Gender Phenotyping of Patients with Obstructive Sleep Apnea Syndrome Using a Network Science Approach




Abstract
1. Introduction
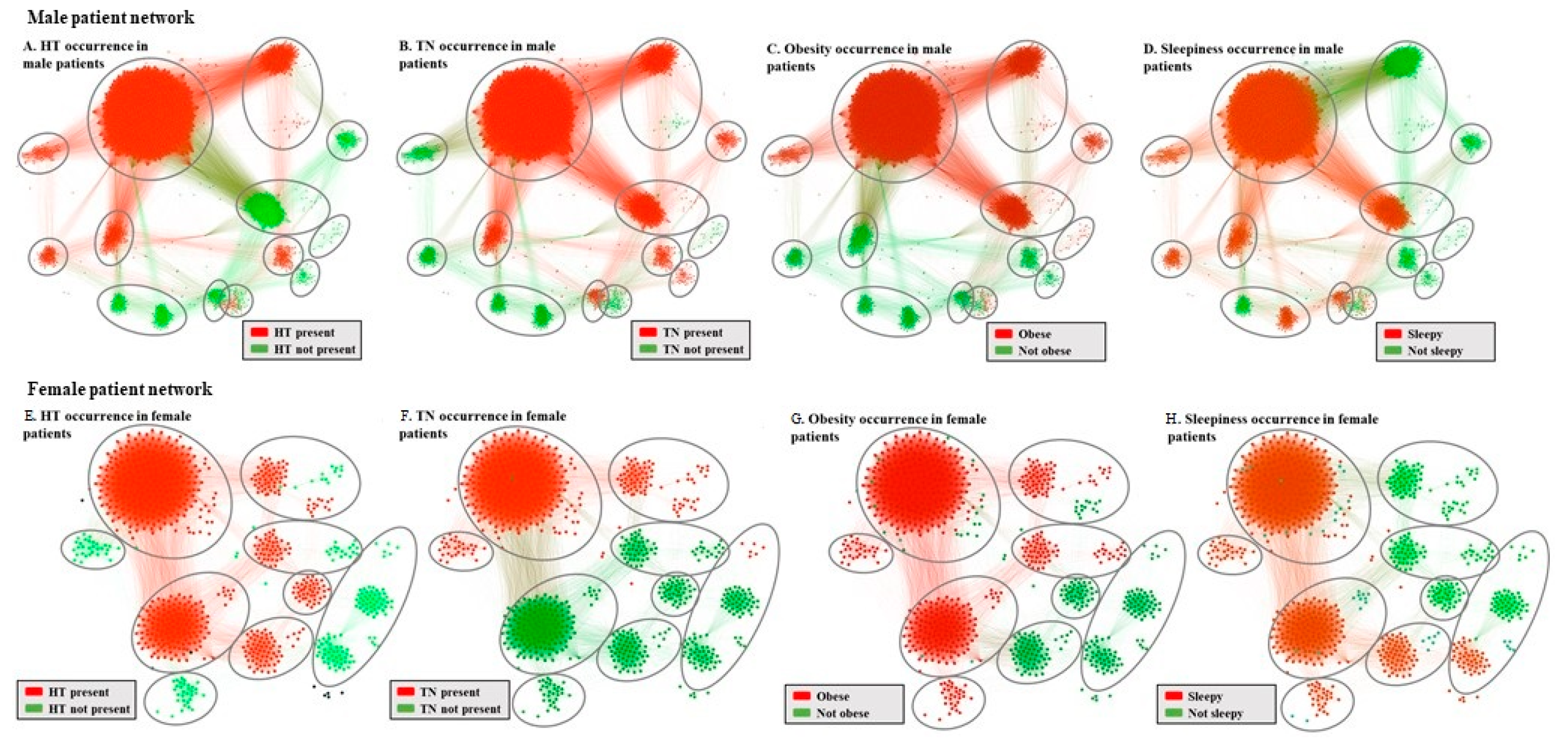
- We apply independent network-based clustering algorithms on a mixed (i.e., male and female) cohort to uncover gender-specific phenotypes.
- We describe each phenotype and compare them in terms of genders to underline the individual role parameters associated with OSAS.
- We associate phenotypes with comorbidities, highlighting the differences between genders and defining characteristic OSAS development patterns.
2. Experimental Section
2.1. Study Design and Participants
2.2. Statistical Analysis and OSAS Risk Assessment
2.3. Network Medicine Modelling
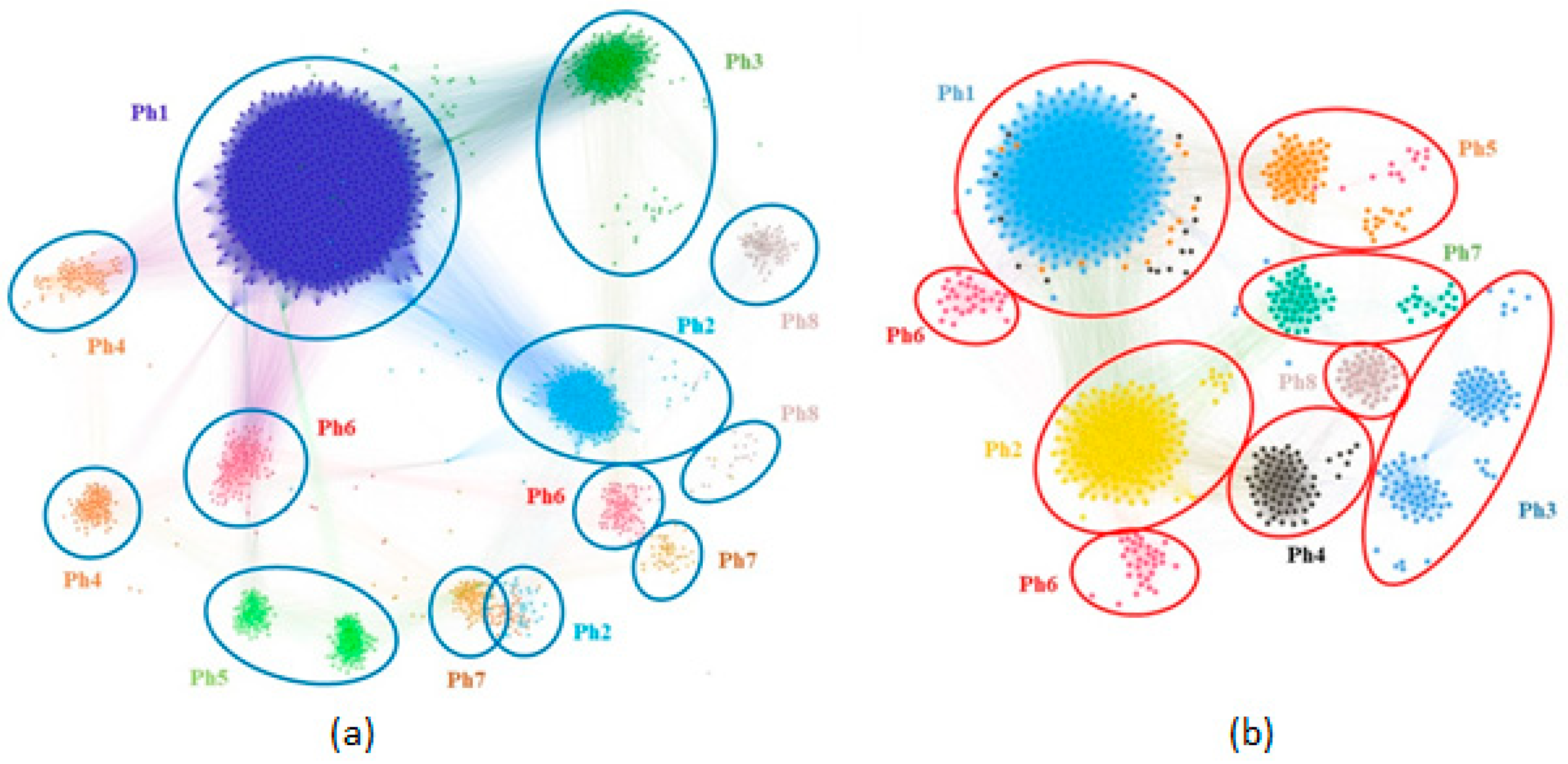
2.4. Patient Phenotyping
3. Results
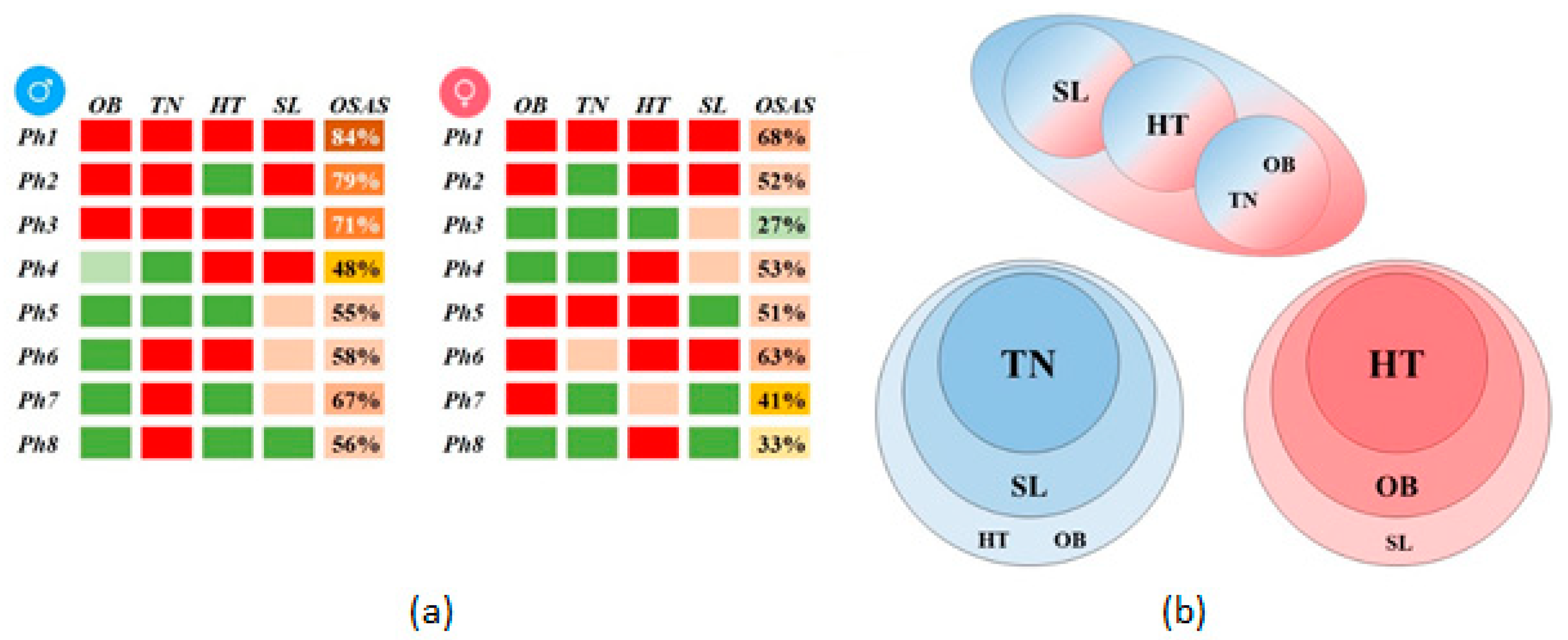
- Phenotype Ph1 (severe) corresponds to the sickest subjects that are obese, have a thick neck, high BP, and sleepiness, with coronary artery disease (CAD), congestive heart failure (CHF), nasal septal deviation (NSD), and arrhythmia (AR).
- Phenotype Ph2 (severe without HBP) corresponds to sick male obese patients, have a thick neck, sleepiness, and normal BP, with NSD.
- Phenotype Ph3 (severe without sleepiness) corresponds to sick patients that are obese, have a thick neck, high BP, and no daytime sleepiness, with AR.
- Phenotype Ph4 (moderate hypertensive and sleepy) corresponds to moderately sick patients having a normal NC, high BP, and sleepiness, with NSD.
- Phenotype Ph5 (mild–healthy) corresponds to the healthiest male patients that are not obese, have normal neck, normal BP, and mixed non-significant sleepiness, with CAD and NSD.
- Phenotype Ph6 (moderate not obese) corresponds to moderately sick patients who are not obese and have a thick neck, high BP, and NSD.
- Phenotype Ph7 (mild, thick neck, and sleepy) corresponds to mild OSAS patients that are not obese, have a thick neck, normal BP, and mixed sleepiness, with CAD, NSD, and AR.
- Phenotype Ph8 (mild, thick neck) corresponds to mild OSAS patients that are not obese, have a thick neck, normal BP, and no sleepiness.
- Phenotype Ph1 (severe) corresponds to the sickest obese, thick neck, high BP with sleepiness, significant CAD, CI, and AR female subjects.
- Phenotype Ph2 (severe without HBP) corresponds to sick patients with obesity, normal NC, high BP and sleepiness, and significant CAD.
- Phenotype Ph3 (mild–healthy) has the healthiest female patients with no obesity, normal NC, normal BP and no sleepiness, and without significant comorbidities.
- Phenotype Ph4 (moderate hypertensive) has moderately sick patients with no obesity, normal NC, high BP and mixed sleepiness, and with AR and CAD.
- Phenotype Ph5 (severe without sleepiness) corresponds to sick patients with obesity, thick NC, high BP with no sleepiness, and significant CAD, AR, and CI;
- Phenotype Ph6 (severe with mixed NC) corresponds to sick patients with obesity, mixed NC values, high BP with sleepiness, and without significant comorbidities.
- Phenotype Ph7 (moderate obese and hypertensive) has moderate OSAS patients with obesity, have normal NC values, mixed BP, no sleepiness, and with CAD.
- Phenotype Ph8 (mild hypertensive) has mild OSAS patients with no obesity, normal NC, high BP, no daytime sleepiness, with AR and CAD.
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Peppard, P.E.; Young, T.; Barnet, J.H.; Palta, M.; Hagen, E.W.; Hla, K.M. Increased Prevalence of Sleep-Disordered Breathing in Adults. Am. J. Epidemiol. 2013, 177, 1006–1014. [Google Scholar] [CrossRef] [PubMed]
- Heinzer, R.; Vat, S.; Marques-Vidal, P.; Marti-Soler, H.; Andries, D.; Tobback, N.; Mooser, V.; Preisig, M.; Malhotra, A.; Waeber, G.; et al. Prevalence of sleep-disordered breathing in the general population: The HypnoLaus study. Lancet Respir. Med. 2015, 3, 310–318. [Google Scholar] [CrossRef]
- Bonsignore, M.R.; Giron, M.C.S.; Marrone, O.; Castrogiovanni, A.; Montserrat, J.M. Personalised medicine in sleep respiratory disorders: Focus on obstructive sleep apnoea diagnosis and treatment. Eur. Respir. Rev. 2017, 26, 170069. [Google Scholar] [CrossRef] [PubMed]
- Lévy, P.; Kohler, M.; McNicholas, W.T.; Barbé, F.; McEvoy, R.D.; Somers, V.K.; Lavie, L.; Pépin, J.-L. Obstructive sleep apnoea syndrome. Nat. Rev. Dis. Primers 2014, 1, 15015. [Google Scholar] [CrossRef] [PubMed]
- Floras, J.S. Sleep apnea and cardiovascular risk. J. Cardiol. 2014, 63, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Nieto, F.J.; Young, T.; Lind, B.K.; Shahar, E.; Samet, J.M.; Redline, S.; D’Agostino, R.B.; Newman, A.B.; Lebowitz, M.D.; Pickering, T.G.; et al. Association of Sleep-Disordered Breathing, Sleep Apnea, and Hypertension in a Large Community-Based Study. JAMA 2000, 283, 1829–1836. [Google Scholar] [CrossRef]
- Gami, A.S.; Pressman, G.; Caples, S.M.; Kanagala, R.; Gard, J.J.; Davison, D.E.; Malouf, J.F.; Ammash, N.M.; Friedman, P.A.; Somers, V.K. Association of Atrial Fibrillation and Obstructive Sleep Apnea. Circulation 2004, 110, 364–367. [Google Scholar] [CrossRef]
- Redline, S.; Yenokyan, G.; Gottlieb, D.J.; Shahar, E.; O’connor, G.T.; Resnick, H.E.; Diener-West, M.; Sanders, M.H.; Wolf, P.A.; Geraghty, E.M.; et al. Obstructive sleep apnea–hypopnea and incident stroke: The sleep heart health study. Am. J. Respir. Crit. Care Med. Am. Thorac. Soc. 2010, 182, 269–277. [Google Scholar] [CrossRef]
- Babu, A.R.; Herdegen, J.; Fogelfeld, L.; Shott, S.; Mazzone, T. Type 2 Diabetes, Glycemic Control, and Continuous Positive Airway Pressure in Obstructive Sleep Apnea. Arch. Intern. Med. 2005, 165, 447–452. [Google Scholar] [CrossRef]
- Campos-Rodriguez, F.; Martinez-Garcia, M.A.; Martinez, M.; Duran-Cantolla, J.; De La Peña, M.; Masdeu, M.J.; Gonzalez, M.; Del Campo, F.; Gallego, I.; Marín, J.M.; et al. Association between Obstructive Sleep Apnea and Cancer Incidence in a Large Multicenter Spanish Cohort. Am. J. Respir. Crit. Care Med. 2013, 187, 99–105. [Google Scholar] [CrossRef]
- Marrone, O.; Battaglia, S.; Steiropoulos, P.; Basoglu, O.K.; Kvamme, J.A.; Ryan, S.; Pepin, J.-L.; Verbraecken, J.; Grote, L.; Hedner, J.; et al. Chronic kidney disease in European patients with obstructive sleep apnea: The ESADA cohort study. J. Sleep Res. 2016, 25, 739–745. [Google Scholar] [CrossRef] [PubMed]
- McNicholas, W.T.; Bonsignore, M.R. Sleep apnoea as an independent risk factor for cardiovascular disease: Current evidence, basic mechanisms and research priorities. Eur. Respir. J. 2006, 29, 156–178. [Google Scholar] [CrossRef] [PubMed]
- Saaresranta, T.; Hedner, J.; Bonsignore, M.R.; Riha, R.L.; McNicholas, W.T.; Penzel, T.; Anttalainen, U.; Kvamme, J.A.; Pretl, M.; Sliwinski, P.; et al. Clinical Phenotypes and Comorbidity in European Sleep Apnoea Patients. PLoS ONE 2016, 11, e0163439. [Google Scholar] [CrossRef] [PubMed]
- Lévy, P.; Bonsignore, M.R.; Eckel, J. Sleep, sleep-disordered breathing and metabolic consequences. Eur. Respir. J. 2009, 34, 243–260. [Google Scholar] [CrossRef]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. Rules for scoring respiratory events in sleep: Update of the 2007 AASM manual for the scoring of sleep and associated events: Deliberations of the sleep apnea definitions task force of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2012, 8, 597. [Google Scholar] [CrossRef]
- Marti-Soler, H.; Hirotsu, C.; Marques-Vidal, P.; Vollenweider, P.; Waeber, G.; Preisig, M.; Tafti, M.; Tufik, S.B.; Bittencourt, L.; Haba-Rubio, J.; et al. The NoSAS score for screening of sleep-disordered breathing: A derivation and validation study. Lancet Respir. Med. 2016, 4, 742–748. [Google Scholar] [CrossRef]
- Vavougios, G.D.; Natsios, G.; Pastaka, C.; Zarogiannis, S.G.; Gourgoulianis, K.I. Phenotypes of comorbidity in OSAS patients: Combining categorical principal component analysis with cluster analysis. J. Sleep Res. 2015, 25, 31–38. [Google Scholar] [CrossRef]
- Arnardottir, E.S.; Verbraecken, J.; Gonçalves, M.; Gjerstad, M.D.; Grote, L.; Puertas, F.J.; Mihaicuta, S.; McNicholas, W.T.; Parrino, L. The National Representatives as Study Collaborators Variability in recording and scoring of respiratory events during sleep in Europe: A need for uniform standards. J. Sleep Res. 2015, 25, 144–157. [Google Scholar] [CrossRef]
- McNicholas, W.T.; Bonsignore, M.R.; Lévy, P.; Ryan, S. Mild obstructive sleep apnoea: Clinical relevance and approaches to management. Lancet Respir. Med. 2016, 4, 826–834. [Google Scholar] [CrossRef]
- Eckert, D.J.; White, D.P.; Jordan, A.S.; Malhotra, A.; Wellman, A. Defining Phenotypic Causes of Obstructive Sleep Apnea. Identification of Novel Therapeutic Targets. Am. J. Respir. Crit. Care Med. 2013, 188, 996–1004. [Google Scholar] [CrossRef]
- Edwards, B.A.; Wellman, A.; Sands, S.A.; Owens, R.L.; Eckert, D.J.; White, D.P.; Malhotra, A. Obstructive Sleep Apnea in Older Adults is a Distinctly Different Physiological Phenotype. Sleep 2014, 37, 1227–1236A. [Google Scholar] [CrossRef] [PubMed]
- Ye, L.; Pien, G.W.; Ratcliffe, S.J.; Björnsdottir, E.; Arnardottir, E.S.; Pack, A.I.; Benediktsdottir, B.; Gislason, T. The different clinical faces of obstructive sleep apnoea: A cluster analysis. Eur. Respir. J. 2014, 44, 1600–1607. [Google Scholar] [CrossRef] [PubMed]
- Mihaicuta, S.; Udrescu, M.; Topirceanu, A.; Udrescu, L. Network science meets respiratory medicine for OSAS phenotyping and severity prediction. PeerJ 2017, 5, e3289. [Google Scholar] [CrossRef] [PubMed]
- Topîrceanu, A.; Udrescu, M.; Udrescu, L.; Ardelean, C.; Dan, R.; Reisz, D.; Mihaicuta, S. SAS score: Targeting high-specificity for efficient population-wide monitoring of obstructive sleep apnea. PLoS ONE 2018, 13, e0202042. [Google Scholar] [CrossRef]
- Fischer, J.; Dogas, Z.; Bassetti, C.L.; Berg, S.; Grote, L.; Jennum, P.; Levy, P.; Mihaicuta, S.; Nobili, L.; Riemann, D.; et al. Standard procedures for adults in accredited sleep medicine centres in Europe. J. Sleep Res. 2011, 21, 357–368. [Google Scholar] [CrossRef]
- Chung, F.; Yegneswaran, B.; Liao, P.; Chung, S.A.; Vairavanathan, S.; Islam, S.; Khajehdehi, A.; Shapiro, C.M. Stop questionnairea tool to screen patients for obstructive sleep apnea. Anesthesiology 2008, 108, 812–821. [Google Scholar] [CrossRef]
- Barabási, A.-L. Network medicine—From obesity to the “diseasome”. N. Engl. J. Med. 2007, 357, 404–407. [Google Scholar] [CrossRef]
- Vidal, M.; Cusick, M.E.; Barabási, A.-L. Interactome Networks and Human Disease. Cell 2011, 144, 986–998. [Google Scholar] [CrossRef]
- Yldrm, M.A.; Goh, K.-I.; Cusick, M.E.; Barabási, A.-L.; Vidal, M. Drug—Target network. Nat. Biotechnol. 2007, 25, 1119–1126. [Google Scholar] [CrossRef]
- Udrescu, L.; Sbârcea, L.; Topîrceanu, A.; Iovanovici, A.; Kurunczi, L.; Bogdan, P.; Udrescu, M. Clustering drug-drug interaction networks with energy model layouts: Community analysis and drug repurposing. Sci. Rep. 2016, 6, 32745. [Google Scholar] [CrossRef]
- Faner, R.; Cruz, T.; López-Giraldo, A.; Agusti, A. Network medicine, multimorbidity and the lung in the elderly. Eur. Respir. J. 2014, 44, 775–788. [Google Scholar] [CrossRef] [PubMed]
- Divo, M.J.; Casanova, C.; Marin, J.M.; Pinto-Plata, V.M.; de-Torres, J.P.; Zulueta, J.J.; Cabrera, C.; Zagaceta, J.; Sanchez-Salcedo, P.; Berto, J.; et al. Chronic obstructive pulmonary disease comorbidities network. Eur. Respir. J. 2015, 46, 640–650. [Google Scholar] [CrossRef] [PubMed]
- Blondel, V.D.; Guillaume, J.-L.; Lambiotte, R.; Lefebvre, E. Fast unfolding of communities in large networks. J. Stat. Mech. Theory Exp. 2008, 2008, P10008. [Google Scholar] [CrossRef]
- Jacomy, M.; Venturini, T.; Heymann, S.; Bastian, M. ForceAtlas2, a Continuous Graph Layout Algorithm for Handy Network Visualization Designed for the Gephi Software. PLoS ONE 2014, 9, e98679. [Google Scholar] [CrossRef] [PubMed]
- Noack, A. Modularity clustering is force-directed layout. Phys. Rev. E 2009, 79, 26102. [Google Scholar] [CrossRef]
- Joosten, S.; Hamza, K.; Sands, S.; Turton, A.; Berger, P.; Hamilton, G.S. Phenotypes of patients with mild to moderate obstructive sleep apnoea as confirmed by cluster analysis. Respirology 2011, 17, 99–107. [Google Scholar] [CrossRef]
- Cairns, A.; Poulos, G.; Bogan, R. Sex differences in sleep apnea predictors and outcomes from home sleep apnea testing. Nat. Sci. Sleep 2016, 8, 197–205. [Google Scholar] [CrossRef]
- Gabbay, I.E.; Lavie, P. Age- and gender-related characteristics of obstructive sleep apnea. Sleep Breath. 2012, 16, 453–460. [Google Scholar] [CrossRef]
- Vagiakis, E.; Kapsimalis, F.; Lagogianni, I.; Perraki, H.; Minaritzoglou, A.; Alexandropoulou, K.; Roussos, C.; Kryger, M. Gender differences on polysomnographic findings in Greek subjects with obstructive sleep apnea syndrome. Sleep Med. 2006, 7, 424–430. [Google Scholar] [CrossRef]
- Ibáñez, V.; Silva, J.; Cauli, O. A survey on sleep assessment methods. PeerJ 2018, 6, e4849. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Males (N = 1948) Mean/n 1 | Females (N = 848) Mean/n 1 |
|---|---|---|
| Age (years) | 51.29 ± 13.22 | 54.71 ± 12.84 |
| Body-mass index (kg/m2) | 33.59 ± 6.74 | 34.09 ± 7.78 |
| Obesity (BMI > 30) | 1308 (67.14%) | 575 (67.80%) |
| Neck circumference (cm) | 44.83 ± 4.46 | 39.45 ± 4.36 |
| Thick neck (NC > 43/40) | 1458 (74.84%) | 367 (43.27%) |
| Hypertension 2 | 1262 (64.78%) | 624 (73.58%) |
| Systolic BP | 176.54 ± 31.28 | 185.36 ± 32.37 |
| Diastolic BP | 105.50 ± 19.50 | 107.07 ± 20.36 |
| Epworth sleepiness score | 11.38 ± 5.40 | 10.74 ± 5.16 |
| Sleepiness (ESS ≥ 11) | 1316 (67.55%) | 555 (65.44%) |
| Mean AHI | 46.52 ± 26.36 | 36.55 ± 25.53 |
| Obstructive apnea | 25.96 ± 24.88 | 19.52 ± 20.43 |
| Central apnea | 3.51 ± 5.82 | 2.02 ± 3.95 |
| Mixed apnea | 4.09 ± 7.04 | 1.97 ± 4.42 |
| Hypopnea | 13.35 ± 9.88 | 12.67 ± 9.63 |
| Moderate OSAS (30 > AHI ≥ 15) | 370 (18.99%) | 237 (27.95%) |
| Severe OSAS (AHI ≥ 30) | 1369 (70.27%) | 438 (51.65%) |
| STOP-Bang score ≥ 3 | 1863 (95.63%) | 738 (87.02%) |
| NoSAS score ≥ 5 | 1757 (90.19%) | 584 (68.86%) |
| SASscore ≥ 3.7 | 1023 (52.51%) | 463 (54.59%) |
| Parameter | Ph1 | Ph2 | Ph3 | Ph4 | Ph5 | Ph6 | Ph7 | Ph8 |
|---|---|---|---|---|---|---|---|---|
| Size | 648 (33%) | 249 (13%) | 231 (12%) | 202 (10%) | 194 (10%) | 186 (10%) | 184 (9%) | 34 (2%) |
| Age | 54.8 ± 10.2 | 45.6 ± 11.2 | 53.3 ± 11.1 | 43.2 ± 15.8 | 56.7 ± 12.1 | 44.3 ± 13.6 | 56.8 ± 11.6 | 37.3 ± 21.8 |
| BMI | 37.9 ± 5.9 | 36.1 ± 5.2 | 36.5 ± 4.9 | 29.4 ± 5.2 | 29.5 ± 5.5 | 26.9 ± 2.9 | 28 ± 1.6 | 28 ± 9.8 |
| NC | 47.4 ± 3.6 | 45.8 ± 3.9 | 46.4 ± 3.6 | 42 ± 4.3 | 39.5 ± 1.8 | 41 ± 3.8 | 43.7 ± 1.7 | 36.6 ± 4.6 |
| SBP | 183 ± 28.7 | 137.3 ± 19.2 | 185 ± 30.5 | 131.2 ± 13.5 | 174.3 ± 28.7 | 135.3 ± 16.3 | 176.4 ± 25.4 | 120 ± 0.0 |
| DBP | 109.6 ± 18.4 | 85.1 ± 19.5 | 109.1 ± 19 | 79.5 ± 10.6 | 104.9 ± 17.5 | 83.3 ± 11.8 | 104.5 ± 16 | 70 ± 0.0 |
| ESS | 14 ± 4.7 | 13.2 ± 4.8 | 8 ± 4.7 | 6.5 ± 3.9 | 11.1 ± 5.5 | 10.8 ± 4.7 | 10.3 ± 4.9 | 7.3 ± 2.2 |
| AHI | 56.9 ± 0 | 56.2 ± 29.8 | 43.8 ± 23.6 | 31.4 ± 21.5 | 36.1 ± 21.3 | 37 ± 22.4 | 39.6 ± 19.8 | 39.6 ± 23.3 |
| Moderate OSAS | 74 (11.42%) | 37 (14.86%) | 44 (19.05%) | 53 (26.24%) | 55 (28.35%) | 49 (26.34%) | 46 (25.0%) | 8 (23.53%) |
| Severe OSAS | 546 (84.26%) | 196 (78.71%) | 163 (70.56%) | 96 (47.52%) | 107 (55.15%) | 107 (57.53%) | 123 (66.85%) | 19 (55.88%) |
| SB | 648 (100%) | 246 (99%) | 231 (100%) | 164 (81%) | 192 (99%) | 179 (96%) | 184 (100%) | 4 (12%) |
| NS | 648 (100%) | 245 (98%) | 227 (98%) | 151 (75%) | 148 (76%) | 132 (71%) | 182 (99%) | 7 (21%) |
| SS | 593 (92%) | 65 (26%) | 148 (64%) | 1 (1%) | 87 (45%) | 6 (3%) | 119 (65%) | 0 (0%) |
| Parameter | Ph1 | Ph2 | Ph3 | Ph4 | Ph5 | Ph6 | Ph7 | Ph8 |
|---|---|---|---|---|---|---|---|---|
| Size | 217 (26%) | 150 (18%) | 113 (13%) | 85 (10%) | 76 (9%) | 70 (8%) | 64 (8%) | 58 (7%) |
| Age | 56.6 ± 9.9 | 56.9 ± 10.3 | 44.6 ± 18.7 | 58.6 ± 10.1 | 55.4 ± 9.5 | 50.4 ± 10.7 | 54.3 ± 13.2 | 61.9 ± 10.4 |
| BMI | 40.7 ± 6.3 | 35.3 ± 4.8 | 24.6 ± 4.2 | 27.6 ± 2.3 | 37.8 ± 6.1 | 35.6 ± 6.2 | 35 ± 5.9 | 26.9 ± 2.5 |
| NC | 43.5 ± 3 | 37.5 ± 1.7 | 35.1 ± 3.3 | 37.5 ± 3.2 | 42.6 ± 2.5 | 40.6 ± 4.5 | 36.8 ± 2.4 | 37.5 ± 3.8 |
| SBP | 189.8 ± 30 | 189.1 ± 29.5 | 123 ± 14.4 | 188.3 ± 27.1 | 192.8 ± 35.2 | 130 ± 12.5 | 184 ± 30.7 | 183.5 ± 25.4 |
| DBP | 110.3 ± 18.7 | 110.2 ± 19.8 | 72.4 ± 10.4 | 106.8 ± 17.5 | 111.7 ± 21.8 | 76.5 ± 7.8 | 105.5 ± 22.4 | 102.9 ± 15 |
| ESS | 13.3 ± 4.3 | 12 ± 5 | 8.6 ± 5.1 | 11 ± 4.6 | 8.3 ± 4.9 | 12.5 ± 4.7 | 6.5 ± 3.3 | 6.6 ± 4.2 |
| AHI | 48.2 ± 28.6 | 36.6 ± 23.3 | 24.2 ± 25.3 | 31.1 ± 16.8 | 35.6 ± 23.8 | 40.7 ± 25.1 | 30.8 ± 20.2 | 27.2 ± 18.9 |
| Moderate OSAS | 49 (22.58%) | 47 (31.33%) | 32 (28.32%) | 22 (25.88%) | 22 (28.95%) | 15 (21.43%) | 23 (35.94%) | 25 (43.10%) |
| Severe OSAS | 147 (67.74%) | 78 (52.0%) | 31 (27.43%) | 45 (52.94%) | 39 (51.32%) | 44 (62.86%) | 26 (40.63%) | 19 (32.76%) |
| SB | 217 (100%) | 150 (100%) | 44 (39%) | 81 (95%) | 73 (96%) | 63 (90%) | 52 (81%) | 50 (86%) |
| NS | 215 (99%) | 96 (64%) | 22 (19%) | 51 (60%) | 76 (100%) | 49 (70%) | 32 (50%) | 37 (64%) |
| SS | 208 (96%) | 116 (77%) | 0 (0%) | 48 (56%) | 47 (62%) | 14 (20%) | 20 (31%) | 9 (16%) |
| Parameter | Ph1 | Ph2 | Ph3 | Ph4 | Ph5 | Ph6 | Ph7 | Ph8 |
|---|---|---|---|---|---|---|---|---|
| COPD | 146 (23%) | 39 (16%) | 52 (23%) | 16 (8%) | 29 (15%) | 16 (9%) | 24 (13%) | 0 (0%) |
| DM | 81 (13%) | 17 (7%) | 24 (10%) | 3 (1%) | 18 (9%) | 2 (1%) | 9 (5%) | 0 (0%) |
| CAD | 269 (42%) | 29 (12%) | 85 (37%) | 21 (10%) | 68 (35%) | 10 (5%) | 70 (38%) | 0 (0%) |
| CHF | 246 (38%) | 31 (12%) | 76 (33%) | 9 (4%) | 55 (28%) | 11 (6%) | 42 (23%) | 0 (0%) |
| AR | 180 (28%) | 38 (15%) | 58 (25%) | 17 (8%) | 39 (20%) | 12 (6%) | 49 (27%) | 0 (0%) |
| Stroke | 35 (5%) | 4 (2%) | 18 (8%) | 3 (1%) | 9 (5%) | 0(0%) | 8 (4%) | 0 (0%) |
| NSD | 192 (30%) | 76 (31%) | 39 (17%) | 59 (29%) | 53 (27%) | 66 (35%) | 56 (30%) | 1 (3%) |
| PP | 75 (12%) | 32 (13%) | 25 (11%) | 23 (11%) | 18 (9%) | 22 (12%) | 26 (14%) | 1 (3%) |
| UH | 124 (19%) | 41 (16%) | 42 (18%) | 25 (12%) | 27 (14%) | 27 (15%) | 31 (17%) | 0 (0%) |
| AH | 90 (14%) | 43 (17%) | 36 (16%) | 31 (15%) | 25 (13%) | 25 (13%) | 22 (12%) | 0 (0%) |
| Ph1 | Ph2 | Ph3 | Ph4 | Ph5 | Ph6 | Ph7 | Ph8 | |
|---|---|---|---|---|---|---|---|---|
| COPD | 24 (11%) | 14 (9%) | 2 (2%) | 5 (6%) | 8 (11%) | 5 (7%) | 2 (3%) | 4 (7%) |
| DM | 31 (14%) | 9 (6%) | 2 (2%) | 6 (7%) | 10 (13%) | 4 (6%) | 4 (6%) | 3 (5%) |
| CAD | 101 (47%) | 73 (49%) | 11 (10%) | 26 (31%) | 31 (41%) | 12 (17%) | 24 (38%) | 19 (33%) |
| CHF | 96 (44%) | 57 (38%) | 2 (2%) | 19 (22%) | 23 (30%) | 7 (10%) | 14 (22%) | 10 (17%) |
| AR | 82 (38%) | 45 (30%) | 10 (9%) | 31 (36%) | 21 (28%) | 11 (16%) | 14 (22%) | 22 (38%) |
| Stroke | 14 (6%) | 8 (5%) | 0 (0%) | 6 (7%) | 7 (9%) | 0 (0%) | 2 (3%) | 2 (3%) |
| NSD | 40 (18%) | 22 (15%) | 23 (20%) | 16 (19%) | 5 (7%) | 13 (19%) | 13 (20%) | 14 (24%) |
| PP | 20 (9%) | 17 (11%) | 17 (15%) | 5 (6%) | 5 (7%) | 11 (16%) | 8 (13%) | 6 (10%) |
| UH | 28 (13%) | 23 (15%) | 17 (15%) | 16 (19%) | 10 (13%) | 13 (19%) | 8 (13%) | 8 (14%) |
| AH | 36 (17%) | 22 (15%) | 13 (12%) | 9 (11%) | 15 (20%) | 14 (20%) | 8 (13%) | 10 (17%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Topîrceanu, A.; Udrescu, L.; Udrescu, M.; Mihaicuta, S. Gender Phenotyping of Patients with Obstructive Sleep Apnea Syndrome Using a Network Science Approach. J. Clin. Med. 2020, 9, 4025. https://doi.org/10.3390/jcm9124025
Topîrceanu A, Udrescu L, Udrescu M, Mihaicuta S. Gender Phenotyping of Patients with Obstructive Sleep Apnea Syndrome Using a Network Science Approach. Journal of Clinical Medicine. 2020; 9(12):4025. https://doi.org/10.3390/jcm9124025
Chicago/Turabian StyleTopîrceanu, Alexandru, Lucreția Udrescu, Mihai Udrescu, and Stefan Mihaicuta. 2020. "Gender Phenotyping of Patients with Obstructive Sleep Apnea Syndrome Using a Network Science Approach" Journal of Clinical Medicine 9, no. 12: 4025. https://doi.org/10.3390/jcm9124025
APA StyleTopîrceanu, A., Udrescu, L., Udrescu, M., & Mihaicuta, S. (2020). Gender Phenotyping of Patients with Obstructive Sleep Apnea Syndrome Using a Network Science Approach. Journal of Clinical Medicine, 9(12), 4025. https://doi.org/10.3390/jcm9124025