
Nonadditive Entropy Application to Detrended Force Sensor Data to Indicate Balance Disorder of Patients with Vestibular System Dysfunction



Abstract
:1. Introduction
2. Materials and Methods
2.1. Entropy, Tsallis Entropy—Brief Background
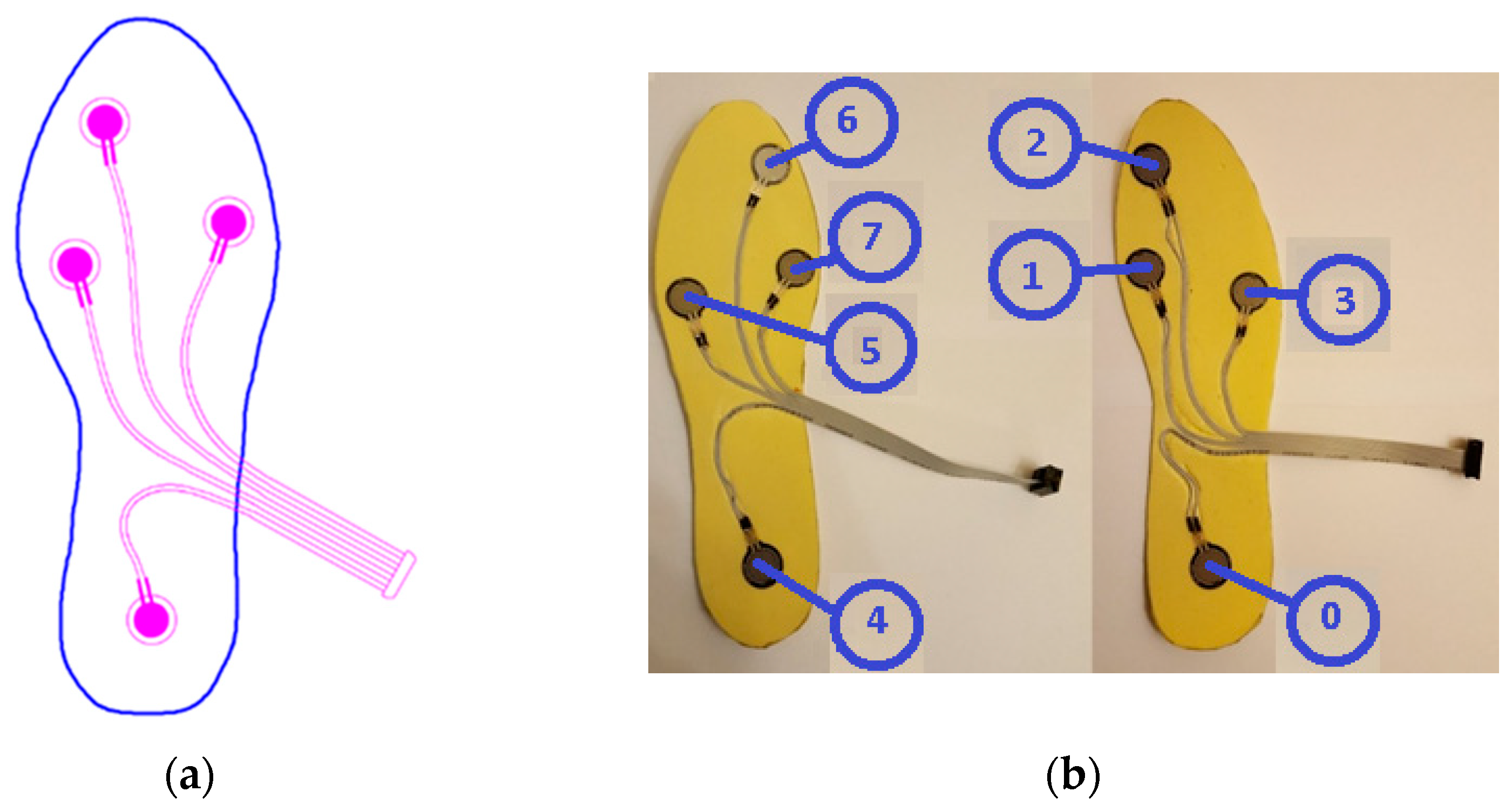
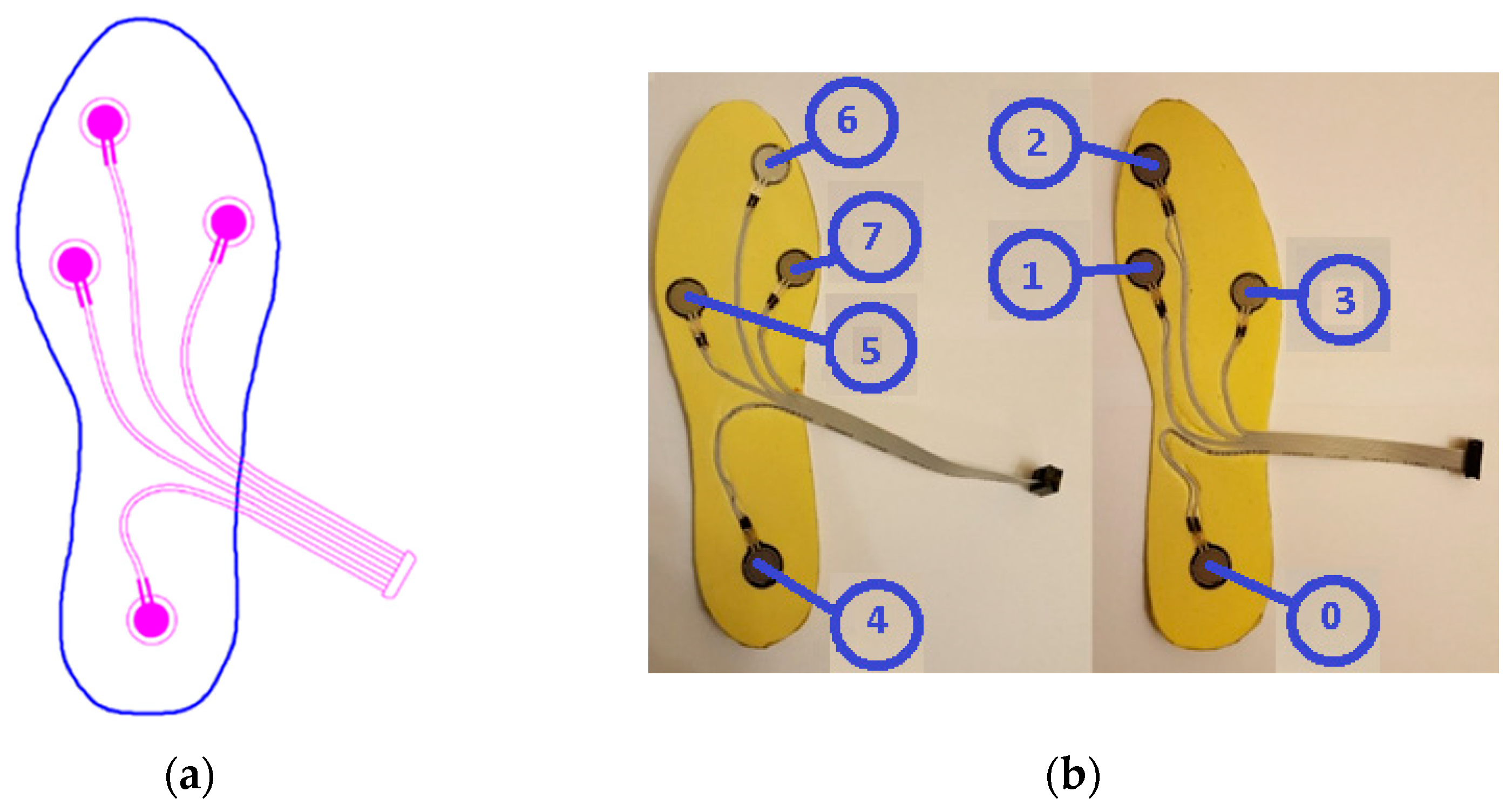
2.2. Data Collection
2.3. Data Processing
- Stage 1—Framing useful data
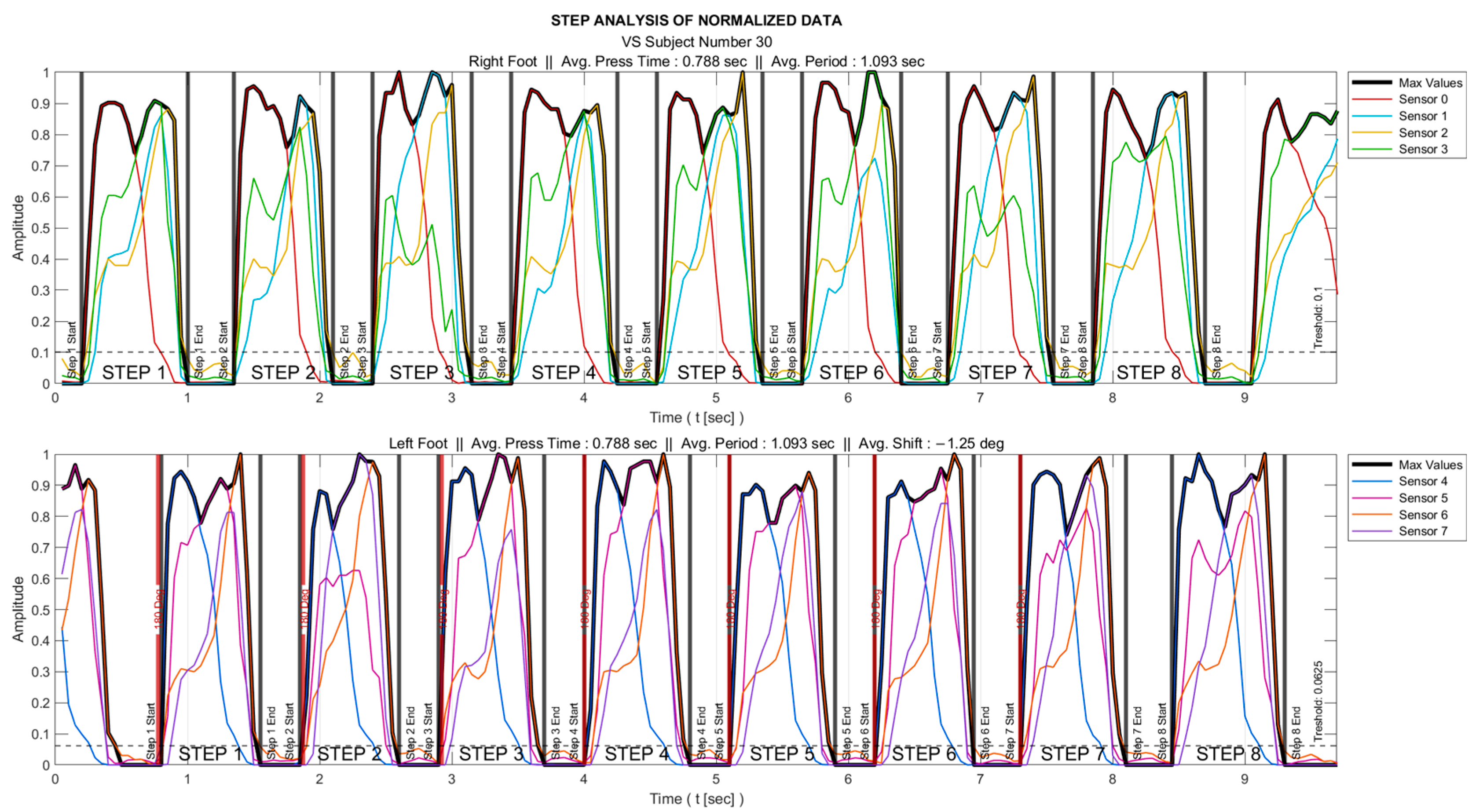
- Stage 2—Determining the intervals when the foot is actively touching the ground
- All the sensor data were normalized to the range 0–1 as
- The maximum of all sensor data () was determined. As an example, for the right foot, these data were obtained as .
- A threshold was set so that the foot was interpreted as being in the air for the time interval where remained below this threshold value.
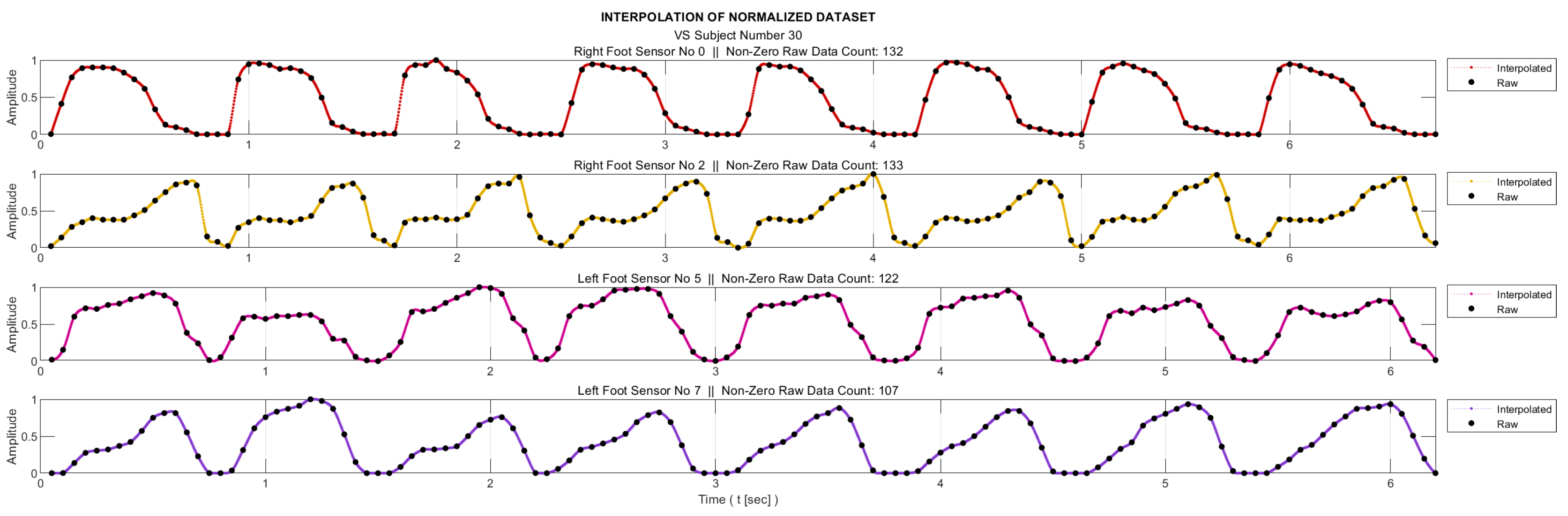
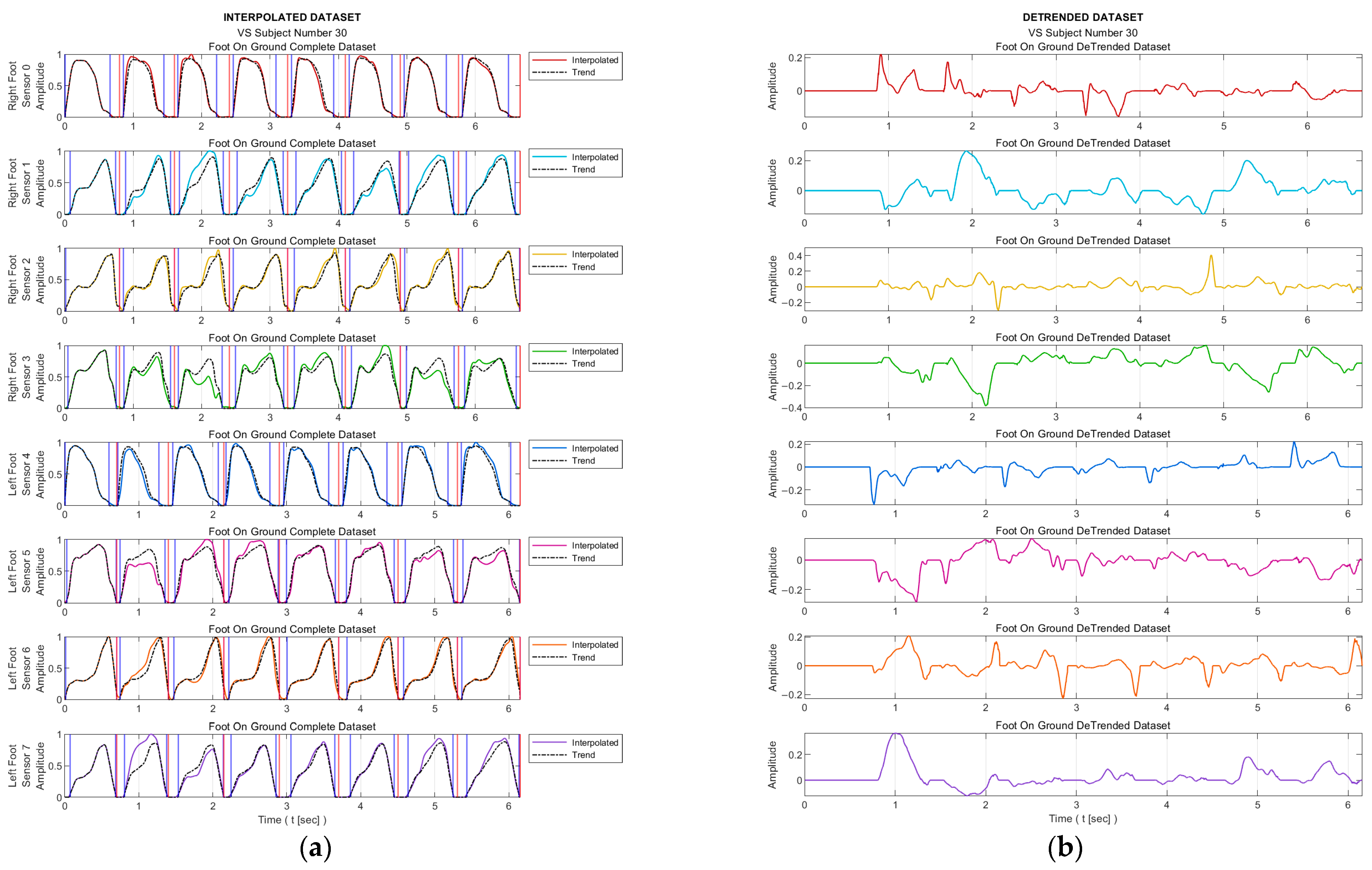
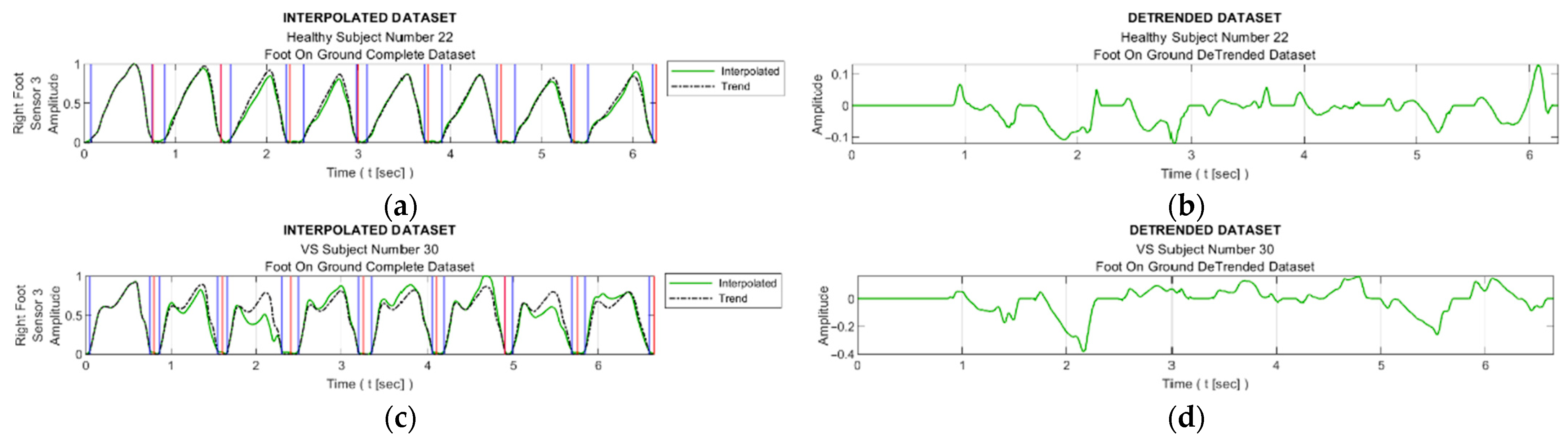
- Stage 3—Interpolation
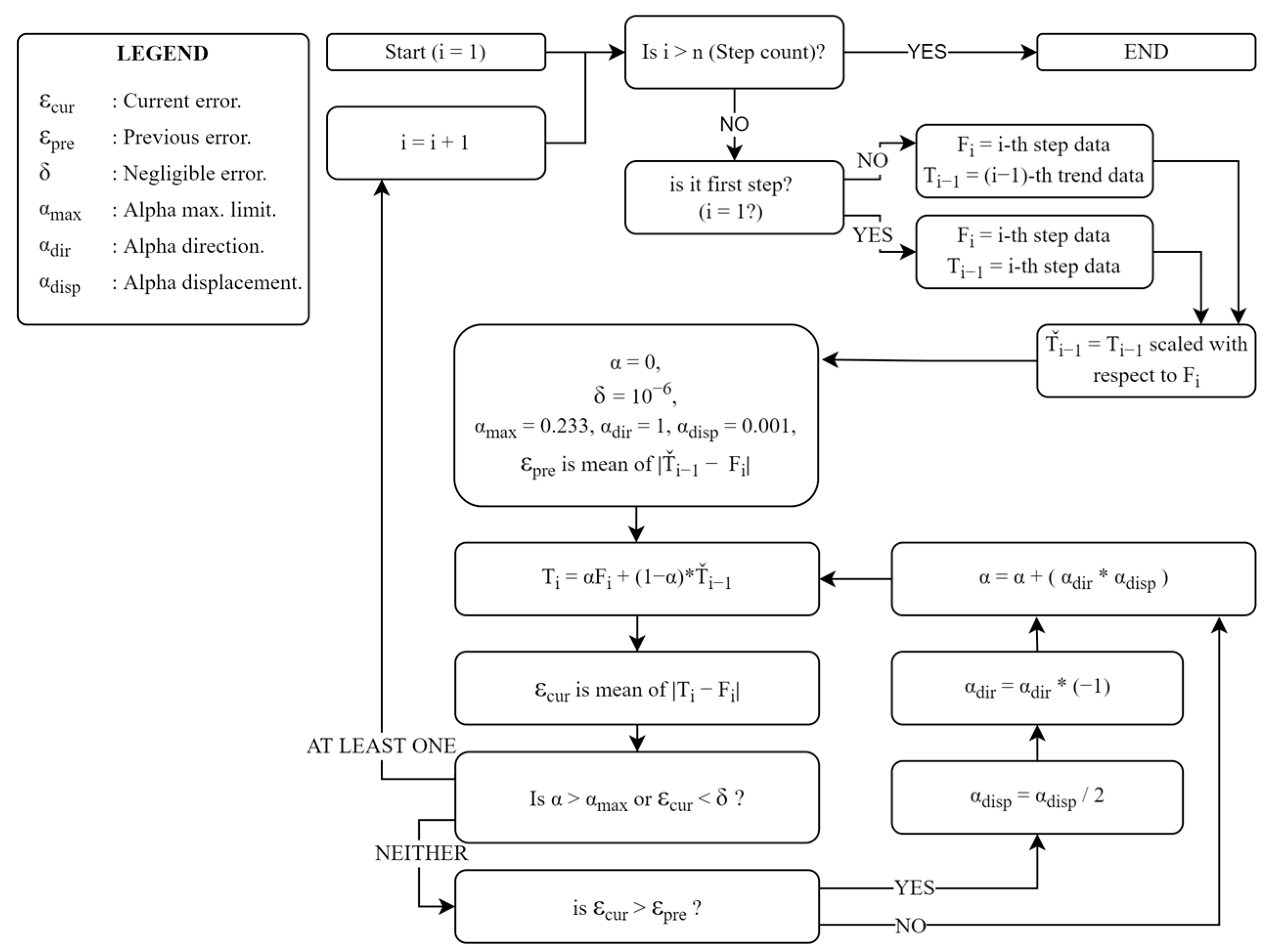
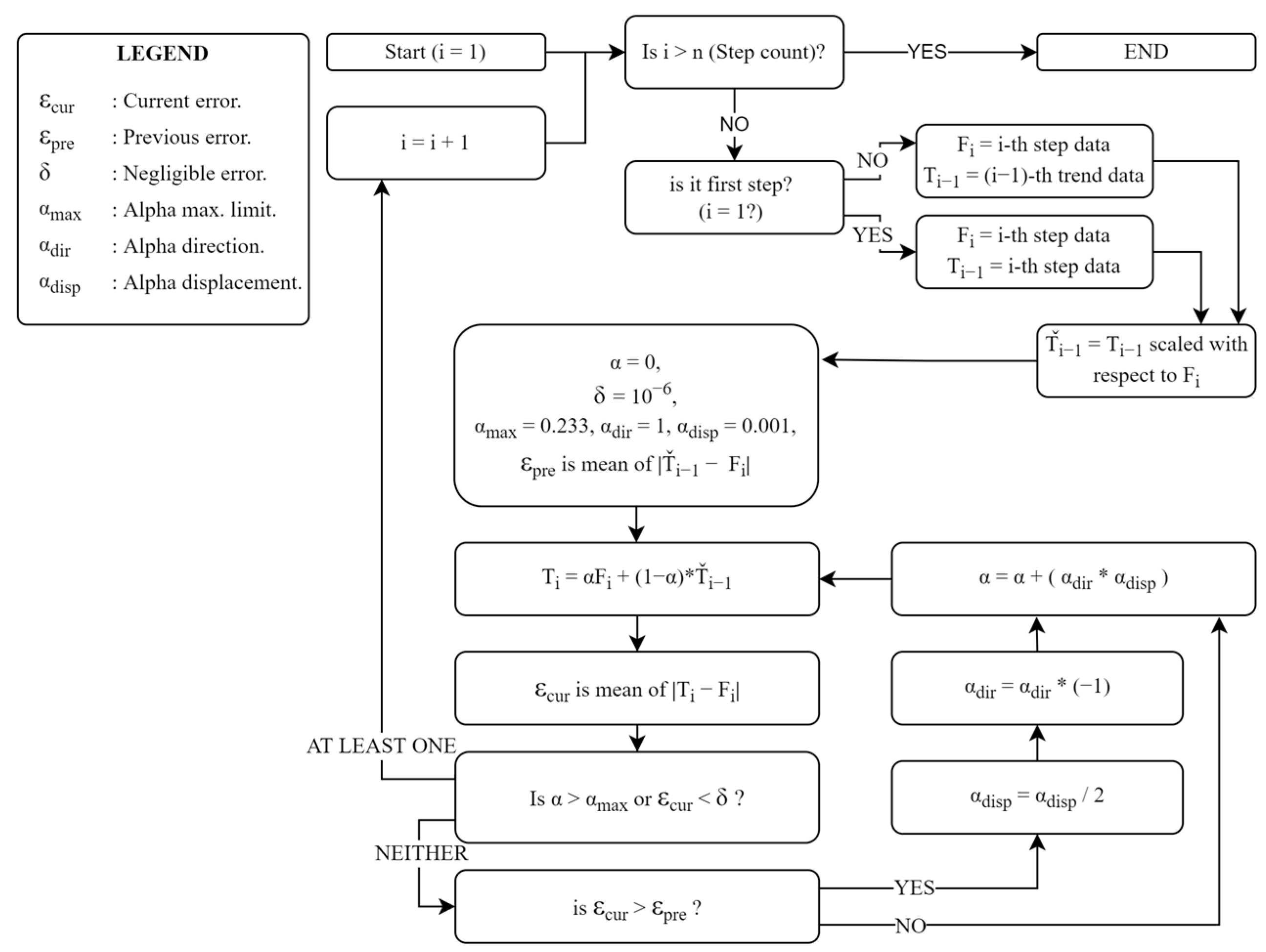
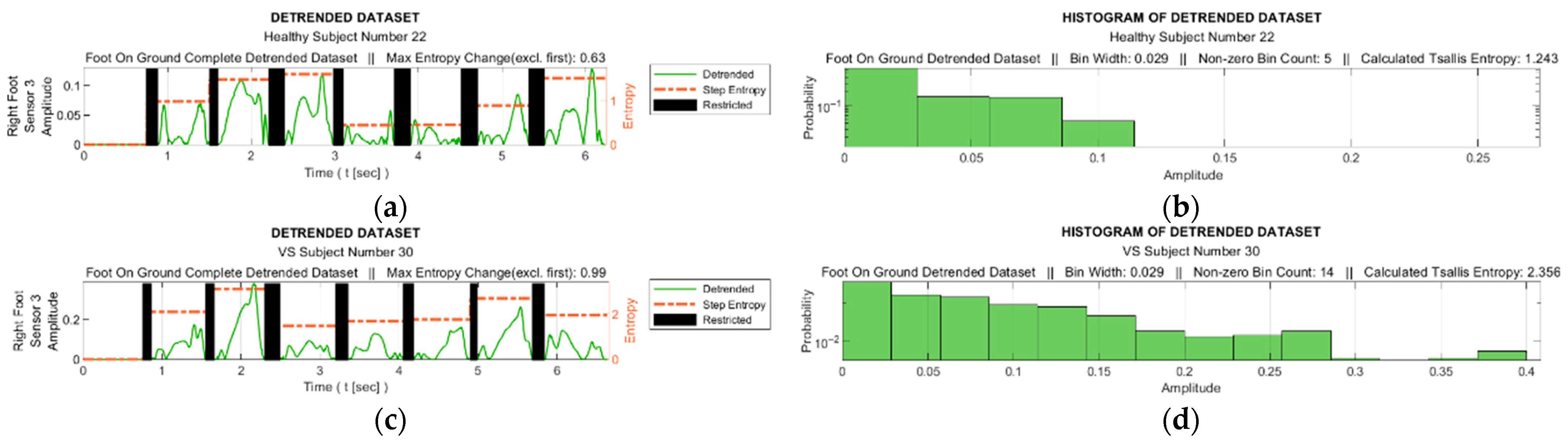
- Stage 4—Detrending
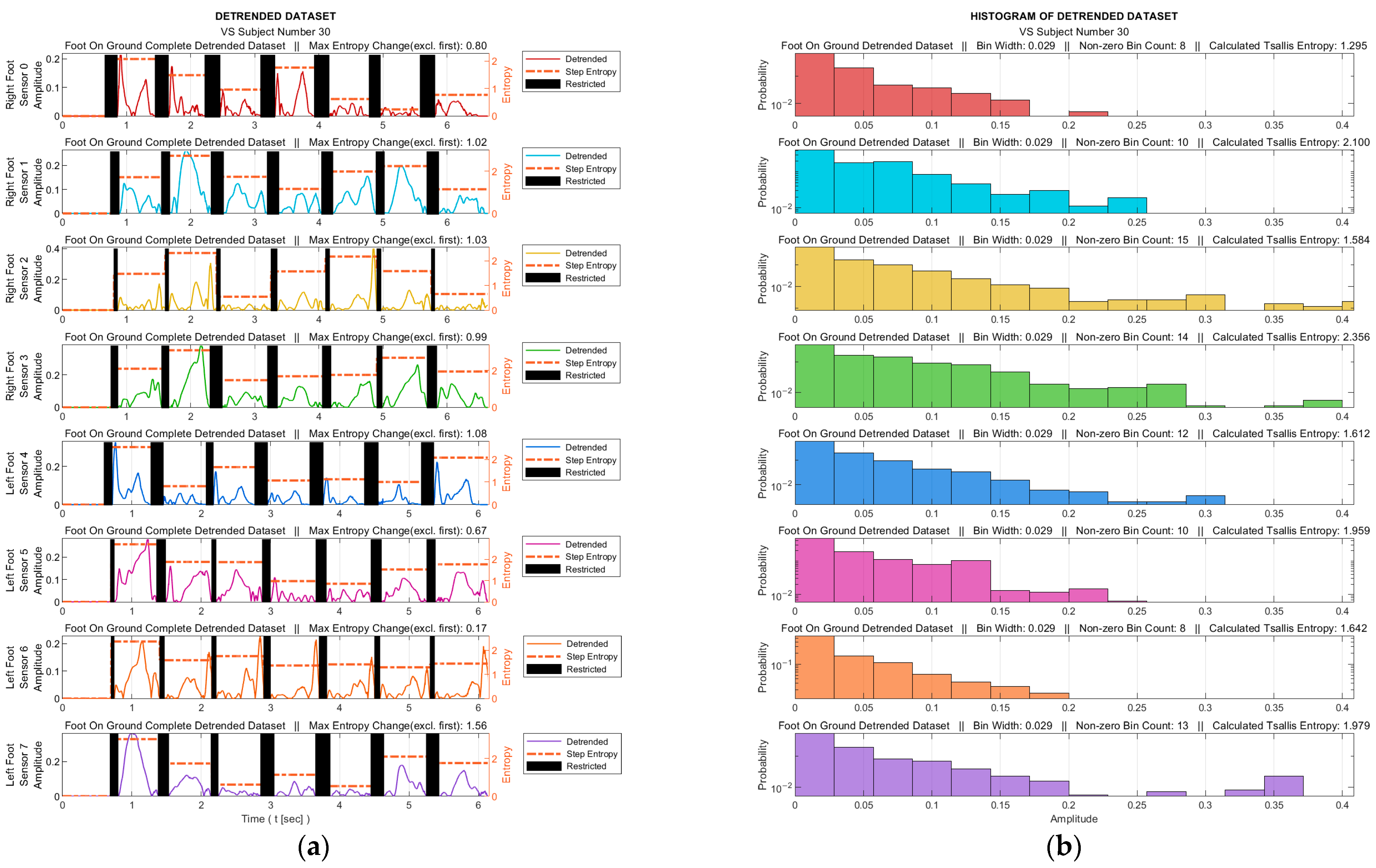
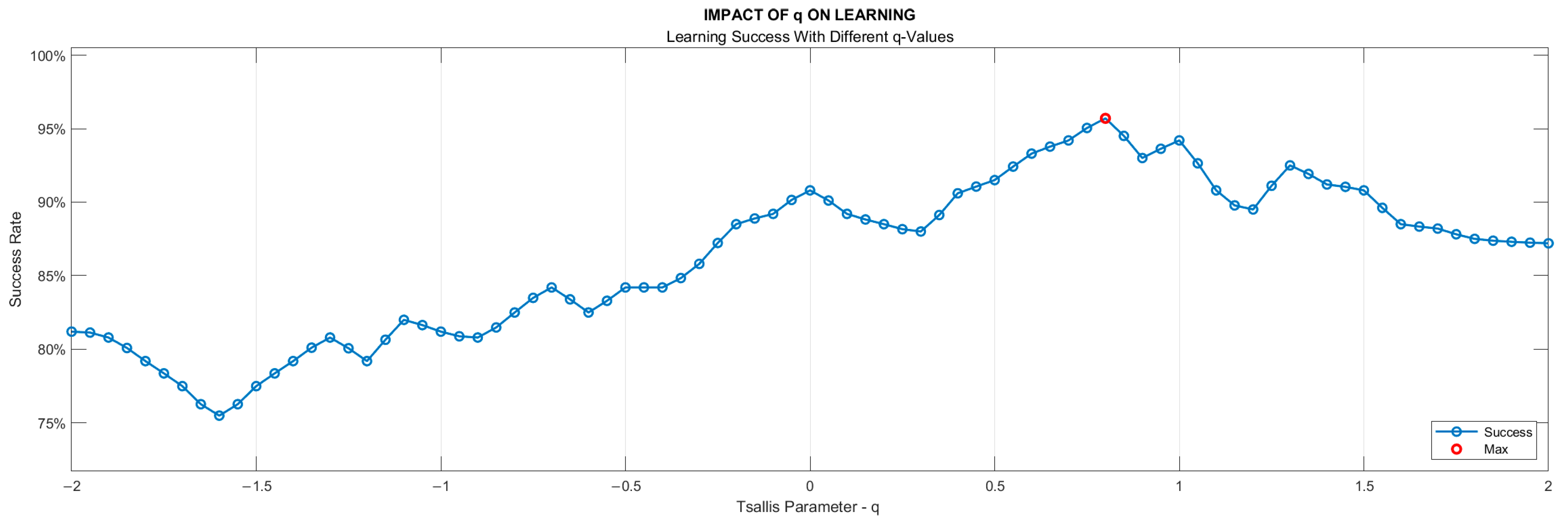
- Stage 5—Tsallis Entropy Calculations
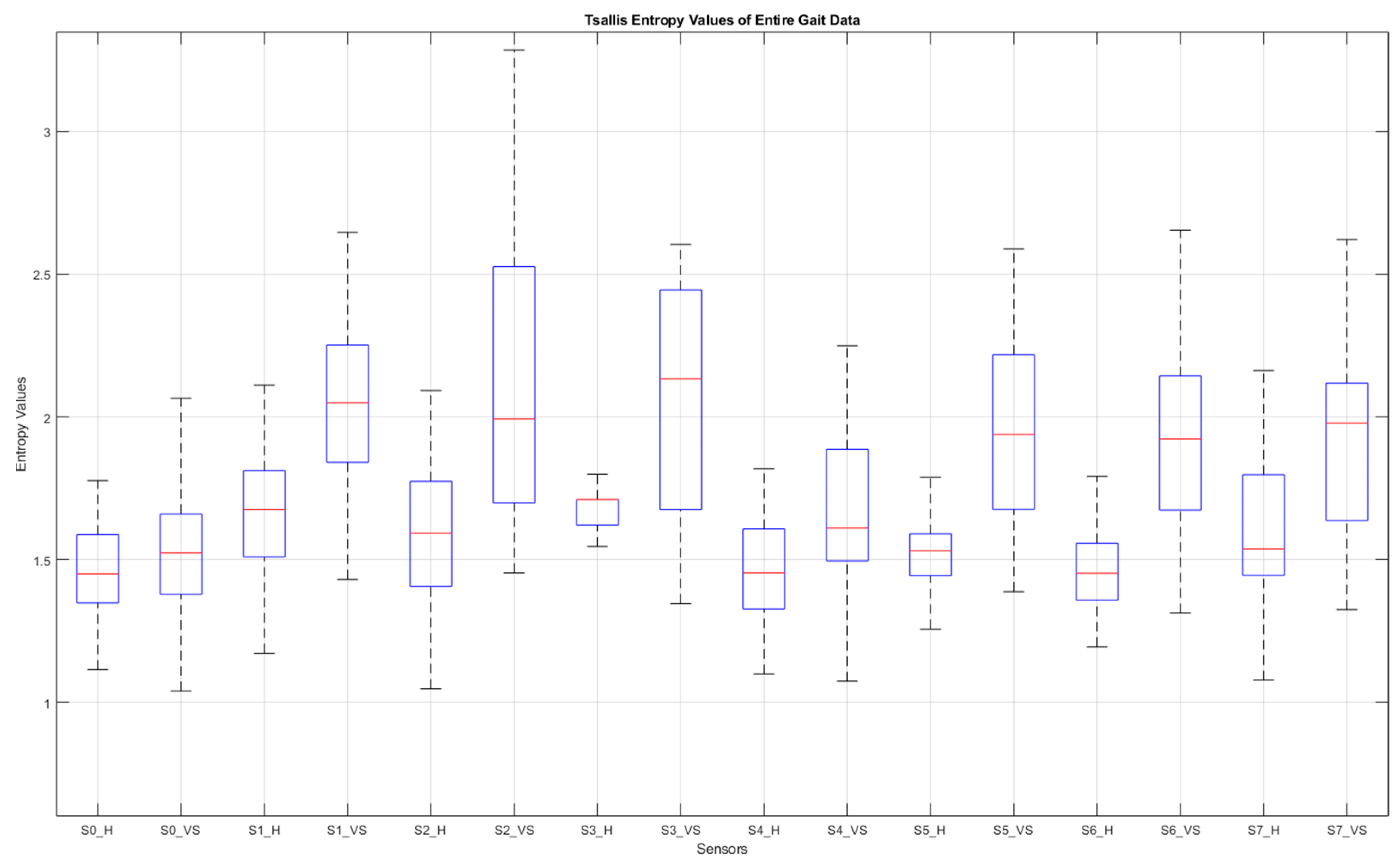
- Stage 6—Feature Extraction
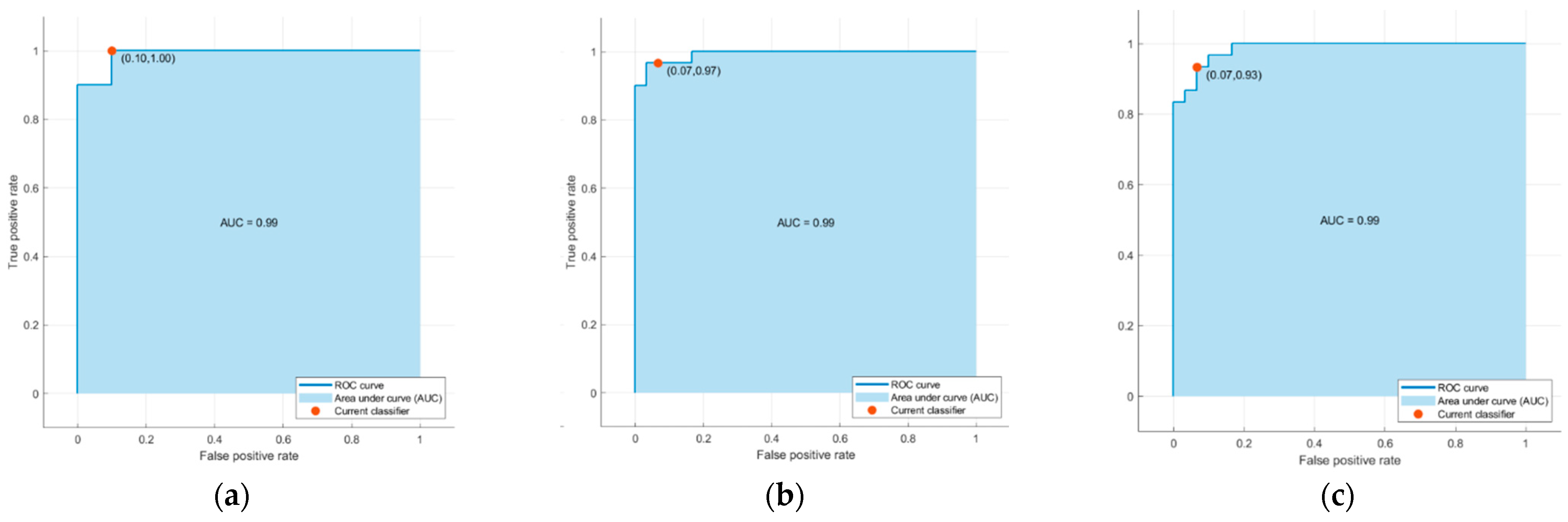
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Khan, S.; Chang, R. Anatomy of the vestibular system: A review. NeuroRehabilitation 2013, 32, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Vanicek, N.; King, S.A.; Gohil, R.; Chetter, I.C.; Coughlin, P.A. Computerized dynamic posturography for postural control assessment in patients with intermittent claudication. JoVE 2013, 82, e51077. [Google Scholar]
- Giladi, N.; Horak, F.B.; Hausdorff, J.M. Classification of gait disturbances: Distinguishing between continuous and episodic changes. Mov. Disord. 2013, 28, 1469–1473. [Google Scholar] [CrossRef] [PubMed]
- Bovonsunthonchai, S.; Vachalathiti, R.; Hiengkaew, V.; Bryant, M.S.; Richards, J.; Senanarong, V. Quantitative gait analysis in mild cognitive impairment, dementia, and cognitively intact individuals: A cross-sectional case–control study. BMC Geriatr. 2022, 22, 767. [Google Scholar] [CrossRef]
- Guo, Y.; Yang, J.; Liu, Y.; Chen, X.; Yang, G.-Z. Detection and assessment of Parkinson’s disease based on gait analysis. Front. Aging Neurosci. 2022, 14, 916971. [Google Scholar] [CrossRef]
- Wagner, A.R.; Reschke, M.F. Aging, vestibular function, and balance control: Physiological and behavioral considerations. Curr. Opin. Physiol. 2021, 19, 67–74. [Google Scholar]
- Ikizoglu, S.; Heydarov, S. Accuracy comparison of dimensionality reduction techniques to determine significant features from IMU sensor-based data to diagnose vestibular system disorders. Biomed. Signal Process. Control. 2020, 61, 101963. [Google Scholar] [CrossRef]
- Agrawal, D.K.; Usaha, W.; Pojprapai, S.; Wattanapan, P. Fall Risk Prediction Using Wireless Sensor Insoles with Machine Learning. IEEE Access 2023, 11, 23119–23126. [Google Scholar] [CrossRef]
- Schmidheiny, A.; Swanenburg, J.; Straumann, D.; de Bruin, E.D.; Knols, R.H. Discriminant validity and test re-test reproducibility of a gait assessment in patients with vestibular dysfunction. BMC Ear Nose Throat Disord. 2015, 15, 6. [Google Scholar] [CrossRef]
- Tsallis, C. Introduction to Nonextensive Statistical Mechanics: Approaching a Complex World. Contemp. Phys. 2009, 431–438. [Google Scholar] [CrossRef]
- Zhang, D.; Jia, X.; Ding, H.; Ye, D.; Thakor, N.V. Application of Tsallis entropy to EEG: Quantifying the presence of burst suppression after asphyxial cardiac arrest in rats. IEEE Trans. Biomed. Eng. 2010, 57, 867–874. [Google Scholar] [CrossRef] [PubMed]
- Tong, S.; Bezerianos, A.; Paul, J.; Zhu, Y.; Thakor, N. Nonextensive entropy measure of EEG following brain injury from cardiac arrest. Phys. A Stat. Mech. Appl. 2002, 305, 619–628. [Google Scholar] [CrossRef]
- Dutta, S.; Ghosh, D.; Chatterjee, S. Multifractal detrended fluctuation analysis of human gait diseases. Front. Physiol. 2013, 4, 274. [Google Scholar] [CrossRef] [PubMed]
- Phinyomark, A.; Larracy, R.; Scheme, E. Fractal analysis of human gait variability via stride interval time series. Front. Physiol. 2020, 11, 333. [Google Scholar] [CrossRef]
- Hausdorff, J.M.; Ashkenazy, Y.; Peng, C.; Ivanov, P.C.; Stanley, H.; Goldberger, A.L. When human walking becomes random walking: Fractal analysis and modeling of gait rhythm fluctuations. Phys. A Stat. Mech. Appl. 2001, 302, 138–147. [Google Scholar] [CrossRef]
- Muñoz-Diosdado, A. Fractal and multifractal analysis of human gait. AIP Conf. Proc. 2003, 682, 243–250. [Google Scholar]
- Günaydın, B.; İkizoğlu, S. Multifractal detrended fluctuation analysis of insole pressure sensor data to diagnose vestibular system disorders. Biomed. Eng. Lett. 2023. [Google Scholar] [CrossRef]
- Higuma, M.; Sanjo, N.; Mitoma, H.; Yoneyama, M.; Yokota, T. Wholeday gait monitoring in patients with Alzheimer’s disease: A relationship between attention and gait cycle. J. Alzheimer’s Dis. Rep. 2017, 1, 1–8. [Google Scholar] [CrossRef]
- Nieto-Hidalgo, M.; Ferrández-Pastor, F.J.; Valdivieso-Sarabia, R.J.; Mora-Pascual, J.; García-Chamizo, J.M. Gait analysis using computer vision based on cloud platform and mobile device. Mobile Inf. Syst. 2018, 2018, 7381264. [Google Scholar] [CrossRef]
- Schwaemmle, V.; Tsallis, C. Two-parameter generalization of the logarithm and exponential functions and Boltzmann-Gibbs-Shannon entropy. J. Math. Phys. 2007, 48, 113301. [Google Scholar] [CrossRef]
- Liang, Z.; Wang, Y.; Sun, X.; Li, D.; Voss, L.J.; Sleigh, J.W.; Hagihira, S.; Li, X. Entropy Measures in Anesthesia. Front. Comput. Neurosci. 2015, 9, 16. [Google Scholar] [CrossRef] [PubMed]
- Xiong, W.; Faes, L.; Ivanov, P.C. Entropy measures, entropy estimators, and their performance in quantifying complex dynamics: Effects of artifacts, nonstationarity, and long-range correlations. Phys. Rev. E 2017, 95, 062114. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Pengjian, S. Multiscale Tsallis permutation entropy analysis for complex physiological time series. Phys. A Stat. Mech. Appl. 2019, 529, 10–20. [Google Scholar] [CrossRef]
- Tsallis, C.; Tirnakli, U. Nonadditive entropy and nonextensive statistical mechanics—Some central concepts and recent applications. J. Phys. Conf. Ser. 2009, 201, 012001. [Google Scholar] [CrossRef]
- Sigalotti, L.D.G.; Ramírez-Rojas, A.; Vargas, C.A. Tsallis q-Statistics in Seismology. Entropy 2023, 25, 408. [Google Scholar] [CrossRef]
- Wilk, G.; Włodarczyk, Z. Some Non-Obvious Consequences of Non-Extensiveness of Entropy. Entropy 2023, 25, 474. [Google Scholar] [CrossRef]
- Healy, A.; Burgess-Walker, P.; Naemi, R.; Chockalingam, N. Repeatability of WalkinSense® in shoe pressure measurement system: A preliminary study. Foot 2012, 22, 35–39. [Google Scholar] [CrossRef]
- Holleczek, T.; Ruegg, A.; Harms, H.; Tro, G. Textile pressure sensors for sports applications. In Proceedings of the 2010 IEEE Sensors, Waikoloa, HI, USA, 1–4 November 2010; pp. 732–737. [Google Scholar]
- Saito, M.; Nakajima, K.; Takano, C.; Ohta, Y.; Sugimoto, C.; Ezoe, R.; Sasaki, K.; Hosaka, H.; Ifukube, T.; Ino, S.; et al. An in -shoe device to measure plantar pressure during daily human activity. Med. Eng. Phys. 2011, 33, 638–645. [Google Scholar] [CrossRef]
- Salpavaara, T.; Verho, J.; Lekkala, J.; Halttunen, J. Wireless insole sensor system for plantar force measurements during sport events. In Proceedings of the IMEKO XIX World Congress on Fundamental and Applied Metrology, Lisbon, Portugal, 6–11 September 2009; pp. 2118–2123. [Google Scholar]
- Shu, L.; Hua, T.; Wang, Y.; Li, Q.; Feng, D.D.; Tao, X. In-shoe plantar pressure measurement and analysis system based on fabric pressure sensing array. IEEE Trans. Inf. Technol. Biomed. 2010, 14, 767–775. [Google Scholar]
- Tahir, A.M.; Chowdhury, M.E.; Khandakar, A.; Al-Hamouz, S.; Abdalla, M.; Awadallah, S.; Reaz, M.B.I.; Al-Emadi, N. A Systematic Approach to the Design and Characterization of a Smart Insole for Detecting Vertical Ground Reaction Force (vGRF) in Gait Analysis. Sensors 2020, 20, 957. [Google Scholar] [CrossRef]
- FSR Technical Paper. Available online: https://cdn2.hubspot.net/hubfs/3899023/Interlinkelectronics%20November2017/Docs/Datasheet_FSR.pdf (accessed on 1 March 2023).
- Burden, R.L.; Faires, J.D. Numerical Analysis; Cengage Learning: Boston, MA, USA, 2019; pp. 144–172. [Google Scholar]
- Peterson, L. K-nearest neighbor. Scholarpedia 2009, 4, 1883. [Google Scholar] [CrossRef]
- Schober, P.; Vetter, T.R. Logistic Regression in Medical Research. Anesth. Analg. 2021, 132, 365–366. [Google Scholar] [CrossRef] [PubMed]
- Geron, A. Chapter 5: Support Vector Machines. In Hands-On Machine Learning with Scikit-Learn, Keras, and TensorFlow: Concepts, Tools, and Techniques to Build Intelligent Systems; O’Reilly Media, Inc.: Sebastopol, CA, USA, 2019. [Google Scholar]
- Lin, Y.; Wang, C.; Wu, T.; Jeng, S.; Chen, J. Support vector machine for EEG signal classification during listening to emotional music. In Proceedings of the 2008 IEEE 10th Workshop on Multimedia Signal Processing, Cairns, QLD, Australia, 8–10 October 2008; pp. 127–130. [Google Scholar]
- Saccà, V.; Campolo, M.; Mirarchi, D.; Gambardella, A.; Veltri, P.; Morabito, F.C. On the Classification of EEG Signal by Using an SVM Based Algorithm; Springer: Cham, Switzerland, 2018; pp. 271–278. [Google Scholar]
- Saini, I.; Singh, D.; Khosla, A. QRS detection using K-Nearest Neighbor algorithm (KNN) and evaluation on standard ECG databases. J. Adv. Res. 2013, 4, 331–344. [Google Scholar] [CrossRef] [PubMed]
- Yean, C.W.; Khairunizam, W.; Omar, M.I.; Murugappan, M.; Zheng, B.S.; Bakar, S.A.; Razlan, Z.M.; Ibrahim, Z. Analysis of the distance metrics of KNN classifier for EEG signal in stroke patients. In Proceedings of the 2018 International Conference on Computational Approach in Smart Systems Design and Applications (ICASSDA), Kuching, Malaysia, 15–17 August 2018. [Google Scholar]
- Erguzel, T.T.; Noyan, C.O.; Eryilmaz, G.; Ünsalver, B.; Cebi, M.; Tas, C.; Dilbaz, N.; Tarhan, N. Binomial Logistic Regression and Artificial Neural Network Methods to Classify Opioid-Dependent Subjects and Control Group Using Quantitative EEG Power Measures. Clin. EEG Neurosci. 2019, 50, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Maria, G.; Juan, S.; Helbert, E. EEG signal analysis using classification techniques: Logistic regression, artificial neural networks, support vector machines, and convolutional neural networks. Heliyon 2021, 7, e07258. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| operation range | 0.2 N–20 N |
| physical dimensions | ϕpad 18.3 mm, ϕsens 12.7 mm |
| thickness | 0.46 mm |
| repeatability | ±2% |
| idle resistance | >10 MΩ |
| hysteresis | 10% max. |
| rising time | <3 µs |
| Healthy (30) | Diseased (30) | |||
|---|---|---|---|---|
| Male (15) | Female (15) | Male (13) | Female (17) | |
| age | 54.3 ± 8.5 | 55.1 ± 7.9 | 54.5 ± 8.5 | 56.8 ± 7.2 |
| mass (kg) | 66.6 ± 9.8 | 65.1 ± 8.8 | 65.9 ± 10.2 | 64.9 ± 7.9 |
| height (cm) | 169.2 ± 10.0 | 164.0 ± 6.2 | 170.3 ± 8.8 | 163.4 ± 5.7 |
| Male | Female | |
|---|---|---|
| BPPV * | 6 | 8 |
| UVW * | 3 | 4 |
| Meniere | 3 | 3 |
| Vestibular Neuritis | 1 | 2 |
| Classification Model | Proposed Algorithm | Second-Degree Polynomial | Third-Degree Polynomial | Fourth-Degree Polynomial |
|---|---|---|---|---|
| SVM-Gaussian | 95.0% | 71.7% | 76.3% | 81.7% |
| Logistic regression (LR) | 95.0% | 63.3% | 78.3% | 76.3% |
| KNN-cosine | 93.3% | 66.7% | 70.0% | 78.3% |
| Model with highest accuracy | 95.0% (with SVM-G and LR) | 83.3% (with Ensemble-Bagged Trees) | 83.3% (with Decision Trees-Fine/Med.) | 86.7% (with Ensemble Subsp. Discr.) |
| Healthy Subject (no. 22) | VS Subject (no. 30) | |||
|---|---|---|---|---|
| Sensor | Entire Gait | Stepwise Max | Entire Gait | Stepwise Max |
| S0 | 1.39 | 0.98 | 1.29 | 0.80 |
| S1 | 2.15 | 0.83 | 2.10 | 1.02 |
| S2 | 1.38 | 0.72 | 1.58 | 1.03 |
| S3 | 1.24 | 0.63 | 2.36 | 0.99 |
| S4 | 1.08 | 0.87 | 1.61 | 1.08 |
| S5 | 1.38 | 0.79 | 1.96 | 0.67 |
| S6 | 1.36 | 0.82 | 1.64 | 0.17 |
| S7 | 1.54 | 0.86 | 1.98 | 1.56 |
| Algorithm | Accuracy (%) |
|---|---|
| SVM (Gaussian) | 95.0 |
| Logistic regression | 95.0 |
| KNN (cosine) | 93.3 |
| Neural network (wide) | 93.3 |
| Kernel (SVM) | 91.7 |
| Ensemble (bagged tree) | 88.3 |
| Naïve Bayes (kernel) | 86.7 |
| Quadratic discriminant | 78.3 |
| Decision tree (fine) | 73.3 |
| Predicted Class | SVM (Gaussian) | Logistic Regression | KNN (Cosine) | |||
|---|---|---|---|---|---|---|
| H | D | H | D | H | D | |
| H | 30 | 0 | 29 | 1 | 28 | 2 |
| D | 3 | 27 | 2 | 27 | 2 | 28 |
| Statistical Property | SVM (Gaussian) | Logistic Regression |
|---|---|---|
| accuracy (%) | 95.0 | 95.0 |
| sensitivity (%) | 91.6 | 94.0 |
| specificity (%) | 97.9 | 95.1 |
| F1 Score | 0.945 | 0.943 |
| MCC | 0.899 | 0.891 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Köse, H.Y.; İkizoğlu, S. Nonadditive Entropy Application to Detrended Force Sensor Data to Indicate Balance Disorder of Patients with Vestibular System Dysfunction. Entropy 2023, 25, 1385. https://doi.org/10.3390/e25101385
Köse HY, İkizoğlu S. Nonadditive Entropy Application to Detrended Force Sensor Data to Indicate Balance Disorder of Patients with Vestibular System Dysfunction. Entropy. 2023; 25(10):1385. https://doi.org/10.3390/e25101385
Chicago/Turabian StyleKöse, Harun Yaşar, and Serhat İkizoğlu. 2023. "Nonadditive Entropy Application to Detrended Force Sensor Data to Indicate Balance Disorder of Patients with Vestibular System Dysfunction" Entropy 25, no. 10: 1385. https://doi.org/10.3390/e25101385
APA StyleKöse, H. Y., & İkizoğlu, S. (2023). Nonadditive Entropy Application to Detrended Force Sensor Data to Indicate Balance Disorder of Patients with Vestibular System Dysfunction. Entropy, 25(10), 1385. https://doi.org/10.3390/e25101385