
Fever after Vaccination against SARS-CoV-2 with mRNA-Based Vaccine Associated with Higher Antibody Levels during 6 Months Follow-Up

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Adverse Reaction Assessment
2.3. Measurement of Antibody Titers
2.4. Ethics Statement
2.5. Statistical Analysis
3. Results
3.1. Study Participants
3.2. Adverse Reactions
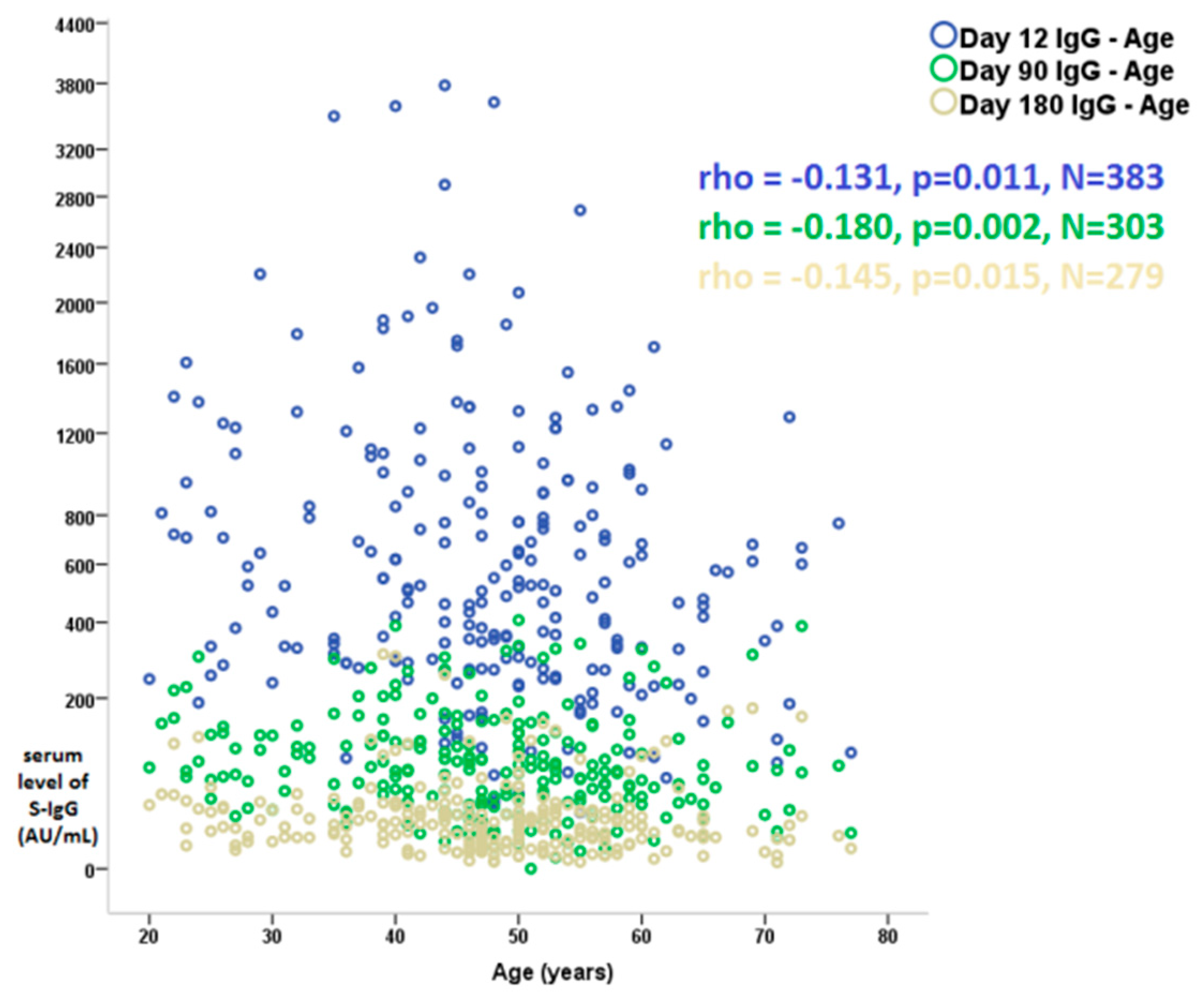
3.3. Relationship between Antibody Levels, Demographics, and Clinical Variables
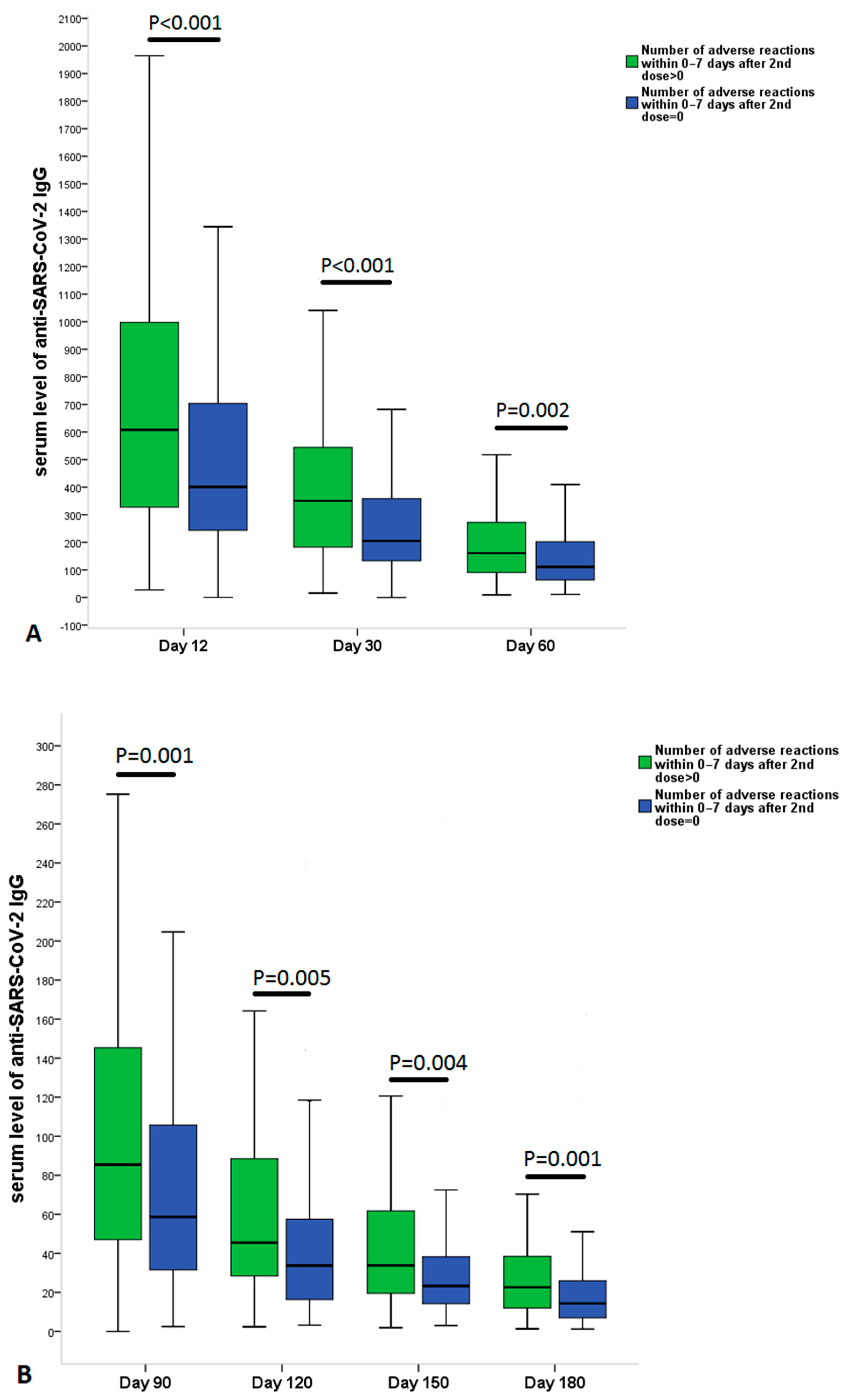
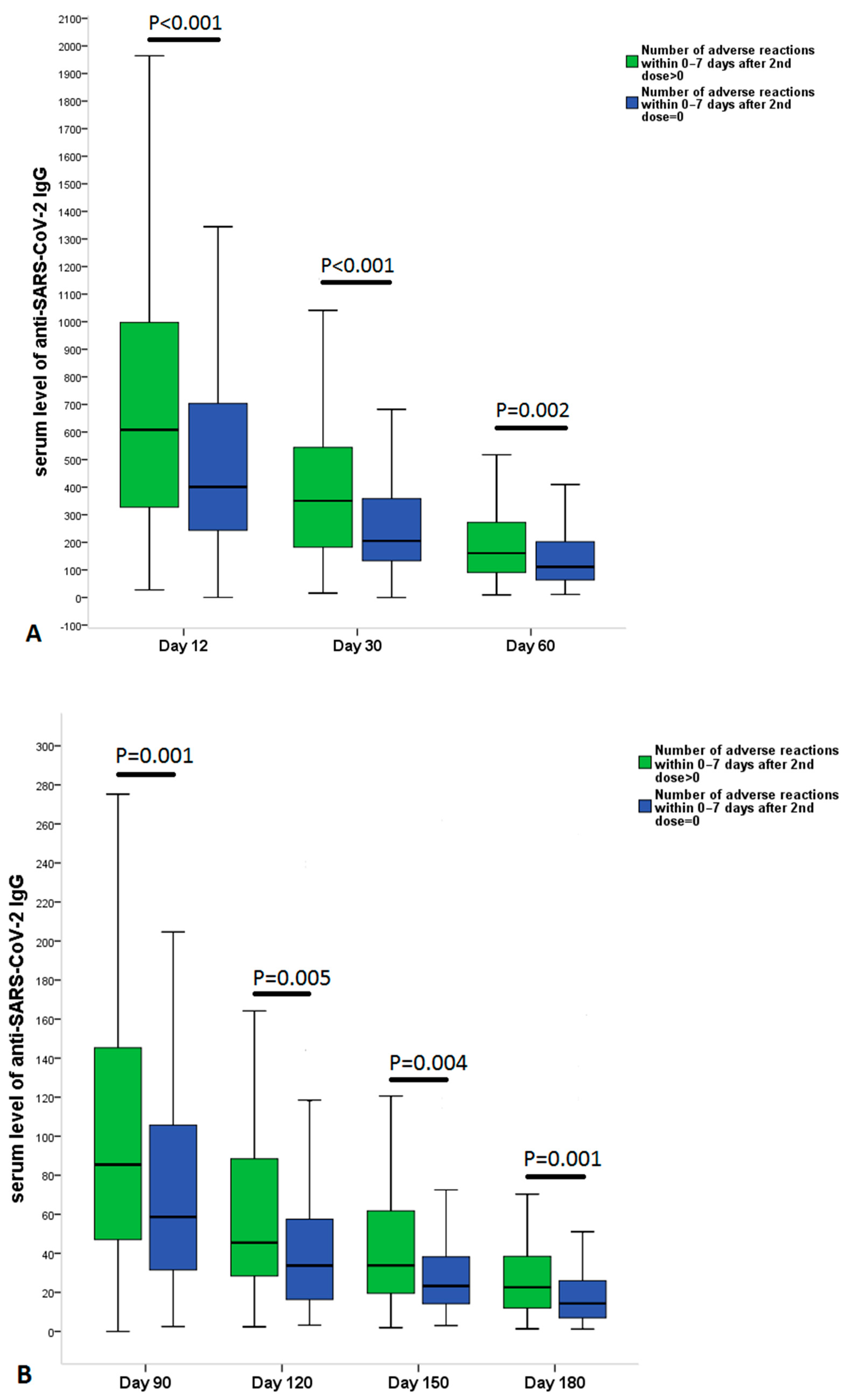
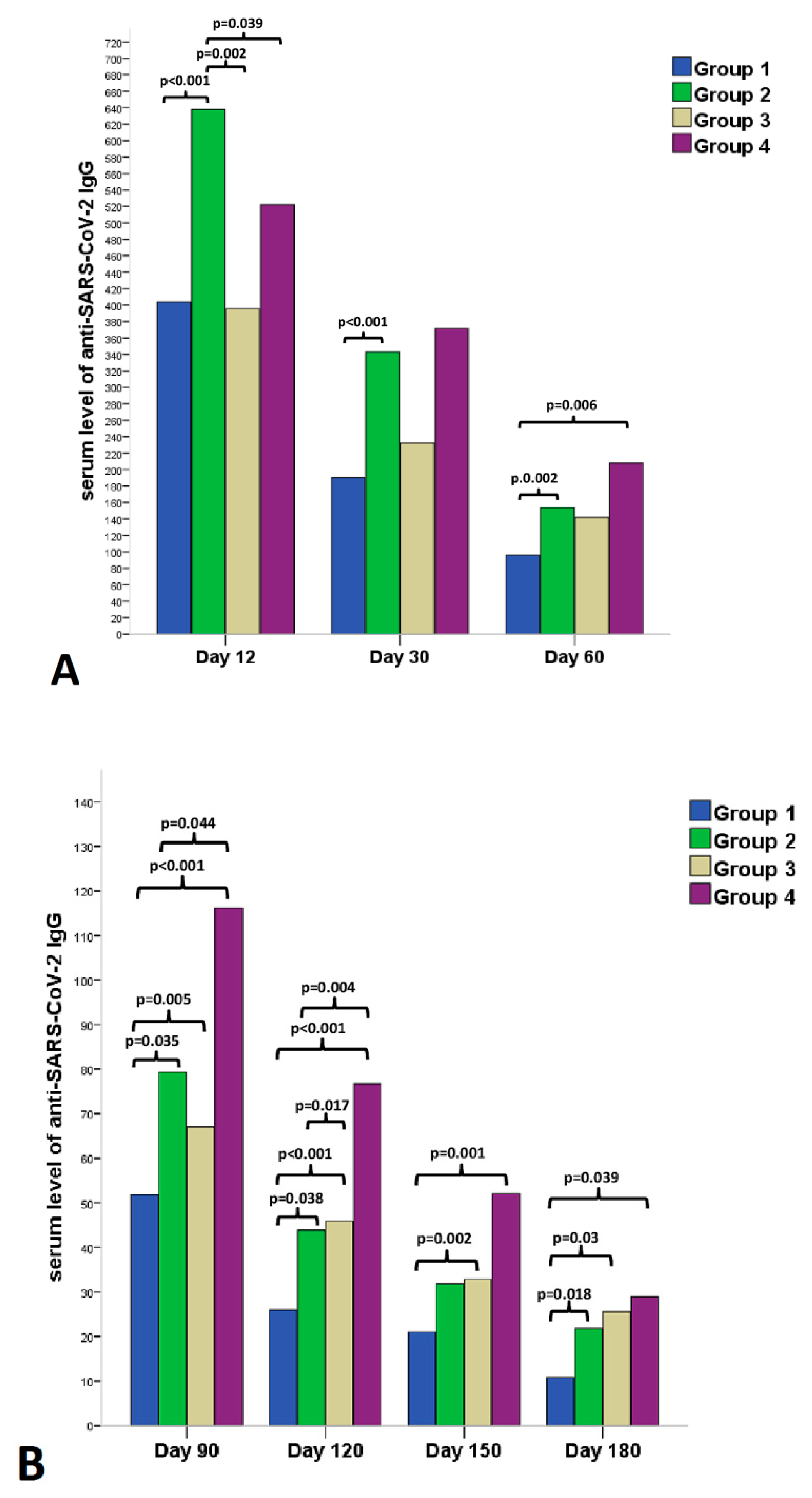
3.4. Relationship between Antibody Levels and Adverse Reactions

| Day 12 | Day 30 | Day 60 | Day 90 | Day 120 | Day 150 | Day 180 | |
| Group 1 | 167 | 129 | 136 | 129 | 108 | 90 | 110 |
| Group 2 | 131 | 119 | 115 | 115 | 109 | 84 | 107 |
| Group 3 | 47 | 42 | 36 | 47 | 26 | 21 | 27 |
| Group 4 | 38 | 33 | 33 | 28 | 24 | 24 | 25 |
| Data are presented as medians and IQR. | |||||||
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 29 January 2022).
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Yoda, T.; Katsuyama, H. Willingness to Receive COVID-19 Vaccination in Japan. Vaccines 2021, 9, 48. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://ourworldindata.org/COVID-vaccinations (accessed on 25 January 2022).
- Coggins, S.A.A.; Laing, E.D.; Olsen, C.H.; Goguet, E.; Moser, M.; Jackson-Thompson, B.M.; Samuels, E.C.; Pollett, S.D.; Tribble, D.R.; Davies, J.; et al. Adverse Effects and Antibody Titers in Response to the BNT162b2 MRNA COVID-19 Vaccine in a Prospective Study of Healthcare Workers. Open Forum. Infect. Dis. 2022, 9, ofab575. [Google Scholar] [CrossRef] [PubMed]
- Uwamino, Y.; Kurafuji, T.; Sato, Y.; Tomita, Y.; Shibata, A.; Tanabe, A.; Yatabe, Y.; Noguchi, M.; Arai, T.; Ohno, A.; et al. Young age, female sex, and presence of systemic adverse reactions are associated with high post-vaccination antibody titer after two doses of BNT162b2 mRNA SARS-CoV-2 vaccination: An observational study of 646 Japanese healthcare workers and university staff. Vaccine 2022, 40, 1019–1025. [Google Scholar] [CrossRef]
- Moderbacher, C.; Ramirez, S.I.; Dan, J.M.; Grifoni, A.; Hastie, K.M.; Weiskopf, D.; Belanger, S.; Abbott, R.K.; Kim, C.; Choi, J.; et al. Antigen-Specific Adaptive Immunity to SARS-CoV-2 in Acute COVID-19 and Associations with Age and Disease Severity. Cell 2020, 183, 996–1012.e19. [Google Scholar] [CrossRef] [PubMed]
- Tarbiah, N.; Todd, I.; Tighe, P.J.; Fairclough, L.C. Cigarette smoking differentially affects immunoglobulin class levels in serum and saliva: An investigation and review. Basic Clin. Pharmacol. Toxicol. 2019, 125, 474–483. [Google Scholar] [CrossRef] [PubMed]
- McMillan, S.A.; Douglas, J.P.; Archbold, G.P.; McCrum, E.E.; Evans, A.E. Effect of low to moderate levels of smoking and alcohol consumption on serum immunoglobulin concentrations. J. Clin. Pathol. 1997, 50, 819–822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiu, F.; Liang, C.L.; Liu, H.; Zeng, Y.Q.; Hou, S.; Huang, S.; Lai, X.; Dai, Z. Impacts of cigarette smoking on immune responsiveness: Up and down or upside down? Oncotarget 2017, 8, 268–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skok, M.V.; Grailhe, R.; Agenes, F.; Changeux, J.P. The role of nicotinic receptors in B-lymphocyte development and activation. Life Sci. 2007, 80, 2334–2336. [Google Scholar] [CrossRef] [PubMed]
- Fischinger, S.; Boudreau, C.M.; Butler, A.L.; Streeck, H.; Alter, G. Sex differences in vaccine-induced humoral immunity. Semin. Immunopathol. 2019, 41, 239–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fathi, A.; Addo, M.M.; Dahlke, C. Sex Differences in Immunity: Implications for the Development of Novel Vaccines against Emerging Pathogens. Front. Immunol. 2021, 11, 601170. [Google Scholar] [CrossRef] [PubMed]
- Naaber, P.; Tserel, L.; Kangro, K.; Sepp, E.; Jürjenson, V.; Adamson, A.; Haljasmägi, L.; Rumm, A.P.; Maruste, R.; Kärner, J.; et al. Dynamics of antibody response to BNT162b2 vaccine after six months: A longitudinal prospective study. Lancet Reg. Health 2021, 10, 100208. [Google Scholar] [CrossRef] [PubMed]
- Hanson, D.F. Fever, temperature, and the immune response. Ann. N. Y. Acad. Sci. 1997, 813, 453–464. [Google Scholar] [CrossRef] [PubMed]
- Evans, S.S.; Repasky, E.A.; Fisher, D.T. Fever and the thermal regulation of immunity: The immune system feels the heat. Nat. Rev. Immunol. 2015, 15, 335–349. [Google Scholar] [CrossRef]
- Müller, L.; Andrée, M.; Moskorz, W.; Drexler, I.; Walotka, L.; Grothmann, R.; Ptok, J.; Hillebrandt, J.; Ritchie, A.; Rabl, D.; et al. Age-dependent Immune Response to the Biontech/Pfizer BNT162b2 Coronavirus Disease 2019 Vaccination. Clin. Infect. Dis. 2021, 73, 2065–2072. [Google Scholar] [CrossRef]
- Andrews, N.J.; Walker, W.T.; Finn, A.; Heath, P.T.; Collinson, A.C.; Pollard, A.J.; Snape, M.D.; Faust, S.N.; Waight, P.A.; Hoschler, K.; et al. Predictors of immune response and reactogenicity to AS03B-adjuvanted split virion and non-adjuvanted whole virion H1N1 (2009) pandemic influenza vaccines. Vaccine 2011, 29, 7913–7919. [Google Scholar] [CrossRef]
- Held, J.; Esse, J.; Tascilar, K.; Steininger, P.; Schober, K.; Irrgang, P.; Alsalameh, R.; Tenbusch, M.; Seggewies, C.; Bogdan, C. Reactogenicity Correlates Only Weakly with Humoral Immunogenicity after COVID-19 Vaccination with BNT162b2 mRNA (Comirnaty®). Vaccines 2021, 9, 1063. [Google Scholar] [CrossRef] [PubMed]
- Hwang, Y.H.; Song, K.H.; Choi, Y.; Go, S.; Choi, S.J.; Jung, J.; Kang, C.K.; Choe, P.G.; Kim, N.J.; Park, W.B.; et al. Can reactogenicity predict immunogenicity after COVID-19 vaccination? Korean J. Intern. Med. 2021, 36, 1486–1491. [Google Scholar] [CrossRef]
- Otani, J.; Ohta, R.; Sano, C. Association between Immunoglobulin G Levels and Adverse Effects Following Vaccination with the BNT162b2 Vaccine among Japanese Healthcare Workers. Vaccines 2021, 9, 1149. [Google Scholar] [CrossRef]
- Prymula, R.; Siegrist, C.A.; Chlibek, R.; Zemlickova, H.; Vackova, M.; Smetana, J.; Lommel, P.; Kaliskova, E.; Borys, D.; Schuerman, L. Effect of prophylactic paracetamol administration at time of vaccination on febrile reactions and antibody responses in children: Two open-label, randomised controlled trials. Lancet 2009, 374, 1339–1350. [Google Scholar] [CrossRef]
- Bancos, S.; Bernard, M.P.; Topham, D.J.; Phipps, R.P. Ibuprofen and other widely used non-steroidal anti-inflammatory drugs inhibit antibody production in human cells. Cell Immunol. 2009, 258, 18–28. [Google Scholar] [CrossRef] [Green Version]
- Paccani, S.R.; Boncristiano, M.; Ulivieri, C.; D’Elios, M.M.; Del Prete, G.; Baldari, C.T. Nonsteroidal anti-inflammatory drugs suppress T-cell activation by inhibiting p38 MAPK induction. J. Biol. Chem. 2002, 277, 1509–1513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryan, E.P.; Pollock, S.J.; Murant, T.I.; Bernstein, S.H.; Felgar, R.E.; Phipps, R.P. Activated human B lymphocytes express cyclooxygenase-2 and cyclooxygenase inhibitors attenuate antibody production. J. Immunol. 2005, 174, 2619–2626. [Google Scholar] [CrossRef] [Green Version]
- Saleh, E.; Moody, M.A.; Walter, E.B. Effect of antipyretic analgesics on immune responses to vaccination. Hum. Vaccines Immunother. 2016, 12, 2391–2402. [Google Scholar] [CrossRef] [Green Version]
- Morales-Núñez, J.J.; Muñoz-Valle, J.F.; Meza-López, C.; Wang, L.F.; Machado Sulbarán, A.C.; Torres-Hernández, P.C.; Bedolla-Barajas, M.; De la O-Gómez, B.; Balcázar-Félix, P.; Hernández-Bello, J. Neutralizing Antibodies Titers and Side Effects in Response to BNT162b2 Vaccine in Healthcare Workers with and without Prior SARS-CoV-2 Infection. Vaccines 2021, 9, 742. [Google Scholar] [CrossRef] [PubMed]
- Ali, H.; Alahmad, B.; Al-Shammari, A.A.; Alterki, A.; Hammad, M.; Cherian, P.; Alkhairi, I.; Sindhu, S.; Thanaraj, T.A.; Mohammad, A.; et al. Previous COVID-19 Infection and Antibody Levels after Vaccination. Front. Public Health 2020, 9, 778243. [Google Scholar] [CrossRef]
- Ebinger, J.E.; Fert-Bober, J.; Printsev, I.; Wu, M.; Sun, N.; Prostko, J.C.; Frias, E.C.; Stewart, J.L.; Van Eyk, J.E.; Braun, J.G.; et al. Antibody responses to the BNT162b2 mRNA vaccine in individuals previously infected with SARS-CoV-2. Nat. Med. 2021, 27, 981–984. [Google Scholar] [CrossRef]
- Xiao, K.; Yang, H.; Liu, B.; Pang, X.; Du, J.; Liu, M.; Liu, Y.; Jing, X.; Chen, J.; Deng, S.; et al. Antibodies Can Last for More Than 1 Year After SARS-CoV-2 Infection: A Follow-Up Study From Survivors of COVID-19. Front. Med. 2021, 8, 684864. [Google Scholar] [CrossRef] [PubMed]
- Haas, J.W.; Bender, F.L.; Ballou, S.; Kelley, J.M.; Wilhelm, M.; Miller, F.G.; Rief, W.; Kaptchuk, T.J. Frequency of Adverse Events in the Placebo Arms of COVID-19 Vaccine Trials: A Systematic Review and Meta-analysis. JAMA 2022, 5, e2143955. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Total Population (N = 383) | Asymptomatic Group (N = 214) | Symptomatic Group (N = 169) | p-Value | |
|---|---|---|---|---|
| Age, (mean ± SD) | 46.5 ± 12 | 47.6 ± 12 | 45.3 ± 12 | NS |
| Female, (N, %) | 303 (76.7) | 159 (74.3) | 139 (82.2) | NS |
| BMI, (mean ± SD) | 27.6 ± 6 | 28.1 ± 7 | 26.9 ± 5 | NS |
| Smoking, (N, %) | 123 (34.7) | 73 (37.2) | 50 (31.8) | NS |
| Flu vaccination, (N, %) | 67 (17.6) | 37 (17.5) | 30 (17.9) | NS |
| Hypertension, (N, %) | 95 (26) | 55 (28.2) | 40 (23.7) | NS |
| Diabetes, (N, %) | 22 (6) | 14 (7.2) | 8 (4.7) | NS |
| Hypothyreosis, (N, %) | 25 (6.9) | 15 (7.7) | 10 (5.9) | NS |
| Autoimmune disease, (N, %) | 20 (5.5) | 10 (5.2) | 10 (5.9) | NS |
| Allergy, (N, %) | 96 (26.2) | 36 (18.3) | 60 (35.5) | <0.001 |
| ACE inhibitors, (N, %) | 63 (17.4) | 34 (17.6) | 29 (17.2) | NS |
| Beta blockers, (N, %) | 60 (16.5) | 30 (15.5) | 30 (17.8) | NS |
| Calcium channel blocker, (N, %) | 25 (6.9) | 9 (4.7) | 16 (9.5) | NS |
| Prior COVID-19 infection, (N, %) | 85 (23.2) | 47 (24) | 38 (22.5) | NS |
| Variable | B | Odds Ratio | 95% C.I. | p-Value | |
|---|---|---|---|---|---|
| Day 12, value of S-IgG (AU/mL, median as the cutoff) § | |||||
| Fever, 2nd | −1.264 | 0.283 | 0.107 | 0.747 | 0.011 |
| Day 30, value of S-IgG (AU/mL, median as the cutoff) § | |||||
| Fever, 2nd | −1.349 | 0.260 | 0.091 | 0.741 | 0.012 |
| Day 60, value of S-IgG (AU/mL, median as the cutoff) § | |||||
| Smoking | 0.651 | 1.917 | 1.157 | 3.176 | 0.012 |
| Fever, 2nd | −1.372 | 0.254 | 0.086 | 0.748 | 0.013 |
| Day 90, value of S-IgG (AU/mL, median as the cutoff) § | |||||
| Chills, 1st | −1.672 | 0.188 | 0.038 | 0.937 | 0.041 |
| Fever, 2nd | −2.482 | 0.084 | 0.018 | 0.389 | 0.002 |
| Day 120, value of S-IgG (AU/mL, median as the cutoff) § | |||||
| Age | −0.037 | 0.964 | 0.941 | 0.988 | 0.003 |
| Smoking | 0.780 | 2.181 | 1.227 | 3.878 | 0.008 |
| Prior COVID+ | −1.159 | 0.314 | 0.150 | 0.659 | 0.002 |
| Fever, 2nd | −2.518 | 0.081 | 0.017 | 0.382 | 0.002 |
| Day 150, value of S-IgG (AU/mL, median as the cutoff) § | |||||
| Prior COVID+ | −0.781 | 0.458 | 0.216 | 0.972 | 0.042 |
| Fever, 2nd | −2.414 | 0.089 | 0.019 | 0.413 | 0.002 |
| Day 180, value of S-IgG (AU/mL, median as the cutoff) § | |||||
| Smoking | 0.651 | 1.918 | 1.100 | 3.345 | 0.022 |
| Fever, 2nd | −1.632 | 0.196 | 0.062 | 0.612 | 0.005 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kanizsai, A.; Molnar, T.; Varnai, R.; Zavori, L.; Tőkés-Füzesi, M.; Szalai, Z.; Berecz, J.; Csecsei, P. Fever after Vaccination against SARS-CoV-2 with mRNA-Based Vaccine Associated with Higher Antibody Levels during 6 Months Follow-Up. Vaccines 2022, 10, 447. https://doi.org/10.3390/vaccines10030447
Kanizsai A, Molnar T, Varnai R, Zavori L, Tőkés-Füzesi M, Szalai Z, Berecz J, Csecsei P. Fever after Vaccination against SARS-CoV-2 with mRNA-Based Vaccine Associated with Higher Antibody Levels during 6 Months Follow-Up. Vaccines. 2022; 10(3):447. https://doi.org/10.3390/vaccines10030447
Chicago/Turabian StyleKanizsai, Andrea, Tihamer Molnar, Reka Varnai, Laszlo Zavori, Margit Tőkés-Füzesi, Zoltan Szalai, Janos Berecz, and Peter Csecsei. 2022. "Fever after Vaccination against SARS-CoV-2 with mRNA-Based Vaccine Associated with Higher Antibody Levels during 6 Months Follow-Up" Vaccines 10, no. 3: 447. https://doi.org/10.3390/vaccines10030447
APA StyleKanizsai, A., Molnar, T., Varnai, R., Zavori, L., Tőkés-Füzesi, M., Szalai, Z., Berecz, J., & Csecsei, P. (2022). Fever after Vaccination against SARS-CoV-2 with mRNA-Based Vaccine Associated with Higher Antibody Levels during 6 Months Follow-Up. Vaccines, 10(3), 447. https://doi.org/10.3390/vaccines10030447