
The Influence of Nordic Walking on Isokinetic Trunk Muscle Endurance and Sagittal Spinal Curvatures in Women after Breast Cancer Treatment: Age-Specific Indicators


Abstract
:1. Introduction
2. Materials and Methods
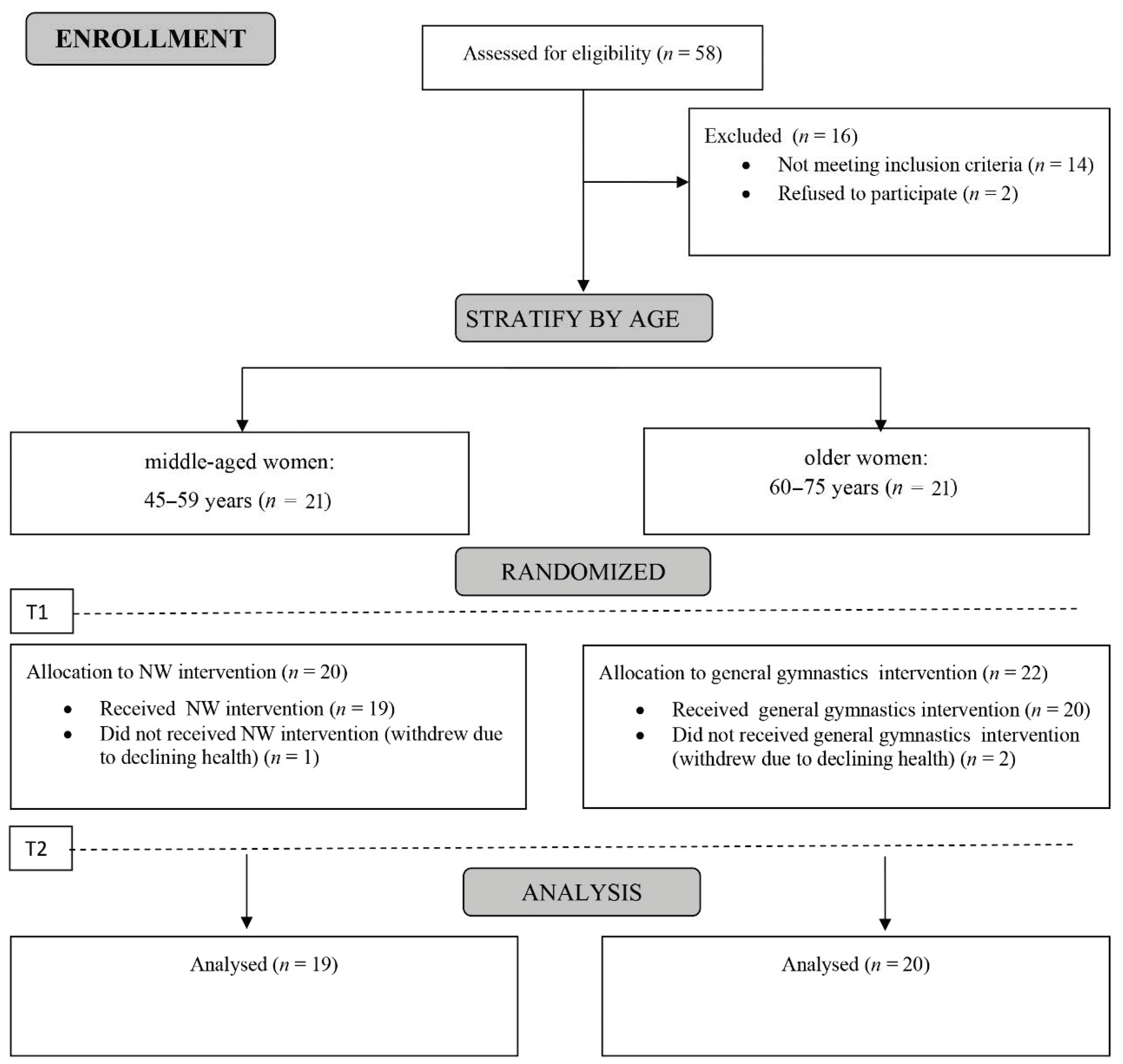
2.1. Study Group
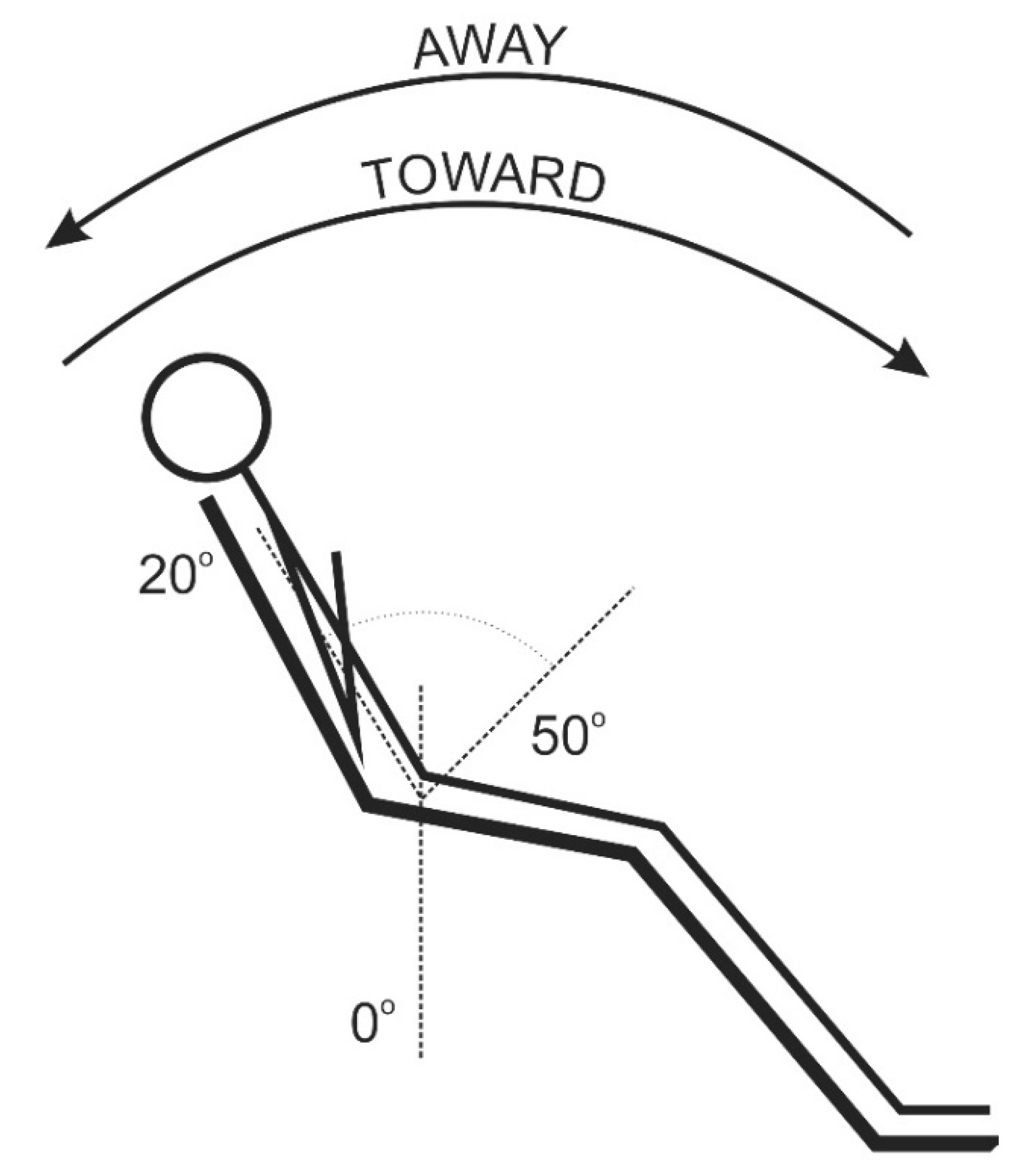
2.2. Trunk Muscle Endurance Testing
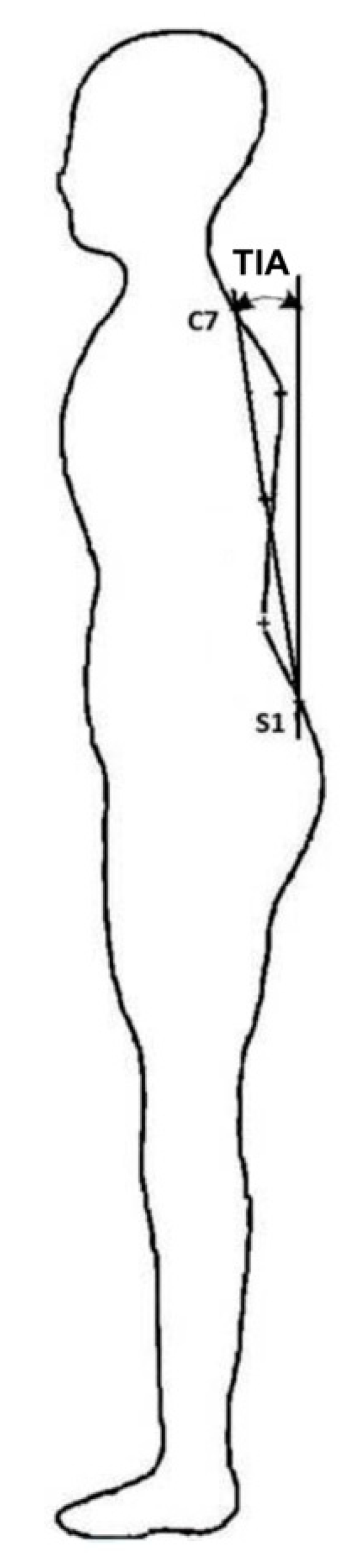
2.3. Sagittal Spinal Curvatures Examination
2.4. Training Intervention
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Milanovic, Z.; Jorgić, B.; Trajković, N.; Sporiš, G.; Pantelić, S.; James, N. Age-related decrease in physical activity and functional fitness among elderly men and women. Clin. Interv. Aging 2013, 8, 549–556. [Google Scholar] [CrossRef] [Green Version]
- Balzini, L.; Vannucchi, L.; Benvenuti, F.; Benucci, M.; Monni, M.; Cappozzo, A.; Stanhope, S.J. Clinical characteristics of flexed posture in elderly women. J. Am. Geriatr. Soc. 2003, 51, 1419–1426. [Google Scholar] [CrossRef]
- Aguirre, L.E.; Villareal, D.T. Physical exercise as therapy for frailty. In Frailty: Pathophysiology, Phenotype and Patient Care; Nestlé Nutr Inst Workshop Ser: Barcelona, Spain, 2015; Volume 83, pp. 83–92. [Google Scholar]
- Cleland, V.; Granados, A.; Crawford, D.; Winzenberg, T.; Ball, K. Effectiveness of interventions to promote physical activity among socioeconomically disadvantaged women: A systematic review and meta-analysis. Obes. Rev. 2012, 14, 197–212. [Google Scholar] [CrossRef] [Green Version]
- Li, R.; Xia, J.; I Zhang, X.; Gathirua-Mwangi, W.G.; Guo, J.; Li, Y.; McKenzie, S.; Song, Y. Associations of Muscle Mass and Strength with All-Cause Mortality among US Older Adults. Med. Sci. Sports Exerc. 2018, 50, 458–467. [Google Scholar] [CrossRef]
- Malicka, I.; Stefańska, M.; Rudziak, M.; Jarmoluk, P.; Pawłowska, K.; Szczepańska-Gieracha, J.; Woźniewski, M. The influence of Nordic walking exercise on upper extremity strength and the volume of lymphoedema in women following breast cancer treatment. Isokinet. Exerc. Sci. 2011, 19, 295–304. [Google Scholar] [CrossRef]
- Barbosa, J.D.A.N.; Amorim, M.H.C.; Zandonade, E.; Delaprane, M.L. Evaluation of body posture in women with breast cancer. Rev. Bras. Ginecol. Obstet 2013, 35, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Głowacka, I.; Nowikiewicz, T.; Hagner, W.; Nowacka, K.; Sowa, M.; Zegarski, W. Sagittal Plane Postural Changes in Female Patients with Breast Cancer after Different Surgical Techniques. Breast J. 2016, 23, 109–111. [Google Scholar] [CrossRef] [PubMed]
- Mangone, M.; Bernetti, A.; Agostini, F.; Paoloni, M.; De Cicco, F.A.; Capobianco, S.V.; Bai, A.V.; Bonifacino, A.; Santilli, V.; Paolucci, T. Changes in Spine Alignment and Postural Balance After Breast Cancer Surgery: A Rehabilitative Point of View. BioResearch Open Access 2019, 8, 121–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serel, S.; Tuzlalı, Z.Y.; Akkaya, Z.; Uzun, Ç.; Kaya, B.; Bayar, S. Physical Effects of Unilateral Mastectomy on Spine Deformity. Clin. Breast Cancer 2017, 17, 29–33. [Google Scholar] [CrossRef]
- Canário, A.C.G.; Cabral, P.U.L.; De Paiva, L.C.; Florencio, G.L.D.; Spyrides, M.H.; Gonçalves, A.K.D.S. Physical activity, fatigue and quality of life in breast cancer patients. Rev. Assoc. Médica Bras. 2016, 62, 38–44. [Google Scholar] [CrossRef] [Green Version]
- Malicka, I.; Hanuszkiewicz, J.; Woźniewski, M. Barriers of physical activity of women post breast cancer treatment in rural Poland. Heal. Care Women Int. 2019, 40, 682–695. [Google Scholar] [CrossRef]
- Courneya, K.S.; Friedenreich, C.M. Physical activity and cancer: An introduction. In Physical Activity and Cancer; Springer: Berlin/Heidelberg, Germany, 2010; pp. 1–10. [Google Scholar]
- Boccia, G.; Zoppirolli, C.; Bortolan, L.; Schena, F.; Pellegrini, B. Shared and task-specific muscle synergies of Nordic walking and conventional walking. Scand. J. Med. Sci. Sports 2017, 28, 905–918. [Google Scholar] [CrossRef] [Green Version]
- Farnsworth, M.; Burtscher, P. Nordic walking: Global trend set to make an impact on Australia’s health and fitness. J. Sci. Med. Sport 2010, 12, e3. [Google Scholar] [CrossRef]
- Kocur, P.; Wilk, M. Nordic Walking—Nowa forma ćwiczeń w rehabilitacji. Rehabil. Med. 2006, 10, 9–14. (In Polish) [Google Scholar]
- Park, H.S.; Lee, S.N.; Sung, D.H.; Choi, H.S.; Kwon, T.D.; Park, G.D. The effect of power Nordic walking on spine deformation and visual analog pain scale in elderly women with low back pain. J. Phys. Ther. Sci 2014, 26, 1809–1812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reuter, I.; Mehnert, S.; Leone, P.; Kaps, M.; Oechsner, M.; Engelhardt, M. Effects of a Flexibility and Relaxation Programme, Walking, and Nordic Walking on Parkinson’s Disease. J. Aging Res. 2011, 2011, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Hanuszkiewicz, J.M.; Woźniewski, M.; Malicka, I. The influence of Nordic walking on isokinetic trunk muscle endurance and sagittal spinal curvatures in women after breast cancer treatment. Acta Bioeng. Biomech. 2020, 22, 22. [Google Scholar] [CrossRef]
- Manikowska, F.; Hojan, K.; Chen, P.-J.B.; Jóźwiak, M.; Jóźwiak, A. The gait pattern in post-menopausal women. Pilot study. Ortop. Traumatol. Rehabil. 2013, 15, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Barczyk-Pawelec, K.; Dziubek, W.; Piechura, J.R.; Rożek, K. Correlations between somatic features, anteroposterior spinal curvatures and trunk muscle strength in schoolchildren. Acta Bioeng. Biomech. 2017, 19, 133–139. [Google Scholar] [CrossRef]
- Elsayed, W.; Farrag, A.; Muaidi, Q.; Almulhim, N. Relationship between sagittal spinal curves geometry and isokinetic trunk muscle strength in adults. Eur. Spine J. 2018, 27, 2014–2022. [Google Scholar] [CrossRef]
- Hanuszkiewicz, J.M.; Woźniewski, M.; Malicka, I. The relationship between sagittal spinal curvatures and isokinetic trunk muscle endurance after aquatic exercise training in survivors of breast cancer. Acta Bioeng. Biomech. 2020, 22, 21–30. [Google Scholar] [CrossRef]
- Rabelo, M.; Fachin-Martins, E. Inter-rater and test/retest reliabilities of the isokinetic measurements: Assessing strength and endurance of the trunk muscles in two different protocols for able-bodied and post-stroke hemiparesis. Top. Stroke Rehabil. 2018, 25, 1–8. [Google Scholar] [CrossRef]
- Quintino, L.F.; Franco, J.; Gusmão, A.F.M.; Silva, P.F.D.S.; Faria, C.D.C.D.M. Trunk flexor and extensor muscle performance in chronic stroke patients: A case–control study. Braz. J. Phys. Ther. 2018, 22, 231–237. [Google Scholar] [CrossRef]
- Reid, K.F.; Fielding, R.A. Skeletal muscle power: A critical determinant of physical functioning in older adults. Exerc. Sport Sci. Rev. 2012, 40, 4–12. [Google Scholar] [CrossRef]
- Anwajler, J.; Barczyk, K.; Wojna, D.; Ostrowska, B.; Skolimowski, T. Characteristics of body posture in the sagittal plane in elderly people-residents of social care centres. Gerontologia Polska 2010, 18, 134–139. [Google Scholar]
- Barczyk-Pawelec, K.; Sipko, T. Active self-correction of spinal posture in pain-free women in response to the command “straighten your back”. Women Health 2016, 57, 1098–1114. [Google Scholar] [CrossRef]
- Zoffoli, L.; Lucertini, F.; Federici, A.; Ditroilo, M. Trunk muscles activation during pole walking vs. walking performed at different speeds and grades. Gait Posture 2016, 46, 57–62. [Google Scholar] [CrossRef]
- Fritschi, J.O.; Brown, W.J.; Laukkanen, R.; Van Uffelen, J.G.Z. The effects of pole walking on health in adults: A systematic review. Scand. J. Med. Sci. Sports 2012, 22, e70–e78. [Google Scholar] [CrossRef]
- Schmitz, K.H.; Courneya, K.S.; Matthews, C.; Demark-Wahnefried, W.; Galvão, D.A.; Pinto, B.M.; Irwin, M.L.; Wolin, K.Y.; Segal, R.J.; Lucia, A.; et al. American College of Sports Medicine Roundtable on Exercise Guidelines for Cancer Survivors. Med. Sci. Sports Exerc. 2010, 42, 1409–1426. [Google Scholar] [CrossRef]
- De Groef, A.; Van Kampen, M.; Dieltjens, E.; Christiaens, M.R.; Neven, P.; Geraerts, I.; Devoogdt, N. Effectiveness of postoperative physical therapy for upper-limb impairments after breast cancer treatment: A systematic review. Arch. Phys. Med. Rehabil. 2015, 96, 1140–1153. [Google Scholar] [CrossRef]
- Hojan, K.; Manikowska, F.; Chen, B.P.-J.; Lin, C.-C. The influence of an external breast prosthesis on the posture of women after mastectomy. J. Back Musculoskelet. Rehabil. 2016, 29, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Montezuma, T.; Guirro, E.C.D.O.; Vaz, M.M.D.O.L.L.; Vernal, S. Changes in Postural Control in Mastectomized Women. J. Cancer Ther. 2014, 5, 493–499. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Session | Nordic Walking (NW) | General Gymnastics |
|---|---|---|
| Warm-up (5 min) | Aerobic activities, mobility exercises with breathing exercises | |
| Main part (35 min) | Learning and improving walking technique with the use of NW poles | General improving exercises using upper and lower limbs, back and abdominal strengthening exercises, balance and coordination exercises |
| Cool-down (5 min) | Stretching with breathing exercises | |
| Session | Distance (m) | Rest Period | Target HR Zone |
|---|---|---|---|
| 1–4 | 6 × 400 = 2400 | 5 × 30 s | 65–70% HR max |
| 5–8 | 5 × 560 = 2800 | 4 × 30 s | |
| 9–12 | 4 × 800 = 3200 | 3 × 30 s | |
| 13–16 | 3 × 1200 = 3600 | 2 × 30 s |
| Somatic Parameters | Nordic Walking n = 19 | General Gymnastics n = 20 | ||
|---|---|---|---|---|
| <60 n = 11 | >60 n = 8 | <60 n = 9 | >60 n = 11 | |
| Age (years) | 53.09 ± 4.57 | 65.25 ± 2.82 * | 52.7 ± 4.46 | 64.82 ± 4.28 * |
| Body height (cm) | 161.27 ± 4.27 | 158.37 ± 7.96 | 162.00 ± 4.95 | 156.18 ± 5.06 |
| Body mass (kg) | 72.64 ± 10.10 | 77.62 ± 8.47 | 71.89 ± 4.46 | 75.91 ± 10.89 |
| Time since surgery (years) | 4.20 ± 3.99 | 8.75 ± 6.96 | 4.44 ± 3.64 | 7.54 ± 5.03 |
| Sagittal Spinal Curvatures Parameters | Pre- | Post- | Within Group Change Scores | p-Value the LSD Post Hoc Test | p-Value Group × Time × Age Interaction (MANOVA) | |
|---|---|---|---|---|---|---|
| Intervention | ||||||
| Alpha, lumbosacral angle (°) | ||||||
| Nordic walking | <60 | 16.06 ± 4.50 | 13.99 ± 5.60 | −2.07 (−4.10, −0.04) | 0.17 | 0.77 |
| >60 | 16.75 ± 4.44 | 13.92 ± 5.36 | −2.83 (−9.29, 3.64) | 0.11 | ||
| General gymnastics | <60 | 16.53 ± 3.24 | 16.15 ± 5.16 | −0.38 (−3.72, 2.96) | 0.82 | |
| >60 | 15.64 ± 7.36 | 15.45 ± 7.10 | −0.19 (−3.15, 2.76) | 0.90 | ||
| Beta, thoracolumbar angle (°) | ||||||
| Nordic walking | <60 | 13.16 ± 1.82 | 11.81 ± 1.44 | −1.35 (−2.54, −0.17) | 0.13 | 0.54 |
| >60 | 11.92 ± 6.97 | 9.94 ± 5.30 | −1.98 (−5.09, 1.12) | 0.06 | ||
| General gymnastics | <60 | 12.38 ± 3.81 | 11.54 ± 4.80 | −0.84 (−3.09, 1.42) | 0.40 | |
| >60 | 11.34 ± 4.58 | 11.04 ± 5.49 | −0.30 (−2.50, 1.90) | 0.74 | ||
| Gamma, upper thoracic angle (°) | ||||||
| Nordic walking | <60 | 17.06 ± 3.48 | 14.77 ± 4.39 | −2.29 (−4.54, −0.04) | <0.01 * | 0.06 |
| >60 | 16.84 ± 2.58 | 17.01 ± 2.73 | 0.17 (−1.04, 1.39) | 0.86 | ||
| General gymnastics | <60 | 16.31 ± 3.81 | 16.69 ± 4.14 | 0.38 (−1.04, 1.80) | 0.49 | |
| >60 | 19.79 ± 3.35 | 19.23 ± 3.61 | −0.56 (−2.72, 1.60) | 0.68 | ||
| TIA, trunk inclination angle (°) | ||||||
| Nordic walking | <60 | −2.48 ± 2.50 | −1.94 ± 2.63 | 0.54 (−0.21, 1.28) | 0.25 | 0.03 * |
| >60 | −2.76 ± 3.34 | −4.09 ± 2.63 | −1.33 (−2.76, 0.11) | 0.02 * | ||
| General gymnastics | <60 | −3.21 ± 3.90 | −3.43 ± 4.17 | −0.22 (−1.42, 0.97) | 0.66 | |
| >60 | −4.41 ± 2.91 | −4.30 ± 3.53 | 0.11 (−1.04, 1.28) | 0.80 | ||
| Trunk Muscle Function | Pre- | Post- | Within Group Change Scores | p-Value the LSD Post Hoc Test | p-Value Group × Time × Age Interaction (MANOVA) | |
|---|---|---|---|---|---|---|
| Intervention | ||||||
| Total work, trunk extensors (J) | ||||||
| Nordic walking | <60 | 236.85 ± 216.23 | 510.73 ± 449.61 | 273.88 (116.85, 330.91) | <0.01 * | 0.23 |
| >60 | 403.44 ± 353.80 | 545.32 ± 255.92 | 141,88 (−160.43, 344.18) | 0.17 | ||
| General gymnastics | <60 | 211.64 ± 204.67 | 206.18 ± 183.06 | −5.46 (−67.49, 56.55) | 0.95 | |
| >60 | 168.25 ± 70.72 | 253.39 ± 200.92 | 85.14 (−82.01, 252.28) | 0.33 | ||
| Total work, trunk flexors (J) | ||||||
| Nordic walking | <60 | 247.52 ± 199.37 | 436.11 ± 309.96 | 188.59 (84.28, 292.90) | <0.01 * | 0.63 |
| >60 | 273.38 ± 228.43 | 447.15 ± 159.75 | 173.77 (−40.46, 388.01) | <0.01 * | ||
| General gymnastics | <60 | 197.78 ± 133.11 | 230.21 ± 118.90 | 32.43 (−31.47, 96.34) | 0.55 | |
| >60 | 173.06 ± 80.81 | 240.67 ± 190.90 | 67.61 (−15.34, 150.55) | 0.17 | ||
| Average power, trunk extensors (W) | ||||||
| Nordic walking | <60 | 12.55 ± 11.72 | 30.09 ± 27.02 | 17.54 (6.36, 28.71) | <0.01 * | 0.42 |
| >60 | 22.49 ± 20.99 | 33.81 ± 21.26 | 11.32 (−14.18, 36.83) | 0.08 | ||
| General gymnastics | <60 | 11.18 ± 10.00 | 11.91 ± 10.22 | 0.73 (−4.44, 5.91) | 0.90 | |
| >60 | 9.17 ± 4.58 | 13.04 ± 12.64 | 3.87 (−3.74, 11.48) | 0.47 | ||
| Average power, trunk flexors (W) | ||||||
| Nordic walking | <60 | 13.30 ± 9.70 | 23.35 ± 16.30 | 10.05 (4.52, 15.59) | <0.01 * | 0.83 |
| >60 | 15.83 ± 13.93 | 27.95 ± 12.51 | 12.12 (−1.40, 25.63) | <0.01 * | ||
| General gymnastics | <60 | 9.9 ± 7.43 | 12.30 ± 7.43 | 2.40 (−1.15, 5.84) | 0.46 | |
| >60 | 9.89 ± 6.50 | 13.00 ± 11.34 | 3.11 (−1.54, 7.76) | 0.28 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hanuszkiewicz, J.; Woźniewski, M.; Malicka, I. The Influence of Nordic Walking on Isokinetic Trunk Muscle Endurance and Sagittal Spinal Curvatures in Women after Breast Cancer Treatment: Age-Specific Indicators. Int. J. Environ. Res. Public Health 2021, 18, 2409. https://doi.org/10.3390/ijerph18052409
Hanuszkiewicz J, Woźniewski M, Malicka I. The Influence of Nordic Walking on Isokinetic Trunk Muscle Endurance and Sagittal Spinal Curvatures in Women after Breast Cancer Treatment: Age-Specific Indicators. International Journal of Environmental Research and Public Health. 2021; 18(5):2409. https://doi.org/10.3390/ijerph18052409
Chicago/Turabian StyleHanuszkiewicz, Justyna, Marek Woźniewski, and Iwona Malicka. 2021. "The Influence of Nordic Walking on Isokinetic Trunk Muscle Endurance and Sagittal Spinal Curvatures in Women after Breast Cancer Treatment: Age-Specific Indicators" International Journal of Environmental Research and Public Health 18, no. 5: 2409. https://doi.org/10.3390/ijerph18052409