
Effectiveness of a Long-Term Training Programme for Teachers in Attention-Deficit/Hyperactivity Disorder on Knowledge and Self-Efficacy

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample of Children
2.2. Sample of Teachers
2.3. Measurements
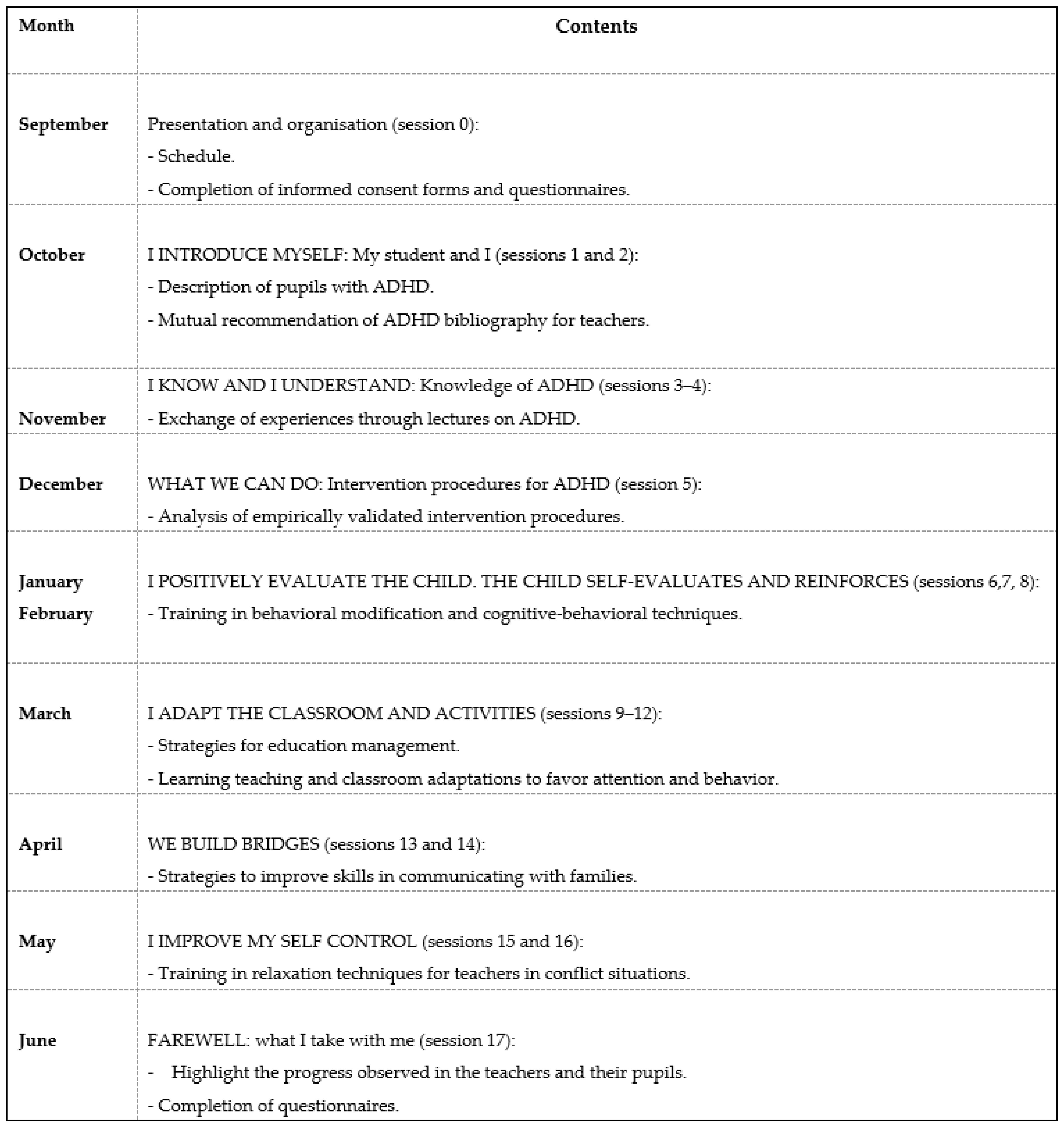
2.4. Procedure
2.5. Statistical Analysis
3. Results
3.1. Knowledge and Perceived Self-Efficacy
3.1.1. Control Group
3.1.2. Multimodal Intervention Group
3.1.3. Comparison Between Both Groups
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Psychiatric Association (APA). Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013; pp. 31–87. [Google Scholar]
- Cabral, M.; Liu, S.; Soares, N. Attention-deficit/hyperactivity disorder: Diagnostic criteria, epidemiology, risk factors and evaluation in youth. Transl. Pediatr. 2020, 9 (Suppl. 1), S104–S113. [Google Scholar] [CrossRef]
- Thapar, A.; Cooper, M. Attention deficit hyperactivity disorder. Lancet 2016, 387, 1240–1250. [Google Scholar] [CrossRef]
- Sexton, C.C.; Gelhorn, H.L.; Bell, J.A.; Classi, P.M. The co-occurrence of reading disorder and ADHD: Epidemiology, treatment, psychosocial impact, and economic burden. J. Learn. Disabil. 2012, 45, 538–564. [Google Scholar] [CrossRef]
- von Wirth, E.; Kujath, K.; Ostrowski, L.; Settegast, E.; Rosarius, S.; Döpfner, M.; Schwenk, C.; Kuhn, J.T. The co-occurrence of Attention-Deficit/Hyperactivity Disorder and mathematical difficulties: An investigation of the role of basic numerical skills. Res. Dev. Disabil. 2021, 112, 103881. [Google Scholar] [CrossRef]
- Tosto, M.G.; Momi, S.K.; Asherson, P.; Malki, K. A systematic review of attention deficit hyperactivity disorder (ADHD) and mathematical ability: Current findings and future implications. BMC Med. 2015, 13, 1–14. [Google Scholar] [CrossRef]
- Faraone, S.V.; Banaschewski, T.; Coghill, D.; Zheng, Y.; Biederman, J.; Bellgrove, M.A.; Newcorn, J.H.; Gignac, M.; Al Saud, N.M.; Wang, Y.; et al. The world federation of ADHD international consensus statement: 208 evidence-based conclusions about the disorder. Neurosci. Biobehav. Rev. 2021, in press. [Google Scholar] [CrossRef]
- Polanczyk, G.; De Lima, M.S.; Horta, B.L.; Biederman, J.; Rohde, L.A. The worldwide prevalence of ADHD: A systematic review and metaregression analysis. Am. J. Psychiatry 2007, 164, 942–948. [Google Scholar] [CrossRef] [PubMed]
- Polanczyk, G.V.; Willcutt, E.G.; Salum, G.A.; Kieling, C.; Rohde, L.A. ADHD prevalence estimates across three decades: An updated systematic review and meta-regression analysis. Int. J. Epidemiol. 2014, 43, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Getahun, D.; Jacobsen, S.J.; Fasset, M.J. Recent trends in childhood Attention-Deficit/Hyperactivity Disorder. JAMA Pediatr. 2013, 167, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Criado-Álvarez, J.J.; Romo-Barrientos, C. Variabilidad y tendencias en el consumo de metilfenidato en España. Estimación de la prevalencia del trastorno por déficit de atención con hiperactividad. Rev. Neurol. 2003, 37, 806–810. [Google Scholar] [CrossRef] [PubMed]
- Fayyad, J.; Sampson, N.A.; Hwang, I.; Adamowski, T.; Aguilar-Gaxiola, S.; Al-Hamzawi, A.; Andrade, L.H.S.G.; Borges, G.; de Girolamo, G.; WHO World Mental Health Survey Collaborators; et al. The descriptive epidemiology of DSM-IV adult ADHD in the world health organization world mental health surveys. ADHD Atten. Deficit Hyperact. Disord. 2017, 9, 47–65. [Google Scholar] [CrossRef]
- Catalá-López, F.; Peiró, S.; Ridao, M.; Sanfélix-Gimeno, G.; Gènova-Maleras, R.; Catalá, M.A. Prevalence of attention deficit hyperactivity disorder among children and adolescents in Spain: A systematic review and meta-analysis of epidemiological studies. BMC Psychiatry 2012, 12, 168–181. [Google Scholar] [CrossRef] [PubMed]
- Canals, J.; Morales-Hidalgo, P.; Jané, M.C.; Domènech, E. ADHD prevalence in Spanish Preschoolers: Comorbidity, Socio-demographic Factors, and Functional Consequences. J. Atten. Disord. 2018, 22, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Coghill, D.R.; Seth, S.; Pedroso, S.; Usala, T.; Currie, J.; Gagliano, A. Effects of methylphenidate on cognitive functions in children and adolescents with Attention-Deficit/Hyperactivity Disorder: Evidence from a systematic review and a meta-analysis. Biol. Psychiatry 2013, 76, 603–615. [Google Scholar] [CrossRef] [PubMed]
- Miranda, A.; Presentación, M.J.; Siegenthaler, R.; Jara, P. Effects of a psychosocial intervention on the executive functioning in children with ADHD. J. Learn. Disabil. 2013, 46, 363–376. [Google Scholar] [CrossRef]
- Evans, S.W.; Owens, J.S.; Wymbs, B.T.; Ray, A.R. Evidence-based psychosocial treatments for children and adolescents with attention deficit/hyperactivity disorder. J. Clin. Child Adolesc. Psychol. 2018, 47, 157–198. [Google Scholar] [CrossRef] [PubMed]
- Dahl, V.; Ramakrishnan, A.; Spears, A.P.; Jorge, A.; Lu, J.; Bigio, N.A.; Chacko, A. Psychoeducation interventions for parents and teachers of children and adolescents with ADHD: A systematic review of the literature. J. Dev. Phys. Disabil. 2020, 32, 257–292. [Google Scholar] [CrossRef]
- Döpfner, M.; Ise, E.; Breuer, D.; Rademacher, C.; Metternich-Kaizman, T.W.; Schürmann, S. Long-term course after adaptive multimodal treatment for children with ADHD: An 8-year follow-up. J. Atten. Disord. 2020, 24, 145–162. [Google Scholar] [CrossRef] [PubMed]
- Kos, J.; Richdale, A.L.; Hay, D.A. Children with Attention deficit Hyperactivity Disorder and their Teachers: A review of the literature. Int. J. Disabil. Dev. Educ. 2006, 53, 147–160. [Google Scholar] [CrossRef]
- Jarque, S.; Tárraga, R.; Miranda, A. Conocimientos, concepciones erróneas y lagunas de los maestros sobre el trastorno por déficit de atención con hiperactividad. Psicothema 2007, 19, 585–590. [Google Scholar]
- Ohan, J.L.; Cormier, N.; Hepp, S.L.; Visser, T.A.V.; Strain, M.C. Does Knowledge About Attention-Deficit/Hyperactivity Disorder Impact Teachers’ Reported Behaviors and Perceptions? Sch. Psychol. Q. 2008, 23, 436–449. [Google Scholar] [CrossRef]
- Sherman, J.; Rasmussen, C.; Baydala, L. The impact of teacher factors on achievement and behavioural outcomes of children with attention Deficit/ Hyperactivity disorder (ADHD): A review of the literature. Educ. Res. 2008, 50, 347–360. [Google Scholar] [CrossRef]
- Sciutto, M.J.; Terjesen, M.D.; Kučerová, A.; Michalová, Z.; Schmiedeler, S.; Antonopoulou, K.; Shaker, N.Z.; Lee, J.-Y.; Alkahtani, K.; Drake, B.; et al. Cross-national comparisons of teachers’ knowledge and misconceptions of ADHD. Int. Perspect. Psychol. 2016, 5, 34–50. [Google Scholar] [CrossRef]
- Soroa, M.; Balluerka, N.; Gorostiaga, A. Development and validation of a questionnaire (the IRA-AGHN) to assess teachers’ knowledge of Attention Deficit Hyperactivity Disorder. An. Psicol. 2014, 30, 1035–1043. [Google Scholar] [CrossRef]
- Arnett, A.B.; MacDonald, B.; Pennington, B.F. Cognitive and behavioural indicators of ADHD symptoms prior to school age. J. Child Psychol. Psychiatry 2013, 54, 1284–1294. [Google Scholar] [CrossRef] [PubMed]
- Bekle, B. Knowledge and attitudes about Attention-Deficit Hyperactivity Disorder (ADHD): A comparison between practicing teachers and undergraduate education students. J. Atten. Disord. 2004, 7, 151–161. [Google Scholar] [CrossRef]
- Anderson, D.L.; Watt, S.E.; Noble, W.; Shanley, D.C. Knowledge of Attention Deficit Hyperactivity Disorder (ADHD) and attitudes toward teaching children with ADHD: The role of teaching experience. Psychol. Sch. 2012, 49, 511–525. [Google Scholar] [CrossRef]
- Rogers, M.; Tannock, R. Are Classrooms meeting the basic psychological needs of children with ADHD symptoms? A self-determination theory perspective. J. Atten. Disord. 2018, 22, 1354–1360. [Google Scholar] [CrossRef]
- Toye, M.K.; Wilson, C.; Wardle, G.A. Education professionals’ attitudes towards the inclusion of children with ADHD: The role of knowledge and stigma. J. Res. Spec. Educ. Needs 2019, 19, 184–196. [Google Scholar] [CrossRef]
- Sciutto, M.J.; Terjesen, M.D.; Bender, A.S. Teachers’ knowledge and misperceptions of Attention-Deficit/Hyperactivity Disorder. Psychol. Sch. 2000, 37, 115–122. [Google Scholar] [CrossRef]
- Jarque, S.; Tárraga, R. Comparación de los conocimientos sobre el trastorno por déficit de atención con hiperactividad (TDAH) de los maestros en activo y los futuros educadores. Infanc. Aprendiz. 2009, 32, 517–529. [Google Scholar] [CrossRef]
- Perold, M.; Louw, C.; Kleymhans, S. Primary school teachers’ knowledge and misperceptions of attention deficit hyperactivity disorder (ADHD). S. Afr. J. Educ. 2010, 30, 457–473. [Google Scholar] [CrossRef]
- Alkahtani, K.D.F. Teachers’ Knowledge and Misconceptions of Attention Deficit/Hyperactivity Disorder. Psychology 2013, 4, 963–969. [Google Scholar] [CrossRef]
- Anderson, D.L.; Watt, S.E.; Shanley, D.C. Ambivalent attitudes about teaching children with attention déficit hyperactivity disorder (ADHD). Emot. Behav. Difficulties 2017, 22, 332–349. [Google Scholar] [CrossRef]
- Martinussen, R.; Tannock, R.; Chaban, P. Teachers’ Reported Use of Instructional and Behavior Management Practices for Students with Behavior. Child Youth Care Forum 2011, 40, 143–210. [Google Scholar] [CrossRef]
- Soroa, M.; Gorostiaga, A.; Balluerka, N. Conocimiento de los docentes sobre el TDAH: Relevancia de la formación y de las percepciones individuales. Rev. Psicodidáctica 2016, 21, 205–226. [Google Scholar] [CrossRef]
- Strelow, A.E.; Dort, M.; Schwinger, M.; Christiansen, H. Influences on Teachers’ Intention to Apply Classroom Management Strategies for Students with ADHD: A Model Analysis. Sustainability 2021, 13, 2558. [Google Scholar] [CrossRef]
- Lawrence, K.; Estrada, R.D.; McCormick, J. Teachers´ experiences with and perceptions of students with attention déficit/hyperactivity disorder. J. Pediatric Nurs. 2018, 36, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Snider, V.E.; Busch, T.; Arrowood, L. Teacher Knowledge of Stimulant Medication and ADHD. Remedial Spec. Educ. 2003, 24, 46–56. [Google Scholar] [CrossRef]
- Ramos, N. Hispanic Teachers’ Perceptions of Children with ADHD. Ph.D. Thesis, University of Texas Pan-American, Edinburgh, TX, USA, 2008. [Google Scholar]
- Youssef, M.K.; Hutchinson, G.; Youssef, F.F. Knowledge of and Attitudes Toward ADHD among Teachers: Insights from a Caribbean Nation. SAGE Open 2015, 5, 1–8. [Google Scholar] [CrossRef]
- Shroff, H.P.; Hardikar-Sawant, S.; Prabhudesai, A.D. Knowledge and misperceptions about Attention Deficit Hyperactivity Disorder (ADHD) among school teachers in Mumbai, India. Int. J. Disabil. Dev. Educ. 2017, 64, 514–525. [Google Scholar] [CrossRef]
- Miranda Padilla, A.; Barrios Cuartas, D.; Duque Henao, L.F.; Burgos Arroyo, E.A.; Salazar Flórez, J.E. Knowledge About ADHD in Primary Teachers of Public Schools of Sabaneta, Antioquia. Rev. Colomb. Psiquiatr. 2018, 47, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Soriano-Ferrer, M.; Echegaray-Bengoa, J. Incidencia de la experiencia docente con el TDAH en los conocimientos, la autoeficacia y los niveles de estrés docente. Univ. Psychol. 2019, 18, 1–13. [Google Scholar] [CrossRef]
- Stacey, M.A. Attention-Deficit/Hyperactivity Disorder: General Education Elementary School Teachers’ Knowledge, Training, and Ratings of Acceptability of Interventions. Ph.D. Thesis, University of South Florida, Tampa, FL, USA, 2003. [Google Scholar]
- Guerra, F.R. Teacher Knowledge of Attention Deficit Hyperactivity Disorder among Middle School Students in South Texas. Ph.D. Thesis, University of Texas, Austin, TX, USA, 2009. Available online: http://gradworks.umi.com/34/00/3400334.html (accessed on 8 April 2021).
- Kos, J.M.; Richdale, A.L.; Jackson, M.S. Knowledge about Attention-Deficit/Hyperactivity Disorder: A comparison of in-service and preservice teachers. Psychol. Sch. 2004, 41, 517–526. [Google Scholar] [CrossRef]
- Niznik, M.E. An Exploratory Study of the Implementation and Teacher outcomes of a Program to Train Elementary Educators about ADHD in the Schools. Ph.D. Thesis, University of Texas, Austin, TX, USA, 2004. [Google Scholar]
- Jones, H.A.; Chronis-Tuscano, A. Efficacy of teacher in-service training for Attention-Deficit/Hyperactivity Disorder. Psychol. Sch. 2008, 45, 918–929. [Google Scholar] [CrossRef]
- Syed, E.U.; Hussein, A.S. Increase in teachers’ knowledge about ADHD Increase in teachers’ Knowledge about ADHD after a week-long training program. J. Atten. Disord. 2010, 13, 420–423. [Google Scholar] [CrossRef] [PubMed]
- Barnet, B.; Corkum, P.; Elik, N. A web-based intervention for elementary school teachers of students with attention-deficit/hyperactivity disorder/ADHD). Psychol. Serv. 2012, 9, 227–230. [Google Scholar] [CrossRef]
- Latouche, A.P.; Gascoigne, M. In-service training for increasing teachers’ ADHD knowledge and self-efficacy. J. Atten. Disord. 2019, 23, 270–281. [Google Scholar] [CrossRef] [PubMed]
- Campbell, D.T.; Stanley, J.C. Experimental and Quasi-Experimental Designs for Research; Ravenio Books: IL, USA, 2015. [Google Scholar]
- Bryman, A. Social Research Methods; OUP Oxford: Oxford, UK, 2016. [Google Scholar]
- Amado, L.; Jarque, S.; Ceccato, R. Differential impact of a multimodal versus pharmacological therapy on the core symptoms of attention deficit/hyperactivity disorder in childhood. Res. Dev. Disabil. 2016, 59, 93–104. [Google Scholar] [CrossRef][Green Version]
- Miranda, A.; Presentación, M.J.; Gargallo, B.; Soriano, M.; Gil, M.D.; Jarque, S. El niño Hiperactivo (TDAH). Intervención en el aula. Un Programa de Formación Para Profesores; Servicio de Publicaciones de la Universidad Jaume I: Castellón, Spain, 1999. [Google Scholar]
- Gargallo, B. Programa de Intervención Educativa Para Aumentar la Atención y la Reflexividad (PIAAR-R); TEA Ediciones: Madrid, Spain, 2000. [Google Scholar]
- Lasisi, D.; Ani, C.; Lasebikan, V.; Sheikh, L.; Omigbodun, O. Effect of attention-deficit–hyperactivity-disorder training program on the knowledge and attitudes of primary school teachers in Kaduna, North West Nigeria. Child Adolesc. Psychiatry Ment. Health 2017, 11, 1–8. [Google Scholar] [CrossRef]
- González Calleros, C.B. Modelo de diseño instruccional para el aprendizaje de matemáticas para estudiantes con TDAH. Ph.D. Thesis, Psychology Degree. Universidad Autónoma de Puebla, Puebla, Mexico, March 2021. [Google Scholar]
- Bandura, A. Social Foundations of Thought and Action: A Social Cognitive Theory; Prentice-Hall: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- Reid, R.; Vasa, S.F.; Magg, J.W.; Wright, G. An Analysis of teachers perceptions of attention deficit disorder. J. Res. Dev. Educ. 1994, 27, 193–202. [Google Scholar]
- Hinshaw, S.P.; Scheffler, R.M.; Fulton, B.D.; Aase, H.; Banaschewski, T.; Cheng, W.; Mattos, P.; Holte, A.; Levy, F.; Sadeh, A.; et al. International variation in treatment procedures for ADHD: Social context and recent trends. Psychiatr. Serv. 2011, 62, 459–464. [Google Scholar] [CrossRef]
- Shehata, A.; Mahrous, E.; Farrag, E.; Hassan, Z. Effectiveness of structured teaching programme on knowledge, attitude, and management strategies among teachers of primary school toward children with attention deficit hyperactivity disorder. IOSR J. Nurs. Health Sci. 2016, 5, 29–37. [Google Scholar]
- Park, S.J.; Park, W.J. Development and effects of an instructional coaching program regarding children with attention deficit hyperactivity disorder for elementary school teachers. J. Korean Acad. Nurs. 2017, 47, 305–318. [Google Scholar] [CrossRef] [PubMed]
- Alabd, A.M.A.; Mesbah, S.K.; Alboliteeh, M. Effect of educational program on elementary school teachers’ knowledge, attitude, and classroom management techniques regards attention deficit hyperactivity disorder. Int. J. Stud. Nurs. 2018, 3, 159–171. [Google Scholar] [CrossRef]
- Khalil, A.I.; Alshareef, F.A.; Alshumrani, H.G. Knowledge, Attitude, and Behavioural Practice of Elementary Teacher of ADHD Children: Impact of an Educational Intervention. Am. J. Nurs. 2019, 8, 330–341. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Control Group | Multimodal Group |
|---|---|---|
| Age | ||
| 7 years | 3 (30%) | 3 (30%) |
| 8 years | 4 (40%) | 4 (40%) |
| 9 years | 3 (30%) | 3 (30%) |
| Mean age | 7.6 | 7.8 |
| Sex | ||
| Male | 8 (80%) | 9 (90%) |
| Female | 2 (20%) | 1 (10%) |
| Characteristics | Control Group | Multimodal Group |
|---|---|---|
| Mean age | 40.3 | 38.4 |
| Sex | ||
| Males | 4 (20%) | 7 (35%) |
| Females | 16 (80%) | 13 (65%) |
| Experience as a teacher (mean) | 23.5 | 19.1 |
| Previous experience with children with Attention-Deficit/Hyperactivity Disorder (ADHD) | 9 (45%) | 12 (60%) |
| Previous attendance of ADHD courses | 0 | 1 (5%) |
| Knowledge | Pre Treatment | Post Treatment | Z | p |
|---|---|---|---|---|
| Total Scale | M 54.6 SD 5.20 | M 53.5 SD 6.04 | −1.080 | 0.280 |
| General Information | M 43.30 SD 9.55 | M 43.96 SD 9.77 | −0.312 | 0.755 |
| Symptoms/ Diagnosis | M 64.38 SD 12.26 | M 63.27 SD 11.44 | −0.933 | 0.351 |
| Treatment | M 56.22 SD 10.77 | M 53.31 SD 9.51 | −1.381 | 0.167 |
| Perceived self-efficacy | M 2.6 SD 0.88 | M 2.3 SD 0.92 | −2.49 | 0.014 * |
| Knowledge | Pre Treatment | Post Treatment | Z | p | d |
|---|---|---|---|---|---|
| Total Scale | M 53.6 SD 5.71 | M 77.30 SD 5.57 | −3.927 | 0.000 ** | 0.90 |
| General Information | M 43.30 SD 10.26 | M 73.96 SD 8.34 | −3.932 | 0.000 ** | 0.85 |
| Symptoms/ Diagnosis | M 60.49 SD 14.33 | M 75.48 SD 11.73 | −2.888 | 0.004 ** | 0.51 |
| Treatment | M 57.05 SD 9.84 | M 82.47 SD 10.07 | −3.835 | 0.000 ** | 0.79 |
| Perceived self-efficacy | M 2.35 SD 0.93 | M 4.75 SD 0.96 | −4.008 | 0.000 ** | 0.78 |
| Knowledge | Control Group | Multimodal Group | Z | p | d |
|---|---|---|---|---|---|
| Total Scale | M 53.5 SD 6.04 | M 77.30 SD 5.57 | −5.414 | 0.000 ** | 0.89 |
| General Information | M 43.96 SD 9.77 | M 73.96 SD 8.34 | −5.416 | 0.000 ** | 0.85 |
| Symptoms/ Diagnosis | M 63.27 SD 11.44 | M 75.48 SD 11.73 | −2.871 | 0.004 ** | 0.47 |
| Treatment | M 53.31 SD 9.51 | M 82.47 SD 10.07 | −5.273 | 0.000 ** | 0.83 |
| Perceived self-efficacy | M 2.3 SD 0.92 | M 4.75 SD 0.96 | −5.150 | 0.000 ** | 0.79 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jarque Fernández, S.; Amado Luz, L.; Oporto Alonso, M.; Fernández-Andújar, M. Effectiveness of a Long-Term Training Programme for Teachers in Attention-Deficit/Hyperactivity Disorder on Knowledge and Self-Efficacy. Mathematics 2021, 9, 1414. https://doi.org/10.3390/math9121414
Jarque Fernández S, Amado Luz L, Oporto Alonso M, Fernández-Andújar M. Effectiveness of a Long-Term Training Programme for Teachers in Attention-Deficit/Hyperactivity Disorder on Knowledge and Self-Efficacy. Mathematics. 2021; 9(12):1414. https://doi.org/10.3390/math9121414
Chicago/Turabian StyleJarque Fernández, Sonia, Laura Amado Luz, Marta Oporto Alonso, and Marina Fernández-Andújar. 2021. "Effectiveness of a Long-Term Training Programme for Teachers in Attention-Deficit/Hyperactivity Disorder on Knowledge and Self-Efficacy" Mathematics 9, no. 12: 1414. https://doi.org/10.3390/math9121414
APA StyleJarque Fernández, S., Amado Luz, L., Oporto Alonso, M., & Fernández-Andújar, M. (2021). Effectiveness of a Long-Term Training Programme for Teachers in Attention-Deficit/Hyperactivity Disorder on Knowledge and Self-Efficacy. Mathematics, 9(12), 1414. https://doi.org/10.3390/math9121414