
A Bioelectrical Impedance Analysis in Adult Subjects: The Relationship between Phase Angle and Body Cell Mass

 , , , , ,
, , , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Setting
2.2. Population Study
- Male and female subjects aged from 23 to 54 years.
- A BMI between 16 and 34.9 kg/m2.
- The presence of clinical conditions that, according to the researcher, potentially render the subject ineligible for the study.
- The presence of any of the following pre-existing conditions: cancer, autoimmune diseases, Type 2 Diabetes Mellitus, Type 1 Diabetes Mellitus, or chronic inflammatory diseases.
- Pregnancy or breastfeeding.
- Alcohol and/or drug abuse.
- Subjects with implanted pacemakers or defibrillators, because of the theoretical possibility of interference with the device activity due to the field of current induced by the impedance measurements.
- The presence of psychiatric disturbances (personality disorders, depression, or alcohol or substance abuse in the past two years) evaluated by a physician.
- Unsigned informed consent.
2.3. Anthropometric Measurements
2.4. Body Composition
2.5. Statistical Analysis
3. Results
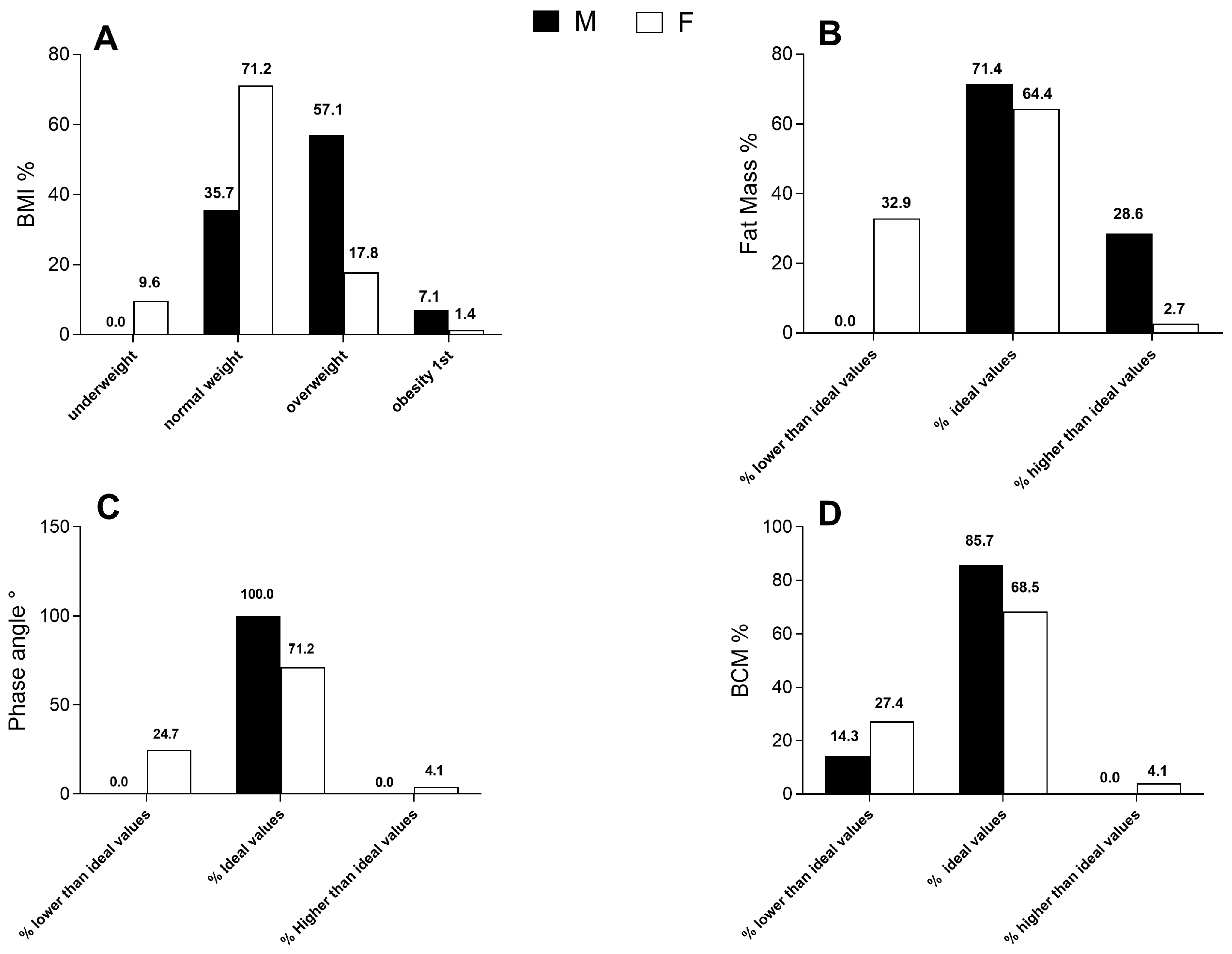
3.1. Body Mass Index
3.2. Fat Mass
3.3. Phase Angle
3.4. BCM
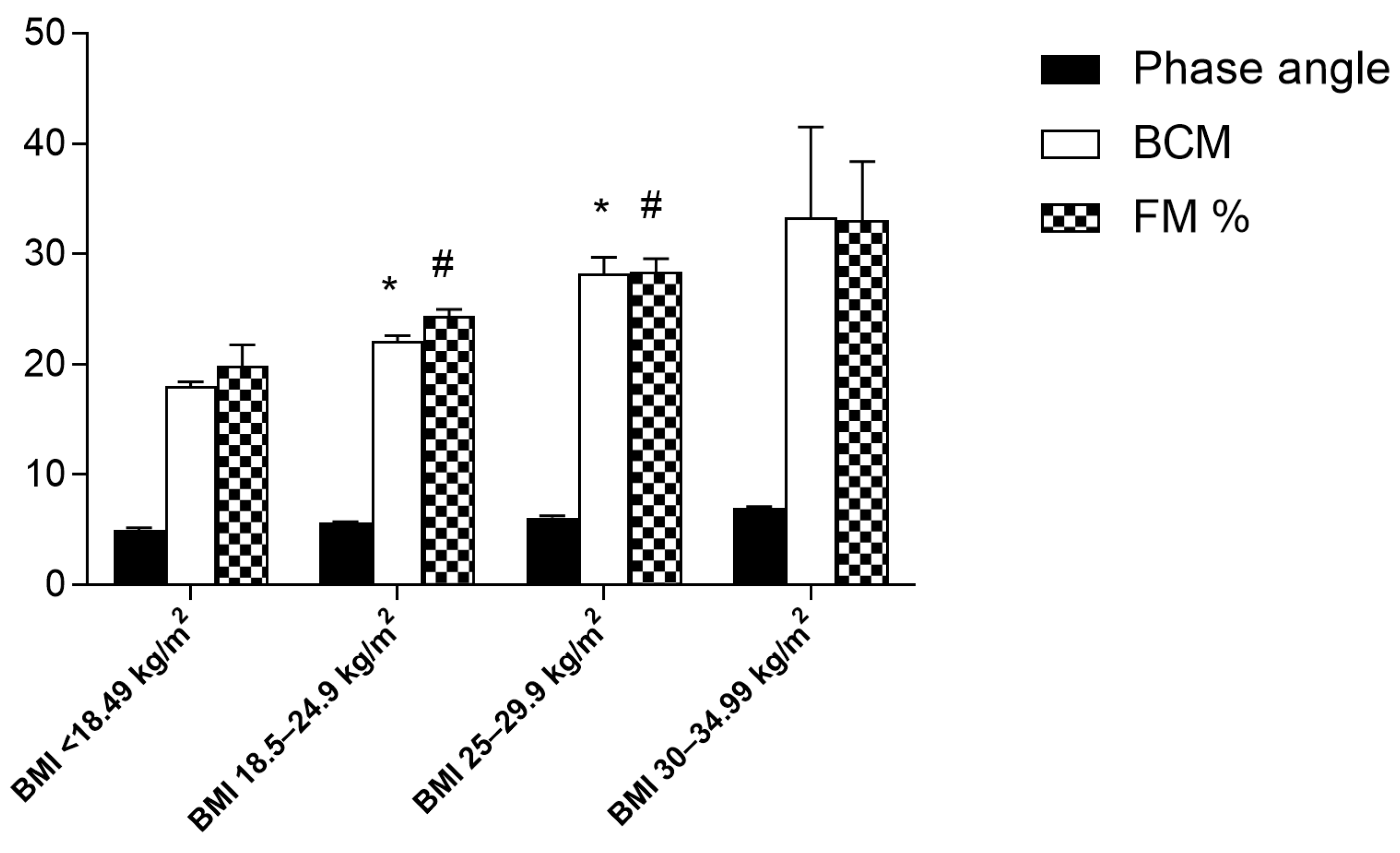
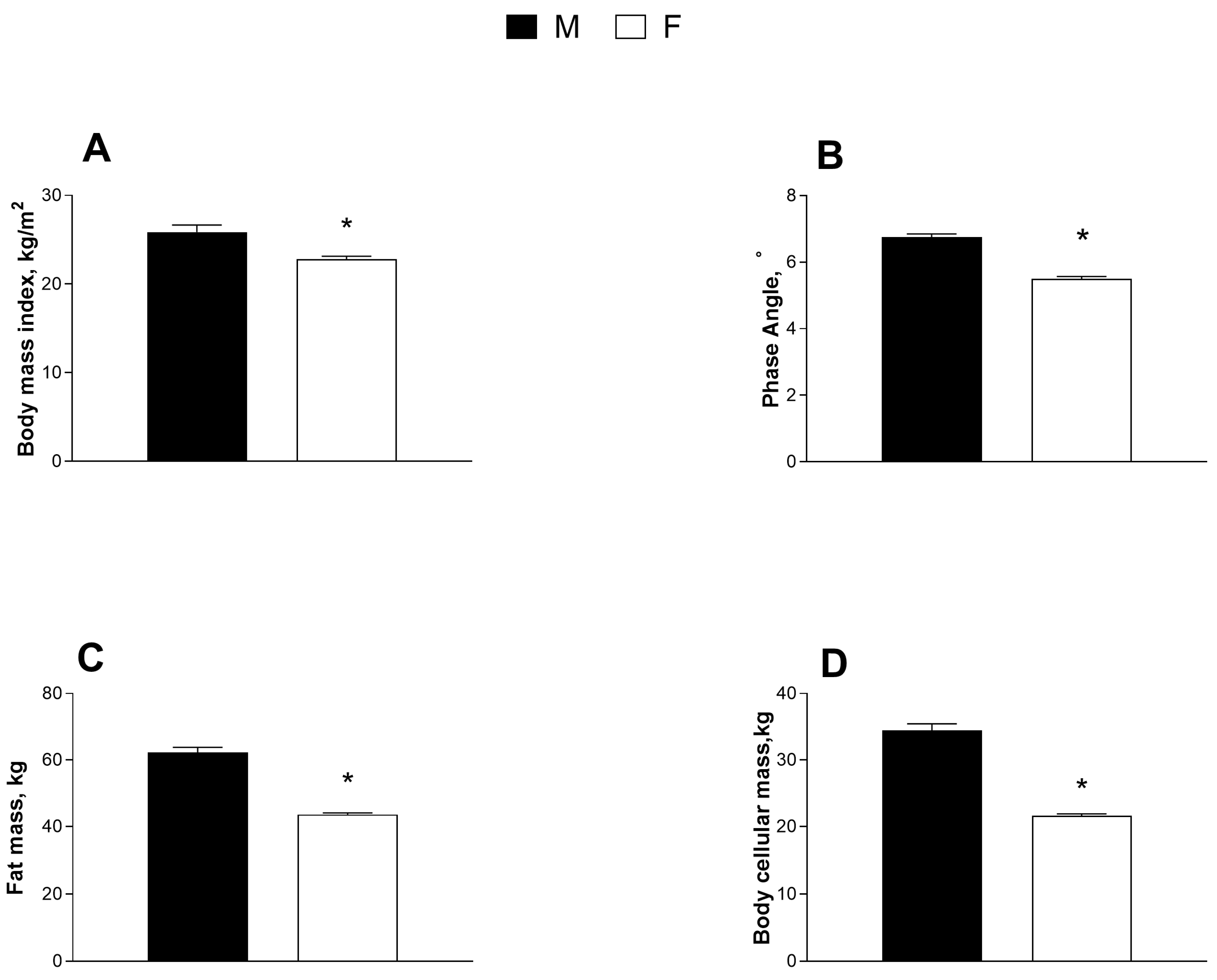
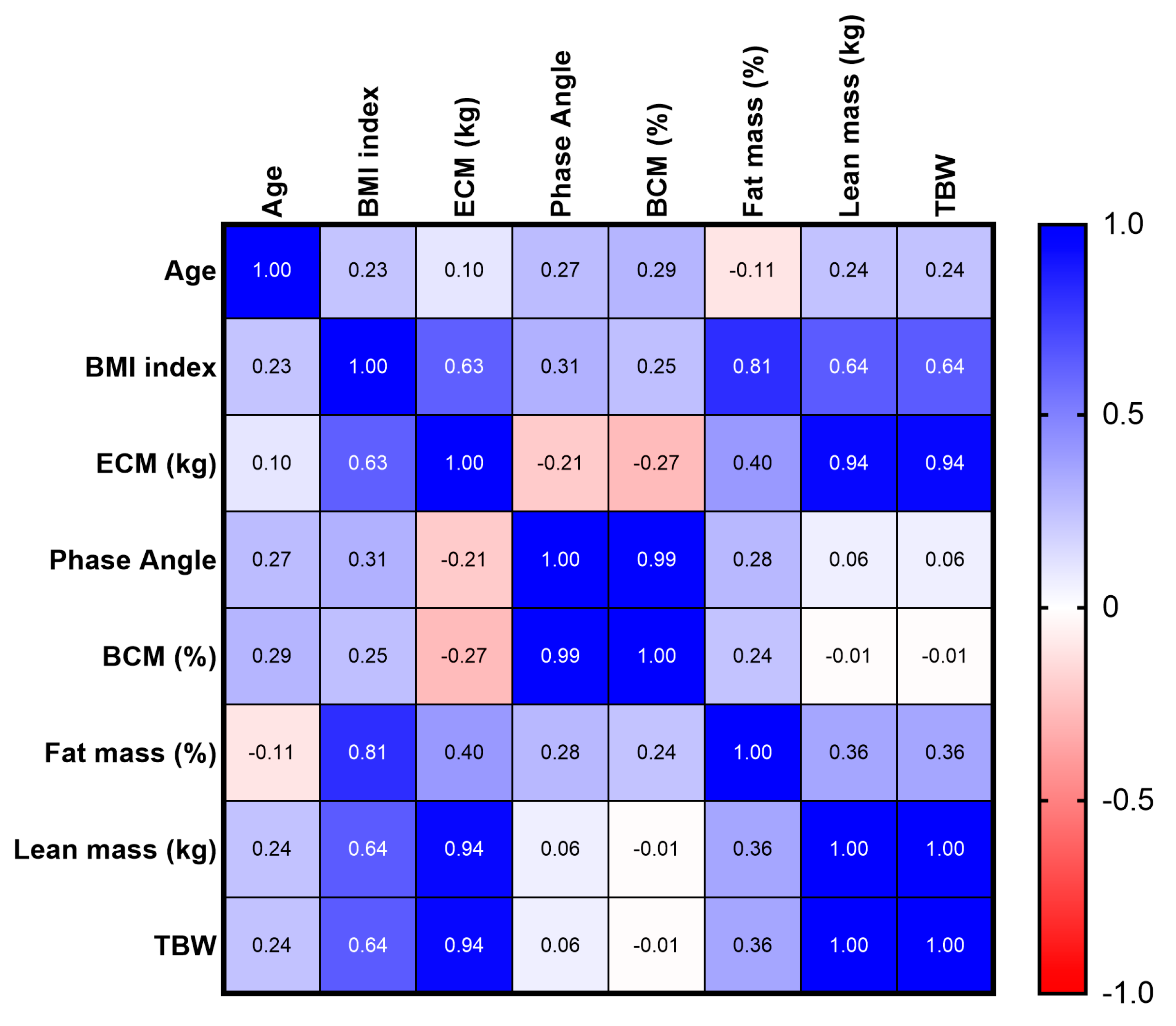
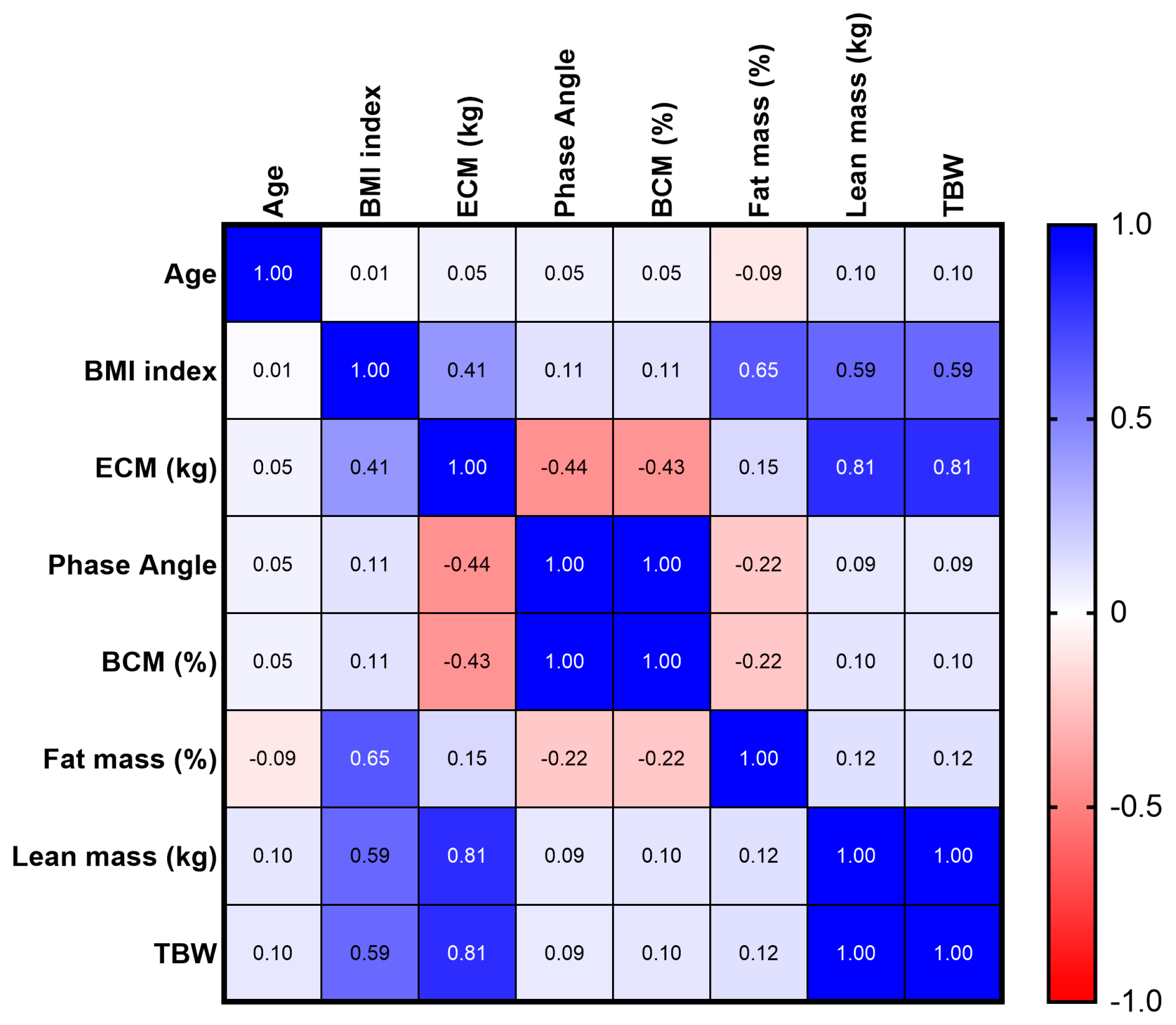
3.5. Body Mass Index, Phase Angle, Body Cell Mass, Fat Mass
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Robinson, S.M. Improving Nutrition to Support Healthy Ageing: What Are the Opportunities for Intervention? Proc. Nutr. Soc. 2018, 77, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Gomez, G.; Botero-Rodríguez, F.; Misas, J.D.; Garcia-Cifuentes, E.; Sulo, S.; Brunton, C.; Venegas-Sanabria, L.C.; Gracia, D.A.; Cano Gutierrez, C.A. A Nutritionally Focused Program for Community-Living Older Adults Resulted in Improved Health and Well-Being. Clin. Nutr. 2022, 41, 1549–1556. [Google Scholar] [CrossRef] [PubMed]
- Lukaski, H.C.; Kyle, U.G.; Kondrup, J. Assessment of Adult Malnutrition and Prognosis with Bioelectrical Impedance Analysis. Curr. Opin. Clin. Nutr. Metab. Care 2017, 20, 330–339. [Google Scholar] [CrossRef] [PubMed]
- Thibault, R.; Genton, L.; Pichard, C. Body Composition: Why, When and for Who? Clin. Nutr. 2012, 31, 435–447. [Google Scholar] [CrossRef] [PubMed]
- Bonaccorsi, G.; Santomauro, F.; Lorini, C.; Indiani, L.; Pellegrino, E.; Pasquini, G.; Molino-Lova, R.; Epifani, F.; Macchi, C. Risk of Malnutrition in a Sample of Nonagenarians: Specific versus Classic Bioelectrical Impedance Vector Analysis. Nutrition 2016, 32, 368–374. [Google Scholar] [CrossRef]
- Ellulu, M.; Abed, Y.; Rahmat, A.; Ranneh, Y.; Ali, F. Epidemiology of Obesity in Developing Countries: Challenges and Prevention. Glob. Epidemic Obes. 2014, 2, 2. [Google Scholar] [CrossRef] [Green Version]
- Swainson, M.G.; Batterham, A.M.; Tsakirides, C.; Rutherford, Z.H.; Hind, K. Prediction of Whole-Body Fat Percentage and Visceral Adipose Tissue Mass from Five Anthropometric Variables. PLoS ONE 2017, 12, e0177175. [Google Scholar] [CrossRef] [PubMed]
- Ehrampoush, E.; Arasteh, P.; Homayounfar, R.; Cheraghpour, M.; Alipour, M.; Naghizadeh, M.M.; Hadibarhaghtalab, M.; Davoodi, S.H.; Askari, A.; Razaz, J.M. New Anthropometric Indices or Old Ones: Which Is the Better Predictor of Body Fat? Diabetes Metab. Syndr. Clin. Res. Rev. 2017, 11, 257–263. [Google Scholar] [CrossRef]
- Biolo, G.; Di Girolamo, F.G.; Breglia, A.; Chiuc, M.; Baglio, V.; Vinci, P.; Toigo, G.; Lucchin, L.; Jurdana, M.; Pražnikar, Z.J.; et al. Inverse Relationship between “a Body Shape Index” (ABSI) and Fat-Free Mass in Women and Men: Insights into Mechanisms of Sarcopenic Obesity. Clin. Nutr. 2015, 34, 323–327. [Google Scholar] [CrossRef] [PubMed]
- Catapano, A.; Trinchese, G.; Cimmino, F.; Petrella, L.; D’Angelo, M.; Di Maio, G.; Crispino, M.; Cavaliere, G.; Monda, M.; Mollica, M.P. Impedance Analysis to Evaluate Nutritional Status in Physiological and Pathological Conditions. Nutrients 2023, 15, 2264. [Google Scholar] [CrossRef] [PubMed]
- Vassilev, G.; Hasenberg, T.; Krammer, J.; Kienle, P.; Ronellenfitsch, U.; Otto, M. The Phase Angle of the Bioelectrical Impedance Analysis as Predictor of Post-Bariatric Weight Loss Outcome. Obes. Surg. 2017, 27, 665–669. [Google Scholar] [CrossRef] [PubMed]
- Schwenk, A.; Beisenherz, A.; Kremer, G.; Diehl, V.; Salzberger, B.; Fätkenheuer, G. Bioelectrical impedance analysis in HIV-infected patients treated with triple antiretroviral treatment. Am. J. Clin. Nutr. 1999, 5, 867–873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamada, Y.; Buehring, B.; Krueger, D.; Anderson, R.M.; Schoeller, D.A.; Binkley, N. Electrical Properties Assessed by Bioelectrical Impedance Spectroscopy as Biomarkers of Age-Related Loss of Skeletal Muscle Quantity and Quality. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 72, glw225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norman, K.; Stobäus, N.; Zocher, D.; Bosy-Westphal, A.; Szramek, A.; Scheufele, R.; Smoliner, C.; Pirlich, M. Cutoff Percentiles of Bioelectrical Phase Angle Predict Functionality, Quality of Life, and Mortality in Patients with Cancer. Am. J. Clin. Nutr. 2010, 92, 612–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wirth, R.; Volkert, D.; Rösler, A.; Sieber, C.C.; Bauer, J.M. Bioelectric Impedance Phase Angle Is Associated with Hospital Mortality of Geriatric Patients. Arch. Gerontol. Geriatr. 2010, 51, 290–294. [Google Scholar] [CrossRef]
- Hedley, A.A. Prevalence of Overweight and Obesity Among US Children, Adolescents, and Adults, 1999-2002. JAMA 2004, 291, 2847. [Google Scholar] [CrossRef] [Green Version]
- Weir, C.B.; Jan, A. BMI Classification Percentile And Cut Off Points; StatPearls Publishing LLC: Tampa, FL, USA, 2023. [Google Scholar]
- Kushner, R.F. Bioelectrical Impedance Analysis: A Review of Principles and Applications. J. Am. Coll. Nutr. 1992, 11, 199–209. [Google Scholar] [CrossRef]
- Piccoli, A.; Nigrelli, S.; Caberlotto, A.; Bottazzo, S.; Rossi, B.; Pillon, L.; Maggiore, Q. Bivariate Normal Values of the Bioelectrical Impedance Vector in Adult and Elderly Populations. Am. J. Clin. Nutr. 1995, 61, 269–270. [Google Scholar] [CrossRef]
- Piccoli, A.; Brunani, A.; Savia, G.; Pillon, L.; Favaro, E.; Berselli, M.; Cavagnini, F. Discriminating between Body Fat and Fluid Changes in the Obese Adult Using Bioimpedance Vector Analysis. Int. J. Obes. 1998, 22, 97–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paiva, S.I.; Borges, L.R.; Halpern-Silveira, D.; Assunção, M.C.; Barros, A.J.; Gonzalez, M.C. Standardized phase angle from bioelectrical impedance analysis as prognostic factor for survival in patients with cancer. Support. Care Cancer 2010, 2, 187–192. [Google Scholar] [CrossRef]
- González Jiménez, E. Body Composition: Assessment and Clinical Value. Endocrinol. Nutr. 2013, 60, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Kyle, U.G.; Soundar, E.P.; Genton, L.; Pichard, C. Can Phase Angle Determined by Bioelectrical Impedance Analysis Assess Nutritional Risk? A Comparison between Healthy and Hospitalized Subjects. Clin. Nutr. 2012, 31, 875–881. [Google Scholar] [CrossRef] [PubMed]
- Identifying Patients at Risk: ADA’s Definitions for Nutrition Screening and Nutrition Assessment. Council on Practice (COP) Quality Management Committee. J. Am. Diet. Assoc. 1994, 94, 838–839. [Google Scholar] [CrossRef]
- Ramírez-Vélez, R.; Correa-Bautista, J.; Sanders-Tordecilla, A.; Ojeda-Pardo, M.; Cobo-Mejía, E.; Castellanos-Vega, R.; García-Hermoso, A.; González-Jiménez, E.; Schmidt-RioValle, J.; González-Ruíz, K. Percentage of Body Fat and Fat Mass Index as a Screening Tool for Metabolic Syndrome Prediction in Colombian University Students. Nutrients 2017, 9, 1009. [Google Scholar] [CrossRef] [Green Version]
- Okorodudu, D.O.; Jumean, M.F.; Montori, V.M.; Romero-Corral, A.; Somers, V.K.; Erwin, P.J.; Lopez-Jimenez, F. Diagnostic Performance of Body Mass Index to Identify Obesity as Defined by Body Adiposity: A Systematic Review and Meta-Analysis. Int. J. Obes. 2010, 34, 791–799. [Google Scholar] [CrossRef] [Green Version]
- Ross, R.; Shaw, K.; Rissanen, J.; Martel, Y.; de Guise, J.; Avruch, L. Sex Differences in Lean and Adipose Tissue Distribution by Magnetic Resonance Imaging: Anthropometric Relationships. Am. J. Clin. Nutr. 1994, 59, 1277–1285. [Google Scholar] [CrossRef]
- Seger, J.C.; Horn, D.B.; Westman, E.C.; Lindquist, R.; Scinta, W.; Richardson, L.A.; Primack, C.; Bryman, D.A.; McCarthy, W.; Hendricks, E.; et al. American Society of Bariatric Physicians Obesity Algorithm: Adult Adiposity Evaluation and Treatment 2013. Available online: www.obesityalgorithm.org (accessed on 28 June 2023).
- Heymsfield, S.B.; Ebbeling, C.B.; Zheng, J.; Pietrobelli, A.; Strauss, B.J.; Silva, A.M.; Ludwig, D.S. Multi-Component Molecular-Level Body Composition Reference Methods: Evolving Concepts and Future Directions. Obes. Rev. 2015, 16, 282–294. [Google Scholar] [CrossRef] [Green Version]
- Dumler, F.; Kilates, C. Use of Bioelectrical Impedance Techniques for Monitoring Nutritional Status in Patients on Maintenance Dialysis. J. Ren. Nutr. 2000, 10, 116–124. [Google Scholar] [CrossRef]
- da Silva, B.R.; Gonzalez, M.C.; Cereda, E.; Prado, C.M. Exploring the potential role of phase angle as a marker of oxidative stress: A narrative review. Nutrition 2022, 93, 111493. [Google Scholar] [CrossRef]
- Campa, F.; Toselli, S.; Mazzilli, M.; Gobbo, L.A.; Coratella, G. Assessment of Body Composition in Athletes: A Narrative Review of Available Methods with Special Reference to Quantitative and Qualitative Bioimpedance Analysis. Nutrients 2021, 5, 1620. [Google Scholar] [CrossRef]
- Langer, R.D.; Larsen, S.C.; Ward, L.C.; Heitmann, B.L. Phase angle measured by bioelectrical impedance analysis and the risk of cardiovascular disease among adult Danes. Nutrition 2021, 89, 111280. [Google Scholar] [CrossRef] [PubMed]
- Dittmar, M.; Reber, H.; Kahaly, G.J. Bioimpedance phase angle indicates catabolism in Type 2 diabetes. Diabet. Med. 2015, 9, 1177–1185. [Google Scholar] [CrossRef] [PubMed]
- Norman, K.; Smoliner, C.; Kilbert, A.; Valentini, L.; Lochs, H.; Pirlich, M. Disease-Related Malnutrition but Not Underweight by BMI Is Reflected by Disturbed Electric Tissue Properties in the Bioelectrical Impedance Vector Analysis. Br. J. Nutr. 2008, 100, 590–595. [Google Scholar] [CrossRef] [PubMed]
- Torres, A.G.; Oliveira, K.J.F.; Oliveira, A.V.; Gonçalves, M.; Koury, J.C. Biological determinants of phase angle among Brazilian elite athletes. Proc. Nutr. Soc. 2009, 67, 2018. [Google Scholar] [CrossRef] [Green Version]
- Koury, J.C.; Trugo, N.M.F.; Torres, A.G. Phase angle and bioelectrical impedance vectors in adolescent and adult male athletes. Int. J. Sports Physiol. Perform. 2014, 5, 798–804. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cimmino, F.; Petrella, L.; Cavaliere, G.; Ambrosio, K.; Trinchese, G.; Monda, V.; D’Angelo, M.; Di Giacomo, C.; Sacconi, A.; Messina, G.; et al. A Bioelectrical Impedance Analysis in Adult Subjects: The Relationship between Phase Angle and Body Cell Mass. J. Funct. Morphol. Kinesiol. 2023, 8, 107. https://doi.org/10.3390/jfmk8030107
Cimmino F, Petrella L, Cavaliere G, Ambrosio K, Trinchese G, Monda V, D’Angelo M, Di Giacomo C, Sacconi A, Messina G, et al. A Bioelectrical Impedance Analysis in Adult Subjects: The Relationship between Phase Angle and Body Cell Mass. Journal of Functional Morphology and Kinesiology. 2023; 8(3):107. https://doi.org/10.3390/jfmk8030107
Chicago/Turabian StyleCimmino, Fabiano, Lidia Petrella, Gina Cavaliere, Katia Ambrosio, Giovanna Trinchese, Vincenzo Monda, Margherita D’Angelo, Cristiana Di Giacomo, Alessandro Sacconi, Giovanni Messina, and et al. 2023. "A Bioelectrical Impedance Analysis in Adult Subjects: The Relationship between Phase Angle and Body Cell Mass" Journal of Functional Morphology and Kinesiology 8, no. 3: 107. https://doi.org/10.3390/jfmk8030107