
Dietary Soy Consumption and Cardiovascular Mortality among Chinese People with Type 2 Diabetes

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
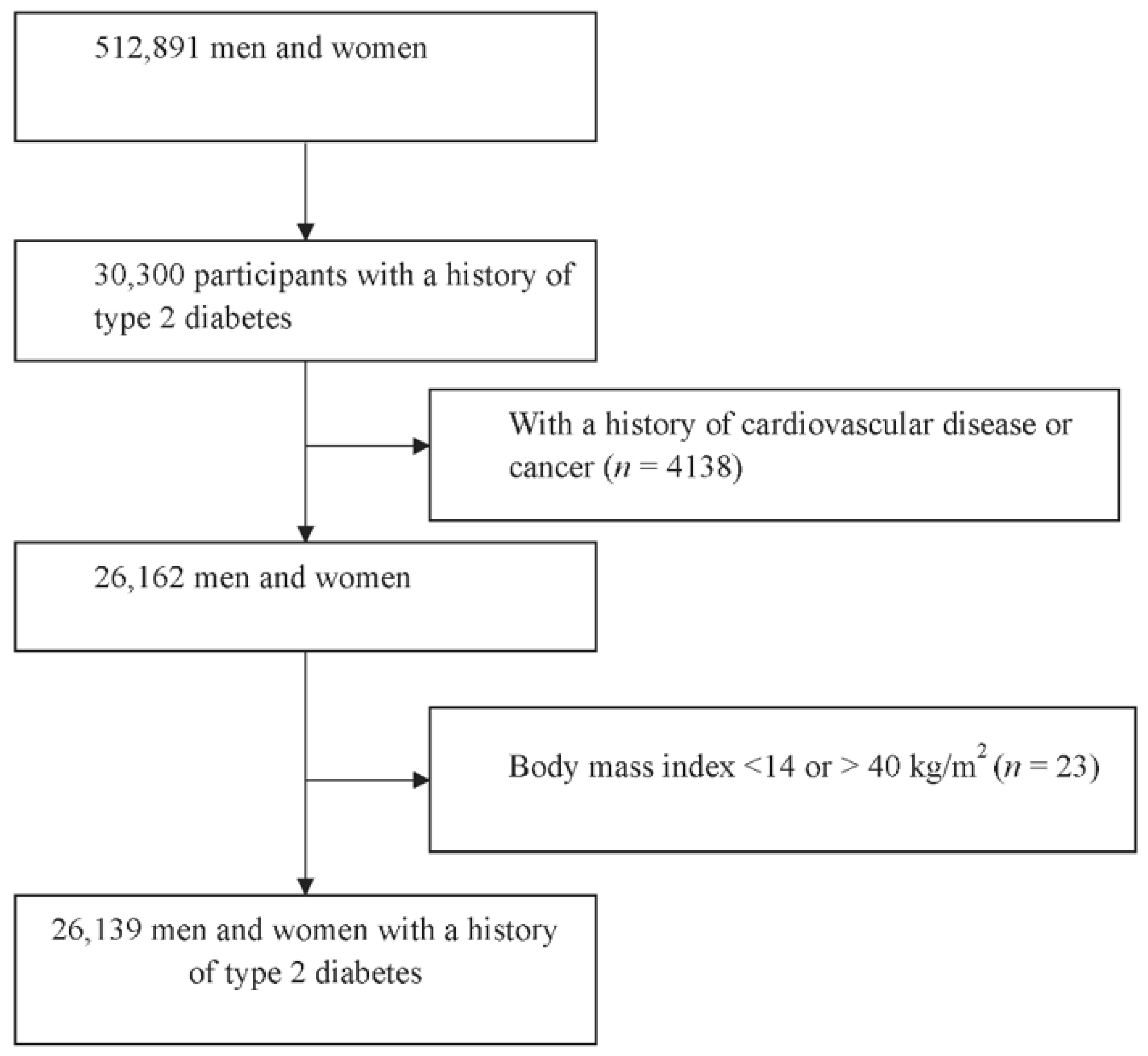
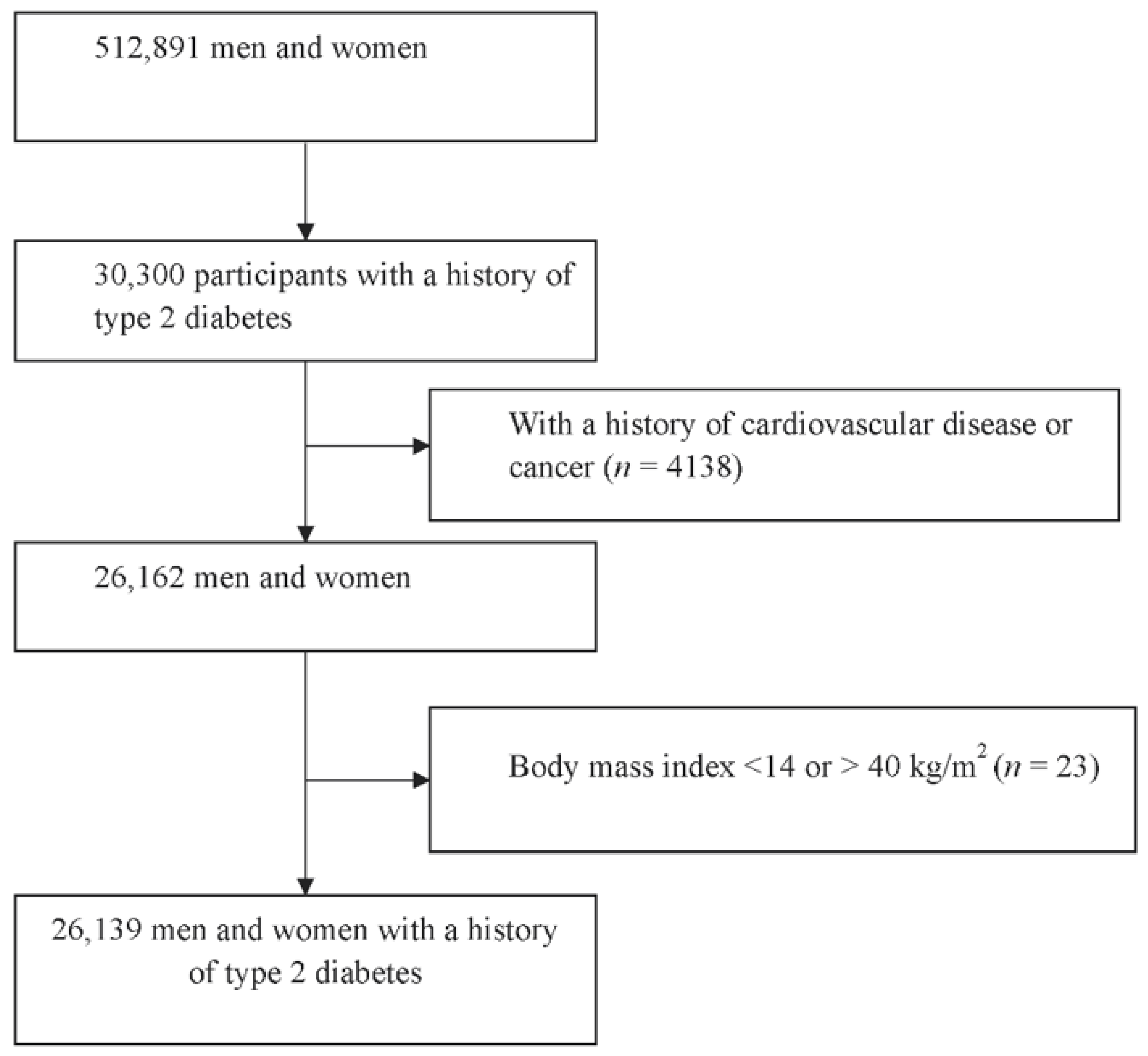
2.1. Study Population
2.2. Assessment of Diet
2.3. Assessment of Covariates
2.4. Follow-Up
2.5. Statistical Analysis
2.6. Patient and Public Involvement
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Rizzo, G.; Baroni, L. Soy, Soy Foods and Their Role in Vegetarian Diets. Nutrients 2018, 10, 43. [Google Scholar] [CrossRef] [Green Version]
- Dong, J.Y.; Tong, X.; Wu, Z.W.; Xun, P.C.; He, K.; Qin, L.Q. Effect of soya protein on blood pressure: A meta-analysis of randomised controlled trials. Br. J. Nutr. 2011, 106, 317–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tokede, O.A.; Onabanjo, T.A.; Yansane, A.; Gaziano, J.M.; Djoussé, L. Soya products and serum lipids: A meta-analysis of randomised controlled trials. Br. J. Nutr. 2015, 114, 831–843. [Google Scholar] [CrossRef]
- Beavers, D.P.; Beavers, K.M.; Miller, M.; Stamey, J.; Messina, M.J. Exposure to isoflavone-containing soy products and endothelial function: A Bayesian meta-analysis of randomized controlled trials. Nutr. Metab. Cardiovasc. Dis. NMCD 2012, 22, 182–191. [Google Scholar] [CrossRef]
- Kokubo, Y.; Iso, H.; Ishihara, J.; Okada, K.; Inoue, M.; Tsugane, S. Association of dietary intake of soy, beans, and isoflavones with risk of cerebral and myocardial infarctions in Japanese populations: The Japan Public Health Center-based (JPHC) study cohort I. Circulation 2007, 116, 2553–2562. [Google Scholar] [CrossRef] [Green Version]
- Ma, L.; Liu, G.; Ding, M.; Zong, G.; Hu, F.B.; Willett, W.C.; Rimm, E.B.; Manson, J.E.; Sun, Q. Isoflavone Intake and the Risk of Coronary Heart Disease in US Men and Women: Results From 3 Prospective Cohort Studies. Circulation 2020, 141, 1127–1137. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Chen, Y.; Xu, T.; Yu, Y.; Huang, T.; Hu, X.; Li, D. Systematic review and meta-analysis of soy products consumption in patients with type 2 diabetes mellitus. Asia Pac. J. Clin. Nutr. 2011, 20, 593–602. [Google Scholar] [PubMed]
- Arsenault, B.J.; Boekholdt, S.M.; Kastelein, J.J. Lipid parameters for measuring risk of cardiovascular disease. Nat. Rev. Cardiol. 2011, 8, 197–206. [Google Scholar] [CrossRef]
- Talaei, M.; Koh, W.P.; van Dam, R.M.; Yuan, J.M.; Pan, A. Dietary soy intake is not associated with risk of cardiovascular disease mortality in Singapore Chinese adults. J. Nutr. 2014, 144, 921–928. [Google Scholar] [CrossRef] [Green Version]
- Chen, Z.; Chen, J.; Collins, R.; Guo, Y.; Peto, R.; Wu, F.; Li, L. China Kadoorie Biobank collaborative, g. China Kadoorie Biobank of 0.5 million people: Survey methods, baseline characteristics and long-term follow-up. Int. J. Epidemiol. 2011, 40, 1652–1666. [Google Scholar] [CrossRef] [Green Version]
- Chen, Z.; Lee, L.; Chen, J.; Collins, R.; Wu, F.; Guo, Y.; Linksted, P.; Peto, R. Cohort profile: The Kadoorie Study of Chronic Disease in China (KSCDC). Int. J. Epidemiol. 2005, 34, 1243–1249. [Google Scholar] [CrossRef] [Green Version]
- Wei, Y.; Lv, J.; Guo, Y.; Bian, Z.; Gao, M.; Du, H.; Yang, L.; Chen, Y.; Zhang, X.; Wang, T.; et al. Soy intake and breast cancer risk: A prospective study of 300,000 Chinese women and a dose-response meta-analysis. Eur. J. Epidemiol. 2020, 35, 567–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, G.; Hu, J.; Rao, K.Q.; Ma, J.; Rao, C.; Lopez, A.D. Mortality registration and surveillance in China: History, current situation and challenges. Popul. Health Metr. 2005, 3, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, N.; Wu, X.; Zhuang, W.; Xia, L.; Chen, Y.; Zhao, R.; Yi, M.; Wan, Q.; Du, L.; Zhou, Y. Soy and Isoflavone Consumption and Multiple Health Outcomes: Umbrella Review of Systematic Reviews and Meta-Analyses of Observational Studies and Randomized Trials in Humans. Mol. Nutr. Food Res. 2020, 64, e1900751. [Google Scholar] [CrossRef] [PubMed]
- Katagiri, R.; Sawada, N.; Goto, A.; Yamaji, T.; Iwasaki, M.; Noda, M.; Iso, H.; Tsugane, S. Association of soy and fermented soy product intake with total and cause specific mortality: Prospective cohort study. BMJ 2020, 368, m34. [Google Scholar] [CrossRef] [Green Version]
- Nagata, C.; Wada, K.; Tamura, T.; Konishi, K.; Goto, Y.; Koda, S.; Kawachi, T.; Tsuji, M.; Nakamura, K. Dietary soy and natto intake and cardiovascular disease mortality in Japanese adults: The Takayama study. Am. J. Clin. Nutr. 2017, 105, 426–431. [Google Scholar] [CrossRef] [Green Version]
- Zamora-Ros, R.; Jiménez, C.; Cleries, R.; Agudo, A.; Sánchez, M.J.; Sánchez-Cantalejo, E.; Molina-Montes, E.; Navarro, C.; Chirlaque, M.D.; María Huerta, J.; et al. Dietary flavonoid and lignan intake and mortality in a Spanish cohort. Epidemiology 2013, 24, 726–733. [Google Scholar] [CrossRef]
- Azadbakht, L.; Atabak, S.; Esmaillzadeh, A. Soy protein intake, cardiorenal indices, and C-reactive protein in type 2 diabetes with nephropathy: A longitudinal randomized clinical trial. Diabetes Care 2008, 31, 648–654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azadbakht, L.; Shakerhosseini, R.; Atabak, S.; Jamshidian, M.; Mehrabi, Y.; Esmaill-Zadeh, A. Beneficiary effect of dietary soy protein on lowering plasma levels of lipid and improving kidney function in type II diabetes with nephropathy. Eur. J. Clin. Nutr. 2003, 57, 1292–1294. [Google Scholar] [CrossRef] [Green Version]
- Pipe, E.A.; Gobert, C.P.; Capes, S.E.; Darlington, G.A.; Lampe, J.W.; Duncan, A.M. Soy protein reduces serum LDL cholesterol and the LDL cholesterol:HDL cholesterol and apolipoprotein B:apolipoprotein A-I ratios in adults with type 2 diabetes. J. Nutr. 2009, 139, 1700–1706. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.M.; Zhang, Y.B.; Chi, M.H. Soy Protein Supplementation Reduces Clinical Indices in Type 2 Diabetes and Metabolic Syndrome. Yonsei Med. J. 2016, 57, 681–689. [Google Scholar] [CrossRef] [Green Version]
- Haffner, S.M.; American Diabetes, A. Management of dyslipidemia in adults with diabetes. Diabetes Care 2003, 26 (Suppl. 1), S83–S86. [Google Scholar] [CrossRef] [PubMed]
- Kengne, A.P.; Patel, A.; Barzi, F.; Jamrozik, K.; Lam, T.H.; Ueshima, H.; Gu, D.F.; Suh, I.; Woodward, M. Systolic blood pressure, diabetes and the risk of cardiovascular diseases in the Asia-Pacific region. J. Hypertens. 2007, 25, 1205–1213. [Google Scholar] [CrossRef] [PubMed]
- Perez-Ros, P.; Navarro-Flores, E.; Julian-Rochina, I.; Martinez-Arnau, F.M.; Cauli, O. Changes in Salivary Amylase and Glucose in Diabetes: A Scoping Review. Diagnostics 2021, 11, 453. [Google Scholar] [CrossRef]
- Atkinson, C.; Frankenfeld, C.L.; Lampe, J.W. Gut bacterial metabolism of the soy isoflavone daidzein: Exploring the relevance to human health. Exp. Biol. Med. 2005, 230, 155–170. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Shu, X.O.; Gao, Y.T.; Yang, G.; Li, Q.; Li, H.; Jin, F.; Zheng, W. Soy food consumption is associated with lower risk of coronary heart disease in Chinese women. J. Nutr. 2003, 133, 2874–2878. [Google Scholar] [CrossRef] [Green Version]
- Blanco Mejia, S.; Messina, M.; Li, S.S.; Viguiliouk, E.; Chiavaroli, L.; Khan, T.A.; Srichaikul, K.; Mirrahimi, A.; Sievenpiper, J.L.; Kris-Etherton, P.; et al. A Meta-Analysis of 46 Studies Identified by the FDA Demonstrates that Soy Protein Decreases Circulating LDL and Total Cholesterol Concentrations in Adults. J. Nutr. 2019, 149, 968–981. [Google Scholar] [CrossRef]
- Heitmann, B.L.; Lissner, L. Dietary underreporting by obese individuals--is it specific or non-specific? BMJ 1995, 311, 986–989. [Google Scholar] [CrossRef] [Green Version]
- Chan, C.Q.H.; Lee, K.H.; Low, L.L. A systematic review of health status, health seeking behaviour and healthcare utilisation of low socioeconomic status populations in urban Singapore. Int. J. Equity Health 2018, 17, 39. [Google Scholar] [CrossRef] [Green Version]
- Lv, J.; Yu, C.; Guo, Y.; Bian, Z.; Yang, L.; Chen, Y.; Hu, X.; Hou, W.; Chen, J.; Chen, Z.; et al. Adherence to a healthy lifestyle and the risk of type 2 diabetes in Chinese adults. Int. J. Epidemiol. 2017, 46, 1410–1420. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Khor, C.C.; Fan, J.; Lv, J.; Yu, C.; Guo, Y.; Bian, Z.; Yang, L.; Millwood, I.Y.; Walters, R.G.; et al. Genetic risk, adherence to a healthy lifestyle, and type 2 diabetes risk among 550,000 Chinese adults: Results from 2 independent Asian cohorts. Am. J. Clin. Nutr. 2020, 111, 698–707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Diabetes Federation. IDF Diabetes Atlas, 9th ed.; International Diabetes Federation: Brussels, Belgium, 2019. [Google Scholar]

{kind=link}
| Never | Monthly | 1–3 days/week | ≥4 days/week | p Trend | |
|---|---|---|---|---|---|
| No. of participants | 2416 | 6518 | 13,811 | 3394 | |
| Age, years | 57.6 ± 9.7 | 57.4 ± 9.5 | 57.3 ± 9.6 | 57.6 ± 9.7 | 0.61 |
| Women, % | 70.7 | 66.3 | 58.5 | 55.7 | <0.001 |
| Body mass index, kg/m2 | 24.8 ± 3.7 | 24.7 ± 3.6 | 25.0 ± 3.5 | 25.1 ± 3.5 | <0.001 |
| Urban, % | 37.3 | 43.1 | 67.5 | 65.8 | <0.001 |
| High school or higher education level, % | 2.1 | 3.0 | 7.3 | 10.8 | <0.001 |
| Farmer, % | 46.8 | 40.3 | 17.6 | 14.4 | <0.001 |
| Married, % | 84.0 | 86.5 | 87.7 | 89.1 | <0.001 |
| Income > RMB 35,000, % | 8.4 | 14.0 | 22.2 | 26.9 | <0.001 |
| Family history of cardiovascular disease, % | 18.7 | 17.3 | 20.3 | 22.2 | <0.001 |
| History of hypertension, % | 21.3 | 21.6 | 26.4 | 26.8 | <0.001 |
| Current smoker, % | 21.0 | 22.4 | 25.7 | 27.0 | <0.001 |
| Current drinker, % | 43.7 | 41.0 | 46.9 | 46.3 | <0.001 |
| Physical activity, MET·hours/day | 15.0 ± 11.2 | 16.2 ± 11.9 | 16.4 ± 12.4 | 16.7 ± 12.4 | <0.001 |
| Use of fish oil, % | 2.8 | 3.3 | 6.5 | 8.8 | <0.001 |
| Use of vitamin supplements, % | 2.9 | 3.8 | 6.0 | 9.7 | <0.001 |
| Daily tea drinking, % | 46.7 | 39.5 | 37.0 | 36.5 | <0.001 |
| Daily dairy consumption, % | 9.6 | 10.5 | 19.2 | 27.2 | <0.001 |
| Daily egg consumption, % | 17.1 | 14.7 | 19.8 | 31.3 | <0.001 |
| Daily fish consumption, % | 3.9 | 4.6 | 3.0 | 5.5 | <0.001 |
| Daily fruit consumption, % | 10 | 11.4 | 23.0 | 29.3 | <0.001 |
| Daily vegetable consumption, % | 94.7 | 91.0 | 97.5 | 97.0 | <0.001 |
| Daily meat consumption, % | 57 | 60.8 | 76.8 | 75.1 | <0.001 |
| Daily rice consumption, % | 43.1 | 44.1 | 45.1 | 46.1 | <0.001 |
| Never | Monthly | 1–3 days/week | ≥4 days/week | p Trend | |
|---|---|---|---|---|---|
| 0 g/day * | 3.6 g/day | 11.5 g/day | 15.3 g/day | ||
| Total CVD | |||||
| Person-year | 18,206 | 49,541 | 107,870 | 26,693 | |
| No. of cases | 216 | 495 | 754 | 161 | |
| Model 1 | 1.00 | 0.87 (0.74, 1.02) | 0.60 (0.52, 0.70) | 0.49 (0.40, 0.60) | <0.001 |
| Model 2 | 1.00 | 0.92 (0.78, 1.09) | 0.89 (0.75, 1.05) | 0.77 (0.62, 0.96) | 0.02 |
| CHD | |||||
| No. of cases | 79 | 158 | 302 | 56 | |
| Model 1 | 1.00 | 0.76 (0.58, 0.99) | 0.66 (0.52, 0.85) | 0.47 (0.33, 0.66) | <0.001 |
| Model 2 | 1.00 | 0.78 (0.59, 1.03) | 0.81 (0.62, 1.07) | 0.56 (0.39, 0.81) | 0.007 |
| Acute myocardial infarction | |||||
| No. of cases | 53 | 97 | 132 | 23 | |
| Model 1 | 1.00 | 0.69 (0.49, 0.96) | 0.43 (0.31, 0.59) | 0.29 (0.18, 0.47) | <0.001 |
| Model 2 | 1.00 | 0.74 (0.52, 1.06) | 0.68 (0.47, 0.98) | 0.44 (0.26, 0.73) | 0.004 |
| Stroke | |||||
| No. of cases | 98 | 232 | 339 | 74 | |
| Model 1 | 1.00 | 0.89 (0.7, 1.13) | 0.59 (0.47, 0.74) | 0.50 (0.37, 0.67) | <0.001 |
| Model 2 | 1.00 | 0.97 (0.76, 1.25) | 0.99 (0.77, 1.27) | 0.92 (0.66, 1.27) | 0.63 |
| Hemorrhagic stroke | |||||
| No. of cases | 51 | 143 | 159 | 30 | |
| Model 1 | 1.00 | 1.05 (0.76, 1.44) | 0.53 (0.39, 0.73) | 0.39 (0.25, 0.62) | <0.001 |
| Model 2 | 1.00 | 1.04 (0.75, 1.46) | 1.03 (0.73, 1.46) | 0.82 (0.51, 1.33) | 0.33 |
| Ischemic stroke | |||||
| No. of cases | 29 | 59 | 113 | 26 | |
| Model 1 | 1.00 | 0.77 (0.5, 1.21) | 0.67 (0.45, 1.01) | 0.58 (0.34, 0.99) | 0.07 |
| Model 2 | 1.00 | 0.95 (0.6, 1.52) | 0.98 (0.62, 1.55) | 0.90 (0.51, 1.60) | 0.76 |
| Cases | HR (95% CI) * | p Value for Interaction | |
|---|---|---|---|
| Age<60 | |||
| Yes | 15,662 | 0.79 (0.52, 1.20) | 0.50 |
| No | 10,477 | 0.76 (0.59, 0.98) | |
| Men | |||
| Yes | 10,133 | 0.69 (0.49, 0.97) | 0.86 |
| No | 16,006 | 0.85 (0.63, 1.14) | |
| BMI < 25 | |||
| Yes | 13,573 | 0.57 (0.43, 0.76) | 0.03 |
| No | 12,566 | 1.12 (0.80, 1.56) | |
| BMI < 23 | |||
| Yes | 7663 | 0.63 (0.44, 0.90) | 0.12 |
| No | 18,476 | 0.89 (0.68, 1.18) | |
| Current smoking | |||
| Yes | 6435 | 0.78 (0.61, 1.00) | 0.94 |
| No | 19,704 | 0.74 (0.48, 1.14) | |
| Current drinking | |||
| Yes | 11,778 | 0.81 (0.61, 1.07) | 0.86 |
| No | 14,361 | 0.70 (0.49, 0.99) | |
| Urban | |||
| Yes | 15,267 | 0.83 (0.59, 1.16) | 0.11 |
| No | 10,872 | 0.67 (0.49, 0.92) | |
| Hypertension | |||
| Yes | 6481 | 0.91 (0.62, 1.33) | 0.33 |
| No | 19,658 | 0.73 (0.56, 0.95) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, X.; Lv, J.; Yu, C.; Li, L.; Hu, Y.; Qin, L.-Q.; Dong, J.-Y. Dietary Soy Consumption and Cardiovascular Mortality among Chinese People with Type 2 Diabetes. Nutrients 2021, 13, 2513. https://doi.org/10.3390/nu13082513
Wang X, Lv J, Yu C, Li L, Hu Y, Qin L-Q, Dong J-Y. Dietary Soy Consumption and Cardiovascular Mortality among Chinese People with Type 2 Diabetes. Nutrients. 2021; 13(8):2513. https://doi.org/10.3390/nu13082513
Chicago/Turabian StyleWang, Xiaowen, Jun Lv, Canqing Yu, Liming Li, Yonghua Hu, Li-Qiang Qin, and Jia-Yi Dong. 2021. "Dietary Soy Consumption and Cardiovascular Mortality among Chinese People with Type 2 Diabetes" Nutrients 13, no. 8: 2513. https://doi.org/10.3390/nu13082513
APA StyleWang, X., Lv, J., Yu, C., Li, L., Hu, Y., Qin, L.-Q., & Dong, J.-Y. (2021). Dietary Soy Consumption and Cardiovascular Mortality among Chinese People with Type 2 Diabetes. Nutrients, 13(8), 2513. https://doi.org/10.3390/nu13082513