
Implementation and Cross-Validation of a Pharmacokinetic Model for Precision Dosing of Busulfan in Hematopoietic Stem Cell Transplanted Children

 , , ,
, , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search for Candidate Population PK Models of Busulfan
2.2. Patients’ Data
2.3. Goodness of Fit of Selected Models
2.4. Model Implementation in Tucuxi and Reference Model in BestDose
2.5. Cross-Validation of Busulfan Model in Tucuxi
3. Results
3.1. Literature Search and Analysis
3.2. Goodness of Fit of the Three Candidate Models for the Entire Dataset
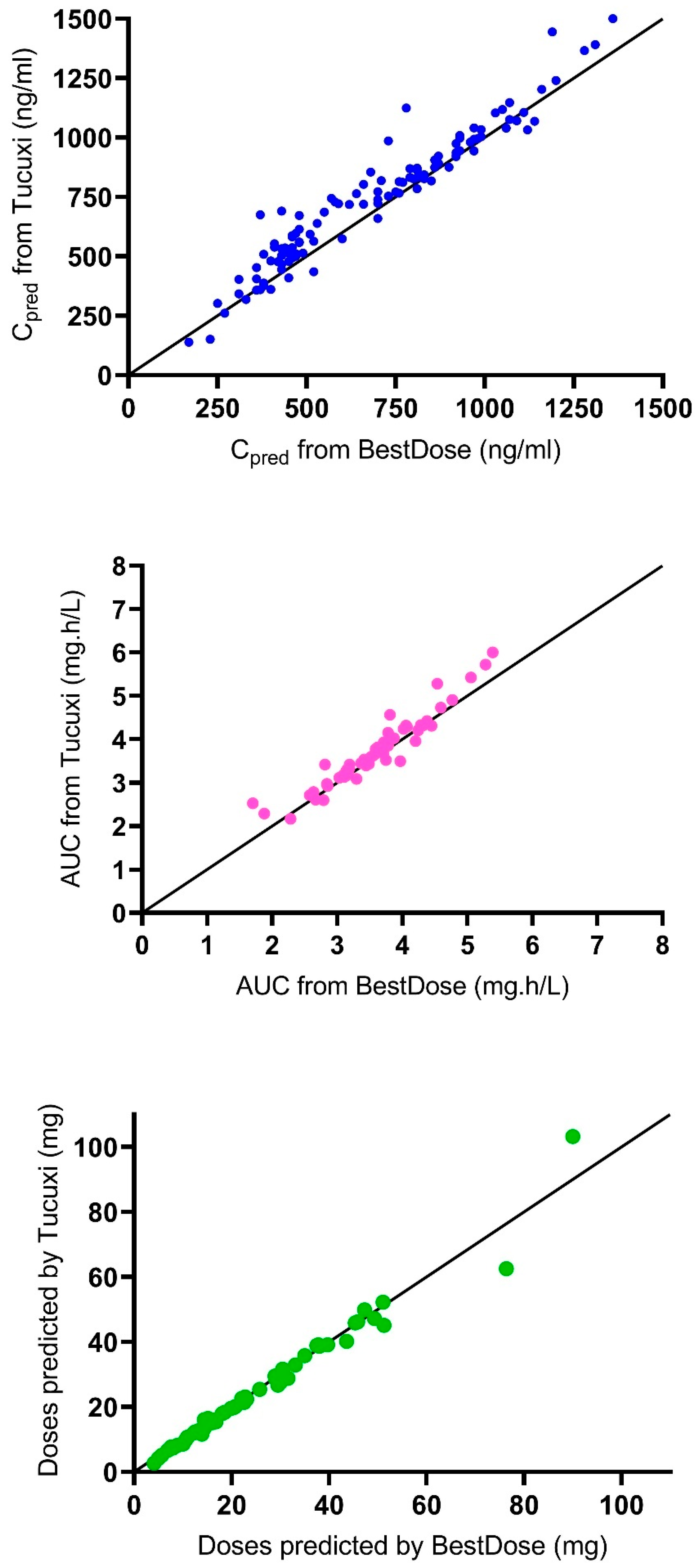
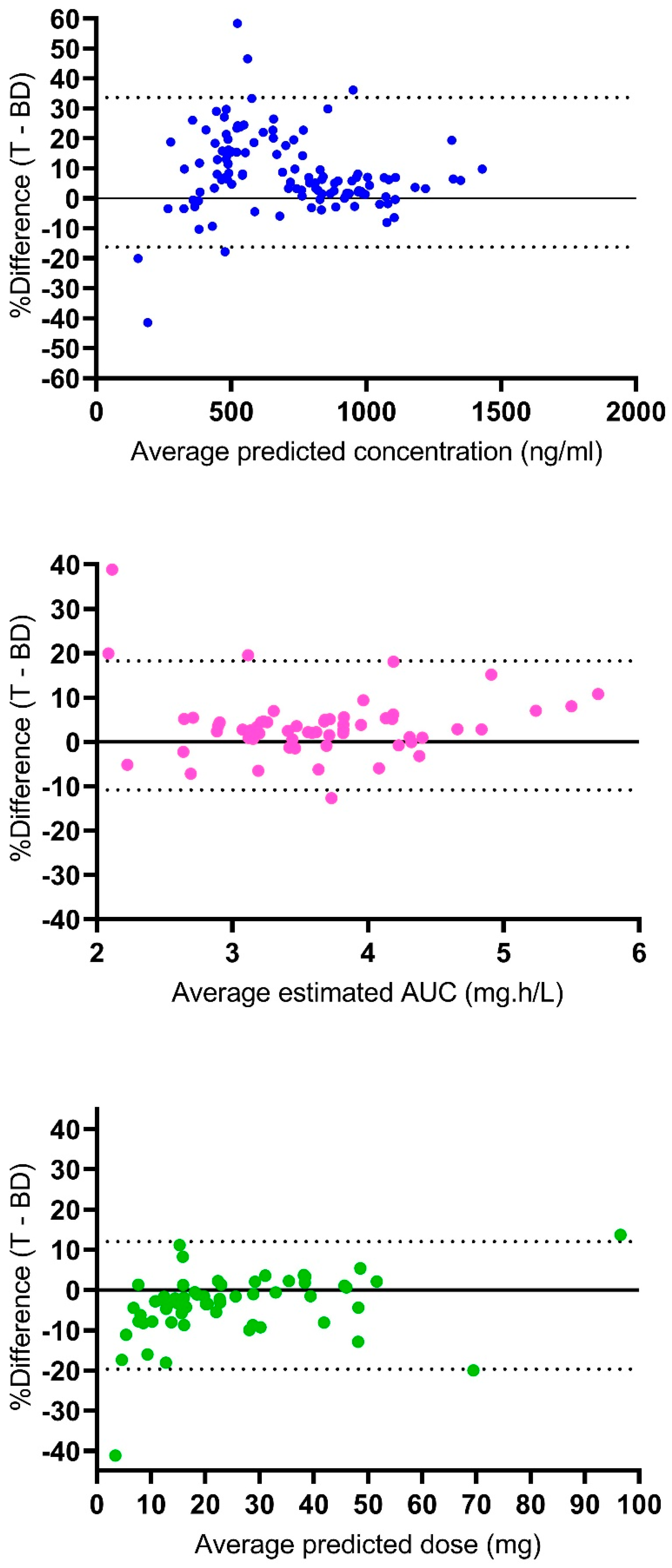
3.3. Comparative Analysis of Tucuxi and BestDose results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hatzimichael, E.; Tuthill, M. Hematopoietic stem cell transplantation. Stem Cells Cloning 2010, 3, 105–117. [Google Scholar] [CrossRef] [PubMed]
- Cremers, S.; Schoemaker, R.; Bredius, R.; Hartigh, J.D.; Ball, L.; Twiss, I.; Vermeij, P.; Vossen, J. Pharmacokinetics of intravenous busulfan in children prior to stem cell transplantation. Br. J. Clin. Pharmacol. 2002, 53, 386–389. [Google Scholar] [CrossRef] [PubMed]
- Lawson, R.; Staatz, C.E.; Fraser, C.J.; Hennig, S. Review of the Pharmacokinetics and Pharmacodynamics of Intravenous Busulfan in Paediatric Patients. Clin. Pharmacokinet. 2021, 60, 17–51. [Google Scholar] [CrossRef] [PubMed]
- Ruutu, T.; van der Werf, S.; van Biezen, A.; Backman, J.T.; Peczynski, C.; Kroger, N.; Mohty, M.; Nagler, A.; Montoto, S.; Langebrake, C.; et al. Use of busulfan in conditioning for allogeneic hematopoietic stem cell transplantation in adults: A survey by the Transplant Complications Working Party of the EBMT. Bone Marrow Transplant. 2019, 54, 2013–2019. [Google Scholar] [CrossRef] [PubMed]
- Bartelink, I.H.; Lalmohamed, A.; van Reij, E.M.; Dvorak, C.C.; Savic, R.M.; Zwaveling, J.; Bredius, R.G.; Egberts, A.C.; Bierings, M.; Kletzel, M.; et al. Association of busulfan exposure with survival and toxicity after haemopoietic cell transplantation in children and young adults: A multicentre, retrospective cohort analysis. Lancet Haematol. 2016, 3, e526–e536. [Google Scholar] [CrossRef]
- Feng, X.; Wu, Y.; Zhang, J.; Li, J.; Zhu, G.; Fan, D.; Yang, C.; Zhao, L. Busulfan systemic exposure and its relationship with efficacy and safety in hematopoietic stem cell transplantation in children: A meta-analysis. BMC Pediatr. 2020, 20, 176. [Google Scholar] [CrossRef]
- Bleyzac, N.; Souillet, G.; Magron, P.; Janoly, A.; Martin, P.; Bertrand, Y.; Galambrun, C.; Dai, Q.; Maire, P.; Jelliffe, R.W.; et al. Improved clinical outcome of paediatric bone marrow recipients using a test dose and Bayesian pharmacokinetic individualization of busulfan dosage regimens. Bone Marrow Transplant. 2001, 28, 743–751. [Google Scholar] [CrossRef]
- Philippe, M.; Goutelle, S.; Guitton, J.; Fonrose, X.; Bergeron, C.; Girard, P.; Bertrand, Y.; Bleyzac, N. Should busulfan therapeutic range be narrowed in pediatrics? Experience from a large cohort of hematopoietic stem cell transplant children. Bone Marrow Transplant. 2016, 51, 72–78. [Google Scholar] [CrossRef]
- Palmer, J.; McCune, J.S.; Perales, M.A.; Marks, D.; Bubalo, J.; Mohty, M.; Wingard, J.R.; Paci, A.; Hassan, M.; Bredeson, C.; et al. Personalizing Busulfan-Based Conditioning: Considerations from the American Society for Blood and Marrow Transplantation Practice Guidelines Committee. Biol. Blood Marrow Transplant. J. Am. Soc. Blood Marrow Transplant. 2016, 22, 1915–1925. [Google Scholar] [CrossRef]
- Neely, M.; Philippe, M.; Rushing, T.; Fu, X.; van Guilder, M.; Bayard, D.; Schumitzky, A.; Bleyzac, N.; Goutelle, S. Accurately Achieving Target Busulfan Exposure in Children and Adolescents With Very Limited Sampling and the BestDose Software. Ther. Drug Monit. 2016, 38, 332–342. [Google Scholar] [CrossRef]
- Jelliffe, R.; Neely, M. Individualized Drug Therapy for Patients. Basic Foundations, Relevant Software and Clinical Applications; Elsevier: Amsterdam, The Netherlands, 2016; p. 434. [Google Scholar]
- Dubovitskaya, A.; Buclin, T.; Schumacher, M.; Aberer, K.; Thoma, Y. TUCUXI: An Intelligent System for Personalized Medicine from Individualization of Treatments to Research Databases and Back. In Proceedings of the 8th ACM International Conference on Bioinformatics, Computational Biology and Health Informatics—ACM-BCB ‘17, Boston, MA, USA, 20–23 August 2017; pp. 223–232. [Google Scholar] [CrossRef]
- Philippe, M.; Neely, M.; Rushing, T.; Bertrand, Y.; Bleyzac, N.; Goutelle, S. Maximal concentration of intravenous busulfan as a determinant of veno-occlusive disease: A pharmacokinetic-pharmacodynamic analysis in 293 hematopoietic stem cell transplanted children. Bone Marrow Transplant. 2019, 54, 448–457. [Google Scholar] [CrossRef] [PubMed]
- Guo, T.; van Hest, R.M.; Roggeveen, L.F.; Fleuren, L.M.; Thoral, P.J.; Bosman, R.J.; van der Voort, P.H.J.; Girbes, A.R.J.; Mathot, R.A.A.; Elbers, P.W.G. External Evaluation of Population Pharmacokinetic Models of Vancomycin in Large Cohorts of Intensive Care Unit Patients. Antimicrob. Agents Chemother. 2019, 63, e02543-18. [Google Scholar] [CrossRef] [PubMed]
- Zhao, C.Y.; Jiao, Z.; Mao, J.J.; Qiu, X.Y. External evaluation of published population pharmacokinetic models of tacrolimus in adult renal transplant recipients. Br. J. Clin. Pharmacol. 2016, 81, 891–907. [Google Scholar] [CrossRef] [PubMed]
- Paci, A.; Vassal, G.; Moshous, D.; Dalle, J.H.; Bleyzac, N.; Neven, B.; Galambrun, C.; Kemmel, V.; Abdi, Z.D.; Broutin, S.; et al. Pharmacokinetic behavior and appraisal of intravenous busulfan dosing in infants and older children: The results of a population pharmacokinetic study from a large pediatric cohort undergoing hematopoietic stem-cell transplantation. Ther. Drug Monit. 2012, 34, 198–208. [Google Scholar] [CrossRef]
- Traub, S.L.; Johnson, C.E. Comparison of methods of estimating creatinine clearance in children. Am. J. Hosp. Pharm. 1980, 37, 195–201. [Google Scholar] [CrossRef]
- Booth, B.P.; Rahman, A.; Dagher, R.; Griebel, D.; Lennon, S.; Fuller, D.; Sahajwalla, C.; Mehta, M.; Gobburu, J.V. Population pharmacokinetic-based dosing of intravenous busulfan in pediatric patients. J. Clin. Pharmacol. 2007, 47, 101–111. [Google Scholar] [CrossRef]
- Trame, M.N.; Bergstrand, M.; Karlsson, M.O.; Boos, J.; Hempel, G. Population pharmacokinetics of busulfan in children: Increased evidence for body surface area and allometric body weight dosing of busulfan in children. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2011, 17, 6867–6877. [Google Scholar] [CrossRef]
- Guidi, M.; Csajka, C.; Buclin, T. Parametric Approaches in Population Pharmacokinetics. J. Clin. Pharmacol. 2020, 62, 125–141. [Google Scholar] [CrossRef]
- Goutelle, S.; Woillard, J.B.; Neely, M.; Yamada, W.; Bourguignon, L. Nonparametric Methods in Population Pharmacokinetics. J. Clin. Pharmacol. 2022, 62, 142–157. [Google Scholar] [CrossRef]
- Goutelle, S.; Woillard, J.B.; Buclin, T.; Bourguignon, L.; Yamada, W.; Csajka, C.; Neely, M.; Guidi, M. Parametric and Nonparametric Methods in Population Pharmacokinetics: Experts’ Discussion on Use, Strengths, and Limitations. J. Clin. Pharmacol. 2022, 62, 158–170. [Google Scholar] [CrossRef]
- Goutelle, S.; Alloux, C.; Bourguignon, L.; Van Guilder, M.; Neely, M.; Maire, P. To Estimate or to Forecast? Lessons From a Comparative Analysis of Four Bayesian Fitting Methods Based on Nonparametric Models. Ther. Drug Monit. 2021, 43, 461–471. [Google Scholar] [CrossRef] [PubMed]
- Kantasiripitak, W.; Van Daele, R.; Gijsen, M.; Ferrante, M.; Spriet, I.; Dreesen, E. Software Tools for Model-Informed Precision Dosing: How Well Do They Satisfy the Needs? Front. Pharmacol. 2020, 11, 620. [Google Scholar] [CrossRef] [PubMed]
- Shukla, P.; Dvorak, C.C.; Long-Boyle, J.; Kharbanda, S. Lower Exposure to Busulfan Allows for Stable Engraftment of Donor Hematopoietic Stem Cells in Children with Mucopolysaccharidosis Type I: A Case Report of Four Patients. Int. J. Mol. Sci. 2020, 21, 5634. [Google Scholar] [CrossRef] [PubMed]
- Lawson, R.; Paterson, L.; Fraser, C.J.; Hennig, S. Evaluation of two software using Bayesian methods for monitoring exposure and dosing once-daily intravenous busulfan in paediatric patients receiving haematopoietic stem cell transplantation. Cancer Chemother. Pharmacol. 2021, 88, 379–391. [Google Scholar] [CrossRef]
- Keizer, R.J.; Ter Heine, R.; Frymoyer, A.; Lesko, L.J.; Mangat, R.; Goswami, S. Model-Informed Precision Dosing at the Bedside: Scientific Challenges and Opportunities. CPT Pharmacomet. Syst. Pharmacol. 2018, 7, 785–787. [Google Scholar] [CrossRef]
- Burgard, M.; Sandaradura, I.; van Hal, S.J.; Stacey, S.; Hennig, S. Evaluation of Tobramycin Exposure Predictions in Three Bayesian Forecasting Programmes Compared with Current Clinical Practice in Children and Adults with Cystic Fibrosis. Clin. Pharmacokinet. 2018, 57, 1017–1027. [Google Scholar] [CrossRef]
- Heitzmann, J.; Thoma, Y.; Bricca, R.; Gagnieu, M.C.; Leclerc, V.; Roux, S.; Conrad, A.; Ferry, T.; Goutelle, S. Implementation and Comparison of Two Pharmacometric Tools for Model-Based Therapeutic Drug Monitoring and Precision Dosing of Daptomycin. Pharmaceutics 2022, 14, 114. [Google Scholar] [CrossRef]
- Goutelle, S.; Jay, L.; Boidin, C.; Cohen, S.; Bourguignon, L.; Bleyzac, N.; Wallet, F.; Vassal, O.; Friggeri, A. Pharmacokinetic/Pharmacodynamic Dosage Individualization of Cefepime in Critically Ill Patients: A Case Study. Ther. Drug Monit. 2021, 43, 451–454. [Google Scholar] [CrossRef]
- Hughes, J.H.; Tong, D.M.H.; Lucas, S.S.; Faldasz, J.D.; Goswami, S.; Keizer, R.J. Continuous Learning in Model-Informed Precision Dosing: A Case Study in Pediatric Dosing of Vancomycin. Clin. Pharmacol. Ther. 2021, 109, 233–242. [Google Scholar] [CrossRef]
- Abrantes, J.A.; Jonsson, S.; Karlsson, M.O.; Nielsen, E.I. Handling interoccasion variability in model-based dose individualization using therapeutic drug monitoring data. Br. J. Clin. Pharmacol. 2019, 85, 1326–1336. [Google Scholar] [CrossRef]
- Keutzer, L.; Simonsson, U.S.H. Individualized Dosing With High Inter-Occasion Variability Is Correctly Handled With Model-Informed Precision Dosing-Using Rifampicin as an Example. Front. Pharmacol. 2020, 11, 794. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Tucuxi Model [16] | BestDose Model [10] | ||
|---|---|---|---|
| Parameter | Value | Parameter | Value |
| Typical CL (L/h) | 2.18 | Median KeS (h−1·kg−0.25) (min–max) | 0.71 (0.42–0.98) |
| Typical V (L) | BW0.86 | Median VS (L·kg−1) (min–max) | 0.72 (0.53–1.40) |
| CL variability (CV) | 23% | KeS variability (CV) | 18% |
| V variability (CV) | 22% | VS variability (CV) | 21% |
| Residual error | 11% (proportional) 57 ng/mL (additive SD) | Residual error a | SD (mg/L) = 0.02 + 0.1·Cobs |
| Model [Reference] | Population Characteristics | Model Characteristics | MPE (%) [95% Confidence Interval] | RMSE (%) | ||
|---|---|---|---|---|---|---|
| Model without IOV | Model with IOV | Model without IOV | Model with IOV | |||
| Paci et al. [16] | n = 205 Median age, 2.5 years (10 days–15 years) Median BW, 12 (3.5–62.5) kg | One-compartment CL~BW (allometric) V~BW (allometric) IOV on CL | 2.7 [1.7–3.7] | 1.6 [0.8–2.3] | 12.2 | 8.7 |
| Booth et al. [18] | n = 24 Mean age, 6.3 years (3 months–16.7 years) Mean BW, 23.8 (7.1–62.6) kg | One-compartment CL~BW (allometric) V~BW (allometric) IOV on CL and V | 2.1 [1.0–3.3] | 1.1 [0.3–1.9] | 13.4 | 9.5 |
| Trame et al. [19] | n = 94 Median age, 9.2 (0.4–18.8) years Median BW, 27.2 (4.2–80) kg | One-compartment CL~BW (allometric) V~BW (allometric) IOV on CL and V | 7.1 [5.1–9.3] | 5.0 [3.2–6.8] | 26.2 | 22.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goutelle, S.; Thoma, Y.; Buffet, R.; Philippe, M.; Buclin, T.; Guidi, M.; Csajka, C. Implementation and Cross-Validation of a Pharmacokinetic Model for Precision Dosing of Busulfan in Hematopoietic Stem Cell Transplanted Children. Pharmaceutics 2022, 14, 2107. https://doi.org/10.3390/pharmaceutics14102107
Goutelle S, Thoma Y, Buffet R, Philippe M, Buclin T, Guidi M, Csajka C. Implementation and Cross-Validation of a Pharmacokinetic Model for Precision Dosing of Busulfan in Hematopoietic Stem Cell Transplanted Children. Pharmaceutics. 2022; 14(10):2107. https://doi.org/10.3390/pharmaceutics14102107
Chicago/Turabian StyleGoutelle, Sylvain, Yann Thoma, Roxane Buffet, Michael Philippe, Thierry Buclin, Monia Guidi, and Chantal Csajka. 2022. "Implementation and Cross-Validation of a Pharmacokinetic Model for Precision Dosing of Busulfan in Hematopoietic Stem Cell Transplanted Children" Pharmaceutics 14, no. 10: 2107. https://doi.org/10.3390/pharmaceutics14102107
APA StyleGoutelle, S., Thoma, Y., Buffet, R., Philippe, M., Buclin, T., Guidi, M., & Csajka, C. (2022). Implementation and Cross-Validation of a Pharmacokinetic Model for Precision Dosing of Busulfan in Hematopoietic Stem Cell Transplanted Children. Pharmaceutics, 14(10), 2107. https://doi.org/10.3390/pharmaceutics14102107