
An Overview of Obesity, Cholesterol, and Systemic Inflammation in Preeclampsia


1
Departments of Veterinary Clinical Sciences, School of Veterinary Medicine, Louisiana State University, Baton Rouge, LA 70803, USA
2
Reproductive Endocrinology and Women’s Health Laboratory, Pennington Biomedical Research Center, Baton Rouge, LA 70808, USA
*
Author to whom correspondence should be addressed.
Nutrients 2022, 14(10), 2087; https://doi.org/10.3390/nu14102087
Submission received: 17 April 2022
/
Revised: 12 May 2022
/
Accepted: 14 May 2022
/
Published: 17 May 2022
(This article belongs to the Special Issue Nutrient and Hormone Sensing Mechanisms and Signaling Pathways)
Abstract
:Preeclampsia (PE), an inflammatory state during pregnancy, is a significant cause of maternal and fetal morbidity and mortality. Adverse outcomes associated with PE include hypertension, proteinuria, uterine/placental abnormalities, fetal growth restriction, and pre-term birth. Women with obesity have an increased risk of developing PE likely due to impaired placental development from altered metabolic homeostasis. Inflammatory cytokines from maternal adipose tissue and circulating cholesterol have been linked to systemic inflammation, hypertension, and other adverse outcomes associated with PE. This review will summarize the current knowledge on the role of nutrients, obesity, and cholesterol signaling in PE with an emphasis on findings from preclinical models.
Keywords:
preeclampsia; inflammation; hypertension; obesity; cytokines; metabolic abnormalities; leptin; cholesterol1. Maternal Risk Factors of PE
Preeclampsia (PE) is a leading cause of maternal and fetal mortality and morbidity [1]. Worldwide, 5–7% of all pregnancies are affected, resulting in 70,000 maternal deaths and 500,000 fetal deaths from PE each year [2]. In human pregnancy, the clinical presentation of PE includes new-onset hypertension along with the development of proteinuria, endothelial dysfunction, or another accompanying signs/symptoms of multiorgan dysfunction [3]. Maternal hypertension is determined when two blood pressure readings taken at least 6 h apart both display a systolic value greater than 140 mmHg and a diastolic value greater than 90 mmHg [4]. Signs and symptoms present after 20 weeks of gestation [4]. Prior to 34 weeks of gestation, PE is considered early onset; however, the disorder can arise through to delivery, and after 34 weeks is considered late onset [4]. Many factors are suspected to contribute to the development of PE, with family history, advanced maternal age in pregnancy (>35 years of age), and pre-existing medical conditions (e.g., obesity, hypertension, diabetes or renal dysfunction) conferring the highest risk [3]. This review specifically describes the potential mechanism linking obesity, cholesterol, and systemic inflammation to PE.
PE is associated with uterine and placental abnormalities and adverse fetal co-morbidities such as intrauterine growth restriction and preterm birth [3]. In a healthy pregnancy, placentation begins with trophoblast invasion into the uterine arteries. Arterioles are remodeled into high capacitance and high flow vessels to provide the fetus with nutrients [2]. In preeclamptic pregnancy, trophoblast invasion is inadequate and thus vascular remodeling is impaired, which results in narrowed maternal vessels and placental ischemia [2]. Poor perfusion of oxygen within the uterine vasculature can lead to hypoxia, oxidative stress and the release of antiangiogenic factors such as soluble fms-like tyrosine kinase 1 (sFLT1) [2]. sFLT1 increases vasoconstriction and contributes to maternal metabolic dysfunction by raising blood pressure [5]. An increase in sFLT1 is also associated with a decrease in placental growth factor (PIGF), a member of the vascular endothelial growth factor (VEGF) family [5]. The imbalance of sFLT1 and PIGF further contributes to the development of placental dysfunction and the clinical presentation of PE [5].
2. Obesity and Systemic Inflammation in Pregnancy
Obesity affects more than 2 billion people worldwide, thus explaining the term “globesity” [6]. Compared to normal weight, obesity causes inflammatory changes in the adipose tissue that increase the risk for PE by worsening metabolic abnormalities such as insulin resistance, inflammation, and atherosclerotic disease [7]. With the incidence of maternal obesity and cases of PE rising worldwide, there is an urgent need to understand whether and how the attenuation of maternal obesity can improve PE and its downstream outcomes [8].
Adipose tissue, composed of adipocytes, immune cells, and stromal vascular cells, acts as an endocrine organ that participates in modulating systemic inflammatory and immune responses [9]. Central or visceral adipose tissue depots release adipokines such as tumor necrosis factor alpha (TNF-α) and interleukin-6 (IL-6) from adipose tissue macrophages and other immune cells that promote cell-to-cell signaling of local and systemic inflammation [10]. For pregnancy success, the maternal-fetal interface undergoes significant changes with trophoblast invasion and remodeling of decidual vasculature [11]. In pregnancies affected by obesity, it is hypothesized that cross-talk between maternal adipose tissue and the maternal-fetal interface may contribute to improper vascularization of the placenta due to high circulating proinflammatory immune cells [11,12]. The release of proinflammatory cytokines (TNF-α and IL-6) and other anti-angiogenic factors from both the adipose tissue and ischemic placenta can result in maternal hypertension and fetal growth restriction [12].
3. Maternal Obesity and Metabolic Abnormalities
Often women with obesity demonstrate metabolic abnormalities such as increased circulating leptin, glucose, insulin, and cholesterol, that play a cumulative and vital role in the development of PE [13]. Leptin is a pleiotropic hormone that is involved in energy homeostasis by regulating satiety in the brain, temperature regulation, and glucose metabolism [14]. Leptin levels increase normally with eating; however, levels increase beyond a normal range in obesity [15]. Additionally, leptin is a cytokine with both innate and adaptive immune responses that specifically promote inflammatory conditions [16]. Hyperleptinemia in people with obesity has been associated with a low-grade inflammatory state that is responsible for the development of autoimmune disease as well as reproductive and gestational disorders [15,16]. The two main sources of leptin during pregnancy are the adipose tissue and the placenta [15]. In normal pregnancy, leptin regulates vascular function and systemic inflammatory responses that impact placentation [15].
Cholesterol is also thought to contribute to pregnancy outcomes [7]. Circulating cholesterol is derived from two sources: dietary intake or cellular biosynthesis. Cellular cholesterol biosynthesis and cholesterol homeostasis is maintained primarily by the liver [17], but cholesterol is also stored in adipose tissue [18]. Recent studies suggest that adipose tissue serves as a major storage site for free cholesterol and an increase in cholesterol accumulation parallels obesity [18]. In an obese state, approximately 50% of the body’s cholesterol is stored in adipose tissue [18]. Cholesterol serves two important functions: a structural role providing cellular support at the level of the plasma membrane and a functional role with cell signaling [19]. The ratio of cholesterol carrying molecules, low density lipoproteins (LDLs), and high-density lipoproteins (HDLs) are also important in the atherogenic process. Increased levels of LDLs, molecules that transport cholesterol from the liver to peripheral tissue, can lead to plaque build-up, atherosclerotic disease, and downstream systemic inflammation [20]. Cholesterol has also been shown to cause an increase in adipose tissue inflammation and adipose tissue remodeling [18].
During pregnancy, an increase in maternal cholesterol, which is often termed maternal physiological hypercholesterolemia (MPH), is a normal physiological adaptation to ensure proper fetal development [21]. However, higher than normal cholesterol during pregnancy, termed maternal supraphysiological hypercholesterolemia (MSPH), is associated with endothelial dysfunction and atherosclerotic lesions in the placental vasculature [22]. Normal endothelial and macrophage function are reliant on the proportion of HDLs and LDLs for differentiation [21]. Macrophages adopt pro- or anti- inflammatory functions depending on the ratio between HDLs and LDLs; higher circulating levels of LDLs and lower levels of HDLs are reflective of processes promoting atherogenesis [21]. Taken together, maternal adiposity and dyslipidemia may play a causal role in PE.
4. Mechanistic Insights from Human Pregnancy Studies
In the past 20 years, several clinical studies supporting the maternal dyslipidemia and obesity hypotheses of PE have been published [12,23,24,25,26,27,28]. Specifically, an abnormal lipid profile in pregnancy has shown to be positively correlated with the development of maternal atherosclerosis and endothelial dysfunction [23]. Moreover, elevated levels of triglycerides, total cholesterol, and LDL cholesterol paired with low levels of HDL are characteristic of PE pregnancies [25]. Table 1 summarizes compiled data from cross-sectional studies as well as meta-analysis from human studies to further explain the contribution of an abnormal lipid profile in the development of pregnancy disorders such as PE. Studies in Table 1 compare serum lipid measurements in women with PE to control women with healthy pregnancies throughout different stages of gestation (1st, 2nd, and 3rd trimesters). These studies report the correlation between elevated serum lipid levels to the development and risk of PE. Additionally, some studies test the effectiveness of nutrient treatments in reversing the adverse outcomes associated with PE.
5. Mechanistic Insights from Animal Models of PE
In vitro studies that investigate the intersection of maternal obesity and circulating lipids on placental development are lacking. Advancements in technology will one day provide model systems such as organoids to study PE [29]; however, the technology has not yet been developed to uncover the mechanistic complexities of PE. Thus, animal models serve as a potential way to test hypotheses that may prevent the adverse outcomes seen in PE, and results can be used to translationally improve PE outcomes seen in high-risk pregnant women with obesity. The Blood Pressure High (BPH)/5 mouse model serves as a preclinical model for PE studies. The BPH/5 female mouse has pre-existing hypertension that increases spontaneously in pregnancy and other adverse outcomes of PE observed in human pregnancy such as proteinuria, endothelial dysfunction, and fetal growth restriction [8]. Compared to controls, pregnant BPH/5 female mice are hyperphagic with increased white adipose tissue (WAT) mass [8] that overexpresses proinflammatory cytokines (TNF- α and IL-6). They are also dyslipidemic with increased circulating cholesterol and leptin [30].
The reduced uteroplacental perfusion pressure (RUPP) rat displays PE associated signs/symptoms such as hypertensive oxidative stress, endothelial dysfunction, and fetal growth restriction [31]. Feeding the RUPP rat a high cholesterol diet beginning in early gestation results in a severe model of PE with signs of maternal neurological disturbances [32]. The high cholesterol diet results in elevated levels of cholesterol that increase oxidative stress and thus impair normal endothelial and vascular functioning specifically in the brain [32,33].
Studies in pregnant rodents have elegantly demonstrated the relationship between leptin and other atherogenic factors that are thought to promote inflammation, ischemia, and endothelial dysfunction, all of which are key features of PE [34]. The subcutaneous administration of leptin to pregnant rats resulted in adverse outcomes such as increased blood pressure, dyslipidemia, endothelial cell dysfunction, and overall increased markers of systemic inflammation [34].
Likewise, the lectin-like oxidized low-density-lipoprotein receptor-2 (LOX1) overexpressing mouse is a model of vascular dysfunction as increased LOX1 induces angiotensin activation and leads to PE associated outcomes [35]. LOX1 has been associated with the development of hypertension, insulin resistance, hyperlipidemia and complications associated with obesity [36].
Research studies have also used mouse models to demonstrate the importance of heme-oxygenase 1 (HO-1), an enzyme expressed in the placenta [37]. HO-1 has protective functions in the placenta and contributes to the maintenance of proper maternal vascularization [37]. Human patients with pregnancy disorders have commonly showed a down-regulation of HO-1 expression in their placentas; thus, lower than normal levels of HO-1 has been correlated to the development of pregnancy disorders such as PE [37]. Breeding mice heterozygous for HO-1 (HO-1+/−) resulted in decreased litter sizes and pup weights compared to wild type (WT) breeding [37]. Animal models such as BPH/5 mice, the RUPP rat, and HO-1 transgenic mice among others serve as a practical preclinical system to test improvements that could potentially mitigate adverse outcomes seen in women who are at high risk for developing PE.
6. Insights from Pharmacological and Lifestyle Interventions in Pregnant Women and Rodents
The American College of Obstetricians and Gynecologists suggests that women who are high risk for developing PE (extensive family history of PE, advanced maternal age, or pre-existing medical conditions such as obesity, diabetes, or renal dysfunction) take a low dose of aspirin (81 mg/d) starting after 12 weeks of gestation [38]. Aspirin acts to normalize angiogenic imbalance by normalizing elevated circulating sFLT1 in a preeclamptic placenta [39]. Human studies have shown that low-dose aspirin (81 mg/day) given from six to 36 weeks of gestation did not significantly increase the risk of emergency medical visits or potential side effects such as nausea, vomiting, rash, vaginal bleeding, diarrhea, or others [40,41,42].
Additionally, celecoxib, a COX-2 inhibitor, has also been shown to restore angiogenic imbalance in the placenta in addition to attenuating maternal hypertension and intrauterine fetal growth restriction in the BPH/5 mouse model [43]. It has been shown that the elevated levels of COX-2 at implantation contribute to factors that can negatively impact decidualization and placentation; however, levels of angiogenic factors are normalized after celecoxib administration [43]. Reports of human studies have shown that high doses of celecoxib administered late in gestation can have adverse fetal effects such as premature closure of the ductus arteriosus [44]. However, some studies have begun to show that administration in pregnancy can impede preterm labor without having detrimental effects on the fetus [45].
Other pharmacological interventions such as the use of statins have shown the potential to improve and counteract the PE phenotype [46]. Statin administered between 12–16 weeks of pregnancy and continued until delivery stimulates trophoblast invasion, improves placental blood flow, and provokes anti-inflammatory agents, which all work to diminish the adverse effects associated with PE [46]. Although there has been promising data on the use of statins in pregnancy, few human studies have successfully shown that statin administration is safe in pregnancy [47,48]. Statin is most commonly deemed as teratogenic and hence contraindicated in pregnancy due to increased risk of congenital abnormalities as well as other complications [49].
Tadalafil, a long-acting phosphodiesterase 5 (PDE5) inhibitor, is another pharmacotherapy under evaluation for the attenuation of PE [50]. In the RUPP model of PE, Tadalafil successfully improved maternal hypertension and attenuated the PE phenotype [50]. Human studies have shown that tadalafil has not adversely affected cardiac function in pregnant women [51]; however, few studies have reported the safety profile for both mother and fetus [52]. Sildenafil citrate, a similar inhibitor, has been investigated in a rodent model for its ability to improve blood flow in the uterine artery and for its vasodilatory effects [53]. Limited studies have shown that sildenafil does not contribute to adverse maternal or fetal side effects [54]. More studies are needed to prove the safety of tadalafil and sildenafil administration in pregnancy.
Unfavorable pregnancy outcomes seen with pharmacological therapy have emphasized the need for lifestyle intervention to attenuate maternal adipose tissue and abnormal maternal metabolic health. Published studies have demonstrated the positive effects of lifestyle interventions, specifically adipose tissue reduction by reduced food intake or increased activity, in pregnancy for both animal models and women.
In the female, hyperphagic BPH/5 mouse, pair feeding to lean control mice (equivalent to 25% calorie restriction) reduced white adipose tissue mass around the reproductive organs [30]. Pair feeding also decreased circulating leptin and WAT-derived inflammatory cytokines, but had no effect on serum cholesterol [30]. Molecular analyses showed pair feeding BPH/5 in early pregnancy decreased prostaglandin synthase 2, the enzyme responsible for prostaglandin formation, in the reproductive WAT and the implantation sites [30]. These molecular results preceded adverse late gestational PE outcomes in BPH/5, i.e., maternal increases in blood pressure. Another study using a mouse model of enriched environment that induced weight loss, displayed the beneficial metabolic improvements with attenuation of maternal obesity in both the pregnant dam and offspring [55]. For example, maternal wight loss in pregnant female mice improved glucose tolerance and insulin sensitivity as well as decreasing adipose tissue [55]. Similarly, offspring whose mothers had undergone maternal weight loss demonstrated similar metabolic improvements as well as a down-regulation of numerous lipid and cholesterol biosynthesis genes [55].
In human pregnancy, gestational weight loss resulted in a decreased incidence of PE, non-elective cesarean, preterm delivery, small/large gestational birth weight, and perinatal mortality [56]. Together, these studies in both animal and human models demonstrate the potential beneficial effects of maternal weight loss and adipose tissue reduction on PE and its associated adverse pregnancy outcomes.
7. Conclusions
PE is a disorder of pregnancy characterized by maternal hypertension and fetal growth restriction [3]. PE is thought to be caused by improper placental vascularization and subsequent increased systemic inflammation as the maternal signs of PE resolve after delivery of the placenta [3]. PE continues to be a leading cause of maternal and fetal morbidity and mortality with limited knowledge regarding the prevention and attenuation of onset or worsening of symptoms [1]. Inflammatory adipokines and cytokines from maternal adipose tissue and circulating cholesterol have been linked to the development of systemic inflammation, pregnancy-induced hypertension, an imbalance of placental angiogenic factors, and other adverse PE outcomes [10,20,43]. Therefore, the reduction of adipose tissue and associated adipokines is hypothesized to be associated with adequate placental angiogenesis and the overall improvement of adverse outcomes associated with PE by altering inflammatory responses [30]. Additionally adipose tissue serves as a major reservoir for free cholesterol [18]. Supraphysiological levels of cholesterol in pregnancy are hypothesized to contribute to the improper vascularization of the placenta and overall systemic inflammation seen with PE [22]. Rodent studies have shown that increased dietary cholesterol leads to an increased accumulation of differentiated pro-inflammatory adipose tissue macrophages [7]. In summary, the adipose tissue plays an important role in pregnancy. Increased maternal adipose tissue mass and cholesterol promote metabolic abnormalities and systemic inflammation, which may contribute to improper placental vascularization that leads to PE with increased maternal blood pressure and fetal growth restriction (Figure 1). Future studies are needed to further elucidate the contribution of pharmacotherapy as well as lifestyle interventions, specifically maternal weight loss, and PE outcomes in high-risk women with obesity.
Author Contributions
Writing—original draft preparation, M.C.A.; writing—review and editing, M.C.A., L.M.R., J.L.S.; funding acquisition, J.L.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the NIH: P20GM135002 to JLS and 5R01DK124806, 5R01NR017644, P30DK072476.
Acknowledgments
Figure assistance using BioRender courtesy of Nataki Douglas.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Huda, S.S.; Jordan, F.; Bray, J.; Love, G.; Payne, R.; Sattar, N.; Freeman, D.J. Visceral adipose tissue activated macrophage content and inflammatory adipokine secretion is higher in pre-eclampsia than in healthy pregnancys. Clin. Sci. 2017, 131, 1529–1540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rana, S.; Lemoine, E.; Granger, J.P.; Karumanchi, S.A. Preeclampsia: Pathophysiology, challenges, and perspectives. Circ. Res. 2019, 124, 1094–1112. [Google Scholar] [CrossRef] [PubMed]
- Portelli, M.; Baron, B. Clinical presentation of preeclampsia and the diagnostic value of proteins and their methylation products as biomarkers in pregnant women with preeclampsia and their newborns. J. Pregnancy 2018, 2018, 2632637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grill, S.; Rusterholz, C.; Zanetti-Dällenbach, R.; Tercanli, S.; Holzgreve, W.; Hahn, S.; Lapaire, O. Potential markers of preeclampsia–a review. Reprod. Biol. Endocrinol. 2009, 7, 70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herraiz, I.; Llurba, E.; Verlohren, S.; Galindo, A.; Spanish Group for the Study of Angiogenic Markers in Preeclampsia. Update on the Diagnosis and Prognosis of Preeclampsia with the Aid of the SFlt-1/ PlGF Ratio in Singleton Pregnancies. Fetal Diagn. Ther. 2018, 43, 81–89. [Google Scholar] [CrossRef] [Green Version]
- Caballero, B. Humans against Obesity: Who Will Win? Adv. Nutr. 2019, 10 (Suppl. 1), S4–S9. [Google Scholar] [CrossRef]
- Subramanian, S.; Han, C.Y.; Chiba, T.; McMillen, T.S.; Wang, S.A.; Haw, A.; Kirk, E.A.; O’Brien, K.D.; Chait, A. Dietary Cholesterol worsens adipose tissue macrophage accumulation and atherosclerosis in obese LDL receptor–deficient mice. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 685–691. [Google Scholar] [CrossRef]
- Sutton, E.F.; Lob, H.E.; Song, J.; Xia, Y.; Butler, S.; Liu, C.-C.; Redman, L.M.; Sones, J.L. Adverse metabolic phenotype of female offspring exposed to preeclampsia in utero: A characterization of the BPH/5 mouse in postnatal life. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2017, 312, R485–R491. [Google Scholar] [CrossRef]
- Naruse, K.; Akasaka, J.; Shigemitsu, A.; Tsunemi, T.; Koike, N.; Yoshimoto, C.; Kobayashi, H. Involvement of Visceral Adipose Tissue in Immunological Modulation of Inflammatory Cascade in Preeclampsia. Mediat. Inflamm. 2015, 2015, 325932. [Google Scholar] [CrossRef]
- Denison, F.C.; Roberts, K.A.; Barr, S.M.; Norman, J.E. Obesity, pregnancy, inflammation, and vascular function. Reproduction 2010, 140, 373–385. [Google Scholar] [CrossRef]
- Lash, G.E. Molecular Cross-Talk at the Feto-Maternal Interface. Cold Spring Harb. Perspect. Med. 2015, 5, a023010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spradley, F.T.; Palei, A.C.; Granger, J.P. Immune Mechanisms Linking Obesity and Preeclampsia. Biomolecules 2015, 5, 3142–3176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spradley, F.T. Metabolic abnormalities and obesity’s impact on the risk for developing preeclampsia. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2017, 312, R5–R12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Münzberg, H.; Morrison, C.D. Structure, production and signaling of leptin. Metabolism 2015, 64, 13–23. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Pérez, A.; Toro, A.; Vilariño-García, T.; Maymó, J.; Guadix, P.; Dueñas, J.L.; Fernández-Sánchez, M.; Varone, C.; Sánchez-Margalet, V. Leptin action in normal and pathological pregnancies. J. Cell. Mol. Med. 2018, 22, 716–727. [Google Scholar] [CrossRef]
- La Cava, A. leptin in inflammation and autoimmunity. Cytokine 2017, 98, 51–58. [Google Scholar] [CrossRef]
- Trapani, L.; Segatto, M.; Pallottini, V. Regulation and deregulation of cholesterol homeostasis: The liver as a metabolic “power station”. World J. Hepatol. 2012, 4, 184–190. [Google Scholar] [CrossRef]
- Chung, S.; Parks, J.S. Dietary cholesterol effects on adipose tissue inflammation. Curr. Opin. Lipidol. 2016, 27, 19–25. [Google Scholar] [CrossRef] [Green Version]
- Craig, M.; Yarrarapu, S.N.S.; Dimri, M. Biochemistry, Cholesterol. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Tall, A.R.; Yvan-Charvet, L. Cholesterol, Inflammation and Innate Immunity. Nat. Rev. Immunol. 2015, 15, 104–116. [Google Scholar] [CrossRef] [Green Version]
- Cantin, C.; Arenas, G.; San Martin, S.; Leiva, A. Effects of lipoproteins on endothelial cells and macrophages function and its possible implications on fetal adverse outcomes associated to maternal hypercholesterolemia during pregnancy. Placenta 2021, 106, 79–87. [Google Scholar] [CrossRef]
- Cantin, C.; Fuenzalida, B.; Leiva, A. Maternal hypercholesterolemia during pregnancy: Potential modulation of cholesterol transport through the human placenta and lipoprotein profile in maternal and neonatal circulation. Placenta 2020, 94, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Manten, G.T.R.; van der Hoek, Y.Y.; Marko Sikkema, J.; Voorbij, H.A.M.; Hameeteman, T.M.; Visser, G.H.A.; Franx, A. The role of lipoprotein (a) in pregnancies complicated by pre-eclampsia. Med. Hypotheses 2005, 64, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Contini, C.; Jansen, M.; König, B.; Markfeld-Erol, F.; Kunze, M.; Zschiedrich, S.; Massing, U.; Merfort, I.; Prömpeler, H.; Pecks, U.; et al. Lipoprotein turnover and possible remnant accumulation in preeclampsia: Insights from the Freiburg Preeclampsia H.E.L.P.-Apheresis Study. Lipids Health Dis. 2018, 17, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spracklen, C.N.; Smith, C.J.; Saftlas, A.F.; Robinson, J.G.; Ryckman, K.K. Maternal Hyperlipidemia and the Risk of Preeclampsia: A Meta-Analysis. Am. J. Epidemiol. 2014, 180, 346–358. [Google Scholar] [CrossRef] [Green Version]
- Pawłowicz, P.; Wilczyński, J.; Stachowiak, G.; Hincz, P. Administration of natural anthocyanins derived from chokeberry retardation of idiopathic and preeclamptic origin. Influence on metabolism of plasma oxidized lipoproteins: The role of autoantibodies to oxidized low density lipoproteins. Ginekol. Pol. 2000, 71, 848–853. [Google Scholar]
- Ziaei, S.; Hantoshzadeh, S.; Rezasoltani, P.; Lamyian, M. The effect of garlic tablet on plasma lipids and platelet aggregation in nulliparous pregnants at high risk of preeclampsia. Eur. J. Obstet. Gynecol. Reprod. Biol. 2001, 99, 201–206. [Google Scholar] [CrossRef]
- Williams, M.A.; Woelk, G.B.; King, I.B.; Jenkins, L.; Mahomed, K. Plasma Carotenoids, Retinol, Tocopherols, and Lipoproteins in Preeclamptic and Normotensive Pregnant Zimbabwean Women. Am. J. Hypertens. 2003, 16, 665–672. [Google Scholar] [CrossRef] [Green Version]
- Haider, S.; Meinhardt, G.; Saleh, L.; Kunihs, V.; Gamperl, M.; Kaindl, U.; Ellinger, A.; Burkard, T.R.; Fiala, C.; Pollheimer, J.; et al. Self-Renewing Trophoblast Organoids Recapitulate the Developmental Program of the Early Human Placenta. Stem Cell Rep. 2018, 1, 537–551. [Google Scholar] [CrossRef] [Green Version]
- Reijnders, D.; Olson, K.N.; Liu, C.-C.; Beckers, K.F.; Ghosh, S.; Redman, L.M.; Sones, J.L. Dyslipidemia and the role of adipose tissue in early pregnancy in the bph/5 mouse model for preeclampsia. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2019, 317, R49–R58. [Google Scholar] [CrossRef]
- Crews, J.K.; Herrington, J.N.; Granger, J.P.; Khalil, R.A. Decreased Endothelium-Dependent Vascular Relaxation during Reduction of Uterine Perfusion Pressure in Pregnant Rat. Hypertension 2000, 35 Pt 2, 367–372. [Google Scholar] [CrossRef] [Green Version]
- Johnson, A.C.; Tremble, S.M.; Chan, S.-L.; Moseley, J.; LaMarca, B.; Nagle, K.J.; Cipolla, M.J. Magnesium Sulfate Treatment Reverses Seizure Susceptibility and Decreases Neuroinflammation in a Rat Model of Severe Preeclampsia. PLoS ONE 2014, 9, e113670. [Google Scholar] [CrossRef] [PubMed]
- Schreurs, M.P.H.; Cipolla, M.J. Pregnancy Enhances the Effects of Hypercholesterolemia on Posterior Cerebral Arteries. Reprod. Sci. 2013, 20, 391–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polyakova, E.A.; Mikhaylov, E.N.; Galagudza, M.M.; Shlyakhto, E.V. Hyperleptinemia results in systemic inflammation and the exacerbation of ischemia-reperfusion myocardial injury. Heliyon 2021, 7, e08491. [Google Scholar] [CrossRef]
- Sáez, T.; Spaans, F.; Kirschenman, R.; Sawamura, T.; Davidge, S.T. High-Cholesterol Diet during Pregnancy Induces Maternal Vascular Dysfunction in Mice: Potential Role for Oxidized LDL-Induced LOX-1 and AT1 Receptor Activation. Clin. Sci. (Lond.) 2020, 134, 2295–2313. [Google Scholar] [CrossRef]
- Yan, M.; Mehta, J.L.; Hu, C. LOX-1 and Obesity. Cardiovasc. Drugs Ther. 2011, 25, 469–476. [Google Scholar] [CrossRef]
- Zhao, H.; Wong, R.J.; Kalish, F.S.; Nayak, N.R.; Stevenson, D.K. Effect of Heme Oxygenase-1 Deficiency on Placental Development. Placenta 2009, 30, 861–868. [Google Scholar] [CrossRef] [Green Version]
- ACOG Committee Opinion No. 743: Low-Dose Aspirin Use During Pregnancy. Obstet. Gynecol. 2018, 132, e44–e52. [CrossRef]
- Li, C.; Raikwar, N.S.; Santillan, M.K.; Santillan, D.A.; Thomas, C.P. Aspirin inhibits expression of sflt1 from human cytotrophoblasts induced by hypoxia, via cyclo-oxygenase 1. Placenta 2015, 36, 446–453. [Google Scholar] [CrossRef] [Green Version]
- Short, V.L.; Hoffman, M.; Metgud, M.; Kavi, A.; Goudar, S.S.; Okitawutshu, J.; Tshefu, A.; Bose, C.L.; Mwenechanya, M.; Chomba, E.; et al. Safety of daily low-dose aspirin use during pregnancy in low-income and middle-income countries. AJOG Glob. Rep. 2021, 1, 100003. [Google Scholar] [CrossRef]
- He, G.; Chen, Y.; Chen, M.; He, G.; Liu, X. Efficacy and Safety of Low Dose Aspirin and Magnesium Sulfate in the Treatment of Pregnancy Induced Hypertension: A Protocol for Systematic Review and Meta-Analysis. Medicine 2020, 99, e22801. [Google Scholar] [CrossRef]
- Rolnik, D.L.; Nicolaides, K.H.; Poon, L.C. Prevention of preeclampsia with aspirin. Am. J. Obstet. Gynecol. 2022, 226, S1108–S1119. [Google Scholar] [CrossRef]
- Reijnders, D.; Liu, C.-C.; Xu, X.; Zhao, A.M.; Olson, K.N.; Butler, S.D.; Douglas, N.C.; Sones, J.L. Celecoxib Restores Angiogenic Factor Expression at the Maternal-Fetal Interface in the BPH/5 Mouse Model of Preeclampsia. Physiol. Genom. 2018, 50, 385–392. [Google Scholar] [CrossRef]
- Risser, A.; Donovan, D.; Heintzman, J.; Page, T. NSAID Prescribing Precautions. Am. Fam. Physician 2009, 80, 1371–1378. [Google Scholar] [PubMed]
- Ohtsuki, M.; Chigusa, Y.; Mogami, H.; Ueda, A.; Kawasaki, K.; Yamaguchi, K.; Mandai, M.; Kondoh, E. The Effect of celecoxib for treatment of preterm labor on fetuses during the second trimester of pregnancy: A Pilot Case Series. Taiwan J. Obstet. Gynecol. 2022, 61, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Ma’ayeh, M.; Rood, K.M.; Kniss, D.; Costantine, M.M. Novel Interventions for the Prevention of Preeclampsia. Curr. Hypertens. Rep. 2020, 22, 17. [Google Scholar] [CrossRef] [PubMed]
- Costantine, M.M.; Ananth, C.V. The early developments of preeclampsia drugs. Expert Opin. Investig. Drugs 2016, 25, 867–870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lefkou, E.; Mamopoulos, A.; Fragakis, N.; Dagklis, T.; Vosnakis, C.; Nounopoulos, E.; Rousso, D.; Girardi, G. Clinical Improvement and Successful Pregnancy in a Preeclamptic Patient with Antiphospholipid Syndrome Treated with Pravastatin. Hypertension 2014, 63, e118–e119. [Google Scholar] [CrossRef] [Green Version]
- Karalis, D.G.; Hill, A.N.; Clifton, S.; Wild, R.A. The Risks of Statin Use in Pregnancy: A Systematic Review. J. Clin. Lipidol. 2016, 10, 1081–1090. [Google Scholar] [CrossRef]
- Sekimoto, A.; Tanaka, K.; Hashizume, Y.; Sato, E.; Sato, H.; Ikeda, T.; Takahashi, N. Tadalafil alleviates preeclampsia and fetal growth restriction in RUPP model of preeclampsia in mice. Biochem. Biophys. Res. Commun. 2020, 521, 769–774. [Google Scholar] [CrossRef]
- Tanaka, K.; Tanaka, H.; Maki, S.; Kubo, M.; Nii, M.; Magawa, S.; Hatano, F.; Tsuji, M.; Osato, K.; Kamimoto, Y.; et al. Cardiac function and tadalafil used for treating fetal growth restriction in pregnant women without cardiovascular disease. J. Matern. Fetal Neonatal Med. 2019, 32, 2460–2462. [Google Scholar] [CrossRef]
- Kubo, M.; Tanaka, H.; Maki, S.; Nii, M.; Murabayashi, N.; Osato, K.; Kamimoto, Y.; Umekawa, T.; Kondo, E.; Ikeda, T. Safety and Dose-Finding Trial of Tadalafil Administered for Fetal Growth Restriction: A Phase-1 Clinical Study. J. Obstet. Gynaecol. Res. 2017, 43, 1159–1168. [Google Scholar] [CrossRef] [PubMed]
- Herraiz, S.; Pellicer, B.; Serra, V.; Cauli, O.; Cortijo, J.; Felipo, V.; Pellicer, A. Sildenafil citrate improves perinatal outcome in fetuses from pre-eclamptic rats. BJOG Int. J. Obstet. Gynaecol. 2012, 119, 1394–1402. [Google Scholar] [CrossRef] [Green Version]
- Dunn, L.; Greer, R.; Flenady, V.; Kumar, S. Sildenafil in Pregnancy: A Systematic Review of Maternal Tolerance and Obstetric and Perinatal Outcomes. Fetal Diagn. Ther. 2017, 41, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Wei, Y.; Yang, C.-R.; Wei, Y.-P.; Ge, Z.-J.; Zhao, Z.-A.; Zhang, B.; Hou, Y.; Schatten, H.; Sun, Q.-Y. Enriched Environment-Induced Maternal Weight Loss Reprograms Metabolic Gene Expression in Mouse Offspring. J. Biol. Chem. 2015, 290, 4604–4619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beyerlein, A.; Schiessl, B.; Lack, N.; von Kries, R. Associations of gestational weight loss with birth-related outcome: A retrospective cohort study. BJOG Int. J. Obstet. Gynaecol. 2011, 118, 55–61. [Google Scholar] [CrossRef] [PubMed]
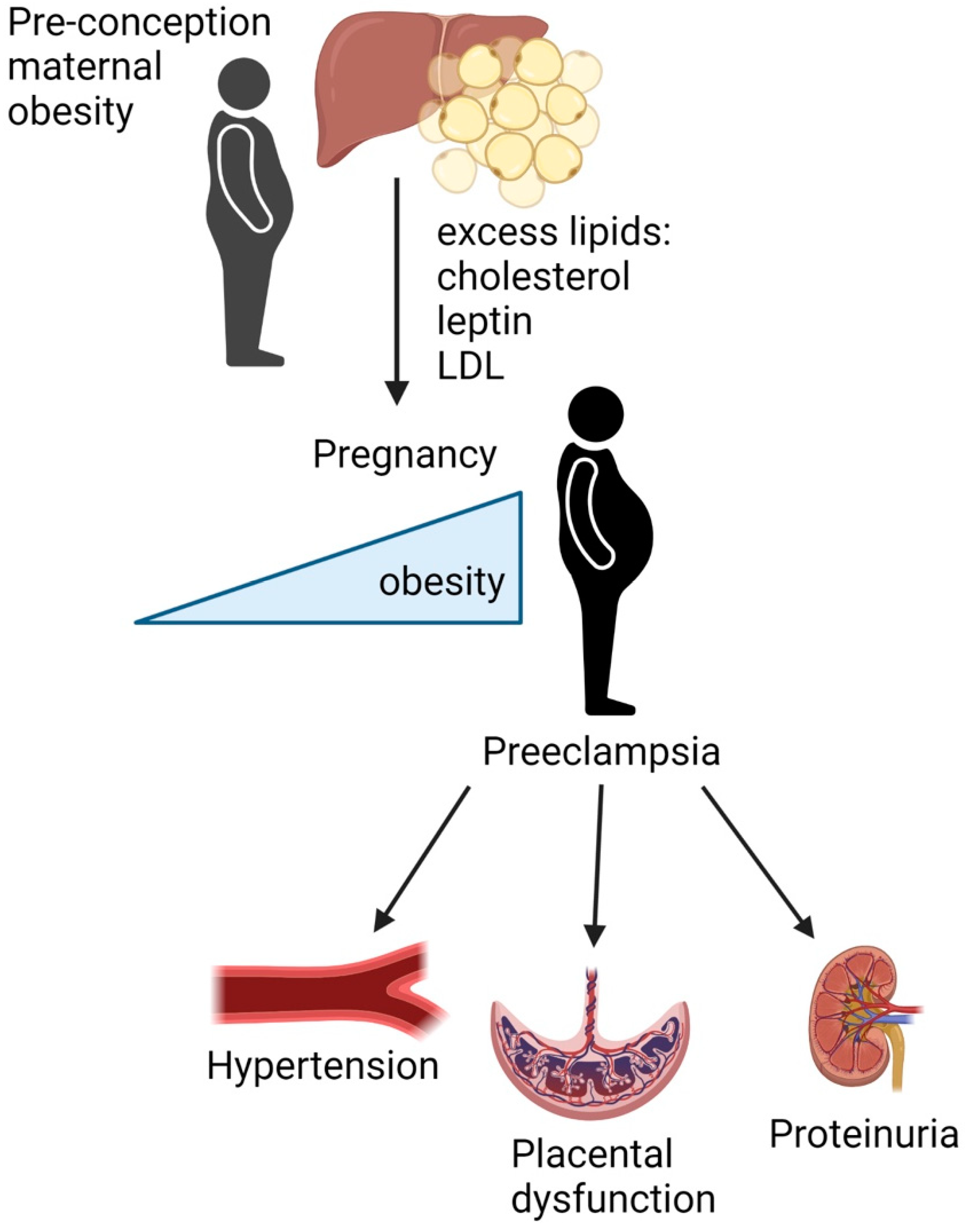
Figure 1.
Maternal obesity and dyslipidemia promotes preeclampsia through abnormal placental development. The liver oxidizes lipids and excess lipids are shunted to adipose tissue for storage. As adipocytes become hypertrophic in obesity, there is an increase in leptin, total cholesterol, as well as low-density lipoproteins (LDL) in the maternal circulation. This increase in lipid accumulation and dyslipidemia results in endothelial dysfunction and an overall increase in inflammation with increased weight gain during pregnancy, which may contribute to improper vascularization of the placenta and adverse outcomes associated with preeclampsia: elevated maternal blood pressure and fetal growth restriction. Made with BioRender.com (accessed on 11 May 2022).
Figure 1.
Maternal obesity and dyslipidemia promotes preeclampsia through abnormal placental development. The liver oxidizes lipids and excess lipids are shunted to adipose tissue for storage. As adipocytes become hypertrophic in obesity, there is an increase in leptin, total cholesterol, as well as low-density lipoproteins (LDL) in the maternal circulation. This increase in lipid accumulation and dyslipidemia results in endothelial dysfunction and an overall increase in inflammation with increased weight gain during pregnancy, which may contribute to improper vascularization of the placenta and adverse outcomes associated with preeclampsia: elevated maternal blood pressure and fetal growth restriction. Made with BioRender.com (accessed on 11 May 2022).

{kind=link}
Table 1.
Human studies providing evidence for a link between dyslipidemia and preeclampsia.
| Subjects | Gestational Age | Measures | Relationship to PE | Treatments/ Nutrients | Citation |
|---|---|---|---|---|---|
| six with early onset PE (pilot study, no control) | 24–27 weeks | Cholesterol LDL Apo B | Lipoprotein remnants = endothelial dysfunction | Apheresis (reduced ApoB) | Contini et al., 2018 [24] |
| 7369–1975 with PE and 5394 healthy (meta-analysis) | first and second trimesters third trimester | Cholesterol LDL TG Cholesterol TG HDL | Elevated in PE Elevated in PE Elevated in PE Elevated in PE Elevated in PE Low in PE | -- | Spracklen et al., 2014 [25] |
| 105 PW- 50 treatment, 55 placebo 60 healthy controls | second trimester | Oxidized low density lipoproteins (oLAB) | oLABs contribute to intrauterine growth retardation | Chokeberry Anthocyanins (controls oxidative stress) | Pawlowicz et al., 2000 [26] |
| 100 PW–50 treated, 50 placebo | third trimester | Cholesterol LDL HDL TG | -- | Garlic Tablet (reduces hypertension) | Ziaei et al., 2001 [27] |
| 173 with PE 186 healthy controls | Post-partum | HDL Triglycerides | Higher levels, decreased risk of PE Higher levels, increased risk of PE | -- | Williams et al., 2003 [28] |
Abbreviations: Preeclampsia (PE), Pregnant Women (PW), Low Density Lipoprotein (LDL), Apolipoprotein B (ApoB), High Density Lipoprotein (HDL), Triglycerides (TG).
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Alston, M.C.; Redman, L.M.; Sones, J.L. An Overview of Obesity, Cholesterol, and Systemic Inflammation in Preeclampsia. Nutrients 2022, 14, 2087. https://doi.org/10.3390/nu14102087
AMA Style
Alston MC, Redman LM, Sones JL. An Overview of Obesity, Cholesterol, and Systemic Inflammation in Preeclampsia. Nutrients. 2022; 14(10):2087. https://doi.org/10.3390/nu14102087
Chicago/Turabian StyleAlston, Morgan C., Leanne M. Redman, and Jennifer L. Sones. 2022. "An Overview of Obesity, Cholesterol, and Systemic Inflammation in Preeclampsia" Nutrients 14, no. 10: 2087. https://doi.org/10.3390/nu14102087
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.