
The Effectiveness of Autologous Platelet Concentrates in the Clinical and Radiographic Healing after Endodontic Surgery: A Systematic Review

 ,
,  and
and 
Abstract
:1. Introduction
2. Methods
2.1. Focused Question
2.2. Search Strategy
2.3. Inclusion and Exclusion Criteria
- The study was randomized controlled trials (RCTs) or clinical controlled trials (CCTs);
- Patients presented with persistent periapical lesions and needed periapical surgery;
- APCs were utilized in the intervention group(s);
- Physiologic healing or regenerative materials alone or combination of APCs and regenerative materials instead of APC were utilized in the control group;
- Reported clinical or radiographical outcomes or both.
- Dual publications, narrative reviews, systematic reviews, case series, questionnaires, animal studies, case reports, letters to the editor, in vitro studies, abstracts;
- Outcomes of interest were not extractable;
- Articles written in any language other than English;
- Full text not available.
2.4. Selecting and Extracting Data from Studies
2.5. Methodological Quality of Included Reviews
3. Results
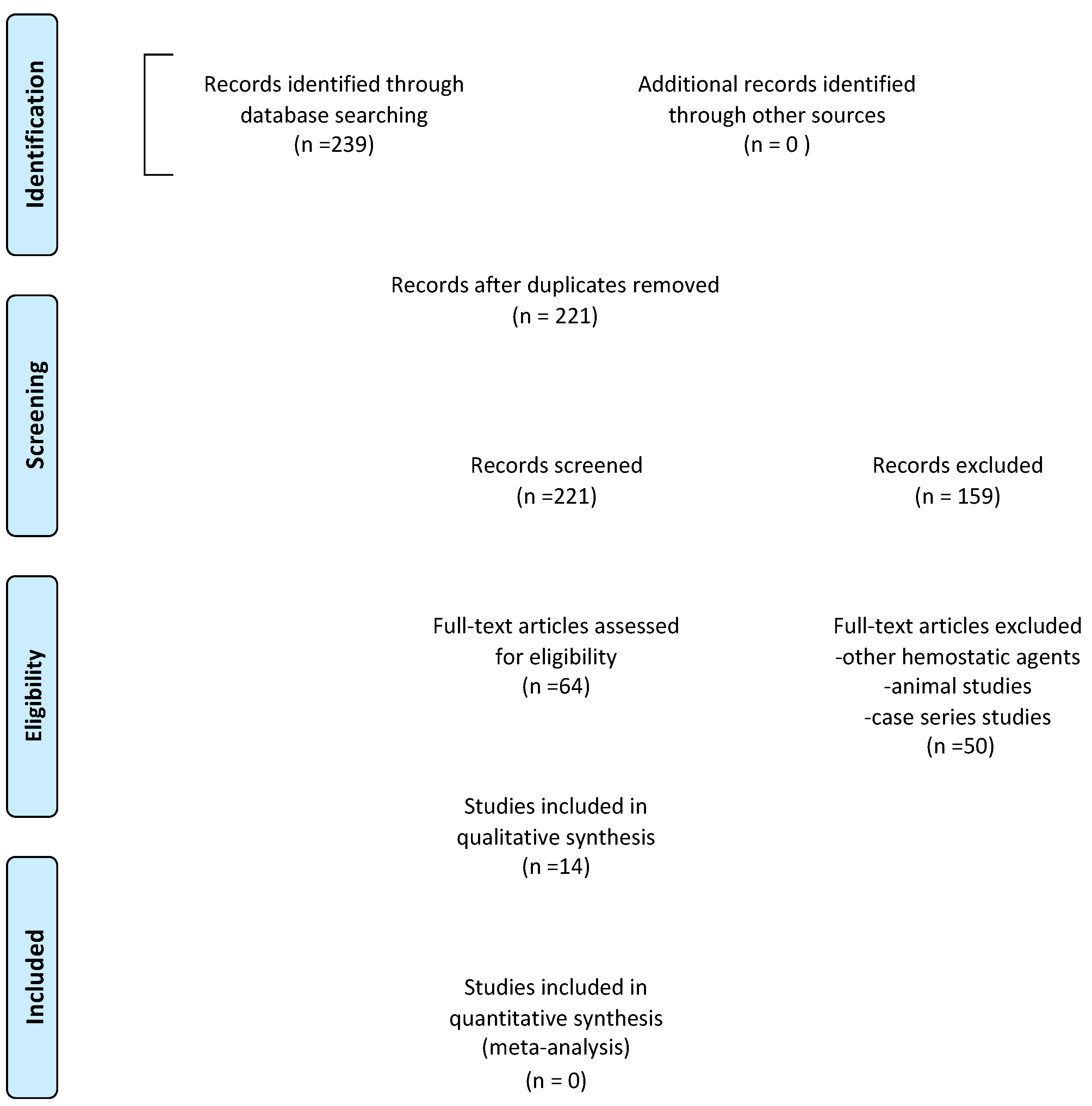
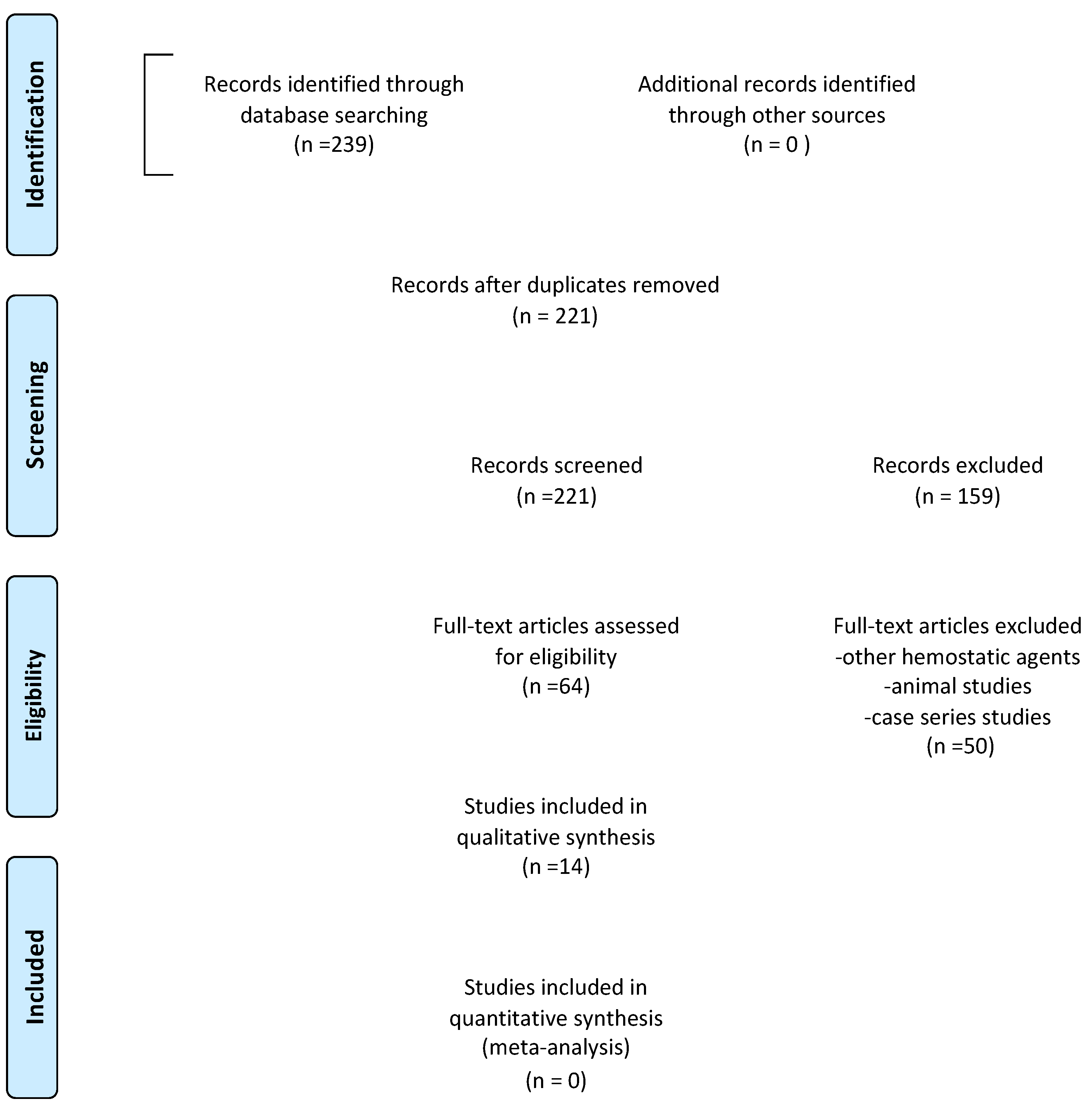
3.1. Search Results
3.2. Summary of Clinical Findings
3.3. Summary of Radiographic Findings
3.4. Risk of Bias Assessment
4. Discussion
4.1. Risk-of-Bias Judgement of Eligible Studies
4.2. Limitations
4.3. Prospective
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Setzer, M.C.; Kohli, M.R.; Shah, S.B. Outcome of endodontic surgery: A meta-analysis of the literature. Part 2: Comparison of endodontic microsurgical techniques with and without the use of higher magnification. J. Endod. 2012, 28, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Di Spirito, F.; Pisano, M.; Caggiano, M.; Bhasin, P.; Lo Giudice, R.; Abdellatif, D. Root Canal Cleaning after Different Irrigation Techniques: An Ex Vivo Analysis. Medicina 2022, 58, 193. [Google Scholar] [CrossRef] [PubMed]
- Ng, Y.L.; Gulabivala, K. Factors that influence the outcomes of surgical endodontic treatment. Int. Endod. J. 2023, 56 (Suppl. S2), 116–139. [Google Scholar] [CrossRef] [PubMed]
- Floratos, S.; Kim, S. Modern Endodontic Microsurgery Concepts: A Clinical Update. Dent. Clin. N. Am. 2017, 61, 81–91. [Google Scholar] [CrossRef]
- Elemam, R.F.; Pretty, I. Comparison of the success rate of endodontic treatment and implant treatment. ISRN Dent. 2011, 2011, 640509. [Google Scholar] [CrossRef]
- Liu, T.J.; Zhou, J.N.; Guo, L.H. Impact of different regenerative techniques and materials on the healing outcome of endodontic surgery: A systematic review and meta-analysis. Int. Endod. J. 2021, 54, 536–555. [Google Scholar] [CrossRef]
- Sanchez-Torres, A.; Sanchez-Garces, M.A.; Gay-Escoda, C. Materials and prognostic factors of bone regeneration in periapical surgery: A systematic review. Med. Oral Patol. Oral Cir. Bucal 2014, 19, e419–e425. [Google Scholar] [CrossRef]
- Deng, Y.; Zhu, X.; Yang, J.; Jiang, H.; Yan, P. The effect of regeneration techniques on periapical surgery with different protocols for different lesion types: A meta-analysis. J. Oral. Maxillofac. Surg. 2016, 74, 239–246. [Google Scholar] [CrossRef]
- von Arx, T.; Alsaeed, M. The use of regenerative techniques in apical surgery: A literature review. Saudi Dent. J. 2011, 23, 113–127. [Google Scholar] [CrossRef]
- Corbella, S.; Taschieri, S.; Elkabbany, A.; Del Fabbro, M.; von Arx, T. Guided tissue regeneration using a barrier mem- brane in endodontic surgery. Swiss Dent. J. 2016, 126, 13–25. [Google Scholar]
- Rohilla, R.; Tewari, S.; Nayyar, A.S. Efficacy of Guided Tissue Regeneration (GTR) membranes in the healing of apico-marginal defects: A prospective, controlled clinical trial. Int. J. Orofac. Res. 2017, 2, 11–17. [Google Scholar] [CrossRef]
- Kurmanalina, M.; Uraz, R.; Skaģers, A.; Locs, J.; Taganiyazova, A.; Omargali, A. Radiological evaluation of endodontic treatment of chronic apical periodontitis using biphasic calcium phosphate biomaterial. Eurasian J. Anal. Chem. 2018, 13, em54. [Google Scholar] [CrossRef]
- Ding, Z.Y.; Tan, Y.; Peng, Q.; Zuo, J.; Li, N. Novel applications of platelet concentrates in tissue regeneration (Review). Exp. Ther. Med. 2021, 21, 226. [Google Scholar] [CrossRef] [PubMed]
- Giannotti, L.; Di Chiara Stanca, B.; Spedicato, F.; Nitti, P.; Damiano, F.; Demitri, C.; Calabriso, N.; Carluccio, M.A.; Palermo, A.; Siculella, L.; et al. Progress in Regenerative Medicine: Exploring Autologous Platelet Concentrates and Their Clinical Applications. Genes 2023, 14, 1669. [Google Scholar] [CrossRef] [PubMed]
- Tang, B.; Huang, Z.; Zheng, X. Impact of autologous platelet concentrates on wound area reduction: A meta-analysis of randomized controlled trials. Int. Wound J. 2023. [Google Scholar] [CrossRef]
- Pensato, R.; Al-Amer, R.; La Padula, S. Protocol for Obtaining Platelet-Rich Plasma (PRP), Platelet-Poor Plasma (PPP), and Thrombin for Autologous use. Aesthetic Plast. Surg. 2023. [Google Scholar] [CrossRef]
- Kobayashi, E.; Flückiger, L.; Fujioka-Kobayashi, M.; Sawada, K.; Sculean, A.; Schaller, B.; Miron, R.J. Comparative release of growth factors from PRP, PRF, and advanced-PRF. Clin. Oral. Investig. 2016, 20, 2353–2360. [Google Scholar] [CrossRef]
- Gasparro, R.; Qorri, E.; Valletta, A.; Masucci, M.; Sammartino, P.; Amato, A.; Marenzi, G. Non-transfusional hemocomponents: From biology to the clinic—A literature review. Bioengineering 2018, 5, 27. [Google Scholar] [CrossRef]
- Brancaccio, Y.; Antonelli, A.; Barone, S.; Bennardo, F.; Fortunato, L.; Giudice, A. Evaluation of local hemostatic efficacy after dental extractions in patients taking antiplatelet drugs: A randomized clinical trial. Clin. Oral. Investig. 2021, 25, 1159–1167. [Google Scholar] [CrossRef]
- Masuki, H.; Okudera, T.; Watanebe, T.; Suzuki, M.; Nishiyama, K.; Okudera, H.; Nakata, K.; Uematsu, K.; Su, C.Y.; Kawase, T. Growth factor and pro-inflammatory cytokine contents in platelet-rich plasma (PRP), plasma rich in growth factors (PRGF), advanced platelet-rich fibrin (A-PRF), and concentrated growth factors (CGF). Int. J. Implant. Dent. 2016, 2, 19. [Google Scholar] [CrossRef]
- D’Esposito, V.; Lecce, M.; Marenzi, G.; Cabaro, S.; Ambrosio, M.R.; Sammartino, G.; Misso, S.; Migliaccio, T.; Liguoro, P.; Oriente, F.; et al. Platelet-rich plasma counteracts detrimental effect of high-glucose concentrations on mesenchymal stem cells from Bichat fat pad. J. Tissue Eng. Regen. Med. 2020, 14, 701–713. [Google Scholar] [CrossRef] [PubMed]
- Shah, N.; Cairns, M. Autologous Platelet Concentrates to improve post extraction outcomes. Evid. Based Dent. 2018, 19, 118–119. [Google Scholar] [CrossRef]
- Yan, L.; Lin, J.; Yang, L.; He, S.; Tan, X.; Huang, D. Clinical Effect Evaluation of Concentrated Growth Factor in Endodontic Microsurgery: A Cross-Sectional Study. J. Endod. 2023, 49, 836–845. [Google Scholar] [CrossRef]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J. CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 10, 28–55. [Google Scholar]
- Ahmed, G.M.; Saif, N.; Nageh, M.; Elbaz, A. CBCT volumetric evaluation of bone healing after endodontic microsurgery using platelet-rich fibrin (PRF). ENDO 2018, 12, 241–248. [Google Scholar]
- Angerame, D.; De Biasi, M.; Kastrioti, I.; Franco, V.; Castaldo, A.; Maglione, M. Application of platelet-rich fibrin in endodontic surgery: A pilot study. Giornale Italiano di Endodonzia 2015, 29, 51–57. [Google Scholar] [CrossRef]
- Del Fabbro, M.; Ceresoli, V.; Lolato, A.; Taschieri, S. Effect of platelet concentrates on quality of life after periradicular surgery: A randomized clinical study. J. Endod. 2012, 38, 733–739. [Google Scholar] [CrossRef]
- Dhiman, M.; Kumar, S.; Duhan, J.; Sangwan, P.; Tewari, S. Effect of Platelet-rich Fibrin on Healing of Apicomarginal Defects: A Randomized Controlled Trial. J. Endod. 2015, 41, 985–991. [Google Scholar] [CrossRef]
- Goyal, B.; Tewari, S.; Duhan, J.; Sehgal, P.K. Comparative evaluation of platelet-rich plasma and guided tissue regeneration membrane in the healing of apicomarginal defects: A clinical study. J. Endod. 2011, 37, 773–780. [Google Scholar] [CrossRef]
- Meschi, N.; Fieuws, S.; Vanhoenacker, A.; Strijbos, O.; Van der Veken, D.; Politis, C.; Lambrechts, P. Root-end surgery with leucocyte- and platelet-rich fibrin and an occlusive membrane: A randomized controlled clinical trial on patients’ quality of life. Clin. Oral. Investig. 2018, 22, 2401–2411. [Google Scholar] [CrossRef]
- Meschi, N.; Vanhoenacker, A.; Strijbos, O.; Camargo Dos Santos, B.; Rubbers, E.; Peeters, V.; Curvers, F.; Van Mierlo, M.; Geukens, A.; Fieuws, S.; et al. Multi-modular bone healing assessment in a randomized controlled clinical trial of root-end surgery with the use of leukocyte- and platelet-rich fibrin and an occlusive membrane. Clin. Oral. Investig. 2020, 24, 4439–4453. [Google Scholar] [CrossRef]
- Monga, P.; Grover, R.; Mahajan, P.; Keshav, V.; Singh, N.; Singh, G. A comparative clinical study to evaluate the healing of large periapical lesions using platelet-rich fibrin and hydroxyapatite. Endodontology 2016, 28, 27–31. [Google Scholar] [CrossRef]
- Parikh, B.; Navin, S.; Vaishali, P. A comparative evaluation of healing with a computed tomography scan of bilateral periapical lesions treated with and without the use of platelet-rich plasma. Indian J. Dent. Res. 2011, 22, 497–498. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.; Ismail, P.M.S.; Kambli, V.; Kumar, R.; Singh, K.D.; Kochhar, A.S.; Babaji, P. Evaluation of Hydroxyapatite Granules, CERAMENT™, and Platelet-rich Fibrin in the Management of Endodontic Apical Surgery. J. Contemp. Dent. Pract. 2020, 21, 554–557. [Google Scholar] [CrossRef] [PubMed]
- Soto-Peñaloza, D.; Peñarrocha-Diago, M.; Cervera-Ballester, J.; Peñarrocha-Diago, M.; Tarazona-Alvarez, B.; Peñarrocha-Oltra, D. Pain and quality of life after endodontic surgery with or without advanced platelet-rich fibrin membrane application: A randomized clinical trial. Clin. Oral. Investig. 2020, 24, 1727–1738. [Google Scholar] [CrossRef]
- Taschieri, S.; Corbella, S.; Tsesis, I.; Del Fabbro, M. Impact of the use of plasma rich in growth factors (PRGF) on the quality of life of patients treated with endodontic surgery when a perforation of sinus membrane occurred. A comparative study. Oral. Maxillofac. Surg. 2014, 18, 43–52. [Google Scholar] [CrossRef]
- Thakur, V.; Mittal, S.; Tewari, S.; Kamboj, M.; Duhan, J.; Sangwan, P.; Kumar, V.; Gupta, A. Comparative histological evaluation of two PRF formulations (PRF High and PRF Medium) on quality of life and healing outcome of apicomarginal defects: A randomized clinical trial. J. Cranio-Maxillofac. Surg. 2023, 51, 166–177. [Google Scholar] [CrossRef]
- Yahata, Y.; Handa, K.; Ohkura, N.; Okamoto, M.; Ohshima, J.; Itoh, S.; Kawashima, N.; Tanaka, T.; Sato, N.; Noiri, Y.; et al. Autologous concentrated growth factor mediated accelerated bone healing in root-end microsurgery: A multicenter randomized clinical trial. Regen. Ther. 2023, 24, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Lisy, K.; Qureshi, R.; Mattis, P.; et al. Chapter 7: Systematic reviews of etiology and risk. JBI Man. Evid. Synth. 2020, 5, 217–269. [Google Scholar]
- Al-Hamed, F.S.; Mahri, M.; Al-Waeli, H.; Torres, J.; Badran, Z.; Tamimi, F. Regenerative Effect of Platelet Concentrates in Oral and Craniofacial Regeneration. Front. Cardiovasc. Med. 2019, 6, 126. [Google Scholar] [CrossRef]
- Pavlíková, G.; Foltán, R.; Horká, M.; Hanzelka, T.; Borunská, H.; Sedý, J. Piezosurgery in oral and maxillofacial surgery. Int. J. Oral. Maxillofac. Surg. 2011, 40, 451–457. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, L.; Ní Ríordáin, R. Autologous platelet concentrates in oral surgery: Protocols, properties, and clinical applications. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. 2022, 133, 156–164. [Google Scholar] [CrossRef]
- Del Fabbro, M.; Bucchi, C.; Lolato, A.; Corbella, S.; Testori, T.; Taschieri, S. Healing of Postextraction Sockets Preserved with Autologous Platelet Concentrates. A Systematic Review and Meta-Analysis. J. Oral. Maxillofac. Surg. 2017, 75, 1601–1615. [Google Scholar] [CrossRef]
- Gasparro, R.; Adamo, D.; Masucci, M.; Sammartino, G.; Mignogna, M.D. Use of injectable platelet-rich fibrin in the treatment of plasma cell mucositis of the oral cavity refractory to corticosteroid therapy: A case report. Dermatol. Ther. 2019, 32, e13062. [Google Scholar] [CrossRef]
- Gasparro, R.; Sammartino, G.; Mariniello, M.; di Lauro, E.A.; Spagnuolo, G.; Marenzi, G. Treatment of periodontal pockets at the distal aspect of mandibular second molar after surgical removal of impacted third molar and application of L-PRF: A split-mouth randomized clinical trial. Quintessence Int. 2020, 51, 204–211. [Google Scholar]
- Marx, R.E.; Carlson, E.R.; Eichstaedt, R.M. Platelet-rich plasma: Growth factor enhancement for bone grafts. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 1998, 85, 638–642. [Google Scholar] [CrossRef]
- Weibrich, G.; Kleis, W.K.; Hafner, G. Growth factor levels in the platelet rich plasma produced by 2 different methods: Curasan PRP kit versus PCCS PRP system. Int. J. Oral. Maxillofac. Implant. 2002, 17, 184–190. [Google Scholar]
- Anitua, E.; Andia, I.; Ardanza, B.; Nurden, P.; Nurden, A.T. Autologous platelets as a source of proteins for healing and tissue regeneration. Thromb. Haemost. 2004, 91, 4–15. [Google Scholar] [CrossRef]
- Plachokova, A.S.; Nikolidakis, D.; Mulder, J.; Jansen, J.A.; Creugers, N.H. Effect of platelet- rich plasma on bone regeneration in dentistry: A systematic review. Clin. Oral. Implants Res. 2008, 19, 539–545. [Google Scholar] [CrossRef]
- Kotsovilis, S.; Markou, N.; Pepelassi, E.; Nikolidakis, D. The adjunctive use of platelet- rich plasma in the therapy of periodontal intraosseous defects: A systematic review. J. Periodontal Res. 2010, 45, 428–443. [Google Scholar] [CrossRef]
- Del Fabbro, M.; Bortolin, M.; Taschieri, S. Is autologous platelet concentrate beneficial for post-extraction socket healing? a systematic review. Int. J. Oral. Maxillofac. Surg. 2011, 40, 891–900. [Google Scholar] [CrossRef]
- Miron, R.J.; Zucchelli, G.; Pikos, M.A.; Salama, M.; Lee, S.; Guillemette, V.; Fujioka-Kobayashi, M.; Bishara, M.; Zhang, Y.; Wang, H.L.; et al. Use of platelet-rich fibrin in regenerative dentistry: A systematic review. Clin. Oral. Investig. 2017, 21, 1913–1927. [Google Scholar] [CrossRef]
- Ahlowalia, M.S.; Patel, S.; Anwar, H.M.; Cama, G.; Austin, R.S.; Wilson, R.; Mannocci, F. Accuracy of CBCT for volumetric measurement of simulated periapical lesions. Int. Endod. J. 2013, 46, 538–546. [Google Scholar] [CrossRef]
- Kanagasingam, S.; Lim, C.X.; Yong, C.P.; Mannocci, F.; Patel, S. Diagnostic accuracy of periapical radiography and cone beam computed tomography in detecting apical periodontitis using histopathological findings as a reference standard. Int. Endod. J. 2017, 50, 417–426. [Google Scholar] [CrossRef]
- Mijiritsky, E.; Assaf, H.D.; Kolerman, R.; Mangani, L.; Ivanova, V.; Zlatev, S. Autologous Platelet Concentrates (APCs) for Hard Tissue Regeneration in Oral Implantology, Sinus Floor Elevation, Peri-Implantitis, Socket Preservation, and Medication-Related Osteonecrosis of the Jaw (MRONJ): A Literature Review. Biology 2022, 11, 1254. [Google Scholar] [CrossRef]
- Işık, G.; Özden Yüce, M.; Koçak-Topbaş, N.; Günbay, T. Guided bone regeneration simultaneous with implant placement using bovine-derived xenograft with and without liquid platelet-rich fibrin: A randomized controlled clinical trial. Clin. Oral. Investig. 2021, 25, 5563–5575. [Google Scholar] [CrossRef]
- Yelamali, T.; Saikrishna, D. Role of platelet rich fibrin and platelet rich plasma in wound healing of extracted third molar sockets: A comparative study. J. Maxillofac. Oral. Surg. 2015, 14, 410–416. [Google Scholar] [CrossRef]

{kind=link}
| Pubmed | (“endodontics” [MeSH Terms] OR “endodontic*” [All Fields] OR “endodontic surgery” [All Fields] OR “root-end surgery” [All Fields] OR “root-end resection” [All Fields] OR “surgical endodontic treatment” [All Fields] OR “endodontic healing” [All Fields] OR “apicoectomy” [MeSH Terms] OR “periapical surgery” [All Fields] OR “endodontic microsurgery” [All Fields]) AND (“platelet concentrates” [All Fields] OR “autologous platelet concentrates” [All Fields] OR “platelet-rich plasma” [All Fields] OR “Platelet-rich fibrin” [All Fields] OR “hemocomponents” [All Fields] OR “platelet rich in growth factors” [All Fields] OR “PRGF” [All Fields] OR “PRP” [All Fields] OR “PRF” [All Fields]) |
| Scopus | (TITLE-ABS-KEY (endodontic*) OR TITLE-ABS-KEY (“endodontic surgery”) OR TITLE-ABS-KEY (“root-end surgery”) OR TITLE-ABS-KEY (“root-end resection”) OR TITLE-ABS-KEY (“surgical endodontic treatment”) OR TITLE-ABS-KEY (“endodontic healing”) OR TITLE-ABS-KEY (apicoectomy*) OR TITLE-ABS-KEY (“periapical surgery”) OR TITLE-ABS-KEY (“endodontic microsurgery”)) AND (TITLE-ABS-KEY (“platelet concentrates”) OR TITLE-ABS-KEY (“autologous platelet concentrates”) OR TITLE-ABS-KEY (“platelet-rich plasma”) OR TITLE-ABS-KEY (“Platelet-rich fibrin”) OR TITLE-ABS-KEY (hemocomponents)) |
| Cochrane Oral Health Group Databases | (platelet concentrates in endodontic surgery);ti,ab,kw |
| Author, Year of Publication | Country | Type of Study | Total. n. of Patients, Age; Gender | Diagnosis | Intervention | Control | Follow-Up | Diagnostic Method | Outcome | Clinical Results | Radiographical Results |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Ahmed G.M. et al., 2018 [25] | Egypt, Cairo | RCT | 12 patients, from 18 to 45 years old; 9 female and 3 males | Periapical lesions in maxillary anterior teeth | Endodontic microsurgery with root-end preparations by ultrasonic retrotips and by filling with PRF gel or combined PRF gel and bioactive glass | 1 year follow-up | Cone beam computed tomography (CBCT) | Bone healing after endodontic microsurgery using PRF and PRF-BG | Decrease in the periapical lesion volume and healing of the periapical defects | ||
| Angerame D. et al., 2015 [26] | Italy, Trieste | RCT | 11 patients aged from 28 to 72: 6 female and 5 males | Chronic apical periodontitis | Endodontic microsurgery with root-end resection and retrograde filling | In the control group the bone defect was not filled | 1 year follow-up | Digital X-ray system was used for radiographic examination. A questionnaire was adopted for pain and swelling information. | Radiographic healing and the postoperative discomfort in patients undergoing apical surgery, either by leaving the apical surgical cavity empty or by filling it with the PRF gel | PRF test group felt less intense pain and swelling than the control group during the first hours and days postoperatively | PRF test group exhibited significantly better periapical healing scores than the control group |
| Del Fabbro M. et al., 2012 [27] | Italy, Milan | RCT | 36 patients; aged from 34 to 62; 20 women and 16 men | Chronic apical periodontitis | Endodontic microsurgery with retrograde root canal preparation: in the test group a thin layer of liquid PRGF was applied into the root-end and the defects was filled with a clot of PRGF | The control group was treated with modern endodontic surgery alone without using PRGF | 7 postoperative days | A quality of life questionnaire was adopted to evaluate postoperative limitations in function as well as pain and the presence of other symptoms. | Evaluate whether the use of PRGF might have a favorable impact on patient’s quality of life after endodontic surgery. | The test group showed significantly less pain and swelling, fewer analgesics taken, and improved functional activities as compared with the control group. | |
| Dhiman M. et al., 2015 [28] | India, Haryana | RCT | 30 patients aged 17–47: 11 women and 19 men | Suppurative chronic apical periodontitis and apicomarginal communication | Endodontic surgery with root-end resection, preparation, and root-end filling. In the test group a PRF membrane was been placed into the bone defect | In the control group no PRF membrane was used | 1 year follow-up | Follow-up radiographs were compared with postoperative radiographs | Healing of apicomarginal | PD showed a statistically significant reduction in the PRF group | Reduction of apical radiolucency in the test group after the 12 months follow-up |
| Goyal B. et al., 2011 [29] | India, Haryana | CCT | 30 patients divided into 3 groups; aged 17–45; 13 women and 17 men | Suppurative chronic apical periodontitis and apicomarginal communication | Endodontic surgery with root-end resection, preparation, and root-end filling. Subjects were assigned to the collagen membrane group, PRP group, and PRP + collagen sponge group without stratification. | In the control group collagen membrane (GTR) was shaped and placed over the defects | 1 year follow-up | The clinical parameters were measured on the buccal aspect of the interproximal space and the midbuccal aspect of the involved teeth using a periodontal Williams O probe. The radiographs were taken with the Rinn parallel technique | Compare the healing responses of platelet-rich plasma (PRP), PRP + a collagen sponge, and a collagen membrane | All the three treatments showed highly significant reductions in the PD, CAL, and in gingival margin position | All the three treatments showed highly significant radiographic reduction of the size of the periapical lesion, the percentage reduction of the periapical rarefactions and periapical healing |
| Meschi N. et al., 2018 [30] | Belgium, Leuven | RCT | 50 patients divided into two groups; aged 16–79; 28 women and 22 men | Patients in need of root-end surgery due to periapical lesions | Endodontic microsurgery with root-end resection, preparation, and filling. In the test group, LPRF with or without BG was placed before flap repositioning. | In the control group was not added LPRF | 1 week post RES | Patients completed daily for 1 week a visual analog pain scale (VAS) and a 5-point Likert-type scale questionnaire | Impact of the adjunct of leukocyte- and platelet-rich fibrin (LPRF) to root-end surgery (RES) on the patients’ quality of life during the first week post RES. | No evidence for a difference between the test and control group in VAS, occurrence of pain symptoms, impairment of daily activities, and medication use, over the 7 days and daily during the 7 days post RES. | |
| Meschi N. et al., 2020 [31] | Belgium, Leuven | RCT | 50 patients divided into four groups; aged 27–57; 28 female and 22 men | Patients in need of root-end surgery due to periapical lesions | 3 mm root-end resection, and removal of the cyst or granuloma; root-end preparation of 3–5 mm with an ultrasonic device and root-end filling with mineral trioxide aggregate | Application of a BG membrane, or nothing | 1 year post RES | Ultrasound imaging, periapical radiographs, and cone-beam computed tomography were used to evaluate bone healing | Periapical bone healing | The addition of an occlusive membrane rather than an autologous platelet concentrates improved bone regeneration 1 year post RES significantly, irrespective of the assessment device applied | |
| Monga P. et al., 2016 [32] | India, Punjab | CCT | 30 patients divided into 3 groups (A, B and C) | Periapical lesions such as granulomas and cysts | Endodontic surgery with root-end resection, preparation, and root-end filling. In Group A, root-end cavity was filled with MTA. In Group B, with MTA followed by placement of hydroxyapatite in the curetted periapical defect. In Group C, with MTA followed by placement of PRF in the curetted periapical defect. | 9 months follow-up | Patients were examined clinically regarding postoperative discomfort, pain, sensitivity to percussion, and presence/absence of swelling. Radiographically, an intraoral periapical radiograph as taken on each follow-up visit. | Effectiveness of periapical surgery using MTA as a retrograde filling material with/without using hydroxyapatite or PRF in curetted periapical defect | A significantly higher rate of healing was observed after 9 months when apicoectomy was performed using retrograde filling materials with PRF as a graft material in Group C followed by hydroxyapatite n Group B as compared to Group A, where no graft material was added in the curetted periapical defect | ||
| Parihk B. et al., 2011 [33] | India, Baroda | CCT | 24-year-old male patient | Upper central incisors fractured and bilateral periapical radiolucency | RES with cystic enucleation bilaterally; retrograde cavity preparations were performed along the long axis of the tooth to a depth of 3–4 mm; MTA was used as a root-end filling material | PRP was applied in only one unilateral incisor | 2 years follow-up | Vitality test, radiographic endoral and spiral computed tomography | Healing periapical lesions treated with and without the use of platelet- rich plasma | Definite healing seen in the lesion treated with PRP on the radiograph | |
| Singh R. et al., 2020 [34] | India, Rajasthan | CCT | 126 patients aged between 18 and 38 years divided into 3 groups | Periapical lesions such as periapical abscess, cyst, and granuloma in the maxillary anterior region | Endodontic surgery with root-end resection, preparation, and root-end filling. | In the other two groups CERAMENT and hydroxyapatite were used | 1 year follow-up | Preoperative and postoperative radiographs were taken by following the paralleling technique. Vitality was evaluated with thermal testing. | Compare hydroxyapatite granules, CERAMENT, and platelet-rich fibrin (PRF) in the management of endodontic apical surgery cases | PRF is superior in terms of reducing pain, mobility, and sinus as compared to hydroxyapatite and CERAMENT | Definite healing seen in the lesion treated with A-PRF on the radiograph |
| Soto-Penaloza D. et al., 2020 [35] | Spain, Valencia | RCT | 50 patients divided into 2 groups; aged 17–79; 28 women and 22 men | 50 apical lesions of upper maxilla (second premolar to the second premolar) | Endodontic surgery with root-end resection, preparation, and root-end filling. In the test group A-PRF + membranes were placed inside the bony crypt | In the control group was not added A-PRF | 1 week after surgery | Pain perception and quality of life (functional limitations and other symptoms) were assessed 1 week after surgery using a visual analog scale and a Likert scale-based questionnaire. | Postoperative pain, and quality of life in endodontic | Pain perception was mild in both groups versus; it proved less variable during the first 4 days in test group, showing lower extreme pain values. | |
| Taschieri S. et al., 2013 [36] | Italy, Milan | CCT | 20 patients divided into 2 groups; aged 29–55; 11 female and 9 males | Patients treated by microsurgical endodontic treatment in molar and premolar maxillary region. | Endodontic retrograde treatment | In the control group platelet concentrates was not used | 1 year follow-up | A questionnaire was administered to all subjects to evaluate postoperative functional limitations as well as pain and the presence of other symptoms. Periapical radiographs were taken at follow-up | Postoperative quality of life | Significantly improved patients’ quality of life was observed in the test group considering symptoms as swelling, or taste, and pain. Also, functional activities were less impaired in the test group. | |
| Thakur V. et al., 2023 [37] | Haryana, India | RCT | 40 patients divided into the following 2 groups: test group with PRF High and control group with PRF Medium (20 male, 20 female). | Patients presenting with endodontic lesions and concomitant periodontal communication. | Endodontic surgery with root-end resection, preparation, and root-end filling. | In the control group PRF-Medium was used. | 1 week after surgery for clinical parameters and 1 year follow-up for radiographical parameters | Quality of life questionnaire and visual analogic scale (VAS) for clinical outcomes and CBCT for radiographic outcomes. | Postoperative quality of life and periapical bone healing. | PRF Medium group patients re- ported significantly less swelling on the 1st and 3rd days, and average pain on the 2nd and 4th days postoperatively. | The difference in success rate for periapical healing was non-significant between the PRF Medium group and PRF High group in both 2D and 3D imaging. |
| Yahata Y. et al., 2023 [38] | Japan | RCT | 24 patients (8 male, 16 female) divided into two groups. | Patients in need of root-end microsurgery due to periapical lesions. | Root-end resection was accomplished approximately 3 mm from the apex. The root-end cavity preparation was performed using ultrasonic microtips up to a depth of 3 mm in the canal space along the long axis. | In the control group no CGF was used. | 1 year follow-up with follow-up cone-beam computed tomography (CBCT) at 6 months. | Periapical radiography and CBCT for radiographic parameters and VAS score for clinical parameters. | Postoperative discomfort and periapical bone healing. | Regard to the VAS scores, there was no significant difference between the two groups preoperatively and at all postoperative appointments. | The lesion volume reduction rate in the CGF group (75.6%) was significantly higher than that in the control (61.0%) group. |
| Study | Was True Randomization Used for Assignment of Participants to Treatment Groups? | Was Allocation to Treatment Groups Concealed? | Were Treatment Groups Similar at the Baseline? | Were Participants Blind to Treatment Assignment? | Were Those Delivering Treatment Blind to Treatment Assignment? | Were Outcomes Assessors Blind to Treatment Assignment? | Were Treatment Groups Treated Identically Other than the Intervention of Interest? | Was Follow-Up Complete and if Not, Were Differences between Groups In Terms of Their Follow-Up Adequately Described and Analyzed? | Were Participants Analyzed in the Groups to Which They Were Randomized? | Were Outcomes Measured in the Same Way for Treatment Groups? | Were Outcomes Measured in a Reliable Way? | Was Appropriate Statistical Analysis Used? | Was the Trial Design Appropriate, and Any Deviations from the Standard RCT Design in the Conduct and Analysis of the Trial? | Overall Risk of Bias |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Angerame D. et al., 2015 [26] | YES | YES | YES | YES | UNCLEAR | UNCLEAR | YES | NO | UNCLEAR | YES | YES | YES | YES | moderate |
| Ahmed G.M. et al., 2018 [25] | YES | YES | YES | UNCLEAR | UNCLEAR | YES | YES | YES | YES | YES | YES | YES | YES | low |
| Del Fabbro M. et al., 2012 [27] | YES | YES | YES | UNCLEAR | UNCLEAR | YES | YES | YES | YES | YES | YES | YES | YES | low |
| Dhiman M. et al., 2015 [28] | YES | YES | YES | UNCLEAR | UNCLEAR | YES | YES | YES | YES | YES | YES | YES | YES | low |
| Meschi N. et al., 2018 [30] | YES | YES | YES | UNCLEAR | UNCLEAR | YES | YES | YES | YES | YES | YES | YES | UNCLEAR | moderate |
| Meschi N. et al., 2020 [31] | YES | YES | YES | UNCLEAR | UNCLEAR | YES | YES | YES | YES | YES | YES | YES | UNCLEAR | moderate |
| Soto-Penaloza D. et al., 2020 [35] | YES | YES | YES | UNCLEAR | UNCLEAR | YES | YES | YES | YES | YES | YES | YES | YES | low |
| Thakur V. et al., 2023 [37] | YES | YES | YES | YES | YES | UNCLEAR | YES | YES | UNCLEAR | YES | YES | YES | YES | low |
| Yahata Y. et al., 2023 [38] | YES | YES | YES | YES | YES | UNCLEAR | YES | YES | UNCLEAR | YES | YES | YES | UNCLEAR | low |
| Study | Is It Clear in the Study What Is the ‘Cause’ and What Is the ‘Effect’? | Were the Participants Included in Any Comparisons Similar? | Were the Participants Included in Any Comparisons Receiving Similar Treatment/Care, Other than the Exposure or Intervention of Interest? | Was There a Control Group? | Were There Multiple Measurements of the Outcome Both Pre and Post the Intervention/Exposure? | Was Follow-Up Complete and if Not, Were Differences between Groups in Terms of Their Follow-Up Adequately Described and Analyzed? | Were the Outcomes of Participants Included in Any Comparisons Measured in the Same Way? | Were Outcomes Measured in a Reliable Way? | Were Appropriate Statistical Analysis Used? | Overall Risk of Bias |
|---|---|---|---|---|---|---|---|---|---|---|
| Goyal B. et al., 2011 [29] | YES | YES | YES | YES | NO | NO | YES | YES | YES | moderate |
| Monga P. et al., 2016 [32] | YES | YES | YES | YES | NO | NO | YES | YES | YES | moderate |
| Parihk B. et al., 2011 [33] | YES | NOT APPLICABLE | NOT APPLICABLE | YES | NO | UNCLEAR | YES | UNCLEAR | YES | high |
| Singh R. et al., 2020 [34] | YES | YES | YES | YES | NO | YES | YES | UNCLEAR | YES | moderate |
| Taschieri S. et al., 2013 [36] | YES | YES | YES | YES | YES | YES | YES | YES | YES | low |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
di Lauro, A.E.; Valletta, A.; Aliberti, A.; Cangiano, M.; Dolce, P.; Sammartino, G.; Gasparro, R. The Effectiveness of Autologous Platelet Concentrates in the Clinical and Radiographic Healing after Endodontic Surgery: A Systematic Review. Materials 2023, 16, 7187. https://doi.org/10.3390/ma16227187
di Lauro AE, Valletta A, Aliberti A, Cangiano M, Dolce P, Sammartino G, Gasparro R. The Effectiveness of Autologous Platelet Concentrates in the Clinical and Radiographic Healing after Endodontic Surgery: A Systematic Review. Materials. 2023; 16(22):7187. https://doi.org/10.3390/ma16227187
Chicago/Turabian Styledi Lauro, Alessandro Espedito, Alessandra Valletta, Angelo Aliberti, Mario Cangiano, Pasquale Dolce, Gilberto Sammartino, and Roberta Gasparro. 2023. "The Effectiveness of Autologous Platelet Concentrates in the Clinical and Radiographic Healing after Endodontic Surgery: A Systematic Review" Materials 16, no. 22: 7187. https://doi.org/10.3390/ma16227187
APA Styledi Lauro, A. E., Valletta, A., Aliberti, A., Cangiano, M., Dolce, P., Sammartino, G., & Gasparro, R. (2023). The Effectiveness of Autologous Platelet Concentrates in the Clinical and Radiographic Healing after Endodontic Surgery: A Systematic Review. Materials, 16(22), 7187. https://doi.org/10.3390/ma16227187