
How Does the Family Influence Adolescent Eating Habits in Terms of Knowledge, Attitudes and Practices? A Global Systematic Review of Qualitative Studies

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search Strategy
2.2. Study Selection
2.3. Data Extraction
2.4. Quality Assessment
2.5. Data Synthesis
3. Results
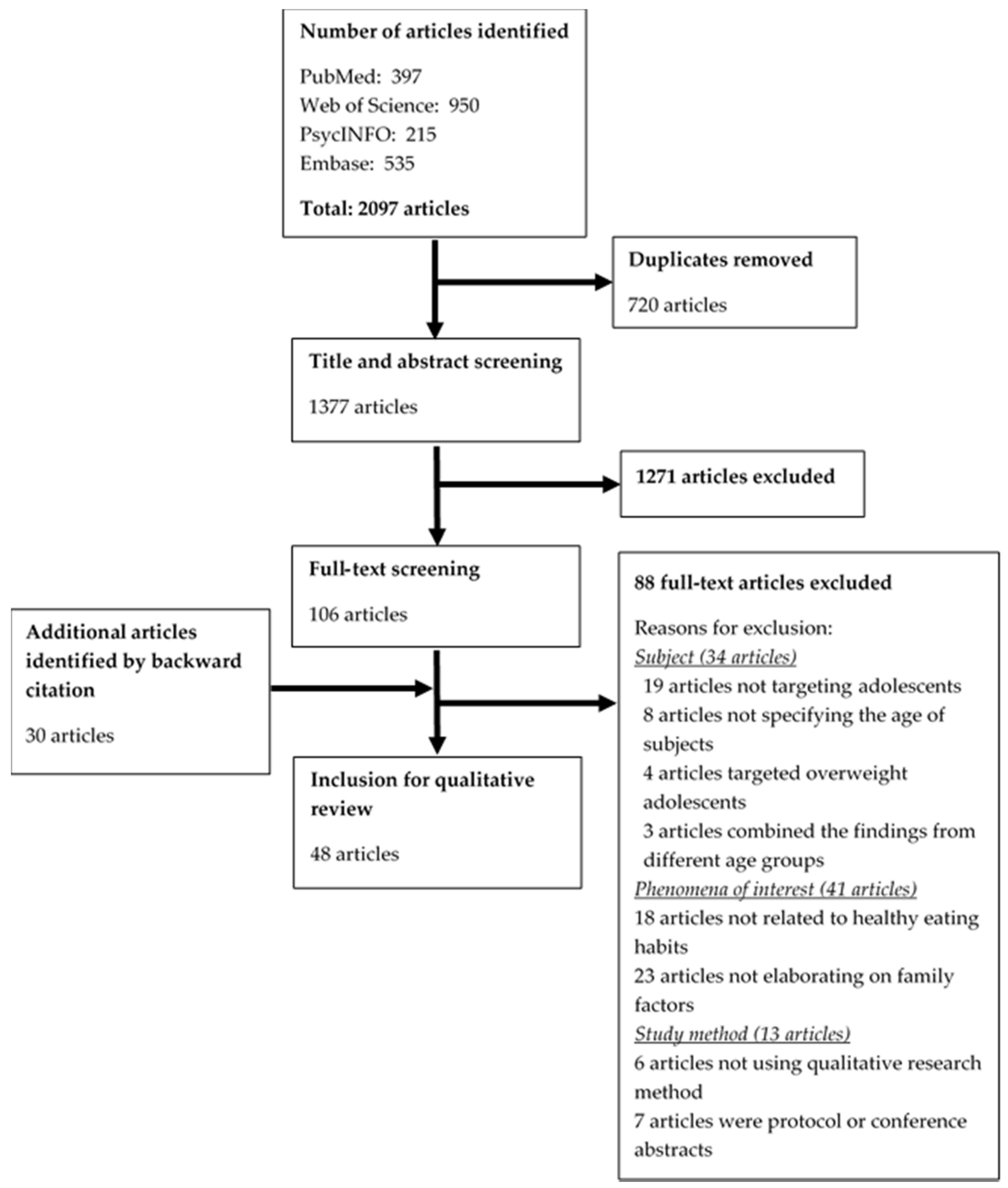
3.1. Study Selection and Study Characteristics
3.2. Study Quality
3.3. Synthesis of Findings
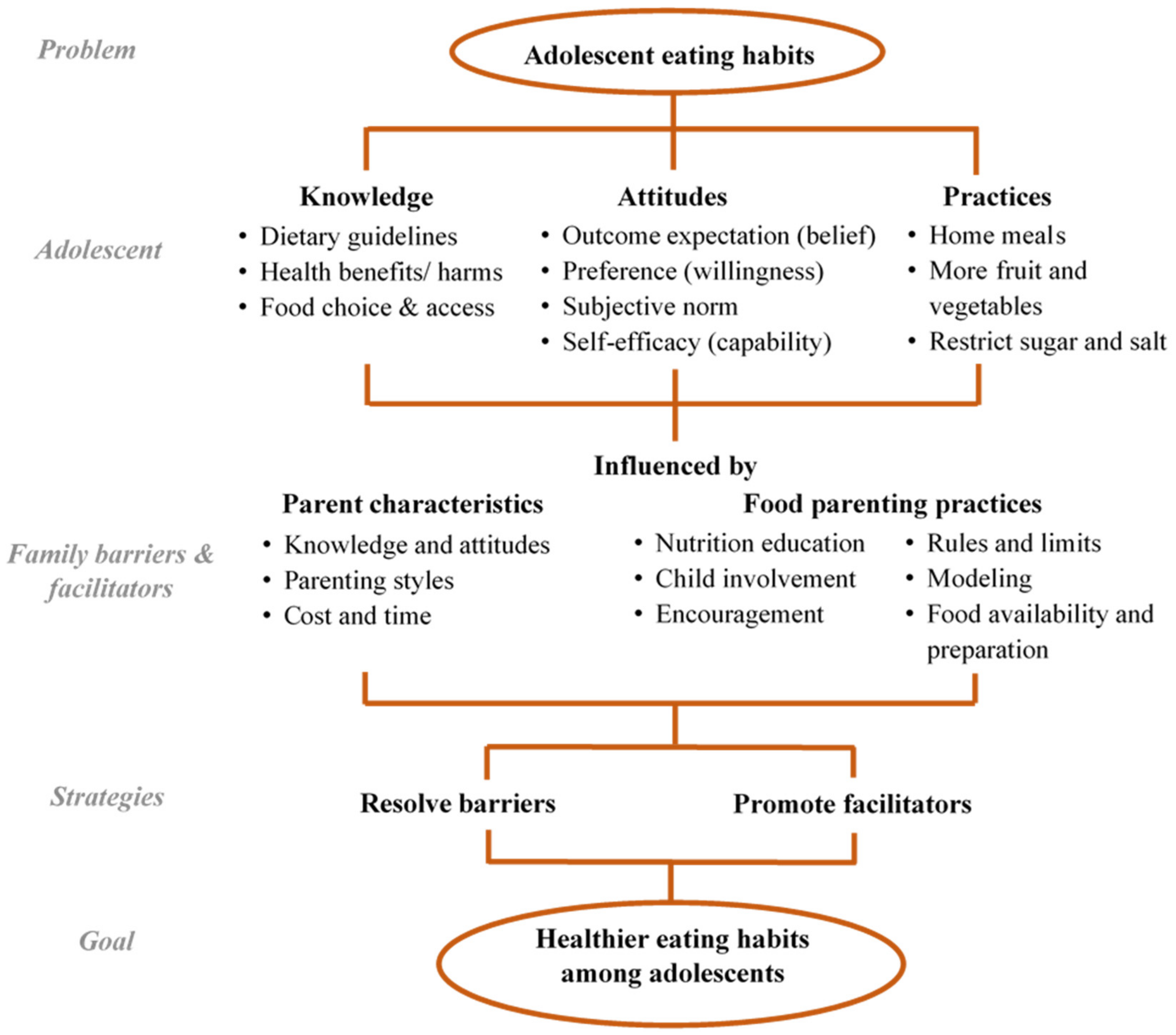
3.3.1. Adolescent Knowledge
- Nutrition education (theme 1)
- Many studies found nutrition education by parents on both types of knowledge is a facilitator for adolescents to eat healthily, specifically, education on nutrition benefits. For example, disease prevention, weight loss and growth [38,43,51,56,66,67,70,74,77,80], health consequences of unhealthy eating such as heart and kidney problems [33,44,47,55], and healthy food choice and cooking skills [38,39,43,44,48,55,56,57,58,61,66,70,71,77,80]. However, parents with inaccurate knowledge can deliver messages that are inconsistent with what is taught at school, which confuses the adolescents [55].
- Child involvement (theme 2)
- Communication between parents and adolescents is important in education [37,47,54], whereas child involvement in meal planning and discussion facilitates effective communication. Four parenting strategies were identified: (1) mealtime and grocery shopping being used as opportunities to teach adolescents nutritional knowledge, such as reading food labels [38,51,55,65,66,71,80]; (2) open discussion on diet-related health outcomes [39,47]; (3) teaching adolescents about self-regulation [55,66]; (4) providing nutritional information in a casual and fun way [37]. Conversely, excluding adolescents from grocery shopping and meal preparation due to their busy study schedules served as a barrier to adolescents’ acquisition of practical nutritional knowledge [39]. Parents also perceived that the ability of food discussion was limited by their own poor eating habits [51].
- Family illness experience (theme 3)
3.3.2. Adolescent Attitudes
- Family health (theme 4)
- Adolescents have become more aware of the negative impacts of unhealthy eating from the experience of health problems, particularly obesity, diabetes mellitus, and heart diseases, among the family members in the US studies [37,39,47,54]. Belief in healthy eating was, on the other hand, enhanced by observing positive outcomes from family members consuming healthy foods such as fruit and vegetables [35,69].
- Cultivation of preference (theme 5)
- Cultivating preference for healthy food was a commonly found family facilitator, particularly in studies where participants were young adolescents [35,37,43,51,58,59,62,64,65,66,70]. Communication on nutritional information influenced their food interpretation and preference for health [37,51,59]. Parents could broaden adolescents’ taste preferences and acceptance by exposing them to a wide variety of nutritious foods at an early age [43,65,70] and by making healthy eating fun, for example, choosing vegetables in certain colors during shopping [35] as well as providing fewer food choices at home [64]. To tackle the taste preference for junk food, parents tried to reduce these temptations by limiting sedentary time and engaging their adolescents in activities such as sports and hobbies [43]. Hygienic concerns could encourage adolescents, particularly in rural areas, to eat at home instead of food stalls on the streets [60]. One barrier hindering adolescents’ preference for healthy food was family’s prioritizing either low cost or unhealthy food [40,51].
- Family motivation (theme 6)
- Family norm and role modeling can be both facilitators of and barriers to healthy eating in adolescents. Aside from listening to their parents’ advice, adolescents also choose their food by observing their parents’ and siblings’ eating habits of both healthy [35,37,43,44,47,55,56,57,59,66,68,70,77,80] and unhealthy foods [39,40,46,47,48,49,50,54,59,68,69,72,73,74,79]. Parents who followed the same rules as they told their children enhanced the formation of the family norm [56,80]. Parents’ verbal encouragement and compliments served as positive reinforcement for healthy eating habits [35,38,44,49,51,68,69,71,75,77]. Examples include setting expectations on diet [51,80], family support on trying healthy foods for the first time [35], making healthy eating their family lifestyle [35], describing the taste of healthy foods [66], and communication between parents regarding adolescent eating habits [80]. Parental encouragement could be initiated by their concerns around adolescents’ health, in particular weight gain and illnesses from eating unhealthy foods [57,66], which formed the subjective norm in their children [38,56,78].
3.3.3. Adolescent Practices
- Food preparation and availability (theme 7)
- Many studies identified home meals as an important facilitator of healthy eating [33,34,35,36,38,42,43,44,48,50,61,62,63,66,70,71,75,77,78,80]. Subjects regarded food prepared at home as healthy due to better variety, freshness, and reduced uses of sugar, oil, and salt [33,71,78]. Apart from home meals, food availability also influenced adolescent food choice at home. Parents could manage the food supply to provide more healthy foods and to restrict food with insufficient nutrients [36,37,39,40,42,43,44,45,47,48,49,50,52,55,56,57,59,60,61,64,65,66,67,68,69,70,73,74,77,79,80]. Failure of some families to provide healthy meals [39,54,63,76,78] or stock healthy foods at home [40,41,46,48,49,53,59,67,68,69,74,78] is explained in more depth in the following themes.
- Time and cost (theme 8)
- Time and cost for healthy food were important barriers to healthy food provision at home. A tight schedule and long working hours of parents prevented them from preparing family meals, encouraging adolescents to consume takeaway, fast, and prepackaged food instead of fresh foods [35,36,37,41,43,45,48,50,52,53,54,59,61,63,64,65,68,69,70,71,76,78,79,80]. Some adolescents explained that more preparation work such as washing, cutting, and cooking is required for fresh production, as compared to ready-to-eat junk food and sugary drinks [40,67,69]. Easy accessibility of restaurants and food shops further attracted families to eat unhealthy food through takeaway or when they were eating out [36,72]. Peeling fruit and vegetables as well as cutting them into ready-to-eat pieces can overcome the ‘inconvenience’ barrier, especially among young adolescents [49,56,67,69,80]. Preparing portable water in the refrigerator provided a healthier alternative to sugary drinks on hand [57,66,73], while keeping snacks in a locked cabinet restricted the accessibility to young adolescents [64].
- Although low food budget might limit the purchase of junk snacks in some Western studies [36,59,66,79], it was also an important barrier to the purchase of more costly healthy food such as fruit, vegetables, and organic products, especially among low-income families who might choose unhealthy high-energy food because of its lower cost [34,35,36,37,38,41,45,46,48,49,51,54,60,61,66,67,69,72,75,77,78,79,80].
- Parenting style (theme 9)
- Several key parenting practices were highlighted in various studies, which could be facilitating or inhibiting adolescents’ eating habits, depending on the parenting styles. Setting family rules facilitated healthy eating in adolescents during home meals and snacking. Some examples of rules include: having vegetables with every dinner, finishing everything on the plate, and serving the same meal to all family members [37,44,49,52,53,61,63,77], as well as restricting the consumption of unhealthy snacks in terms of quantity and frequency, and drinking water between glasses of juice [33,37,42,43,47,50,52,56,59,64,67,68,77,80]. Some parents further monitored their adolescents’ eating practices by verbally checking on food purchases or consumption [49,56,80], tracking food stock at home [56], and requesting adolescents to seek permission before eating unhealthy food [67]. Several authoritative parenting strategies were proposed: (i) controlling or providing supervision on food choices such as asking adolescents to at least try a few bites of healthy food [44,48,49,69,74,75]; (ii) encouraging or prompting adolescents to try healthier alternatives with reasoning [37,57,60,66,70]; (iii) having regular meal schedules and eating with family [35,52,55,71]; (iv) setting a snacking allowance [43,64]; (v) being responsive to adolescents’ preference, especially on nutritious foods [64,80]. Except for one Canadian study that found parents preferred grocery shopping alone to prevent requests for junk foods by adolescents [44], involving them in meal planning, shopping and preparation with limited/ guided choices, such as selecting from a list of food choices, and washing and cutting fresh produce [37,44,59,64,80], was perceived as a facilitator to their eating habits.
- Unstructured practices are a major barrier to healthy eating practices in adolescents. Accommodating taste preference of family members, usually towards fast food [37,42,64,68,78], a lack of monitoring when not eating together at a table [66], and failing to negotiate for healthy eating [79] could counteract the benefits of home meals. The lack of parental supervision also encouraged adolescents’ unhealthy snacking habits as their food choice tended to be based on taste preferences and minimal preparation effort [39,40,50,51,53,59,66,67,69,72,76,79,80]. Family members, especially grandparents, might provide adolescents with unhealthy foods as treats and bribes [36,50], and these items such as chocolates, candies, and pizza were often used as rewards for good academic performance, helping out with chores, or even eating healthy foods [53,59,66,67,72,80]. On the other hand, over-restriction could have an opposite effect on adolescents as they might want the restricted food items more and consume them on other occasions when they are not monitored [70,80]. Some adolescents with poor family relationships mentioned that the unpleasant atmosphere of eating with their family sometimes prevented them from eating at home [63].
- Parental practical knowledge and attitudes (theme 10)
- The perception of home meals as inferior in taste with little variation [60,62,63] could be the result of insufficient knowledge on the range of healthy food choices and inadequate skills to prepare tasty, healthy meals. To facilitate healthy eating at home, some parents highlighted the importance of cooking skills to better the presentation of healthy food, for example, hiding fruit and vegetables in soup, stew, or smoothies [43,59,66,67,80], while others would modify recipes, attempting to use healthier cooking methods, optimizing food choices, and preparing meals at lower costs [36,72]. A number of US studies reported that a high level of health awareness in parents was essential to maintaining a healthy food environment at home [40,51,58,59,63].
4. Discussion
4.1. Major Findings
4.1.1. Parental Knowledge
4.1.2. Parental Attitudes
4.1.3. Parenting Style
4.1.4. Lack of Time
4.1.5. Cost Concern
4.1.6. Effect of Study Population and Design on Results
4.2. Implications of Findings
4.3. Gaps in the Existing Knowledge
4.4. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Llewellyn, A.; Simmonds, M.C.; Owen, C.; Woolacott, N. Childhood obesity as a predictor of morbidity in adulthood: A systematic review and meta-analysis. Obes. Rev. 2016, 17, 56–67. [Google Scholar] [CrossRef]
- Sommer, A.; Twig, G. The Impact of Childhood and Adolescent Obesity on Cardiovascular Risk in Adulthood: A Systematic Review. Curr. Diabetes Rep. 2018, 18, 91. [Google Scholar] [CrossRef]
- World Health Organization. Noncommunicable Diseases 2018. Available online: https://www.who.int/en/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 30 April 2021).
- Sun, H.; Ma, Y.; Han, D.; Pan, C.W.; Xu, Y. Prevalence and trends in obesity among China’s children and adolescents, 1985–2010. PLoS ONE 2014, 9, e105469. [Google Scholar]
- Zhang, J.; Wang, H.; Wang, Z.; Du, W.; Su, C.; Zhang, J.; Jiang, H.; Jia, X.; Huang, F.; Ouyang, Y.; et al. Prevalence and stabilizing trends in overweight and obesity among children and adolescents in China, 2011–2015. BMC Public Health 2018, 18, 571. [Google Scholar] [CrossRef] [PubMed]
- Roberts, C.; Steer, T.; Maplethorpe, N.; Cox, L.; Meadows, S.; Nicholson, S.; Page, P.; Swan, G. National Diet and Nutrition Survey: Results from Years 7 and 8 (Combined); Department of Health and Social Care: London, UK, 2018.
- Batis, C.; Aburto, T.C.; Sánchez-Pimienta, T.G.; Pedraza, L.S.; Rivera, J.A. Adherence to Dietary Recommendations for Food Group Intakes Is Low in the Mexican Population. J. Nutr. 2016, 146, 1897S–1906S. [Google Scholar] [CrossRef]
- Centre for Health Protection. Report of Population Health Survey 2014/15; Department of Health, HKSAR: Hong Kong, China, 2017.
- World Health Organization. Advocacy, Communication and Social Mobilization for TB Control: A Guide to Developing Knowledge, Attitude and Practice Surveys; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Marías, Y.; Glasauer, P. Guidelines for Assessing Nutrition-Related Knowledge, Attitudes and Practices; Food and Agriculture Organization of the United Nations: Rome, Italy, 2014. [Google Scholar]
- Hyun, H.; Lee, H.; Ro, Y.; Gray, H.L.; Song, K. Body image, weight management behavior, nutritional knowledge and dietary habits in high school boys in Korea and China. Asia Pac. J. Clin. Nutr. 2017, 26, 923–930. [Google Scholar] [PubMed]
- Son, S.; Ro, Y.; Hyun, H.; Lee, H.; Song, K. A comparative study on dietary behavior, nutritional knowledge and life stress between Korean and Chinese female high school students. Nutr. Res. Pract. 2014, 8, 205. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.; He, J.; Fan, X. Mapping and Predicting Patterns of Chinese Adolescents’ Food Preferences. Nutrients 2019, 11, 2124. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, S.; Basil, M.D.; Basil, D.Z. Factors Influencing Healthy Eating Habits among College Students: An Application of the Health Belief Model. Heal. Mark. Q. 2009, 26, 145–164. [Google Scholar] [CrossRef]
- Sleddens, E.F.C.; Kroeze, W.; Kohl, L.F.M.; Bolten, L.M.; Velema, E.; Kaspers, P.J.; Brug, J.; Kremers, S.P.J. Determinants of dietary behavior among youth: An umbrella review. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 7. [Google Scholar] [CrossRef]
- Riebl, S.K.; Estabrooks, P.A.; Dunsmore, J.C.; Salva, J.; Frisard, M.I.; Dietrich, A.M.; Peng, Y.; Zhang, X.; Davy, B.M. A systematic literature review and meta-analysis: The Theory of Planned Behavior’s application to understand and predict nutrition-related behaviors in youth. Eat. Behav. 2015, 18, 160–178. [Google Scholar] [CrossRef]
- Ashton, L.; Hutchesson, M.J.; Rollo, M.E.; Morgan, P.J.; Collins, C.E. Motivators and Barriers to Engaging in Healthy Eating and Physical Activity. Am. J. Men Health 2017, 11, 330–343. [Google Scholar] [CrossRef]
- O’Dea, J.A. Why do kids eat healthful food? Perceived benefits of and barriers to healthful eating and physical activity among children and adolescents. J. Am. Diet. Assoc. 2003, 103, 497–501. [Google Scholar]
- Beck, A.L.; Iturralde, E.; Haya-Fisher, J.; Kim, S.; Keeton, V.; Fernandez, A. Barriers and facilitators to healthy eating among low-income Latino adolescents. Appetite 2019, 138, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Vaughn, A.E.; Ward, D.S.; Fisher, J.O.; Faith, M.S.; Hughes, S.O.; Kremers, S.P.; Musher-Eizenman, D.R.; O’Connor, T.M.; Patrick, H.; Power, T.G. Fundamental constructs in food parenting practices: A content map to guide future research. Nutr. Rev. 2016, 74, 98–117. [Google Scholar] [CrossRef] [PubMed]
- Rodenburg, G.; Kremers, S.P.; Oenema, A.; van de Mheen, D. Associations of parental feeding styles with child snacking behaviour and weight in the context of general parenting. Public Health Nutr. 2014, 17, 960–969. [Google Scholar] [CrossRef]
- Sleddens, E.F.; Kremers, S.P.; Stafleu, A.; Dagnelie, P.C.; De Vries, N.K.; Thijs, C. Food parenting practices and child dietary behavior. Prospective relations and the moderating role of general parenting. Appetite 2014, 79, 42–50. [Google Scholar] [CrossRef]
- Peters, J.; Dollman, J.; Petkov, J.; Parletta, N. Associations between parenting styles and nutrition knowledge and 2–5-year-old children’s fruit, vegetable and non-core food consumption. Public Health Nutr. 2013, 16, 1979–1987. [Google Scholar] [CrossRef]
- Shepherd, J.; Harden, A.; Rees, R.; Brunton, G.; Garcia, J.; Oliver, S.; Oakley, A. Young people and healthy eating: A systematic review of research on barriers and facilitators. Health Educ. Res. 2006, 21, 239–257. [Google Scholar] [CrossRef]
- Pearson, N.; Biddle, S.; Gorely, T. Family correlates of fruit and vegetable consumption in children and adolescents: A systematic review. Public Health Nutr. 2009, 12, 267–283. [Google Scholar] [CrossRef] [PubMed]
- Yee, A.Z.H.; Lwin, M.O.; Ho, S.S. The influence of parental practices on child promotive and preventive food consumption behaviors: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 47. [Google Scholar] [CrossRef] [PubMed]
- Dixon-Woods, M.; Fitzpatrick, R.; Roberts, K. Including qualitative research in systematic reviews: Opportunities and problems. J. Evaluation Clin. Pract. 2001, 7, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, M.; Krølner, R.; Klepp, K.-I.; Lytle, L.; Brug, J.; Bere, E.; Due, P. Determinants of fruit and vegetable consumption among children and adolescents: A review of the literature. Part I: Quantitative studies. Int. J. Behav. Nutr. Phys. Act. 2006, 3, 22. [Google Scholar] [CrossRef]
- Krølner, R.; Rasmussen, M.; Brug, J.; Klepp, K.-I.; Wind, M.; Due, P. Determinants of fruit and vegetable consumption among children and adolescents: A review of the literature. Part II: Qualitative studies. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 112. [Google Scholar] [CrossRef]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef]
- Critical Appraisal Skills Programme. CASP Qualitative Studies Checklist 2018. Available online: https://casp-uk.net/wp-content/uploads/2018/03/CASP-Qualitative-Checklist-2018_fillable_form.pdf (accessed on 13 August 2020).
- Harden, A.; Garcia, J.; Oliver, S.; Rees, R.; Shepherd, J.; Brunton, G.; Oakley, A. Applying systematic review methods to studies of people’s views: An example from public health research. J. Epidemiol. Community Health 2004, 58, 794–800. [Google Scholar] [CrossRef]
- Chan, K.; Prendergast, G.; Grønhøj, A.; Bech-Larsen, T. Adolescents’ perceptions of healthy eating and communication about healthy eating. Health Educ. 2009, 109, 474–490. [Google Scholar] [CrossRef]
- Siu, J.Y.-M.; Chan, K.; Lee, A. Adolescents from low-income families in Hong Kong and unhealthy eating behaviours: Implications for health and social care practitioners. Health Soc. Care Community 2019, 27, 366–374. [Google Scholar] [CrossRef] [PubMed]
- Berge, J.M.; Arikian, A.; Doherty, W.J.; Neumark-Sztainer, D. Healthful Eating and Physical Activity in the Home Environment: Results from Multifamily Focus Groups. J. Nutr. Educ. Behav. 2012, 44, 123–131. [Google Scholar] [CrossRef]
- Fuster, M.; Weindorf, S.; Mateo, K.F.; Barata-Cavalcanti, O.; Leung, M.M. “It’s Sort Of, Like, in My Family’s Blood”: Exploring Latino Pre-adolescent Children and Their Parents’ Perceived Cultural Influences on Food Practices. Ecol. Food Nutr. 2019, 58, 620–636. [Google Scholar] [CrossRef]
- Kaplan, M.; Kiernan, N.E.; James, L. Intergenerational Family Conversations and Decision Making about Eating Healthfully. J. Nutr. Educ. Behav. 2006, 38, 298–306. [Google Scholar] [CrossRef]
- Banna, J.C.; Buchthal, O.V.; Delormier, T.; Creed-Kanashiro, H.M.; Penny, M.E. Influences on eating: A qualitative study of adolescents in a periurban area in Lima, Peru. BMC Public Health 2016, 16, 40. [Google Scholar] [CrossRef]
- Darling, C.A.; Rehm, M.; Coccia, C.; Cui, M. Adolescent Eating Behavior: The Role of Indulgent Parenting. Fam. Soc. J. Contemp. Soc. Serv. 2015, 96, 257–267. [Google Scholar] [CrossRef]
- Ortega-Avila, A.G.; Papadaki, A.; Jago, R. The role of the home environment in sugar-sweetened beverage intake among northern Mexican adolescents: A qualitative study. J. Public Health 2019, 27, 791–801. [Google Scholar] [CrossRef]
- Sedibe, M.; Feeley, A.; Voorend, C.; Griffiths, P.; Doak, C.; Norris, S. Narratives of urban female adolescents in South Africa: Dietary and physical activity practices in an obesogenic environment. S. Afr. J. Clin. Nutr. 2014, 27, 114–119. [Google Scholar] [CrossRef]
- Backett-Milburn, K.C.; Wills, W.J.; Gregory, S.; Lawton, J. Making sense of eating, weight and risk in the early teenage years: Views and concerns of parents in poorer socio-economic circumstances. Soc. Sci. Med. 2006, 63, 624–635. [Google Scholar] [CrossRef] [PubMed]
- Backett-Milburn, K.C.; Wills, W.J.; Roberts, M.-L.; Lawton, J. Food, eating and taste: Parents’ perspectives on the making of the middle class teenager. Soc. Sci. Med. 2010, 71, 1316–1323. [Google Scholar] [CrossRef]
- Bassett, R.; Chapman, G.E.; Beagan, B. Autonomy and control: The co-construction of adolescent food choice. Appetite 2008, 50, 325–332. [Google Scholar] [CrossRef]
- Brown, C.; Shaibu, S.; Maruapula, S.; Malete, L.; Compher, C. Perceptions and attitudes towards food choice in adolescents in Gaborone, Botswana. Appetite 2015, 95, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Calvert, S.; Dempsey, R.C.; Povey, R. A qualitative study investigating food choices and perceived psychosocial influences on eating behaviours in secondary school students. Br. Food J. 2020, 122, 1027–1039. [Google Scholar] [CrossRef]
- Christiansen, K.M.; Qureshi, F.; Schaible, A.; Park, S.; Gittelsohn, J. Environmental Factors That Impact the Eating Behaviors of Low-income African American Adolescents in Baltimore City. J. Nutr. Educ. Behav. 2013, 45, 652–660. [Google Scholar] [CrossRef]
- Correa, N.; Rajaraman, D.; Swaminathan, S.; Vaz, M.; Jayachitra, K.; Lear, S.A.; Punthakee, Z. Perceptions of healthy eating amongst Indian adolescents in India and Canada. Appetite 2017, 116, 471–479. [Google Scholar] [CrossRef]
- Cullen, K.W.; Baranowski, T.; Rittenberry, L.; Olvera, N. Social-environmental influences on children’s diets: Results from focus groups with African-, Euro- and Mexican-American children and their parents. Health Educ. Res. 2000, 15, 581–590. [Google Scholar] [CrossRef]
- Fielding-Singh, P. Dining with dad: Fathers’ influences on family food practices. Appetite 2017, 117, 98–108. [Google Scholar] [CrossRef]
- Fielding-Singh, P.; Wang, J. Table talk: How mothers and adolescents across socioeconomic status discuss food. Soc. Sci. Med. 2017, 187, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, A.; Heary, C.; Nixon, E.; Kelly, C. Factors influencing the food choices of Irish children and adolescents: A qualitative investigation. Health Promot. Int. 2010, 25, 289–298. [Google Scholar] [CrossRef]
- Garcia, M.L.; Gatdula, N.; Bonilla, E.; Frank, G.C.; Bird, M.; Rascón, M.S.; Rios-Ellis, B. Engaging Intergenerational Hispanics/Latinos to Examine Factors Influencing Childhood Obesity Using the PRECEDE–PROCEED Model. Matern. Child Health J. 2019, 23, 802–810. [Google Scholar] [CrossRef]
- Goh, Y.-Y.; Bogart, L.M.; Sipple-Asher, B.K.; Uyeda, K.; Hawes-Dawson, J.; Olarita-Dhungana, J.; Ryan, G.W.; Schuster, M.A. Using community-based participatory research to identify potential interventions to overcome barriers to adolescents’ healthy eating and physical activity. J. Behav. Med. 2009, 32, 491–502. [Google Scholar] [CrossRef] [PubMed]
- Gray, S. Bringing Policy and Practice to the Table: Young Women’s Nutritional Experiences in an Ontario Secondary School. Brock Educ. J. 2015, 24, 74–87. [Google Scholar] [CrossRef]
- Gunther, C.; Reicks, M.; Banna, J.; Suzuki, A.; Topham, G.; Richards, R.; Jones, B.; Lora, K.; Anderson, A.K.; Da Silva, V.; et al. Food Parenting Practices That Influence Early Adolescents’ Food Choices During Independent Eating Occasions. J. Nutr. Educ. Behav. 2019, 51, 993–1002. [Google Scholar] [CrossRef] [PubMed]
- Hattersley, L.A.; Shrewsbury, V.A.; King, L.A.; Howlett, S.A.; Hardy, L.L.; Baur, L.A. Adolescent-parent interactions and attitudes around screen time and sugary drink consumption: A qualitative study. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 61. [Google Scholar] [CrossRef]
- Heidelberger, L.; Smith, C. The Food Environment Through the Camera Lenses of 9-to 13-Year-Olds Living in Urban, Low-Income, Midwestern Households: A Photovoice Project. J. Nutr. Educ. Behav. 2015, 47, 437. [Google Scholar] [CrossRef]
- Holsten, J.E.; Deatrick, J.A.; Kumanyika, S.; Pinto-Martin, J.; Compher, C.W. Children’s food choice process in the home environment. A qualitative descriptive study. Appetite 2012, 58, 64–73. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.R.; Trenholm, J.; Rahman, A.; Pervin, J.; Ekström, E.-C.; Rahman, S.M. Sociocultural Influences on Dietary Practices and Physical Activity Behaviors of Rural Adolescents—A Qualitative Exploration. Nutrients 2019, 11, 2916. [Google Scholar] [CrossRef] [PubMed]
- Kumar, J.; Adhikari, K.; Li, Y.; Lindshield, E.; Muturi, N.; Kidd, T. Identifying barriers, perceptions and motivations related to healthy eating and physical activity among 6th to 8th grade, rural, limited-resource adolescents. Health Educ. 2016, 116, 123–137. [Google Scholar] [CrossRef]
- Monge-Rojas, R.; Garita, C.; Sánchez, M.; Muñoz, L. Barriers to and Motivators for Healthful Eating as Perceived by Rural and Urban Costa Rican Adolescents. J. Nutr. Educ. Behav. 2005, 37, 33–40. [Google Scholar] [CrossRef]
- Neumark-Sztainer, D.; Story, M.; Ackard, D.; Moe, J.; Perry, C. The “Family Meal”: Views of adolescents. J. Nutr. Educ. 2000, 32, 329–334. [Google Scholar] [CrossRef]
- O’Dougherty, M.; Story, M.; Lytle, L. Food choices of young African-American and Latino adolescents: Where do parents fit in? J. Am. Diet. Assoc. 2006, 106, 1846–1850. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Kang, J.-H.; Lawrence, R.; Gittelsohn, J. Environmental Influences on Youth Eating Habits: Insights from Parents and Teachers in South Korea. Ecol. Food Nutr. 2014, 53, 347–362. [Google Scholar] [CrossRef] [PubMed]
- Pinard, C.A.; Byker, C.; Harden, S.M.; Carpenter, L.R.; Serrano, E.L.; Schober, D.J.; Yaroch, A.L. Influences on Food Away from Home Feeding Practices Among English and Spanish Speaking Parent–Child Dyads. J. Child Fam. Stud. 2014, 24, 2099–2106. [Google Scholar] [CrossRef]
- Povey, R.; Cowap, L.; Gratton, L. “They said I’m a square for eating them” Children’s beliefs about fruit and vegetables in England. Br. Food J. 2016, 118, 2949–2962. [Google Scholar] [CrossRef]
- Power, T.G.; Bindler, R.C.; Goetz, S.; Daratha, K.B. Obesity Prevention in Early Adolescence: Student, Parent, and Teacher Views. J. Sch. Health 2009, 80, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Rakhshanderou, S.; Ramezankhani, A.; Mehrabi, Y.; Ghaffari, M. Determinants of fruit and vegetable consumption among Tehranian adolescents: A qualitative research. J. Res. Med Sci. 2014, 19, 482–489. [Google Scholar]
- Rathi, N.; Riddell, L.; Worsley, A. What influences urban Indian secondary school students’ food consumption?—A qualitative study. Appetite 2016, 105, 790–797. [Google Scholar] [CrossRef]
- Rawlins, E.; Baker, G.; Maynard, M.; Harding, S. Perceptions of healthy eating and physical activity in an ethnically diverse sample of young children and their parents: The DEAL prevention of obesity study. J. Hum. Nutr. Diet. 2013, 26, 132–144. [Google Scholar] [CrossRef]
- Rodríguez-Pérez, R.; Correa-Matos, N.; Valdés-Valderrama, A.; Rodríguez-Cruz, L.A.; Rodriguez, R. A Qualitative Study of Puerto Rican Parent and ChildPerceptions Regarding Eating Patterns. J. Nutr. Educ. Behav. 2019, 51, 608–615. [Google Scholar] [CrossRef]
- Roth-Yousey, L.; Chu, Y.L.; Reicks, M. A Qualitative Study to Explore How Parental Expectations and Rules Influence Beverage Choices in Early Adolescence. J. Nutr. Educ. Behav. 2012, 44, 644–652. [Google Scholar] [CrossRef] [PubMed]
- Ishak, S.I.Z.S.; Chin, Y.S.; Taib, M.N.M.; Shariff, Z.M. Malaysian adolescents’ perceptions of healthy eating: A qualitative study. Public Health Nutr. 2020, 23, 1440–1449. [Google Scholar] [CrossRef] [PubMed]
- Silva, D.C.D.; Frazao, I.D.; Osorio, M.M.; de Vasconcelos, M.G.L. Perception of adolescents on healthy eating. Cienc. Saude Coletiva 2015, 20, 3299–3308. [Google Scholar] [CrossRef]
- Snethen, J.A.; Hewitt, J.B.; Petering, D.H. Addressing Childhood Overweight: Strategies Learned from One Latino Community. J. Transcult. Nurs. 2007, 18, 366–372. [Google Scholar] [CrossRef]
- Steeves, E.T.A.; Johnson, K.A.; Pollard, S.L.; Jones-Smith, J.; Pollack, K.; Johnson, S.L.; Hopkins, L.; Gittelsohn, J. Social influences on eating and physical activity behaviours of urban, minority youths. Public Health Nutr. 2016, 19, 3406–3416. [Google Scholar] [CrossRef]
- Tiedje, K.; Wieland, M.L.; Meiers, S.J.; Mohamed, A.A.; Formea, C.M.; Ridgeway, J.L.; Asiedu, G.B.; Boyum, G.; Weis, J.A.; Nigon, J.A.; et al. A focus group study of healthy eating knowledge, practices, and barriers among adult and adolescent immigrants and refugees in the United States. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 63. [Google Scholar] [CrossRef]
- Verstraeten, R.; Van Royen, K.; Ochoa-Avilés, A.; Penafiel, D.; Holdsworth, M.; Donoso, S.; Maes, L.; Kolsteren, P. A Conceptual Framework for Healthy Eating Behavior in Ecuadorian Adolescents: A Qualitative Study. PLoS ONE 2014, 9, e87183. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Hurtado, G.A.; Flores, R.; Alba-Meraz, A.; Reicks, M. Latino Fathers’ Perspectives and Parenting Practices Regarding Eating, Physical Activity, and Screen Time Behaviors of Early Adolescent Children: Focus Group Findings. J. Acad. Nutr. Diet. 2018, 118, 2070–2080. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Action Plan for the Prevention and Control of NCDs 2013–2020; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Muzaffar, H.; Metcalfe, J.J.; Fiese, B. Narrative Review of Culinary Interventions with Children in Schools to Promote Healthy Eating: Directions for Future Research and Practice. Curr. Dev. Nutr. 2018, 2, nzy016. [Google Scholar] [CrossRef] [PubMed]
- Hutchinson, J.; Watt, J.F.; Strachan, E.K.; Cade, J.E. Evaluation of the effectiveness of the Ministry of Food cooking programme on self-reported food consumption and confidence with cooking. Public Health Nutr. 2016, 19, 3417–3427. [Google Scholar] [CrossRef]
- Overcash, F.; Ritter, A.; Mann, T.; Mykerezi, E.; Redden, J.; Rendahl, A.; Vickers, Z.; Reicks, M. Impacts of a Vegetable Cooking Skills Program Among Low-Income Parents and Children. J. Nutr. Educ. Behav. 2018, 50, 795–802. [Google Scholar] [CrossRef]
- Gevers, D.W.; van Assema, P.; Sleddens, E.F.; de Vries, N.K.; Kremers, S.P. Associations between general parenting, restrictive snacking rules, and adolescent’s snack intake. The roles of fathers and mothers and interparental congruence. Appetite 2015, 87, 184–191. [Google Scholar] [CrossRef]
- Rahill, S.; Kennedy, A.; Kearney, J. A review of the influence of fathers on children’s eating behaviours and dietary intake. Appetite 2020, 147, 104540. [Google Scholar] [CrossRef]
- Rampersaud, G.C.; Pereira, M.A.; Girard, B.L.; Adams, J.; Metzl, J.D. Breakfast Habits, Nutritional Status, Body Weight, and Academic Performance in Children and Adolescents. J. Am. Diet. Assoc. 2005, 105, 743–760. [Google Scholar] [CrossRef]
- Florence, M.D.; Asbridge, M.; Veugelers, P.J. Diet Quality and Academic Performance. J. Sch. Health 2008, 78, 209–215. [Google Scholar] [CrossRef]
- Busch, V.; Loyen, A.; Lodder, M.; Schrijvers, A.J.; van Yperen, T.A.; de Leeuw, J.R. The effects of adolescent health-related behavior on academic performance: A systematic review of the longitudinal evidence. Rev. Educ. Res. 2014, 84, 245–274. [Google Scholar] [CrossRef]
- So, E.S.; Park, B.M. Health Behaviors and Academic Performance Among Korean Adolescents. Asian Nurs. Res. 2016, 10, 123–127. [Google Scholar] [CrossRef]
- Levpušček, M.P. Adolescent individuation in relation to parents and friends: Age and gender differences. Eur. J. Dev. Psychol. 2006, 3, 238–264. [Google Scholar] [CrossRef]
- Larson, N.I.; Story, M.; Eisenberg, M.E.; Neumark-Sztainer, D. Food Preparation and Purchasing Roles among Adolescents: Associations with Sociodemographic Characteristics and Diet Quality. J. Am. Diet. Assoc. 2006, 106, 211–218. [Google Scholar] [CrossRef]
- Berge, J.M.; MacLehose, R.F.; Larson, N.; Laska, M.; Neumark-Sztainer, D. Family Food Preparation and Its Effects on Adolescent Dietary Quality and Eating Patterns. J. Adolesc. Health 2016, 59, 530–536. [Google Scholar] [CrossRef]
- Quelly, S.B. Helping with Meal Preparation and Children’s Dietary Intake: A Literature Review. J. Sch. Nurs. 2019, 35, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Möser, A.; Chen, S.E.; Jilcott, S.B.; Nayga, R.M. Associations between maternal employment and time spent in nutrition-related behaviours among German children and mothers. Public Health Nutr. 2012, 15, 1256–1261. [Google Scholar] [CrossRef]
- Bauer, K.W.; Hearst, M.O.; Escoto, K.; Berge, J.; Neumark-Sztainer, D. Parental employment and work-family stress: Associations with family food environments. Soc. Sci. Med. 2012, 75, 496–504. [Google Scholar] [CrossRef] [PubMed]
- Devine, C.M.; Farrell, T.J.; Blake, C.E.; Jastran, M.; Wethington, E.; Bisogni, C.A. Work Conditions and the Food Choice Coping Strategies of Employed Parents. J. Nutr. Educ. Behav. 2009, 41, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Datar, A.; Nicosia, N.; Shier, V. Maternal work and children’s diet, activity, and obesity. Soc. Sci. Med. 2014, 107, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Darmon, N.; Drewnowski, A. Does social class predict diet quality? Am. J. Clin. Nutr. 2008, 87, 1107–1117. [Google Scholar] [CrossRef] [PubMed]
- Murayama, N.; Ishida, H.; Yamamoto, T.; Hazano, S.; Nakanishi, A.; Arai, Y.; Nozue, M.; Yoshioka, Y.; Saito, S.; Abe, A. Household income is associated with food and nutrient intake in Japanese schoolchildren, especially on days without school lunch. Public Health Nutr. 2017, 20, 2946–2958. [Google Scholar] [CrossRef]
- Daniel, C. Economic constraints on taste formation and the true cost of healthy eating. Soc. Sci. Med. 2016, 148, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Kuhn, M.; Prettner, K.; Bloom, D.E. The macroeconomic burden of noncommunicable diseases in the United States: Estimates and projections. PLoS ONE 2018, 13, e0206702. [Google Scholar] [CrossRef]
- Devaux, M.; Graf, S.; Goryakin, Y.; Cecchini, M.; Huber, H.; Colombo, F. Obesity Update 2017; Organization for Economic Co-operation Development: Paris, France, 2017. [Google Scholar]
- Bauer, K.W.; Laska, M.N.; Fulkerson, J.A.; Neumark-Sztainer, D. Longitudinal and Secular Trends in Parental Encouragement for Healthy Eating, Physical Activity, and Dieting Throughout the Adolescent Years. J. Adolesc. Health 2011, 49, 306–311. [Google Scholar] [CrossRef] [PubMed]
- Research Office. Information Note: Overall Study Hours and Student Well-Being in Hong Kong; Legislative Council Secretariat: Hong Kong, China, 2018. [Google Scholar]
- Shek, D.T.L.; Siu, A.M.H. “UNHAPPY” Environment for Adolescent Development in Hong Kong. J. Adolesc. Health 2019, 64, S1–S4. [Google Scholar] [CrossRef] [PubMed]
- Morgan, D.L.; Ataie, J.; Carder, P.; Hoffman, K. Introducing Dyadic Interviews as a Method for Collecting Qualitative Data. Qual. Health Res. 2013, 23, 1276–1284. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Categories | Search Terms |
|---|---|
| Adolescents and family | (adolescen * OR teen * OR youth) AND (famil * OR parent * OR home) |
| Knowledge, attitudes, practices | (knowledge OR literacy OR attitude * OR perception OR belie * OR willing * OR efficacy * OR ability * OR practice*) |
| Eating habits | (diet* OR eating habit * OR eating behavio * OR eating pattern * OR food intake OR food consumption OR food choice *) |
| Types of qualitative data collection and analysis | (qualitative OR interview * OR focus group *) OR (themes OR thematic OR content analys * OR framework analys * OR template analys * OR IPA OR grounded theory OR discourse analys * OR phenomenology * OR ethnograph * OR interpretative * OR inductive * OR reflexive * OR triangulat *) |
| Study | Research Design | Sample Characteristics | Themes of the Findings on Family Factors of Adolescent KAP |
|---|---|---|---|
| Author, year, country of origin Aim(s) | Data collection method, setting, source of data, analytical method | Sample size, age and sex of adolescents (other informants indicated in brackets), sampling method | |
| Backett-Milburn, 2006, UK [42] To examine the perceptions and understandings underpinning the dietary practices in families with ‘normal’ weight and ‘overweight’ young teenagers living in poorer socio-economic circumstances | DI Home setting in socio-economically disadvantaged areas in Eastern Scotland Reported by parents/main food providers Inductive thematic analysis | n = (34) Aged 13–14 years Female = (97%) Purposive sampling by gender, BMI, and sociodemographic details | Attitudes: Family motivation (B) Practices: Food preparation and availability (F), Parenting style (F/B) |
| Backett-Milburn, 2010, UK [43] To understand more about the social and cultural conditions which might be promoting more positive dietary health and physical well-being amongst middle class families | DI School setting in relatively advantaged areas in Eastern Scotland Reported by parents Not specified (Inductive thematic analysis) | n = (35) Aged 13–14 years Female = (94%) Purposive sampling by sociodemographic details | Knowledge: Nutrition Education (F) Attitudes: Cultivation of food preference (F), Family motivation (F) Practices: Food preparation and availability (F), Time and cost (B), Parenting style (F), Parental practical knowledge and attitudes (F) |
| Banna et al., 2016, Peru [38] To understand socio-cultural influences on eating among adolescents in periurban Lima, Peru using qualitative methods | DI Home setting in low-income Spanish-speaking district Reported by adolescents Direct content analysis | n = 14 Aged 15–17 years Female = 43% Purposeful random sample from census | Knowledge: Nutrition Education (F), Child involvement (F) Attitudes: Family motivation (F) Practices: Food preparation and availability (F), Time and cost (B) |
| Bassett, 2008, Canada [44] To explore how adolescents and parents negotiate adolescents’ increasing food choice autonomy in European Canadian, Punjabi Canadian, and African Canadian families | DI, participant observation at a family meal and a grocery shopping trip with the family shopper(s) Home setting Reported by related adolescents and parents separately Thematic and constant comparative analyses | n = 47 (62) from 36 families Aged 13–19 years (mean = 41 years) Female = 72% (68%) Snowball sampling | Knowledge: Nutrition Education (F), Family illness experience (F) Attitudes: Family motivation (F) Practices: Food preparation and availability (F), Parenting style (F) |
| Berge et al., 2012, USA [35] To explore multiple family members’ perceptions of risk and protective factors for healthy eating and physical activity in the home. | Multi-family FG Community setting Reported by adolescents and family members, jointly Grounded hermeneutic approach | n = 70 (33) from 26 families Aged 8–12, 13–18 and ≥19 years (26–61 years) Female = 54% (67%) Voluntary response sampling | Attitudes: Family Health (F, Cultivation of food preference (F, Family Motivation (F) Practices: Food preparation and availability (F), Time and cost (B), Parenting style (F) |
| Brown et al., 2015, Botswana [45] To describe the factors that influence adolescent and adult perceptions and attitudes related to adolescent diet in Botswana | FG School setting Reported by unrelated adolescents and parents Not specified (low level, non-abstract, direct interpretation) | n = 12 (3) groups Aged 12–18 years Female = 6 groups (not specified) Purposive sampling by SES | Practices: Food preparation and availability (F), Time and cost (B) |
| Calvert et al., 2020, UK [46] To explore the perceptions of healthy eating behaviours and the influences on eating behaviours amongst 11-to-13-year-old secondary school students | Semi-structured same-sex FG Schools located in deprived areas of England Reported by adolescents Thematic framework analysis | n = 46 Aged 11–13 years Female = 54% Purposive sampling of selected community (low-income) | Attitudes: Family motivation (B) Practices: Food preparation and availability (B), Time and cost (B) |
| Chan et al., 2009, HK [33] To explore Chinese adolescents’ perceptions of healthy eating, their perceptions of various socializing agents shaping their eating habits, and their opinions about various regulatory measures which might be imposed to encourage healthy eating | FG Low to middle class population Reported by adolescents Comparison analysis method | n = 22 Aged 13–15 years Female = 41% Purposive sampling of selected community | Knowledge: Nutrition Education (F) Practices: Time and cost (F), Parenting style (F) |
| Christiansen et al., 2013, USA [47] To understand environmental factors influencing the food-related habits of low-income urban African American adolescents | DI, FG sessions, and direct observation Baltimore City Recreation Centers located in low-income predominantly African-American neighborhoods participating in Baltimore Healthy Eating Zones (BHEZ) Reported by adolescents Thematic analysis | n = 20 Aged 10–16 years Female = 75% Stratified, purposive sampling | Knowledge: Nutrition Education (F), Child involvement (F), Family illness experience (F) Attitudes: Family health (F), Family motivation (F/B) Practices: Food preparation and availability (F), Parenting style (F) |
| Correa et al., 2017, India and Canada [48] To understand perceptions and attitudes of Indian-origin adolescents in India and Canada that may contribute to healthy eating behaviour | FG School setting in rural and urban India, and urban Canada Reported by adolescents Thematic analysis with framework approach | n = 73 Aged 11–18 years Female = 53% Stratified, purposive sampling | Knowledge: Nutrition Education (F) Attitudes: Family motivation (B) Practices: Food preparation and availability (F/B), Time and cost (B), Parenting style (F) |
| Cullen, 2002, US [49] To assess social-environmental influences on children’s FJV and low-fat choices | FG by ethnicity School setting among low-income families Reported by adolescents and parents separately (relationship not specified) Not specified | n = 180 (40) Aged 9–12 years (mean = 36, 41, 44 years) Female = not specified (91.7–100%) Voluntary participation | Attitudes: Family motivation (F/B) Practices: Food preparation and availability (F/B), Time and cost (F/B), Parenting style (F) |
| Darling, 2015, US [39] To gain a deeper and more insightful understanding of the family food ecosystem, parental modeling, and parental indulgence, and their potential relationship to adolescent health and well-being | DI School setting Reported by parents Content analysis | n = (29) Grade 10, appx aged 15 years (35–60 years) Female: (86%) Voluntary response sampling | Knowledge: Child involvement (F/B), Family illness experience (B) Attitudes: Family health (F), Family motivation (B) Practices: Food preparation and availability (B), Time and cost (B), Parenting style (B) |
| Fielding-Singh, 2017, USA [50] To examine an overlooked contributor to family diet: fathers | DI Home setting in middle or upper class families Reported by related adolescents and parents separately Qualitative content analysis | n = 53 (56) from 44 families Aged 12–19 years Female = not specified (75%) Purposive sampling by family characteristics of interest | Attitudes: Family motivation (B) Practices: Food preparation and availability (F), Time and cost (B), Parenting style (F/B), Parental practical knowledge and attitudes (B) |
| Fielding-Singh and Wang, 2017, USA [51] To explore how mothers and adolescents across SES talk about food | DI Community setting across socioeconomic status Reported by related adolescents and parents separately Qualitative content analysis | n = 62 (62) from 62 families Aged 12–19 years Female = 61.3% (100%) Purposive and theoretical sampling by socioeconomic status | Knowledge: Nutrition Education (F), Child involvement (F/B) Attitudes: Cultivation of food preference (F/B), Family motivation (F/B) Practices: Time and cost (B), Parenting style (B). Parental practical knowledge and attitudes (F) |
| Fitzgerald et al., 2010, Ireland [52] To explore children’s and adolescents’ perspectives on the potential individual, social, environmental, and developmental factors that influence their food choices. | FG Primary and secondary schools Reported by adolescents Inductive thematic analysis | n = 29 Aged 9–18 years, mean = 13.67 Female = 55% Random sampling | Practices: Food preparation and availability (F), Time and cost (B), Parenting style (F) |
| Fuster et al., 2019, USA [36] To examine the perceived connections between culture and food practices among Latino pre-adolescents and their parents | DI Community setting Reported by parent-adolescent dyads/triads jointly Not specified (Content analysis) | n = 17 (15) from 15 families Aged 9–12 years (37.4 ± 5.1 years) Female = 47.1% (93%) Purposive sampling by ethnicity and age, and convenience sampling | Practices: Food preparation and availability (F), Time and cost (F/B), Parenting style (B), Parental practical knowledge and attitudes (F) |
| Garcia et al., 2019, USA [53] To increase understanding of the factors that influence Hispanic/Latino childhood obesity through an intergenerational lens including children, parents/caregivers, and grandparents. | Semi-structured FG Community based organizations in Los Angeles County Reported by adolescents Thematic analysis | n = 22 Aged 10–17 years Female = 52%, one unknown Not specified | Practices: Food preparation and availability (B), Time and cost (B), Parenting style (F/B) |
| Goh, 2009, US [54] To explore adolescent, parent, and community stakeholder perspectives on barriers to healthy eating and physical activity, and intervention ideas to address adolescent obesity | FG and DI School setting Reported by related adolescents, parents and community members separately Not specified | n = 119 (63) Mean age = 12 years Female = 61% (84%) Not specified | Knowledge: Child involvement (F) Attitudes: Family health (F), Family motivation (B) Practices: Food preparation and availability (B), Time and cost (B), Parental practical knowledge and attitudes (B) |
| Gray, 2015, Canada [55] To examine the eating behaviours and nutrition knowledge of young women in an Ontario secondary school | DI Private room within school Reported by adolescents Not specified (Thematic analysis) | n = 20 Aged 14–17 years Female = 100% Not specified | Knowledge: Nutrition Education (F/B), Child involvement (F), Family illness experience (F) Attitudes: Family motivation (F) Practices: Food preparation and availability (F), Parenting style (F) |
| Gunther et al., 2019, USA [56] To identify practices that parents use to influence early adolescents’ food choices during independent eating occasions (iEOs) from parent and child perspectives. | DI Community setting among low income families Reported by related adolescents and parents separately Directed content analysis | n = 44 (49) Aged 10–13 years (26–65 years) Female = 56.8% (89.8%) Purposive sampling by race and ethnicity, and convenience sampling | Knowledge: Nutrition Education (F) Attitudes: Family motivation (F) Practices: Food preparation and availability (F), Parenting style (F) |
| Hattersley, 2009, Australia [57] To explore adolescents’ and parents’ perceptions, attitudes, and interactions in regards to screen time (ST) and sugary drink (SD) consumption | Semi-structured FG School setting in low to middle SES areas Reported by unrelated adolescents and parents Thematic analysis | n = 31 (32) in 9 FG Aged 13–16 years (mean = 46 years for mothers, 43 years for fathers) Females = 42% (63%) Purposive for low-middle SES | Knowledge: Nutrition Education (F) Attitudes: Family motivation (F) Practices: Food preparation and availability (F), Parenting style (F) |
| Heidelberger and Smith, 2015, USA [58] To pilot Photovoice methodology with low-income, urban 9- to 13-year-olds to gain insight about their food environment and to determine whether this methodology was engaging and acceptable to them | DI Afterschool programs for youths in Supplemental Nutrition Assistance Program (SNAP)-eligible low income households Reported by adolescents Open coding method | n = 29 Aged 9–13 years, mean = 11 Female = 31% Not specified | Knowledge: Nutrition Education (F) Attitudes: Cultivation of food preference (F) Practices: Food preparation and availability (F), Parental practical knowledge and attitudes (F) |
| Holsten, 2012, US [59] To explore children’s food choices in the home with particular attention to environmental influences | DI School setting Reported by adolescents Grounded theory and content analysis | n = 47 Aged 11–14 years Female = 51% Maximum variation sampling by race, ethnicity, household income, and BMI | Attitudes: Cultivation of food preference (F), Family motivation (F/B) Practices: Food preparation and availability (F/B), Time and cost (F/B), Parenting style (F/B), Parental practical knowledge and attitudes (F) |
| Islam et al., 2019, Bangladesh [60] To explore adolescents’ and mothers’ perception of broader sociocultural aspects that sculpt the food choices, eating habits and physical activity behaviours of adolescents in Matlab, Bangladesh | FG Home setting in poor, rural areas Reported by related adolescents and parents separately Inductive thematic analysis | n = 4 (2) groups with 6–8 participants per group Aged 14–17 years Female = 2 groups (2) Purposive sampling | Attitudes: Cultivation of food preference (F) Practices: Food preparation and availability (F), Time and cost (B), Parenting style (F), Parental practical knowledge and attitudes (B) |
| Kaplan et al., 2006, USA [37] To explore how youth, parents, and grandparents discuss issues related to eating healthfully and unhealthfully and to identify intergenerational strategies for educators to improve this communication. | Semi-structured FG Community setting among low-income populations Reported by adolescents, parents and grandparents jointly Not specified (Content and ethnographic analysis) | n = 21 (23) from 17 families Aged 10–13 years Female = not specified (not specified) Purposive site selection and voluntary response sampling | Knowledge: Child involvement (F) Attitudes: Family health (F), Cultivation of food preference (F), Family motivation (F) Practices: Food preparation and availability (F), Time and cost (B), Parenting style (F/B), Parental practical knowledge and attitudes (B) |
| Kumar et al., 2016, USA [61] To enable community members to discuss their perceptions of eating habits and physical activity in relation to sixth, seventh, and eighth graders, and reveal facilitators and barriers to healthy eating behaviour and physical activity engagement. | FG Middle school among rural, limited-resources adolescents Reported by related adolescents, parents and teachers separately Not specified | n = 6 groups with 6–8 each (13) 6th grade to 8th grade Female = not specified (not specified) Voluntary response sampling in selected school | Knowledge: Nutrition Education (F) Practices: Food preparation and availability (F), Time and cost (B), Parenting style (F) |
| Monge-Rojas et al., 2005, Costa Rica [62] To assess the perceptions of rural and urban Costa Rican adolescents about their diet and the factors they consider significant to healthful eating. | FG School setting Reported by adolescents Content analysis | n = 108 Aged 12–18 years Female = unknown, both sex Random sampling | Attitudes: Cultivation of food preference (F) Practices: Food preparation and availability (F), Parental practical knowledge and attitudes (B) |
| Neumark-Sztainer et al., 2000, USA [63] To (1) increase our knowledge about family meal patterns of adolescents, (2) identify factors that adolescents perceive as reasons for not eating meals with their family, and (3) assess adolescents’ perceptions on whether they eat more healthful foods at family meals than in other eating situations. | FG School setting Reported by adolescents Content analysis | n = 141 Age mean = 12.6 years, 16 years Female = 61% Not specified | Practices: Food preparation and availability (F/B), Time and cost (B), Parenting style (F/B), Parental practical knowledge and attitudes (F/B) |
| O’dougherty et al., 2006, US [64] To gain insight into parents’ perceptions of the food preferences of their young adolescents, and their negotiating and decision-making strategies around food purchasing and meals | FG School setting among nonwhite and immigrant parents with generally low socioeconomic status Reported by parents Not specified | n = (52) Aged 11–15 years (mean = 37.4 years) Female: (90%) Voluntary response sampling | Attitudes: Cultivation of food preference (F) Practices: Food preparation and availability (F), Time and cost (F/B), Parenting style (F/B) |
| Ortega-Avila et al., 2019, Mexico [40] To explore adolescents’ perceptions of how the home environment promotes the intake of sugar-sweetened beverages (SSBs) and to identify the potential environmental cues that trigger SSB intake at home | DI Home setting or in public spaces Reported by adolescents Thematic analysis using framework approach | n = 29 Aged 15–19 years Female = 55% Purposive sampling by age and SSB intake | Attitudes: Cultivation of food preference (B), Family motivation (B) Practices: Food preparation and availability (B), Time and cost (B), Parenting style (B), Parental practical knowledge and attitudes (F/B) |
| Park et al., 2014, South Korea [65] To identify physical and social environments that influence the eating habits of adolescents living in urban South Korea | DI and FG Schools in urban areas Reported by parents and teachers Not specified (Deductive thematic analysis) | n = (9) Aged 10–16 years Female = (not specified) Snowball sampling | Knowledge: Child involvement (F) Attitudes: Cultivation of food preference (F) Practices: Food preparation and availability (F), Time and cost (B) |
| Pinard et al., 2015, USA [66] To understand influential factors related to family feeding practices among low-income English and Spanish speaking families with school-aged children when eating food away from home (FAFH) | DI Community setting Reported by related parent-adolescent separately Not specified | n = 20 (20) Aged 8–13 years, mean = 10.5 (<21–44 years) Female = 35% (80%) Voluntary response and snowball followed by purposive sampling by dominant language | Knowledge: Nutrition Education (F), Child involvement (F) Attitudes: Family motivation (F) Practices: Food preparation and availability (F), Time and cost (F), Parenting style (F/B) |
| Povey et al., 2016, UK [67] To explore the beliefs towards eating fruit and vegetables among children aged 9–11 years in a primary school setting | DI School setting in low SE group Reported by adolescents Inductive thematic analysis | n = 11 Aged 9–11 years, mean = 10 Females = 73% Convenience sampling | Knowledge: Nutrition Education (F) Practices: Food preparation and availability (B), Time and cost (F/B), Parenting style (F/B), Parental practical knowledge and attitudes (F) |
| Power et al., 2010, US [68] To provide insight into the development of a comprehensive program for the prevention of adolescent obesity: the Teen Eating and Activity Mentoring in Schools project | FG School setting from middle-class families Reported by unrelated adolescents, parents and teachers Not specified | n = 16 (6) Aged 12–14 years Female = 69% (67%) Not specified | Attitudes: Family motivation (F/B) Practices: Food preparation and availability (F/B), Time and cost (B), Parenting style (F/B) |
| Rakhshanderou et al., 2014, Iran [69] To explore the determinants of fruit and vegetable consumption among Tehranian adolescents in 2012 | DI School setting Reported by adolescents Qualitative content analysis | n = 31 Aged 11–14 years Female = 48% Convenience sampling | Attitudes: Family health (F), Family motivation (F/B) Practices: Food preparation and availability (F/B), Time and cost (F/B), Parenting style (F/B), Parental practical knowledge and attitudes (F/B) |
| Rathi et al., 2016, India [70] To investigate adolescents’, parents’, teachers’, and school principals’ perceptions of the main influences on adolescent eating behaviours | DI School setting Reported by related adolescents, parents, teachers and principals separately Thematic analysis | n = 15 (15) Aged 14–15 years Female = 67% (93%) Purposive sampling for participating schools | Knowledge: Nutrition Education (F) Attitudes: Cultivation of food preference (F), Family motivation (F) Practices: Food preparation and availability (F), Time and cost (B), Parenting style (F/B) |
| Rawlins et al., 2013, UK [71] To explore both individual and family perceptions, intentions and beliefs relating to healthy lifestyles | FG and DI School and community setting Reported by related adolescents and their parents separately Thematic analysis | n = 70 (43) Aged 8–13 years Female = 56% (79%) Purposive sampling by ethnicity and age | Knowledge: Child involvement (F) Attitudes: Family motivation (F) Practices: Food preparation and availability (F), Time and cost (B), Parenting style (F/B), Parental practical knowledge and attitudes (B) |
| Rodriguez-Perez et al., 2019, Puerto Rico [72] To identify barriers that prevent healthy eating practices in Puerto Rican early adolescents (EAs). | FG Underserved community in both urban and rural settings Reported by related adolescents and parents/caregivers separately Content analysis | n = 52 (17) Aged 12–14 years Female = 67% (76%) Purposive sampling of sites by socioeconomic status | Attitudes: Family motivation (B) Practices: Time and cost (B), Parenting style (B), Parental practical knowledge and attitudes (F/B) |
| Roth-Yousey, 2012, US [73] To understand parent beverage expectations for early adolescents (EAs) by eating occasion at home and in various settings | FG School and community settings in low-income neighborhoods Reported by parents/ caregivers Not specified | n = (49) Aged 10–13 years Female = (86%) Purposive sampling by BMI | Attitudes: Family motivation (B) Practices: Food preparation and availability (F), Time and cost (F) |
| Sedibe et al., 2014, South Africa [41] To investigate the narratives pertaining to dietary and physical activity practices by female adolescents in Soweto. | Duo DI School setting Reported by adolescents Thematic analysis | n = 58 Aged 15.3–21.6 years (mean = 18) Female = 100% Voluntary response sampling | Practices: Food preparation and availability (B), Time and cost (B) |
| Sharif-Ishak et al., 2020, Malaysia [74] To explore the concepts of healthy eating and to identify the barriers and facilitating factors for dietary behaviour change in adolescents. | FG School setting Reported by adolescents Thematic analysis | n = 72 Aged 13–14 years Female = 48.6% Randomly selected schools followed by voluntary response sampling | Knowledge: Nutrition Education (F) Attitudes: Family motivation (B) Practices: Food preparation and availability (F/B), Parenting style (F) |
| Silva et al., 2015, Brazil [75] To explore how adolescents at a school in the interior of the State of Pernambuco, Brazil, perceive healthy eating | DI School setting in low HDI, agricultural region Reported by adolescents Lexical analysis | n = 40 Aged 10–14 years Female = 62.5% Purposive sampling | Attitudes: Family motivation (F/B) Practices: Food preparation and availability (F), Time and cost (B), Parenting style (F) |
| Siu et al., 2019, Hong Kong [34] To investigate the barriers to adopting healthy eating habits among secondary school students from low-income families in Hong Kong | FG School setting in a low-income district Reported by adolescents Thematic content analysis | n = 30 Secondary 1 and 4 Female = 50% Purposive sampling by gender, lunchbox practice, and CSSA assistance | Practices: Food preparation and availability (F), Time and cost (B), Parental practical knowledge and attitudes (B) |
| Snethen et al., 2007, US [76] To understand one Latino community’s perspectives about childhood overweight within this high-risk ethnic group | FG Community setting Reported by unrelated adolescents and parents Thematic analysis | n = 12 (24) Aged 10–12 years Female = 33% (50%) Convenience sampling | Practices: Food preparation and availability (B), Time and cost (B), Parenting style (B) |
| Steeves et al., 2016, US [77] To provide in-depth information on the social roles that youths’ parents and friends play related to eating and physical activity behaviours and to explore the impact of other social relationships on youths’ eating and physical activity behaviours. | DI Community setting in low-income neighbourhoods Reported by related adolescents and parents separately Direct content analysis | n = 38 (10) Aged 9–15 years Female = 42% (80%) Purposive sampling by genders, ages and neighbourhood locations | Knowledge: Nutrition Education (F) Attitudes: Family motivation (F) Practices: Food preparation and availability (F), Time and cost (B), Parenting style (F), Parental practical knowledge and attitudes (B) |
| Tiedje et al., 2014, USA [78] To describe the meanings of food, health, and wellbeing through the reported dietary preferences, beliefs, and practices of adults and adolescents from four immigrant and refugee communities in the Midwestern United States. | FG Immigrant and refugee communities Reported by adolescents Content analysis and grounded theory | n = 73 Aged 11–18 years Female = 53% Purposive sampling by age and gender | Attitudes: Family motivation (F/B) Practices: Food preparation and availability (F/B), Time and cost (B), Parenting style (F), Parenting style (B) |
| Verstraeten et al., 2014, Ecuador [79] To identify factors influencing eating behaviour of Ecuadorian adolescents—from the perspective of parents, school staff, and adolescents—to develop a conceptual framework for adolescents’ eating behaviour. | Semi-structured FG School setting in low- and middle-income countries Reported by unrelated adolescents, parents and school staff Deductive thematic content analysis | n = 80 (32) Aged 11–15 years (mean = 41.2 years) Female = 52.1% (75%) Convenience sampling | Attitudes: Family motivation (B) Practices: Food preparation and availability (F), Time and cost (F/B), Parenting style (B) |
| Zhang et al., 2018, USA [80] To explore Latino fathers’ perspectives and parenting experiences regarding early adolescents’ eating, physical activity, and screen-time behaviours using the focus group method. | FG Community setting Reported by fathers Grounded theory | n = (26) Aged 10–14 years (33–53 years) Female = (0%) Convenience sampling | Knowledge: Nutrition Education (F), Child involvement (F) Attitudes: Family motivation (F) Practices: Food preparation and availability (F), Time and cost (F/B), Parenting style (F/B), Parental practical knowledge and attitudes (F) |
| Author, Year | Q1. Was There a Clear Statement of the Aims of the Research? | Q2. Is a Qualitative Methodology Appropriate? | Q3. Was the Research Design Appropriate to Address the Aims of the Research? | Q4. Was the Recruitment Strategy Appropriate to the Aims of the Study? | Q5. Was the Data Collected in a Way that Addressed the Research Issue? | Q6. Has the Relationship between Researcher and Participants Been Adequately Considered? | Q7. Have Ethical Consideration Been Taken into Consideration? | Q8. Was the Data Analysis Sufficiently Rigorous? | Q9. Is There a Clear Statement of Findings? | Q10. How Valuable Is the Research? | Quality Score (Max = 20) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Backett-Milburn, 2006 [42] | 2 | 2 | 1 | 2 | 1 | 1 | 1 | 2 | 2 | 2 | 16 |
| Backett-Milburn, 2010 [43] | 2 | 2 | 1 | 2 | 1 | 0 | 2 | 2 | 1 | 1 | 14 |
| Banna et al., 2016 [38] | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 20 |
| Bassett, 2008 [44] | 2 | 2 | 1 | 1 | 1 | 2 | 2 | 2 | 2 | 2 | 17 |
| Berge et al., 2012 [35] | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 20 |
| Brown et al., 2015 [45] | 2 | 2 | 1 | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 18 |
| Calvert et al., 2019 [46] | 2 | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 19 |
| Chan et al., 2009 [33] | 2 | 2 | 2 | 0 | 2 | 0 | 1 | 1 | 2 | 2 | 14 |
| Christiansen et al., 2013 [47] | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 19 |
| Correa et al., 2017 [48] | 2 | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 18 |
| Cullen, 2002 [49] | 2 | 2 | 1 | 1 | 2 | 1 | 1 | 1 | 2 | 2 | 15 |
| Darling, 2015 [39] | 2 | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 18 |
| Fielding-Singh, 2017 [50] | 2 | 2 | 1 | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 18 |
| Fielding-Singh and Wang, 2017 [51] | 2 | 2 | 1 | 2 | 1 | 1 | 2 | 2 | 2 | 2 | 17 |
| Fitzgerald et al., 2010 [52] | 2 | 2 | 1 | 1 | 2 | 1 | 2 | 2 | 2 | 2 | 17 |
| Fuster et al., 2019 [36] | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 19 |
| Garcia et al., 2019 [53] | 2 | 2 | 1 | 1 | 2 | 0 | 2 | 2 | 2 | 2 | 16 |
| Goh, 2009 [54] | 2 | 2 | 2 | 1 | 2 | 1 | 2 | 2 | 2 | 2 | 18 |
| Gray, 2015 [55] | 2 | 2 | 2 | 2 | 1 | 0 | 2 | 2 | 2 | 2 | 17 |
| Gunther et al., 2019 [56] | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 20 |
| Hattersley, 2009 [57] | 2 | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 19 |
| Heidelberger & Smith, 2015 [58] | 2 | 2 | 1 | 0 | 1 | 1 | 1 | 2 | 2 | 2 | 14 |
| Holsten, 2012 [59] | 2 | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 19 |
| Islam et al., 2019 [60] | 2 | 2 | 1 | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 18 |
| Kaplan et al., 2006 [37] | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 20 |
| Kumar et al., 2016 [61] | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 20 |
| Monge-Rojas et al., 2005 [62] | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 19 |
| Neumark-Sztainer et al., 2000 [63] | 2 | 2 | 2 | 2 | 1 | 1 | 1 | 2 | 2 | 2 | 17 |
| O’Dougherty et al., 2006 [64] | 2 | 2 | 1 | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 13 |
| Ortega-Avila et al., 2019 [40] | 2 | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 1 | 2 | 18 |
| Park et al., 2014 [65] | 2 | 2 | 1 | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 18 |
| Pinard et al., 2015 [66] | 2 | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 19 |
| Povey et al., 2016 [67] | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 20 |
| Power et al., 2010 [68] | 2 | 2 | 2 | 1 | 1 | 1 | 2 | 2 | 2 | 2 | 17 |
| Rakhshanderou et al., 2014 [69] | 2 | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 18 |
| Rathi et al., 2016 [70] | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 2 | 19 |
| Rawlins et al., 2013 [71] | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 19 |
| Rodriguez-Perez et al., 2019 [72] | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 20 |
| Roth-Yousey, 2012 [73] | 2 | 2 | 1 | 1 | 1 | 2 | 1 | 2 | 2 | 2 | 16 |
| Sedibe et al., 2014 [41] | 2 | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 19 |
| Sharif-Ishak et al., 2020 [74] | 2 | 2 | 1 | 1 | 2 | 1 | 2 | 2 | 1 | 2 | 16 |
| Silva et al., 2015 [75] | 2 | 2 | 2 | 1 | 2 | 1 | 2 | 2 | 1 | 2 | 17 |
| Siu et al., 2018 [34] | 2 | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 18 |
| Snethen et al., 2007 [76] | 2 | 2 | 2 | 1 | 2 | 1 | 2 | 2 | 2 | 2 | 18 |
| Steeves et al., 2016 [77] | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 19 |
| Tiedje et al., 2014 [78] | 2 | 2 | 1 | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 18 |
| Verstraeten et al., 2014 [79] | 2 | 2 | 2 | 2 | 2 | 1 | 1 | 2 | 2 | 2 | 18 |
| Zhang et al., 2018 [80] | 2 | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 19 |
| KAP Constructs | Family Influence | ||
|---|---|---|---|
| Facilitators | Barriers | ||
| Adolescent Knowledge | Nutrition education | Education on nutrition benefits [38,43,51,56,66,67,70,74,77,80] Education on undesirable consequences of unhealthy eating [33,44,47,55] Advice on healthy food choice [38,39,43,44,48,55,56,57,58,61,66,70,71,77] Fostering cooking skills [38,58,77,80] | Inconsistent message between parents and school [55] |
| Child involvement | Education during mealtimes and grocery shopping [38,51,55,65,66,71,80] Good communication with adolescents (e.g., open discussion, fun style) [37,39,47,54,55,66] | Adolescents having minimal responsibility in diet-related tasks [39] Limited ability for food discussion in parents with poor role model [51] | |
| Family illness experience | Emphasis on diet-related health risks experienced by family members with health problems [44,47,55] | Health-related topics as a taboo in families with illnesses [39] | |
| Adolescent Attitudes | Family health | Perceived importance of diet-related health risks in family members with health problems [37,39,47,54] Modeling of positive outcome of healthy eating [35,69] | |
| Cultivation of preference | Cultivate taste preference for healthy food [35,37,43,51,58,59,62,64,65,70] Reducing temptation of unhealthy foods by limiting sedentary time [43] Home cooking perceived as more hygienic than street foods [60] | Family preference on low cost/ unhealthy foods [40,51] | |
| Family motivation | Family modeling of healthy eating habits [35,37,43,44,47,55,56,57,59,66,68,70,77,80] Encouragement and praise [35,38,44,49,51,66,68,69,71,75,77,80] Parental concern on adolescent’s health [38,56,57,66,78] Adolescent acting as a role model in the family [77,78] | Family modeling of unhealthy eating habits [39,40,46,47,48,49,50,54,59,68,69,72,73,74,79] Lack of parental concern on adolescent dietary issues (e.g., body weight is not important for the young) [42,50,51,78,79] Busy parents lacking time for encouragement [75] | |
| Adolescent Practices | Food preparation and availability | Provision of healthy home meals [33,34,35,36,38,42,43,44,48,50,61,62,63,66,70,71,75,77,78,80] Home availability of healthy food/ unavailability of unhealthy foods [36,37,39,40,42,43,44,45,47,48,49,50,52,55,56,57,60,61,64,65,66,67,68,69,70,73,74,77,79,80] | Unhealthy home meals [39,54,63,76,78] Home availability of unhealthy/ unavailability of healthy foods [40,41,46,48,49,53,59,67,68,69,74,78] |
| Time and cost | Controlling access (e.g., increased access to ready-to-eat FV and healthier drinks, storing unhealthy snacks out-of-reach) [49,56,57,64,66,67,69,73,80] Limiting the budget of junk food [36,59,66,79] | Convenience of packaged and takeaway foods over home cooking [35,36,37,39,43,45,48,50,52,53,54,59,61,63,64,65,68,70,76,78,79,80] and time barrier for preparing FV and healthy beverages [40,67,69] Financial preferences on affordable but unhealthy foods [34,35,36,37,38,41,45,46,48,49,51,54,60,61,66,67,69,72,75,77,78,79,80] Easy accessibility of unhealthy food shops and restaurants [36,72] | |
| Parenting style | Rules and monitoring of mealtimes [37,44,49,52,53,61,63,77] and snacking [33,37,42,43,47,50,52,56,59,64,67,68,77,80] Authoritative practices (e.g., reasoning, regular meal schedule) [35,37,43,44,48,49,52,55,57,59,60,64,66,69,70,71,74,75,80] Child involvement with limited/ guided choices [37,44,59,64,80] Grocery shopping without adolescents to avoid their request on unhealthy foods [44] | Unstructured practices (e.g., accommodating family taste preference, lack of monitoring at mealtimes [37,42,64,66,68,78,79] and snacking [39,40,50,51,53,59,66,67,69,76,79,80] Restriction on snacking [70,80] Treats and bribes of unhealthy foods by family members [36,50] Atmosphere of meals with dissatisfying family relation [63] | |
| Parental practical knowledge and attitudes | Healthy cooking skills/ varying food presentation [36,43,59,66,67,72,80] Healthy home food availability by health-conscious parents [40,51,58,59,63] | Lack of nutrition knowledge to make healthy choices or provide appropriate amounts [34,37,40,50,54,71,72,77] Lack of cooking skills to provide healthy and tasty meals with variety [60,62,63] Lack of parental concern on healthy eating [50] | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, K.S.N.; Chen, J.Y.; Ng, M.Y.C.; Yeung, M.H.Y.; Bedford, L.E.; Lam, C.L.K. How Does the Family Influence Adolescent Eating Habits in Terms of Knowledge, Attitudes and Practices? A Global Systematic Review of Qualitative Studies. Nutrients 2021, 13, 3717. https://doi.org/10.3390/nu13113717
Liu KSN, Chen JY, Ng MYC, Yeung MHY, Bedford LE, Lam CLK. How Does the Family Influence Adolescent Eating Habits in Terms of Knowledge, Attitudes and Practices? A Global Systematic Review of Qualitative Studies. Nutrients. 2021; 13(11):3717. https://doi.org/10.3390/nu13113717
Chicago/Turabian StyleLiu, Kiki S. N., Julie Y. Chen, Michelle Y. C. Ng, Maegan H. Y. Yeung, Laura E. Bedford, and Cindy L. K. Lam. 2021. "How Does the Family Influence Adolescent Eating Habits in Terms of Knowledge, Attitudes and Practices? A Global Systematic Review of Qualitative Studies" Nutrients 13, no. 11: 3717. https://doi.org/10.3390/nu13113717
APA StyleLiu, K. S. N., Chen, J. Y., Ng, M. Y. C., Yeung, M. H. Y., Bedford, L. E., & Lam, C. L. K. (2021). How Does the Family Influence Adolescent Eating Habits in Terms of Knowledge, Attitudes and Practices? A Global Systematic Review of Qualitative Studies. Nutrients, 13(11), 3717. https://doi.org/10.3390/nu13113717