
Efficacy of Bilberry and Grape Seed Extract Supplement Interventions to Improve Glucose and Cholesterol Metabolism and Blood Pressure in Different Populations—A Systematic Review of the Literature

 ,
,
Abstract
1. Introduction
2. Materials and Methods
3. Results
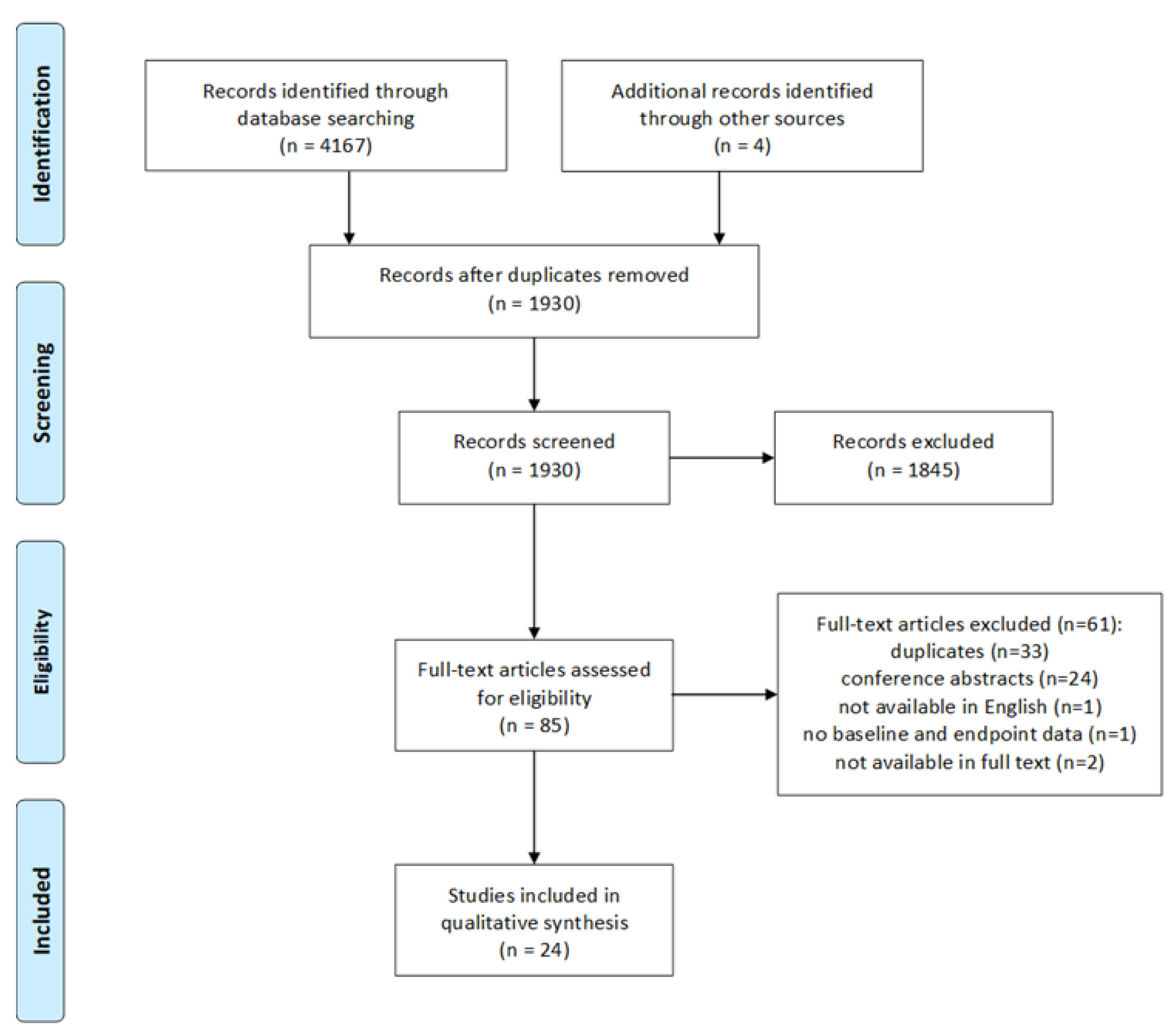
3.1. Study Selection
3.2. Study Characteristics
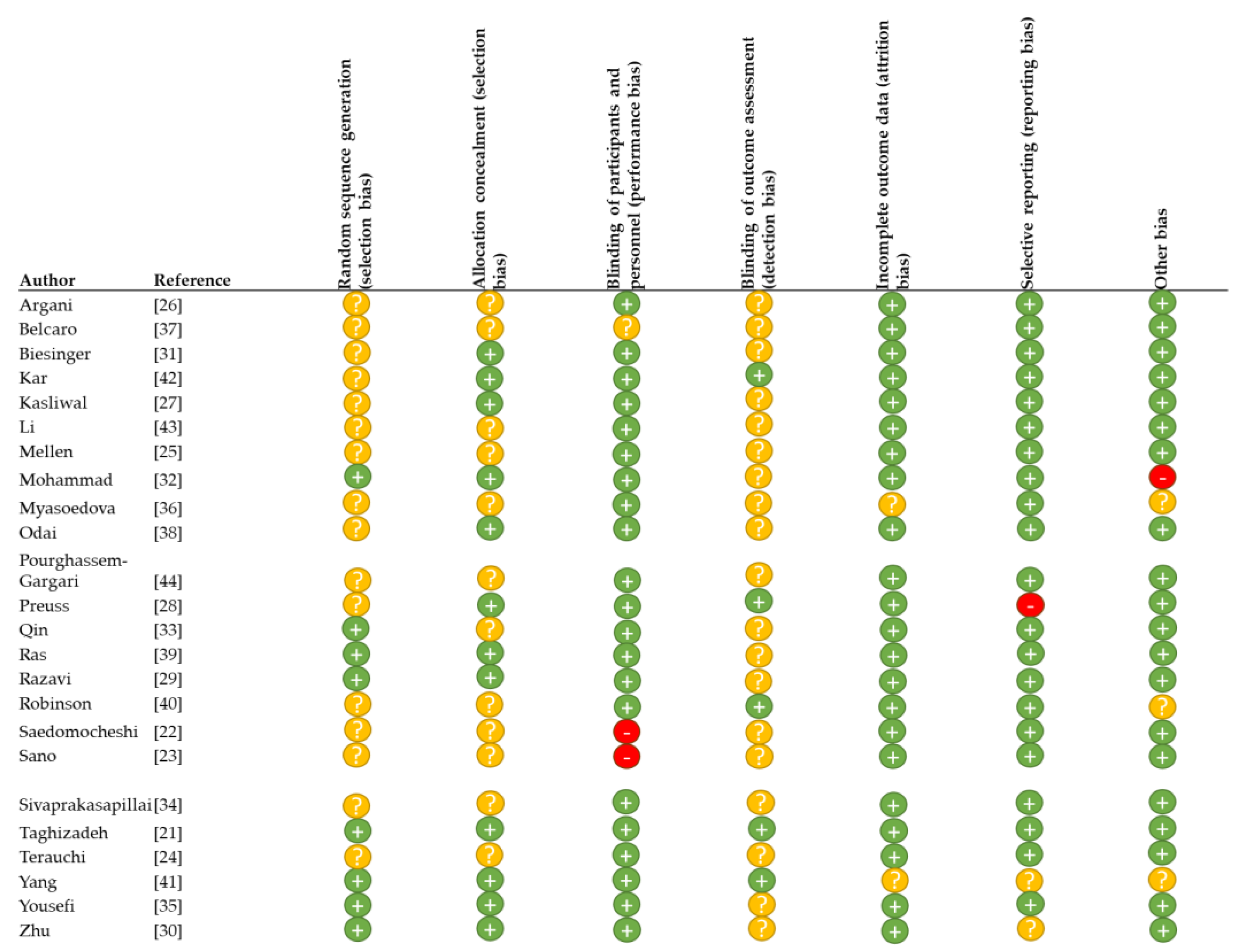
3.3. Evaluation of Study and Reporting Quality
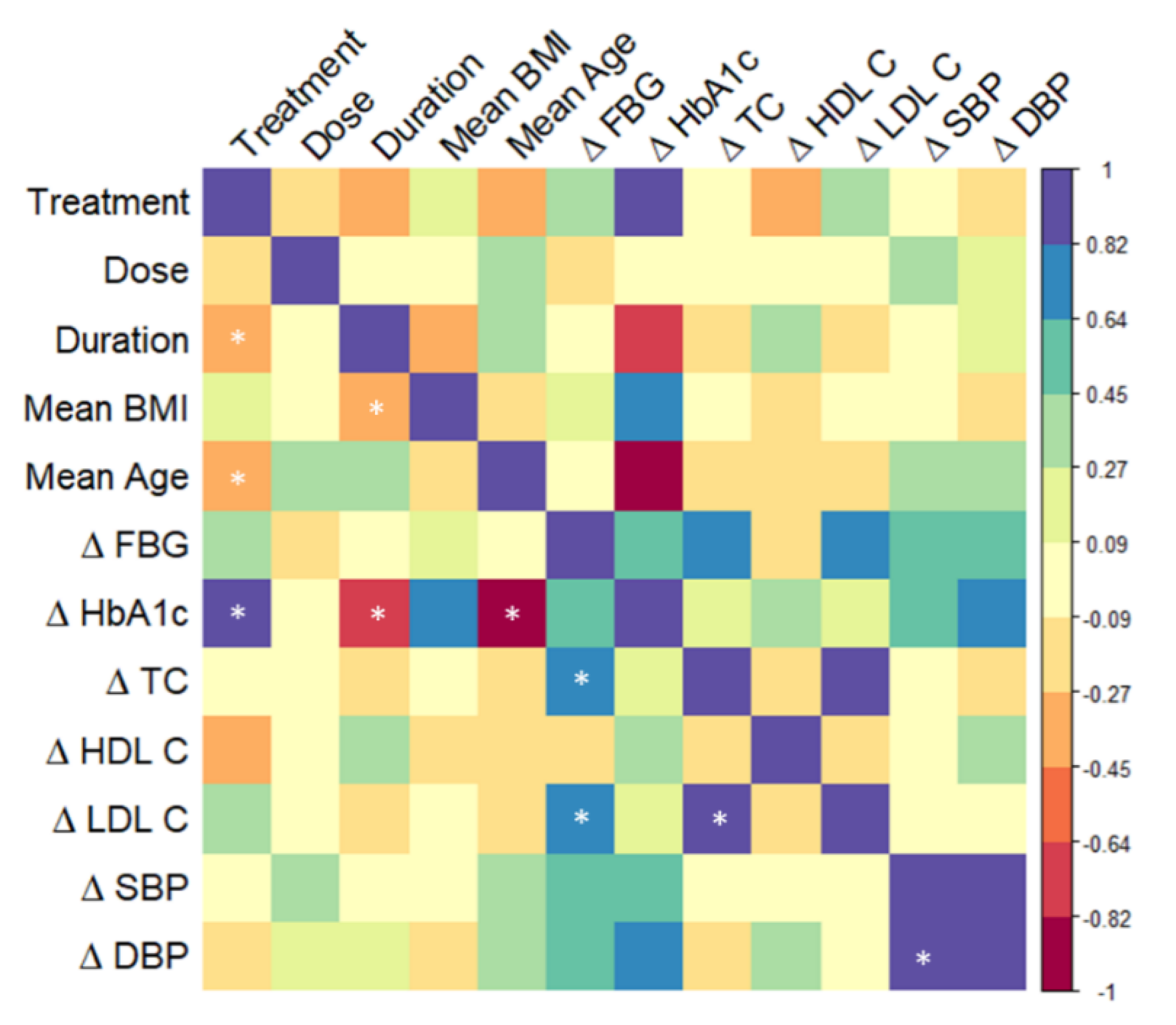
3.4. Correlation Analysis
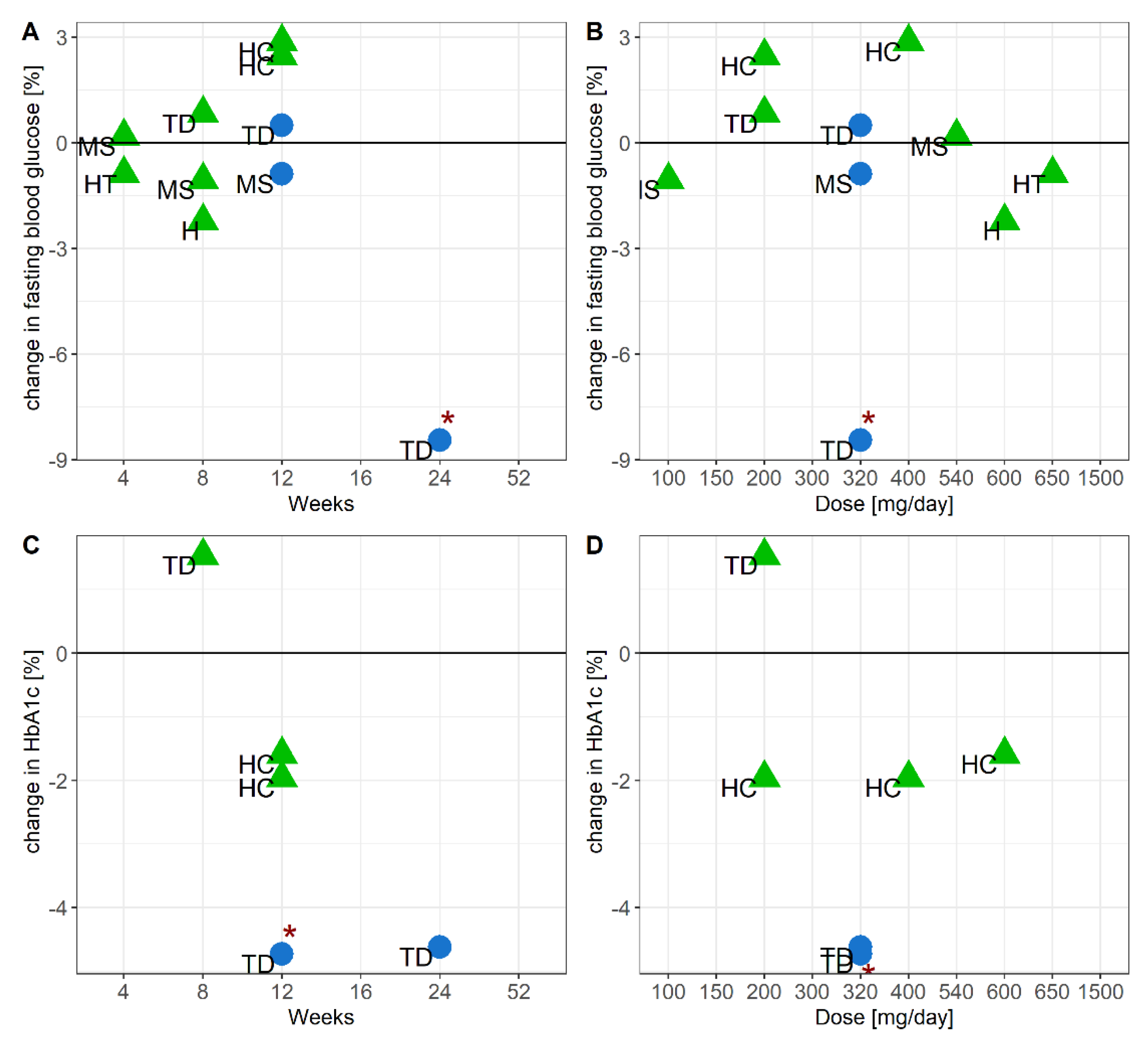
3.5. Efficacy of Grape Seed or Bilberry and Blackcurrant Extract Supplements to Modulate Glucoses Metabolism
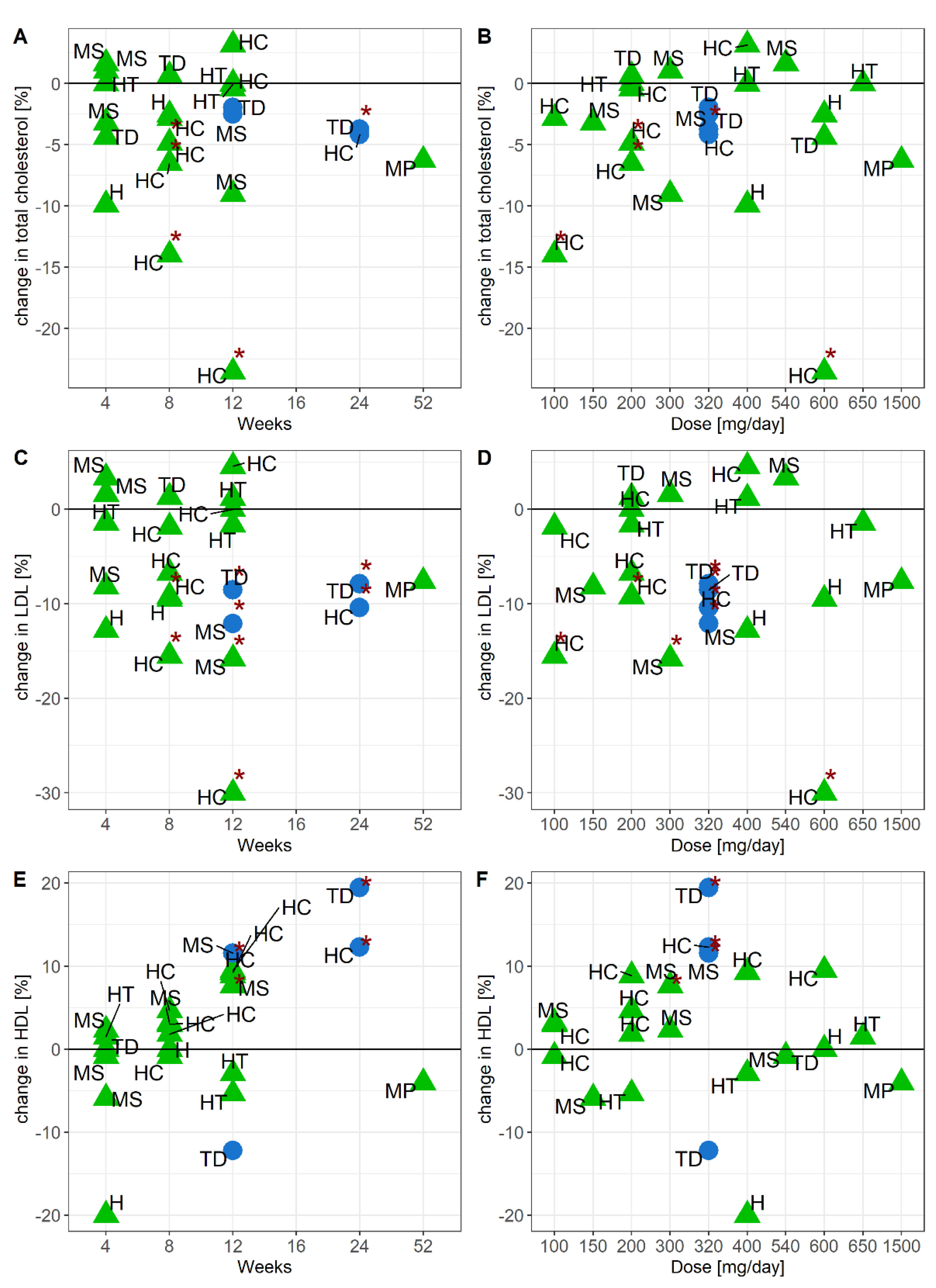
3.6. Efficacy of Grape Seed or Bilberry and Blackcurrant Extract Supplements to Modulate Cholesterol Metabolism
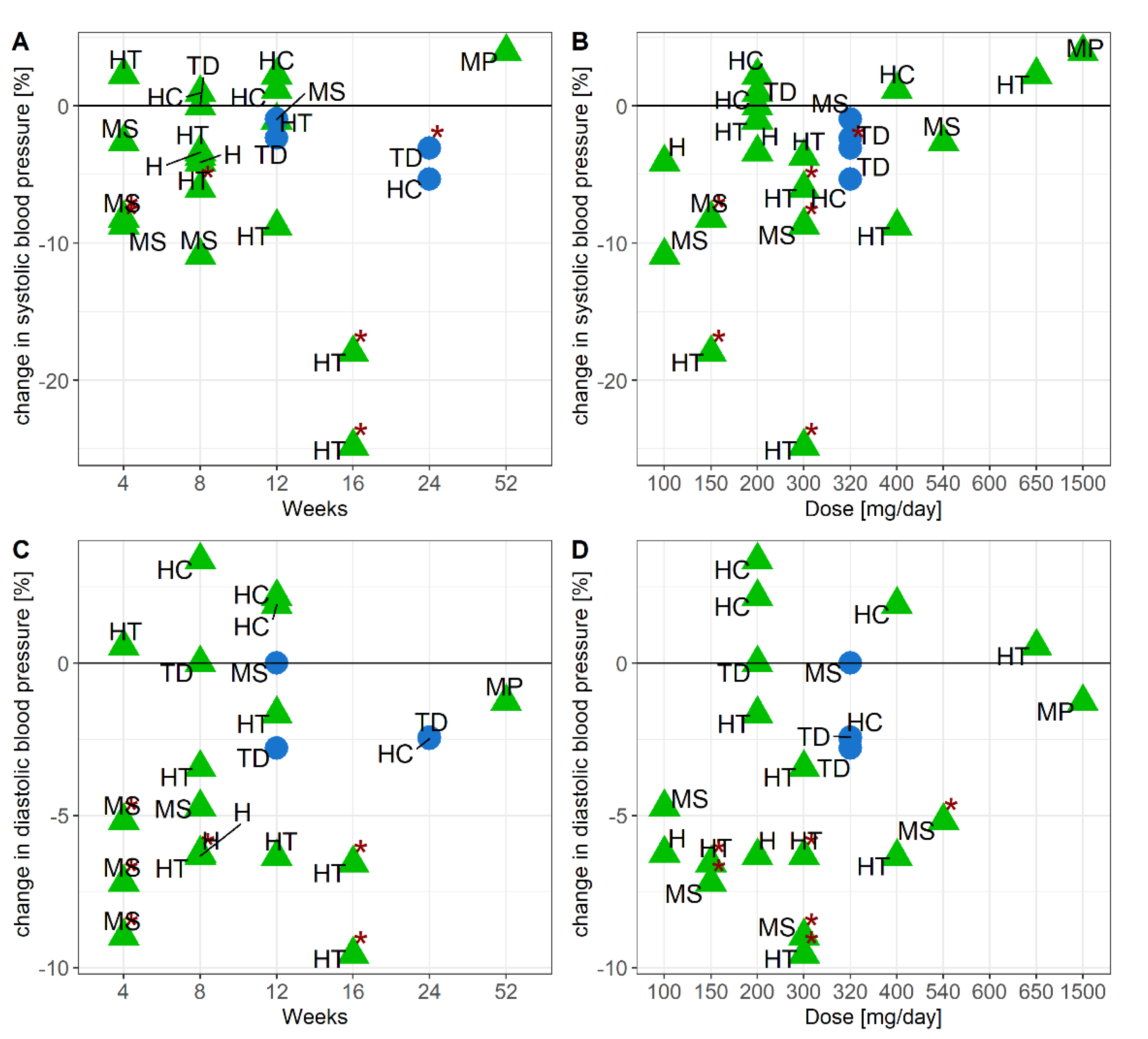
3.7. Efficacy of Grape Seed and Bilberry and Blackcurrant Extract Supplements to Modulate Blood Pressure
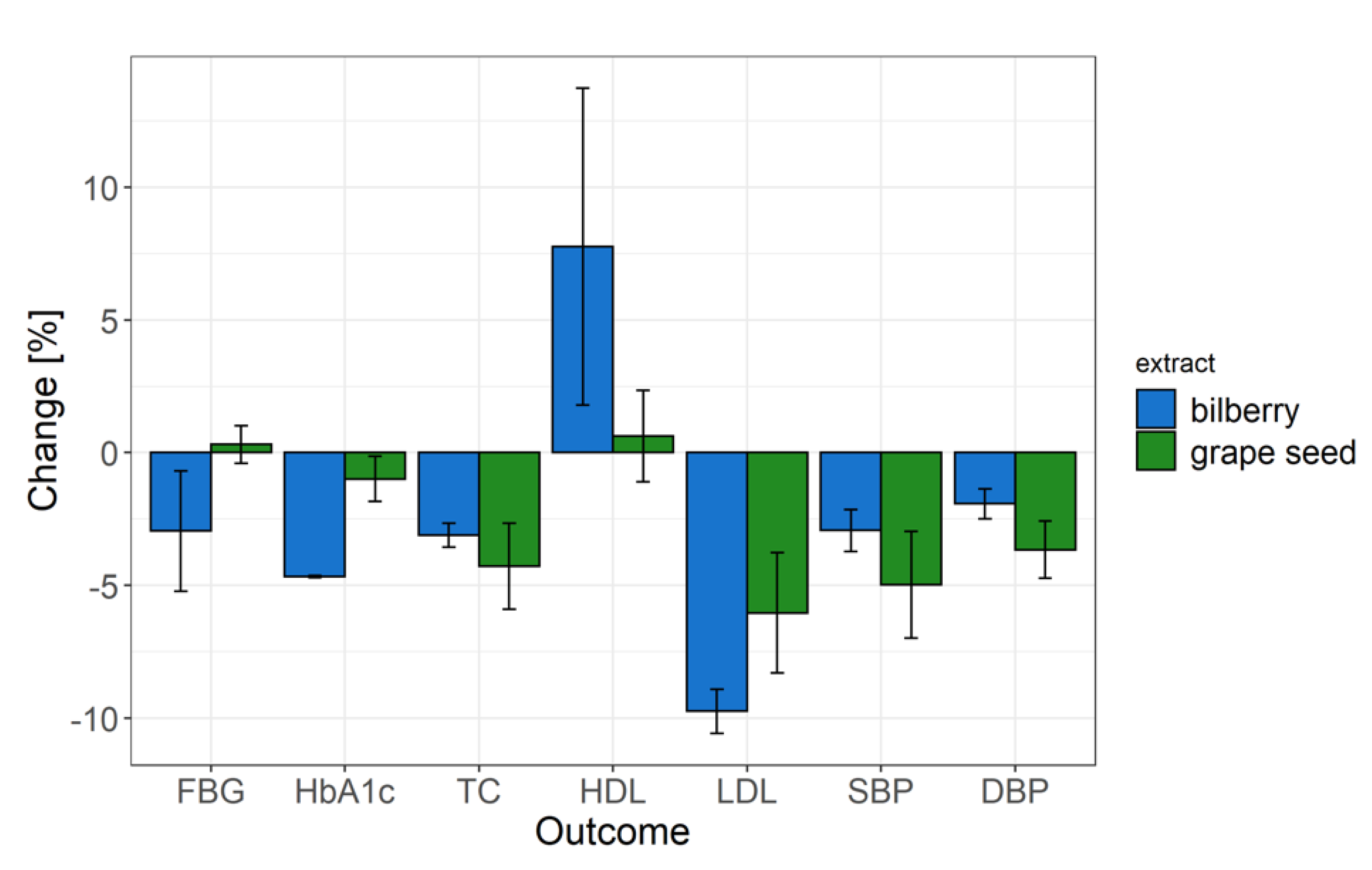
3.8. Overall Efficacy of Grape Seed and Bilberry and Blackcurrant Extracts to Modulate Glucose and Cholesterol Metabolism, and Blood Pressure
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organisation. Global Report on Diabetes; World Health Organisation: Geneva, Switzarland, 2014. [Google Scholar]
- Mozaffarian, D. Dietary and Policy Priorities for Cardiovascular Disease, Diabetes, and Obesity. Circulation 2016, 133, 187–225. [Google Scholar] [CrossRef] [PubMed]
- Salvadó, M.J.; Casanova, E.; Fernández-Iglesias, A.; Arola, L.; Bladé, C. Roles of proanthocyanidin rich extracts in obesity. Food Funct. 2015, 6, 1053–1071. [Google Scholar] [CrossRef] [PubMed]
- Gu, L.; Kelm, M.A.; Hammerstone, J.F.; Beecher, G.; Holden, J.; Haytowitz, D.; Gebhardt, S.; Prior, R.L. Concentrations of Proanthocyanidins in Common Foods and Estimations of Normal Consumption. J. Nutr. 2004, 134, 613–617. [Google Scholar] [CrossRef] [PubMed]
- Fraga, C.G. Plant Phenolics and Human Health: Biochemistry, Nutrition and Pharmacology; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2009. [Google Scholar]
- Williamson, G.; Kay, C.D.; Crozier, A. The Bioavailability, Transport, and Bioactivity of Dietary Flavonoids: A Review from a Historical Perspective. Compr. Rev. Food Sci. Food Saf. 2018, 17, 1054–1112. [Google Scholar] [CrossRef]
- Walther, B.; Lett, A.M.; Bordoni, A.; Cobos, L.T.; Nieto, J.A.; Dupont, D.; Danesi, F.; Shahar, D.R.; Echaniz, A.; Re, R.; et al. GutSelf: Interindividual Variability in the Processing of Dietary Compounds by the Human Gastrointestinal Tract. Mol. Nutr. Food Res. 2019, 3, 1–28. [Google Scholar] [CrossRef]
- Manach, C.; Milenkovic, D.; van de Wiele, T.; Rodriguez-Mateos, A.; de Roos, B.; Garcia-Conesa, M.T.; Landberg, R.; Gibney, E.R.; Heinonen, M.; Tomás-Barberán, F.; et al. Addressing the inter-individual variation in response to consumption of plant food bioactives: Towards a better understanding of their role in healthy aging and cardiometabolic risk reduction. Mol. Nutr. Food Res. 2017, 61, 1–16. [Google Scholar] [CrossRef]
- Laouali, N.; Berrandou, T.; Rothwell, J.A.; Shah, S.; El Fatouhi, D.; Mancini, F.R.; Boutron-Ruault, M.; Fagherazzi, G. Profiles of polyphenol intake and type 2 diabetes risk in 60,586 women followed for 20 years: Results from the E3N cohort study. Nutrients 2020, 12, 1934. [Google Scholar] [CrossRef]
- Chan, S.W.; Tomlinson, B. Effects of bilberry supplementation on metabolic and cardiovascular disease risk. Molecules 2020, 25, 1653. [Google Scholar] [CrossRef]
- Calvano, A.; Izuora, K.; Oh, E.C.; Ebersole, J.L.; Lyons, T.J.; Basu, A. Dietary berries, insulin resistance and type 2 diabetes: An overview of human feeding trials. Food Funct. 2019, 10, 6227–6243. [Google Scholar] [CrossRef]
- Zhang, L.; Wang, Y.; Li, D.; Ho, C.T.; Li, J.; Wan, X. The absorption, distribution, metabolism and excretion of procyanidins. Food Funct. 2016, 7, 1273–1281. [Google Scholar] [CrossRef]
- Zhu, Y.; Miao, Y.; Meng, Z.; Zhong, Y. Effects of Vaccinium Berries on Serum Lipids: A Meta-Analysis of Randomized Controlled Trials. Evid.-Based Complement. Altern. Med. 2015, 1–11. [Google Scholar] [CrossRef]
- Woerdeman, J.; van Poelgeest, E.; Ket, J.C.F.; Eringa, E.C.; Serné, E.H.; Smulders, Y.M. Do grape polyphenols improve metabolic syndrome components? A systematic review. Eur. J. Clin. Nutr. 2017, 71, 1381–1392. [Google Scholar] [CrossRef] [PubMed]
- Anjom-Shoae, J.; Milajerdi, A.; Larijani, B.; Esmaillzadeh, A. Effects of grape seed extract on dyslipidaemia: A systematic review and dose-response meta-analysis of randomised controlled trials. Br. J. Nutr. 2020, 1–14. [Google Scholar] [CrossRef]
- Zhang, L.; Shuang, L.; Lan, L.; Liu, S.; Geng, T. The impact of grape seed extract treatment on blood pressure changes: A meta-analysis of 16 randomized controlled trials. Medicine 2016, 95, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Savović, J.; Page, M.J.; Elbers, R.G.; Sterne, J.A. Assessing risk of bias in a randomized trial. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.1; John Wiley & Sons: Chichester, UK, 2020; Chapter 8. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.R-project.org/ (accessed on 16 May 2021).
- Wei, T.; Simko, V. R Package ‘Corrplot’: Visualization of a Correlation Matrix (Version 0.84). 2017. Available online: https://rdrr.io/cran/corrplot/ (accessed on 11 May 2021).
- Wickam, H. ggplot2: Elegant Graphics for Data Analysis; Springer International Publishing: Berlin, Germany, 2016. [Google Scholar]
- Taghizadeh, M.; Malekian, E.; Memarzadeh, M.R.; Mohammadi, A.A.; Asemi, Z. Grape Seed Extract Supplementation and the Effects on the Biomarkers of Oxidative Stress and Metabolic Profiles in Female Volleyball Players: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Iran. Red Crescent Med. J. 2016, 18, 1–9. [Google Scholar] [CrossRef]
- Saedomocheshi, S. The effects of regular aerobic training and grape seed extract on the cardiovascular risk factors in obese older women. J. Kurdistan Univ. Med. Sci. 2015, 1, 8–14. [Google Scholar]
- Sano, A.; Uchida, R.; Saito, M.; Shioya, N.; Komori, Y.; Tho, Y.; Hashizume, N. Beneficial effects of grape seed extract on malondialdehyde-modified LDL. J. Nutr. Sci. Vitaminol. 2007, 53, 174–182. [Google Scholar] [CrossRef] [PubMed]
- Terauchi, M.; Horiguchi, N.; Kajiyama, A.; Akiyoshi, M.; Owa, Y.; Kato, K.; Kubota, T. Effects of grape seed proanthocyanidin extract on menopausal symptoms, body composition, and cardiovascular parameters in middle-aged women: A randomized, double-blind, placebo-controlled pilot study. Menopause 2014, 21, 990–996. [Google Scholar] [CrossRef]
- Mellen, P.B.; Daniel, K.R.; Brosnihan, K.B.; Hansen, K.J.; Herrington, D.M. Effect of muscadine grape seed supplementation on vascular function in subjects with or at risk for cardiovascular disease: A randomized crossover trial. J. Am. Coll. Nutr. 2010, 29, 469–475. [Google Scholar] [CrossRef]
- Argani, H.; Ghorbanihaghjo, A.; Vatankhahan, H.; Rashtchizadeh, N.; Raeisi, S.; Ilghami, H. O efeito do extrato de semente de uva vermelha na atividade do soro paraoxonase em doentes com hiperlipidemia leve a moderada. Sao Paulo Med. J. 2016, 134, 234–239. [Google Scholar] [CrossRef]
- Kasliwal, R.R.; Bansal, M.; Gupta, R.; Shah, S.; Dani, S.; Oomman, A.; Pai, V.; Prasad, G.M.; Singhvi, S.; Patel, J. ESSENS dyslipidemia: A placebo-controlled, randomized study of a nutritional supplement containing red yeast rice in subjects with newly diagnosed dyslipidemia. Nutrition 2016, 32, 767–776. [Google Scholar] [CrossRef] [PubMed]
- Preuss, H.G.; Wallerstedt, D.; Talpur, N.; Tutuncuoglu, S.O.; Echard, B.; Myers, A.; Bui, M.; Bagchi, D. Effects of Niacin-bound chromium and Grape seed proanthocyanidin extract on the Lipid Profile of Hypercholesterolemic Subjects. J. Med. 2000, 31, 227–244. [Google Scholar]
- Razavi, S.-M.; Gholamin, S.; Eskandari, A.; Mohsenian, N.; Ghorbanihaghjo, A.; Delazar, A.; Rashtchizadeh, N.; Keshtkar-Jahromi, M.; Argani, H. Red Grape Seed Extract Improves Lipid Profiles and Decreases Oxidized Low-Density Lipoprotein in Patients with Mild Hyperlipidemia. J. Med. Food 2013, 16, 255–258. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Ling, W.; Guo, H.; Song, F.; Ye, Q.; Zou, T.; Li, D.; Zhang, Y.; Li, G.; Xiao, Y.; et al. Anti-inflammatory effect of purified dietary anthocyanin in adults with hypercholesterolemia: A randomized controlled trial. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 843–849. [Google Scholar] [CrossRef] [PubMed]
- Biesinger, S.; Michaels, H.A.; Quadros, A.S.; Qian, Y.; Rabovsky, A.B.; Badger, R.S.; Jalili, T. A combination of isolated phytochemicals and botanical extracts lowers diastolic blood pressure in a randomized controlled trial of hypertensive subjects. Eur. J. Clin. Nutr. 2016, 70, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Mohammad, A.; Shahnaz, T.; Sorayya, K. Effect of 8 weeks’ supplementation grape seed extract on insulin resistance in iranian adolescents with metabolic syndrome: A randomized controlled trial. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 197–203. [Google Scholar] [CrossRef]
- Qin, Y.; Xia, M.; Ma, J.; Hao, Y.; Liu, J.; Mou, H.; Cao, L.; Ling, W. Anthocyanin supplementation improves serum LDL- and HDL-cholesterol concentrations associated with the inhibition of cholesteryl ester transfer protein in dyslipidemic subjects. Am. J. Clin. Nutr. 2009, 90, 485–492. [Google Scholar] [CrossRef]
- Sivaprakasapillai, B.; Edirisinghe, I.; Randolph, J.; Steinberg, F.; Kappagoda, T. Effect of grape seed extract on blood pressure in subjects with the metabolic syndrome. Metab. Clin. Exp. 2009, 58, 1743–1746. [Google Scholar] [CrossRef]
- Yousefi, R.; Parandoosh, M.; Khorsandi, H.; Hosseinzadeh, N.; Tonekaboni, M.M.; Saidpour, A.; Babaei, H.; Ghorbani, A. Grape seed extract supplementation along with a restricted-calorie diet improves cardiovascular risk factors in obese or overweight adult individuals: A randomized, placebo-controlled trial. Phyther. Res. 2020, 1–9. [Google Scholar] [CrossRef]
- Myasoedova, V.; Kirichenko, T.V.; Melnichenko, A.A.; Orekhova, V.A.; Ravani, A.; Poggio, P.; Sobenin, I.A.; Bobryshev, Y.V.; Orekhov, A.N. Anti-Atherosclerotic Effects of a Phytoestrogen-Rich Herbal Preparation in Postmenopausal Women. Int. J. Mol. Sci. 2016, 17, 1318. [Google Scholar] [CrossRef]
- Belcaro, G.; Ledda, A.; Hu, S.; Cesarone, M.R.; Feragalli, B.; Dugall, M. Grape seed procyanidins in pre- and mild hypertension: A registry study. Evid.-Based Complement. Altern. Med. 2013, 2013, 1–5. [Google Scholar] [CrossRef]
- Odai, T.; Terauchi, M.; Kato, K.; Hirose, A.; Miyasaka, N. Effects of Grape Seed Proanthocyanidin Extract on Vascular Endothelial Function in Participants with Prehypertension: A Randomized, Double-Blind, Placebo-Controlled Study. Nutrients 2019, 11, 2844. [Google Scholar] [CrossRef] [PubMed]
- Ras, R.T.; Zock, P.L.; Zebregs, Y.E.M.P.; Johnston, N.R.; Webb, D.J.; Draijer, R. Effect of polyphenol-rich grape seed extract on ambulatory blood pressure in subjects with pre- and stage I hypertension. Br. J. Nutr. 2013, 110, 2234–2241. [Google Scholar] [CrossRef] [PubMed]
- Robinson, M.; Lu, B.; Edirisinghe, I.; Kappagoda, C.T. Effect of grape seed extract on blood pressure in subjects with pre-hypertension. J. Pharm. Nutr. Sci. 2012, 2, 155–159. [Google Scholar]
- Yang, L.; Ling, W.; Yang, Y.; Chen, Y.; Tian, Z.; Du, Z.; Chen, J.; Xie, Y.; Liu, Z.; Yang, L. Role of Purified Anthocyanins in Improving Cardiometabolic Risk Factors in Chinese Men and Women with Prediabetes or Early Untreated Diabetes-A Randomized Controlled Trial. Nutrients 2017, 9, 1104. [Google Scholar] [CrossRef] [PubMed]
- Kar, P.; Laight, D.; Rooprai, H.K.; Shaw, K.M.; Cummings, M. Effects of grape seed extract in Type 2 diabetic subjects at high cardiovascular risk: A double blind randomized placebo controlled trial examining metabolic markers, vascular tone, inflammation, oxidative stress and insulin sensitivity. Diabet. Med. 2009, 26, 526–531. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Zhang, Y.; Liu, Y.; Sun, R.; Xia, M. Purified Anthocyanin Supplementation Reduces Dyslipidemia, Enhances Antioxidant Capacity, and Prevents Insulin Resistance in Diabetic Patients. J. Nutr. 2015, 145, 742–748. [Google Scholar] [CrossRef] [PubMed]
- Pourghassem-Gargari, B.; Abedini, S.; Babaei, H.; Aliasgarzadeh, A.; Pourabdollahi, P. Effect of supplementation with grape seed (Vitis vinifera) extract on antioxidant status and lipid peroxidation in patient with type II diabetes. J. Med. Plants Res. 2011, 5, 2029–2034. [Google Scholar]
- García-Conesa, M.-T.; Chambers, K.; Combet, E.; Pinto, P.; Garcia-Aloy, M.; Andrés-Lacueva, C.; de Pascual-Teresa, S.; Mena, P.; Ristic, A.K.; Hollands, W.J.; et al. Meta-Analysis of the Effects of Foods and Derived Products Containing Ellagitannins and Anthocyanins on Cardiometabolic Biomarkers: Analysis of Factors Influencing Variability of the Individual Responses. Int. J. Mol. Sci. 2018, 19, 694. [Google Scholar] [CrossRef]
- Menezes, R.; Rodriguez-Mateos, A.; Kaltsatou, A.; González-Sarrías, A.; Greyling, A.; Giannaki, C.; Andres-Lacueva, C.; Milenkovic, D.; Gibney, E.R.; Dumont, J.; et al. Impact of Flavonols on Cardiometabolic Biomarkers: A Meta-Analysis of Randomized Controlled Human Trials to Explore the Role of Inter-Individual Variability. Nutrients 2017, 9, 117. [Google Scholar] [CrossRef]
- Schork, N.J.; Goetz, L.H. Single-Subject Studies in Translational Nutrition Research. Annu. Rev. Nutr. 2017, 37, 395–422. [Google Scholar] [CrossRef] [PubMed]
- Schweizer, A.; Couturier, A.; Foley, J.E.; Dejager, S. Comparison between vildagliptin and metformin to sustain reductions in HbA1c over 1 year in drug-naïve patients with Type 2 diabetes. Diabet. Med. 2007, 24, 955–961. [Google Scholar] [CrossRef]
- Giugliano, D.; Ceriello, A.; Esposito, K. Glucose metabolism and hyperglycemia. Am. J. Clin. Nutr. 2008, 87, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Hoggard, N.; Cruickshank, M.; Moar, K.; Bestwick, C.; Holst, J.J.; Russell, W.; Horgan, G. A single supplement of a standardised bilberry (Vaccinium myrtillus L.) extract (36 % wet weight anthocyanins) modifies glycaemic response in individuals with type 2 diabetes controlled by diet and lifestyle. J. Nutr. Sci. 2013, 2, 1–9. [Google Scholar] [CrossRef]
- Lewington, S.; Clarke, R.; Qizilbash, N.; Peto, R.; Collins, R. Age-specific relevance of usual blood pressure to vascular mortality: A meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002, 360, 1903–1913. [Google Scholar] [PubMed]
- Bohn, T. Dietary factors affecting polyphenol bioavailability. Nutr. Rev. 2014, 72, 429–452. [Google Scholar] [CrossRef]
- Babu, P.V.A.; Liu, D.; Gilbert, E.R. Recent advances in understanding the anti-diabetic actions of dietary flavonoids. J. Nutr. Biochem. 2013, 24, 1777–1789. [Google Scholar] [CrossRef]
- Johnston, K.; Sharp, P.; Clifford, M.; Morgan, L. Dietary polyphenols decrease glucose uptake by human intestinal Caco-2 cells. FEBS Lett. 2005, 579, 1653–1657. [Google Scholar] [CrossRef]
- Wood, E.; Hein, S.; Heiss, C.; Williams, C.; Rodriguez-Mate, A. Blueberries and cardiovascular disease prevention. Food Funct. 2019, 10, 7621–7633. [Google Scholar] [CrossRef]
- Krga, I.; Milenkovic, D. Anthocyanins: From Sources and Bioavailability to Cardiovascular-Health Benefits and Molecular Mechanisms of Action. J. Agric. Food Chem. 2019, 67, 1771–1783. [Google Scholar] [CrossRef]
- Nie, Y.; Stürzenbaum, S.R. Proanthocyanidins of Natural Origin: Molecular Mechanisms and Implications for Lipid Disorder and Aging-Associated Diseases. Adv. Nutr. 2019, 10, 464–478. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intervention | Dose [mg/d] | Study Design | Study Duration [wks] | Number of Subjects | Age Range | BMI Range | Male/Female Ratio | Health Status of Subjects | Participant Drop-Out Rate (%) | Country | Reference |
|---|---|---|---|---|---|---|---|---|---|---|---|
| GSE | 600 | Double blind, parallel | 8 | 40 | 14–28 | 18–25 | all female | Healthy | - | Iran | [21] |
| GSE | 400 | Double blind, parallel | 4 | 20 | 60+ | 30–36 | all female | Healthy and obese | - | Iran | [22] |
| GSE | 200 | Single blind, parallel | 12 | 53 | 40–62 | 22–27 | 10/11 (not considering dropouts) | Healthy, mild hypercholesterolemia | 13 | Japan | [23] |
| GSE | 400 | Single blind, parallel | 12 | 53 | 40–62 | 22–27 | 9/11 (not considering dropouts) | Healthy, mild hypercholesterolemia | 13 | Japan | [23] |
| GSE | 100 | Double blind, parallel | 8 | 96 | 44–56 | 18–24 | all female | Healthy: pre-menopausal, in menopause, post-menopausal | 5 | Japan | [24] |
| GSE | 200 | Double blind, parallel | 8 | 96 | 44–56 | 18–24 | all female | Healthy: pre-menopausal, in menopause, post-menopausal | 5 | Japan | [24] |
| GSE | 650 | Double blind, cross–over with 2 week washout | 4 | 50 | 44–60 | 23–35 | 25/25 | Heart disease or Hypertension | - | USA | [25] |
| GSE | 200 | Double blind, parallel | 8 | 70 | 39–57 | – | 27/43 | Hypercholesterolemia | 7 | Iran | [26] |
| GSE in formulation | 600 | Double blind, parallel | 12 | 180 | 37–57 | 21–31 | 58/34 (intervention) 45/43 (placebo) | Hypercholesterolemia | 6 | India | [27] |
| GSE | 100 | Double blind, parallel | 8 | 38 | - | - | - | Hypercholesterolemia | 5 | USA | [28] |
| GSE + chromium | 100 | Double blind, parallel | 8 | 38 | - | - | - | Hypercholesterolemia | 5 | USA | [28] |
| GSE | 200 | Double blind, cross–over with 8 week washout | 8 | 42 | 39–57 | - | 18/24 | Hypercholesterolemia | 19 | Iran | [29] |
| Bilberry and blackcurrant extract | 320 | Double blind, parallel | 24 | 146 | 40–65 | - | 31/42 | Hypercholesterolemia | 3 | China | [30] |
| GSE in formulation | 540 | Double blind, cross–over with 2 week washout | 4 | 18 | 41–47 | 31–34 | 15/3 | Metabolic syndrome | 38 | USA | [31] |
| GSE | 100 | Double blind, parallel | 8 | 42 | 13–19 | 27–36 | 14/7 (intervention) 5/16 (placebo) | Metabolic syndrome | 13 | Iran | [32] |
| Bilberry and blackcurrant extract | 320 | Double blind, parallel | 12 | 120 | 40–65 | 22–31 | 21/39 | Metabolic syndrome | - | China | [33] |
| GSE | 150 | Double blind, parallel | 4 | 27 | 42–48 | 34–37 | 4/5 | Metabolic syndrome | - | USA | [34] |
| GSE | 300 | Double blind, parallel | 4 | 27 | 43–51 | 34–39 | 4/5 | Metabolic syndrome | - | USA | [34] |
| GSE | 300 | Double blind, parallel | 12 | 40 | 31–36 | 27–39 | 4/16 (intervention) 3/17 (placebo) | Metabolic syndrome | 20 | Iran | [35] |
| GSE in formulation | 1500 | Double blind, parallel | 52 | 131 | 58–72 | 23–31 | all female | Postmenopausal | 17 | Russia | [36] |
| GSE | 150 | Double blind, parallel | 16 | 119 | 44–56 | 24–26 | 17/18 | Pre-hypertension | - | Italy | [37] |
| GSE | 300 | Double blind, parallel | 16 | 119 | 44–56 | 24–26 | 23/14 | Pre-hypertension | - | Italy | [37] |
| GSE | 200 | Double blind, parallel | 12 | 30 | 40–64 | 19–27 | 2/8 | Pre-hypertension | - | Japan | [38] |
| GSE | 400 | Double blind, parallel | 12 | 30 | 40–64 | 19–27 | 2/8 | Pre-hypertension | - | Japan | [38] |
| GSE | 300 | Double blind, parallel | 8 | 70 | 62–64 | 18–30 | 19/16 | Pre-hypertension | 1 | The Netherlands | [39] |
| GSE | 300 | Double blind, parallel | 8 | 32 | 48–57 | - | 9/7 (intervention) 6/10 (placebo) | Pre-hypertension | - | USA | [40] |
| Bilberry and blackcurrant extract | 320 | Double blind, parallel | 12 | 160 | 40–75 | 21–28 | 25/55 | Pre-diabetes and T2DM | 14 | China | [41] |
| GSE | 600 | Double blind, cross–over with 2 week washout | 4 | 32 | 55–68 | 24–36 | 16/16 | T2DM | - | UK | [42] |
| Bilberry and blackcurrant extract | 320 | Double blind, parallel | 24 | 58 | 56–67 | 20–27 | 17/12 | T2DM | - | China | [43] |
| GSE | 200 | Double blind, parallel | 8 | 48 | 30–65 | 25–37 | - | T2DM | 20 | Iran | [44] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grohmann, T.; Litts, C.; Horgan, G.; Zhang, X.; Hoggard, N.; Russell, W.; de Roos, B. Efficacy of Bilberry and Grape Seed Extract Supplement Interventions to Improve Glucose and Cholesterol Metabolism and Blood Pressure in Different Populations—A Systematic Review of the Literature. Nutrients 2021, 13, 1692. https://doi.org/10.3390/nu13051692
Grohmann T, Litts C, Horgan G, Zhang X, Hoggard N, Russell W, de Roos B. Efficacy of Bilberry and Grape Seed Extract Supplement Interventions to Improve Glucose and Cholesterol Metabolism and Blood Pressure in Different Populations—A Systematic Review of the Literature. Nutrients. 2021; 13(5):1692. https://doi.org/10.3390/nu13051692
Chicago/Turabian StyleGrohmann, Teresa, Caroline Litts, Graham Horgan, Xuguang Zhang, Nigel Hoggard, Wendy Russell, and Baukje de Roos. 2021. "Efficacy of Bilberry and Grape Seed Extract Supplement Interventions to Improve Glucose and Cholesterol Metabolism and Blood Pressure in Different Populations—A Systematic Review of the Literature" Nutrients 13, no. 5: 1692. https://doi.org/10.3390/nu13051692
APA StyleGrohmann, T., Litts, C., Horgan, G., Zhang, X., Hoggard, N., Russell, W., & de Roos, B. (2021). Efficacy of Bilberry and Grape Seed Extract Supplement Interventions to Improve Glucose and Cholesterol Metabolism and Blood Pressure in Different Populations—A Systematic Review of the Literature. Nutrients, 13(5), 1692. https://doi.org/10.3390/nu13051692