
A Machine Learning Model for the Prognosis of Pulseless Electrical Activity during Out-of-Hospital Cardiac Arrest


Abstract
:1. Introduction
2. Data Collection
3. Methods
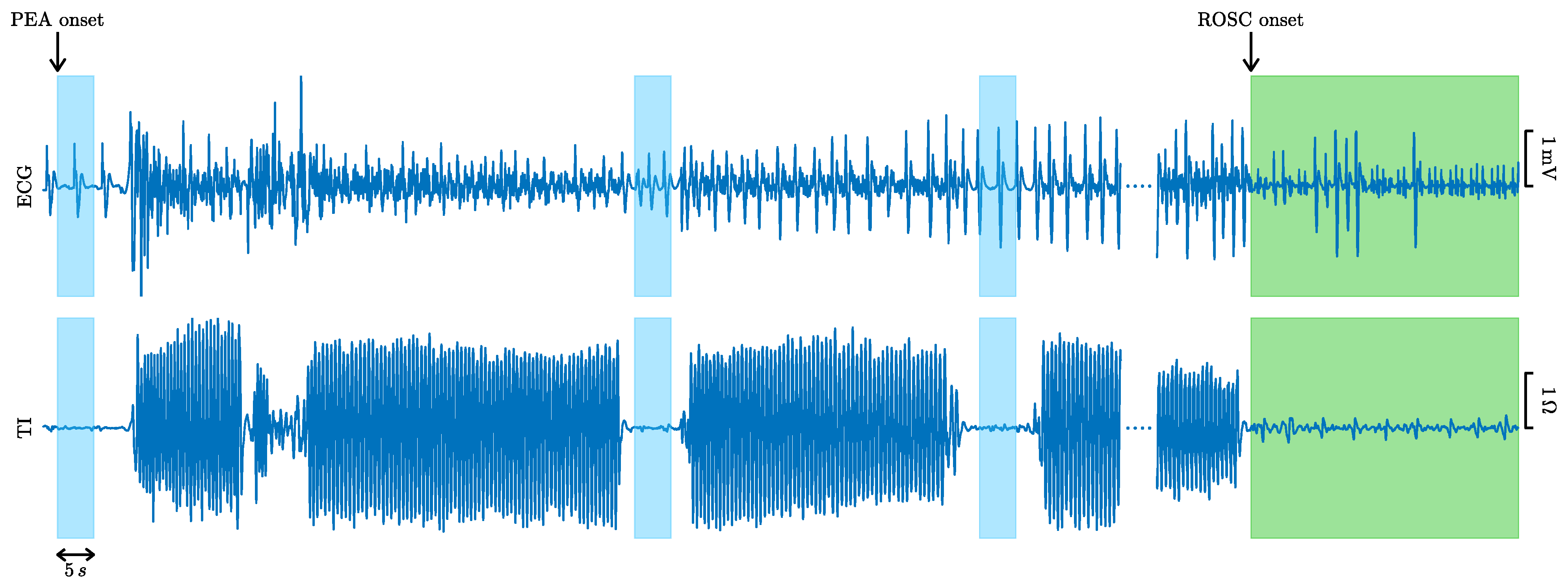
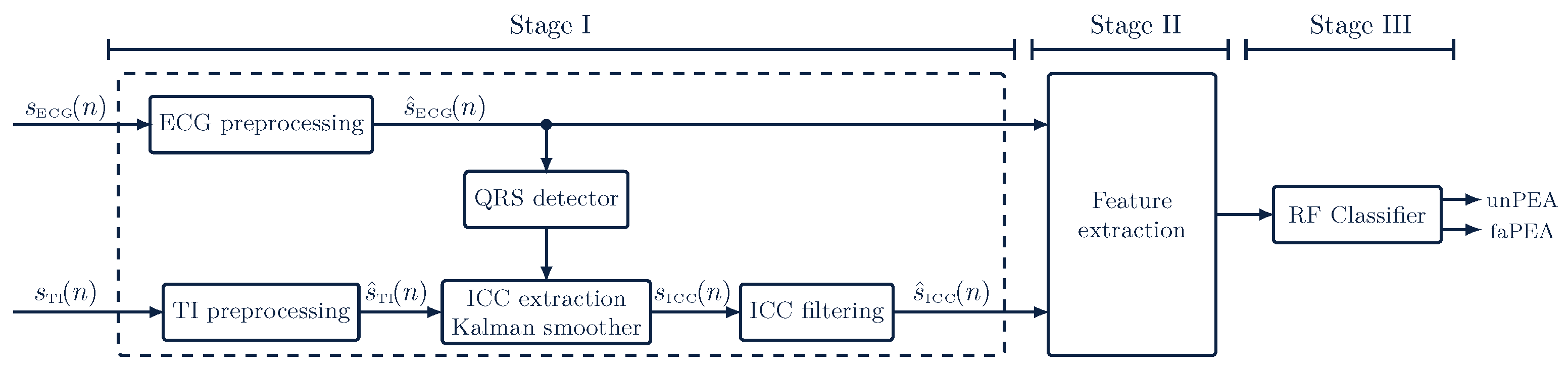
3.1. Processing of ECG and TI Signals
3.1.1. ECG Processing
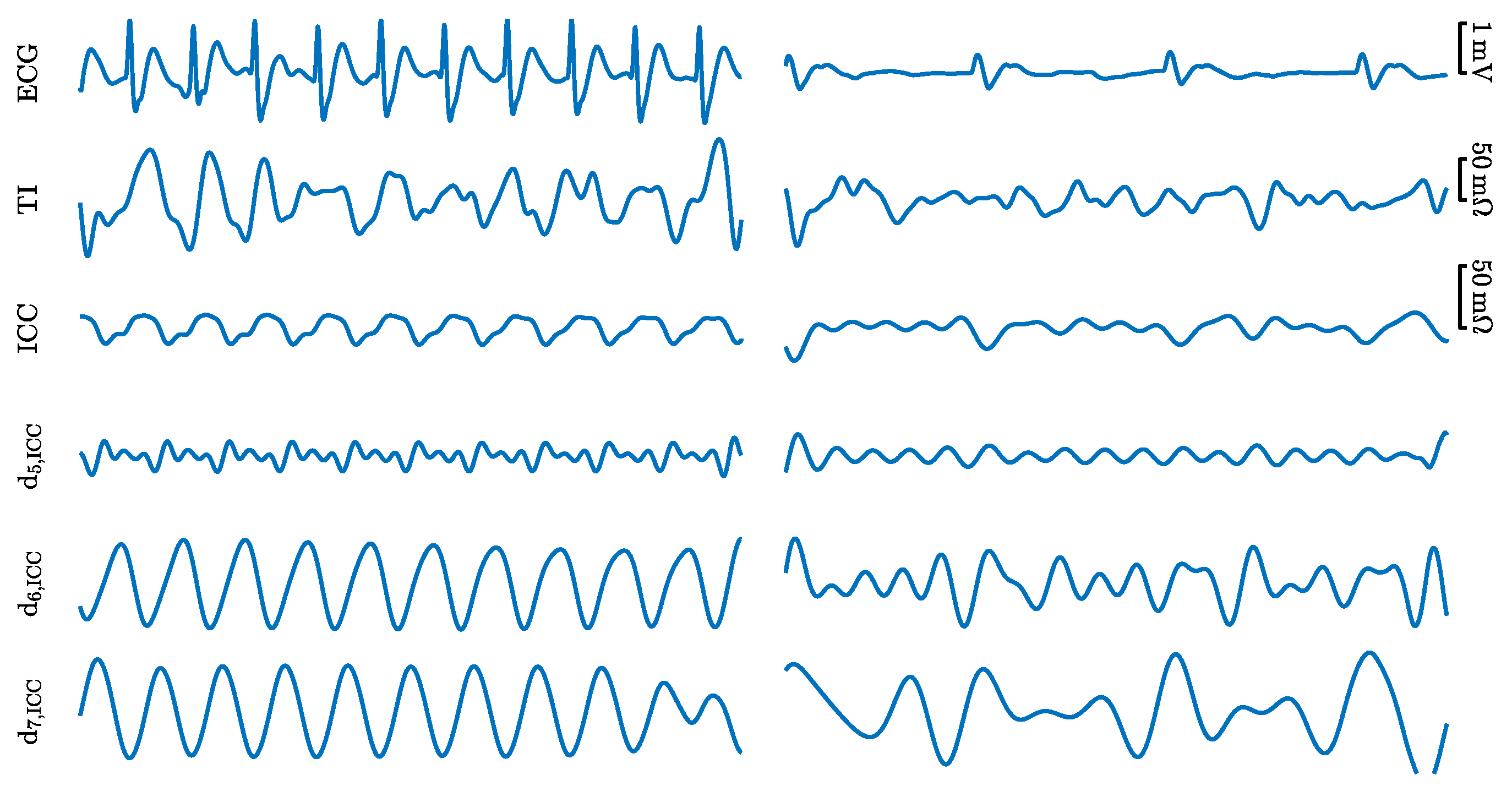
3.1.2. TI Processing and ICC Extraction
3.2. Feature Extraction
3.2.1. ECG Features
- The AMSA, the amplitude spectrum area, which is the weighted sum of the amplitudes of the ECG in the spectral domain, and it quantifies the variability and spectral dispersion of the signal. The AMSA was computed as described in [35];
- FuzzEn, fuzzy entropy, which measures the regularity of the signal, computed as described in [35];
- The SNEO, the smoothed nonlinear energy operator, as described in [37], which measures the local energy content of the ECG;
- The IQR values of the denoised ECG and its SWT detail coefficients , which are denoted by for [29];
3.2.2. ICC Features
- , the logarithmic energy (time domain) of the denoised ICC, which has been shown to correlate with ventricular wall movement [22];
- The SNEO, the smoothed nonlinear energy operator, as described in [37], which measures the local energy content of the ICC;
- The IQR values of the denoised ICC and its SWT detail coefficients , which are denoted by for [29];
- , the cross-power between the denoised ECG and ICC signals, as described in [36].
3.3. Building the Classifier
3.4. Evaluation of the Models
4. Results
4.1. Performance of the RF Classifier
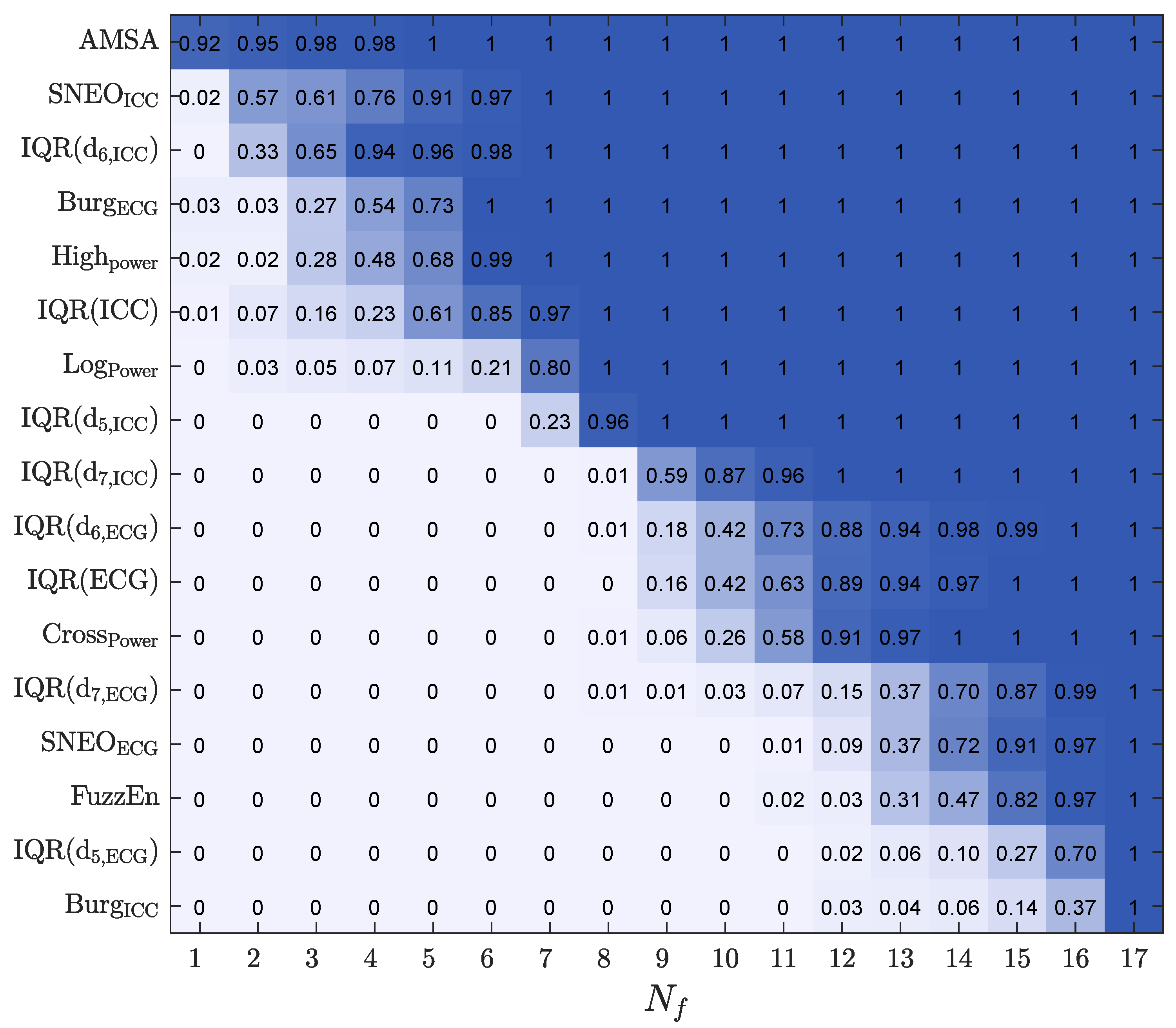
4.2. Feature Selection and Feature Analysis
4.3. Time Interval for a Prediction
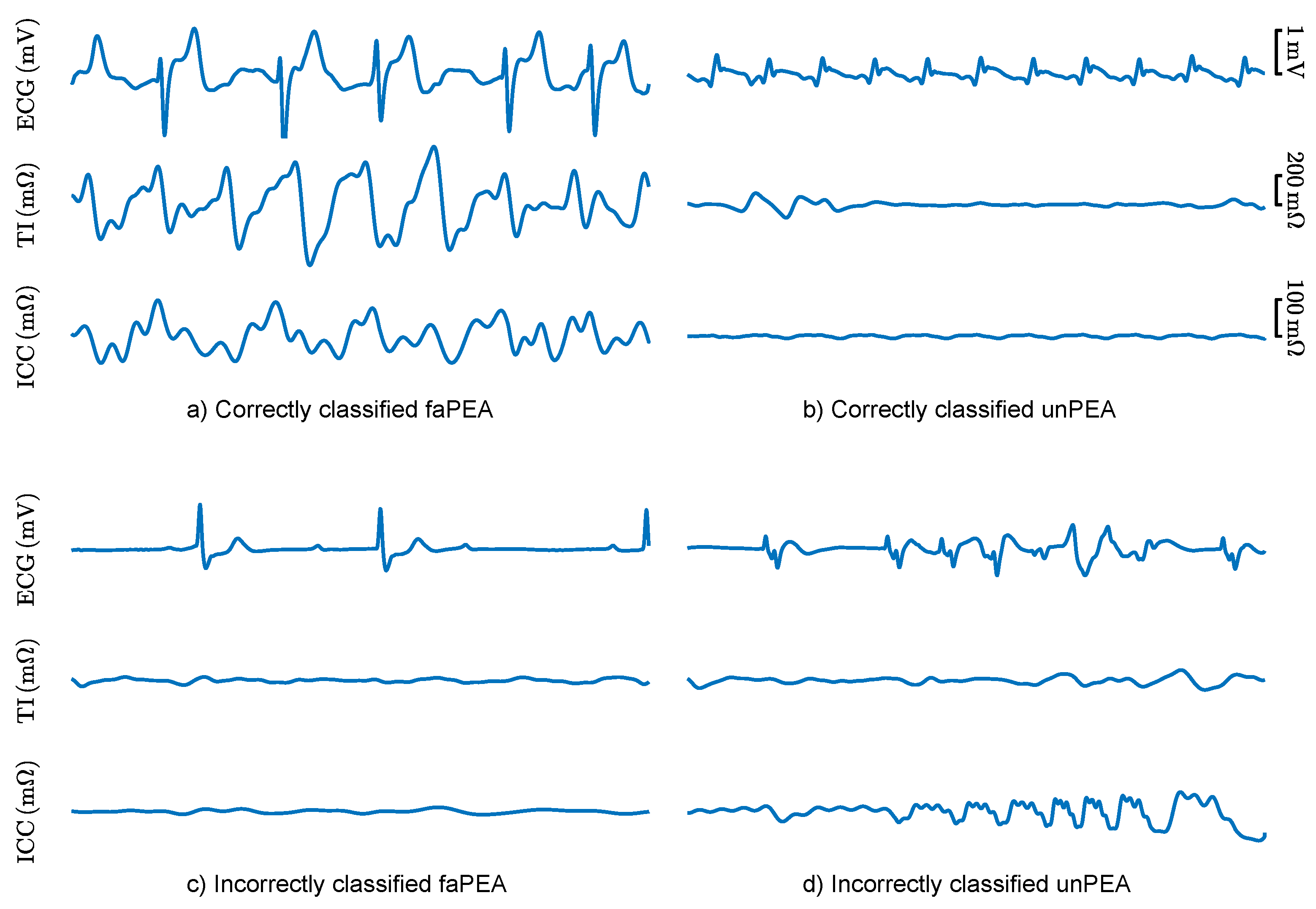
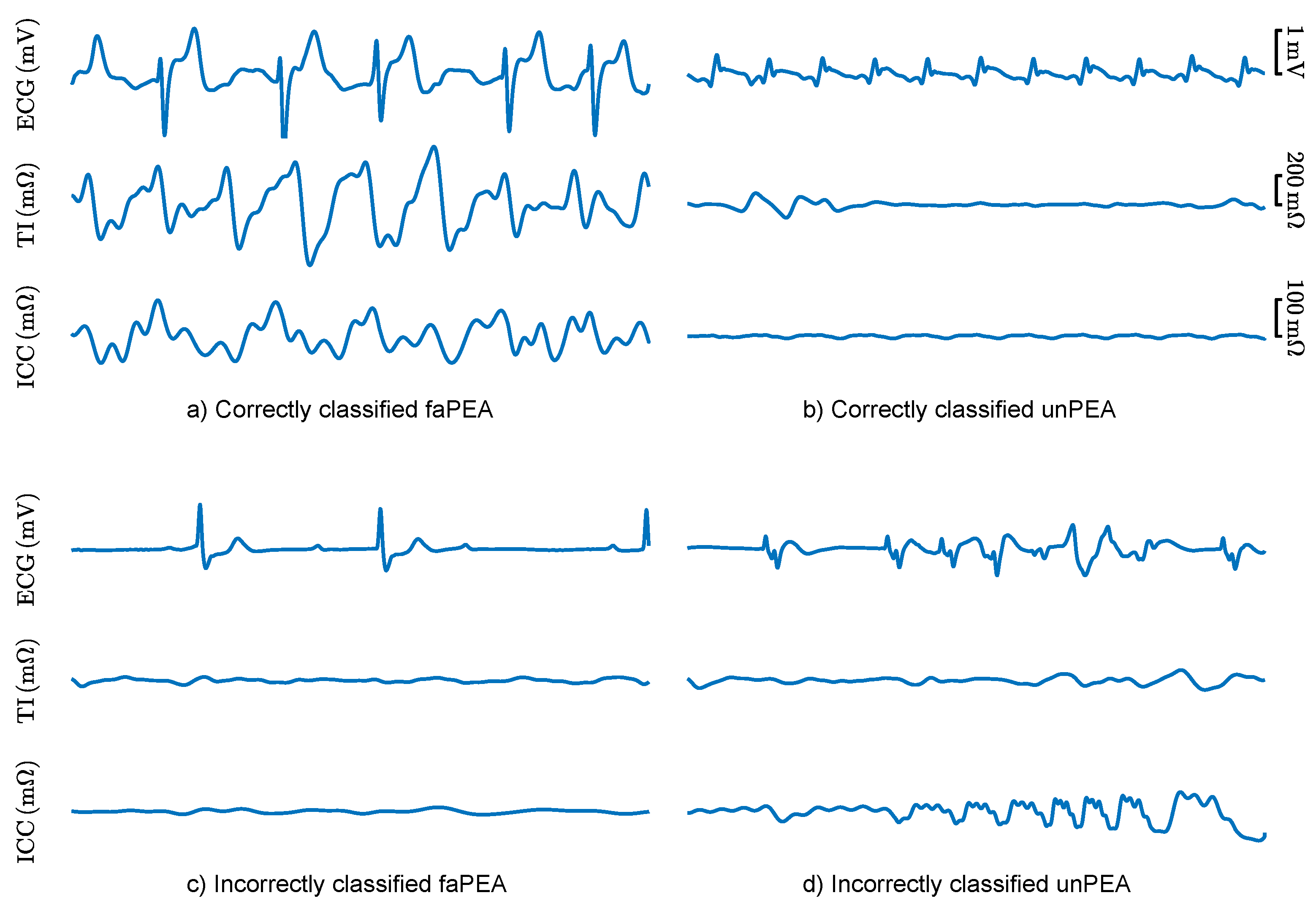
4.4. Analysis of the Classification Errors
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| OHCA | out-of-hospital cardiac arrest |
| ROSC | return of spontaneous circulation |
| CPR | cardiopulmonary resuscitation |
| EMS | emergency medical services |
| PEA | pulseless electrical activity |
| faPEA | pulseless electrical activity with favorable evolution |
| unPEA | pulseless electrical activity with unfavorable evolution |
| VF | ventricular fibrillation |
| ECG | electrocardiogram |
| TI | thoracic impedance |
| ICC | impedance circulation component |
| RF | random forest |
| LR | logistic regression |
| SVM | support vector machine |
| AUC | area under the curve |
| BAC | balanced accuracy |
| Se | sensitivity |
| Sp | specificity |
References
- Atwood, C.; Eisenberg, M.S.; Herlitz, J.; Rea, T.D. Incidence of EMS-treated out-of-hospital cardiac arrest in Europe. Resuscitation 2005, 67, 75–80. [Google Scholar] [CrossRef]
- Berdowski, J.; Berg, R.A.; Tijssen, J.G.; Koster, R.W. Global incidences of out-of-hospital cardiac arrest and survival rates: Systematic review of 67 prospective studies. Resuscitation 2010, 81, 1479–1487. [Google Scholar] [CrossRef] [PubMed]
- Perkins, G.D.; Handley, A.J.; Koster, R.W.; Castrén, M.; Smyth, M.A.; Olasveengen, T.; Monsieurs, K.G.; Raffay, V.; Gräsner, J.T.; Wenzel, V.; et al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 2. Adult basic life support and automated external defibrillation. Resuscitation 2015, 95, 81–99. [Google Scholar] [CrossRef] [Green Version]
- Rad, A.B.; Eftestøl, T.; Engan, K.; Irusta, U.; Kvaløy, J.T.; Kramer-Johansen, J.; Wik, L.; Katsaggelos, A.K. ECG-based classification of resuscitation cardiac rhythms for retrospective data analysis. IEEE Trans. Biomed. Eng. 2017, 64, 2411–2418. [Google Scholar] [CrossRef] [PubMed]
- Gräsner, J.T.; Wnent, J.; Herlitz, J.; Perkins, G.D.; Lefering, R.; Tjelmeland, I.; Koster, R.W.; Masterson, S.; Rossell-Ortiz, F.; Maurer, H.; et al. Survival after out-of-hospital cardiac arrest in Europe-Results of the EuReCa TWO study. Resuscitation 2020, 148, 218–226. [Google Scholar] [CrossRef]
- Oving, I.; de Graaf, C.; Karlsson, L.; Jonsson, M.; Kramer-Johansen, J.; Berglund, E.; Hulleman, M.; Beesems, S.G.; Koster, R.W.; Olasveengen, T.M.; et al. Occurrence of shockable rhythm in out-of-hospital cardiac arrest over time: A report from the COSTA group. Resuscitation 2020, 151, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Myerburg, R.J.; Halperin, H.; Egan, D.A.; Boineau, R.; Chugh, S.S.; Gillis, A.M.; Goldhaber, J.I.; Lathrop, D.A.; Liu, P.; Niemann, J.T.; et al. Pulseless electric activity: Definition, causes, mechanisms, management, and research priorities for the next decade: Report from a National Heart, Lung, and Blood Institute workshop. Circulation 2013, 128, 2532–2541. [Google Scholar] [CrossRef]
- Mader, T.J.; Nathanson, B.H.; Millay, S.; Coute, R.A.; Clapp, M.; McNally, B. Out-of-hospital cardiac arrest outcomes stratified by rhythm analysis. Resuscitation 2012, 83, 1358–1362. [Google Scholar] [CrossRef]
- Ko, D.T.; Qiu, F.; Koh, M.; Dorian, P.; Cheskes, S.; Austin, P.C.; Scales, D.C.; Wijeysundera, H.C.; Verbeek, P.R.; Drennan, I.; et al. Factors associated with out-of-hospital cardiac arrest with pulseless electric activity: A population-based study. Am. Heart J. 2016, 177, 129–137. [Google Scholar] [CrossRef]
- Meaney, P.A.; Nadkarni, V.M.; Kern, K.B.; Indik, J.H.; Halperin, H.R.; Berg, R.A. Rhythms and outcomes of adult in-hospital cardiac arrest. Crit. Care Med. 2010, 38, 101–108. [Google Scholar] [CrossRef]
- Nordseth, T.; Niles, D.E.; Eftestøl, T.; Sutton, R.M.; Irusta, U.; Abella, B.S.; Berg, R.A.; Nadkarni, V.M.; Skogvoll, E. Rhythm characteristics and patterns of change during cardiopulmonary resuscitation for in-hospital paediatric cardiac arrest. Resuscitation 2019, 135, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Weiser, C.; Poppe, M.; Sterz, F.; Herkner, H.; Clodi, C.; Schriefl, C.; Warenits, A.; Vossen, M.; Schwameis, M.; Nürnberger, A.; et al. Initial electrical frequency predicts survival and neurological outcome in out of hospital cardiac arrest patients with pulseless electrical activity. Resuscitation 2018, 125, 34–38. [Google Scholar] [CrossRef]
- Hauck, M.; Studnek, J.; Heffner, A.C.; Pearson, D.A. Cardiac arrest with initial arrest rhythm of pulseless electrical activity: Do rhythm characteristics correlate with outcome? Am. J. Emerg. Med. 2015, 33, 891–894. [Google Scholar] [CrossRef]
- Skjeflo, G.W.; Nordseth, T.; Loennechen, J.P.; Bergum, D.; Skogvoll, E. ECG changes during resuscitation of patients with initial pulseless electrical activity are associated with return of spontaneous circulation. Resuscitation 2018, 127, 31–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergum, D.; Skjeflo, G.W.; Nordseth, T.; Mjølstad, O.C.; Haugen, B.O.; Skogvoll, E.; Loennechen, J.P. ECG patterns in early pulseless electrical activity-Associations with aetiology and survival of in-hospital cardiac arrest. Resuscitation 2016, 104, 34–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehta, C.; Brady, W. Pulseless electrical activity in cardiac arrest: Electrocardiographic presentations and management considerations based on the electrocardiogram. Am. J. Emerg. Med. 2012, 30, 236–239. [Google Scholar] [CrossRef]
- Van den Bempt, S.; Wauters, L.; Dewolf, P. Pulseless Electrical Activity: Detection of Underlying Causes in a Prehospital Setting. Med. Princ. Pract. 2021, 30, 212–222. [Google Scholar] [CrossRef]
- Rabjohns, J.; Quan, T.; Boniface, K.; Pourmand, A. Pseudo-pulseless electrical activity in the emergency department, an evidence based approach. Am. J. Emerg. Med. 2020, 38, 371–375. [Google Scholar] [CrossRef] [PubMed]
- Flato, U.A.P.; Paiva, E.F.; Carballo, M.T.; Buehler, A.M.; Marco, R.; Timerman, A. Echocardiography for prognostication during the resuscitation of intensive care unit patients with non-shockable rhythm cardiac arrest. Resuscitation 2015, 92, 1–6. [Google Scholar] [CrossRef]
- Prosen, G.; Križmarić, M.; Završnik, J.; Grmec, Š. Impact of modified treatment in echocardiographically confirmed pseudo-pulseless electrical activity in out-of-hospital cardiac arrest patients with constant end-tidal carbon dioxide pressure during compression pauses. J. Int. Med. Res. 2010, 38, 1458–1467. [Google Scholar] [CrossRef]
- Losert, H.; Risdal, M.; Sterz, F.; Nysæther, J.; Köhler, K.; Eftestøl, T.; Wandaller, C.; Myklebust, H.; Uray, T.; Aase, S.O.; et al. Thoracic-impedance changes measured via defibrillator pads can monitor signs of circulation. Resuscitation 2007, 73, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Alonso, E.; Aramendi, E.; Daya, M.; Irusta, U.; Chicote, B.; Russell, J.K.; Tereshchenko, L.G. Circulation detection using the electrocardiogram and the thoracic impedance acquired by defibrillation pads. Resuscitation 2016, 99, 56–62. [Google Scholar] [CrossRef] [Green Version]
- Elola, A.; Aramendi, E.; Irusta, U.; Berve, P.O.; Wik, L. Multimodal algorithms for the classification of circulation states during out-of-hospital cardiac arrest. IEEE Trans. Biomed. Eng. 2021, 68, 1913–1922. [Google Scholar] [CrossRef] [PubMed]
- Alonso, E.; Eftestøl, T.; Aramendi, E.; Kramer-Johansen, J.; Skogvoll, E.; Nordseth, T. Beyond ventricular fibrillation analysis: Comprehensive waveform analysis for all cardiac rhythms occurring during resuscitation. Resuscitation 2014, 85, 1541–1548. [Google Scholar] [CrossRef]
- Lasa, H.; Irusta, U.; Eftestol, T.; Aramendi, E.; Rad, A.B.; Kramer-Johansen, J.; Wik, L. Multimodal Biosignal Analysis Algorithm for the Classification of Cardiac Rhythms During Resuscitation. In Proceedings of the 2020 Computing in Cardiology, Rimini, Italy, 13–16 September 2020; pp. 1–4. [Google Scholar]
- Urteaga Urizarbarrena, J.; Aramendi Ecenarro, E.; Elola Artano, A.; Irusta Zarandona, U.; Idris, A. Modelo predictivo del retorno de circulación espontánea en la parada cardiorrespiratoria utilizando el ECG y la impedancia torácica. In Proceedings of the Libro de Actas del XXXVIII Congreso Anual de la Sociedad Española de Ingeniería Biomédica CASEIB, Madrid, Spain, 25–27 November 2020. [Google Scholar]
- Ayala, U.; Eftestøl, T.; Alonso, E.; Irusta, U.; Aramendi, E.; Wali, S.; Kramer-Johansen, J. Automatic detection of chest compressions for the assessment of CPR-quality parameters. Resuscitation 2014, 85, 957–963. [Google Scholar] [CrossRef]
- Stecher, F.S.; Olsen, J.A.; Stickney, R.E.; Wik, L. Transthoracic impedance used to evaluate performance of cardiopulmonary resuscitation during out of hospital cardiac arrest. Resuscitation 2008, 79, 432–437. [Google Scholar] [CrossRef] [PubMed]
- Isasi, I.; Irusta, U.; Elola, A.; Aramendi, E.; Ayala, U.; Alonso, E.; Kramer-Johansen, J.; Eftestøl, T. A machine learning shock decision algorithm for use during piston-driven chest compressions. IEEE Trans. Biomed. Eng. 2018, 66, 1752–1760. [Google Scholar] [CrossRef]
- Isasi, I.; Irusta, U.; Elola, A.; Aramendi, E.; Eftestøl, T.; Kramer-Johansen, J.; Wik, L. A Robust Machine Learning Architecture for a Reliable ECG Rhythm Analysis during CPR. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 1903–1907. [Google Scholar]
- Ruiz, J.; Alonso, E.; Aramendi, E.; Kramer-Johansen, J.; Eftestøl, T.; Ayala, U.; González-Otero, D. Reliable extraction of the circulation component in the thoracic impedance measured by defibrillation pads. Resuscitation 2013, 84, 1345–1352. [Google Scholar] [CrossRef]
- Risdal, M.; Aase, S.O.; Kramer-Johansen, J.; Eftestol, T. Automatic identification of return of spontaneous circulation during cardiopulmonary resuscitation. IEEE Trans. Biomed. Eng. 2007, 55, 60–68. [Google Scholar] [CrossRef]
- Hamilton, P.S.; Tompkins, W.J. Quantitative investigation of QRS detection rules using the MIT/BIH arrhythmia database. IEEE Trans. Biomed. Eng. 1986, 12, 1157–1165. [Google Scholar] [CrossRef]
- Zhao, Z.; Särkkä, S.; Rad, A.B. Spectro-temporal ECG analysis for atrial fibrillation detection. In Proceedings of the 2018 IEEE 28th International Workshop on Machine Learning for Signal Processing (MLSP), Aalborg, Denmark, 17–20 September 2018; pp. 1–6. [Google Scholar]
- Elola, A.; Aramendi, E.; Irusta, U.; Del Ser, J.; Alonso, E.; Daya, M. ECG-based pulse detection during cardiac arrest using random forest classifier. Med. Biol. Eng. Comput. 2019, 57, 453–462. [Google Scholar] [CrossRef]
- Ruiz, J.M.; de Gauna, S.R.; González-Otero, D.M.; Saiz, P.; Gutiérrez, J.J.; Veintemillas, J.F.; Bastida, J.M.; Alonso, D. Circulation assessment by automated external defibrillators during cardiopulmonary resuscitation. Resuscitation 2018, 128, 158–163. [Google Scholar] [CrossRef]
- Chicote, B.; Irusta, U.; Aramendi, E.; Isasi, I.; Alonso, D.; Vicente, F.; Sanchez, M. Nonlinear energy operators for defibrillation shock outcome prediction. In Proceedings of the 2016 Computing in Cardiology Conference (CinC), Vancouver, BC, Canada, 11–14 September 2016; pp. 61–64. [Google Scholar]
- Jekova, I.; Krasteva, V. Real time detection of ventricular fibrillation and tachycardia. Physiol. Meas. 2004, 25, 1167. [Google Scholar] [CrossRef]
- Bos, R.; De Waele, S.; Broersen, P.M. Autoregressive spectral estimation by application of the Burg algorithm to irregularly sampled data. IEEE Trans. Instrum. Meas. 2002, 51, 1289–1294. [Google Scholar] [CrossRef] [Green Version]
- Elola, A.; Aramendi, E.; Rueda, E.; Irusta, U.; Wang, H.; Idris, A. Towards the Prediction of Rearrest during Out-of-Hospital Cardiac Arrest. Entropy 2020, 22, 758. [Google Scholar] [CrossRef]
- Breiman, L. Random forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Isasi, I.; Irusta, U.; Rad, A.B.; Aramendi, E.; Zabihi, M.; Eftestøl, T.; Kramer-Johansen, J.; Wik, L. Automatic cardiac rhythm classification with concurrent manual chest compressions. IEEE Access 2019, 7, 115147–115159. [Google Scholar] [CrossRef]
- Martínez, J.P.; Almeida, R.; Olmos, S.; Rocha, A.P.; Laguna, P. A wavelet-based ECG delineator: Evaluation on standard databases. IEEE Trans. Biomed. Eng. 2004, 51, 570–581. [Google Scholar] [CrossRef]
- Soar, J.; Böttiger, B.W.; Carli, P.; Couper, K.; Deakin, C.D.; Djärv, T.; Lott, C.; Olasveengen, T.; Paal, P.; Pellis, T.; et al. European Resuscitation Council Guidelines 2021: Adult advanced life support. Resuscitation 2021, 161, 115–151. [Google Scholar] [CrossRef] [PubMed]
- Sandroni, C.; De Santis, P.; D’Arrigo, S. Capnography during cardiac arrest. Resuscitation 2018, 132, 73–77. [Google Scholar] [CrossRef]
- Sanfilippo, F.; Serena, G.; Corredor, C.; Benedetto, U.; Maybauer, M.O.; Al-Subaie, N.; Madden, B.; Oddo, M.; Cecconi, M. Cerebral oximetry and return of spontaneous circulation after cardiac arrest: A systematic review and meta-analysis. Resuscitation 2015, 94, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Takegawa, R.; Hayashida, K.; Rolston, D.M.; Li, T.; Miyara, S.J.; Ohnishi, M.; Shiozaki, T.; Becker, L.B. Near-infrared spectroscopy assessments of regional cerebral oxygen saturation for the prediction of clinical outcomes in patients with cardiac arrest: A review of clinical impact, evolution, and future directions. Front. Med. 2020, 7, 736. [Google Scholar] [CrossRef]
- Breitkreutz, R.; Price, S.; Steiger, H.V.; Seeger, F.H.; Ilper, H.; Ackermann, H.; Rudolph, M.; Uddin, S.; Weigand, M.A.; Müller, E.; et al. Focused echocardiographic evaluation in life support and peri-resuscitation of emergency patients: A prospective trial. Resuscitation 2010, 81, 1527–1533. [Google Scholar] [CrossRef]
- Kim, Y.J.; Lee, Y.J.; Ryoo, S.M.; Sohn, C.H.; Ahn, S.; Seo, D.W.; Lim, K.S.; Kim, W.Y. Role of blood gas analysis during cardiopulmonary resuscitation in out-of-hospital cardiac arrest patients. Medicine 2016, 95, e3960. [Google Scholar] [CrossRef]
- Elola, A.; Aramendi, E.; Irusta, U.; Picón, A.; Alonso, E.; Owens, P.; Idris, A. Deep neural networks for ECG-based pulse detection during out-of-hospital cardiac arrest. Entropy 2019, 21, 305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isasi, I.; Irusta, U.; Aramendi, E.; Eftestøl, T.; Kramer-Johansen, J.K.J.; Wik, L. Rhythm Analysis during Cardiopulmonary Resuscitation Using Convolutional Neural Networks. Entropy 2020, 22, 595. [Google Scholar] [CrossRef]
- Jaureguibeitia, X.; Zubia, G.; Irusta, U.; Aramendi, E.; Chicote, B.; Alonso, D.; Larrea, A.; Corcuera, C. Shock Decision Algorithms for Automated External Defibrillators Based on Convolutional Networks. IEEE Access 2020, 8, 154746–154758. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ECG Features | ICC Features | ||||||
|---|---|---|---|---|---|---|---|
| Feature | faPEA | unPEA | AUC (%) | Feature | faPEA | unPEA | AUC (%) |
| Burg | 2.4 × (3.8 ×) | 5.6 × (1.1 ×) | 81.6 (5.6) | 1310 (2151) | 425 (1083) | 71.6 (3.4) | |
| AMSA | 31.2 (22.3) | 13.1 (14.1) | 81.3 (4.9) | IQR() | 22.1 (36.3) | 10.5 (30.2) | 66.5 (1.6) |
| 74.3 (166.0) | 8.3 (24.8) | 80.3 (8.1) | SNEO | 2930 (10,001) | 445 (4427) | 65.7 (7.8) | |
| IQR() | 1.1 (1.2) | 0.5 (0.6) | 72.6 (15.0) | 5131 (2783) | 2822 (5259) | 64.4 (7.5) | |
| IQR() | 0.31 (0.65) | 0.17 (0.29) | 71.0 (11.1) | IQR() | 84.2 (136.1) | 32.5 (88.9) | 64.3 (5.2) |
| SNEO | 0.21 (0.82) | 0.06 (0.20) | 71.0 (14.4) | IQR | 18.6 (26.9) | 7.2 (30.5) | 61.5 (10.3) |
| IQR | 0.17 (0.17) | 0.10 (0.10) | 68.8 (14.4) | IQR() | 150.9 (253.8) | 66.3 (247.5) | 54.9 (13.0) |
| IQR() | 1.3 (1.5) | 1.0 (1.0) | 65.2 (12.6) | Burg | 0.21 (1.9) | 0.05 (0.8) | 54.6 (14.4) |
| FuzzEn | 0.22 (0.13) | 0.23 (0.14) | 52.9 (20.4) | ||||
| No. Features | AUC (%) | BAC (%) | Se (%) | Sp (%) | |
|---|---|---|---|---|---|
| This study(ECG+TI) | 17 | 85.7 (8.6) | 77.8 (8.9) | 79.8 (11.3) | 77.3 (12.1) |
| This study(ECG) | 9 | 82.1 (9.7) | 73.5 (11.2) | 79.7 (14.1) | 69.0 (15.9) |
| This study, reduced(ECG+TI) | 7 | 85.7 (9.8) | 78.8 (9.8) | 80.1 (12.6) | 76.7 (13.6) |
| This study, reduced(ECG) | 4 | 83.2 (8.5) | 75.7 (10.7) | 78.9 (15.9) | 75.7 (11.4) |
| Urteaga et al. [26] | 2 | 82.0 (10.5) | 74.8 (11.3) | 77.0 (13.9) | 73.5 (14.6) |
| Alonso et al. [24] | 6 | 81.4 (10.3) | 74.4 (8.9) | 73.2 (15.1) | 77.8 (15.3) |
| HR [12] | 1 | 67.2 (12.9) | 62.1 (11.8) | 80.2 (14.5) | 45.1 (21.1) |
| QRS width [14] | 1 | 69.2 (12.9) | 67.8 (13.3) | 74.8 (20.2) | 61.5 (26.6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urteaga, J.; Aramendi, E.; Elola, A.; Irusta, U.; Idris, A. A Machine Learning Model for the Prognosis of Pulseless Electrical Activity during Out-of-Hospital Cardiac Arrest. Entropy 2021, 23, 847. https://doi.org/10.3390/e23070847
Urteaga J, Aramendi E, Elola A, Irusta U, Idris A. A Machine Learning Model for the Prognosis of Pulseless Electrical Activity during Out-of-Hospital Cardiac Arrest. Entropy. 2021; 23(7):847. https://doi.org/10.3390/e23070847
Chicago/Turabian StyleUrteaga, Jon, Elisabete Aramendi, Andoni Elola, Unai Irusta, and Ahamed Idris. 2021. "A Machine Learning Model for the Prognosis of Pulseless Electrical Activity during Out-of-Hospital Cardiac Arrest" Entropy 23, no. 7: 847. https://doi.org/10.3390/e23070847
APA StyleUrteaga, J., Aramendi, E., Elola, A., Irusta, U., & Idris, A. (2021). A Machine Learning Model for the Prognosis of Pulseless Electrical Activity during Out-of-Hospital Cardiac Arrest. Entropy, 23(7), 847. https://doi.org/10.3390/e23070847