
Relationship between Thyroid Status during the First Trimester of Pregnancy and Neonatal Well-Being


Abstract
1. Introduction
2. Materials and Methods
2.1. Laboratory Methods
2.2. Variables
2.3. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Teng, W.; Shan, Z.; Patil Sisodia, K.; Cooper, D.S. Hypothyroidism in pregnancy. Lancet Diabetes Endocrinol. 2013, 3, 228–237. [Google Scholar] [CrossRef]
- Prezioso, G.; Giannini, C.; Chiarelli, F. Effect of Thyroid Hormones on Neurons and Neurodevelopment. Horm. Res. Paediatr. 2018, 2, 73–81. [Google Scholar] [CrossRef]
- Niwattisaiwong, S.; Burman, K.D.; Li-Ng, M. Iodine deficiency: Clinical implications. Clevel. Clin. J. Med. 2017, 3, 236–244. [Google Scholar] [CrossRef]
- Milman, N.; Paszkowski, T.; Cetin, I.; Castelo-Branco, C. Supplementation during pregnancy: Beliefs and science. Gynecol. Endocrinol. 2016, 7, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Petersen, T.G.; Andersen, A.N.; Uldall, P.; Paneth, N.; Feld-Rasmussen, F.; Christophersen, M.; Standberg-Larsen, K. Maternal thyroid disorder in pregnancy and risk of cerebral palsy in the child: A population-based cohort study. BMC Pediatr. 2018, 1, 181. [Google Scholar] [CrossRef]
- Kiran, Z.; Sheikh, A.; Malik, S.; Meraj, A.; Masood, M.; Ismail, S.; Rashid, M.O.; Shaikh, Q.; Majeed, N.; Sheikh, L.; et al. Maternal characteristics and outcomes affected by hypothyroidism during pregnancy (maternal hypothyroidism on pregnancy outcomes, MHPO-1). BMC Pregnancy Childbirth 2019, 1, 476. [Google Scholar] [CrossRef]
- Yang, J.; Liu, Y.; Liu, H.; Zheng, H.; Li, X.; Zhu, L.; Wang, Z. Associations of maternal iodine status and thyroid function with adverse pregnancy outcomes in Henan Province of China. J. Trace Elements Med. Biol. 2018, 47, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Maraka, S.; Ospina, N.M.; O’Keeffe, D.T.; Espinosa, A.E.; Gionfriddo, M.R.; Erwin, P.J.; Coddington, C.C.; Stan, M.N.; Hassan, M.; Montori, V.M. Subclinical Hypothyroidism in Pregnancy: A Systematic Review and Meta-Analysis. Thyroid 2016, 4, 580–590. [Google Scholar] [CrossRef]
- Korevaar, T.I.; Chaker, L.; Jaddoe, V.W.; Visser, T.J.; Medici, M.; Peeters, R.P. Maternal and Birth Characteristics Are Determinants of Offspring Thyroid Function. J. Clin. Endocrinol. Metab. 2016, 1, 206–213. [Google Scholar] [CrossRef]
- Angermayr, L.; Clar, C. WITHDRAWN: Iodine supplementation for preventing iodine deficiency disorders in children. Cochrane Database Syst. Rev. 2018, 11, CD003819. [Google Scholar] [CrossRef]
- Vila, L.; Lucas, A.; Donnay, S.; de la Vieja, A.; Wengrovicz, S.; Santiago, P.; Bandrés, O.; Velasco, I.; Garcia-Fuentes, E.; Ares, S.; et al. Iodine nutrition status in Spain Needs for the future. Endocrinol. Diabetes Nutr. 2020, 1, 61–69. [Google Scholar] [CrossRef] [PubMed]
- García-Ascaso, M.T.; Ares-Segura, S.; Ros-Pérez, P. Is iodine nutrition in the Spanish pediatric population adequate? Historical review and current situation. Endocrinol. Diabetes Nutr. 2018, 8, 458–467. [Google Scholar] [CrossRef] [PubMed]
- García Ascaso, M.T.; Pérez, P.R.; Alcol, E.C.; López, A.L.; de Lucas Collantes, C.; Santos, I.M.; Tessier, E.; Segura, S.A. Nutritional status of iodine in children: When appropriateness relies on milk consumption and not adequate coverage of iodized salt in households. Clin. Nutr. ESPEN 2019, 30, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Vila, L.; Donnay, S.; Arena, J.; Arrizabalaga, J.J.; Pineda, J.; Garcia-Fuentes, E.; García-Rey, C.; Marín, J.L.; Serra-Prat, M.; Velasco, I.; et al. Iodine status and thyroid function among Spanish schoolchildren aged 6–7 years: The Tirokid study. Br. J. Nutr. 2016, 9, 1623–1631. [Google Scholar] [CrossRef] [PubMed]
- Harding, K.B.; Peña-Rosas, J.P.; Webster, A.C.; Yap, C.M.; Payne, B.A.; Ota, E.; De-Regil, L.M. Iodine supplementation for women during the preconception, pregnancy and postpartum period. Cochrane Database Syst. Rev. 2017, 3, CD011761. [Google Scholar] [CrossRef] [PubMed]
- WHO. Assessment of Iodine Deficiency disorders and Monitoring Their Elimination. World Health Organization: Geneva. Available online: http://apps.who.int/iris/bitstream/10665/43781/1/9789241595827_eng.pdf (accessed on 2 June 2020).
- International Council for Control of Iodine Deficiency Disorders-ICCIDD. Iodine Requirements in Pregnancy and Infancy. IDD Newsletter 2007, 23. Available online: http://www.thyroid.org/wp-content/uploads/professionals/education/IDD_NL_Feb07.pdf (accessed on 21 February 2021).
- Alexander, E.K.; Pearce, E.N.; Brent, G.A.; Brown, R.S.; Chen, H.; Dosiou, C.; Grobman, W.A.; Laurberg, P.; Lazarus, J.H.; Mandel, S.J.; et al. Guidelines of the American Thyroid Association for the Diagnosis and Management of Thyroid Disease During Pregnancy and the Postpartum. Thyroid 2017, 3, 315–389. [Google Scholar] [CrossRef]
- Endocrine Society; American Association Clinical Endocrinologists; Asia & Oceania Thyroid Association; American Thyroid Association; European Thyroid Association; Latin American Thyroid Association. Management of thyroid dysfunction during pregnancy and postpartum: An Endocrine Society Clinical Practice Guideline. Thyroid 2007, 17, 1159–1167. [Google Scholar]
- Waugh, D.T. Fluoride Exposure Induces Inhibition of Sodium/Iodide Symporter (NIS) Contributing to Impaired Iodine Absorption and Iodine Deficiency: Molecular Mechanisms of Inhibition and Implications for Public Health. Int. J. Environ. Res. Public Health 2019, 6, 1086. [Google Scholar] [CrossRef] [PubMed]
- Snart, C.J.P.; Keeble, C.; Taylor, E.; Cade, J.E.; Stewart, P.M.; Zimmermann, M.; Reid, S.; Threapleton, D.E.; Poston, L.; Myers, J.E.; et al. Maternal Iodine Status and Associations with Birth Outcomes in Three Major Cities in the United Kingdom. Nutrients 2019, 2, 441. [Google Scholar] [CrossRef]
- Martínez, M.; Soldevila, B.; Lucas, A.; Velasco, I.; Vila, L.; Puig-Domingo, M. Hypothyroidism during pregnancy and its association to perinatal and obstetric morbidity: A review. Endocrinol. Diabetes Nutr. 2018, 2, 107–113. [Google Scholar] [CrossRef]
- Moog, N.K.; Entringer, S.; Heim, C.; Wadhwa, P.D.; Kathmann, N.; Buss, C. Influence of maternal thyroid hormones during gestation on fetal brain development. Neuroscience 2017, 342, 68–100. [Google Scholar] [CrossRef]
- Lazarus, J.; Brown, R.S.; Daumerie, C.; Hubalewska-Dydejczyk, A.; Negro, R.; Vaidya, B. European thyroid association guidelines for the management of subclinical hypothyroidism in pregnancy and in children. Eur. Thyroid J. 2014, 3, 76–94. [Google Scholar] [CrossRef] [PubMed]
- Sheehan, P.M.; Nankervis, A.; Araujo, E.; Da Silva, F. Maternal Thyroid Disease and Preterm Birth: Systematic Review and Meta-Analysis. J. Clin. Endocrinol. Metab. 2015, 11, 4325–4331. [Google Scholar] [CrossRef]
- Chapman, A.K.; Farmer, Z.J.; Mastrandrea, L.D.; Matlock, K.A. Neonatal Thyroid Function and Disorders. Clin. Obstet. Gynecol. 2019, 2, 373–387. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.H.; Bestwick, J.P.; Channon, S.; Paradice, R.; Maina, A.; Rees, R.; Chiusano, E.; John, R.; Guaraldo, V.; George, L.M.; et al. Antenatal thyroid screening and childhood cognitive function. N. Engl. J. Med. 2012, 366, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Casey, B.M.; Thom, E.A.; Peaceman, A.M.; Varner, M.W.; Sorokin, Y.; Hirtz, D.G.; Reddy, U.M.; Wapner, R.J.; Thorp, J.M.; Saade, G.; et al. Treatment of Subclinical Hypothyroidism or Hypothyroxinemia in Pregnancy. N. Engl. J. Med. 2017, 376, 815–825. [Google Scholar] [CrossRef]
- Pearce, E.N.; Oken, E.; Gilman, M.W.; Lee, S.L.; Magnani, B.; Platek, D.; Braverman, L.E. Values With Thyroperoxidase Antibody Status, smoking, and multivitamin use. Endocr. Pract. 2008, 14, 33–39. [Google Scholar] [CrossRef]
- Haddow, J.E.; McClain, M.R.; Lambert-Messerlian, G.; Palomaki, G.E.; Canick, J.A.; Cleary-Goldman, J.; Malone, F.D.; Porter, T.F.; Nyberg, D.A.; Bernstein, P.; et al. Variability in thyroid-stimulating hormone suppression by human chorionic gonadotropin during early pregnancy. J. Clin. Endocrinol. Metab. 2008, 93, 3341–3347. [Google Scholar] [CrossRef]
- Korevaar, T.I.M.; Steegers, E.A.P.; de Rijke, Y.B.; Schalekamp-Timmermans, S.; Visser, W.E.; Hofman, A.; Jaddoe, V.W.; Tiemeier, H.; Visser, T.J.; Medici, M.; et al. Reference ranges and determinants of total hCG levels during pregnancy: The Generation R Study. Eur. J. Epidemiol. 2015, 30, 1057–1066. [Google Scholar] [CrossRef]
- Delgado, Y.P.; Rodríguez, G.; Samper, M.P.; Caballero, V.; Cuadrón, L.; Alvarez, M.L.; Grupo Colaborativo CALINA. Socio-cultural, obstetric and anthropometric characteristics of newborn children of mothers who smoke in Spain. An. Pediatr. 2012, 1, 4–9. [Google Scholar] [CrossRef]
- Kataoka, M.C.; Carvalheira, A.P.P.; Ferrari, A.P.; Marreto, M.; de Barros, M.A.; Garcia de Lima, C.M. Smoking during pregnancy and harm reduction in birth weight: A cross-sectional study. BMC Pregnancy Childbirth 2018, 18, 67. [Google Scholar] [CrossRef]
- Zheng, W.; Suzuki, K.; Tanaka, T.; Kohama, M.; Yamagata, Z.; Okinawa Child Health Study Group. Association between Maternal Smoking during Pregnancy and Low Birthweight: Effects by Maternal Age. PLoS ONE 2016, 11, e0146241. [Google Scholar] [CrossRef]
- Abraham, M.; Alramadhan, S.; Iniguez, C.; Duijts, L.; Jaddoe, V.W.; Den Dekker, H.T.; Crozier, S.; Godfrey, K.M.; Hindmarsh, P.; Vik, T.; et al. A systematic review of maternal smoking during pregnancy and fetal measurements with meta-analysis. PLoS ONE 2017, 2, e0170946. [Google Scholar] [CrossRef]
- Konig, F.; Andersson, M.; Hotz, K.; Aeberli, I.; Zimmerman, M.B. Ten repeat collections for urinary iodine from spot samples or 24-hour samples are needed to reliable estimate individual iodine status in women. J. Nutr. 2011, 141, 2049–2054. [Google Scholar] [CrossRef]
- Dunn, J.T.; Crutchfield, H.E.; Gutekunst, R.; Dunn, A.D. Two simple methods for measuring iodine in urine. Thyroid 1993, 3, 119–123. [Google Scholar] [CrossRef]
- Reed, A.H.; Henry, R.J.; Mason, W.B. Influence of statistical method used on the resulting estimate of normal range. Clin. Chem. 1971, 174, 275–284. [Google Scholar] [CrossRef]
- Chen, S.; Zhou, X.; Zhu, H.; Yang, H.; Gong, F.; Wang, L.; Zhang, M.; Jiang, Y.; Yan, C.; Li, J.; et al. Preconception TSH and pregnancy out-comes: A population-based cohort study in 184 611 women. Clin. Endocrinol. 2017, 6, 816–824. [Google Scholar] [CrossRef] [PubMed]
- Schneuer, F.J.; Nassar, N.; Tasevski, V.; Morris, J.M.; Roberts, C.L. Association and predictive accuracy of high TSH serum levels in first trimester and adverse pregnancy outcomes. J. Clin. Endocrinol. Metab. 2012, 9, 3115–3122. [Google Scholar] [CrossRef] [PubMed]
- Hernández, M.; López, C.; Soldevila, B.; Cecenarro, L.; Martínez-Barahona, M.; Palomera, E.; Rius, F.; Lecube, A.; Pelegay, M.J.; García, J.; et al. Impact of TSH during the first trimester of pregnancy on obstetric and foetal complications: Usefulness of 2.5 mIU/L cut-off value. Clin. Endocrinol. 2018, 5, 728–734. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Cabral, H.J.; Aschengrau, A.; Pearce, E.N. Associations Between Maternal Thyroid Function in Pregnancy and Obstetric and Perinatal Outcomes. J. Clin. Endocrinol. Metab. 2020, 5, e2015–e2023. [Google Scholar] [CrossRef] [PubMed]
- Zhao, W.; Li, X.; Xia, X.; Gao, Z.; Han, C. Iodine Nutrition During Pregnancy: Past, Present, and Future. Biol. Trace Elem. Res. 2019, 1, 196–207. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, A.C.F.; Lima, L.P.; Araújo, R.L.; Müller, G.; Rocha, R.P.; Rosenthal, D.; Carvalho, D.P. Rapid regulation of thyroid sodium–iodide symporter activity by thyrotrophin and iodine. J. Endocrinol. 2005, 184, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, I.B.; Laurberg, P.; Knudsen, N.; Jørgensen, T.; Perrild, H.; Ovesen, L.; Rasmussen, L.B. An increased incidence of overt hypothyroidism after iodine fortification of salt in Denmark: A prospective population study. J. Clin. Endocrinol. Metab. 2007, 92, 3122–3127. [Google Scholar] [CrossRef]
- Chow, C.C.; Phillips, D.I.; Lazarus, J.H.; Parkes, A.B. Effects of low doses iodide supplementation on thyroid function in potentially susceptible subjects: Are dietary iodide levels in Britain acceptable? Clin. Endocrinol. 1991, 34, 413–416. [Google Scholar] [CrossRef]
- Moleti, M.; Di Bella, B.; Giorgianni, G.; Mancuso, A.; De Vivo, A.; Alibrandi, A.; Trimarchi, F.; Vermiglio, F. Maternal thyroid function in different conditions of iodine nutrition in pregnant women exposed to mild-moderate iodine deficiency: An observational study. Clin. Endocrinol. 2011, 74, 762–768. [Google Scholar] [CrossRef]
- Ajmani, S.N.; Aggarwal, D.; Bhatia, P.; Sharma, M.; Sarabhai, V.; Paul, M. Prevalence of overt and subclinical thyroid dysfunction among pregnant women and its effect on maternal and fetal outcome. J. Obstet. Gynaecol. 2014, 2, 105–110. [Google Scholar] [CrossRef]
- Saki, F.; Dabbaghmanesh, M.H.; Ghaemi, S.Z.; Forouhari, S.; Ranjbar, G.; Bakhshayeshkaram, M. Thyroid function in pregnancy and its influences on maternal and fetal outcomes. Int. J. Endocrinol. Metab. 2014, 4, e19378. [Google Scholar] [CrossRef] [PubMed]
- Casey, B.M.; Dashe, J.S.; Wells, C.E.; McIntire, D.D.; Leveno, K.J.; Cunningham, F.G. Subclinical hyperthyroidism and pregnancy outcomes. Obstet. Gynecol. 2006, 107, 337–341. [Google Scholar] [CrossRef]
- Cohen, N.; Levy, A.; Wiznitzer, A.; Sheiner, E. Perinatal outcomes in post-thyroidectomy pregnancies. Gynecol. Endocrinol. 2011, 27, 314–318. [Google Scholar] [CrossRef]
- Wang, S.; Teng, W.P.; Li, J.X.; Wang, W.W.; Shan, Z.Y. Effects of maternal subclinical hypothyroidism on obstetrical outcomes during early pregnancy. J. Endocrinol. Investig. 2012, 35, 322–325. [Google Scholar] [CrossRef]
- Furukawa, S.; Miyakawa, K.; Shibata, J.; Iwashita, M. Women with Subclinical Hypothyroidism Are at Low Risk of Poor Pregnancy Outcome in Japan. Tohoku J. Exp. Med. 2017, 242, 167–172. [Google Scholar] [CrossRef]
- Goel, P.; Radotra, A.; Devi, K.; Malhotra, S.; Aggarwal, A.; Huria, A. Maternal and perinatal outcome in pregnancy with hypothyroidism. Indian J. Med. Sci. 2005, 59, 116–117. [Google Scholar] [CrossRef]
- Mannisto, T.; Vaarasmaki, M.; Pouta, A.; Hartikainen, A.L.; Ruokonen, A.; Surcel, H.M.; Bloigu, A.; Järvelin, M.R.; Suvanto-Luukkonen, E. Perinatal outcome of children born to mothers with thyroid dysfunction or antibodies: A prospective population-based cohort study. J. Clin. Endocrinol. Metab. 2009, 94, 772–779. [Google Scholar] [CrossRef] [PubMed]
- León, G.; Murcia, M.; Rebagliato, M.; Álvarez-Pedrerol, M.; Castilla, A.M.; Basterrechea, M.; Iñiguez, C.; Fernández-Somoano, A.; Blarduni, E.; Foradada, C.M.; et al. Maternal thyroid dysfunction during gestation, preterm delivery, and birthweight. The Infancia y Medio Ambiente Cohort, Spain. Paediatr. Perinat. Epidemiol. 2015, 2, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Derakhshan, A.; Peeters, R.P.; Taylor, P.N.; Bliddal, S.; Carty, D.M.; Meems, M.; Vaidya, B.; Chen, L.; Knight, B.A.; Ghafoor, F.; et al. Association of maternal thyroid function with birthweight: A systematic review and individual-participant data meta-analysis. Lancet Diabetes Endocrinol. 2020, 6, 501–510. [Google Scholar] [CrossRef]
- Gowachirapant, S.; Jaiswal, N.; Melse-Boonstra, A.; Galetti, V.; Stinca, S.; Mackenzie, I.; Thomas, S.; Thomas, T.; Winichagoon, P.; Srinivasan, K.; et al. Effect of iodine supplementation in pregnant women on child neurodevelopment: A randomised, double-blind, placebo-controlled trial. Lancet Diabetes Endocrinol. 2017, 11, 853–863. [Google Scholar] [CrossRef]
- Velasco, I.; Carreira, M.; Santiago, P.; Muela, J.A.; García-Fuentes, E.; Sánchez-Muñoz, B.; Garriga, M.J.; González-Fernández, M.C.; Rodríguez, A.; Caballero, F.F.; et al. Effect of iodine prophylaxis during pregnancy on neurocognitive development of children during the first two years of life. J. Clin. Endocrinol. Metab. 2009, 9, 3234–3241. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Mean ± SD or n (%) | p-Value | |
|---|---|---|
| Maternal age (years) | 30.80 ± 5.15 | |
| Advanced Maternal Age (AMA) | ||
| Yes (n = 32; 16.8%) | 37.97 ± 2.12 | 0.000 * |
| No (n = 158; 83.2%) | 29.35 ± 4.29 | |
| BMI first Trimester (Kg/m2) | 23.95 ± 4.41 | |
| Gestational age (weeks) | 39.34 ± 1.42 | |
| Gestations | ||
| 1 | 80 (42.1%) | |
| 2 | 64 (33.7%) | |
| 3 | 33 (17.4%) | |
| >3 | 13 (6.8%) | |
| Gender newborns | ||
| Male | 97 (51.05%) | |
| Female | 93 (48.95%) | |
| Newborn’s weight (g) | 3311.70 ± 428.80 | |
| Male | 3391.01 ± 440.91 | 0.009 * |
| Female | 3328.98 ± 401.66 | |
| Newborn’s length (cm) | 49.71 ± 2.11 | |
| Male | 50.22 ± 2.02 | <0.001 * |
| Female | 49.19 ± 2.09 | |
| Type of delivery | ||
| Natural | 127 (66.8%) | |
| Instrumented | 42 (22.1%) | |
| Caesarean section | 21 (11.1%) | |
| Delivery complications | ||
| None | 137 (72.1%) | |
| Loss of fetal well-being | 23 (12.1%) | |
| Prolonged second stage of labor | 19 (10%) | |
| Breech presentation | 6 (3.2%) | |
| Fetal/pelvic disproportion | 5 (2.6%) |
| n (%) | Mean ± SD | p-Value ** | |
|---|---|---|---|
| Maternal TSH in 1st trimester (mUI/L) | 190 (100%) | 2.22 ± 1.32 | |
| TSH < 4 | 160 (84.2%) | 1.78 ± 0.87 | 0.000 |
| TSH > 4 | 30 (15.8%) | 4.61 ± 0.44 | |
| Iodine supplements yes | 123 (64.7%) | 2.39 ± 1.39 | 0.013 |
| Iodine supplements no | 67 (35.3%) | 1.93 ± 1.12 | |
| Iodized salt yes | 98 (51.6%) | 2.44 ± 1.92 | 0.021 |
| Iodized salt no | 92 (48.4%) | 2.00 ± 1.16 | |
| Maternal ioduria in 1st trimester (µg/L) * | 190 (100%) | 89.15 (41.9–165.15) * | |
| Ioduria < 150 | 129 (67.9%) | 49.1 (32.1–93.9) * | 0.000 |
| Ioduria > 150 | 61 (32.1%) | 184 (166.75–217.75) * | |
| Iodine supplements yes | 123 (64.7%) | 50.2(109.7–167.65) * | 0.017 |
| Iodine supplements no | 67 (35.3%) | 49.0 (26.68–151.78) * | |
| Iodized salt yes | 98 (51.6%) | 153.65 (85.55–185.93) * | 0.000 |
| Iodized salt no | 92 (48.4%) | 46.15 (28.28–89.23) * | |
| Newborn’s weight (g) | 190 (100%) | 3311.7 ± 428.8 | |
| Smokers | 70 (36.8%) | 3165.5 ± 402.9 | 0.014 |
| Non-smokers | 120 (63.2%) | 3355.5 ± 410.3 | |
| Non-smokers | |||
| Iodine supplements yes | 73 (60.8%) | 3400.59 ± 429.69 | 0.134 |
| Iodine supplements no | 47 (39.2%) | 3255.53 ± 371.87 | |
| Iodized salt yes | 64 (53.3%) | 3388.36 ± 417.43 | 0.351 |
| Iodized salt no | 56 (46.7%) | 3318.00 ± 402.33 | |
| Smokers | |||
| Iodine supplements yes | 50 (71.4%) | 3249.80 ± 447.37 | 0.702 |
| Iodine supplements no | 20 (28.6%) | 3203.50 ± 473.25 | |
| Iodized salt yes | 34 (48.6%) | 3279.58 ± 537.01 | 0.417 |
| Iodized salt no | 36 (51.4%) | 3191.00 ± 347.12 | |
| Newborn’s length (cm) | 190 (100%) | 49.71 ± 2.11 | |
| Smokers | 70 (36.8%) | 49.1 ± 1.81 | 0.030 |
| Non-smokers | 120 (63.2%) | 49.9 ± 1.96 | |
| Non-smokers | |||
| Iodine supplements yes | 73 (60.8%) | 49.97 ± 2.00 | 0.576 |
| Iodine supplements no | 47 (39.2%) | 49.77 ± 1.89 | |
| Iodized salt yes | 64 (53.3%) | 49.90 ± 2.00 | 0.961 |
| Iodized salt no | 56 (46.7%) | 49.88 ± 1.92 | |
| Smokers | |||
| Iodine supplements yes | 50 (71.4%) | 49.46 ± 2.13 | 0.784 |
| Iodine supplements no | 20 (28.6%) | 49.29 ± 2.84 | |
| Iodized salt yes | 34 (48.6%) | 49.5 ±2.93 | 0.735 |
| Iodized salt no | 36 (51.4%) | 49.31 ± 1.50 | |
| APGAR 1 min | 190 (100%) | 9.53 ± 0.91 | |
| Maternal ioduria < 150 | 129 (67.9%) | 9.33 ± 1.03 | 0.000 |
| Maternal ioduria > 150 | 61 (32.1%) | 9.95 ± 0.22 | |
| Maternal TSH < 4 | 160 (84.2%) | 9.45 ± 0.96 | 0.000 |
| Maternal TSH > 4 | 30 (15.8%) | 9.97 ± 0.18 | |
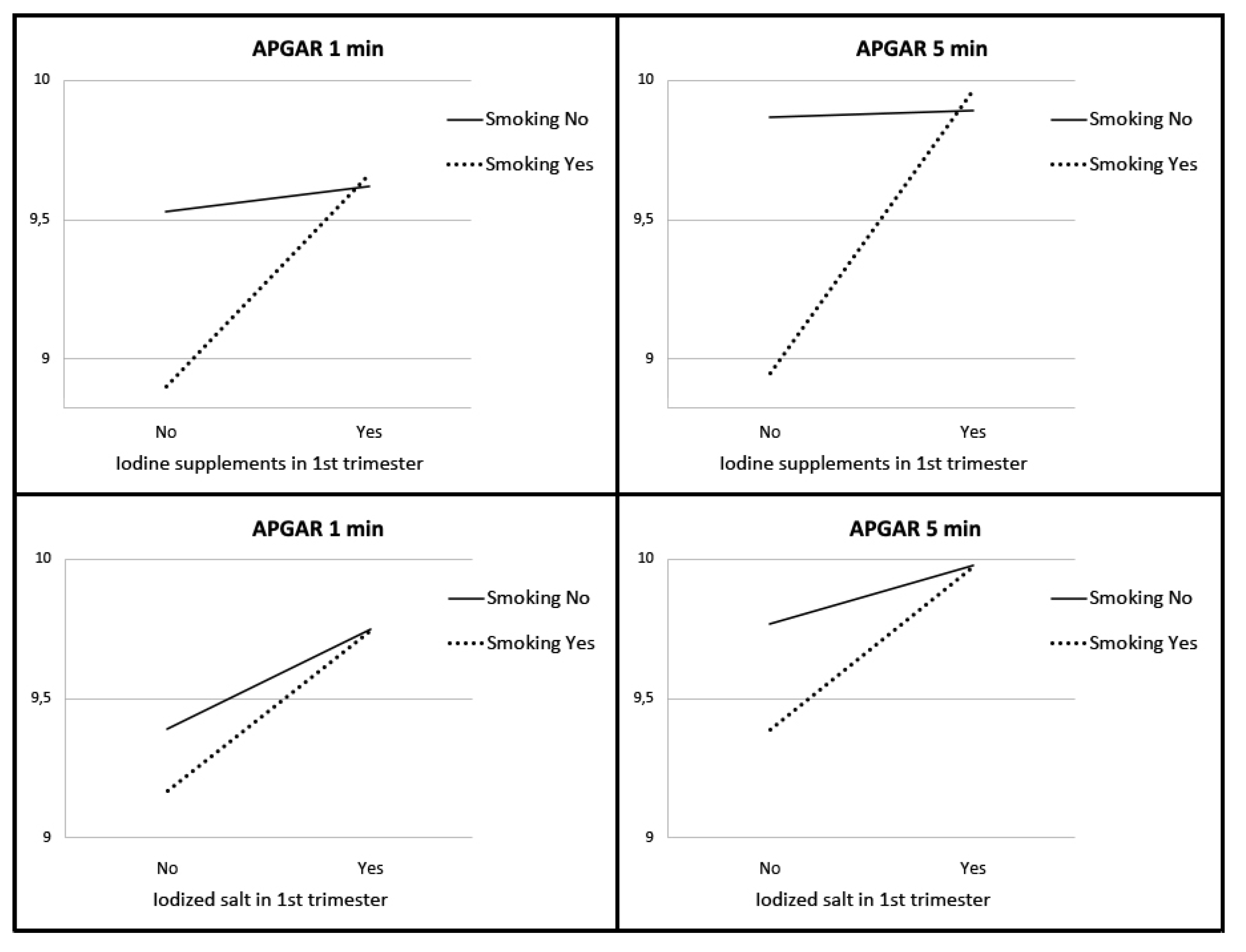
| Iodine supplements yes | 123 (64.7%) | 9.63 ± 0.87 | 0.034 |
| Iodine supplements no | 67 (35.3%) | 9.34 ± 0.95 | |
| Iodized salt yes | 98 (51.6%) | 9.74 ± 0.48 | 0.001 |
| Iodized salt no | 92 (48.4%) | 9.30 ± 1.17 | |
| Non-smokers | |||
| Iodine supplements yes | 73 (60.8%) | 9.62 ± 1.02 | 0.615 |
| Iodine supplements no | 47 (39.2%) | 9.53 ± 0.65 | |
| Iodized salt yes | 64 (53.3%) | 9.75 ± 0.47 | 0.028 |
| Iodized salt no | 56 (46.7%) | 9.39 ± 1.19 | |
| Smokers | |||
| Iodine supplements yes | 50 (71.4%) | 9.66 ± 0.59 | 0.001 |
| Iodine supplements no | 20 (28.6%) | 8.90 ± 1.33 | |
| Iodized salt yes | 34 (48.6%) | 9.74 ± 0.51 | 0.009 |
| Iodized salt no | 36 (51.4%) | 9.17 ± 1.13 | |
| APGAR 5 min | 190 (100%) | 9.81 ± 0.91 | |
| Maternal ioduria < 150 | 129 (67.9%) | 9.71 ± 1.1 | 0.004 |
| Maternal ioduria > 150 | 61 (32.1%) | 10.0 ± 0.0 | |
| Maternal TSH < 4 | 160 (84.2%) | 9.77 ± 0.99 | 0.004 |
| Maternal TSH > 4 | 30 (15.8%) | 10.0 ± 0.0 | |
| Iodine supplements yes | 123 (64.7%) | 9.92 ± 0.51 | 0.020 |
| Iodine supplements no | 67 (35.3%) | 9.60 ± 1.36 | |
| Iodized salt yes | 98 (51.6%) | 9.98 ± 0.14 | 0.006 |
| Iodized salt no | 92 (48.4%) | 9.62 ± 1.28 | |
| Non-smokers | |||
| Iodine supplements yes | 73 (60.8%) | 9.89 ± 0.64 | 0.858 |
| Iodine supplements no | 47 (39.2%) | 9.87 ± 0.34 | |
| Iodized salt yes | 64 (53.3%) | 9.98 ± 0.13 | 0.027 |
| Iodized salt no | 56 (46.7%) | 9.77 ± 0.76 | |
| Smokers | |||
| Iodine supplements yes | 50 (71.4%) | 9.96 ± 0.20 | 0.003 |
| Iodine supplements no | 20 (28.6%) | 8.95 ± 2.35 | |
| Iodized salt yes | 34 (48.6%) | 9.97 ± 0.17 | 0.066 |
| Iodized salt no | 36 (51.4%) | 9.39 ± 1.81 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murillo-Llorente, M.T.; Llorca-Colomer, F.; Pérez-Bermejo, M. Relationship between Thyroid Status during the First Trimester of Pregnancy and Neonatal Well-Being. Nutrients 2021, 13, 872. https://doi.org/10.3390/nu13030872
Murillo-Llorente MT, Llorca-Colomer F, Pérez-Bermejo M. Relationship between Thyroid Status during the First Trimester of Pregnancy and Neonatal Well-Being. Nutrients. 2021; 13(3):872. https://doi.org/10.3390/nu13030872
Chicago/Turabian StyleMurillo-Llorente, Maria Teresa, Francisco Llorca-Colomer, and Marcelino Pérez-Bermejo. 2021. "Relationship between Thyroid Status during the First Trimester of Pregnancy and Neonatal Well-Being" Nutrients 13, no. 3: 872. https://doi.org/10.3390/nu13030872
APA StyleMurillo-Llorente, M. T., Llorca-Colomer, F., & Pérez-Bermejo, M. (2021). Relationship between Thyroid Status during the First Trimester of Pregnancy and Neonatal Well-Being. Nutrients, 13(3), 872. https://doi.org/10.3390/nu13030872