Adherence to the World Cancer Research Fund/American Institute for Cancer Research Recommendations and the Risk of Breast Cancer

 , , , ,
, , , ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Data Collection
2.2. WCRF/AICR Score
2.3. Statistical Analysis
2.4. Meta-Analysis
3. Results
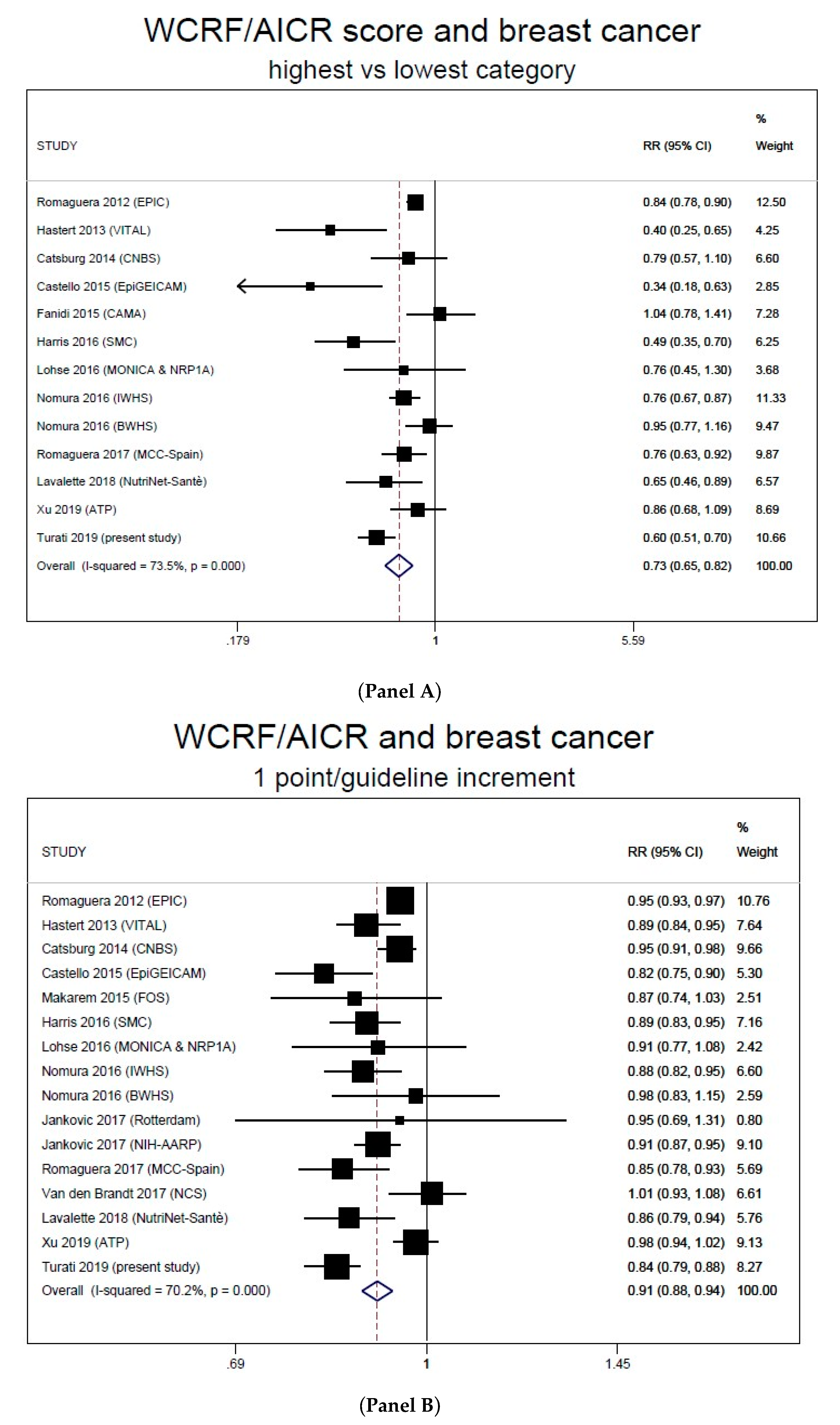
Meta-Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Islami, F.; Goding Sauer, A.; Miller, K.D.; Siegel, R.L.; Fedewa, S.A.; Jacobs, E.J.; McCullough, M.L.; Patel, A.V.; Ma, J.; Soerjomataram, I.; et al. Proportion and number of cancer cases and deaths attributable to potentially modifiable risk factors in the United States. CA Cancer J. Clin. 2018, 68, 31–54. [Google Scholar] [CrossRef] [PubMed]
- Gapstur, S.M.; Drope, J.M.; Jacobs, E.J.; Teras, L.R.; McCullough, M.L.; Douglas, C.E.; Patel, A.V.; Wender, R.C.; Brawley, O.W. A blueprint for the primary prevention of cancer: Targeting established, modifiable risk factors. CA Cancer J. Clin. 2018, 68, 446–470. [Google Scholar] [CrossRef] [PubMed]
- La Vecchia, C.; Giordano, S.H.; Hortobagyi, G.N.; Chabner, B. Overweight, obesity, diabetes, and risk of breast cancer: Interlocking pieces of the puzzle. Oncologist 2011, 16, 726–729. [Google Scholar] [CrossRef] [PubMed]
- Chan, D.S.M.; Abar, L.; Cariolou, M.; Nanu, N.; Greenwood, D.C.; Bandera, E.V.; McTiernan, A.; Norat, T. World Cancer Research Fund International: Continuous Update Project-systematic literature review and meta-analysis of observational cohort studies on physical activity, sedentary behavior, adiposity, and weight change and breast cancer risk. Cancer Causes Control. 2019, 30, 1183–1200. [Google Scholar] [CrossRef]
- Mourouti, N.; Kontogianni, M.D.; Papavagelis, C.; Panagiotakos, D.B. Diet and breast cancer: A systematic review. Int. J. Food Sci. Nutr. 2015, 66, 1–42. [Google Scholar] [CrossRef]
- Bagnardi, V.; Rota, M.; Botteri, E.; Tramacere, I.; Islami, F.; Fedirko, V.; Scotti, L.; Jenab, M.; Turati, F.; Pasquali, E.; et al. Alcohol consumption and site-specific cancer risk: A comprehensive dose-response meta-analysis. Br. J. Cancer 2015, 112, 580–593. [Google Scholar] [CrossRef]
- Van den Brandt, P.A.; Schulpen, M. Mediterranean diet adherence and risk of postmenopausal breast cancer: Results of a cohort study and meta-analysis. Int. J. Cancer 2017, 140, 2220–2231. [Google Scholar] [CrossRef]
- Turati, F.; Carioli, G.; Bravi, F.; Ferraroni, M.; Serraino, D.; Montella, M.; Giacosa, A.; Toffolutti, F.; Negri, E.; Levi, F.; et al. Mediterranean Diet and Breast Cancer Risk. Nutrients 2018, 10, 326. [Google Scholar] [CrossRef]
- Xiao, Y.; Xia, J.; Li, L.; Ke, Y.; Cheng, J.; Xie, Y.; Chu, W.; Cheung, P.; Kim, J.H.; Colditz, G.A.; et al. Associations between dietary patterns and the risk of breast cancer: A systematic review and meta-analysis of observational studies. Breast Cancer Res. 2019, 21, 16. [Google Scholar] [CrossRef]
- Grosso, G.; Bella, F.; Godos, J.; Sciacca, S.; Del Rio, D.; Ray, S.; Galvano, F.; Giovannucci, E.L. Possible role of diet in cancer: Systematic review and multiple meta-analyses of dietary patterns, lifestyle factors, and cancer risk. Nutr. Rev. 2017, 75, 405–419. [Google Scholar] [CrossRef] [PubMed]
- Hou, R.; Wei, J.; Hu, Y.; Zhang, X.; Sun, X.; Chandrasekar, E.K.; Voruganti, V.S. Healthy dietary patterns and risk and survival of breast cancer: A meta-analysis of cohort studies. Cancer Causes Control. 2019, 30, 835–846. [Google Scholar] [CrossRef] [PubMed]
- World Cancer Research Fund/American Institute for Cancer Research. Food, Nutrition, Physical Activity, and the Prevention of Cancer: A Global Perspective; AICR: Washington, DC, USA, 2007. [Google Scholar]
- World Cancer Research Fund/American Institute for Cancer Research. Diet, Nutrition, Physical Activity and Cancer: A Global Perspective. Continuous Update Project Expert Report 2018. Available online: Dietandcancerreport.org (accessed on 1 October 2019).
- Clinton, S.K.; Giovannucci, E.L.; Hursting, S.D. The World Cancer Research Fund/American Institute for Cancer Research Third Expert Report on Diet, Nutrition, Physical Activity, and Cancer: Impact and Future Directions. J. Nutr. 2019. [Google Scholar] [CrossRef] [PubMed]
- Kohler, L.N.; Garcia, D.O.; Harris, R.B.; Oren, E.; Roe, D.J.; Jacobs, E.T. Adherence to Diet and Physical Activity Cancer Prevention Guidelines and Cancer Outcomes: A Systematic Review. Cancer Epidemiol. Biomark. Prev. 2016, 25, 1018–1028. [Google Scholar] [CrossRef]
- Lohse, T.; Faeh, D.; Bopp, M.; Rohrmann, S.; Swiss National Cohort Study Group. Adherence to the cancer prevention recommendations of the World Cancer Research Fund/American Institute for Cancer Research and mortality: A census-linked cohort. Am. J. Clin. Nutr. 2016, 104, 678–685. [Google Scholar] [CrossRef]
- Fanidi, A.; Ferrari, P.; Biessy, C.; Ortega, C.; Angeles-Llerenas, A.; Torres-Mejia, G.; Romieu, I. Adherence to the World Cancer Research Fund/American Institute for Cancer Research cancer prevention recommendations and breast cancer risk in the Cancer de Mama (CAMA) study. Public Health Nutr. 2015, 18, 3337–3348. [Google Scholar] [CrossRef]
- Romaguera, D.; Vergnaud, A.C.; Peeters, P.H.; van Gils, C.H.; Chan, D.S.; Ferrari, P.; Romieu, I.; Jenab, M.; Slimani, N.; Clavel-Chapelon, F.; et al. Is concordance with World Cancer Research Fund/American Institute for Cancer Research guidelines for cancer prevention related to subsequent risk of cancer? Results from the EPIC study. Am. J. Clin. Nutr. 2012, 96, 150–163. [Google Scholar] [CrossRef]
- Nomura, S.J.; Inoue-Choi, M.; Lazovich, D.; Robien, K. WCRF/AICR recommendation adherence and breast cancer incidence among postmenopausal women with and without non-modifiable risk factors. Int. J. Cancer 2016, 138, 2602–2615. [Google Scholar] [CrossRef]
- Nomura, S.J.; Dash, C.; Rosenberg, L.; Yu, J.; Palmer, J.R.; Adams-Campbell, L.L. Adherence to diet, physical activity and body weight recommendations and breast cancer incidence in the Black Women’s Health Study. Int. J. Cancer 2016, 139, 2738–2752. [Google Scholar] [CrossRef]
- Harris, H.R.; Bergkvist, L.; Wolk, A. Adherence to the World Cancer Research Fund/American Institute for Cancer Research recommendations and breast cancer risk. Int. J. Cancer 2016, 138, 2657–2664. [Google Scholar] [CrossRef]
- Catsburg, C.; Miller, A.B.; Rohan, T.E. Adherence to cancer prevention guidelines and risk of breast cancer. Int. J. Cancer 2014, 135, 2444–2452. [Google Scholar] [CrossRef] [PubMed]
- Hastert, T.A.; Beresford, S.A.; Patterson, R.E.; Kristal, A.R.; White, E. Adherence to WCRF/AICR cancer prevention recommendations and risk of postmenopausal breast cancer. Cancer Epidemiol. Biomark. Prev. 2013, 22, 1498–1508. [Google Scholar] [CrossRef] [PubMed]
- Franceschi, S.; Favero, A.; La Vecchia, C.; Negri, E.; Dal Maso, L.; Salvini, S.; Decarli, A.; Giacosa, A. Influence of food groups and food diversity on breast cancer risk in Italy. Int. J. Cancer 1995, 63, 785–789. [Google Scholar] [CrossRef] [PubMed]
- Levi, F.; Pasche, C.; Lucchini, F.; La Vecchia, C. Dietary intake of selected micronutrients and breast-cancer risk. Int. J. Cancer 2001, 91, 260–263. [Google Scholar] [CrossRef]
- Decarli, A.; Franceschi, S.; Ferraroni, M.; Gnagnarella, P.; Parpinel, M.T.; La Vecchia, C.; Negri, E.; Salvini, S.; Falcini, F.; Giacosa, A. Validation of a food-frequency questionnaire to assess dietary intakes in cancer studies in Italy. Results for specific nutrients. Ann. Epidemiol. 1996, 6, 110–118. [Google Scholar] [CrossRef]
- Franceschi, S.; Negri, E.; Salvini, S.; Decarli, A.; Ferraroni, M.; Filiberti, R.; Giacosa, A.; Talamini, R.; Nanni, O.; Panarello, G.; et al. Reproducibility of an Italian food frequency questionnaire for cancer studies: Results for specific food items. Eur. J. Cancer 1993, 29A, 2298–2305. [Google Scholar] [CrossRef]
- Gnagnarella, P.; Parpinel, M.; Salvini, S.; Franceschi, S.; Palli, D.; Boyle, P. The update of the Italian food composition database. J. Food Comp. Anal. 2004, 17, 509–522. [Google Scholar] [CrossRef]
- Salvini, S.; Parpinel, M.; Gnagnarella, P.; Maisonneuve, P.; Turrini, A. Banca di Composizione Degli Alimenti per Studi Epidemiologici in Italia; Istituto Europeo di Oncologia: Milano, Italy, 1998. [Google Scholar]
- Shams-White, M.M.; Brockton, N.T.; Mitrou, P.; Romaguera, D.; Brown, S.; Bender, A.; Kahle, L.L.; Reedy, J. Operationalizing the 2018 World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) Cancer Prevention Recommendations: A Standardized Scoring System. Nutrients 2019, 11, 1572. [Google Scholar] [CrossRef]
- Turati, F.; Bravi, F.; Di Maso, M.; Bosetti, C.; Polesel, J.; Serraino, D.; Dalmartello, M.; Giacosa, A.; Montella, M.; Tavani, A.; et al. Adherence to the World Cancer Research Fund/American Institute for Cancer Research recommendations and colorectal cancer risk. Eur. J. Cancer 2017, 85, 86–94. [Google Scholar] [CrossRef]
- Bravi, F.; Polesel, J.; Garavello, W.; Serraino, D.; Negri, E.; Franchin, G.; La Vecchia, C.; Bosetti, C. Adherence to the World Cancer Research Fund/American Institute for Cancer Research recommendations and head and neck cancers risk. Oral. Oncol. 2017, 64, 59–64. [Google Scholar] [CrossRef]
- Lucas, A.L.; Bravi, F.; Boffetta, P.; Polesel, J.; Serraino, D.; La Vecchia, C.; Bosetti, C. Adherence to World Cancer Research Fund/American Institute for Cancer Research recommendations and pancreatic cancer risk. Cancer Epidemiol. 2016, 40, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Bruzzi, P.; Green, S.B.; Byar, D.P.; Brinton, L.A.; Schairer, C. Estimating the population attributable risk for multiple risk factors using case-control data. Am. J. Epidemiol. 1985, 122, 904–914. [Google Scholar] [CrossRef] [PubMed]
- Lavalette, C.; Adjibade, M.; Srour, B.; Sellem, L.; Fiolet, T.; Hercberg, S.; Latino-Martel, P.; Fassier, P.; Deschasaux, M.; Kesse-Guyot, E.; et al. Cancer-Specific and General Nutritional Scores and Cancer Risk: Results from the Prospective NutriNet-Santé Cohort. Cancer Res. 2018, 78, 4427–4435. [Google Scholar] [CrossRef] [PubMed]
- Castello, A.; Martin, M.; Ruiz, A.; Casas, A.M.; Baena-Canada, J.M.; Lope, V.; Antolin, S.; Sanchez, P.; Ramos, M.; Anton, A.; et al. Lower Breast Cancer Risk among Women following the World Cancer Research Fund and American Institute for Cancer Research Lifestyle Recommendations: EpiGEICAM Case-Control Study. PLoS ONE 2015, 10, e0126096. [Google Scholar] [CrossRef] [PubMed]
- Makarem, N.; Lin, Y.; Bandera, E.V.; Jacques, P.F.; Parekh, N. Concordance with World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) guidelines for cancer prevention and obesity-related cancer risk in the Framingham Offspring cohort (1991–2008). Cancer Causes Control 2015, 26, 277–286. [Google Scholar] [CrossRef]
- Jankovic, N.; Geelen, A.; Winkels, R.M.; Mwungura, B.; Fedirko, V.; Jenab, M.; Illner, A.K.; Brenner, H.; Ordonez-Mena, J.M.; Kiefte de Jong, J.C.; et al. Adherence to the WCRF/AICR Dietary Recommendations for Cancer Prevention and Risk of Cancer in Elderly from Europe and the United States: A Meta-Analysis within the CHANCES Project. Cancer Epidemiol. Biomark. Prev. 2017, 26, 136–144. [Google Scholar] [CrossRef]
- Romaguera, D.; Gracia-Lavedan, E.; Molinuevo, A.; de Batlle, J.; Mendez, M.; Moreno, V.; Vidal, C.; Castello, A.; Perez-Gomez, B.; Martin, V.; et al. Adherence to nutrition-based cancer prevention guidelines and breast, prostate and colorectal cancer risk in the MCC-Spain case-control study. Int. J. Cancer 2017, 141, 83–93. [Google Scholar] [CrossRef]
- Xu, J.Y.; Vena, J.E.; Whelan, H.K.; Robson, P.J. Impact of adherence to cancer-specific prevention recommendations on subsequent risk of cancer in participants in Alberta’s Tomorrow Project. Public Health Nutr. 2019, 22, 235–245. [Google Scholar] [CrossRef]
- Karavasiloglou, N.; Husing, A.; Masala, G.; van Gils, C.H.; Turzanski Fortner, R.; Chang-Claude, J.; Huybrechts, I.; Weiderpass, E.; Gunter, M.; Arveux, P.; et al. Adherence to the World Cancer Research Fund/American Institute for Cancer Research cancer prevention recommendations and risk of in situ breast cancer in the European Prospective Investigation into Cancer and Nutrition (EPIC) cohort. BMC Med. 2019, 17, 221. [Google Scholar] [CrossRef]
- Greenland, S. Quantitative methods in the review of epidemiologic literature. Epidemiol. Rev. 1987, 9, 1–30. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef] [PubMed]
- Solans, M.; Romaguera, D.; Gracia-Lavedan, E.; Molinuevo, A.; Benavente, Y.; Saez, M.; Marcos-Gragera, R.; Costas, L.; Robles, C.; Alonso, E.; et al. Adherence to the 2018 WCRF/AICR cancer prevention guidelines and chronic lymphocytic leukemia in the MCC-Spain study. Cancer Epidemiol. 2019, 64, 101629. [Google Scholar] [CrossRef] [PubMed]
- Petimar, J.; Smith-Warner, S.A.; Rosner, B.; Chan, A.T.; Giovannucci, E.L.; Tabung, F.K. Adherence to the World Cancer Research Fund/American Institute for Cancer Research 2018 Recommendations for Cancer Prevention and Risk of Colorectal Cancer. Cancer Epidemiol. Biomark. Prev. 2019, 28, 1469–1479. [Google Scholar] [CrossRef]
- El Kinany, K.; Huybrechts, I.; Kampman, E.; Boudouaya, H.A.; Hatime, Z.; Mint Sidi Deoula, M.; El Asri, A.; Benslimane, A.; Nejjari, C.; Ibrahimi, S.A.; et al. Concordance with the World Cancer Research Fund/American Institute for Cancer Research recommendations for cancer prevention and colorectal cancer risk in Morocco: A large, population-based case-control study. Int. J. Cancer 2019, 145, 1829–1837. [Google Scholar] [CrossRef]
- Bagnardi, V.; Rota, M.; Botteri, E.; Tramacere, I.; Islami, F.; Fedirko, V.; Scotti, L.; Jenab, M.; Turati, F.; Pasquali, E.; et al. Light alcohol drinking and cancer: A meta-analysis. Ann. Oncol. 2013, 24, 301–308. [Google Scholar] [CrossRef]
- Hodge, A.M.; Bassett, J.K.; Milne, R.L.; English, D.R.; Giles, G.G. Consumption of sugar-sweetened and artificially sweetened soft drinks and risk of obesity-related cancers. Public Health Nutr. 2018, 21, 1618–1626. [Google Scholar] [CrossRef]
- Boyle, P.; Koechlin, A.; Autier, P. Sweetened carbonated beverage consumption and cancer risk: Meta-analysis and review. Eur. J. Cancer Prev. 2014, 23, 481–490. [Google Scholar] [CrossRef]
- Thomson, C.A.; McCullough, M.L.; Wertheim, B.C.; Chlebowski, R.T.; Martinez, M.E.; Stefanick, M.L.; Rohan, T.E.; Manson, J.E.; Tindle, H.A.; Ockene, J.; et al. Nutrition and physical activity cancer prevention guidelines, cancer risk, and mortality in the women’s health initiative. Cancer Prev. Res. (Phila) 2014, 7, 42–53. [Google Scholar] [CrossRef]
- Kabat, G.C.; Matthews, C.E.; Kamensky, V.; Hollenbeck, A.R.; Rohan, T.E. Adherence to cancer prevention guidelines and cancer incidence, cancer mortality, and total mortality: A prospective cohort study. Am. J. Clin. Nutr. 2015, 101, 558–569. [Google Scholar] [CrossRef]
- Mullooly, M.; Khodr, Z.G.; Dallal, C.M.; Nyante, S.J.; Sherman, M.E.; Falk, R.; Liao, L.M.; Love, J.; Brinton, L.A.; Gierach, G.L. Epidemiologic Risk Factors for In Situ and Invasive Breast Cancers Among Postmenopausal Women in the National Institutes of Health-AARP Diet and Health Study. Am. J. Epidemiol. 2017, 186, 1329–1340. [Google Scholar] [CrossRef] [PubMed]
- World Cancer Research Fund International/American Institute for Cancer Research. Continuous Update Project Report: Diet, Nutrition, Physical Activity and Breast Cancer. 2017. Available online: Wcrf.org/breast-cancer–2017 (accessed on 27 November 2019).
- Edefonti, V.; Randi, G.; La Vecchia, C.; Ferraroni, M.; Decarli, A. Dietary patterns and breast cancer: A review with focus on methodological issues. Nutr. Rev. 2009, 67, 297–314. [Google Scholar] [CrossRef] [PubMed]
- Franceschi, S.; Barbone, F.; Negri, E.; Decarli, A.; Ferraroni, M.; Filiberti, R.; Giacosa, A.; Gnagnarella, P.; Nanni, O.; Salvini, S.; et al. Reproducibility of an Italian food frequency questionnaire for cancer studies. Results for specific nutrients. Ann. Epidemiol. 1995, 5, 69–75. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | Cases | Controls |
|---|---|---|
| n (%) | n (%) | |
| Centre | ||
| Pordenone/Gorizia | 1046 (34.5) | 1015 (29.9) |
| Milan | 585 (19.3) | 623 (18.4) |
| Genoa | 290 (9.6) | 310 (9.1) |
| Forlì | 212 (7.0) | 213 (6.3) |
| Naples | 258 (8.5) | 249 (7.3) |
| Rome/Latina | 178 (5.9) | 178 (5.3) |
| Switzerland | 465 (15.3) | 804 (23.7) |
| Age group | ||
| <45 | 562 (18.5) | 686 (20.2) |
| 45–54 | 898 (29.6) | 870 (25.7) |
| 55–64 | 912 (30.1) | 978 (28.8) |
| ≥65 | 662 (21.8) | 858 (25.3) |
| Menopausal status a | ||
| Premenopause | 1150 (38.0) | 1180 (34.8) |
| Postmenopause | 1880 (62.1) | 2212 (65.2) |
| Education (years) a | ||
| <7 | 1273 (42.2) | 1583 (47.0) |
| 7–11 | 972 (32.2) | 1120 (33.2) |
| ≥12 | 775 (25.7) | 666 (19.8) |
| Parity a | ||
| Nulliparae | 504 (16.6) | 597 (17.6) |
| 1 | 676 (22.3) | 688 (20.3) |
| 2 | 1163 (38.4) | 1179 (34.8) |
| ≥3 | 688 (22.7) | 926 (27.3) |
| Family history of breast cancer in first-degree relatives | ||
| No | 2724 (89.8) | 3249 (95.8) |
| Yes | 310 (10.2) | 143 (4.2) |
| Cases (%) | Controls (%) | OR (95% CI) a | OR (95% CI) b | |
|---|---|---|---|---|
| R1—Be a healthy weight c | ||||
| 0 | 505 (16.7) | 589 (17.4) | 1.00 d | 1.00d |
| 0.5 | 960 (31.7) | 1128 (33.3) | 0.99 (0.85–1.15) | 0.97 (0.83–1.13) |
| 0.5 | 1562 (51.6) | 1667 (49.3) | 1.01 (0.88–1.17) | 0.99 (0.86–1.15) |
| ptrend | 0.763 | 0.984 | ||
| R2—Be physically active c | ||||
| 0 | 223 (7.4) | 149 (4.4) | 1.00 d | 1.00 d |
| 0.5 | 2098 (69.4) | 2207 (65.5) | 0.75 (0.60–0.94) | 0.76 (0.60–0.95) |
| 1 | 702 (23.2) | 1016 (30.1) | 0.60 (0.47–0.76) | 0.61 (0.48–0.78) |
| ptrend | <0.001 | <0.001 | ||
| R3—Eat a diet rich in wholegrains vegetables fruit and beans | ||||
| <0.5 | 356 (11.7) | 452 (13.3) | 1.00 d | 1.00 d |
| 0.5–<1 | 2176 (71.7) | 2421 (71.4) | 1.03 (0.88–1.20) | 0.79 (0.66–0.94) |
| 1 | 502 (16.5) | 519 (15.3) | 1.03 (0.85–1.25) | 0.63 (0.50–0.80) |
| ptrend | 0.793 | <0.001 | ||
| R4—Limit consumption of fast foods and other processed food high in fat starches or sugar | ||||
| 0 | 456 (15.0) | 419 (12.4) | 1.00 d | 1.00 d |
| 0.5 | 1752 (57.7) | 1807 (53.3) | 0.90 (0.78–1.05) | 0.95 (0.81–1.11) |
| 1 | 826 (27.2) | 1166 (34.4) | 0.67 (0.57–0.79) | 0.75 (0.63–0.90) |
| ptrend | <0.001 | <0.001 | ||
| R5—Limit consumption of red meat and processed meat | ||||
| 0 | 2236 (73.7) | 2451 (72.3) | 1.00 d | 1.00 d |
| 0.5 | 655 (21.6) | 703 (20.7) | 0.91 (0.80–1.03) | 1.04 (0.91–1.19) |
| 1 | 143 (4.7) | 238 (7.0) | 0.66 (0.53–0.82) | 0.81 (0.64–1.02) |
| ptrend | <0.001 | 0.329 | ||
| R6—Limit consumption of sugar sweetened drinks c | ||||
| 0 | 187 (6.2) | 148 (4.4) | 1.00 d | 1.00 d |
| 0.5 | 1147 (37.8) | 1216 (35.8) | 0.72 (0.57–0.91) | 0.74 (0.58–0.94) |
| 1 | 1700 (56.0) | 2028 (59.8) | 0.61 (0.48–0.76) | 0.68 (0.53–0.86) |
| ptrend | <0.001 | 0.003 | ||
| R7—Limit alcohol consumption | ||||
| 0 | 1081 (35.7) | 989 (29.2) | 1.00 d | 1.00 d |
| 0.5 | 937 (30.9) | 937 (27.7) | 0.92 (0.81–1.05) | 0.91 (0.80–1.04) |
| 1 | 1014 (33.4) | 1462 (43.2) | 0.70 (0.62–0.79) | 0.74 (0.65–0.84) |
| ptrend | <0.001 | <0.001 | ||
| S1—For mothers, breastfeed if you can c | ||||
| 0 | 1083 (35.8) | 1194 (35.3) | 1.00 d | 1.00 d |
| 0.5 | 602 (19.9) | 571 (16.9) | 1.09 (0.95–1.26) | 1.02 (0.86–1.20) |
| 0.5 | 1342 (44.3) | 1613 (47.8) | 0.97 (0.86–1.08) | 0.96 (0.83–1.11) |
| ptrend | 0.512 | 0.496 |
| Cases (%) | Controls (%) | OR (95% CI) a | OR (95% CI) b | |
|---|---|---|---|---|
| Overall WCRF/AICR score c | ||||
| ≤4.25 | 1103 (36.7) | 939 (28.1) | 1.00 d | 1.00 d |
| >4.25–<4.75 | 577 (19.2) | 676 (20.2) | 0.74 (0.64–0.85) | 0.75 (0.65–0.87) |
| 4.75–<5.5 | 838 (27.9) | 964 (28.8) | 0.76 (0.67–0.87) | 0.79 (0.69–0.90) |
| ≥5.5 | 490 (16.3) | 768 (22.9) | 0.57 (0.49–0.66) | 0.60 (0.51–0.70) |
| ptrend | <0.001 | <0.001 | ||
| WCRF, a increment unit | 0.82 (0.78–0.86) | 0.83 (0.79–0.88) | ||
| Diet WCRF/AICR score c | ||||
| <2.25 | 744 (24.5) | 636 (18.8) | 1.00 d | 1.00 d |
| 2.25–3 | 1183 (39.0) | 1231 (36.3) | 0.82 (0.72–0.94) | 0.84 (0.73–0.96) |
| 3–3.5 | 603 (19.9) | 787 (23.2) | 0.66 (0.57–0.77) | 0.71 (0.60–0.83) |
| >3.5 | 502 (16.6) | 734 (21.7) | 0.58 (0.49–0.68) | 0.62 (0.53–0.73) |
| ptrend | <0.001 | <0.001 |
| Author | Region | Study Design | Study Period | BC Cases/Person at Risk or Controls | Recommendations ǁ in the WCRF/AICR Score | Extreme Categories Compared | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | ||||||
| Romaguera 2012 [19] | Europe | Cohort EPIC | from 1992 mean f-u: 11 yrs | 9358/386,355 | x | x | x | x | x | x | x | 6–7 vs. 0–3 | ||
| Hastert 2013 [24] | USA | Cohort VITAL | 2000–2008 | 899/30,797 postmenopausal | x | x | x | x | x | x | 5–6 vs. 0 | |||
| Catsburg 2014 [23] | Canada | Cohort NBSS | 1982–2000 | 2503/49,613 | x | x | x | x | x | x | x | 6–7 vs. 0–1 | ||
| Castello 2015 [37] | Spain | Case–control EpiGEICAM | 2006–2011 | 973/973 | x | x | x | x | x | x | x | x | 0–<3 vs. 6–9 § | |
| Fanidi 2015 [18] | Mexico | Case–control CAMA | 2004–2007 | 1000/1074 | x | x | x | x | x | x | x | IV vs. I (<3.25) quartile | ||
| Makarem 2015 [38] | USA | Cohort FOS | 1991–2008 | 124/2983 | x | x | x | x | x | x | x | NA ¥ | ||
| Harris 2016 [22] | Sweden | Cohort SMC | 1997–2012 | 1388/31,514 mostly postmenopausal | x | x | x | x | x | x | x | x | 6–7 vs. 0–2 | |
| Lohse 2016 [17] | Switzerland | Cohort MONICA & NRP1A | MONICA: from 1983 NRP1A: from 1977 mean f-u: 21.7 yrs | 1332 */16,722 * deaths from BC | x | x | x | x | x | x | x | 5–9 vs. 0–3.5 | ||
| Nomura 2016 [20] | USA | Cohort IWHS | 1986–2010 | 3189/36,626 postmenopausal | x | x | x | x | x | x | x | 6–8 vs. 0–3.5 | ||
| Nomura 2016 [21] | USA | Cohort BWHS | 1995–2011 | 1827/49,103 | x | x | x | x | x | x | x | 4–7 vs. 0–3 | ||
| Jancovic 2017 [39] | Worldwide | Pooled analysis of cohort studies EPIC-Elderly NIH-AARP Rotterdam Study | 1988–2011 | 6994/362,114 >60 yrs postmenopausal | x | x | x | x | NA ¥ | |||||
| Romaguera 2017 [40] | Spain | Case–control MCC-Spain | 2007–2012 | 1343/3431 | x | x | x | x | x | x | III vs. I tertile | |||
| Van den Brandt 2017 [8] | The Netherlands | Cohort NLCS | 1986–2007 | 2321/1665 ^ postmenopausal | x | x | x | x | x | NA ¥ | ||||
| Lavalette 2018 [36] | France | Cohort NutriNet-Santè | 2009–2017 | 488/41,547 | x | x | x | x | x | x | x | x | V vs. I quintile | |
| Xu 2019 [41] | Canada | Cohort ATP | 2001– | 454/15,787 | x | x | x | x | x | x | 4–6 vs. 0–2 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Turati, F.; Dalmartello, M.; Bravi, F.; Serraino, D.; Augustin, L.; Giacosa, A.; Negri, E.; Levi, F.; La Vecchia, C. Adherence to the World Cancer Research Fund/American Institute for Cancer Research Recommendations and the Risk of Breast Cancer. Nutrients 2020, 12, 607. https://doi.org/10.3390/nu12030607
Turati F, Dalmartello M, Bravi F, Serraino D, Augustin L, Giacosa A, Negri E, Levi F, La Vecchia C. Adherence to the World Cancer Research Fund/American Institute for Cancer Research Recommendations and the Risk of Breast Cancer. Nutrients. 2020; 12(3):607. https://doi.org/10.3390/nu12030607
Chicago/Turabian StyleTurati, Federica, Michela Dalmartello, Francesca Bravi, Diego Serraino, Livia Augustin, Attilio Giacosa, Eva Negri, Fabio Levi, and Carlo La Vecchia. 2020. "Adherence to the World Cancer Research Fund/American Institute for Cancer Research Recommendations and the Risk of Breast Cancer" Nutrients 12, no. 3: 607. https://doi.org/10.3390/nu12030607
APA StyleTurati, F., Dalmartello, M., Bravi, F., Serraino, D., Augustin, L., Giacosa, A., Negri, E., Levi, F., & La Vecchia, C. (2020). Adherence to the World Cancer Research Fund/American Institute for Cancer Research Recommendations and the Risk of Breast Cancer. Nutrients, 12(3), 607. https://doi.org/10.3390/nu12030607