
Impact of Early Intrapatient Variability of Tacrolimus Concentrations on the Risk of Graft-Versus-Host Disease after Allogeneic Stem Cell Transplantation Using High-Dose Post-Transplant Cyclophosphamide
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. Baseline Characteristics of the Patients
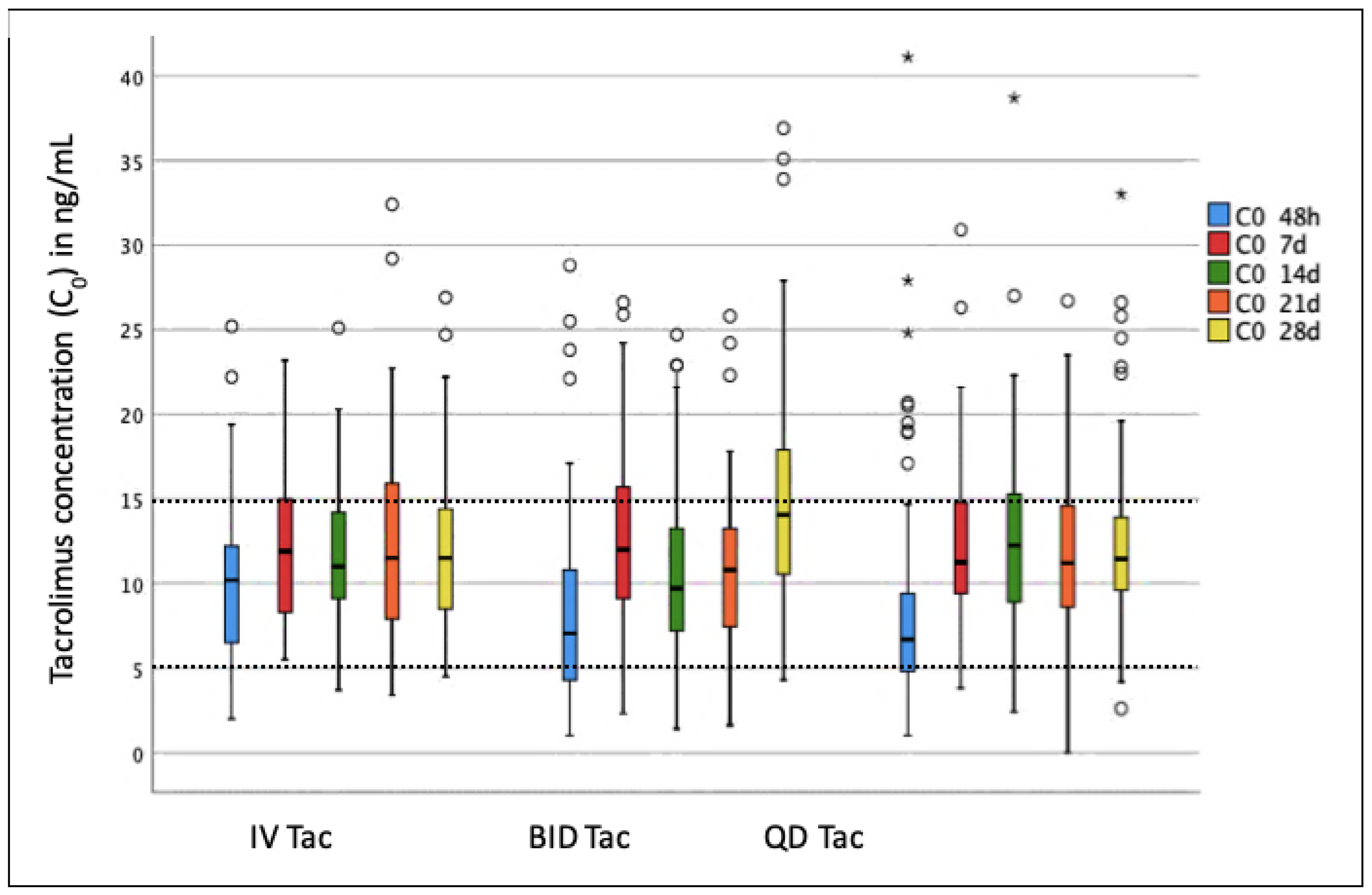
2.2. Tacrolimus IPV, TISS, and C0 Levels
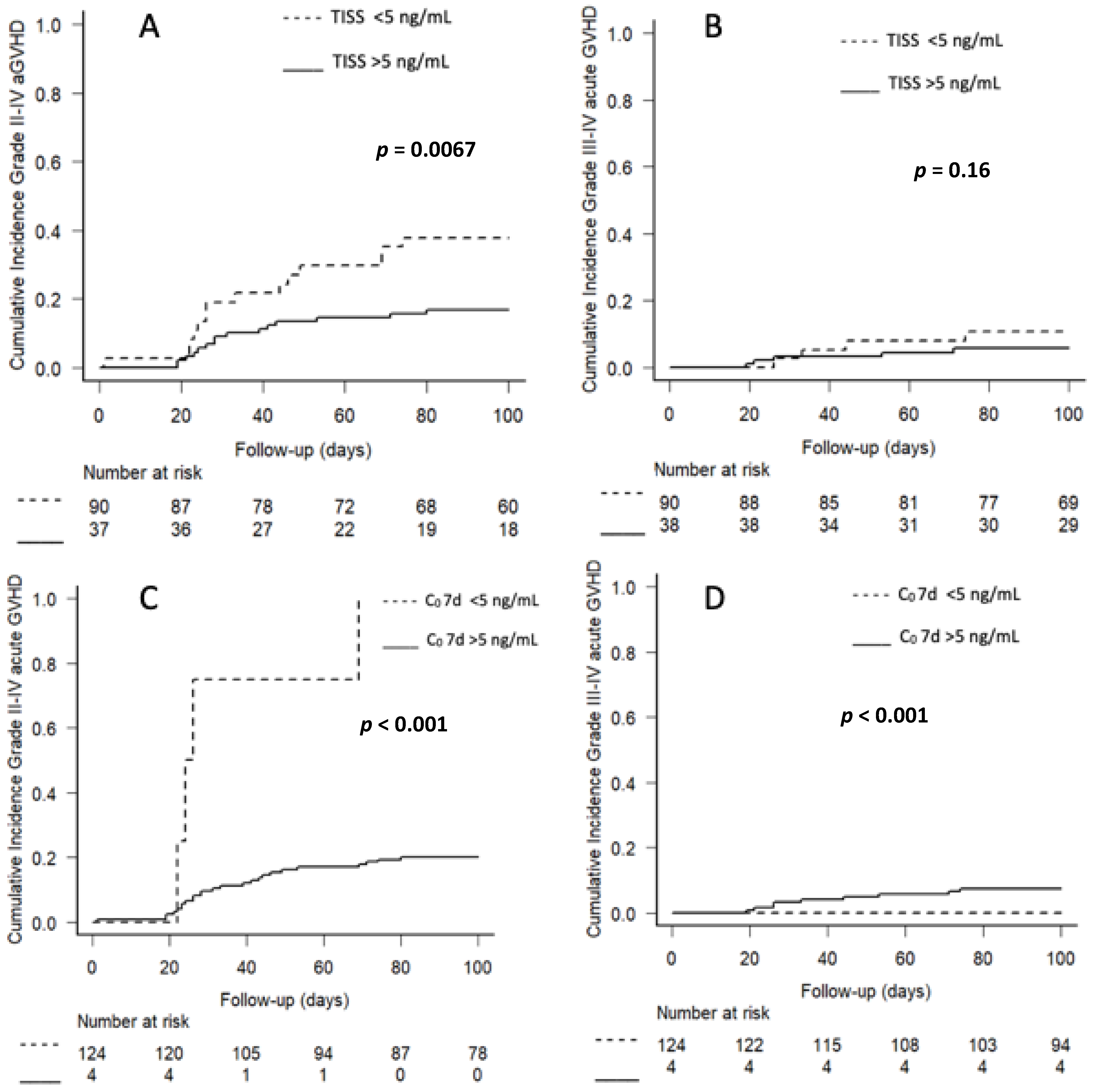
2.3. Impact of Tacrolimus IPV, TISS, and C0 on Acute GVHD
2.4. Impact of Tacrolimus IPV, TISS, and C0 on Toxicity
2.5. Impact of Tacrolimus IPV, TISS, and C0 on Transplant Related Mortality, Relapse Rate, Overall Survival, and Disease-Free Survival
3. Discussion
4. Materials and Methods
4.1. Patients and Donors
4.2. Treatment Protocol and Supportive Care
4.3. Laboratory Measurements
4.4. Endpoints of the Study
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- McDonald, G.B.; Sandmaier, B.M.; Mielcarek, M.; Sorror, M.; Pergam, S.A.; Cheng, G.-S.; Hingorani, S.; Boeckh, M.; Flowers, M.D.; Lee, S.J.; et al. Survival, Nonrelapse Mortality, and Relapse-Related Mortality After Allogeneic Hematopoietic Cell Transplantation: Comparing 2003–2007 Versus 2013–2017 Cohorts. Ann. Intern. Med. 2020, 172, 229–239. [Google Scholar] [CrossRef]
- Choi, S.W.; Reddy, P. Current and emerging strategies for the prevention of graft-versus-host disease. Nat. Rev. Clin. Oncol. 2014, 11, 536–547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Penack, O.; Marchetti, M.; Ruutu, T.; Aljurf, M.; Bacigalupo, A.; Bonifazi, F.; Ciceri, F.; Cornelissen, J.; Malladi, R.; Duarte, R.F.; et al. Prophylaxis and management of graft versus host disease after stem-cell transplantation for haematological malignancies: Updated consensus recommendations of the European Society for Blood and Marrow Transplantation. Lancet Haematol. 2020, 7, e157–e167. [Google Scholar] [CrossRef]
- Bacigalupo, A.; Lamparelli, T.; Barisione, G.; Bruzzi, P.; Guidi, S.; Alessandrino, P.E.; di Bartolomeo, P.; Oneto, R.; Bruno, B.; Sacchi, N.; et al. Thymoglobulin Prevents Chronic Graft-versus-Host Disease, Chronic Lung Dysfunction, and Late Transplant-Related Mortality: Long-Term Follow-Up of a Randomized Trial in Patients Undergoing Unrelated Donor Transplantation. Biol. Blood Marrow Transplant. 2006, 12, 560–565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soiffer, R.J.; Kim, H.T.; McGuirk, J.; Horwitz, M.E.; Johnston, L.; Patnaik, M.M.; Rybka, W.; Artz, A.; Porter, D.L.; Shea, T.C.; et al. Prospective, Randomized, Double-Blind, Phase III Clinical Trial of Anti–T-Lymphocyte Globulin to Assess Impact on Chronic Graft-Versus-Host Disease–Free Survival in Patients Undergoing HLA-Matched Unrelated Myeloablative Hematopoietic Cell Transplantation. J. Clin. Oncol. 2017, 35, 4003–4011. [Google Scholar] [CrossRef] [PubMed]
- Luznik, L.; O’Donnell, P.V.; Symons, H.J.; Chen, A.R.; Leffell, M.S.; Zahurak, M.; Gooley, T.A.; Piantadosi, S.; Kaup, M.; Ambinder, R.F.; et al. HLA-Haploidentical Bone Marrow Transplantation for Hematologic Malignancies Using Nonmyeloablative Conditioning and High-Dose, Posttransplantation Cyclophosphamide. Biol. Blood Marrow Transplant. 2008, 14, 641–650. [Google Scholar] [CrossRef] [Green Version]
- Bolaños-Meade, J.; Reshef, R.; Fraser, R.; Fei, M.; Abhyankar, S.; Al-Kadhimi, Z.; Alousi, A.M.; Antin, J.H.; Arai, S.; Bickett, K.; et al. Three prophylaxis regimens (tacrolimus, mycophenolate mofetil, and cyclophosphamide; tacrolimus, methotrexate, and bortezomib; or tacrolimus, methotrexate, and maraviroc) versus tacrolimus and methotrexate for prevention of graft-versus-host disease with haemopoietic cell transplantation with reduced-intensity conditioning: A randomised phase 2 trial with a non-randomised contemporaneous control group (BMT CTN 1203). Lancet Haematol. 2019, 6, e132–e143. [Google Scholar] [CrossRef] [PubMed]
- De Jong, C.N.; Meijer, E.; Bakunina, K.; Nur, E.; Kooij, M.V.M.; De Groot, M.R.; Van Gelder, M.; Maertens, J.A.; Kuball, J.H.; Deeren, D.; et al. Post-Transplantation Cyclophosphamide after Allogeneic Hematopoietic Stem Cell Transplantation: Results of the Prospective Randomized HOVON-96 Trial in Recipients of Matched Related and Unrelated Donors. Blood 2019, 134, 1. [Google Scholar] [CrossRef]
- Brunet, M.; Van Gelder, T.; Åsberg, A.; Haufroid, V.; Hesselink, D.A.; Langman, L.; Lemaitre, F.; Marquet, P.; Seger, C.; Shipkova, M.; et al. Therapeutic Drug Monitoring of Tacrolimus-Personalized Therapy: Second Consensus Report. Ther. Drug Monit. 2019, 41, 261–307. [Google Scholar] [CrossRef]
- Gao, Y.; Ma, J. Tacrolimus in adult hematopoietic stem cell transplantation. Expert Opin. Drug Metab. Toxicol. 2019, 15, 803–811. [Google Scholar] [CrossRef]
- Wingard, J.R.; Nash, R.A.; Przepiorka, N.; Klein, J.L.; Weisdorf, D.J.; Fay, J.W.; Zhu, J.; Maher, R.M.; Fitzsimmons, W.E.; Ratanatharathorn, V. Relationship of tacrolimus (FK506) whole blood concentrations and efficacy and safety after HLA-identical sibling bone marrow transplantation. Biol. Blood Marrow Transplant. 1998, 4, 157–163. [Google Scholar] [CrossRef]
- Przepiorka, D.; Devine, S.; Fay, J.; Uberti, J.; Wingard, J. Practical considerations in the use of tacrolimus for allogeneic marrow transplantation. Bone Marrow Transplant. 1999, 24, 1053–1056. [Google Scholar] [CrossRef] [Green Version]
- Cutler, C.; Logan, B.R.; Nakamura, R.; Johnston, L.J.; Choi, S.; Porter, D.L.; Hogan, W.J.; Pasquini, M.C.; MacMillan, M.; Hsu, J.W.; et al. Tacrolimus/sirolimus vs tacrolimus/methotrexate as GVHD prophylaxis after matched, related donor allogeneic HCT. Blood 2014, 124, 1372–1377. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, R.; Rodriguez, R.; Nademanee, A.; Palmer, J.; Senitzer, D.; Snyder, D.; Zain, J.; Pullarkat, V.; Forman, S.J.; Parker, P.M. The Use of Sirolimus Combined with Tacrolimus and Low-Dose Methotrexate Is Effective in Preventing Graft-Versus-Host Disease after Unrelated Donor Hematopoietic Stem Cell Transplantation. Blood 2006, 108, 2866. [Google Scholar] [CrossRef]
- Ganetsky, A.; Shah, A.; Miano, T.; Hwang, W.-T.; He, J.; Loren, A.W.; Hexner, E.O.; Frey, N.V.; Porter, D.L.; Reshef, R. Higher tacrolimus concentrations early after transplant reduce the risk of acute GvHD in reduced-intensity allogeneic stem cell transplantation. Bone Marrow Transplant. 2015, 51, 568–572. [Google Scholar] [CrossRef] [Green Version]
- Mori, T.; Kato, J.; Shimizu, T.; Aisa, Y.; Nakazato, T.; Yamane, A.; Ono, Y.; Kunimoto, H.; Okamoto, S. Effect of Early Posttransplantation Tacrolimus Concentration on the Development of Acute Graft-versus-Host Disease after Allogeneic Hematopoietic Stem Cell Transplantation from Unrelated Donors. Biol. Blood Marrow Transplant. 2011, 18, 229–234. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, N.; Matsumoto, K.; Muramatsu, H.; Horibe, K.; Matsuyama, T.; Kojima, S.; Kato, K. Relationship between tacrolimus blood concentrations and clinical outcome during the first 4 weeks after SCT in children. Bone Marrow Transplant. 2009, 45, 1161–1166. [Google Scholar] [CrossRef]
- Schumacher, L.; Leino, A.D.; Park, J.M. Tacrolimus intrapatient variability in solid organ transplantation: A multiorgan perspective. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2020, 41, 103–118. [Google Scholar] [CrossRef] [PubMed]
- Kuypers, D.R.J. Intrapatient Variability of Tacrolimus Exposure in Solid Organ Transplantation: A Novel Marker for Clinical Outcome. Clin. Pharmacol. Ther. 2020, 107, 347–358. [Google Scholar] [CrossRef] [PubMed]
- Gonzales, H.M.; McGillicuddy, J.W.; Rohan, V.; Chandler, J.L.; Nadig, S.N.; Dubay, D.A.; Taber, D.J. A comprehensive review of the impact of tacrolimus intrapatient variability on clinical outcomes in kidney transplantation. Am. J. Transplant. 2020, 20, 1969–1983. [Google Scholar] [CrossRef] [PubMed]
- Whalen, H.R.; Glen, J.A.; Harkins, V.; Stevens, K.K.; Jardine, A.G.; Geddes, C.C.; Clancy, M.J. High Intrapatient Tacrolimus Variability Is Associated With Worse Outcomes in Renal Transplantation Using a Low-Dose Tacrolimus Immunosuppressive Regime. Transplantation 2017, 101, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Del Bello, A.; Congy-Jolivet, N.; Danjoux, M.; Muscari, F.; Lavayssière, L.; Esposito, L.; Hebral, A.-L.; Bellière, J.; Kamar, N. High tacrolimus intra-patient variability is associated with graft rejection, and de novo donor-specific antibodies occurrence after liver transplantation. World J. Gastroenterol. 2018, 24, 1795–1802. [Google Scholar] [CrossRef] [PubMed]
- Gueta, I.; Markovits, N.; Yarden-Bilavsky, H.; Raichlin, E.; Freimark, D.; Lavee, J.; Loebstein, R.; Peled, Y. High tacrolimus trough level variability is associated with rejections after heart transplant. Am. J. Transplant. 2018, 18, 2571–2578. [Google Scholar] [CrossRef] [Green Version]
- Beilhack, A.; Schulz, S.; Baker, J.; Beilhack, G.F.; Wieland, C.B.; Herman, E.I.; Baker, E.M.; Cao, Y.-A.; Contag, C.; Negrin, R.S. In vivo analyses of early events in acute graft-versus-host disease reveal sequential infiltration of T-cell subsets. Blood 2005, 106, 1113–1122. [Google Scholar] [CrossRef]
- Hagen, P.A.; Adams, W.; Smith, S.; Tsai, S.; Stiff, P. Low mean post-transplantation tacrolimus levels in weeks 2–3 correlate with acute graft-versus-host disease in allogeneic hematopoietic stem cell transplantation from related and unrelated donors. Bone Marrow Transplant. 2018, 54, 155–158. [Google Scholar] [CrossRef]
- Yao, J.M.; Yang, D.; Clark, M.C.; Otoukesh, S.; Cao, T.; Ali, H.; Arslan, S.; Aldoss, I.; Artz, A.; Amanam, I.; et al. Tacrolimus initial steady state level in post-transplant cyclophosphamide-based GvHD prophylaxis regimens. Bone Marrow Transplant. 2021, 57, 232–242. [Google Scholar] [CrossRef]
- Pedraza, A.; Jorge, S.; Suárez-Lledó, M.; Pereira, A.; Gutiérrez-García, G.; Fernández-Avilés, F.; Rosiñol, L.; Llobet, N.; Solano, T.; Urbano-Ispízua, Á.; et al. High-Dose Cyclophosphamide and Tacrolimus as Graft-versus-Host Disease Prophylaxis for Matched and Mismatched Unrelated Donor Transplantation. Transplant. Cell. Ther. 2021, 27, 619.e1–619.e8. [Google Scholar] [CrossRef]
- Ljungman, P.; de la Camara, R.; Robin, C.; Crocchiolo, R.; Einsele, H.; Hill, J.A.; Hubacek, P.; Navarro, D.; Cordonnier, C.; Ward, K.N. Guidelines for the management of cytomegalovirus infection in patients with haematological malignancies and after stem cell transplantation from the 2017 European Conference on Infections in Leukaemia (ECIL 7). Lancet Infect. Dis. 2019, 19, e260–e272. [Google Scholar] [CrossRef]
- Einsele, H.; Ljungman, P.T.; Boeckh, M.J. How I treat CMV reactivation after allogeneic hematopoietic stem cell transplantation. Blood 2020, 135, 1619–1629. [Google Scholar] [CrossRef] [PubMed]
- Levine, J.E.; Hogan, W.J.; Harris, A.; Litzow, M.R.; Efebera, Y.A.; Devine, S.M.; Reshef, R.; Ferrara, J.L. Improved accuracy of acute graft-versus-host disease staging among multiple centers. Best Pract. Res. Clin. Haematol. 2014, 27, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Kellum, J.A.; Lameire, N.; Aspelin, P.; Barsoum, R.S.; Burdmann, E.A.; Goldstein, S.L.; Herzog, C.A.; Joannidis, M.; Kribben, A.; Levey, A.S.; et al. Improving global outcomes (KDIGO) acute kidney injury work group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int. Suppl. 2012, 2, 1–138. [Google Scholar] [CrossRef] [Green Version]
- Cho, B.-S.; Yahng, S.-A.; Lee, S.-E.; Eom, K.-S.; Kim, Y.-J.; Kim, H.-J.; Lee, S.; Min, C.-K.; Cho, S.-G.; Kim, D.-W.; et al. Validation of Recently Proposed Consensus Criteria for Thrombotic Microangiopathy After Allogeneic Hematopoietic Stem-Cell Transplantation. Transplantation 2010, 90, 918–926. [Google Scholar] [CrossRef] [PubMed]
- Jodele, S.; Laskin, B.L.; Dandoy, C.E.; Myers, K.C.; El-Bietar, J.; Davies, S.M.; Goebel, J.; Dixon, B.P. A new paradigm: Diagnosis and management of HSCT-associated thrombotic microangiopathy as multi-system endothelial injury. Blood Rev. 2015, 29, 191–204. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | All Patients n = 128 |
|---|---|
| Age at HSCT, years | |
| Median (range) | 49 (18–69) |
| Sex (male/female) n (%) | 72 (56)/56 (44) |
| HCT Comorbidity Index n (%) | |
| ≤2 | 66 (52) |
| >2 | 62 (48) |
| Primary Diagnosis n (%) | |
| Acute leukemia/Myelodysplastic syndrome | 89 (70) |
| Lymphoma | 23 (18) |
| Multiple myeloma | 4 (3) |
| Chronic mieloproliferative syndromes | 11 (8) |
| Malignant histiocytosis | 1 (1) |
| Disease Status at Transplant n (%) | |
| Complete response | 86 (67) |
| Partial response | 25 (20) |
| Stable disease/Progression of disease | 17 (13) |
| Conditioning Regimen n (%) | |
| Myeloablative | 49 (38) |
| Fludarabine-busulphan | 27 |
| Fludarabine-total body irradiation 12 Gy | 17 |
| Other | 5 |
| Reduced intensity | 79 (62) |
| Fludarabine-busulphan | 45 |
| Fludarabine-total body irradiation 8 Gy | 27 |
| FLAG-IDA-melphalan | 4 |
| Other | 3 |
| Donor Type n (%) | |
| HLA 10/10 matched sibling | 24 (19) |
| HLA 5/10 haploidentical sibling | 22 (17) |
| HLA 10/10 matched unrelated | 41 (32) |
| HLA 9/10 mismatched unrelated | 41 (32) |
| Graft Source n (%) | |
| Peripheral blood | 125 (98) |
| Bone marrow | 3 (2) |
| GVHD Prophylaxis Regimen n (%) | |
| PTCy-tacrolimus | 94 (73) |
| PTCy-tacrolimus-MMF | 34 (27) |
| Tacrolimus Formulation at Initiation n (%) | |
| Intravenous | 36 (28) |
| Twice daily oral | 32 (25) |
| Once daily oral modified release | 60 (47) |
| Cytomegalovirus Risk n (%) | |
| Low | 18 (14) |
| Intermediate | 70 (55) |
| High | 40 (31) |
| Pretransplant Renal Function | |
| Creatinine, mg/dL, median (range) | 0.76 (0.39–1.85) |
| Grade II–IV aGVHD HR (95% CI) | p | Grade III–IV aGVHD HR (95% CI) | p | ||
|---|---|---|---|---|---|
| Patient Age | Continuous variable | 1.01 (0.98–1.03) | 0.56 | 1.04 (0.99–1.08) | 0.07 |
| Conditioning Regimen | Myeloablative (vs. RIC) | 2.77 (1.36–5.88) | 0.005 | 2.53 (0.72–8.79) | 0.15 |
| Disease Status at Transplant | Complete remission (vs. other) | 0.99 (0.91–1.08) | 0.82 | 0.93 (0.79–1.09) | 0.39 |
| Donor sex | Female (vs. male) | 0.89 (0.43–1.85) | 0.76 | 2.06 (0.43–9.72) | 0.36 |
| Donor Type | Mismatch (vs. match) | 0.67 (0.32–1.39) | 0.28 | 0.80 (0.23–2.83) | 0.73 |
| CMV | High risk (vs. other) | 1.19 (0.56–2.58) | 0.65 | 0.55 (0.11–2.61) | 0.45 |
| Tac formulation | Oral (vs. intravenous) | 1.31 (0.56–3.06) | 0.54 | 1.58 (0.33–7.50) | 0.57 |
| Tac IPV | >25th percentile (vs. ≤25th) >50th percentile (vs. ≤50th) >75th percentile (vs. ≤75th) | 5.53 (0.87–7.35) 3.86 (1.65–9.01) 3.30 (1.62–6.7) | 0.088 0.0018 <0.001 | 3.32 (0.41–26.8) 9.69 (1.20–77.9) 4.99 (1.42–17.49) | 0.26 0.033 0.012 |
| Tac TISS | <5 ng/mL (vs. ≥5) | 2.65 (1.31–5.36) | 0.0067 | 2.39 (0.7–8.16) | 0.16 |
| Tac C0 at 7 days | <5 ng/mL (vs. ≥5) | 10.52 (4.88–22.68) | <0.001 | * | |
| Tac C0 at 14 days | <5 ng/mL (vs. ≥5) | 1.01 (0.27–3.79) | 0.99 | 4.30 (0.99–18.72) | 0.05 |
| Tac C0 at 21 days | ** | - | - | - | - |
| Tac C0 at 28 days | <5 ng/mL (vs. ≥5) | 1.08 (0.14–8.28) | 0.94 | 4.96 (0.60–41.01) | 0.14 |
| Grade II-IV aGVHD HR (95% CI) | p | Grade III-IV aGVHD HR (95% CI) | p | ||
|---|---|---|---|---|---|
| Patient Age | Continuous variable | 1.03 (1.00–1.07) | 0.028 | 1.11 (1.05–1.18) | <0.001 |
| Conditioning Regimen | Myeloablative (vs. RIC) | 4.46 (1.87–10.65) | <0.001 | 9.94 (2.84–34.77) | <0.001 |
| Donor Type | Mismatch (vs. match) | 0.57 (0.27–1.22) | 0.15 | 0.79 (0.20–3.17) | 0.75 |
| Tac IPV | >50th percentile (vs. ≤50th) | 2.99 (1.21–7.39) | 0.018 | 9.12 (1.03–80.56) | 0.047 |
| Tac TISS | ≥5 ng/mL | 1.45 (0.65–3.21) | 0.36 | 0.77 (0.22–2.71) | 0.69 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marco, D.N.; Salas, M.Q.; Gutiérrez-García, G.; Monge, I.; Riu, G.; Carcelero, E.; Roma, J.R.; Llobet, N.; Arcarons, J.; Suárez-Lledó, M.; et al. Impact of Early Intrapatient Variability of Tacrolimus Concentrations on the Risk of Graft-Versus-Host Disease after Allogeneic Stem Cell Transplantation Using High-Dose Post-Transplant Cyclophosphamide. Pharmaceuticals 2022, 15, 1529. https://doi.org/10.3390/ph15121529
Marco DN, Salas MQ, Gutiérrez-García G, Monge I, Riu G, Carcelero E, Roma JR, Llobet N, Arcarons J, Suárez-Lledó M, et al. Impact of Early Intrapatient Variability of Tacrolimus Concentrations on the Risk of Graft-Versus-Host Disease after Allogeneic Stem Cell Transplantation Using High-Dose Post-Transplant Cyclophosphamide. Pharmaceuticals. 2022; 15(12):1529. https://doi.org/10.3390/ph15121529
Chicago/Turabian StyleMarco, Daniel N., María Queralt Salas, Gonzalo Gutiérrez-García, Inés Monge, Gisela Riu, Esther Carcelero, Joan Ramón Roma, Noemí Llobet, Jordi Arcarons, María Suárez-Lledó, and et al. 2022. "Impact of Early Intrapatient Variability of Tacrolimus Concentrations on the Risk of Graft-Versus-Host Disease after Allogeneic Stem Cell Transplantation Using High-Dose Post-Transplant Cyclophosphamide" Pharmaceuticals 15, no. 12: 1529. https://doi.org/10.3390/ph15121529