
Systematic Review of Alexithymia in the Population of Hemodialysis Patients


Abstract
:1. Introduction
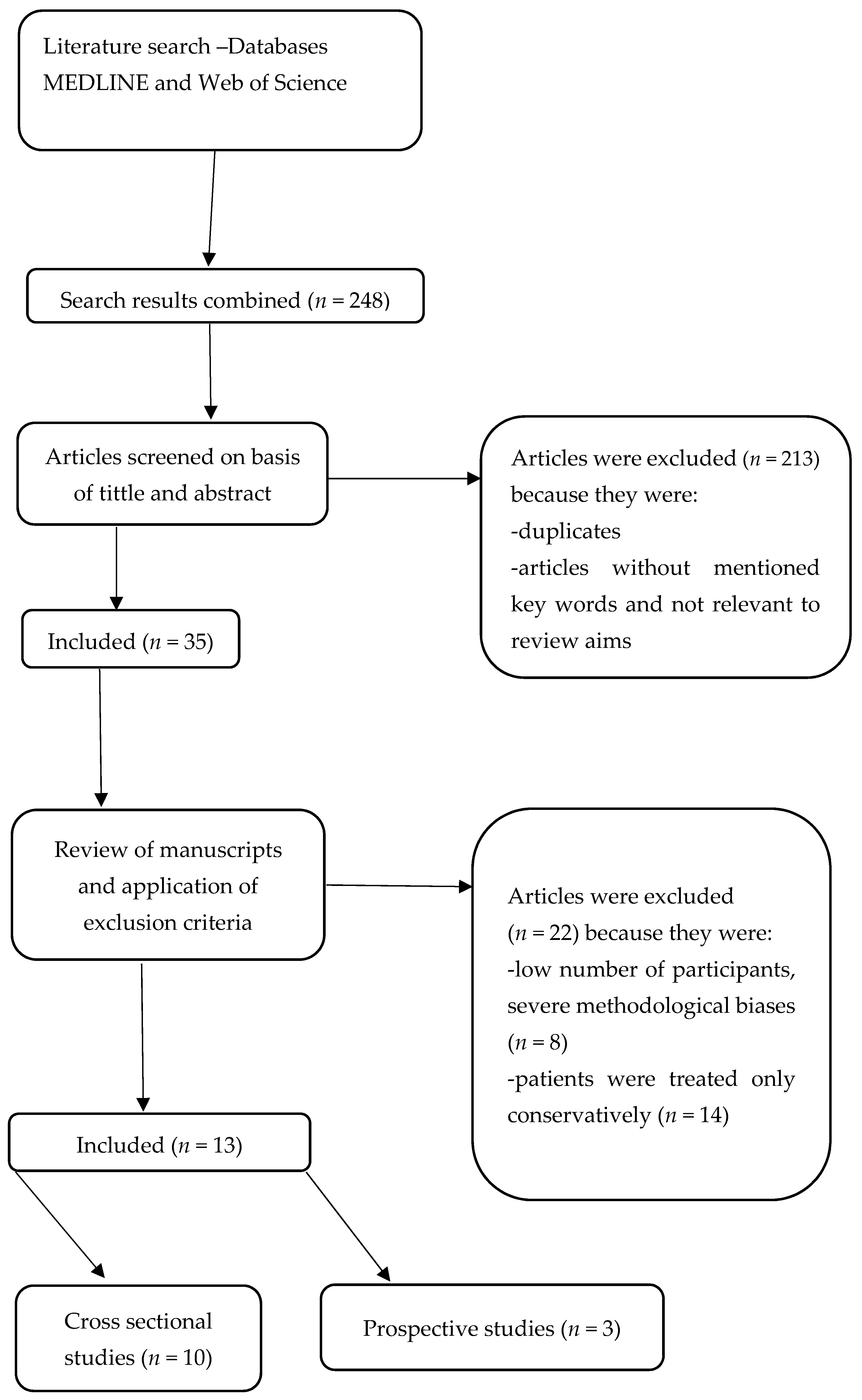
2. Materials and Methods
3. Results
3.1. Prevalence of Alexithymia in the Population of HD Patients
3.2. Correlation between Alexithymia, Laboratory Values and Comorbidities in HD Patients
3.3. Alexithymia and HD Patients’ Mental Health
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rocco, M.; Daugirdas, J.T.; Depner, T.A.; Inrig, J.; Mehrotra, R.; Rocco, M.V.; Suri, R.S.; Weiner, D.E.; Greer, N.; Ishani, A.; et al. KDOQI Clinical practice guideline for hemodialysis adequacy: 2015 Update. Am. J. Kidney Dis. 2015, 66, 884–930. [Google Scholar] [CrossRef] [Green Version]
- Steinwandel, U.; Gibson, N.P.; Rippey, J.C.; Towell, A.; Rosman, J. Use of ultrasound by registered nurses—A systematic literature review. J. Ren. Care 2017, 43, 132–142. [Google Scholar] [CrossRef] [Green Version]
- Fukunishi, I.; Saito, S.; Ozaki, S. The influence of defense mechanisms on secondary alexithymia on hemodilyzed patients. Psychother. Psychosom. 1992, 57, 50–56. [Google Scholar] [CrossRef]
- Besharat, M.A.; Shahidi, S. What is the relationship between alexithymia and ego defense styles? A correlational study with Iranian students. Asian J. Psychiatr. 2011, 4, 145–149. [Google Scholar] [CrossRef]
- Basta, F.; Paolo, D.; Margiotta, E.; Mazzuca, C.; Batani, V.; Dolcini, G.; Moras, P.; Vadacca, M.; Afeltra, A. Factors related to alexithymia in patients with systemic sclerosis: A tight relationship with facial image dissatisfaction. Rheumatol. Int. 2018, 39, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Lumley, M.A.; Neely, L.C.; Burger, A.J. The Assessment of Alexithymia in Medical Settings: Implications for Understanding and Treating Health Problems. J. Pers. 2010, 89, 230–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kojima, M.; Hayano, J.; Suzuki, S.; Seno, H.; Kasuga, H.; Takahashi, H.; Toriyama, T.; Kawahara, H.; Furukawa, T.A. Depression, alexithymia and long-term mortality in chronic hemodialysis patients. Psyhother. Psychosom. 2010, 79, 303–311. [Google Scholar] [CrossRef]
- Donges, U.; Suslow, T. Alexithymia and automatic processing of emotional stimuli: A systematic review. Rev. Neurosci. 2017, 28, 1–18. [Google Scholar] [CrossRef]
- Fukunishi, I. Psychosomatic aspects of patients on hemodialysis 1. With special reference to aged patients. Psychother. Psychosom. 1989, 52, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Larsen, J.K.; Van Strien, T.; Eisinga, R.; Engels, R.C.M.E. Gender differences in the association between alexithymia and emotional eating in obese individuals. J. Psychosom. Res. 2006, 60, 237–243. [Google Scholar] [CrossRef] [Green Version]
- Helmers, K.F.; Mente, A. Alexithyimia and health behaviors in healthy male volunteers. J. Psychosom. Res. 1999, 47, 635–645. [Google Scholar] [CrossRef]
- Cozzolino, M.; Mangano, M.; Stucchi, A.; Ciceri, P.; Conte, F.; Galassi, A. Cardiovascular disease in dialysis patients. Nephrol. Dial. Transplant. 2018, 33, 28–34. [Google Scholar] [CrossRef]
- Carvalho, A.F.; Ramírez, S.P.; Macedo, D.S.; Sales, P.M.G.; Rebouças, J.C.; Daher, E.F.; Hyphantis, T.N. The psychological defensive profile of hemodialysis patients and its relationship to health-related quality of life. J. Nerv. Ment. Dis. 2013, 201, 621–628. [Google Scholar] [CrossRef]
- Helmes, E.; Mcneill, P.D.; Holden, R.R.; Jackson, C. The construct of alexithymia: Associations with defense mechanisms. J. Clin. Psychol. 2008, 64, 318–331. [Google Scholar] [CrossRef] [PubMed]
- Goldman, K.D.; Schmalz, K.J. The Matrix Method of literature reviews. Health Promot. Pract. 2004, 5, 5–7. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.; Godfrey, C.; McInerney, P.; Soares, C.; Khalil, H.; Parker, D. The Joanna Briggs Institute Reviewers’ Manual 2015: Methodology for JBI Scoping Reviews; The Joanna Briggs Institute: Adelaide, Australia, 2015; ISBN 61-249-878-937. [Google Scholar]
- Bagby, R.M.; Taylor, G.J.; Parker, J.D.A. The twenty-item Toronto Alexithymia scale-II. convergent, discriminant, and concurrent validity. J. Psychosom. Res. 1994, 38, 33–40. [Google Scholar] [CrossRef]
- Akyüz, O.; Parmaksiz, E. Investigation of the relationship between biochemical parameters, alexithymia and stress levels in hemodialysis patients. South. Clin. Istanb. Eurasia 2021, 32, 13–18. [Google Scholar] [CrossRef]
- Tayaz, E.; Koç, A. Influence of selected biomarkers on stress and alexithymia in patients under hemodialysis treatment. Yonago Acta Med. 2019, 62, 285–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heisig, M.; Reich, A.; Szepietowski, J.C. Alexithymia in Uraemic Pruritus. Acta Derm. Venereol. 2016, 96, 699–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pop-Jordanova, N.; Polenakovic, M. Alexithymia Construct in Dialysis Patients. Bantao J. 2014, 12, 45–51. [Google Scholar] [CrossRef] [Green Version]
- Sinatra, M.; Curci, A.; Palo, V.D.; Monacis, L. How dialysis patients live: A study on their depression and associated factors in Southern Italy. Psychology 2011, 2, 969–977. [Google Scholar] [CrossRef] [Green Version]
- De Santo, R.M.; Livrea, A.; De Santo, N.G.; Conzo, G.; Bilancio, G.; Celsi, S.; Cirillo, M. The high prevalence of alexithymia in hemodialyzed patients with secondary hyperparathyroidism unsuppressed by medical therapy is cured by parathyroidectomy. J. Ren. Nutr. 2010, 20, 64–70. [Google Scholar] [CrossRef]
- Kojima, M.; Hayano, J.; Tokudome, S.; Suzuki, S. Independent associations of alexithymia and social support with depression in hemodialysis patients. J. Psychosom. Res. 2007, 63, 349–356. [Google Scholar] [CrossRef]
- Oogai, Y.; Ishiburo, M.; Urae, J.; Hisano, T.; Nagura, Y.; Takanashi, S.; Fukunishi, I. Are there overlapping constructs between alexithymia and depression in hemodialysis patients. J. Psychosom. Res. 2003, 55, 172. [Google Scholar] [CrossRef]
- Fukunishi, I. Alexithymic characteristics of bulimia nervosa in diabetes mellitus with end-stage renal disease. Psychol. Rep. 1997, 81, 627–633. [Google Scholar] [CrossRef]
- Fukunishi, I. Psychological problems of kidney transplantation: Satisfaction with dialysis therapy and desire for transplantation in hemodialysis patients. Nephron 1993, 64, 146–149. [Google Scholar] [CrossRef]
- Fukunishi, I. Psychosomatic problems surrounding kidney transplantation. Psychother. Psychosom. 1992, 57, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Salminen, J.K.; Saarija, S.; Rela, E.A.A. Prevalence of alexithymia and its association with sociodemographic variables in the general population of Finland. J. Psychosom. Res. 1999, 46, 75–82. [Google Scholar] [CrossRef]
- Onor, M.; Trevisiol, M.; Spano, M.; Aguglia, E.; Paradiso, S. Alexithymia and aging: A neuropsychological perspective. J. Nerv. Ment. Dis. 2013, 198, 891–895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kauhanen, J.; Wilson, T.W.; Salonen, J.T.; Kaplan, G.A.; Julkunen, J. Social factors in alexithymia. Compr. Psychiatry 1993, 34, 330–335. [Google Scholar] [CrossRef]
- Lumley, M.A.; Norman, S. Alexithymia and health care utilization. Psychosom. Med. 1996, 58, 197–202. [Google Scholar] [CrossRef]
- Carrozzino, D.; Porcelli, P. Alexithymia in gastroenterology and hepatology: A systematic review. Front. Psychol. 2018, 9, 470–493. [Google Scholar] [CrossRef] [Green Version]
- Pinna, F. Alexithymia in eating disorders: Therapeutic implications. Psychol. Res. Behav. Manag. 2015, 8, 1–15. [Google Scholar]
- Laudanski, K. Denial defense mechanism in dialyzed patients. Med. Sci. Monit. 2015, 21, 1798–1805. [Google Scholar] [CrossRef] [Green Version]
- Lumley, M.A. How are alexithymia and physical illness linked? A review and critique of pathways. J. Psychosom. Res. 1996, 41, 505–518. [Google Scholar] [CrossRef]
- Kusević, Z.; Marusić, K. The relationship between alexithymia and morbidity. Lijec. Vjesn. 2014, 136, 44–48. [Google Scholar] [PubMed]
- Tella, M.D.; Castelli, L. Alexithymia in Chronic Pain Disorders. Curr. Rheumatol. Rep. 2016, 18, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kojima, M.; Senda, Y.; Nagaya, T.; Tokudome, S.; Furukawa, T.A. Alexithymia, depression and social support among Japanese workers. Psychother. Psychosom. 2003, 72, 307–314. [Google Scholar] [CrossRef]
- Thorberg, F.A.; Young, R.M.D.; Hasking, P.; Lyvers, M.; Connor, J.P.; London, E.D.; Huang, Y.L.; Feeney, G.F.X. Alexithymia and alcohol dependence: The roles of negative mood and alcohol craving. Subst. Use Misuse 2019, 54, 2380–2386. [Google Scholar] [CrossRef]
- Casagrande, M.; Boncompagni, I.; Forte, G.; Guarino, A.; Favieri, F. Emotion and overeating behavior: Effects of alexithymia and emotional regulation on overweight and obesity. Eat. Weight Disord. 2019, 54, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Koh, K.B.; Cho, S.Y.; Kim, J.W.; Rho, K.S.; Lee, S.H.; Park, I.H. The relationship of anger expression and alexithymia with coronary artery stenosis in patients with coronary artery diseases. Yonsei Med. J. 2004, 45, 181–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinna, F.; Manchia, M.; Paribello, P. The impact of alexithymia on treatment response in psychiatric disorders: A systematic review. Front. Psychiatry 2020, 11, 311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beresnevaite, M. Exploring the benefits of group psychotherapy in reducing alexithymia in coronary heart disease patients: A preliminary study. Psychother. Psychosom. 2000, 69, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Kojima, M. Epidemiologic studies of psychosocial factors associated with quality of life among patients with chronic diseases in Japan. J. Epidemiol. 2012, 22, 7–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Author (Year) | Aims of the Study | Study Design/Methods | Number of Patients (HD) | Strenghts | Limits |
|---|---|---|---|---|---|
| Akyüz, O. et al. (2021); [18] | Investigation of the relationship between biochemical variables, alexithymia and stress levels. | CSD; TAS 20 | 51 | The sample of patients correctly represents population of HD patients in relation to age and comorbidities | Single center study with a small patient sample; there was retrospective insight in biochemical values |
| Tayaz E. (2019); [19] | Association of alexithymia with laboratory values in HD patients. | CSD; TAS 20 | 72 | Single center study | CSD, small number of participants, single measurement of laboratory values. |
| Heisig M. et al. (2016); [20] | Comparison of levels of alexithymia in HD patients with and without uraemic pruritus. | CSD; BVAQ | 42 of 90 patients had pruritus | Multicentric study | CSD |
| Pop Jordanova et al. (2014); [21] | Evaluating the effects of age, duration of dialysis and gender on levels of alexithymia in HD patients. | CSD; TAS 20 | 230 HD patients | Multicentric study, large sample of patients | |
| Sinatra M. et al. (2011); [22] | Comparison of depression, alexithymia, social support and quality of life between HD patients dialyzed for less than 4 years and those dialyzed for more than 4 years. | CSD; TAS 20 | 103 HD patients, 101 patient in control group | CSD, self-reported questionnaires and relatively old participants | |
| De Santo et al. (2010); [23] | Comparison of alexithymia levels in HD patients requiring parathyroidectomy (PTX) and those not requiring PTX at baseline and 24 months following PTX. | PD; TAS 20 | 40 HD patients needing PTX, 80 HD patients not needing PTX | Prospective design of a study enables establishment of causality | |
| Kojima M. et al. (2010); [7] | Analyzing the effect of alexithymia, depression and laboratory values on five-year mortality among HD patients. | PMD; TAS 20 | 230 HD patients | Prospective study; Comorbidities and laboratory values at the baseline and excludes confounders | Self-reported scales; small sample size for Cox regression analysis |
| Kojima M. et al. (2007); [24] | Assesing the effect of baseline alexithymia, depression and percieved social support on deterioration of depression after a 6-months follow up period in HD patients. | PMD; TAS 20 | 229 HD patients | PMD | Self-reported questionnaires, depression is defined through result of BDI-II questionnaire, sample is grouped in small area of city |
| Oogai Y. et al. (2003); [25] | Examination of overlapping of alexithymia and depression constructs in HD patients. | CSD; TAS 20, CES-D | 507 HD patients | Multicentric study, includes a large number of participants | |
| Fukunishi I. (1997); [26] | Comparison of prevalence of alexithymia in HD patients in terms of etiology of ESRD and presence of bulimia nervosa. | CSD; TAS 20 | 312 HD patients (130 in diabetic group), 16 patients had bulimia nervosa | High number of patients in each group enables good statistical strength | Single center study |
| Fukunishi I. (1993); [27] | Determining the effect of alexithymia on satisfaction with HD, sense of purpose in life and desire for kidney transplantation. | CSD; BIQ | 191 HD patient younger of 59 years and 84 patients who are 60 years old or older | Large number of patients | Single center study and cross-sectional design |
| Fukunishi I. et al. (1992); [3] | Comparing alexithymic HD patients and their family members to those without alexithymia on family environment subscales. | CSD; BIQ, TAS 20 | 35 HD patients and 35 of their family members | A single center study with a small number of participants and cross-sectional design does not allow establishment of causality | |
| Fukunishi I. (1989); [9] | Comparing the levels of alexithymia in patients over 65 on long term HD (S1 group) and HD patients 65 who just started hemodialysis (S2 group) | CSD; BIQ | 50 HD patients in S1 group and S2 group, control groups (C1-Hd patients younger than 65 years, C2 groups) with 50 patients each | There is no causality, because of a small number of patients in S1 group stratified by comorbidities, leading to a high possibility of a type 2 statistical error |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pojatić, Đ.; Tolj, I.; Pezerović, D.; Degmečić, D. Systematic Review of Alexithymia in the Population of Hemodialysis Patients. J. Clin. Med. 2021, 10, 2862. https://doi.org/10.3390/jcm10132862
Pojatić Đ, Tolj I, Pezerović D, Degmečić D. Systematic Review of Alexithymia in the Population of Hemodialysis Patients. Journal of Clinical Medicine. 2021; 10(13):2862. https://doi.org/10.3390/jcm10132862
Chicago/Turabian StylePojatić, Đorđe, Ivana Tolj, Davorin Pezerović, and Dunja Degmečić. 2021. "Systematic Review of Alexithymia in the Population of Hemodialysis Patients" Journal of Clinical Medicine 10, no. 13: 2862. https://doi.org/10.3390/jcm10132862
APA StylePojatić, Đ., Tolj, I., Pezerović, D., & Degmečić, D. (2021). Systematic Review of Alexithymia in the Population of Hemodialysis Patients. Journal of Clinical Medicine, 10(13), 2862. https://doi.org/10.3390/jcm10132862