
Short-Term Magnesium Therapy Alleviates Moderate Stress in Patients with Fibromyalgia: A Randomized Double-Blind Clinical Trial

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
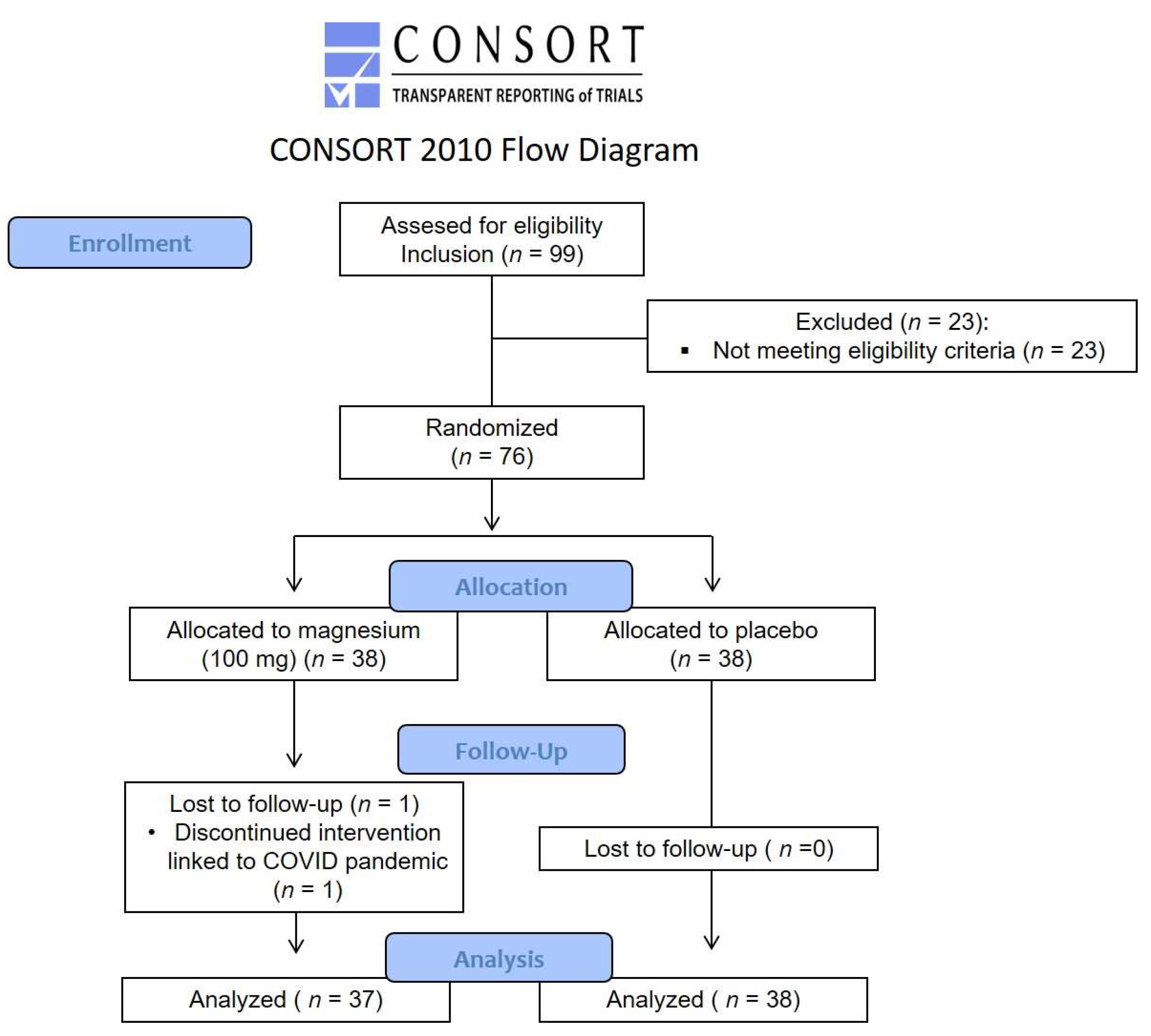
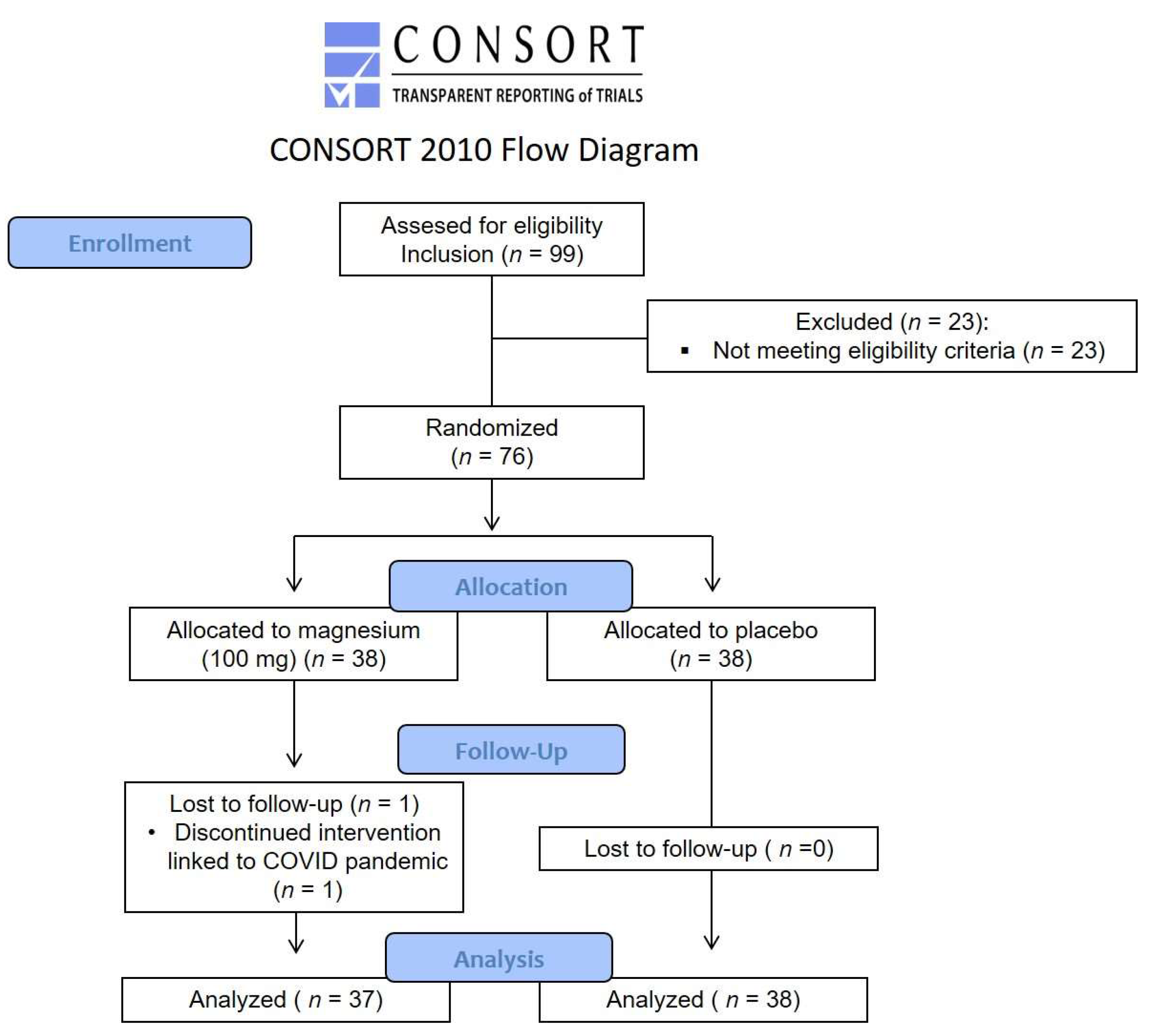
2.1. Study Design
2.2. Study Population
2.3. FM Diagnosis, Impact of FM, and Pain Status
2.4. Study Treatment
2.5. Primary Outcome
2.6. Secondary Outcomes
2.7. Statistical Methods
3. Results
3.1. Clinical Characteristics
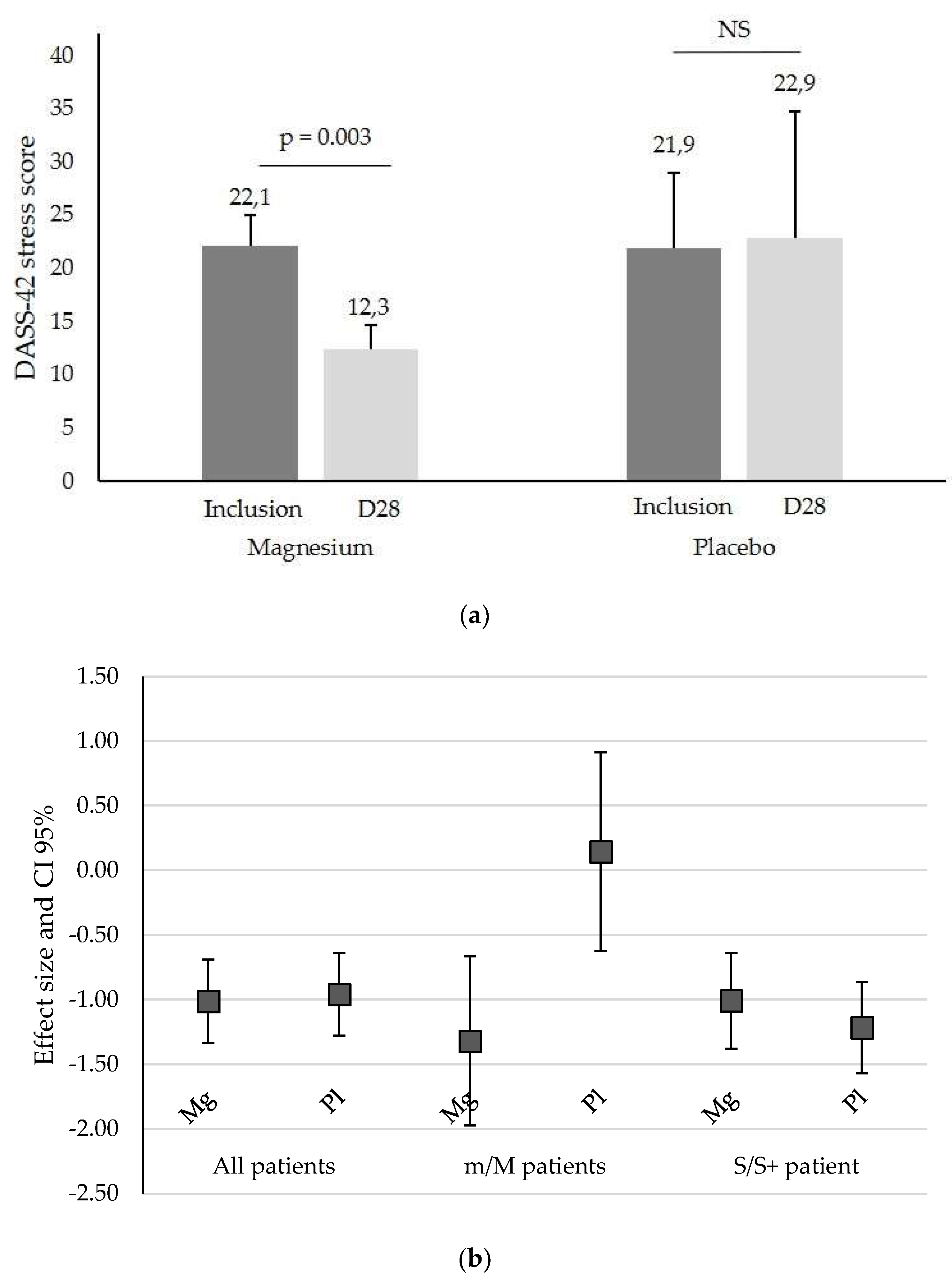
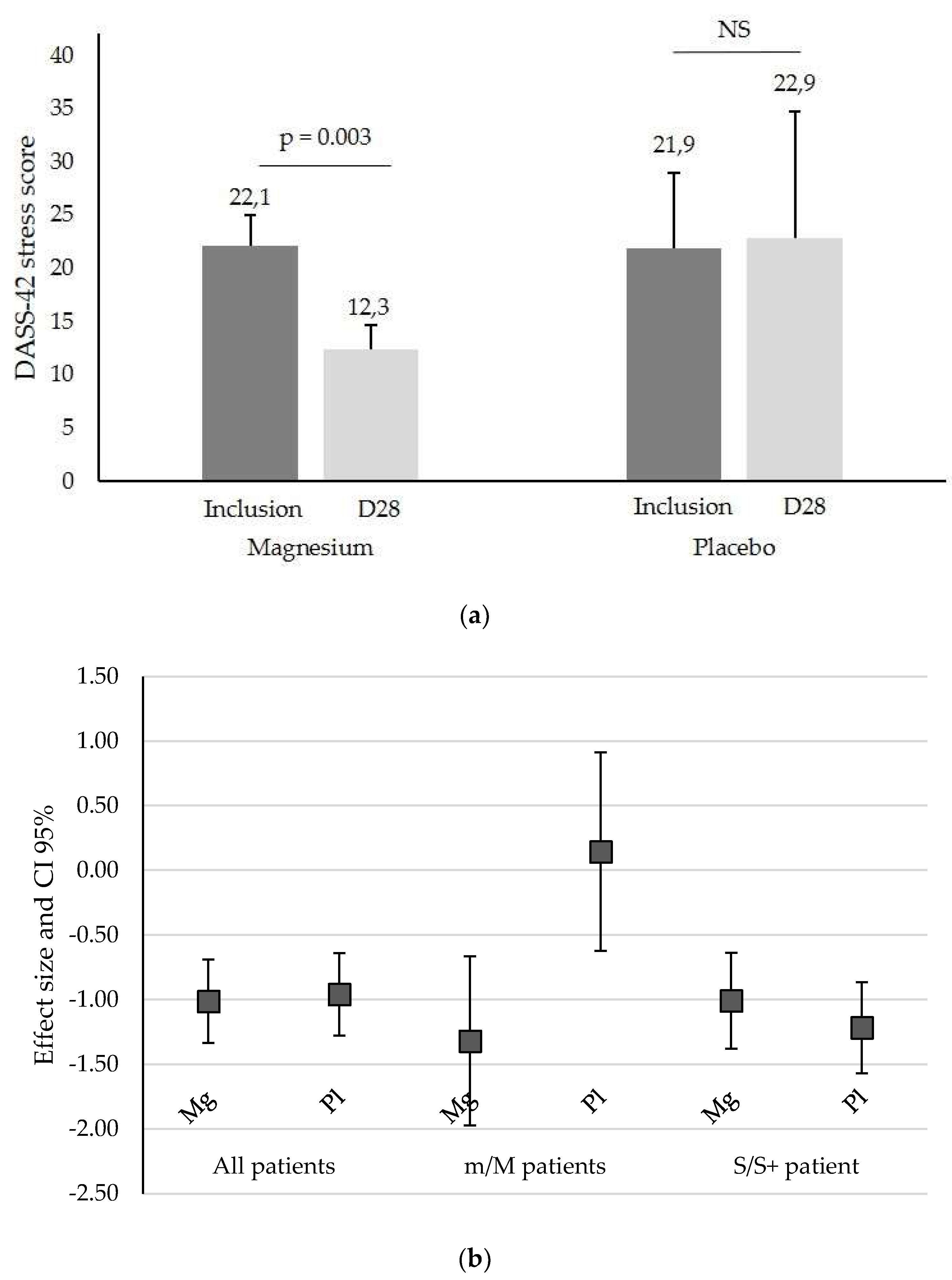
3.2. Primary Outcome Results
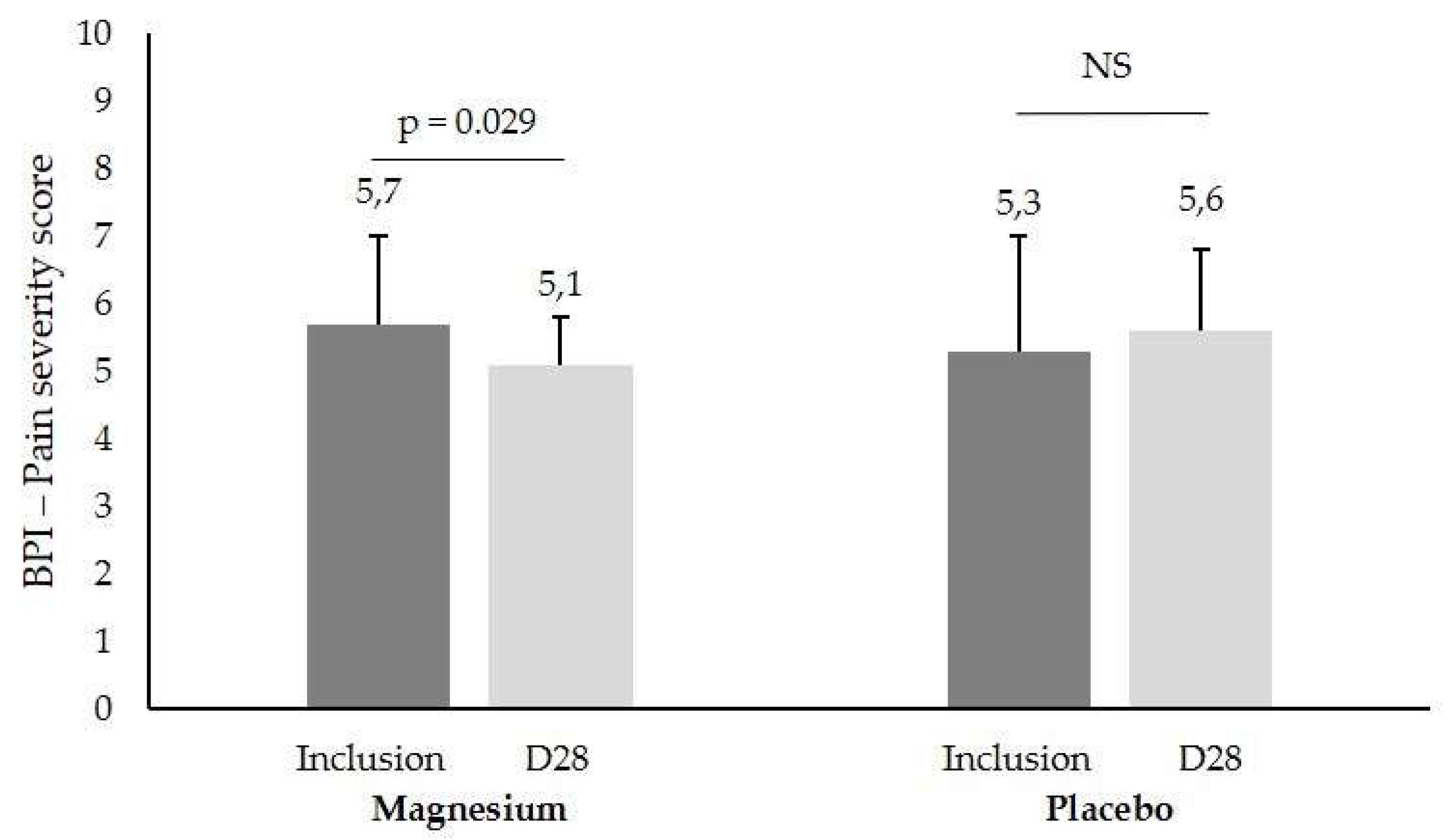
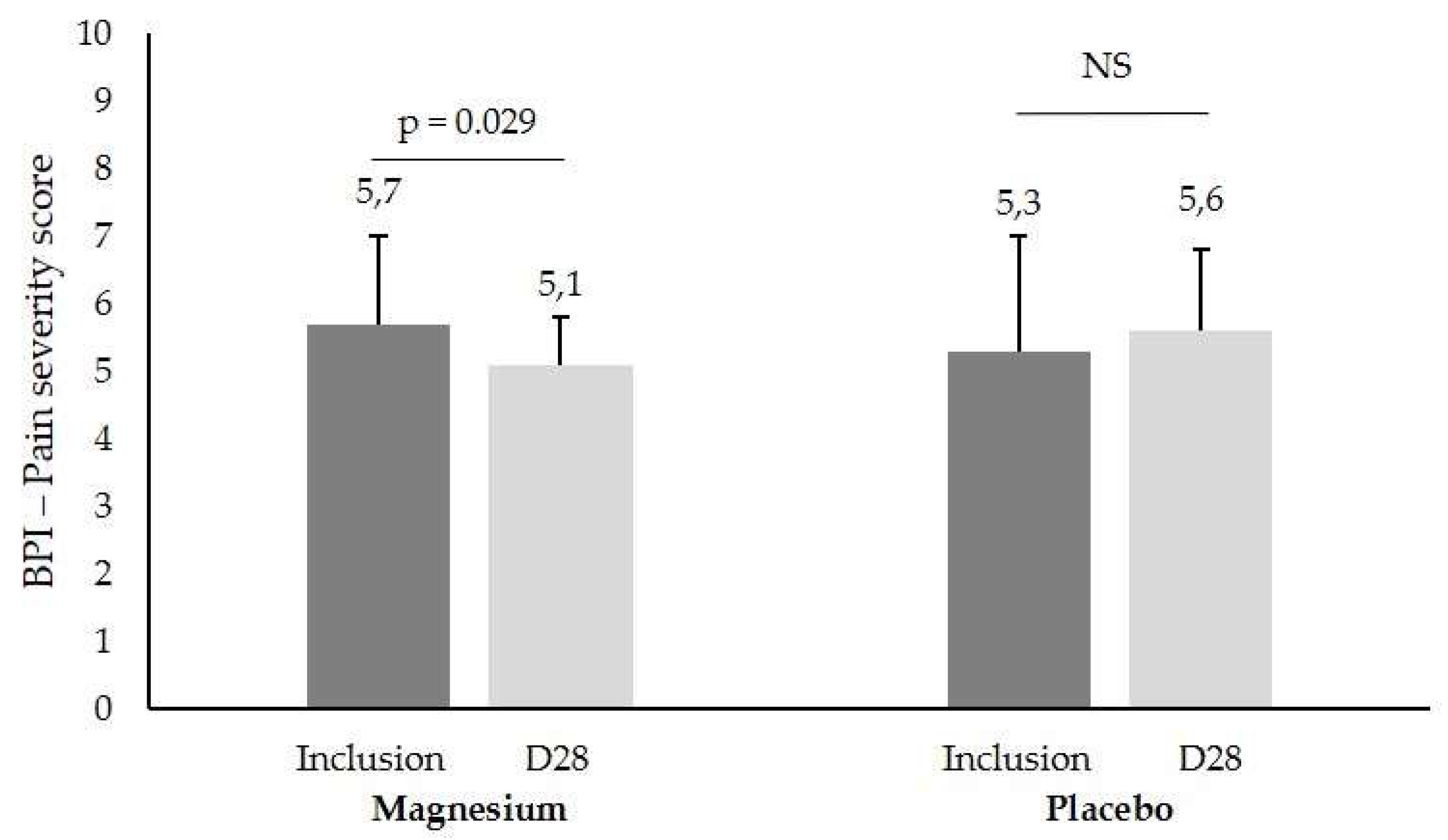
3.3. Secondary Outcomes Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Heidari, F.; Afshari, M.; Moosazadeh, M. Prevalence of Fibromyalgia in General Population and Patients, a Systematic Review and Meta-Analysis. Rheumatol. Int. 2017, 37, 1527–1539. [Google Scholar] [CrossRef] [PubMed]
- Theoharides, T.C.; Tsilioni, I.; Arbetman, L.; Panagiotidou, S.; Stewart, J.M.; Gleason, R.M.; Russell, I.J. Fibromyalgia Syndrome in Need of Effective Treatments. J. Pharmacol. Exp. Ther. 2015, 355, 255–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chinn, S.; Caldwell, W.; Gritsenko, K. Fibromyalgia Pathogenesis and Treatment Options Update. Curr. Pain Headache Rep. 2016, 20, 25. [Google Scholar] [CrossRef] [PubMed]
- Doerr, J.M.; Fischer, S.; Nater, U.M.; Strahler, J. Influence of Stress Systems and Physical Activity on Different Dimensions of Fatigue in Female Fibromyalgia Patients. J. Psychosom. Res. 2017, 93, 55–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiao, J.; Cheng, Z.; Wang, W.; Zhao, Y.; Jiang, Q. Demographic Characteristics and Clinical Features of Fibromyalgia in China: A Cross-Sectional Study. Rheumatol. Ther. 2021, 8, 817–831. [Google Scholar] [CrossRef]
- Martinez-Lavin, M. Biology and Therapy of Fibromyalgia. Stress, the Stress Response System, and Fibromyalgia. Arthritis Res. Ther. 2007, 9, 216. [Google Scholar] [CrossRef] [Green Version]
- McEwen, B.S.; Akil, H. Revisiting the Stress Concept: Implications for Affective Disorders. J. Neurosci. 2020, 40, 12–21. [Google Scholar] [CrossRef] [Green Version]
- Pickering, G.; Mazur, A.; Trousselard, M.; Bienkowski, P.; Yaltsewa, N.; Amessou, M.; Noah, L.; Pouteau, E. Magnesium Status and Stress: The Vicious Circle Concept Revisited. Nutrients 2020, 12, 3672. [Google Scholar] [CrossRef]
- Noushad, S.; Ahmed, S.; Ansari, B.; Mustafa, U.-H.; Saleem, Y.; Hazrat, H. Physiological Biomarkers of Chronic Stress: A Systematic Review. Int. J. Health Sci. 2021, 15, 46–59. [Google Scholar]
- Gupta, A.; Silman, A.J. Psychological Stress and Fibromyalgia: A Review of the Evidence Suggesting a Neuroendocrine Link. Arthritis Res. Ther. 2004, 6, 98–106. [Google Scholar] [CrossRef] [Green Version]
- Adler, G.K.; Geenen, R. Hypothalamic-Pituitary-Adrenal and Autonomic Nervous System Functioning in Fibromyalgia. Rheum. Dis. Clin. N. Am. 2005, 31, 187–202. [Google Scholar] [CrossRef] [PubMed]
- Alok, R.; Das, S.K.; Agarwal, G.G.; Salwahan, L.; Srivastava, R. Relationship of Severity of Depression, Anxiety and Stress with Severity of Fibromyalgia. Clin. Exp. Rheumatol. 2011, 29, S70–S72. [Google Scholar] [PubMed]
- Malin, K.; Littlejohn, G.O. Stress Modulates Key Psychological Processes and Characteristic Symptoms in Females with Fibromyalgia. Clin. Exp. Rheumatol. 2013, 31, S64–S71. [Google Scholar]
- Taylor, A.G.; Fischer-White, T.G.; Anderson, J.G.; Adelstein, K.E.; Murugesan, M.; Lewis, J.E.; Scott, M.M.; Gaykema, R.P.A.; Goehler, L.E. Stress, Inflammation and Pain: A Potential Role for Monocytes in Fibromyalgia-Related Symptom Severity. Stress Health J. Int. Soc. Investig. Stress 2016, 32, 503–513. [Google Scholar] [CrossRef]
- Rico-Villademoros, F.; Postigo-Martin, P.; Garcia-Leiva, J.M.; Ordoñez-Carrasco, J.L.; Calandre, E.P. Patterns of Pharmacologic and Non-Pharmacologic Treatment, Treatment Satisfaction and Perceived Tolerability in Patients with Fibromyalgia: A Patients’ Survey. Clin. Exp. Rheumatol. 2020, 38 (Suppl. S123), 72–78. [Google Scholar] [PubMed]
- Thour, A.; Marwaha, R. Amitriptyline. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Seelig, M.S. Consequences of Magnesium Deficiency on the Enhancement of Stress Reactions; Preventive and Therapeutic Implications (a Review). J. Am. Coll. Nutr. 1994, 13, 429–446. [Google Scholar] [CrossRef] [PubMed]
- Cuciureanu, M.D.; Vink, R. Magnesium and Stress. In Magnesium in the Central Nervous System; Vink, R., Nechifor, M., Eds.; University of Adelaide Press: Adelaide, AU, USA, 2011; ISBN 978-0-9870730-5-1. [Google Scholar]
- Costello, R.; Wallace, T.C.; Rosanoff, A. Magnesium. Adv. Nutr. 2016, 7, 199–201. [Google Scholar] [CrossRef]
- Pickering, G.; Morel, V.; Simen, E.; Cardot, J.-M.; Moustafa, F.; Delage, N.; Picard, P.; Eschalier, S.; Boulliau, S.; Dubray, C. Oral Magnesium Treatment in Patients with Neuropathic Pain: A Randomized Clinical Trial. Magnes. Res. 2011, 24, 28–35. [Google Scholar] [CrossRef] [Green Version]
- Bradley, L.A. Pathophysiology of Fibromyalgia. Am. J. Med. 2009, 122, S22–S30. [Google Scholar] [CrossRef] [Green Version]
- Abraham, G.E.; Flechas, J.D. Management of Fibromyalgia: Rationale for the Use of Magnesium and Malic Acid. J. Nutr. Med. 1992, 3, 49–59. [Google Scholar] [CrossRef]
- Bagis, S.; Karabiber, M.; As, I.; Tamer, L.; Erdogan, C.; Atalay, A. Is Magnesium Citrate Treatment Effective on Pain, Clinical Parameters and Functional Status in Patients with Fibromyalgia? Rheumatol. Int. 2013, 33, 167–172. [Google Scholar] [CrossRef]
- Engen, D.J.; McAllister, S.J.; Whipple, M.O.; Cha, S.S.; Dion, L.J.; Vincent, A.; Bauer, B.A.; Wahner-Roedler, D.L. Effects of Transdermal Magnesium Chloride on Quality of Life for Patients with Fibromyalgia: A Feasibility Study. J. Integr. Med. 2015, 13, 306–313. [Google Scholar] [CrossRef]
- Kim, Y.-S.; Kim, K.-M.; Lee, D.-J.; Kim, B.-T.; Park, S.-B.; Cho, D.-Y.; Suh, C.-H.; Kim, H.-A.; Park, R.-W.; Joo, N.-S. Women with Fibromyalgia Have Lower Levels of Calcium, Magnesium, Iron and Manganese in Hair Mineral Analysis. J. Korean Med. Sci. 2011, 26, 1253–1257. [Google Scholar] [CrossRef] [PubMed]
- Kasim, A.A. Calcium, Magnesium and Phosphorous Levels in Serum of Iraqi Women with Fibromyalgia. Iraqi J. Pharm. Sci. 2011, 20, 34–37. [Google Scholar]
- Boulis, M.; Boulis, M.; Clauw, D. Magnesium and Fibromyalgia: A Literature Review. J. Prim. Care Community Health 2021, 12, 215013272110384. [Google Scholar] [CrossRef]
- Andretta, A.; Dias Batista, E.; Madalozzo Schieferdecker, M.E.; Rasmussen Petterle, R.; Boguszewski, C.L.; Dos Santos Paiva, E. Relation between Magnesium and Calcium and Parameters of Pain, Quality of Life and Depression in Women with Fibromyalgia. Adv. Rheumatol. Lond. Engl. 2019, 59, 55. [Google Scholar] [CrossRef] [Green Version]
- Russell, I.J.; Michalek, J.E.; Flechas, J.D.; Abraham, G.E. Treatment of Fibromyalgia Syndrome with Super Malic: A Randomized, Double Blind, Placebo Controlled, Crossover Pilot Study. J. Rheumatol. 1995, 22, 953–958. [Google Scholar]
- Ng, S.Y. Hair Calcium and Magnesium Levels in Patients with Fibromyalgia: A Case Center Study. J. Manip. Physiol. Ther. 1999, 22, 586–593. [Google Scholar] [CrossRef]
- Porter, N.S.; Jason, L.A.; Boulton, A.; Bothne, N.; Coleman, B. Alternative Medical Interventions Used in the Treatment and Management of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome and Fibromyalgia. J. Altern. Complement. Med. 2010, 16, 235–249. [Google Scholar] [CrossRef]
- Shin, H.-J.; Na, H.-S.; Do, S.-H. Magnesium and Pain. Nutrients 2020, 12, 2184. [Google Scholar] [CrossRef]
- Tarasov, E.A.; Blinov, D.V.; Zimovina, U.V.; Sandakova, E.A. Magnesium deficiency and stress: Issues of their relationship, diagnostic tests, and approaches to therapy. Ter. Arkh. 2015, 87, 114–122. [Google Scholar] [CrossRef] [PubMed]
- Mohabbat, A.B.; Mahapatra, S.; Jenkins, S.M.; Bauer, B.A.; Vincent, A.; Wahner-Roedler, D.L. Use of Complementary and Integrative Therapies by Fibromyalgia Patients: A 14-Year Follow-Up Study. Mayo Clin. Proc. Innov. Qual. Outcomes 2019, 3, 418–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.-A.; Goldenberg, D.L.; Häuser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. 2016 Revisions to the 2010/2011 Fibromyalgia Diagnostic Criteria. Semin. Arthritis Rheum. 2016, 46, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Bennett, R. The Fibromyalgia Impact Questionnaire (FIQ): A Review of Its Development, Current Version, Operating Characteristics and Uses. Clin. Exp. Rheumatol. 2005, 23, S154. [Google Scholar]
- Perrot, S.; Bouhassira, D.; Fermanian, J. Development and Validation of the Fibromyalgia Rapid Screening Tool (FiRST). Pain 2010, 150, 250–256. [Google Scholar] [CrossRef]
- Lovibond, P.F.; Lovibond, S.H. The Structure of Negative Emotional States: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Cleeland, C.S.; Ryan, K.M. Pain Assessment: Global Use of the Brief Pain Inventory. Ann. Acad. Med. 1994, 23, 129–138. [Google Scholar]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A New Instrument for Psychiatric Practice and Research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Ware, J.E., Jr.; Kosinski, M.; Keller, S.D. A 12-Item Short-Form Health Survey: Construction of Scales and Preliminary Tests of Reliability and Validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef] [Green Version]
- Ware, J.E.; Sherbourne, C.D. The MOS 36-Item Short-Form Health Survey (SF-36). I. Conceptual Framework and Item Selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Krupp, L.B.; LaRocca, N.G.; Muir-Nash, J.; Steinberg, A.D. The Fatigue Severity Scale. Application to Patients with Multiple Sclerosis and Systemic Lupus Erythematosus. Arch. Neurol. 1989, 46, 1121–1123. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, M.J.L.; Bishop, S.R.; Pivik, J. The Pain Catastrophizing Scale: Development and Validation. Psychol. Assess. 1995, 7, 524. [Google Scholar] [CrossRef]
- Sass, C.; Dupré, C.; Giordanella, J.P.; Girard, F.; Guenot, C.; Labbe, É.; Rosa, E.L.; Magnier, P.; Martin, É.; Royer, B.; et al. Le score Epices: Un score individuel de précarité. Construction du score et mesure des relations avec des données de santé, dans une population de 197 389 personnes. Bull. Epidemiol. Hebd. 2006, 14, 93–96. [Google Scholar]
- Committee for Proprietary Medicinal Products (CPMP). Points to Consider on Adjustment for Baseline Covariates. Stat. Med. 2004, 23, 701–709. [Google Scholar] [CrossRef]
- Ruwaard, J.; Lange, A.; Bouwman, M.; Broeksteeg, J.; Schrieken, B. E-Mailed Standardized Cognitive Behavioural Treatment of Work-Related Stress: A Randomized Controlled Trial. Cogn. Behav. Ther. 2007, 36, 179–192. [Google Scholar] [CrossRef] [PubMed]
- Dualé, C.; Cardot, J.-M.; Joanny, F.; Trzeciakiewicz, A.; Martin, E.; Pickering, G.; Dubray, C. An Advanced Formulation of a Magnesium Dietary Supplement Adapted for a Long-Term Use Supplementation Improves Magnesium Bioavailability: In Vitro and Clinical Comparative Studies. Biol. Trace Elem. Res. 2018, 186, 1–8. [Google Scholar] [CrossRef]
- Eisinger, J.; Plantamura, A.; Marie, P.A.; Ayavou, T. Selenium and Magnesium Status in Fibromyalgia. Magnes. Res. 1994, 7, 285–288. [Google Scholar]
- Romano, T.; Stiller, J. Magnesium Deficiency in Fibromyalgia Syndrome. J. Nutr. Environ. Med. 1994, 4, 165–167. [Google Scholar] [CrossRef]
- Costello, R.B.; Elin, R.J.; Rosanoff, A.; Wallace, T.C.; Guerrero-Romero, F.; Hruby, A.; Lutsey, P.L.; Nielsen, F.H.; Rodriguez-Moran, M.; Song, Y.; et al. Perspective: The Case for an Evidence-Based Reference Interval for Serum Magnesium: The Time Has Come. Adv. Nutr. 2016, 7, 977–993. [Google Scholar] [CrossRef]
- Batista, E.D.; Andretta, A.; de Miranda, R.C.; Nehring, J.; Paiva, E.D.S.; Schieferdecker, M.E.M. Avaliação da ingestão alimentar e qualidade de vida de mulheres com fibromialgia. Rev. Bras. Reumatol. 2016, 56, 105–110. [Google Scholar] [CrossRef]
- Elin, R.J. Assessment of Magnesium Status for Diagnosis and Therapy. Magnes. Res. 2010, 23, S194–S198. [Google Scholar] [CrossRef] [PubMed]
- Barbagallo, M.; Veronese, N.; Dominguez, L.J. Magnesium in Aging, Health and Diseases. Nutrients 2021, 13, 463. [Google Scholar] [CrossRef] [PubMed]
- Noah, L.; Pickering, G.; Mazur, A.; Dubray, C.; Hitier, S.; Dualé, C.; Pouteau, E. Impact of Magnesium Supplementation, in Combination with Vitamin B6, on Stress and Magnesium Status: Secondary Data from a Randomized Controlled Trial. Magnes. Res. 2020, 33, 45–57. [Google Scholar] [CrossRef] [PubMed]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on Dietary Reference Values for Magnesium. EFSA J. 2015, 13, 4186. [Google Scholar] [CrossRef] [Green Version]
- Morris, M.E. Brain and CSF Magnesium Concentrations during Magnesium Deficit in Animals and Humans: Neurological Symptoms. Magnes. Res. 1992, 5, 303–313. [Google Scholar]
- Ross, A.C.; Caballero, B.H.; Cousins, R.J.; Tucker, K.L.; Ziegler, T.R. Modern Nutrition in Health and Disease: Eleventh Edition; Wolters Kluwer Health Adis (ESP): Amsterdam, The Netherlands, 2012; ISBN 978-1-60547-461-8. [Google Scholar]
- Botturi, A.; Ciappolino, V.; Delvecchio, G.; Boscutti, A.; Viscardi, B.; Brambilla, P. The Role and the Effect of Magnesium in Mental Disorders: A Systematic Review. Nutrients 2020, 12, E1661. [Google Scholar] [CrossRef]
- Benedetti, F.; Mayberg, H.S.; Wager, T.D.; Stohler, C.S.; Zubieta, J.-K. Neurobiological Mechanisms of the Placebo Effect. J. Neurosci. 2005, 25, 10390–10402. [Google Scholar] [CrossRef] [Green Version]
- Migliorini, F.; Maffulli, N.; Eschweiler, J.; Betsch, M.; Tingart, M.; Colarossi, G. Placebo Effect in Pharmacological Management of Fibromyalgia: A Meta-Analysis. Br. Med. Bull. 2021, 139, 73–85. [Google Scholar] [CrossRef]
- Kosek, E.; Rosen, A.; Carville, S.; Choy, E.; Gracely, R.H.; Marcus, H.; Petzke, F.; Ingvar, M.; Jensen, K.B. Lower Placebo Responses After Long-Term Exposure to Fibromyalgia Pain. J. Pain 2017, 18, 835–843. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Zou, K.; Abdullah, N.; Whiteside, N.; Sarmanova, A.; Doherty, M.; Zhang, W. The Placebo Effect and Its Determinants in Fibromyalgia: Meta-Analysis of Randomised Controlled Trials. Clin. Rheumatol. 2017, 36, 1623–1630. [Google Scholar] [CrossRef] [Green Version]
- Tseng, M.-T.; Chiang, M.-C.; Chao, C.-C.; Tseng, W.-Y.I.; Hsieh, S.-T. FMRI Evidence of Degeneration-Induced Neuropathic Pain in Diabetes: Enhanced Limbic and Striatal Activations. Hum. Brain Mapp. 2013, 34, 2733–2746. [Google Scholar] [CrossRef] [PubMed]
- Keulers, E.H.H.; Stiers, P.; Nicolson, N.A.; Jolles, J. The Association between Cortisol and the BOLD Response in Male Adolescents Undergoing FMRI. Brain Res. 2015, 1598, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Reicherts, P.; Wiemer, J.; Gerdes, A.B.M.; Schulz, S.M.; Pauli, P.; Wieser, M.J. Anxious Anticipation and Pain: The Influence of Instructed vs Conditioned Threat on Pain. Soc. Cogn. Affect. Neurosci. 2017, 12, 544–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berretz, G.; Packheiser, J.; Kumsta, R.; Wolf, O.T.; Ocklenburg, S. The Brain under Stress—A Systematic Review and Activation Likelihood Estimation Meta-Analysis of Changes in BOLD Signal Associated with Acute Stress Exposure. Neurosci. Biobehav. Rev. 2021, 124, 89–99. [Google Scholar] [CrossRef]
- Peyron, R.; Faillenot, I. Functional brain mapping of pain perception. Med. Sci. 2011, 27, 82–87. [Google Scholar] [CrossRef]
- Garland, E.L. Pain Processing in the Human Nervous System: A Selective Review of Nociceptive and Biobehavioral Pathways. Prim. Care 2012, 39, 561–571. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Larrea, L.; Peyron, R. Pain Matrices and Neuropathic Pain Matrices: A Review. Pain 2013, 154 (Suppl. S1), S29–S43. [Google Scholar] [CrossRef] [Green Version]
- Peyron, R. Functional imaging of pain. Biol. Aujourdhui 2014, 208, 5–12. [Google Scholar] [CrossRef]
- Wager, T.D.; Rilling, J.K.; Smith, E.E.; Sokolik, A.; Casey, K.L.; Davidson, R.J.; Kosslyn, S.M.; Rose, R.M.; Cohen, J.D. Placebo-Induced Changes in FMRI in the Anticipation and Experience of Pain. Science 2004, 303, 1162–1167. [Google Scholar] [CrossRef]
- Wager, T.D.; Atlas, L.Y. The Neuroscience of Placebo Effects: Connecting Context, Learning and Health. Nat. Rev. Neurosci. 2015, 16, 403–418. [Google Scholar] [CrossRef]
- Zunhammer, M.; Spisák, T.; Wager, T.D.; Bingel, U. Meta-Analysis of Neural Systems Underlying Placebo Analgesia from Individual Participant FMRI Data. Nat. Commun. 2021, 12, 1391. [Google Scholar] [CrossRef] [PubMed]
- Vachon-Presseau, E.; Martel, M.-O.; Roy, M.; Caron, E.; Albouy, G.; Marin, M.-F.; Plante, I.; Sullivan, M.J.; Lupien, S.J.; Rainville, P. Acute Stress Contributes to Individual Differences in Pain and Pain-Related Brain Activity in Healthy and Chronic Pain Patients. J. Neurosci. 2013, 33, 6826–6833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Houdenhove, B.; Egle, U.; Luyten, P. The Role of Life Stress in Fibromyalgia. Curr. Rheumatol. Rep. 2005, 7, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Samartin-Veiga, N.; González-Villar, A.J.; Pidal-Miranda, M.; Vázquez-Millán, A.; Carrillo-de-la-Peña, M.T. Active and Sham Transcranial Direct Current Stimulation (TDCS) Improved Quality of Life in Female Patients with Fibromyalgia. Qual. Life Res. 2022. [Google Scholar] [CrossRef]
- Park, R.; Ho, A.M.-H.; Pickering, G.; Arendt-Nielsen, L.; Mohiuddin, M.; Gilron, I. Efficacy and Safety of Magnesium for the Management of Chronic Pain in Adults: A Systematic Review. Anesth. Analg. 2020, 131, 764–775. [Google Scholar] [CrossRef]
- Morel, V.; Pickering, M.-E.; Goubayon, J.; Djobo, M.; Macian, N.; Pickering, G. Magnesium for Pain Treatment in 2021? State of the Art. Nutrients 2021, 13, 1397. [Google Scholar] [CrossRef]
- Ali, A.; Njike, V.Y.; Northrup, V.; Sabina, A.B.; Williams, A.-L.; Liberti, L.S.; Perlman, A.I.; Adelson, H.; Katz, D.L. Intravenous Micronutrient Therapy (Myers’ Cocktail) for Fibromyalgia: A Placebo-Controlled Pilot Study. J. Altern. Complement. Med. 2009, 15, 247–257. [Google Scholar] [CrossRef]
- Ferreira, I.; Ortigoza, Á.; Moore, P. Magnesium and malic acid supplement for fibromyalgia. Medwave 2019, 19, e7633. [Google Scholar] [CrossRef]
- Calandre, E.P.; Morillas-Arques, P.; Molina-Barea, R.; Rodriguez-Lopez, C.M.; Rico-Villademoros, F. Trazodone plus Pregabalin Combination in the Treatment of Fibromyalgia: A Two-Phase, 24-Week, Open-Label Uncontrolled Study. BMC Musculoskelet. Disord. 2011, 12, 95. [Google Scholar] [CrossRef] [Green Version]
- Abdel Fattah, Y.H.; Elnemr, R. Efficacy of Pregabalin as a Monotherapy versus Combined Pregabalin and Milnacipran in the Management of Fibromyalgia. Int. J. Rheum. Dis. 2020, 23, 1474–1480. [Google Scholar] [CrossRef]
- Karamanlioglu, D.S.; Geler Kulcu, D.; Ozturk, G.; Akpinar, P.; Unlu Ozkan, F.; Aktas, I. Effectiveness of Pregabalin Treatment for Trigger Points in Patients with Comorbid Myofascial Pain Syndrome and Fibromyalgia Syndrome: A Randomized Controlled Trial. Somatosens. Mot. Res. 2021, 38, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Lunn, M.P.; Hughes, R.A.; Wiffen, P.J. Duloxetine for Treating Painful Neuropathy, Chronic Pain or Fibromyalgia. Cochrane Database Syst. Rev. 2014, 1, CD007115. [Google Scholar] [CrossRef] [PubMed]
- Ghavidel-Parsa, B.; Bidari, A.; Rahimi, A.; Gharibpoor, F.; Khosousi, M.-J. No Effect of Approved Fibromyalgia Drugs on the Social Pain (Invalidation) Contrary to Physical Pain: An Open-Label Short-Term Randomized Clinical Trial. Clin. Rheumatol. 2021, 41, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Häuser, W.; Petzke, F.; Üçeyler, N.; Sommer, C. Comparative Efficacy and Acceptability of Amitriptyline, Duloxetine and Milnacipran in Fibromyalgia Syndrome: A Systematic Review with Meta-Analysis. Rheumatology 2011, 50, 532–543. [Google Scholar] [CrossRef] [Green Version]
- Macfarlane, G.J.; Kronisch, C.; Atzeni, F.; Häuser, W.; Choy, E.H.; Amris, K.; Branco, J.; Dincer, F.; Leino-Arjas, P.; Longley, K.; et al. EULAR Recommendations for Management of Fibromyalgia. Ann. Rheum. Dis. 2017, 76, e54. [Google Scholar] [CrossRef]
- Martínez-Rodríguez, A.; Rubio-Arias, J.Á.; Ramos-Campo, D.J.; Reche-García, C.; Leyva-Vela, B.; Nadal-Nicolás, Y. Psychological and Sleep Effects of Tryptophan and Magnesium-Enriched Mediterranean Diet in Women with Fibromyalgia. Int. J. Environ. Res. Public. Health 2020, 17, 2227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arab, A.; Rafie, N.; Amani, R.; Shirani, F. The Role of Magnesium in Sleep Health: A Systematic Review of Available Literature. Biol. Trace Elem. Res. 2022. [Google Scholar] [CrossRef] [PubMed]
- Pickering, G.; Macian, N.; Delage, N.; Picard, P.; Cardot, J.-M.; Sickout-Arondo, S.; Giron, F.; Dualé, C.; Pereira, B.; Marcaillou, F. Milnacipran Poorly Modulates Pain in Patients Suffering from Fibromyalgia: A Randomized Double-Blind Controlled Study. Drug Des. Devel. Ther. 2018, 12, 2485–2496. [Google Scholar] [CrossRef] [Green Version]
- Macian, N.; Pereira, B.; Shinjo, C.; Dubray, C.; Pickering, G. Fibromyalgia, Milnacipran and Experimental Pain Modulation: Study Protocol for a Double Blind Randomized Controlled Trial. Trials 2015, 16, 134. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Mg (n = 37) | Placebo (n = 38) | |
|---|---|---|
| Age (years, mean ± SD) | 54.0 ± 11.5 | 51.8 ± 10.9 |
| BMI (mean ± SD) | 25.7 ± 5.1 | 26.5 ± 6.1 |
| FM duration (years, mean ± SD) | 9.6 ± 7.1 | 7.8 ± 6.2 |
| Widespread Pain Index, ACR 2016 (0–19) (mean ± SD) | 12.3 ± 3.1 | 12.8 ± 3.2 |
| SSS, ACR 2016 (0–12) (mean ± SD) | 8.6 ± 1.5 | 8.8 ± 1.8 |
| DASS-42 stress score (0–42) (mean ± SD) | 30.8 ± 6.3 | 30.4 ± 5.8 |
| Pain (numerical scale) (0–10) (mean ± SD) | 6.0 ± 1.8 | 6.4 ± 1.5 |
| FIRST (0–6) (mean ± SD) | 5.4 ± 0.8 | 5.6 ± 0.8 |
| FIQ (0–100) (mean ± SD) | 59.7 ± 10.7 | 62.3 ± 14.5 |
| BPI Pain severity (0–10) (mean ± SD) | 5.4 ± 1.2 | 5.7 ± 1.2 |
| BPI Pain interference (0–10) (mean ± SD) | 5.8 ± 1.7 | 5.9 ± 2.1 |
| BPI Pain Experience (0–10) (mean ± SD) | 5.6 ± 1.2 | 5.8 ± 1.3 |
| PSQI Global score (0–21) (mean ± SD) | 11.5 ± 3.2 | 13.8 ± 3.2 |
| PSQI Subjective sleep quality (0–3) (mean ± SD) | 2.1 ± 0.7 | 2.2 ± 0.7 |
| PSQI Sleep latency (0–3) (mean ± SD) | 2.1 ± 0.9 | 2.4 ± 0.8 |
| PSQI Sleep duration (0–3) (mean ± SD) | 1.2 ± 0.9 | 1.8 ± 0.9 |
| PSQI Sleep efficiency (0–3) (mean ± SD) | 1.3 ± 1.2 | 2.0 ± 1.1 |
| PSQI Sleep disturbance (0–3) (mean ± SD) | 2.2 ± 0.6 | 2.1 ± 0.5 |
| PSQI Use of sleep medication (0–3) (mean ± SD) | 1.2 ± 1.4 | 1.5 ± 1.5 |
| PSQI Daytime dysfunction (0–3) (mean ± SD) | 1.5 ± 0.8 | 1.9 ± 0.8 |
| SF12-Mental score (0–100) (mean ± SD) | 31.6 ± 6.2 | 33.0 ± 9.3 |
| SF12-Physical score (0–100) (mean ± SD) | 30.9 ± 5.8 | 30.7 ± 5.7 |
| FSS (9–63) (mean ± SD) | 51.9 ± 10.3 | 50.0 ± 12.0 |
| PCS Total (0–52) (mean ± SD) | 29.7 ± 10.5 | 28.9 ± 13.1 |
| PCS Rumination (0–16) (mean ± SD) | 9.3 ± 4.1 | 8.6 ± 4.9 |
| PCS Magnification (0–12) (mean ± SD) | 5.3 ± 2.8 | 6.1 ± 3.5 |
| PCS Helplessness (0–24) (mean ± SD) | 15.2 ± 4.9 | 14.2 ± 6.1 |
| Precariousness (EPICES), (10–75) (mean ± SD) | 26.9 ± 21.0 | 24.0 ± 19.8 |
| Serum Mg (mmol/L) (mean ± SD) | 0.92 ± 0.08 | 0.91 ± 0.08 |
| Erythrocyte Mg (mmol/L) (mean ± SD) | 2.86 ± 0.32 | 2.97 ± 0.31 |
| m/M Subgroup (n = 16) | S/S+ Subgroup (n = 59) | p | |
|---|---|---|---|
| Mean FM duration (mean ± SD) | 6.1 ± 5.1 | 9.3 ± 7.0 | 0.09 |
| Age < 50 years (percent) | 50 | 34 | 0.5 |
| Age ≥ 50 years (percent) | 50 | 66 | 0.6 |
| Pain (numerical scale) (0–10) (mean ± SD) | 6.2 ± 1.6 | 6.2 ± 1.7 | 0.9 |
| BPI Pain severity (0–10) (mean ± SD) | 5.5 ± 1.0 | 5.6 ± 1.3 | 0.7 |
| Mg (n = 37) | Placebo (n = 38) | p | |
|---|---|---|---|
| Serum Mg (mmol/L) (mean ± SD) | 0.87 ± 0.07 | 0.87 ± 0.08 | 0.422 |
| Erythrocyte Mg (mmol/L) (mean ± SD) | 2.87 ± 0.37 | 2.91 ± 0.37 | 0.875 |
| Mg (n = 37) | Placebo (n = 38) | p | |
|---|---|---|---|
| WHO level I analgesics (percent (number)) | 46.0 (17) | 29.0 (11) | 0.13 |
| WHO level II analgesics (percent (number)) | 13.5 (5) | 2.6 (1) | 0.11 |
| WHO level III analgesics (percent (number)) | 2.7 (1) | 0 (0) | 0.49 |
| Co-analgesics (percent (number)) | 2.7 (1) | 7.9 (3) | 0.62 |
| Antidepressants (percent (number)) | 10.8 (4) | 7.9 (3) | 0.71 |
| Antiepileptics (percent (number)) | 0 (0) | 2.6 (1) | 1.00 |
| Hypnotics (percent (number)) | 5.4 (2) | 0 (0) | 0.24 |
| Anxiolytics (percent (number)) | 2.7 (1) | 7.9 (3) | 0.62 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Macian, N.; Dualé, C.; Voute, M.; Leray, V.; Courrent, M.; Bodé, P.; Giron, F.; Sonneville, S.; Bernard, L.; Joanny, F.; et al. Short-Term Magnesium Therapy Alleviates Moderate Stress in Patients with Fibromyalgia: A Randomized Double-Blind Clinical Trial. Nutrients 2022, 14, 2088. https://doi.org/10.3390/nu14102088
Macian N, Dualé C, Voute M, Leray V, Courrent M, Bodé P, Giron F, Sonneville S, Bernard L, Joanny F, et al. Short-Term Magnesium Therapy Alleviates Moderate Stress in Patients with Fibromyalgia: A Randomized Double-Blind Clinical Trial. Nutrients. 2022; 14(10):2088. https://doi.org/10.3390/nu14102088
Chicago/Turabian StyleMacian, Nicolas, Christian Dualé, Marion Voute, Vincent Leray, Marion Courrent, Paula Bodé, Fatiha Giron, Sylvie Sonneville, Lise Bernard, Fabienne Joanny, and et al. 2022. "Short-Term Magnesium Therapy Alleviates Moderate Stress in Patients with Fibromyalgia: A Randomized Double-Blind Clinical Trial" Nutrients 14, no. 10: 2088. https://doi.org/10.3390/nu14102088
APA StyleMacian, N., Dualé, C., Voute, M., Leray, V., Courrent, M., Bodé, P., Giron, F., Sonneville, S., Bernard, L., Joanny, F., Menard, K., Ducheix, G., Pereira, B., & Pickering, G. (2022). Short-Term Magnesium Therapy Alleviates Moderate Stress in Patients with Fibromyalgia: A Randomized Double-Blind Clinical Trial. Nutrients, 14(10), 2088. https://doi.org/10.3390/nu14102088