
Long-Term Analysis of Resilience of the Oral Microbiome in Allogeneic Stem Cell Transplant Recipients

 , , ,
, , ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Sample Collection and Clinical Measurements
2.3. Sequencing of Oral Rinsing Samples
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
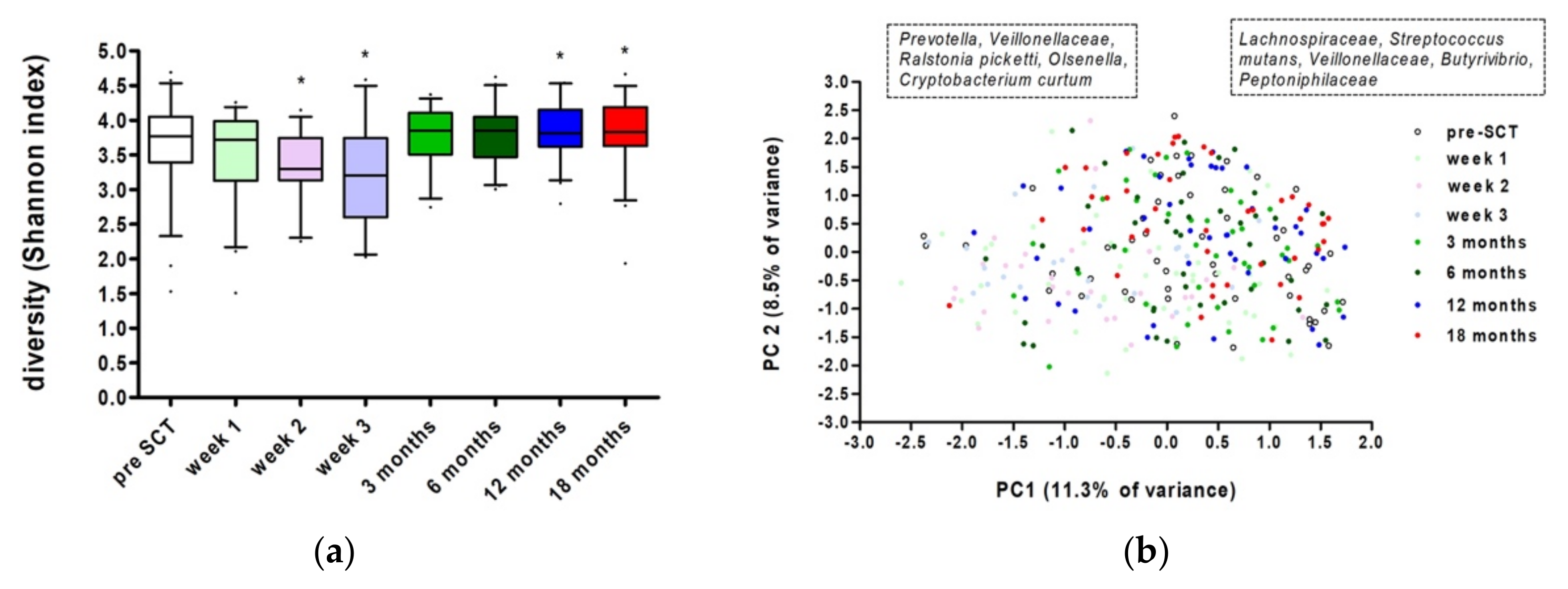
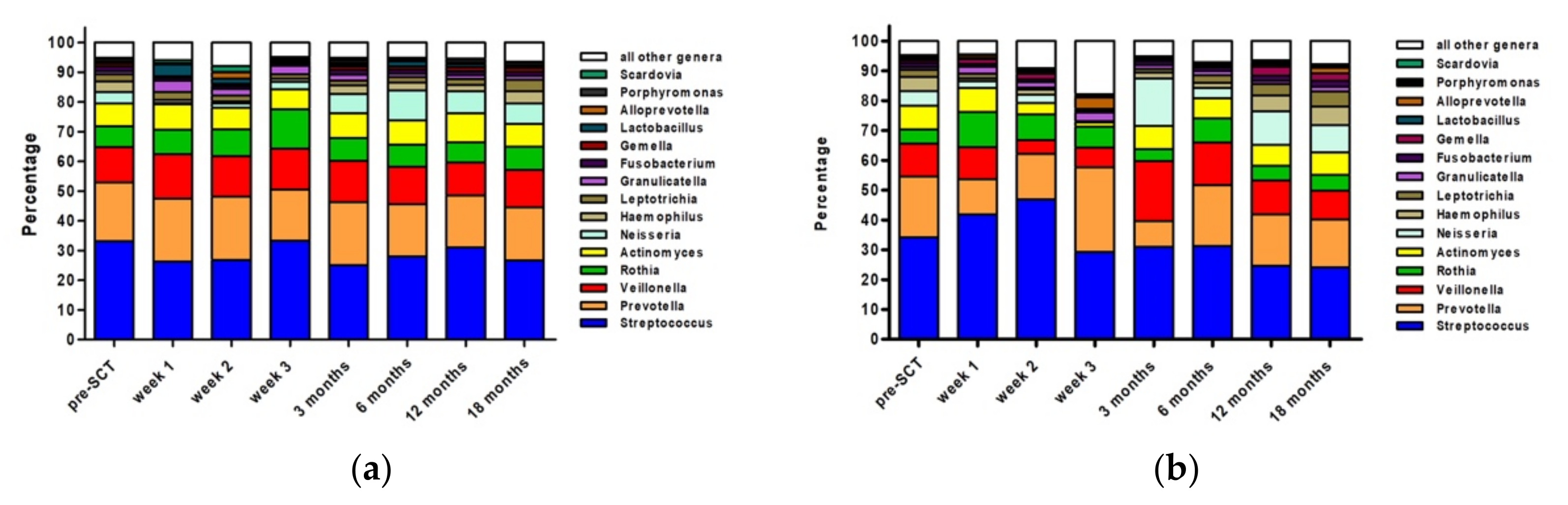
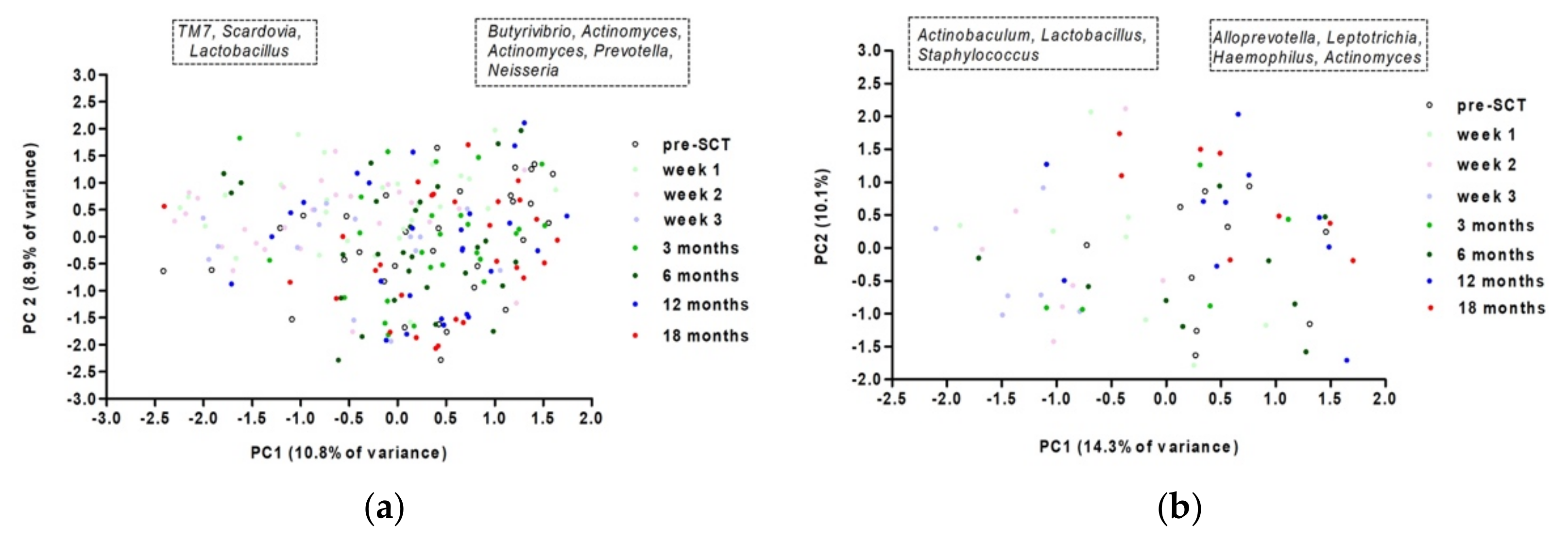
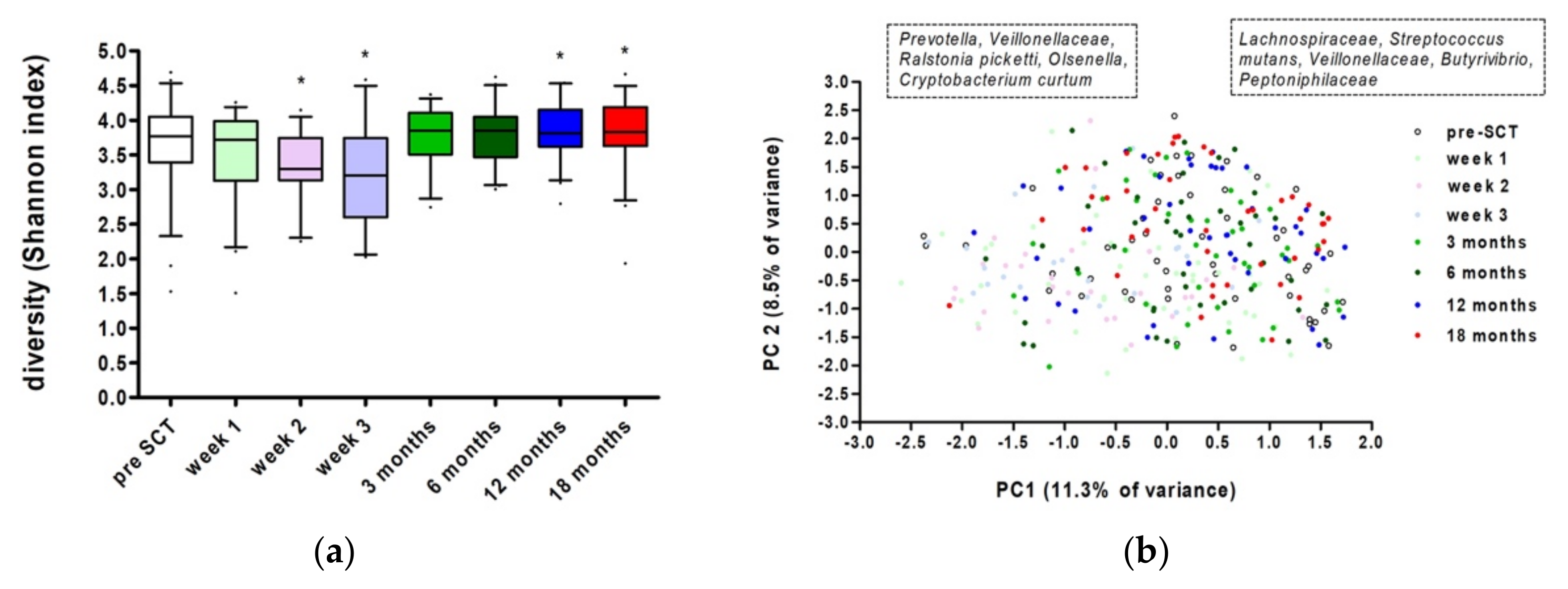
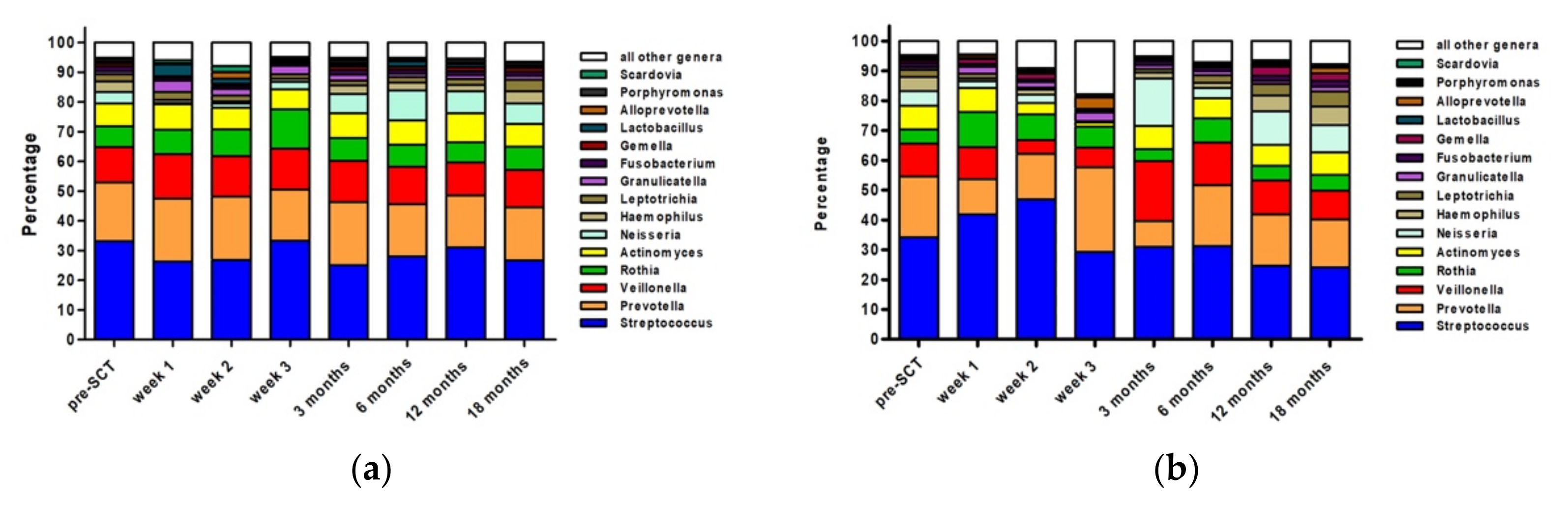
3.2. Microbiome Analyses
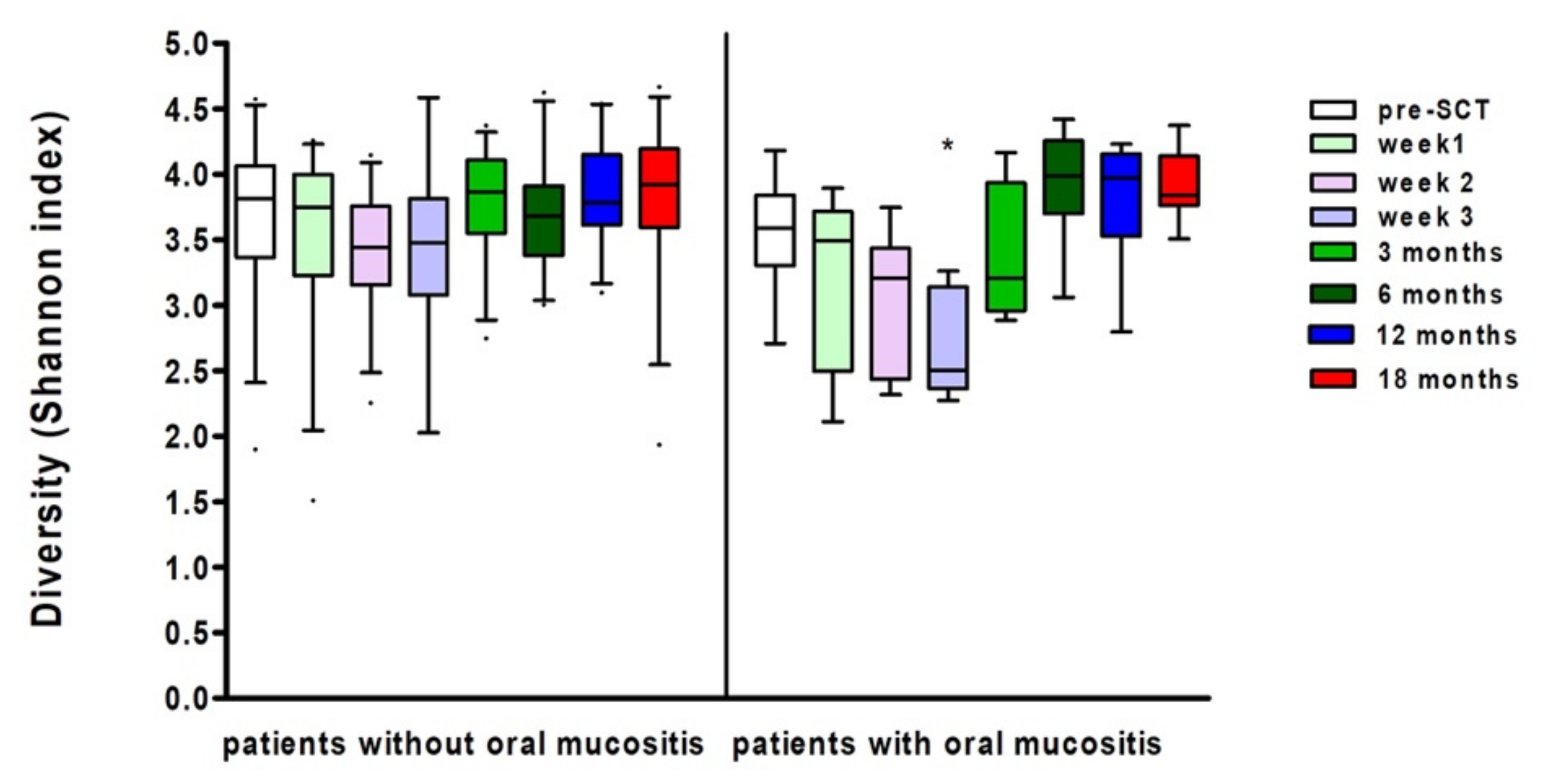
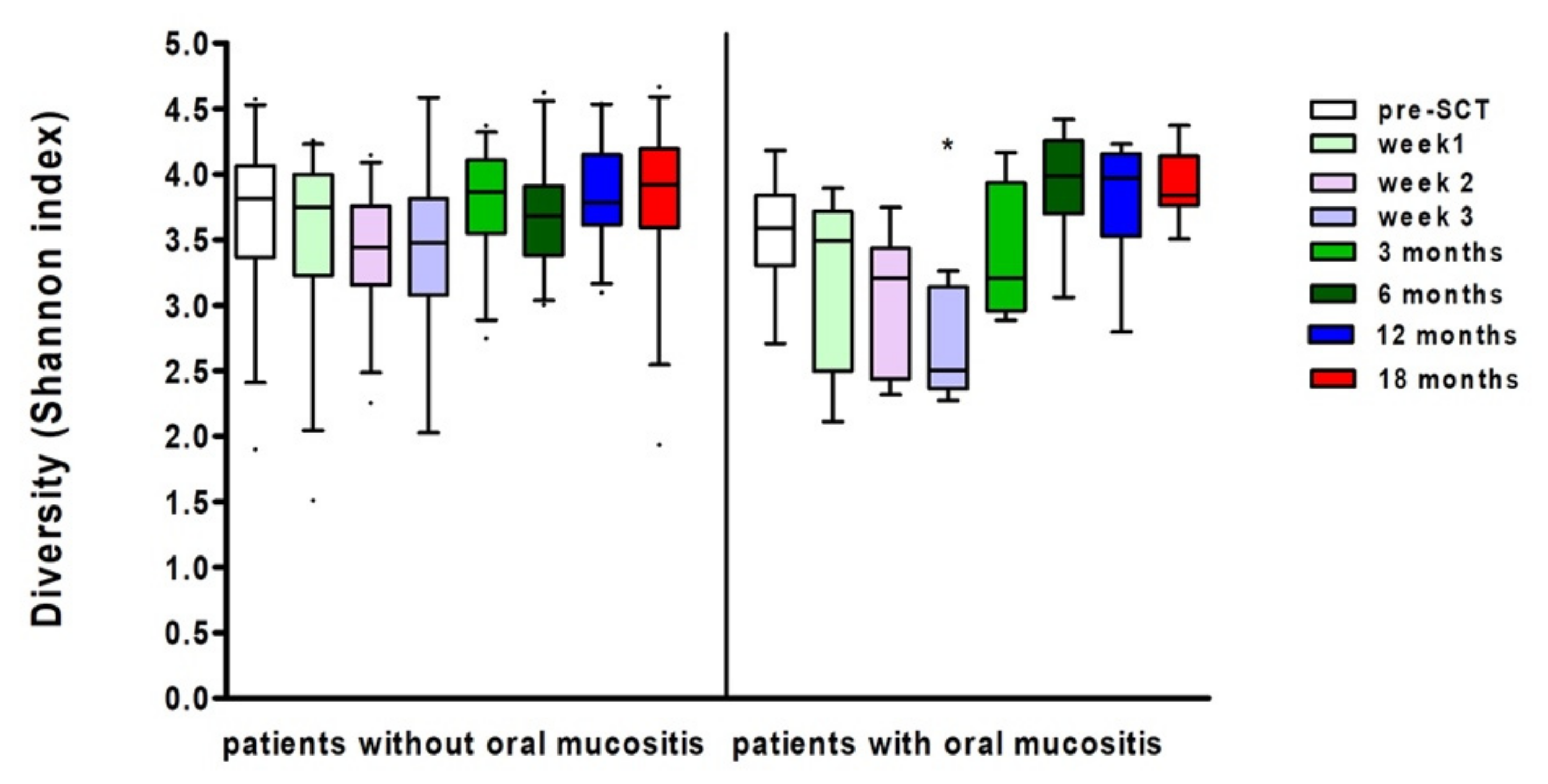
3.3. Ulcerative Oral Mucositis
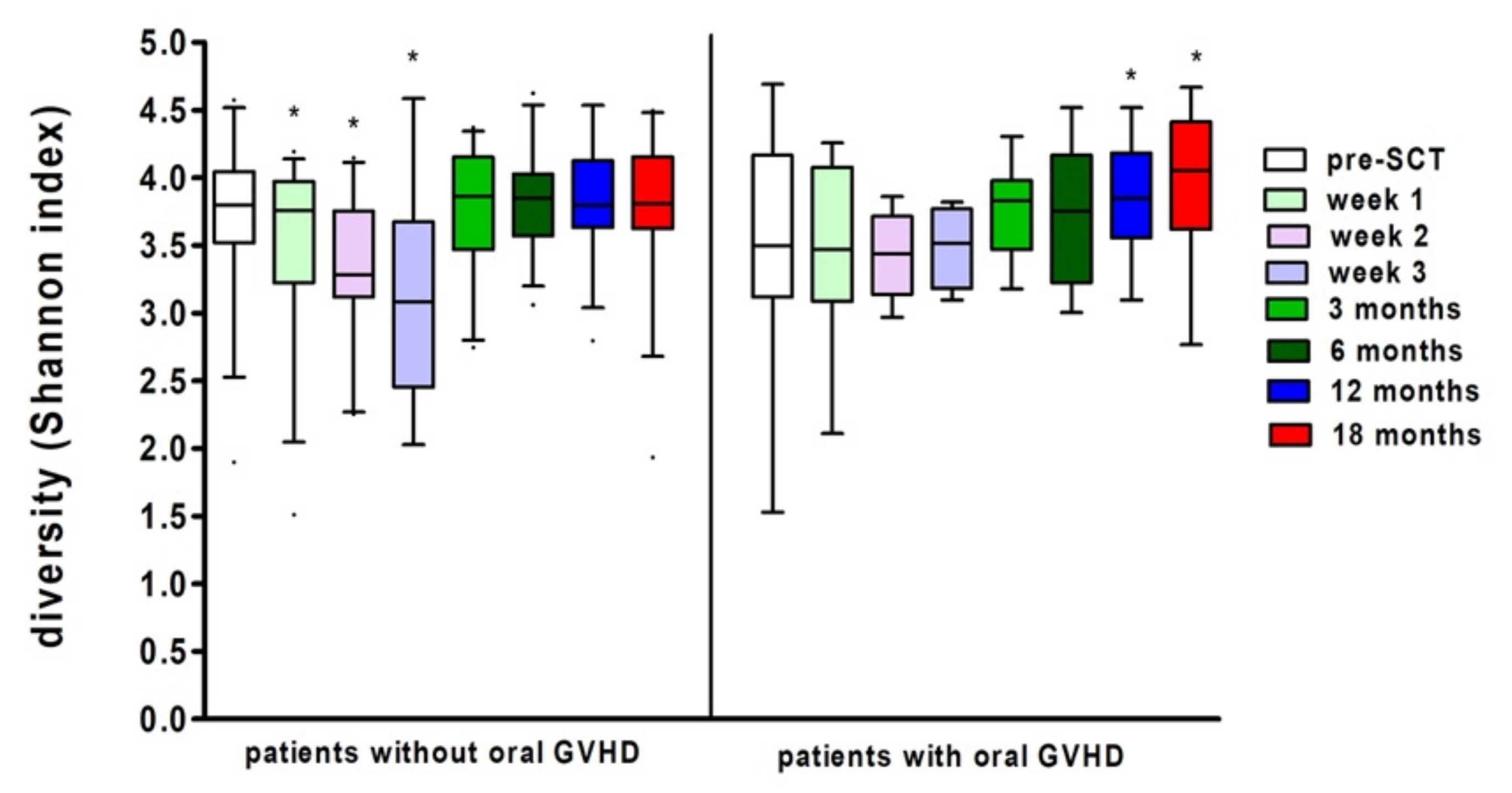
3.4. Oral Chronic Graft-versus-Host Disease
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dewhirst, F.E.; Chen, T.; Izard, J.; Paster, B.J.; Tanner, A.C.; Yu, W.H.; Lakshmanan, A.; Wade, W.G. The Human Oral Microbiome. J. Bacteriol. 2010, 192, 5002–5017. [Google Scholar] [CrossRef] [Green Version]
- Zaura, E.; Nicu, E.A.; Krom, B.P.; Keijser, B.J. Acquiring and Maintaining a Normal Oral Microbiome: Current Perspective. Front. Cell. Infect. Microbiol. 2014, 4, 85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, K.; Bihan, M.; Methé, B.A. Analyses of the Stability and Core Taxonomic Memberships of the Human Microbiome. PLoS ONE 2013, 8, e63139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berger, D.; Rakhamimova, A.; Pollack, A.; Loewy, Z. Oral Biofilms: Development, Control, and Analysis. High Throughput 2018, 7, 24. [Google Scholar]
- Novak, N.; Haberstok, J.; Bieber, T.; Allam, J.P. The Immune Privilege of the Oral Mucosa. Trends Mol. Med. 2008, 14, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Tamashiro, R.; Strange, L.; Schnackenberg, K.; Santos, J.; Gadalla, H.; Zhao, L.; Li, E.C.; Hill, E.; Hill, B.; Sidhu, G.; et al. Stability of Healthy Subgingival Microbiome across Space and Time. Sci. Rep. 2021, 11, 23987. [Google Scholar] [CrossRef]
- Kruse, A.B.; Schlueter, N.; Kortmann, V.K.; Frese, C.; Anderson, A.; Wittmer, A.; Hellwig, E.; Vach, K.; Al-Ahmad, A. Long-Term Use of Oral Hygiene Products Containing Stannous and Fluoride Ions: Effect on Viable Salivary Bacteria. Antibiotics 2021, 10, 481. [Google Scholar] [CrossRef]
- Haverman, T.M.; Raber-Durlacher, J.E.; Rademacher, W.M.; Vokurka, S.; Epstein, J.B.; Huisman, C.; Hazenberg, M.D.; de Soet, J.J.; de Lange, J.; Rozema, F.R. Oral Complications in Hematopoietic Stem Cell Recipients: The Role of Inflammation. Mediat. Inflamm. 2014, 2014, 378281. [Google Scholar] [CrossRef]
- Shouval, R.; Eshel, A.; Dubovski, B.; Kuperman, A.A.; Danylesko, I.; Fein, J.A.; Fried, S.; Geva, M.; Kouniavski, E.; Neuman, H.; et al. Patterns of Salivary Microbiota Injury and Oral Mucositis in Recipients of Allogeneic Hematopoietic Stem Cell Transplantation. Blood Adv. 2020, 4, 2912–2917. [Google Scholar] [CrossRef]
- Laheij, A.M.G.A.; Raber-Durlacher, J.E.; Koppelmans, R.G.A.; Huysmans, M.D.N.J.M.; Potting, C.; van Leeuwen, S.J.M.; Hazenberg, M.D.; Brennan, M.T.; von Bültzingslöwen, I.; Johansson, J.E.; et al. Microbial Changes in Relation to Oral Mucositis in Autologous Hematopoietic Stem Cell Transplantation Recipients. Sci. Rep. 2019, 9, 16929. [Google Scholar] [CrossRef]
- Laheij, A.M.; de Soet, J.J.; von dem Borne, P.A.; Kuijper, E.J.; Kraneveld, E.A.; van Loveren, C.; Raber-Durlacher, J.E. Oral Bacteria and Yeasts in Relationship to Oral Ulcerations in Hematopoietic Stem Cell Transplant Recipients. Support. Care Cancer 2012, 20, 3231–3240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diaz, P.I.; Hong, B.Y.; Frias-Lopez, J.; Dupuy, A.K.; Angeloni, M.; Abusleme, L.; Terzi, E.; Ioannidou, E.; Strausbaugh, L.D.; Dongari-Bagtzoglou, A. Transplantation-Associated Long-Term Immunosuppression Promotes Oral Colonization by Potentially Opportunistic Pathogens without Impacting Other Members of the Salivary Bacteriome. Clin. Vaccine Immunol. 2013, 20, 920–930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hou, J.; Zheng, H.M.; Li, P.; Liu, H.Y.; Zhou, H.W.; Yang, X.J. Distinct Shifts in the Oral Microbiota Are Associated with the Progression and Aggravation of Mucositis During Radiotherapy. Radiother. Oncol. 2018, 129, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Heidrich, V.; Bruno, J.S.; Knebel, F.H.; de Molla, V.C.; Miranda-Silva, W.; Asprino, P.F.; Tucunduva, L.; Rocha, V.; Novis, Y.; Arrais-Rodrigues, C.; et al. Dental Biofilm Microbiota Dysbiosis Is Associated with the Risk of Acute Graft-Versus-Host Disease after Allogeneic Hematopoietic Stem Cell Transplantation. Front. Immunol. 2021, 12, 692225. [Google Scholar] [CrossRef]
- Ingham, A.C.; Kielsen, K.; Mordhorst, H.; Ifversen, M.; Aarestrup, F.M.; Müller, K.G.; Pamp, S.J. Microbiota Long-Term Dynamics and Prediction of Acute Graft-Versus-Host Disease in Pediatric Allogeneic Stem Cell Transplantation. Microbiome 2021, 9, 148. [Google Scholar] [CrossRef]
- Lee, A.; Hong, J.; Shin, D.Y.; Koh, Y.; Yoon, S.S.; Kim, P.J.; Kim, H.G.; Kim, I.; Park, H.K.; Choi, Y. Association of Hsv-1 and Reduced Oral Bacteriota Diversity with Chemotherapy-Induced Oral Mucositis in Patients Undergoing Autologous Hematopoietic Stem Cell Transplantation. J. Clin. Med. 2020, 9, 1090. [Google Scholar] [CrossRef]
- Brennan, M.T.; Hasseus, B.; Hovan, A.J.; Raber-Durlacher, J.E.; Blijlevens, N.M.; Huysmans, M.C.; Legert, K.G.; Johansson, J.E.; Moore, C.G.; von Bultzingslowen, I. Impact of Oral Side Effects from Conditioning Therapy before Hematopoietic Stem Cell Transplantation: Protocol for a Multicenter Study. JMIR Res. Protoc. 2018, 7, e103. [Google Scholar] [CrossRef] [Green Version]
- Van Leeuwen, S.J.M.; Proctor, G.B.; Laheij, A.M.G.A.; Potting, C.M.J.; Smits, O.; Bronkhorst, E.M.; Hazenberg, M.D.; Haverman, T.M.; Brennan, M.T.; von Bültzingslöwen, I.; et al. Significant Salivary Changes in Relation to Oral Mucositis Following Autologous Hematopoietic Stem Cell Transplantation. Bone Marrow Transplant. 2021, 56, 1381–1390. [Google Scholar] [CrossRef]
- World Health Organization. Handbook for Reporting Results of Cancer Treatment; World Health Organization: Geneva, Switzerland, 1979; pp. 16–17. [Google Scholar]
- Elad, S.; Zeevi, I.; Or, R.; Resnick, I.B.; Dray, L.; Shapira, M.Y. Validation of the National Institutes of Health (Nih) Scale for Oral Chronic Graft-Versus-Host Disease (Cgvhd). Biol. Blood Marrow Transplant. 2010, 16, 62–69. [Google Scholar] [CrossRef] [Green Version]
- Ciric, L.; Pratten, J.; Wilson, M.; Spratt, D. Development of a Novel Multi-Triplex Qpcr Method for the Assessment of Bacterial Community Structure in Oral Populations. Environ. Microbiol. Rep. 2010, 2, 770–774. [Google Scholar] [CrossRef] [PubMed]
- Kozich, J.J.; Westcott, S.L.; Baxter, N.T.; Highlander, S.K.; Schloss, P.D. Development of a Dual-Index Sequencing Strategy and Curation Pipeline for Analyzing Amplicon Sequence Data on the Miseq Illumina Sequencing Platform. Appl. Environ. Microbiol. 2013, 79, 5112–5120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gregory, C.J.; Lauber, C.L.; Walters, W.A.; Berg-Lyons, D.; Lozupone, C.A.; Turnbaugh, P.J.; Fierer, N.; Knight, R. Global Patterns of 16s Rrna Diversity at a Depth of Millions of Sequences Per Sample. Proc. Natl. Acad. Sci. USA 2011, 108 (Suppl. 1), 4516–4522. [Google Scholar]
- Chen, T.; Yu, W.H.; Izard, J.; Baranova, O.V.; Lakshmanan, A.; Dewhirst, F.E. The Human Oral Microbiome Database: A Web Accessible Resource for Investigating Oral Microbe Taxonomic and Genomic Information. Database 2010, 2010, baq013. [Google Scholar] [CrossRef] [PubMed]
- Koopman, J.E.; Buijs, M.J.; Brandt, B.W.; Keijser, B.J.; Crielaard, W.; Zaura, E. Nitrate and the Origin of Saliva Influence Composition and Short Chain Fatty Acid Production of Oral Microcosms. Microb. Ecol. 2016, 72, 479–492. [Google Scholar] [CrossRef] [Green Version]
- Hammer, Ø.; Harper, D.A.T.; Ryan, P.D. Past: Paleontological Statistics Software Package for Education and Data Analysis. Palaeontol. Electron. 2001, 4, 1–9. [Google Scholar]
- R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2015.
- Vegan: Community Ecology Package; R Package Version 2.5-7; R Foundation for Statistical Computing: Vienna, Austria, 2020.
- Lahti, L.; Shetty, S. Tools for Microbiome Analysis in R. 2017. Available online: http://microbiome.github.com/microbiome (accessed on 28 October 2021).
- McMurdie, P.J.; Holmes, S. Phyloseq: An R Package for Reproducible Interactive Analysis and Graphics of Microbiome Census Data. PLoS ONE 2013, 8, e61217. [Google Scholar]
- Takahashi, M.; Toyosaki, M.; Matsui, K.; Machida, S.; Kikkawa, E.; Ota, Y.; Kaneko, A.; Ogawa, Y.; Ando, K.; Onizuka, M. An Analysis of Oral Microbial Flora by T-Rflp in Patients Undergoing Hematopoietic Stem Cell Transplantation. Int. J. Hematol. 2020, 112, 690–696. [Google Scholar] [CrossRef]
- De Molla, V.C.; Heidrich, V.; Bruno, J.S.; Knebel, F.H.; Miranda-Silva, W.; Asprino, P.F.; Tucunduva, L.; Rocha, V.; Novis, Y.; Camargo, A.A.; et al. Disruption of the Oral Microbiota Is Associated with a Higher Risk of Relapse after Allogeneic Hematopoietic Stem Cell Transplantation. Sci. Rep. 2021, 11, 17552. [Google Scholar] [CrossRef]
- Badia, P.; Andersen, H.; Haslam, D.; Nelson, A.S.; Pate, A.R.; Golkari, S.; Teusink-Cross, A.; Flesch, L.; Bedel, A.; Hickey, V.; et al. Improving Oral Health and Modulating the Oral Microbiome to Reduce Bloodstream Infections from Oral Organisms in Pediatric and Young Adult Hematopoietic Stem Cell Transplantation Recipients: A Randomized Controlled Trial. Biol. Blood Marrow Transplant. 2020, 26, 1704–1710. [Google Scholar] [CrossRef]
- Petersen, C.; Round, J.L. Defining Dysbiosis and Its Influence on Host Immunity and Disease. Cell. Microbiol. 2014, 16, 1024–1033. [Google Scholar] [CrossRef]
- Ryan, M.P.; Adley, C.C. Ralstonia Spp.: Emerging Global Opportunistic Pathogens. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 291–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oku, S.; Takeshita, T.; Futatsuki, T.; Kageyama, S.; Asakawa, M.; Mori, Y.; Miyamoto, T.; Hata, J.; Ninomiya, T.; Kashiwazaki, H.; et al. Disrupted Tongue Microbiota and Detection of Nonindigenous Bacteria on the Day of Allogeneic Hematopoietic Stem Cell Transplantation. PLoS Pathog. 2020, 16, e1008348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, P.M.; Jacinto, R.C.; Pizzol, T.S.D.; Ferreira, M.B.; Montagner, F. Resistance Profiles to Antimicrobial Agents in Bacteria Isolated from Acute Endodontic Infections: Systematic Review and Meta-Analysis. Int. J. Antimicrob. Agents 2016, 48, 467–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, G.; Wu, C.; Abrams, W.R.; Li, Y. Structural and Functional Characteristics of the Microbiome in Deep-Dentin Caries. J. Dent. Res. 2020, 99, 713–720. [Google Scholar] [CrossRef]
- Celik, Z.C.; Cakiris, A.; Abaci, N.; Yaniikoglu, F.; Ilgin, C.; Ekmekci, S.S.; Celik, H.; Tagtekin, D. The Complex Microbiome of Caries-Active and Caries-Free Supragingival Plaques in Permanent Dentition. Niger. J. Clin. Pract. 2021, 24, 1535–1540. [Google Scholar] [CrossRef]
- Robertson, D.; Smith, A.J. The Microbiology of the Acute Dental Abscess. J. Med. Microbiol. 2009, 58 Pt 2, 155–162. [Google Scholar] [CrossRef]
- Hiranmayi, K.V.; Sirisha, K.; Rao, M.V.R.; Sudhakar, P. Novel Pathogens in Periodontal Microbiology. J. Pharm. Bioallied Sci. 2017, 9, 155–163. [Google Scholar] [CrossRef]
- Gajdács, M.; Urbán, E. The Pathogenic Role of Actinomyces spp. and Related Organisms in Genitourinary Infections: Discoveries in the New, Modern Diagnostic Era. Antibiotics 2020, 9, 524. [Google Scholar] [CrossRef]
- Fakhruddin, K.S.; Ngo, H.C.; Samaranayake, L.P. Cariogenic Microbiome and Microbiota of the Early Primary Dentition: A Contemporary Overview. Oral Dis. 2018, 25, 982–995. [Google Scholar] [CrossRef]
- Bor, B.; Bedree, J.K.; Shi, W.; McLean, J.S.; He, X. Saccharibacteria (Tm7) in the Human Oral Microbiome. J. Dent. Res. 2019, 98, 500–509. [Google Scholar] [CrossRef]
- Jo, R.; Nishimoto, Y.; Umezawa, K.; Yama, K.; Aita, Y.; Ichiba, Y.; Murakami, S.; Kakizawa, Y.; Kumagai, T.; Yamada, T.; et al. Comparison of Oral Microbiome Profiles in Stimulated and Unstimulated Saliva, Tongue, and Mouth-Rinsed Water. Sci. Rep. 2019, 9, 16124. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Conditioning Regimens | Diagnoses | Donor Source | GVHD Prophylaxis | ||||
|---|---|---|---|---|---|---|---|
| ATG, Bu, Flu | 11 | Acute myeloid leukemia | 19 | Matched unrelated donor | 34 | Cyclosporin | 33 |
| Flu, TBI | 10 | Myelodysplastic syndrome | 7 | Sibling | 10 | Cyclosporine and methotrexate | 6 |
| ATG, Cy, TBI | 7 | Lymphoma | 6 | Mismatched unrelated donor | 2 | Cyclosporine and other | 6 |
| ATG, Flu, TBI | 6 | Acute lymphoid leukemia | 4 | Female donor | 2 | Cyclosporin and prednisolone | 1 |
| ATG, Flu, TBI | 4 | Chronic lymphoid leukemia | 2 | Unknown | 2 | Cyclosporine, methotrexate, and anti-thymocyte globulin | 1 |
| ATG, Cy | 3 | Severe aplastic anemia | 2 | Cyclosporin and T-cell depleted transplant | 1 | ||
| Cy, TBI | 3 | Myelofibrosis | 2 | Cyclosporine, methotrexate, and prednisolone | 1 | ||
| Flu, TBI, Cy | 2 | Myeloma | 2 | Tacrolimus and prednisolone | 1 | ||
| Other | 4 | Chronic lymphoid leukemia | 1 | ||||
| ATG, Bu, Flu | 11 | Other | 5 | ||||
| Developed Oral Mucositis? | ||||
|---|---|---|---|---|
| no | Yes | |||
| Developed oral GVHD? | no | 25 | 6 | 31 |
| yes | 7 | 4 | 11 | |
| Total | 32 | 10 | 42 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laheij, A.M.G.A.; Rozema, F.R.; Brennan, M.T.; von Bültzingslöwen, I.; van Leeuwen, S.J.M.; Potting, C.; Huysmans, M.-C.D.N.J.M.; Hazenberg, M.D.; Brandt, B.W.; Zaura, E.; et al. Long-Term Analysis of Resilience of the Oral Microbiome in Allogeneic Stem Cell Transplant Recipients. Microorganisms 2022, 10, 734. https://doi.org/10.3390/microorganisms10040734
Laheij AMGA, Rozema FR, Brennan MT, von Bültzingslöwen I, van Leeuwen SJM, Potting C, Huysmans M-CDNJM, Hazenberg MD, Brandt BW, Zaura E, et al. Long-Term Analysis of Resilience of the Oral Microbiome in Allogeneic Stem Cell Transplant Recipients. Microorganisms. 2022; 10(4):734. https://doi.org/10.3390/microorganisms10040734
Chicago/Turabian StyleLaheij, Alexa M. G. A., Frederik R. Rozema, Michael T. Brennan, Inger von Bültzingslöwen, Stephanie J. M. van Leeuwen, Carin Potting, Marie-Charlotte D. N. J. M. Huysmans, Mette D. Hazenberg, Bernd W. Brandt, Egija Zaura, and et al. 2022. "Long-Term Analysis of Resilience of the Oral Microbiome in Allogeneic Stem Cell Transplant Recipients" Microorganisms 10, no. 4: 734. https://doi.org/10.3390/microorganisms10040734
APA StyleLaheij, A. M. G. A., Rozema, F. R., Brennan, M. T., von Bültzingslöwen, I., van Leeuwen, S. J. M., Potting, C., Huysmans, M.-C. D. N. J. M., Hazenberg, M. D., Brandt, B. W., Zaura, E., Buijs, M. J., de Soet, J. J., Blijlevens, N. N. M., & Raber-Durlacher, J. E. (2022). Long-Term Analysis of Resilience of the Oral Microbiome in Allogeneic Stem Cell Transplant Recipients. Microorganisms, 10(4), 734. https://doi.org/10.3390/microorganisms10040734