cancer. Int. J. Mol. Sci. 2021, 22, 5792. [Google Scholar] [CrossRef]
- Yazdi, A.S.; Ghoreschi, K. The Interleukin-1 Family. Adv. Exp. Med. Biol. 2016, 941, 21–29. [Google Scholar] [CrossRef]
- Chen, S.F.; Nieh, S.; Jao, S.W.; Wu, M.Z.; Liu, C.L.; Chang, Y.C.; Lin, Y.S. The paracrine effect of cancer-associated fibroblast-induced interleukin-33 regulates the invasiveness of head and neck squamous cell carcinoma. J. Pathol. 2013, 231, 180–189. [Google Scholar] [CrossRef] [PubMed]
- Choi, M.-R.; Sosman, J.A.; Zhang, B. The Janus Face of IL-33 Signaling in Tumor Development and Immune Escape. Cancers 2021, 13, 3281. [Google Scholar] [CrossRef]
- Alvarez, F.; Fritz, J.H.; Piccirillo, C.A. Pleiotropic Effects of IL-33 on CD4+ T Cell Differentiation and Effector Functions. Front. Immunol. 2019, 10, 522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qin, L.; Dominguez, D.; Chen, S.; Fan, J.; Long, A.; Zhang, M.; Fang, D.; Zhang, Y.; Kuzel, T.M.; Zhang, B. Exogenous IL-33 overcomes T cell tolerance in murine acute myeloid leukemia. Oncotarget 2016, 7, 61069–61080. [Google Scholar] [CrossRef] [Green Version]
- Casciaro, M.; Cardia, R.; Di Salvo, E.; Tuccari, G.; Ieni, A.; Gangemi, S. Interleukin-33 Involvement in Nonsmall Cell Lung Carcinomas: An Update. Biomolecules 2019, 9, 203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishikawa, K.; Yagi-Nakanishi, S.; Nakanishi, Y.; Kondo, S.; Tsuji, A.; Endo, K.; Wakisaka, N.; Murono, S.; Yoshizaki, T. Expression of interleukin-33 is correlated with poor prognosis of patients with squamous cell carcinoma of the tongue. Auris Nasus Larynx 2014, 41, 552–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, L.; Ren, J.; Zhang, D.; Li, Y.; Huang, X.; Hu, Q.; Wang, H.; Song, Y.; Ni, Y.; Hou, Y. A novel stromal lncRNA signature reprograms fibroblasts to promote the growth of oral squamous cell carcinoma via LncRNA-CAF/interleukin-33. Carcinogenesis 2018, 39, 397–406. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A language and environment for statistical computing. In R Foundation for Statistical Computing; European Environment Agency: Vienna, Austria, 2020. [Google Scholar]
- Kassambara, A.; Kosinski, M.; Biecek, P. Survminer: Drawing Survival Curves Using “ggplot2”. R Package Version 0.4.8 2020. Available online: https://cran.r-project.org/web/packages/survminer/ (accessed on 30 April 2021).
- Xiao, N. ggsci: Scientific Journal and Sci-Fi Themed Color Palettes for “ggplot2”. R Packag. Version 2. 2018. Available online: https://CRAN.R-project.org/package=ggsci (accessed on 30 April 2021).
- Kuchar, M.; Strizova, Z.; Capkova, L.; Komarc, M.; Skrivan, J.; Bartunkova, J.; Smrz, D.; Plzak, J. The Periphery of Salivary Gland Carcinoma Tumors Reveals a PD-L1/PD-1 Biomarker Niche for the Evaluation of Disease Severity and Tumor—Immune System Interplay. Biomedicines. 2021, 9, 97. [Google Scholar] [CrossRef]
- Plzák, J.; Bouček, J.; Bandúrová, V.; Kolář, M.; Hradilová, M.; Szabo, P.; Lacina, L.; Chovanec, M.; Smetana, K. The Head and Neck Squamous Cell Carcinoma Microenvironment as a Potential Target for Cancer Therapy. Cancers 2019, 11, 440. [Google Scholar] [CrossRef] [Green Version]
- Valero, C.; Zanoni, D.K.; Pillai, A.; Xu, B.; Katabi, N.; Ghossein, R.A.; Ganly, I.; Morris, L.G.T.; Shah, J.P.; Wong, R.J.; et al. Nodal characteristics associated with adverse prognosis in oral cavity cancer are linked to host immune status. J. Surg. Oncol. 2021, 123, 141–148. [Google Scholar] [CrossRef]
- Ho, A.S.; Kim, S.; Tighiouart, M.; Gudino, C.; Mita, A.; Scher, K.S.; Laury, A.; Prasad, R.; Shiao, S.L.; Van Eyk, J.E.; et al. Metastatic Lymph Node Burden and Survival in Oral Cavity Cancer. J. Clin. Oncol. 2017, 35, 3601–3609. [Google Scholar] [CrossRef] [Green Version]
- Lequerica-Fernández, P.; Suárez-Canto, J.; Rodriguez-Santamarta, T.; Rodrigo, J.P.; Suárez-Sánchez, F.J.; Blanco-Lorenzo, V.; Domínguez-Iglesias, F.; García-Pedrero, J.M.; de Vicente, J.C. Prognostic Relevance of CD4+, CD8+ and FOXP3+ TILs in Oral Squamous Cell Carcinoma and Correlations with PD-L1 and Cancer Stem Cell Markers. Biomedicines 2021, 9, 653. [Google Scholar] [CrossRef]
- Cui, B.; Chen, J.; Luo, M.; Wang, L.; Chen, H.; Kang, Y.; Wang, J.; Zhou, X.; Feng, Y.; Zhang, P. Protein kinase D3 regulates the expression of the immunosuppressive protein, PD-L1, through STAT1/STAT3 signaling. Int. J. Oncol. 2020, 56, 909–920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meehan, K.; Leslie, C.; Lucas, M.; Jacques, A.; Mirzai, B.; Lim, J.; Bulsara, M.; Khan, Y.; Wong, N.C.; Solomon, B.; et al. Characterization of the immune profile of oral tongue squamous cell carcinomas with advancing disease. Cancer Med. 2020, 9, 4791–4807. [Google Scholar] [CrossRef] [PubMed]
- Quan, H.; Shan, Z.; Liu, Z.; Liu, S.; Yang, L.; Fang, X.; Li, K.; Wang, B.; Deng, Z.; Hu, Y.; et al. The repertoire of tumor-infiltrating lymphocytes within the microenvironment of oral squamous cell carcinoma reveals immune dysfunction. Cancer Immunol. Immunother. 2020, 69, 465–476. [Google Scholar] [CrossRef]
- Wilms, T.; Gu, X.; Boldrup, L.; Coates, P.J.; Fahraeus, R.; Wang, L.; Sgaramella, N.; Nielsen, N.; Norberg-Spaak, L.; Nylander, K. PD-L1 in squamous cell carcinoma of the oral tongue shows gender-specific association with prognosis. Oral Dis. 2020, 26, 1414–1423. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Li, P.; Zhao, L.; Wang, M.; Tong, D.; Meng, Z.; Zhang, Q.; Li, Q.; Zhang, F. Expression and clinical value of PD-L1 which is regulated by BRD4 in tongue squamous cell carcinoma. J. Cell. Biochem. 2020, 121, 1855–1869. [Google Scholar] [CrossRef]
- Ahmadi, N.; Gao, K.; Chia, N.; Kwon, M.S.; Palme, C.E.; Gupta, R.; Clark, J. Association of PD-L1 expression in oral squamous cell carcinoma with smoking, sex, and p53 expression. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2019, 128, 631–638. [Google Scholar] [CrossRef]
- de Vicente, J.C.; Rodríguez-Santamarta, T.; Rodrigo, J.P.; Blanco-Lorenzo, V.; Allonca, E.; García-Pedrero, J.M. PD-L1 Expression in Tumor Cells Is an Independent Unfavorable Prognostic Factor in Oral Squamous Cell Carcinoma. Cancer Epidemiol. Biomark. Prev. 2019, 28, 546–554. [Google Scholar] [CrossRef] [Green Version]
- Kouketsu, A.; Sato, I.; Oikawa, M.; Shimizu, Y.; Saito, H.; Takahashi, T.; Kumamoto, H. Expression of immunoregulatory molecules PD-L1 and PD-1 in oral cancer and precancerous lesions: A cohort study of Japanese patients. J. Cranio-Maxillofac. Surg. 2019, 47, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, H.; Sakakura, K.; Arisaka, Y.; Tokue, A.; Kaira, K.; Tada, H.; Higuchi, T.; Okamoto, A.; Tsushima, Y.; Chikamatsu, K. Clinical and Biological Significance of PD-L1 Expression Within the Tumor Microenvironment of Oral Squamous Cell Carcinoma. Anticancer. Res. 2019, 39, 3039–3046. [Google Scholar] [CrossRef]
- Tojyo, I.; Shintani, Y.; Nakanishi, T.; Okamoto, K.; Hiraishi, Y.; Fujita, S.; Enaka, M.; Sato, F.; Muragaki, Y. PD-L1 expression correlated with p53 expression in oral squamous cell carcinoma. Maxillofac. Plast. Reconstr. Surg. 2019, 41, 56. [Google Scholar] [CrossRef] [Green Version]
- Hanna, G.J.; Woo, S.-B.; Li, Y.Y.; Barletta, J.A.; Hammerman, P.S.; Lorch, J.H. Tumor PD-L1 expression is associated with improved survival and lower recurrence risk in young women with oral cavity squamous cell carcinoma. Int. J. Oral Maxillofac. Surg. 2018, 47, 568–577. [Google Scholar] [CrossRef] [PubMed]
- Maruse, Y.; Kawano, S.; Jinno, T.; Matsubara, R.; Goto, Y.; Kaneko, N.; Sakamoto, T.; Hashiguchi, Y.; Moriyama, M.; Toyoshima, T.; et al. Significant association of increased PD-L1 and PD-1 expression with nodal metastasis and a poor prognosis in oral squamous cell carcinoma. Int. J. Oral Maxillofac. Surg. 2018, 47, 836–845. [Google Scholar] [CrossRef] [Green Version]
- Stasikowska-Kanicka, O.; Wągrowska-Danilewicz, M.; Danilewicz, M. Immunohistochemical Analysis of Foxp3+, CD4+, CD8+ Cell Infiltrates and PD-L1 in Oral Squamous Cell Carcinoma. Pathol. Oncol. Res. 2018, 24, 497–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stasikowska-Kanicka, O.; Wągrowska-Danilewicz, M.; Danilewicz, M. CD8+ and CD163+ infiltrating cells and PD-L1 immunoexpression in oral leukoplakia and oral carcinoma. APMIS 2018, 126, 732–738. [Google Scholar] [CrossRef] [PubMed]
- Udeabor, S.E.; Adisa, A.O.; Orlowska, A.; Sader, R.A.; Ghanaati, S. Assessment of programmed cell death proteins in oral squamous cell carcinoma. Afr. J. Biomed. Res. 2018, 21, 11–13. [Google Scholar]
- Wirsing, A.M.; Ervik, I.K.; Seppola, M.; Uhlin-Hansen, L.; Steigen, S.E.; Hadler-Olsen, E. Presence of high-endothelial venules correlates with a favorable immune microenvironment in oral squamous cell carcinoma. Mod. Pathol. 2018, 31, 910–922. [Google Scholar] [CrossRef] [PubMed]
- Ahn, H.; Yang, J.M.; Kim, H.; Chung, J.H.; Ahn, S.-H.; Jeong, W.J.; Paik, J.H. Clinicopathologic implications of the miR-197/PD-L1 axis in oral squamous cell carcinoma. Oncotarget 2017, 8, 66178–66194. [Google Scholar] [CrossRef] [Green Version]
- Feng, Z.; Bethmann, D.; Kappler, M.; Ballesteros-Merino, C.; Eckert, A.; Bell, R.B.; Cheng, A.; Bui, T.; Leidner, R.; Urba, W.J.; et al. Multiparametric immune profiling in HPV– oral squamous cell cancer. JCI Insight 2017, 2. [Google Scholar] [CrossRef]
- Foy, J.P.; Bertolus, C.; Michallet, M.C.; Deneuve, S.; Incitti, R.; Bendriss-Vermare, N.; Albaret, M.A.; Ortiz-Cuaran, S.; Thomas, E.; Colombe, A.; et al. The immune microenvironment of HPV-negative oral squamous cell carcinoma from never-smokers and never-drinkers patients suggests higher clinical benefit of IDO1 and PD1/PD-L1 blockade. Ann. Oncol. 2017, 28, 1934–1941. [Google Scholar] [CrossRef] [PubMed]
- Groeger, S.; Denter, F.; Lochnit, G.; Schmitz, M.L.; Meyle, J. Porphyromonas gingivalis Cell Wall Components Induce Programmed Death Ligand 1 (PD-L1) Expression on Human Oral Carcinoma Cells by a Receptor-Interacting Protein Kinase 2 (RIP2)-Dependent Mechanism. Infect. Immun. 2020, 88, e00051-20. [Google Scholar] [CrossRef]
- Hirai, M.; Kitahara, H.; Kobayashi, Y.; Kato, K.; Bou-Gharios, G.; Nakamura, H.; Kawashiri, S. Regulation of PD-L1 expression in a high-grade invasive human oral squamous cell carcinoma microenvironment. Int. J. Oncol. 2017, 50, 41–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kogashiwa, Y.; Yasuda, M.; Sakurai, H.; Nakahira, M.; Sano, Y.; Gonda, K.; Ikeda, T.; Inoue, H.; Kuba, K.; Oba, S.; et al. PD-L1 Expression Confers Better Prognosis in Locally Advanced Oral Squamous Cell Carcinoma. Anticancer Res. 2017, 37, 1417–1424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kubota, K.; Moriyama, M.; Furukawa, S.; Rafiul, H.A.S.M.; Maruse, Y.; Jinno, T.; Tanaka, A.; Ohta, M.; Ishiguro, N.; Yamauchi, M.; et al. CD163+CD204+ tumor-associated macrophages contribute to T cell regulation via interleukin-10 and PD-L1 production in oral squamous cell carcinoma. Sci. Rep. 2017, 7, 1755. [Google Scholar] [CrossRef] [PubMed]
- Mattox, A.K.; Lee, J.; Westra, W.H.; Pierce, R.H.; Ghossein, R.; Faquin, W.C.; Diefenbach, T.J.; Morris, L.G.; Lin, D.T.; Wirth, L.J.; et al. PD-1 Expression in Head and Neck Squamous Cell Carcinomas Derives Primarily from Functionally Anergic CD4 + TILs in the Presence of PD-L1 + TAMs. Cancer Res. 2017, 77, 6365–6374. [Google Scholar] [CrossRef] [Green Version]
- Takaura, H.; Domae, S.; Ono, T.; Sasaki, A. The Immunological Impact of Chemotherapy on the Tumor Microenvironment of Oral Squamous Cell Carcinoma. Acta Med. Okayama 2017, 71, 219–226. [Google Scholar] [CrossRef]
- Troeltzsch, M.; Woodlock, T.; Pianka, A.; Otto, S.; Troeltzsch, M.; Ehrenfeld, M.; Knösel, T. Is There Evidence for the Presence and Relevance of the PD-1/PD-L1 Pathway in Oral Squamous Cell Carcinoma? Hints from an Immunohistochemical Study. J. Oral Maxillofac. Surg. 2017, 75, 969–977. [Google Scholar] [CrossRef] [PubMed]
- Satgunaseelan, L.; Gupta, R.; Madore, J.; Chia, N.; Lum, T.; Palme, C.E.; Boyer, M.; Scolyer, R.A.; Clark, J.R. Programmed cell death-ligand 1 expression in oral squamous cell carcinoma is associated with an inflammatory phenotype. Pathology 2016, 48, 574–580. [Google Scholar] [CrossRef]
- Straub, M.; Drecoll, E.; Pfarr, N.; Weichert, W.; Langer, R.; Hapfelmeier, A.; Götz, C.; Wolff, K.-D.; Kolk, A.; Specht, K. CD274/PD-L1 gene amplification and PD-L1 protein expression are common events in squamous cell carcinoma of the oral cavity. Oncotarget 2016, 7, 12024–12034. [Google Scholar] [CrossRef] [Green Version]
- Chen, T.C.; Wu, C.T.; Wang, C.P.; Hsu, W.L.; Yang, T.L.; Lou, P.J.; Ko, J.Y.; Chang, Y.L. Associations among pretreatment tumor necrosis and the expression of HIF-1α and PD-L1 in advanced oral squamous cell carcinoma and the prognostic impact thereof. Oral Oncol. 2015, 51, 1004–1010. [Google Scholar] [CrossRef]
- Lin, Y.M.; Sung, W.W.; Hsieh, M.J.; Tsai, S.C.; Lai, H.W.; Yang, S.M.; Shen, K.H.; Chen, M.K.; Lee, H.; Yeh, K.T.; et al. High PD-L1 Expression Correlates with Metastasis and Poor Prognosis in Oral Squamous Cell Carcinoma. PLoS ONE 2015, 10, e0142656. [Google Scholar] [CrossRef] [Green Version]
- Oliveira-Costa, J.P.; de Carvalho, A.F.; da Silveira, G.G.; Amaya, P.; Wu, Y.; Park, K.-J.J.; Gigliola, M.P.; Lustberg, M.; Buim, M.E.C.; Ferreira, E.N.; et al. Gene expression patterns through oral squamous cell carcinoma development: PD-L1 expression in primary tumor and circulating tumor cells. Oncotarget 2015, 6, 20902–20920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, Y.A.; Yoon, H.J.; Lee, J.I.; Hong, S.P.; Hong, S.D. Relationship between the expressions of PD-L1 and tumor-infiltrating lymphocytes in oral squamous cell carcinoma. Oral Oncol. 2011, 47, 1148–1153. [Google Scholar] [CrossRef]
- Malaspina, T.S.; Gasparoto, T.H.; Costa, M.R.; de Melo, E.F., Jr.; Ikoma, M.R.; Damante, J.H.; Cavassani, K.A.; Garlet, G.P.; da Silva, J.S.; Campanelli, A.P. Enhanced programmed death 1 (PD-1) and PD-1 ligand (PD-L1) expression in patients with actinic cheilitis and oral squamous cell carcinoma. Cancer. Immunol. Immunother. 2011, 60, 965–974. [Google Scholar] [CrossRef] [PubMed]
- Strati, A.; Koutsodontis, G.; Papaxoinis, G.; Angelidis, I.; Zavridou, M.; Economopoulou, P.; Kotsantis, I.; Avgeris, M.; Mazel, M.; Perisanidis, C.; et al. Prognostic significance of PD-L1 expression on circulating tumor cells in patients with head and neck squamous cell carcinoma. Ann. Oncol. 2017, 28, 1923–1933. [Google Scholar] [CrossRef]
- Green, V.L.; Michno, A.; Stafford, N.D.; Greenman, J. Increased prevalence of tumour infiltrating immune cells in oropharyngeal tumours in comparison to other subsites: Relationship to peripheral immunity. Cancer Immunol. Immunother. 2013, 62, 863–873. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.; Zhang, C.; Ohno, T.; Azuma, M. Unique B7-H1 expression on masticatory mucosae in the oral cavity and trans-coinhibition by B7-H1-expressing keratinocytes regulating CD4+ T cell-mediated mucosal tissue inflammation. Mucosal Immunol. 2017, 10, 650–660. [Google Scholar] [CrossRef] [PubMed]
- Chattopadhyay, I.; Verma, M.; Panda, M. Role of Oral Microbiome Signatures in Diagnosis and Prognosis of Oral Cancer. Technol. Cancer Res. Treat. 2019, 18, 153303381986735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, H.; Chu, M.; Huang, Z.; Yang, X.; Ran, S.; Hu, B.; Zhang, C.; Liang, J. Variations in oral microbiota associated with oral cancer. Sci. Rep. 2017, 7, 11773. [Google Scholar] [CrossRef]
- Cillo, A.R.; Kürten, C.H.L.; Tabib, T.; Qi, Z.; Onkar, S.; Wang, T.; Liu, A.; Duvvuri, U.; Kim, S.; Soose, R.J.; et al. Immune Landscape of Viral- and Carcinogen-Driven Head and Neck Cancer. Immunity 2020, 52, 183–199.e9. [Google Scholar] [CrossRef]
- Wolf, G.T.; Chepeha, D.B.; Bellile, E.; Nguyen, A.; Thomas, D.; McHugh, J. Tumor infiltrating lymphocytes (TIL) and prognosis in oral cavity squamous carcinoma: A preliminary study. Oral Oncol. 2015, 51, 90–95. [Google Scholar] [CrossRef] [Green Version]
- Vassilakopoulou, M.; Avgeris, M.; Velcheti, V.; Kotoula, V.; Rampias, T.; Chatzopoulos, K.; Perisanidis, C.; Kontos, C.K.; Giotakis, A.I.; Scorilas, A.; et al. Evaluation of PD-L1 Expression and Associated Tumor-Infiltrating Lymphocytes in Laryngeal Squamous Cell Carcinoma. Clin. Cancer Res. 2016, 22, 704–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gavrielatou, N.; Doumas, S.; Economopoulou, P.; Foukas, P.G.; Psyrri, A. Biomarkers for immunotherapy response in head and neck cancer. Cancer Treat. Rev. 2020, 84, 101977. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Case Number n (%) | PD-L1 on TCs | PD-L1 on TILs | ||||
|---|---|---|---|---|---|---|---|
| Low n (%) | High n (%) | p | Low n (%) | High n (%) | p | ||
| Gender | |||||||
| Female | 32 (33.68) | 16 (16.84) | 16 (16.84) | 0.607 | 20 (21.05) | 12 (12.63) | 0.292 |
| Male | 63 (66.32) | 35 (36.84) | 28 (29.47) | 46 (48.42) | 17 (17.89) | ||
| Smoking | |||||||
| No | 22 (30.14) | 11 (15.07) | 11 (15.07) | 0.939 | 15 (20.55) | 7 (10.27) | 0.548 |
| Yes | 51 (69.86) | 26 (35.62) | 25 (34.25) | 31 (42.47) | 20 (27.40) | ||
| Alcohol | |||||||
| No | 58 (80.56) | 29 (40.28) | 29 (40.28) | 1.000 | 35 (48.61) | 23 (31.94) | 0.415 |
| Yes | 14 (19.44) | 7 (9.72) | 7 (9.72) | 10 (13.70) | 4 (5.56) | ||
| Grade | |||||||
| 1 | 39 (42.05) | 22 (23.16) | 17 (17.89) | 0.656 | 26 (27.37) | 13 (13.68) | 0.620 |
| 2–3 | 56 (58.95) | 29 (30.53) | 27 (28.42) | 40 (42.11) | 16 (16.84) | ||
| Stage | |||||||
| I–II | 32 (42.67) | 17 (22.08) | 15 (15.79) | 0.832 | 14 (18.18) | 18 (18.18) | 0.004 * |
| III–IV | 45 (57.33) | 25 (32.47) | 20 (25.97) | 34 (44.16) | 11 (14.29) | ||
| T | |||||||
| 1–2 | 42 (55.26) | 23 (30.26) | 18 (23.68) | 0.874 | 23 (30.26) | 19 (25.00) | 0.157 |
| 3–4 | 34 (44.74) | 18 (23.68) | 16 (21.05) | 24 (31.58) | 10 (10.53) | ||
| N | |||||||
| 0 | 39 (52.70) | 17 (22.97) | 22 (29.73) | 0.097 | 18 (24.32) | 21 (28.38) | 0.006 * |
| 1–3 | 35 (47.30) | 22 (29.73) | 13 (17.57) | 27 (36.49) | 8 (10.81) | ||
| Location | |||||||
| Tongue/ Floor of the oral cavity | 55 (57.89) | 35 (36.84) | 20 (21.05) | 0.022 * | 37 (38.95) | 18 (18.95) | 0.584 |
| Other | 40 (42.11) | 16 (16.84) | 24 (25.26) | 29 (30.53) | 11 (11.58) | ||
| Feature | Univariate Cox’s Proportional Hazard Analysis | Multivariate Cox Regression Model | ||
|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | |
| Gender (Male vs. Female) | 1.026 (0.626–1.681) | 0.919 | ||
| Smoking (No vs. Yes) | 0.738 (0.392–1.389) | 0.347 | ||
| Alcohol (No vs. Yes) | 1.001 (0.485–2.065) | 0.997 | ||
| Location (Tongue/floor of the oral cavity vs. other) | 0.957 (0.596–1.537) | 0.855 | ||
| Grade (2–3 vs. 1) | 1.767 (1.074–2.906) | 0.025 * | ||
| Stage (1–2 vs. 3–4) | 0.333 (0.185–0.598) | <0.001 * | ||
| T (1–2 vs. 3–4) | 0.383 (0.221–0.664) | <0.001 * | ||
| N (0 vs. 1–3) | 0.343 (0.196–0.600) | <0.001 * | 0.345 (0.193–0.617) | <0.001 |
| PD-L1 TCs (high vs. low) | 0.991 (0.618–1.589) | 0.971 | ||
| PD-L1 TILs (high vs. low) | 0.525 (0.306–0.902) | 0.012 * | ||
| IL-33 TCs (positive vs. negative) | 0.837 (0.428–1.637) | 0.603 | ||
| IL-33 TILs (positive vs. negative) | 1.036 (0.566–1.894) | 0.909 | ||
| Multivariate Cox Regression Model | ||
|---|---|---|
| Feature | HR (95% CI) | p |
| Tongue/Floor of the oral cavity | ||
| T (1–2 vs. 3–4) | 0.229 (0.101–0.518) | <0.001 * |
| PD-L1 TCs (high vs. low) | 2.514 (1.977–5.282) | 0.014 * |
| Other locations | ||
| N (0 vs. 1–3) | 0.239 (0.081–0.699) | 0.008 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adamski, Ł.J.; Starzyńska, A.; Adamska, P.; Kunc, M.; Sakowicz-Burkiewicz, M.; Marvaso, G.; Alterio, D.; Korwat, A.; Jereczek-Fossa, B.A.; Pęksa, R. High PD-L1 Expression on Tumor Cells Indicates Worse Overall Survival in Advanced Oral Squamous Cell Carcinomas of the Tongue and the Floor of the Mouth but Not in Other Oral Compartments. Biomedicines 2021, 9, 1132. https://doi.org/10.3390/biomedicines9091132
Adamski ŁJ, Starzyńska A, Adamska P, Kunc M, Sakowicz-Burkiewicz M, Marvaso G, Alterio D, Korwat A, Jereczek-Fossa BA, Pęksa R. High PD-L1 Expression on Tumor Cells Indicates Worse Overall Survival in Advanced Oral Squamous Cell Carcinomas of the Tongue and the Floor of the Mouth but Not in Other Oral Compartments. Biomedicines. 2021; 9(9):1132. https://doi.org/10.3390/biomedicines9091132
Chicago/Turabian StyleAdamski, Łukasz Jan, Anna Starzyńska, Paulina Adamska, Michał Kunc, Monika Sakowicz-Burkiewicz, Giulia Marvaso, Daniela Alterio, Aleksandra Korwat, Barbara Alicja Jereczek-Fossa, and Rafał Pęksa. 2021. "High PD-L1 Expression on Tumor Cells Indicates Worse Overall Survival in Advanced Oral Squamous Cell Carcinomas of the Tongue and the Floor of the Mouth but Not in Other Oral Compartments" Biomedicines 9, no. 9: 1132. https://doi.org/10.3390/biomedicines9091132
APA StyleAdamski, Ł. J., Starzyńska, A., Adamska, P., Kunc, M., Sakowicz-Burkiewicz, M., Marvaso, G., Alterio, D., Korwat, A., Jereczek-Fossa, B. A., & Pęksa, R. (2021). High PD-L1 Expression on Tumor Cells Indicates Worse Overall Survival in Advanced Oral Squamous Cell Carcinomas of the Tongue and the Floor of the Mouth but Not in Other Oral Compartments. Biomedicines, 9(9), 1132. https://doi.org/10.3390/biomedicines9091132