
Virtual Reality as a Promising Tool Supporting Oncological Treatment in Breast Cancer



Abstract
1. Introduction
Virtual Reality
2. Materials and Methods
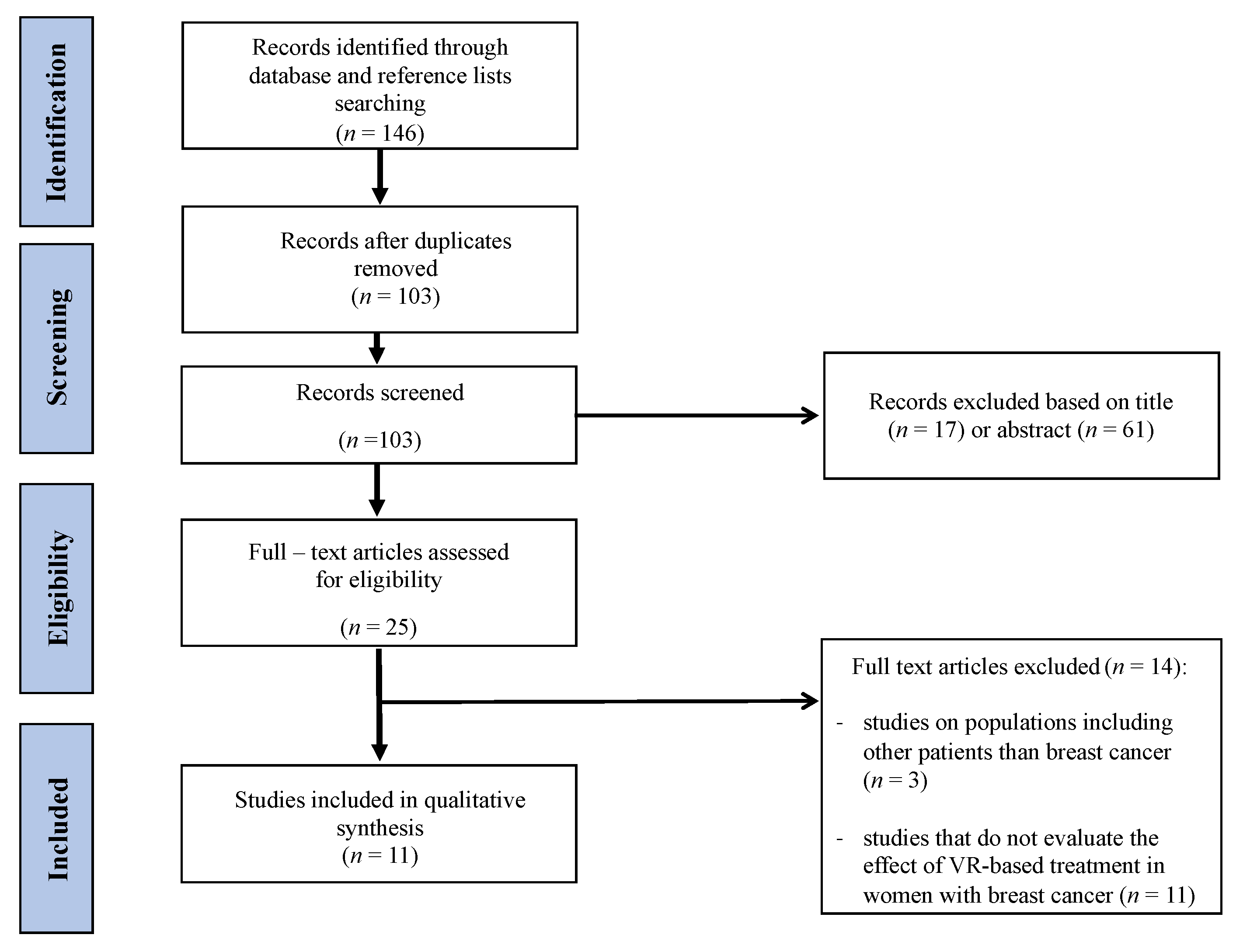
2.1. Search Strategy
2.2. Outcome Measure
2.2.1. Primary Outcome
2.2.2. Secondary Outcome Measure
2.3. Data Collection and Analysis
2.4. Inclusion and Exclusion Criteria for the Articles
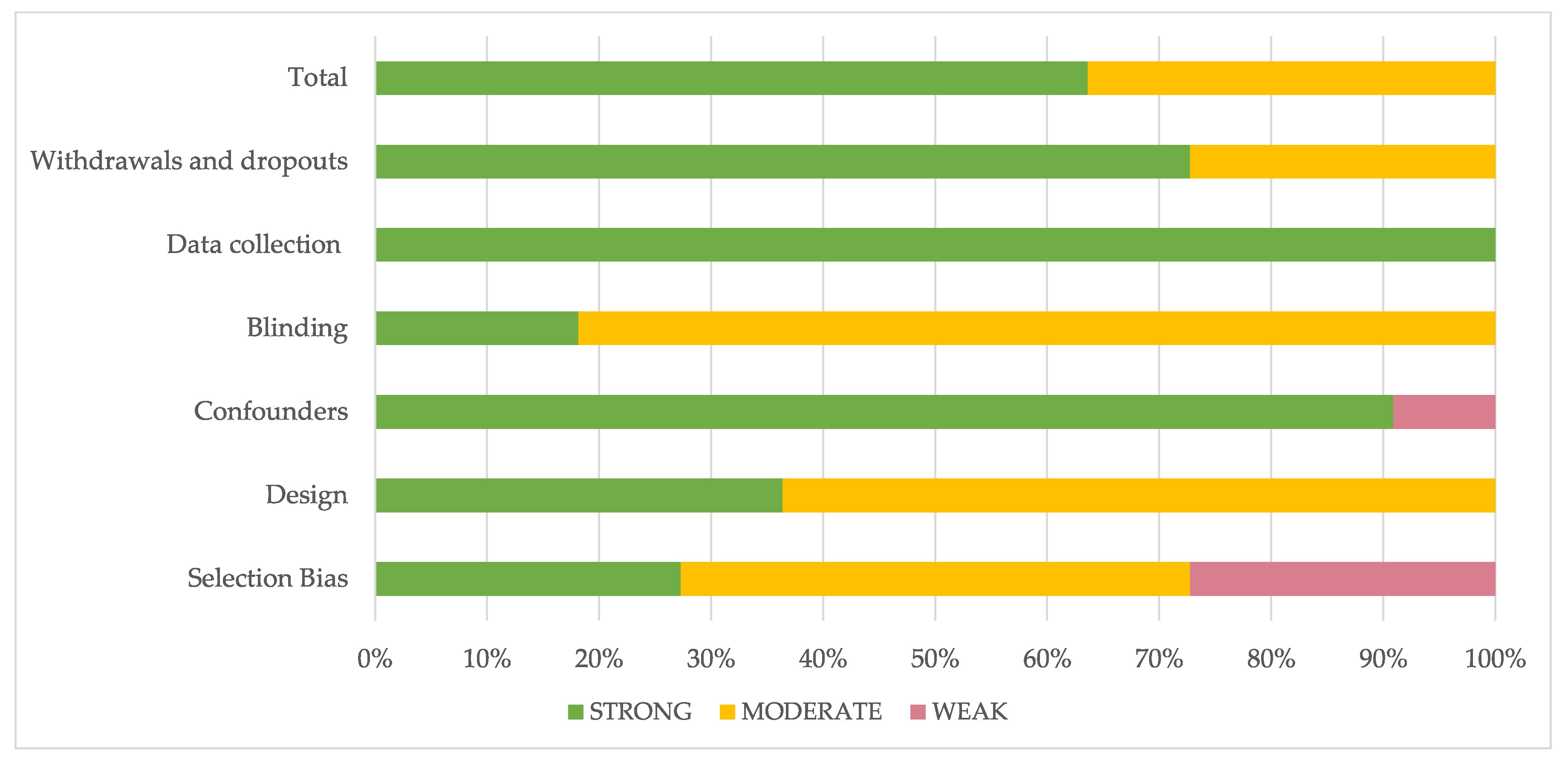
2.5. Quality Assessment
3. Results
3.1. Evaluation of the Study
3.2. Methodological Quality
3.3. Characteristics of Study Participants
3.4. Characteristics of VR Interventions, Outcome Measure, and Study Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McGuire, A.; Brown, J.A.L.; Malone, C.; McLaughlin, R.; Kerin, M.J. Effects of age on the detection and management of breast cancer. Cancers 2015, 7, 908–929. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2016. CA Cancer J. Clin. 2016, 66, 7–30. [Google Scholar] [CrossRef]
- Chirico, A.; Lucidi, F.; Mallia, L.; D’Aiuto, M.; Merluzzi, T.V. Indicators of distress in newly diagnosed breast cancer patients. PeerJ 2015, 3, e1107. [Google Scholar] [CrossRef] [PubMed]
- Hill, J.; Holcombe, C.; Clark, L.; Boothby, M.R.K.; Hincks, A.; Fisher, J.; Tufail, S.; Salmon, P. Predictors of onset of depression and anxiety in the year after diagnosis of breast cancer. Psychol. Med. 2011, 41, 1429–1436. [Google Scholar] [CrossRef] [PubMed]
- Sivabalan, T.; Upasani, S.V. Effectiveness of Nursing Interventions on Physical and Psychological Outcome among Cancer Patients Undergoing Chemotherapy. 2016. Available online: https://www.semanticscholar.org/paper/Effectiveness-of-Nursing-Interventions-on-Physical-Sivabalan-Upasani/a6cb27b1341777e2f6fedae26fe44de2c1010ea1 (accessed on 10 February 2021).
- Zaidi, S.; Hussain, S.; Verma, S.; Veqar, Z.; Khan, A.; Nazir, S.U.; Singh, N.; Moiz, J.A.; Tanwar, P.; Srivastava, A.; et al. Efficacy of Complementary Therapies in the Quality of Life of Breast Cancer Survivors. Front. Oncol. 2017, 7, 326. [Google Scholar] [CrossRef]
- Mijwel, S.; Backman, M.; Bolam, K.A.; Olofsson, E.; Norrbom, J.; Bergh, J.; Sundberg, C.J.; Wengström, Y.; Rundqvist, H. Highly favorable physiological responses to concurrent resistance and high-intensity interval training during chemotherapy: The OptiTrain breast cancer trial. Breast Cancer Res. Treat. 2018, 169, 93–103. [Google Scholar] [CrossRef]
- Stubblefield, M.D.; Keole, N. Upper body pain and functional disorders in patients with breast cancer. PM&R 2014, 6, 170–183. [Google Scholar] [CrossRef]
- Khan, J.S.; Ladha, K.S.; Abdallah, F.; Clarke, H. Treating Persistent Pain After Breast Cancer Surgery. Drugs 2020, 80, 23–31. [Google Scholar] [CrossRef]
- Tantawy, S.A.; Kamel, D.M. The effect of kinesio taping with exercise compared with exercise alone on pain, range of motion, and disability of the shoulder in postmastectomy females: A randomized control trial. J. Phys. Ther. Sci. 2016, 28, 3300–3305. [Google Scholar] [CrossRef][Green Version]
- Wilson, D.J. Exercise for the Patient after Breast Cancer Surgery. Semin. Oncol. Nurs. 2017, 33, 98–105. [Google Scholar] [CrossRef]
- De Groef, A.; van Kampen, M.; Vervloesem, N.; De Geyter, S.; Christiaens, M.-R.; Neven, P.; Vos, L.; De Vrieze, T.; Geraerts, I.; Devoogdt, N. Myofascial techniques have no additional beneficial effects to a standard physical therapy programme for upper limb pain after breast cancer surgery: A randomized controlled trial. Clin. Rehabil. 2017, 31, 1625–1635. [Google Scholar] [CrossRef]
- Rafn, B.S.; Hung, S.; Hoens, A.M.; McNeely, M.L.; Singh, C.A.; Kwan, W.; Dingee, C.; McKevitt, E.C.; Kuusk, U.; Pao, J.; et al. Prospective surveillance and targeted physiotherapy for arm morbidity after breast cancer surgery: A pilot randomized controlled trial. Clin. Rehabil. 2018, 32, 811–826. [Google Scholar] [CrossRef]
- Fernandes, A.F.C.; Vidal, G.O.; Moreira, C.B.; Silva, T.B.D.C.E.; Valentim, P.N.R.; Santos, M.C.L. Lymphedema in the Mastectomy Postoperative Period: An Integrative Literature Review. ABCR 2013, 2, 154–160. [Google Scholar] [CrossRef][Green Version]
- Smoot, B.; Wong, J.; Cooper, B.; Wanek, L.; Topp, K.; Byl, N.; Dodd, M. Upper extremity impairments in women with or without lymphedema following breast cancer treatment. J. Cancer Surviv. 2010, 4, 167–178. [Google Scholar] [CrossRef]
- Arman, N.; Tarakci, E.; Tarakci, D.; Kasapcopur, O. Effects of Video Games-Based Task-Oriented Activity Training (Xbox 360 Kinect) on Activity Performance and Participation in Patients with Juvenile Idiopathic Arthritis: A Randomized Clinical Trial. Am. J. Phys. Med. Rehabil. 2019, 98, 174–181. [Google Scholar] [CrossRef]
- Yang, Z.; Rafiei, M.H.; Hall, A.; Thomas, C.; Midtlien, H.A.; Hasselbach, A.; Adeli, H.; Gauthier, L.V. A Novel Methodology for Extracting and Evaluating Therapeutic Movements in Game-Based Motion Capture Rehabilitation Systems. J. Med. Syst. 2018, 42, 255. [Google Scholar] [CrossRef]
- Glennon, C.; McElroy, S.F.; Connelly, L.M.; Mische Lawson, L.; Bretches, A.M.; Gard, A.R.; Newcomer, L.R. Use of Virtual Reality to Distract From Pain and Anxiety. Oncol. Nurs. Forum 2018, 45, 545–552. [Google Scholar] [CrossRef] [PubMed]
- Indovina, P.; Barone, D.; Gallo, L.; Chirico, A.; de Pietro, G.; Giordano, A. Virtual Reality as a Distraction Intervention to Relieve Pain and Distress During Medical Procedures: A Comprehensive Literature Review. Clin. J. Pain 2018, 34, 858–877. [Google Scholar] [CrossRef] [PubMed]
- Zeng, N.; Pope, Z.; Lee, J.E.; Gao, Z. Virtual Reality Exercise for Anxiety and Depression: A Preliminary Review of Current Research in an Emerging Field. J. Clin. Med. 2018, 7, 42. [Google Scholar] [CrossRef] [PubMed]
- Biocca, F. Virtual Reality Technology: A Tutorial. J. Commun. 1992, 42, 23–72. [Google Scholar] [CrossRef]
- Mesa-Gresa, P.; Gil-Gómez, H.; Lozano-Quilis, J.-A.; Gil-Gómez, J.-A. Effectiveness of Virtual Reality for Children and Adolescents with Autism Spectrum Disorder: An Evidence-Based Systematic Review. Sensors 2018, 18, 2486. [Google Scholar] [CrossRef] [PubMed]
- Chirico, A.; Lucidi, F.; de Laurentiis, M.; Milanese, C.; Napoli, A.; Giordano, A. Virtual Reality in Health System: Beyond Entertainment. A Mini-Review on the Efficacy of VR During Cancer Treatment. J. Cell. Physiol. 2016, 231, 275–287. [Google Scholar] [CrossRef]
- Sharar, S.R.; Alamdari, A.; Hoffer, C.; Hoffman, H.G.; Jensen, M.P.; Patterson, D.R. Circumplex Model of Affect: A Measure of Pleasure and Arousal During Virtual Reality Distraction Analgesia. Games Health J. 2016, 5, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Jennett, C.; Cox, A.L.; Cairns, P.; Dhoparee, S.; Epps, A.; Tijs, T.; Walton, A. Measuring and defining the experience of immersion in games. Int. J. Hum. Comput. Stud. 2008, 66, 641–661. [Google Scholar] [CrossRef]
- Napolitano, M.A.; Hayes, S.; Russo, G.; Muresu, D.; Giordano, A.; Foster, G.D. Using avatars to model weight loss behaviors: Participant attitudes and technology development. J. Diabetes Sci. Technol. 2013, 7, 1057–1065. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- National Collaborating Centre for Methods and Tools. Quality assessment tool for quantitative studies. Available online: https://www.nccmt.ca/knowledge-repositories/search/14 (accessed on 15 March 2021).
- Atef, D.; Elkeblawy, M.M.; El-Sebaie, A.; Abouelnaga, W.A.I. A quasi-randomized clinical trial: Virtual reality versus proprioceptive neuromuscular facilitation for postmastectomy lymphedema. J. Egypt. Natl. Cancer Inst. 2020, 32, 29. [Google Scholar] [CrossRef] [PubMed]
- Chirico, A.; Maiorano, P.; Indovina, P.; Milanese, C.; Giordano, G.G.; Alivernini, F.; Iodice, G.; Gallo, L.; de Pietro, G.; Lucidi, F.; et al. Virtual reality and music therapy as distraction interventions to alleviate anxiety and improve mood states in breast cancer patients during chemotherapy. J. Cell. Physiol. 2020, 235, 5353–5362. [Google Scholar] [CrossRef] [PubMed]
- Feyzioğlu, Ö.; Dinçer, S.; Akan, A.; Algun, Z.C. Is Xbox 360 Kinect-based virtual reality training as effective as standard physiotherapy in patients undergoing breast cancer surgery? Support. Care Cancer 2020, 28, 4295–4303. [Google Scholar] [CrossRef]
- House, G.; Burdea, G.; Grampurohit, N.; Polistico, K.; Roll, D.; Damiani, F.; Hundal, J.; Demesmin, D. A feasibility study to determine the benefits of upper extremity virtual rehabilitation therapy for coping with chronic pain post-cancer surgery. Br. J. Pain 2016, 10, 186–197. [Google Scholar] [CrossRef]
- McGarvey, E.L.; Leon-Verdin, M.; Baum, L.D.; Bloomfield, K.; Brenin, D.R.; Koopman, C.; Acton, S.; Clark, B.; Parker, B.E. An evaluation of a computer-imaging program to prepare women for chemotherapy-related alopecia. Psychooncology 2010, 19, 756–766. [Google Scholar] [CrossRef]
- Bani Mohammad, E.; Ahmad, M. Virtual reality as a distraction technique for pain and anxiety among patients with breast cancer: A randomized control trial. Palliat. Supportive Care 2019, 17, 29–34. [Google Scholar] [CrossRef]
- Piejko, L.; Niewolak, K.; Fielek, D.; Pecyna, P.; Chełminiak, D.; Zieliński, P.; Kobylarz, K.; Grzmilas, M.; Cygoń, K.; Stanisławski, P.; et al. Medical Resort Treatment Extended with Modern Feedback Exercises Using Virtual Reality Improve Postural Control in Breast Cancer Survivors. Preliminary Study. Acta Balneol. 2020, 62, 92–98. [Google Scholar] [CrossRef]
- Schneider, S.M.; Ellis, M.; Coombs, W.T.; Shonkwiler, E.L.; Folsom, L.C. Virtual reality intervention for older women with breast cancer. Cyberpsychol. Behav. 2003, 6, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Schneider, S.M.; Prince-Paul, M.; Allen, M.J.; Silverman, P.; Talaba, D. Virtual reality as a distraction intervention for women receiving chemotherapy. Oncol. Nurs. Forum 2004, 31, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Schneider, S.M.; Hood, L.E. Virtual reality: A distraction intervention for chemotherapy. Oncol. Nurs. Forum 2007, 34, 39–46. [Google Scholar] [CrossRef]
- Schneider, S.M.; Kisby, C.K.; Flint, E.P. Effect of virtual reality on time perception in patients receiving chemotherapy. Support. Care Cancer 2011, 19, 555–564. [Google Scholar] [CrossRef]
- Costa, M.T.S.; Vieira, L.P.; Barbosa, E.D.O.; Mendes Oliveira, L.; Maillot, P.; Otero Vaghetti, C.A.; Giovani Carta, M.; Machado, S.; Gatica-Rojas, V.; Monteiro-Junior, R.S. Virtual Reality-Based Exercise with Exergames as Medicine in Different Contexts: A Short Review. Clin. Pract. Epidemiol. Ment. Health 2019, 15, 74. [Google Scholar] [CrossRef] [PubMed]
- de Luca, R.; Portaro, S.; Le Cause, M.; Domenico, C.; Maggio, M.G.; Cristina Ferrera, M.; Giuffrè, G.; Bramanti, A.; Calabrò, R.S. Cognitive rehabilitation using immersive virtual reality at young age: A case report on traumatic brain injury. Appl. Neuropsychol. Child 2020, 9, 282–287. [Google Scholar] [CrossRef]
- de Luca, R.; Russo, M.; Naro, A.; Tomasello, P.; Leonardi, S.; Santamaria, F.; Desireè, L.; Bramanti, A.; Silvestri, G.; Bramanti, P.; et al. Effects of virtual reality-based training with BTs-Nirvana on functional recovery in stroke patients: Preliminary considerations. Int. J. Neurosci. 2018, 128, 791–796. [Google Scholar] [CrossRef]
- Maresca, G.; Maggio, M.G.; Buda, A.; La Rosa, G.; Manuli, A.; Bramanti, P.; de Luca, R.; Calabrò, R.S. A novel use of virtual reality in the treatment of cognitive and motor deficit in spinal cord injury: A case report. Medicine 2018, 97, e13559. [Google Scholar] [CrossRef] [PubMed]
- Russo, M.; Dattola, V.; de Cola, M.C.; Logiudice, A.L.; Porcari, B.; Cannavò, A.; Sciarrone, F.; de Luca, R.; Molonia, F.; Sessa, E.; et al. The role of robotic gait training coupled with virtual reality in boosting the rehabilitative outcomes in patients with multiple sclerosis. Int. J. Rehabil. Res. 2018, 41, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Maggio, M.G.; Maresca, G.; de Luca, R.; Stagnitti, M.C.; Porcari, B.; Ferrera, M.C.; Galletti, F.; Casella, C.; Manuli, A.; Calabrò, R.S. The Growing Use of Virtual Reality in Cognitive Rehabilitation: Fact, Fake or Vision? A Scoping Review. J. Natl. Med. Assoc. 2019, 111, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Zengin, S.; Kabul, S.; Al, B.; Sarcan, E.; Doğan, M.; Yildirim, C. Effects of music therapy on pain and anxiety in patients undergoing port catheter placement procedure. Complementary Ther. Med. 2013, 21, 689–696. [Google Scholar] [CrossRef]
- Espinoza, M.; Baños, R.M.; García-Palacios, A.; Cervera, J.M.; Esquerdo, G.; Barrajón, E.; Botella, C. Promotion of emotional wellbeing in oncology inpatients using VR. Stud. Health Technol. Inform. 2012, 181, 53–57. [Google Scholar] [PubMed]
- Rosa, G.M.M.V. Efeito da realidade virtual na recuperação da função motora do membro superior em paciente com AVC crônico. Fisioter. Bras. 2016, 13, 380–383. [Google Scholar] [CrossRef]
- Taddei, F.; Bultrini, A.; Spinelli, D.; Di Russo, F. Neural correlates of attentional and executive processing in middle-age fencers. Med. Sci. Sports Exerc. 2012, 44, 1057–1066. [Google Scholar] [CrossRef] [PubMed]
- Booth, V.; Masud, T.; Connell, L.; Bath-Hextall, F. The effectiveness of virtual reality interventions in improving balance in adults with impaired balance compared with standard or no treatment: A systematic review and meta-analysis. Clin. Rehabil. 2014, 28, 419–431. [Google Scholar] [CrossRef]
- Maillot, P.; Perrot, A.; Hartley, A. Effects of interactive physical-activity video-game training on physical and cognitive function in older adults. Psychol. Aging 2012, 27, 589–600. [Google Scholar] [CrossRef]
- You, S.H.; Jang, S.H.; Kim, Y.-H.; Hallett, M.; Ahn, S.H.; Kwon, Y.-H.; Kim, J.H.; Lee, M.Y. Virtual reality-induced cortical reorganization and associated locomotor recovery in chronic stroke: An experimenter-blind randomized study. Stroke 2005, 36, 1166–1171. [Google Scholar] [CrossRef]
- Cheville, A.L. Adjunctive Rehabilitation Approaches to Oncology; Elsevier Health Sciences: Philadelphia, PA, USA, 2017. [Google Scholar]
- Nekhlyudov, L.; Duijts, S.; Hudson, S.V.; Jones, J.M.; Keogh, J.; Love, B.; Lustberg, M.; Smith, K.C.; Tevaarwerk, A.; Yu, X.; et al. Addressing the needs of cancer survivors during the COVID-19 pandemic. J. Cancer Surviv. 2020, 14, 601–606. [Google Scholar] [CrossRef] [PubMed]
- Cox, A.; Lucas, G.; Marcu, A.; Piano, M.; Grosvenor, W.; Mold, F.; Maguire, R.; Ream, E. Cancer Survivors’ Experience With Telehealth: A Systematic Review and Thematic Synthesis. J. Med. Internet Res. 2017, 19, e11. [Google Scholar] [CrossRef] [PubMed]
- Bekelis, K.; Calnan, D.; Simmons, N.; MacKenzie, T.A.; Kakoulides, G. Effect of an Immersive Preoperative Virtual Reality Experience on Patient Reported Outcomes: A Randomized Controlled Trial. Ann. Surg. 2017, 265, 1068–1073. [Google Scholar] [CrossRef]
- Orlosky, J.; Itoh, Y.; Ranchet, M.; Kiyokawa, K.; Morgan, J.; Devos, H. Emulation of Physician Tasks in Eye-Tracked Virtual Reality for Remote Diagnosis of Neurodegenerative Disease. IEEE Trans. Vis. Comput. Graph. 2017, 23, 1302–1311. [Google Scholar] [CrossRef] [PubMed]
- Pulijala, Y.; Ma, M.; Pears, M.; Peebles, D.; Ayoub, A. Effectiveness of Immersive Virtual Reality in Surgical Training-A Randomized Control Trial. J. Oral Maxillofac. Surg. 2018, 76, 1065–1072. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study | Selection Bias | Design | Confounders | Blinding | Data Collection | Withdrawals and Dropouts | Total |
|---|---|---|---|---|---|---|---|
| Atef 2020 [29] | 1 | 1 | 1 | 2 | 1 | 1 | 1 |
| Chirico 2019 [30] | 1 | 1 | 1 | 2 | 1 | 1 | 1 |
| Feyzioğlu 2020 [31] | 2 | 1 | 1 | 1 | 1 | 1 | 1 |
| House 2016 [32] | 1 | 2 | 3 | 1 | 1 | 2 | 2 |
| McGarvey 2009 [33] | 2 | 2 | 1 | 2 | 1 | 1 | 1 |
| Mohammad 2018 [34] | 2 | 1 | 1 | 2 | 1 | 1 | 1 |
| Piejko 2020 [35] | 2 | 2 | 1 | 2 | 1 | 2 | 1 |
| Schneider 2003 [36] | 3 | 2 | 1 | 2 | 1 | 2 | 2 |
| Schneider 2004 [37] | 3 | 2 | 1 | 2 | 1 | 1 | 2 |
| Schneider 2007 [38] | 3 | 2 | 1 | 2 | 1 | 1 | 2 |
| Schneider 2011 [39] | 2 | 2 | 1 | 2 | 1 | 1 | 1 |
| First Author and Year [No. Ref.] | Number of Participants [N] and Design of Study | Age [Years] | Inclusion Criteria | Exclusion Criteria |
|---|---|---|---|---|
| Atef 2020 [29] | N = 30 (Quasi-randomised study of 2 groups: 15 women had VR-based therapy, and 15 had PNF therapy) | range: 40–65 | BC women with unilateral lymphoedema after mastectomy, min. 6 months after surgery, min. 5% difference in limb volume, not undergoing physiotherapy for at least 3 months. | musculoskeletal, neurological, and visual disorders, uncontrolled cardiovascular or pulmonary diseases that are not controlled, psychiatric illness, bilateral lymphedema, elephantiasis, current metastases, continuing RT and venous thrombosis |
| Chirico 2019 [30] | N = 94 (Non-randomised study: 3 groups: 30 patients were included in the VR IG, 30 patients in MT IG, and 34 patients constituted the CG with standard care) | mean (SD): VR: 55.18 (5.7) MT: 55.7 (5.26) CG: 56.2(6.79) | age 18–70 years, CHT as a treatment for BC (Epirubicin, Cyclophosphamide) | epilepsy, drug and/or alcohol addictions, metastasis, wearing glasses, or having ports |
| Feyzioğlu 2020 [31] | N = 40 (Randomised, clinical study: 2 groups: 20 patients were included in the Kinect-based rehabilitation group (KBRG), and 20 in the standardised physical therapy group (SPTG); | mean (SD): KBRG: 50.84 (8.53) SPTG: 51.00 (7.06) | women aged 30–60 years, in the second week after surgery with axillary dissection, without vision, hearing, and speech impairment | previous BC surgery, cancer focus, reduced range of motion of upper limb before surgery, pace-maker, infection, open wounds, or wound drains; and mental disorders or cooperation issues |
| House 2016 [32] | N = 6 (Pilot and single-arm study) | range: 22–78 mean (SD): 57.8 (20.4) | age ≥ 22, regular intake of painkillers, mild to moderate depression, upper limb impairments | immobilised upper limb, visual or hearing impairments, severe cognitive problems, violent behaviour, metastases to the upper limb bones |
| McGarvey 2009 [33] | N = 45 (Simple size, evaluation study: patients were assigned to the HAAIR–IG or a control group (SCG)). | mean (SD): IG: 51.72 (10.55) SCG: 50.85 (10.31) | women with BC or other cancers treated with CHT that has been associated with alopecia | age < 17 or >75, severe physical or mental disability, previous episode related to cancer and alopecia |
| Bani Mohammad 2018 [34] | N = 80 (Randomised, controlled trial: 40 in IG and 40 in CG) | range: 30–70 | women aged 18–70 years with BC, current history of chronic pain treated with morphine or other painkillers, writing and reading, no epilepsy and brain metastases, no motion sickness, no significant cognitive, visual, and hearing impairment. | - |
| Piejko 2020 [35] | N = 46 (Pilot, clinical, non-controlled study) | range: 36–63 mean (SD): 51.67(6.62) | women age > 18, after mastectomy for BC (grade I-III clinical advancement) and adjuvant treatment, completed RT and CHT a min. of 8 wks. before the start of the study, consent to participate in the study. | Barthel scale < 65 points, lymphoedema, body imbalance due to other diseases, inability to cooperate |
| Schneider 2003 [36] | N = 16 (IG and CG—crossover design. Participants received the VR treatment during either their 1st CHT treatment (group A) or their 2nd CHT treatment (group B). During the alternate CHT treatment (CG) subjects received standard care. | range: 50–77 | age ≥ 50, BC, no history of other cancer, at least two matched cycles of IV CHT, reading and writing in English, no metastasis and primary brain disease, without a history of seizures, no history of motion sickness, Mini-Mental ≥ 24 | - |
| Schneider 2004 [37] | N = 20 (Crossover design. Participants received the VR treatment during either their 1st CHT treatment (group A) or their 2nd CHT treatment (group B). During the alternate CHT treatment (CG) subjects received standard care) | range: 27–55 | women age 18–55 with BC, no history of other cancer, require at least two matched cycles of IV CHT, reading and writing in English, no metastasis and primary brain disease, without a history of seizures, no history of motion sickness. | - |
| Schneider 2007 [38] | N = 105 (Crossover design. Participants received the VR treatment during either their 1st CHT treatment (group A) or their 2nd CHT treatment (group B). During the alternate CHT treatment (CG) subjects received standard care) | range: 32–78 | breast, lung, or colon cancer; no previous history of cancer, age ≥ 18, requires at least two matched cycles of IV CHT, reading and writing in English, no metastasis and primary brain disease, without a history of seizures, no history of motion sickness, consent to participate in the study | - |
| Schneider 2011 [39] | N = 137 (Crossover design; requiring two matched IV CHT treatments. Participants were randomly assigned to receive VR distraction intervention during the 1st or 2nd treatment and standard care with no distraction during the alternate treatment) | range: 27–78 | breast, lung, or colon cancer; no previous history of cancer, age ≥ 18, requires at least two matched cycles of IV CHT, reading and writing in English, consent to participate in the study | metastasis and primary brain disease, history of motion sickness or seizures |
| First Author and Year [No. Ref.] | Aim of the Study | Type of Intervention Using VR | Duration of Therapy | Tested Variables | Result |
|---|---|---|---|---|---|
| Atef 2020 [29] | Establishing and comparing PNF and VR therapy in the treatment of lymphoedema after mastectomy | non-immersive VR Nintendo Wii® video game (exercises such as boxing, tennis, triceps extension) | 2 sessions per wk. of 30 min, for 4 wks. | -Lymphedema: circumferential method: The excess arm volume (EAV) = VL − VH, where VL refers to the lymphoedematous limb’s volume, and VH refers to the healthy extremity’s volume. -Function: QuickDASH-9 scale | -In the VR group was a greater improvement in lymphedema and upper limb function than in the PNF group. -No statistically significant differences were found between EAVs and QuickDASH-9 scores between these groups. The results before and after therapy with the use of VR improved EAVs (p = 0.001) and QuickDASH-9 scores (p = 0.001) |
| Chirico 2019 [30] | Effectiveness and comparison of the effects of therapy with the use of VR and MT in alleviating the psychological stress associated with CHT in BC patients | Immersive and interactive VR. The VR equipment: head-mounted glasses (Vuzix Wrap 1200 VR) with a head motion tracking system. Relaxing images virtual surroundings created on the Second Life® platform (Linden Lab), e.g., being on an island, walking through a forest, observing animals, climbing a mountain, and swimming in the sea. | 20 min. during CHT treatment lasted 45–90 min. | -Anxiety levels: State Anxiety Inventory (SAI) for adults -Mood states: short version of Profile of Mood States (SV-POMS) -Cybersickness symptoms: The Virtual Reality Symptom Questionnaire (VRSQ) | VR therapy turned out to be more effective than MT. The anxiety decreased significantly in the CG group and was statistically insignificant in IG. Cybersickness symptoms occurred at a frequency of less than 20% (except for difficulty concentrating). |
| Feyzioğlu 2020 [31] | Evaluation of the impact of VR therapy with the use of Kinect equipment on the functions of the upper limb in women after BC surgery. | Kinect Sports I (boxing, darts, bowling,), Kinect Sports I (beach volleyball, table tennis), and Fruit Ninja. | 35 min for one session during 6 wks. | -Pain intensity: VAS -Shoulder range of motion was measured in degrees using a digital goniometer -Arm strength was measured during maximal voluntary isometric muscle contraction with the J Tech Commender Muscle Tester handheld dynamometer -Handgrip strength was measured with the Saehan hydraulic hand dynamometer -The disability of the arm, shoulder, and hand (DASH) questionnaire was used to assess upper extremity functionality -Fear of movement as assessed with the Tampa Kinesiophobia Scale (TKS) | Kinect therapy was more effective in improving the assessed parameters than standard therapy (apart from the DASH results and the strength of the handgrip strength) |
| House 2016 [32] | BrightArm Duo therapy assessment in the context of coping with postoperative pain and disability after surgery treatment in BC patients with depression | The BrightArm Duo Rehabilitation System consisted of a low-friction robotic rehabilitation table, computerised forearm supports, a display, a laptop computer for the therapist station, a remote clinical server, and rehabilitation games. Nine games for manual motor training, cognitive and emotive training. | 2 sessions (session lasted 20–50 min) per wk. for 8 wks | -Therapy session data consisted of supported arm reach baseline on the BrightArm Duo table (as measured by overhead digital cameras), power grasp strength baseline (as measured by a forearm support grasp sensor), HR and BP, number of active movements, and grasp repetitions for each arm during a session collected during play. -Pain: Numerical Rating Scale -The subjects rated their experience on a custom subjective questionnaire. The 10 questions were rated using a 5-point Likert scale; -Upper extremity function: the Fulg–Meyer Assessment, Upper Extremity Section, the Chedokee Arm and Hand Activity Inventory-9 (CAHAI-9) for bimanual tasks, and the Jebsen Hand Function Test (JHFT)24 for hand function. -Arm and hand range of motion: mechanical goniometers -Shoulder strength: wrist weights, -Grasp strength: a Jamar mechanical dynamometer and a pinch meter. -Independence in ADL involving the upper extremity: the upper extremity functional index 20 (UEFI-20). -Neuropsychological evaluations: the Beck Depression Inventory, Second Edition (BDI-II), the Neuropsychological Assessment Battery (NAB) Attention Module (orientation, digit span, and dots) and Executive Functioning Module (generation subtest), the Hopkins Verbal Learning Test, Revised (HVLT-R), the Brief Visuospatial Memory Test, Revised (BVMT-R), and the Trail Making Test (TMT) A and B. | There was a decrease in pain and severity of depression (p = 0.1; p = 0.04), an increase in 17 out of 18 motor indices, an improvement in 13 out of 15 indices of strength and function. |
| McGarvey 2009 [33] | using a computer-imaging program called help with adjustment to alopecia by image recovery (HAAIR) to provide educational support and reduce stress in women with post-chemotherapy hair loss | HAAIR system allows you to see yourself in VR with a bald head and of her head wearing a variety of different wigs and hairstyles | one session (60-90 min) | -Qualitative data were obtained verbally by open-ended questions asked during or following use of HAAIR (e.g., ‘Did you enjoy using the system?’, ‘Are you glad that you were able to try the system?’) -The quantitative measures: A Demographic Characteristics Questionnaire, The Brief Symptom Inventory (BSI-18), The Importance of Hair Questionnaire (IHQ), The Brief Cope, was used to assess the manner in which patients coped with having cancer. | Hair loss distress decreased in both the CG and IG groups at time after hair loss than at baseline with 3 months follow-up distress scores increasing in the SCG and decreasing in the IG. Those with avoidance coping reported more distress. |
| Mohammad 2018 [34] | Assessment of the effectiveness of immersive VR distraction technology in reducing pain and anxiety among female BC patients. | -Immersive VR -The IG chose from two scenarios on a CD-ROM, which included deep-sea diving ‘Ocean Rift,’ or sitting on the beach with the ‘Happy Place’ track. Then, the patients wore a head-mounted display with headphones. The VR exposure session was ended at the peak time of painkiller efficacy. | once | -Pain intensity: VAS -Anxiety: The State Anxiety Inventory (SAI) | -One session of the immersive VR plus morphine made a significant reduction in pain and anxiety self-reported scores, compared with morphine alone, in BC patients. -The independent-sample t-test showed a significant difference post intervention between the two groups’ pain scores. -The paired t-test showed a significant difference in the means of pain scores at the pre-and post-test in IG and the CG. -Regarding the anxiety testing, the independent sample t-test showed a significant difference post intervention between the two groups. The IG mean was lower than in the CG (p < 0.001). |
| Piejko 2020 [35] | Impact of medical resort treatment extended with modern feedback exercises using VR to improve postural control in BC survivors. | -Individual exercises were conducted using feedback based on VR and were aimed at improving motor coordination and body balance. Exercises on Alfa and Gamma stabilometric platforms and exercises of motor coordination of lower limbs with elastic resistance were used using the Telko device. Rehab software enabling feedback based on VR and collecting data on the type of tasks ordered to patients and the accuracy of their performance by patients. | 3 weeks (6 d/wk, for 45 min./d) | -Static postural control was assessed in a Romberg test -Dynamic postural control was evaluated in the dynamic test, during which the patient’s task was to move the centre of gravity of the body in different directions in a targeted and controlled manner in accordance with the task displayed on the monitor screen. | -In the assessment of dynamic postural control, the length of the centre of foot pressure (COP) movement path before the treatment and after treatment was statistically significant (p = 0.0083) shortened. In the assessment of static postural control, no statistically significant differences were found between the length of the COP pathway before treatment compared to the condition before treatment (p > 0.05). |
| Schneider 2003 [36] | Answer the questions: -Is VR an effective distraction intervention for reducing CHT-related symptom distress levels in older women with BC? -Does VR have a lasting effect? | -The individual wears an 8-oz head-mounted device, which projects an image with the corresponding sounds. The sense of touch is involved through the use of a computer mouse that allows for the manipulation of the image. Participants chose from three CD-ROM-based scenarios; (Oceans Below®, A World of Art®, or Titanic: Adventure Out of Time®). | once during IV CHT | -Fatigue measures: Revised Piper Fatigue Scale (PFS) -Transitory anxiety states in adults: State-Anxiety Inventory for Adults (SAI) -Indicator of symptoms experienced by cancer patients Symptom Distress Scale (SDS) | Analysis using paired t-tests demonstrated a significant decrease in the SAI (p = 0.10) scores following CHT treatments when participants used VR. -No significant changes were found in SDS or PFS values. There was a consistent trend toward improved symptoms on all measures 48 h following completion of CHT. Evaluation of the intervention indicated that women t experienced no cybersickness, and 100% would use VR again. |
| Schneider 2004 [37] | To explore the use of VR as a distraction intervention to relieve symptom distress in women receiving CHT for BC. | For this study, a commercially available headset (Sony PC Glasstron PLM-S700) was used. Subjects chose from three scenarios on CD-ROM. Each scenario lasts several hours, and choices included deep-sea diving, walking through an art museum, or solving a mystery. | once during IV CHT | -Concerns of patients receiving CHT treatments: The Symptom Distress Scale (SDS) -Anxiety and fatigue: The State-Trait Anxiety Inventory (SAI) for Adults and Revised Piper Fatigue Scale (PFS) -Evaluation of VR intervention-open-ended questionnaire that was used to elicit subjects’ opinions about the intervention | Significant decreases in symptom distress and fatigue occurred immediately following CHT treatments when women used the VR intervention. |
| Schneider 2007 [38] | To explore VR as a distraction intervention to relieve symptom distress in adults receiving CHT for breast, colon, and lung cancer. | A commercially available headset (i-Glasses® SVGA Head-Mounted Display, i-O Display Systems, Menlo Park, CA) was used. Participants chose from 4 possible CD-ROM–based VR scenarios: deep-sea diving (Oceans Below®, CounterTop Software, Renton, WA), walking through an art museum (A World of Art®, CounterTop Software), exploring ancient worlds (Timelapse®, Hammerhead Entertainment, Encinitas, CA), and solving a mystery (Titanic: Adventure Out of Time®, Hammerhead Entertainment). | once during IV CHT | -Validation of the distracting qualities of the intervention: Presence Questionnaire (PQ) and the Evaluation of Virtual Reality Intervention -Symptom distress: Adapted Symptom Distress Scale-2 (ASDS-2), State Anxiety Inventory for Adults (SAI), Revised Piper Fatigue Scale (PFS) | Individuals who received the VR during their first CHT had significantly less anxiety, compared with the control condition during the second CHT treatment. |
| Schneider 2011 [39] | Explore the influence of age, gender, state anxiety, fatigue, and diagnosis on time perception in cancer patients receiving IV CHT with a VR intervention within the cognitive model of time perception and predict the effects of these variables on the difference between the actual time elapsed while patients received CHT while immersed in a VR environment and their retrospective estimates of elapsed time. | The VR intervention delivered using commercially available HMDs, it was provided during the entire period of IV infusion, including delivery of pre-medications, antiemetics, and CHT agents. The researcher installed the HMD on the participant’s head as IV infusion started and removed the HMD as soon as the infusion process was completed. Patients selected an initial VR scenario from a menu of multiple options and were free to switch scenarios at any point during the treatment period. | once during IV CHT | -Anxiety: State-Trait Anxiety Inventory for Adults (STAI) -Fatigue: Revised Piper Fatigue Scale (PFS) -Actual time elapsed during CHT | In a forward regression model, three predictors (diagnosis, gender, and anxiety) explained a significant portion of the variability for altered time perception (p = 0.0008). Diagnosis was the strongest predictor; individuals with breast and colon cancer perceived time passed more quickly. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zasadzka, E.; Pieczyńska, A.; Trzmiel, T.; Hojan, K. Virtual Reality as a Promising Tool Supporting Oncological Treatment in Breast Cancer. Int. J. Environ. Res. Public Health 2021, 18, 8768. https://doi.org/10.3390/ijerph18168768
Zasadzka E, Pieczyńska A, Trzmiel T, Hojan K. Virtual Reality as a Promising Tool Supporting Oncological Treatment in Breast Cancer. International Journal of Environmental Research and Public Health. 2021; 18(16):8768. https://doi.org/10.3390/ijerph18168768
Chicago/Turabian StyleZasadzka, Ewa, Anna Pieczyńska, Tomasz Trzmiel, and Katarzyna Hojan. 2021. "Virtual Reality as a Promising Tool Supporting Oncological Treatment in Breast Cancer" International Journal of Environmental Research and Public Health 18, no. 16: 8768. https://doi.org/10.3390/ijerph18168768
APA StyleZasadzka, E., Pieczyńska, A., Trzmiel, T., & Hojan, K. (2021). Virtual Reality as a Promising Tool Supporting Oncological Treatment in Breast Cancer. International Journal of Environmental Research and Public Health, 18(16), 8768. https://doi.org/10.3390/ijerph18168768