Conservative Treatment for Acute Ankle Sprain: A Systematic Review

 , , , ,
, , , , 
Abstract
1. Introduction
2. Methods
2.1. Design
2.2. Search Strategy
2.3. Eligibility Criteria
- -
- In every case, the study population was diagnosed with acute ankle sprain and given conservative treatment as the first option.
- -
- All studies included in the review were randomised controlled clinical trials (RCTs) in which one or more types of conservative treatment were applied in response to an acute ankle sprain, with a maximum of 7 days after initial injury.
- -
- All the studies included evaluated pain, functionality and/or disability caused by an ankle sprain, using one or more measurement instruments.
- -
- The language of publication was Spanish or English.
- -
- The study population was diagnosed with chronic or recurrent ankle sprain.
- -
- Those in which both conservative and surgical treatments were applied.
- -
- Those not consisting of an RCT (such as pilot studies, research protocols or quasi-experimental studies).
- -
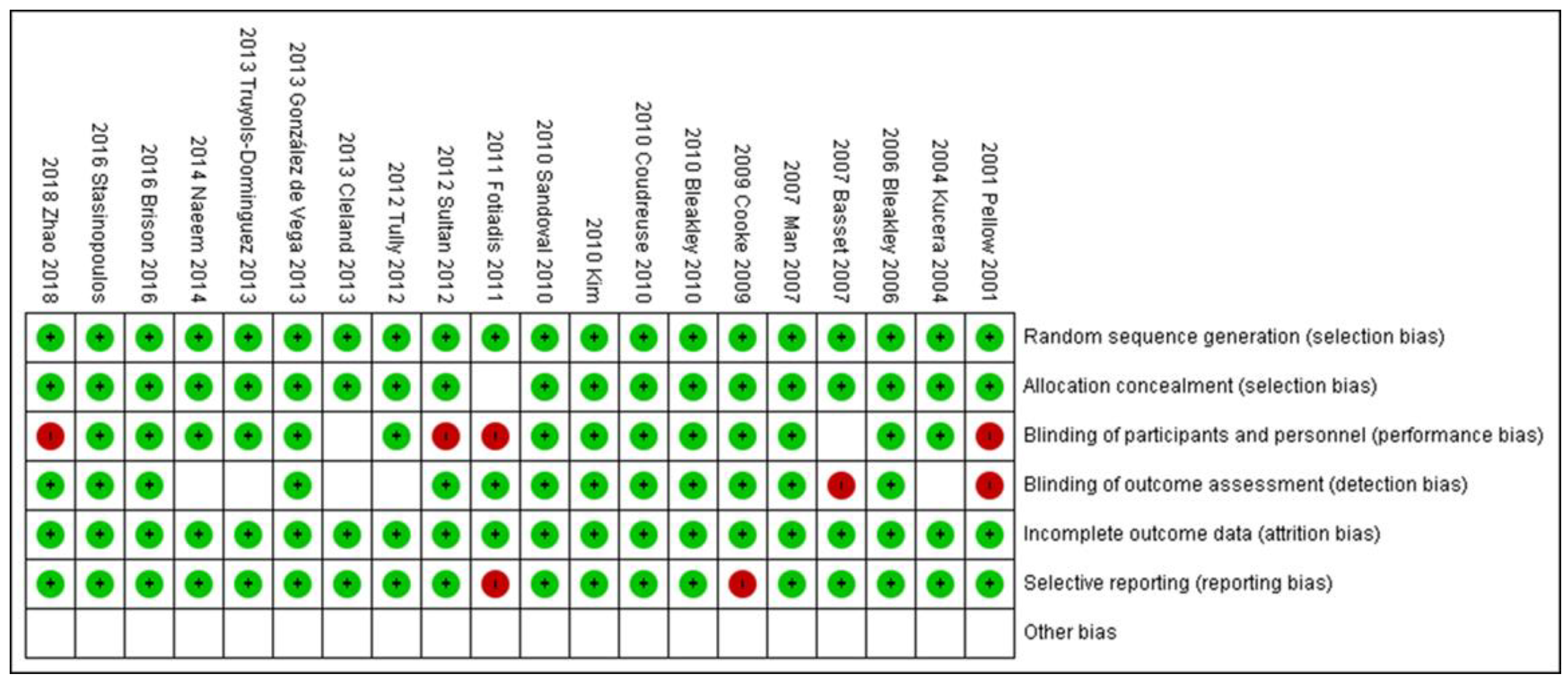
- Those in which the assessment of risk of bias, using the Cochrane risk of bias tool included in RevMan 5 was high risk (it was not consider random sequence generation, allocation concealment and blinding of participants and personnel).
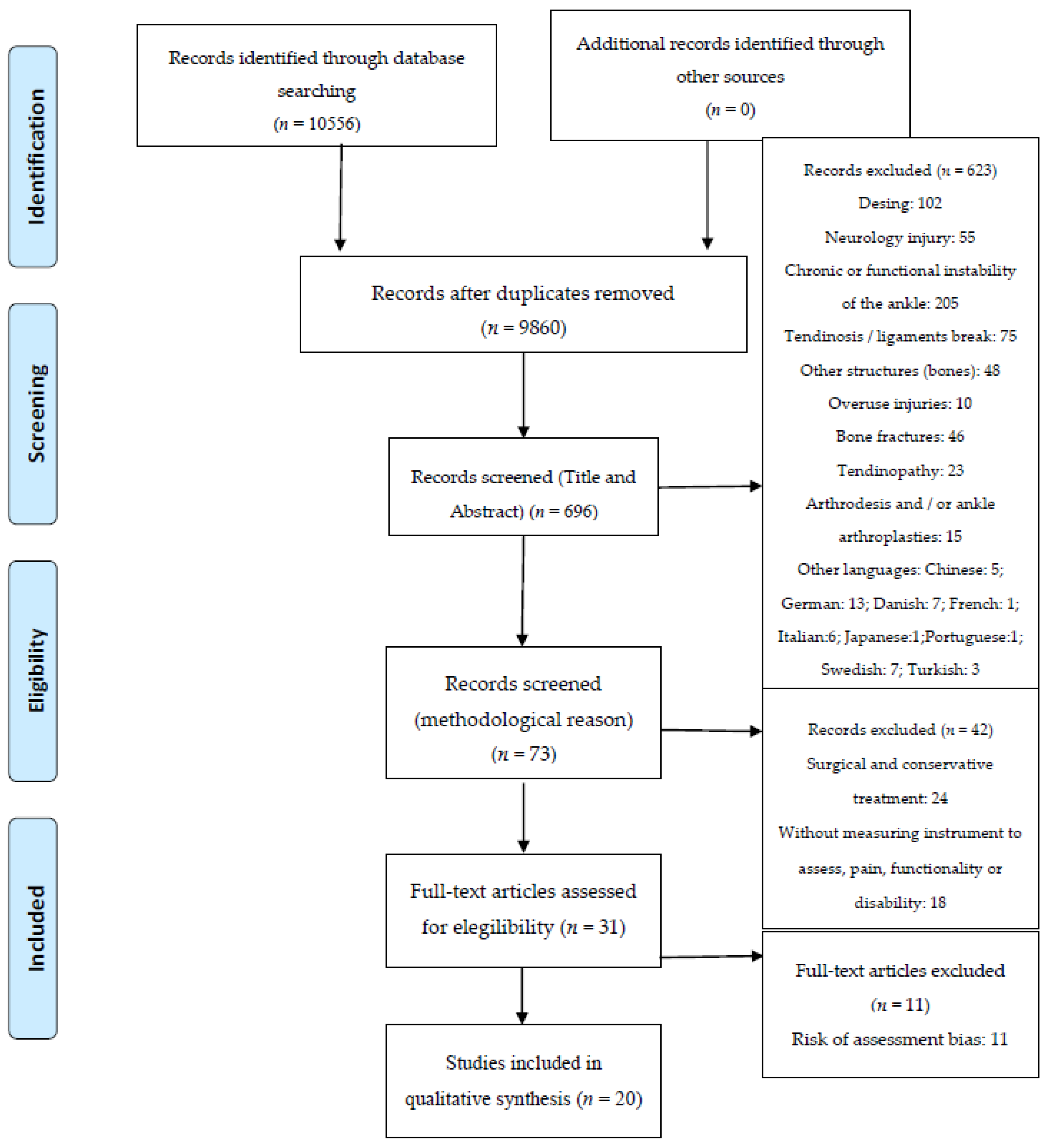
2.4. Study Selection
2.5. Data Extraction
2.6. Quality Assessment
3. Results
3.1. Study Characteristics
3.2. Risk of Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| 1 | Ankle |
| 2 | Talocrural |
| 3 | Talo-crural |
| 4 | Talocalcaneal |
| 5 | Talo-calcaneal |
| 6 | Talofibular |
| 7 | Talo-fibular |
| 8 | Ligament |
| 9 | Lateral Ligament ankle |
| 10 | Medial Ligament ankle |
| 11 | 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10 |
| 12 | Sprain |
| 13 | Strain |
| 14 | Ankle injury |
| 15 | Ankle sprain |
| 16 | Inversion sprain |
| 17 | Eversion sprain |
| 18 | 12 OR 13 OR 14 OR 15 OR 16 OR 17 |
| 19 | 11 AND 18 |
| 20 | Conservative treatment |
| 21 | Conservative management |
| 22 | Non-surgical treatment |
| 23 | CAST |
| 24 | Rehabilitation program |
| 25 | Myofascial |
| 26 | Conservative program |
| 27 | Manual Therapy |
| 28 | Physiotherapeutic intervention |
| 29 | Bandage |
| 30 | Plaster |
| 31 | Exercise programme |
| 32 | Home exercise |
| 33 | RICE |
| 34 | Taping |
| 35 | TENSE |
| 36 | Ultrasound |
| 37 | 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26 OR 27 OR 28 OR 29 OR 30 OR 31 OR 32 OR 33 OR 34 OR 35 OR 36 |
| 38 | 19 AND 37 |
| 1 | Ankle Sprains |
| 2 | Inversion Sprain |
| 3 | Eversion Sprain |
| 4 | Ankle Injury |
| 5 | 1 OR 2 OR 3 OR 4 |
| 6 | Conservative treatment |
| 7 | Conservative management |
| 8 | Rehabilitation programs |
| 9 | Bandage |
| 10 | Physiotherapeutic |
| 11 | 6 OR 7 OR 8 OR 9 OR 10 |
| 12 | 5 AND 11 |
| 1 | TITLE-ABS-KEY (Ankle Sprain) |
| 2 | TITLE-ABS-KEY (Inversion Sprain) |
| 3 | TITLE-ABS-KEY (Eversion Sprain) |
| 4 | TITLE-ABS-KEY (Ankle Injury) |
| 5 | 1 OR 2 OR 3 OR 4 |
| 6 | TITLE-ABS-KEY (Conservative treatment) |
| 7 | TITLE-ABS-KEY (Conservative management) |
| 8 | TITLE-ABS-KEY (TENSE) |
| 9 | TITLE-ABS-KEY (Bandage) |
| 10 | TITLE-ABS-KEY (Rehabilitation program) |
| 11 | TITLE-ABS-KEY (Physiotherapeutic) |
| 12 | 6 OR 7 OR 8 OR 9 OR 10 OR 11 |
| 13 | 5 AND 12 |
| 1 | Ankle Sprains |
| 2 | Inversion Sprain |
| 3 | Eversion Sprain |
| 4 | Ankle injury |
| 5 | 1 OR 2 OR 3 OR 4 |
| 6 | Conservative treatment |
| 7 | Conservative management |
| 8 | Rehabilitation program |
| 9 | Physiotherapeutic |
| 10 | 6 OR 7 OR 8 OR 9 OR 10 |
| 11 | 5 AND 10 |
| 1 | Ankle Sprains |
| 2 | Inversion Ankle sprain |
| 3 | Eversion Ankle sprain |
| 4 | 1 OR 2 OR 3 |
| 5 | Conservative treatment |
| 6 | Conservative management |
| 7 | Rehabilitation program |
| 8 | Physiotherapeutic |
| 9 | 5 OR 6 OR 7 OR 8 |
| 10 | 4 AND 9 |
| 1 | Ankle Sprains |
References
- Vuurberg, G.; Hoorntje, A.; Wink, L.M.; Van Der Doelen, B.F.W.; Van Den Bekerom, M.P.; Dekker, R.; Van Dijk, C.N.; Krips, R.; Loogman, M.C.M.; Ridderikhof, M.L.; et al. Diagnosis, treatment and prevention of ankle sprains: Update of an evidence-based clinical guideline. Br. J. Sports Med. 2018, 52, 956. [Google Scholar] [CrossRef]
- Cooke, M.W.; Marsh, J.L.; Clark, M.; Nakash, R.; Jarvis, R.M.; Hutton, J.L.; Szczepura, A.; Wilson, S.; Lamb, S.E. Treatment of severe ankle sprain: A pragmatic randomised controlled trial comparing the clinical effectiveness and cost-effectiveness of three types of mechanical ankle support with tubular bandage. The CAST trial. Health Technol. Assess. 2009, 13. [Google Scholar] [CrossRef] [PubMed]
- Hertel, J. Functional anatomy, pathomechanics, and pathophysiology of lateral ankle instability. J. Athl. Train. 2002, 37, 364–375. [Google Scholar] [PubMed]
- Herzog, M.M.; Kerr, Z.Y.; Marshall, S.W.; Wikstrom, E.A. Epidemiology of ankle sprains and chronic ankle instability. J. Athl. Train. 2019, 54, 603–610. [Google Scholar] [CrossRef] [PubMed]
- Purevsuren, T.; Kim, K.; Batbaatar, M.; Lee, S.K.; Kim, Y.H. Influence of ankle joint plantarflexion and dorsiflexion on lateral ankle sprain: A computational study. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2018, 232, 458–467. [Google Scholar] [CrossRef]
- van Rijn, R.M.; van Os, A.G.; Bernsen, R.M.D.; Luijsterburg, P.A.; Koes, B.W.; Bierma-Zeinstra, S.M.A. What Is the Clinical Course of Acute Ankle Sprains? A Systematic Literature Review. Am. J. Med. 2008, 121, 324–331. [Google Scholar] [CrossRef]
- Kamper, S.J.; Grootjans, S.J.M. Surgical versus conservative treatment for acute ankle sprains. Br. J. Sports Med. 2012, 46, 77–78. [Google Scholar] [CrossRef]
- Lamb, S.E.; Nakash, R.A.; Withers, E.J.; Clark, M.; Marsh, J.L.; Wilson, S.; Hutton, J.L.; Szczepura, A.; Dale, J.R.; Cooke, M.W. Clinical and cost effectiveness of mechanical support for severe ankle sprains: Design of a randomised controlled trial in the emergency department [ISRCTN 37807450]. BMC Musculoskelet. Disord. 2005, 26, 2221–2228. [Google Scholar] [CrossRef]
- Brison, R.J.; Day, A.G.; Pelland, L.; Pickett, W.; Johnson, A.P.; Aiken, A.; Pichora, D.R.; Brouwer, B. Effect of early supervised physiotherapy on recovery from acute ankle sprain: Randomised controlled trial. BMJ 2016, 355, i5650. [Google Scholar] [CrossRef]
- González De Vega, C.; Speed, C.; Wolfarth, B.; González, J. Traumeel vs. diclofenac for reducing pain and improving ankle mobility after acute ankle sprain: A multicentre, randomised, blinded, controlled and non-inferiority trial. Int. J. Clin. Pract. 2013, 67, 979–989. [Google Scholar] [CrossRef]
- Bassett, S.F.; Prapavessis, H. Home-Based Physical Therapy Intervention With Adherence-Enhancing Strategies Versus Clinic-Based Management for Patients With Ankle Sprains. Phys. Ther. 2007, 87, 1132–1143. [Google Scholar] [CrossRef] [PubMed]
- Wainwright, T.W.; Burgess, L.C.; Middleton, R.G. Does Neuromuscular Electrical Stimulation Improve Recovery Following Acute Ankle Sprain? A Pilot Randomised Controlled Trial. Clin. Med. Insights Arthritis Musculoskelet. Disord. 2019, 12. [Google Scholar] [CrossRef] [PubMed]
- Kemler, E.; Van De Port, I.; Backx, F.; Van Dijk, C.N. A systematic review on the treatment of acute ankle sprain: Brace versus other functional treatment types. Sports Med. 2011, 41, 185–197. [Google Scholar] [CrossRef]
- Kerkhoffs, G.M.M.J.; Rowe, B.H.; Assendelft, W.J.J.; Kelly, K.D.; Struijs, P.A.A.; Van Dijk, C.N. Immobilisation for acute ankle sprain. A systematic review. Arch. Orthop. Trauma Surg. 2001, 121, 462–471. [Google Scholar] [CrossRef]
- Al Bimani, S.A.; Gates, L.S.; Warner, M.; Bowen, C. Factors influencing return to play following conservatively treated ankle sprain: A systematic review. Phys. Sportsmed. 2019, 47, 31–46. [Google Scholar] [CrossRef] [PubMed]
- Ivins, D. Acute Ankle Sprain: An Update. Am. Fam. Physician 2006, 74, 1714–1720. [Google Scholar]
- Delahunt, E.; Bleakley, C.M.; Bossard, D.S.; Caulfield, B.M.; Docherty, C.L.; Doherty, C.; Fourchet, F.; Fong, D.T.; Hertel, J.; Hiller, C.E.; et al. Clinical assessment of acute lateral ankle sprain injuries (ROAST): 2019 consensus statement and recommendations of the International Ankle Consortium. Br. J. Sports Med. 2018, 52, 1304–1310. [Google Scholar] [CrossRef]
- Doherty, C.; Bleakley, C.; Delahunt, E.; Holden, S. Treatment and prevention of acute and recurrent ankle sprain: An overview of systematic reviews with meta-analysis. Br. J. Sports Med. 2017, 51, 113–125. [Google Scholar] [CrossRef]
- Petersen, W.; Rembitzki, I.V.; Koppenburg, A.G.; Ellermann, A.; Liebau, C.; Brüggemann, G.P.; Best, R. Treatment of acute ankle ligament injuries: A systematic review. Arch. Orthop. Trauma Surg. 2013, 133, 1129–1141. [Google Scholar] [CrossRef]
- Han, L.; Zhang, C.; Liu, B.; Ting, H.; Jihong, W. A Meta-analysis of treatment methods for acute ankle sprain. Pak. J. Med. Sci. 2012, 28, 895–899. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Santesso, N.; Helfand, M.; Vist, G.E.; Kunz, R.; Brozek, J.; Norris, S.; Meerpohl, J.J.; Djulbegovic, B.; et al. The Cochrane Collaboration. Review Manager (RevMan). Pain 2009, 9, 205–213. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. PRISMA 2009 Flow Diagram. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Pellow, J.E.; Brantingham, J.W. The efficacy of adjusting the ankle in the treatment of subacute and chronic grade I and grade II ankle inversion sprains. J. Manip. Physiol. Ther. 2001, 24, 17–24. [Google Scholar] [CrossRef]
- Kučera, M.; Barna, M.; Horáček, O.; Kováriková, J.; Kučera, A. Efficacy and safety of topically applied Symphytum herb extract cream in the treatment of ankle distortion: Results of a randomized controlled clinical double blind study. Wien. Med. Wochenschr. 2004, 154, 498–507. [Google Scholar] [CrossRef]
- Truyols-Domínguez, S.; Salom-Moreno, J.; Abian-Vicen, J.; Cleland, J.A.; Fernández-De-Las-Peñas, C. Efficacy of thrust and nonthrust manipulation and exercise with or without the addition of myofascial therapy for the management of acute inversion ankle sprain: A randomized clinical trial. J. Orthop. Sports Phys. Ther. 2013, 43, 300–309. [Google Scholar] [CrossRef]
- Bleakley, C.M.; McDonough, S.M.; MacAuley, D.C. Cryotherapy for acute ankle sprains: A randomised controlled study of two different icing protocols. Br. J. Sports Med. 2006, 40, 700–705. [Google Scholar] [CrossRef]
- Bleakley, C.M.; O’Connor, S.R.; Tully, M.A.; Rocke, L.G.; MacAuley, D.C.; Bradbury, I.; Keegan, S.; McDonough, S.M. Effect of accelerated rehabilitation on function after ankle sprain: Randomised controlled trial. BMJ 2010, 340, 1122. [Google Scholar] [CrossRef]
- Cleland, J.A.; Mintken, P.; McDevitt, A.; Bieniek, M.; Carpenter, K.; Kulp, K.; Whitman, J.M. Manual physical therapy and exercise versus supervised home exercise in the management of patients with inversion ankle sprain: A multicenter randomized clinical trial. J. Orthop. Sports Phys. Ther. 2013, 43, 443–455. [Google Scholar] [CrossRef]
- Coudreuse, J.M.; De Vathaire, F. Effect of a plaster containing DHEP and heparin in acute ankle sprains with oedema: A randomized, double-blind, placebo-controlled, clinical study. Curr. Med. Res. Opin. 2010, 26, 2221–2228. [Google Scholar] [CrossRef]
- Fotiadis, E.; Kenanidis, E.; Samoladas, E.; Chytas, A.; Lyrtzis, C.; Koimtzis, M.; Chalidis, B. Are venotonic drugs effective for decreasing acute posttraumatic oedema following ankle sprain? A prospective randomized clinical trial. Arch. Orthop. Trauma Surg. 2011, 131, 389–392. [Google Scholar] [CrossRef] [PubMed]
- Cheung, S.M.; Chen, C.J.; Hsin, Y.J.; Tsai, Y.T.; Leong, C.P. Effect of neuromuscular electrical stimulation in a patient with Sjogren’s syndrome with dysphagia: A real time videofluoroscopic swallowing study. Chang Gung Med. J. 2010, 33, 338–345. [Google Scholar] [PubMed]
- Kim, M.K.; Shin, Y.J. Immediate effects of ankle balance taping with kinesiology tape for amateur soccer players with lateral ankle sprain: A randomized cross-over design. Med. Sci. Monit. 2017, 23, 5534–5541. [Google Scholar] [CrossRef] [PubMed]
- Naeem, M.; Rahimnajjad, M.K.; Rahimnajjad, N.A.; Idrees, Z.; Shah, G.A.; Abbas, G. Assessment of functional treatment versus plaster of Paris in the treatment of grade 1 and 2 lateral ankle sprains. J. Orthop. Traumatol. 2015, 16, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Sandoval, M.C.; Ramirez, C.; Camargo, D.M.; Salvini, T.F. Effect of high-voltage pulsed current plus conventional treatment on acute ankle sprain. Rev. Bras. Fisioter. 2010, 14, 193–199. [Google Scholar] [CrossRef]
- Stasinopoulos, D.; Papadopoulos, C.; Lamnisos, D.; Stasinopoulos, I. The use of Bioptron light (polarized, polychromatic, non-coherent) therapy for the treatment of acute ankle sprains. Disabil. Rehabil. 2017, 39, 450–457. [Google Scholar] [CrossRef]
- Sultan, M.J.; McKeown, A.; McLaughlin, I.; Kurdy, N.; McCollum, C.N. Elastic stockings or Tubigrip for ankle sprain: A randomised clinical trial. Injury 2012, 43, 1079–1083. [Google Scholar] [CrossRef]
- Tully, M.A.; Bleakley, C.M.; O’Connor, S.R.; McDonough, S.M. Functional management of ankle sprains: What volume and intensity of walking is undertaken in the first week postinjury. Br. J. Sports Med. 2012, 46, 877–882. [Google Scholar] [CrossRef]
- Zhao, M.; Gao, W.; Zhang, L.; Huang, W.; Zheng, S.; Wang, G.; Hong, B.Y.; Tang, B. Acupressure Therapy for Acute Ankle Sprains: A Randomized Clinical Trial. PM&R 2018, 10, 36–44. [Google Scholar] [CrossRef]
- Kosik, K.B.; McCann, R.S.; Terada, M.; Gribble, P.A. Therapeutic interventions for improving self-reported function in patients with chronic ankle instability: A systematic review. Br. J. Sports Med. 2017, 51, 105–112. [Google Scholar] [CrossRef]
- Van Ochten, J.M.; Van Middelkoop, M.; Meuffels, D.; Bierma-Zeinstra, S.M.A. Chronic complaints after ankle sprains: A systematic review on effectiveness of treatments. J. Orthop. Sports Phys. Ther. 2014, 44, 862–871. [Google Scholar] [CrossRef] [PubMed]
- Feger, M.A.; Goetschius, J.; Love, H.; Saliba, S.A.; Hertel, J. Electrical stimulation as a treatment intervention to improve function, edema or pain following acute lateral ankle sprains: A systematic review. Phys. Ther. Sport 2015, 16, 361–369. [Google Scholar] [CrossRef] [PubMed]



| Author Year Country | Patients (n) | Age (years) | Sex | Type of RCT Design | Type of Sprain | Type of Treatment | Follow Up | Outcome | |
|---|---|---|---|---|---|---|---|---|---|
| Female | Male | ||||||||
| Pellow JE et al., 2001 [24]. South Africa | 30 | 15–50 Total mean age: 24.9 Group 1: 23.7 Group 2: 26.1 | 11 Group 1: 9 Group 2: 2 | 19 Group 1: 6 Group 2: 13 | Single-blind, comparative, controlled study | Subacute ankle inversion sprains (<48 h after initial injury) | Mortise separation adjustment, group 1 (n = 15) Detuned ultrasound machine, group 2 (n = 15) | 28 days | McGill Pain Questionnaire Numerical Pain Rating Scale 101 |
| Kucera et al., 2004 [25]. Prague | 203 | 18–50 Group 1: 27.7 Group 2: 28.3 | 78 Group 1: 38 Group 2: 40 | 125 Group 1: 66 Group 2: 59 | Randomised, double-blind clinical multicentre parallel study | Acute lateral ankle distortions (24h after the injury) | Verum, Group 1: Cream 10% Reference, Group 2: Cream 1% | 14 days | VAS-10 |
| Truyols-Dominguez S. et al., 2013 [26]. Spain | 50 | 28–38 Total mean age: 33 | 13 Group 1: 6 Group 2: 7 | 37 Group 1: 19 Group 2: 18 | Randomised clinical trial | Acute inversion ankle sprain Grade I and II (Injured <5 days) | Thrust and nonthrust manipulation and exercise interven tion, group 1 (n = 25) The same protocol plus myofascial manual therapy techniques, group 2 (n = 25) | 28 days | Numeric pain rating scale Total Functional Score for Assessment of Acute Lateral Ankle Sprains |
| Bleakley et al., 2006 [27]. UK | 89 | Total mean age: 29.9 Group 1: 29.8 Group 2: 31.2 | 31 Group 1: 15 Group 2: 16 | 58 Group1: 28 Group2: 30 | Randomised controlled trial, double-blind | Mild/moderate ankle sprain <48h after injury) Grades I and II | Intermittent ice, group 1 (n = 43) Standard ice application, group 2 (n = 46) | 42 days | Binskley’s lower extremity functional scale VAS |
| Cooke et al., 2009 [2]. UK | 584 | 16–72 Total mean age: 30 Group 1: 31 Group 2: 30 Group 3: 29 Group 4: 30 | 247 Group 1: 64 Group 2: 54 Group 3: 65 Group 4: 64 | 337 Group 1: 80 Group 2: 88 Group 3: 84 Group 4: 85 | Multicentred RCT with blinded assessment of outcome | Acute severe ankle sprain | Group 1: Tubular bandage (n = 144) Group 2: Below-knee cast (n = 142) Group 3: Aircast brace (n = 149) Group 4: Bledsoe boot (n = 149) | 270 days | FAOS Functional Limitations Profile SF-12 EQ-5D VAS |
| Bassett et al., 2007 [11]. New Zealand | 47 | 13–62 | 19 Group 1: 11 Group 2: 8 | 28 Group 1: 14 Group 2: 14 | Controlled trial | Acute ankle sprain (first-time) Grades I, II and III | Clinical intervention, group 1 (n = 25) Home intervention, group 2 (n = 22) | 14 days | Lower Limb Task Questionnaire Motor Activity Scale |
| Bleakley et al., 2010 [28]. UK | 101 | 16–65 | 32 Group1: 17 Group2: 15 | 69 Group1: 34 Group 2: 35 | Randomised controlled trial, blinded outcome assessor | Acute ankle sprain Grade I or II | Standard, group 1 (n = 51) Exercise, group 2 (n = 50) | 112 days | VAS LEFS |
| Brison et al., 2016 [9]. Canada | 504 | - | 280 Group1: 146 Group 2: 134 | 224 Group 1: 108 Group 2: 116 | Randomised controlled trial | Simple Grade I or II ankle sprain. | Physiotherapy, group 1 (n = 254) Usual care, group 2 (n = 250) | 180 days | Foot and Ankle Outcome Score |
| Cleland et al., 2013 [29]. USA | 74 | 16–60 | 36 Group 1: 19 Group 2: 17 | 38 Group 1: 18 Group 2: 20 | Randomised clinical trial, non-blinded | Inversion ankle sprain, acute and subacute | Manual therapy and exercise, group 1 (n = 37) Home exercise programme, group 2 (n = 37) | 180 days | FAAM LEFS Numeric pain rating scale |
| Coudreuse et al., 2010 [30]. France | 233 | 18–65 | 86 | 148 | Randomised, double-blind, placebo-controlled study | Lateral ankle sprain (<48 hours after the injury) | Novel plaster with diclofenac, epolamine and heparin, group 1 Placebo plaster, group 2 | 7 days | VAS |
| Fotiadis et al., 2011 [31]. Greece | 79 | Mean age Group 1: 38.21 Group 2: 35.35 | 35 Group 1: 20 Group 2: 15 | 44 Group 1: 22 Group 2: 24 | Prospective randomised study | Type II and III acute (less than 24 h) lateral ankle sprain | Group 1: Micronized purified flavonoid fraction (Daflon 1000 mg) (n = 42) Group 2: (Control group) Standard treatment (n = 39) | 20 days | VAS |
| Gonzalez de Vega et al., 2013 [10]. Spain | 420 | 18–40 | 112 Group 1: 39 Group 2: 39 Group3: 34 | 308 Group 1: 104 Group 2: 101 Group 3: 103 | Multicentre, randomised, blinded and active-controlled study | Acute unilateral ankle sprain within the past 24 h. Grades I, II and III | Traumeel ointment (T-O), group 1 (n = 143) Traumeel gel (T-G), group 2 (n = 140) Diclofenac gel, group 3 (n = 137) | 42 days | VAS FAAM |
| Man et al., 2007 [32]. UK | 34 | Total mean age 30.2 Group 1 34 Group 2 29 Group 3 28 | 11 | 23 | Randomised trial | Acute ankle sprain injury (within 5 days) | Neuromuscular electrical stimulation treatment, group 1 (n = 11) Submotor ES treatment (control group), group 2 (n = 11) Sham ES, group 3 (n = 12) | 14 days | Adapted Hughston Clinic Subjective Rating Scale for Ankle Disorders score |
| Kim et al., 2017 [33]. South Korea | 22 | Total mean age: 17.72 | 0 | 22 | Cross-over randomised design | Grades I and II lateral ankle sprain | Ankle balance taping group 1 Placebo taping group 2 No taping group 3 | 28 days | VAS |
| Naeem et al., 2014. [34]. Pakistan | 120 | Group 1: 28.77 Group 2: 29.83 | 77 Group 1: 35 Group 2: 42 | 43 Group 1: 25 Group 2: 18 | Level I Randomised controlled trial | Grade I or II lateral ankle sprain | Functional treatment tubigrip, group 1 (n = 60) Plaster of Paris, group 2 (n = 60) | 42 days | VAS Karlsson score |
| Sandoval et al., 2010 [35]. Colombia | 28 | Total mean age: 21 Group 1: 21.3 Group 2: 22.5 Group 3: 20.3 | 10 | 18 | Double-blind, controlled clinical trial | Grade I and II sprain mild or moderate, non-severe | Conventional treatment, group 1 (n = 10) HVPC (+) group 2. Conventional treatment and HVPC (positive polarity) (n = 8) HVPC (−) group 3. Conventional treatment and HVPC (negative polarity) (n = 10) | 56 days | VAS |
| Stasinopoulos et al., 2016 [36]. Greece. | 50 | 18–35 Group 1: 27.92 Group 2: 27.96 | 15 Group 1: 8 Group 2: 7 | 35 Group 1: 19 Group 2: 16 | Single-centre, parallel group, single-blind, controlled study | Acute ankle sprain Grade II | Group 1: Cryotherapy plus Bioptron light therapy (n = 27) Group 2: Control group, cryotherapy only (n = 23) | 5 days | VAS |
| Sultan et al., 2012 [37]. England | 36 | Group 1: 30 Group 2: 34 | - | - | Single-centre, randomised, single-blinded, clinical trial | Ankle sprains sustained within 72 h. Grade I, II, III. | Tubigrip, group 1 (n = 18) Elastic stocking, group 2 (n = 18) | 56 days | VAS SF12 |
| Tully et al., 2012 [38]. Northern Ireland. | 52 | 16–65 Group 1: 24.1 Group 2: 26.1 Group 3: 21.9 | 23 Group 1 6 Group2: 8 Group 3: 9 | 29 Group 1: 10 Group 2: 10 Group 3: 9 | Randomised controlled trial | Acute ankle sprain (<7 days) Grade I or II | Standard, group 1 (n = 16) Exercise, group 2 (n = 18) Non-injured control. Group 3 (n = 18) | 7 days | Lower Extremity Functional Scale VAS |
| Zhao et al., 2018 [39]. China. | 62 | Group 1: 34 Group 2: 30 Group3: 33 | - | - | Randomised controlled trial | Acute ankle sprains identified at 48 hours since the injury. Grades I and II | Standard treatment (RICE), group 1 (n = 19) Standard treatment (RICE) plus acupressure therapy, group 2 (n = 21) Standard treatment plus mock acupressure therapy, group 3 (n = 22) | 56 days | VAS American Orthopedic Foot and Ankle Score SF12v2 |
| Author | Outcome | Treatment | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pellow JE et al. [24] | Experimental group: Mortise separation adjustment | Control group: Detuned ultrasound machine | |||||||||||||
| Pre | Post 1 month | p-value | Pre | Post 1 month | p-value | ||||||||||
| McGill Pain Questionnaire | 0.20 | 0.03 | 0.42 | 0.24 | 0.12 | 0.01 | |||||||||
| NPRS (0–10) | 28.73 | 8.33 | 0.72 | 30.73 | 16.87 | 0.040 | |||||||||
| Kucera et al. [25] | Cream 10% | Cream 1% | |||||||||||||
| Visit 3/4 | Visit 14 | Visit 3/4 | Visit 14 | ||||||||||||
| VAS-10 pain at rest (mm) | 28.7 ± 17.1 | 43.9 ± 22.3 46 | 14.7 ± 13.5 | 41.6 ± 21.1 | |||||||||||
| VAS-10 functional (mm) | 28.7 ± 18.0 | 50.8 ± 18.9 | 18.1 ± 13.6 | 48.1 ± 19.8 | |||||||||||
| Truyols-Dominguez S. et al. [26] | Experimental Group | Comparison Group | |||||||||||||
| Pre-treatment | Post-treatment | Pre-treatment | Post-treatment | Pre p-value | |||||||||||
| NPRS (0–10) | 5.4 ± 2.0 | 2.1 ± 1.4 | 5.1 ± 1.0 | 3.2 ± 1.5 | 0.641 | ||||||||||
| Total Functional Score | 38.9 ± 8.8 | 78.6 ± 13.9 | 40.9 ± 18.0 | 64.0 ± 17.8 | 0.621 | ||||||||||
| Bleakley et al. [27] | Intermittent ice group | Standard ice application group | p-value | ||||||||||||
| LEFS | 24.6 ± 1.96 | 22.3 ± 2.23 | 0.38 | ||||||||||||
| Pain intensity at rest (0–10) | 1.0 ± 0.16 | 1.7 ± 0.22 | 0.08 | ||||||||||||
| Pain intensity activity (0–10) | 3.9 (0.28) | 4.7 (0.27) | 0.3 | ||||||||||||
| Cooke et al. [2] | Tubular bandage (mean) | Bledsoe (difference) | Aircast difference | Below-knee cast difference | |||||||||||
| 4 weeks | 9 months | 4 weeks | 9 months | 4 weeks | 9 months | 4 weeks | 9 months | ||||||||
| Score | Score | Score | ES | Score | ES | Score | ES | Score | ES | Score | ES | Score | ES | ||
| FAOS pain | 62.3 | 81.1 | 0.6 | 0.03 | 1.7 | 0.09 | 3.5 | 0.19 | 1.9 | 0.10 | 5.1 | 0.28 | 4.3 | 0.23 | |
| FAOS symptoms | 59.8 | 79.2 | −0.8 | −0.04 | −1.1 | −0.06 | 2.2 | 0.12 | 0.1 | 0.01 | 3.8 | 0.21 | 0.4 | 0.02 | |
| FAOS ADL | 82.3 | 93.1 | −0.1 | −0.01 | 0.1 | 0.01 | 0.6 | 0.05 | 1.0 | 0.10 | 3.0 | 0.24 | 1.2 | 0.12 | |
| FAOS sports | 44.7 | 76.8 | −0.3 | −0.01 | 1.0 | 0.04 | 0.0 | 0.00 | 0.8 | 0.03 | 5.0 | 0.20 | 2.4 | 0.10 | |
| FAOS QoL | 43.0 | 64.9 | 1.9 | 0.08 | 4.0 | 0.15 | 4.9 | 0.22 | 6.1 | 0.24 | 5.9 | 0.26 | 6.3 | 0.24 | |
| FLP ambulatory | 16.9 | 6.3 | 0.1 | 0.01 | −1.5 | −0.18 | −0.1 | 0.00 | −2.2 | −0.26 | −3.1 | −0.24 | −1.7 | −0.21 | |
| SF-12 physical | 39.2 | 49.7 | −1.3 | −0.16 | 0.2 | 0.03 | −1.4 | −0.17 | −0.1 | −0.01 | 2.2 | 0.27 | 0.3 | 0.04 | |
| SF-12 mental | 43.4 | 47.7 | 1.0 | 0.10 | 1.4 | 0.14 | 0.1 | 0.01 | 1.8 | 0.18 | −0.6 | −0.05 | 1.2 | 0.12 | |
| EQ-5D | 0.60 | 0.73 | 0.03 | 0.14 | 0.06 | 0.28 | 0.00 | 0.02 | 0.05 | 0.25 | 0.06 | 0.28 | 0.04 | 0.18 | |
| VAS pain at rest | 19.2 | 10.1 | −0.7 | −0.04 | 0.7 | 0.05 | −0.7 | −0.04 | −2.9 | −0.19 | −4.8 | −0.27 | −0.8 | −0.05 | |
| Bassett et al. [11] | Clinical intervention group | Home intervention group | |||||||||||||
| Pre | Post | Pre | Post | ||||||||||||
| LLTQ recreational subscale | 27.92 ± 11.36 | 12.00 ± 10.10 | 20.27 ± 12.58 | 8.18 ± 7.24 | |||||||||||
| LLTQ ADL subscale | 13.72 ± 11.29 | 2.32 ± 3.60 | 7.18 ± 7.06 | 1.82 ± 3.58 | |||||||||||
| Motor Activity Scale | 1.20 ± 2.00 | 5.14 ± 1.28 | 1.77 ± 1.60 | 5.73 ± 1.08 | |||||||||||
| Bleakley et al. [28] | Standard | Exercise | |||||||||||||
| Score | Score | p-value | |||||||||||||
| Pain intensity at rest | 1.7 ± 0.22 | 1.0 ± 0.16 | 0.008 | ||||||||||||
| Pain intensity on activity | 4.7 ± 0.27 | 3.9 ± 0.28 | 0.3 | ||||||||||||
| Subjective function (LEFS) | 22.3 ± 2.23 | 24.6 ± 1.96 | 0.38 | ||||||||||||
| Brison et al. [9] | Physiotherapy group | Usual care group | |||||||||||||
| 1 month | 6 months | 1 month | 6 months | p-value 1 month | p-value 6 months | ||||||||||
| FAOS | 23/180 | 92/165 | 33/213 | 113/174 | 0.65 | 0.09 | |||||||||
| Cleland et al. [29] | Home Exercise Programme | Manual Therapy and Exercise (MTEX) | Between-Group Differences | ||||||||||||
| 4 weeks | 6 months | 4 weeks | 6 months | 4 weeks | 6 months | ||||||||||
| FAAM ADL (0–100%) | 9.6 | 24.6 | 21.3 | 30.8 | 11.7 | 6.2 | |||||||||
| FAAM sports (0–100%) | 13.8 | 33.5 | 27.1 | 40.7 | 13.3 | 7.2 | |||||||||
| LEFS (0–80) | 5.6 | 17.3 | 18.4 | 25.3 | 12.8 | 8.1 | |||||||||
| NPRS (0–10) | −1.5 | −3.1 | −2.7 | −3.6 | −1.2 | −0.47 | |||||||||
| Coudreuse et al. [30] | DHEP group | Placebo group | p-value | ||||||||||||
| Baseline | 7 days | Baseline | 7 days | Baseline | 7 days | ||||||||||
| VAS pain (0–100) | 73.2 ± 1.0 | 69.3 ± 1.1 | p = 0.007 | p < 0.01 | |||||||||||
| Fotiadis et al. [31] | Daflon group | Control group | p-value | ||||||||||||
| 2 days | 20 days | 2 days | 20 days | 2 days | 20 days | ||||||||||
| VAS pain (1–10) | 2.26 ± 1.86 | 0.64 ± 1.39 | 2.0 ± 1.64 | 0.32 ± 0.57 | 0.625 | 0.908 | |||||||||
| Gonzalez de Vega et al. [10] | Traumeel ointment | Traumeel gel | Diclofenac gel | ||||||||||||
| Pre | Post | Pre | Post | Pre | Post | ||||||||||
| VAS ankle pain | 52.6 | 3.1 | 53.1 | 4.1 | 55.7 | 3.1 | |||||||||
| FAAM ADL | 51.2 | 41.7 | 56.0 | 40.5 | 51.2 | 41.7 | |||||||||
| FAAM Sports | 18.8 | 50.0 | 25.0 | 50.0 | 18.8 | 50.0 | |||||||||
| Man et al. [32] | NMES Group | Submotor ES Group | Sham ES Group | ||||||||||||
| Session 1 | Session 3 | Session 1 | Session 3 | Session 1 | Session 3 | ||||||||||
| Adapted HCSRSAD | 65 (13) | 42 (20) | 70 (10) | 45 (17) | 63 (12) | 46 (16) | |||||||||
| Kim et al. [33] | Aquatic exercise | Land-based Exercise | Interaction Effect | ||||||||||||
| Baseline | 4 weeks | Baseline | 4 weeks | ||||||||||||
| VAS for pain | 5.70 (0.36) | 0.17 (0.16) | 5.66 (0.36) | 0.73 (0.16) | F = 3.75 | P = 0.033 | |||||||||
| Naeem et al. [34] | Functional Treatment Tubigrip group | Plaster of Paris (POP) group | p-value | ||||||||||||
| At presentation | At 6 weeks | at presentation | at 6 weeks | At presentation | At 6 weeks | ||||||||||
| VAS | 8.40 ± 0.92 | 3.88 ± 0.85 | 8.27 ± 0.94 | 4.97 ± 0.82 | 0.434 | <0.001 | |||||||||
| Karlsson score | 21.17 ± 6.31 | 76.25 ± 10.67 | 23.67 ± 5.24 | 70.10 ± 6.35 | 0.571 | <0.001 | |||||||||
| Sandoval et al. [35] | Conventional treatment GC | Conventional treatment EEAV (+) | Conventional treatment EEAV (−) | p value | |||||||||||
| First | Last | First | Last | First | Last | First | Last | ||||||||
| VAS at rest | 1.0 ± 1.6 | 0.03 ± 0.09 | 1.6 ± 2.8 | 0 | 0.8 ± 1.8 | 0 | 0.75 | 0.29 | |||||||
| VAS palpation | 5.8 ± 2.9 | 0.7 ± 0.84 | 5.6 ± 3.3 | 0.4 ± 0.6 | 6.9 ± 1.4 | 0.91 ± 0.91 | 0.53 | 0.41 | |||||||
| Stasinopoulos et al. [36] | Cryotherapy and Bioptron Light group | Cryotherapy only group | p-values | ||||||||||||
| Pre-treatment | Post-treatment | Before treatment | Post-treatment | Post-treatment | |||||||||||
| VAS pain (0–10) | 6.66 (6.89–6.46) | 4.46 (4.62–4.30) | 6.62 (6.79–6.41) 62.88 | 5.34 (5.48–5.28) | p < 0.0005 | ||||||||||
| Stocking group | Tubigrip | ||||||||||||||
| Sultan et al. [37] | Initial | 8 weeks | Initial | 8 weeks | |||||||||||
| Total SF-12 score | 100 (95–105) | 119 (118–121) | 100 (94–107) | 102 (99–107) | |||||||||||
| VAS score | 65 (56–73) | 5 (0–11) | 66 (59–73) | 18 (10–26) | |||||||||||
| Standard group | Exercise group | p Value | |||||||||||||
| Tully et al. [38] | At baseline | At 1 week | At baseline | 1 week | Baseline | 1 week | |||||||||
| LEFS | 35.31 ± 16.56 | 54.00 ± 12.61 | 38.22 ± 19.81 | 61.63 ± 13.05 | 0.65 | 0.10 | |||||||||
| VAS Pain at rest | 26.5 (23.3) | 7.1 ± 7.5 | 19.6 (17.5) | 3.3 ± 4.4 | 0.33 | 0.98 | |||||||||
| VAS Pain with activity | 53.06 ± 27.7 | 34.3 ± 22.9 | 53.3 ± 22.7 | 25.7 ± 22.1 | 0.08 | 0.26 | |||||||||
| Zhao et al. [39] | STG group | APG group | Mock APG group | ||||||||||||
| Baseline | 8 weeks | Baseline | 8 weeks | Baseline | 8 weeks | ||||||||||
| VAS pain | 5.05 | 0.26 | 5.05 | 0.10 | 4.86 | 0.41 | |||||||||
| AOFAS | 39.53 | 97.47 | 38.14 | 99.04 | 38.95 | 96.86 | |||||||||
| Total SF-12 score | 107.63 | 116.21 | 106.14 | 119.67 | 104.95 | 112.05 | |||||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortega-Avila, A.B.; Cervera-Garvi, P.; Marchena-Rodriguez, A.; Chicharro-Luna, E.; Nester, C.J.; Starbuck, C.; Gijon-Nogueron, G. Conservative Treatment for Acute Ankle Sprain: A Systematic Review. J. Clin. Med. 2020, 9, 3128. https://doi.org/10.3390/jcm9103128
Ortega-Avila AB, Cervera-Garvi P, Marchena-Rodriguez A, Chicharro-Luna E, Nester CJ, Starbuck C, Gijon-Nogueron G. Conservative Treatment for Acute Ankle Sprain: A Systematic Review. Journal of Clinical Medicine. 2020; 9(10):3128. https://doi.org/10.3390/jcm9103128
Chicago/Turabian StyleOrtega-Avila, Ana Belen, Pablo Cervera-Garvi, Ana Marchena-Rodriguez, Esther Chicharro-Luna, Christopher J. Nester, Chelsea Starbuck, and Gabriel Gijon-Nogueron. 2020. "Conservative Treatment for Acute Ankle Sprain: A Systematic Review" Journal of Clinical Medicine 9, no. 10: 3128. https://doi.org/10.3390/jcm9103128
APA StyleOrtega-Avila, A. B., Cervera-Garvi, P., Marchena-Rodriguez, A., Chicharro-Luna, E., Nester, C. J., Starbuck, C., & Gijon-Nogueron, G. (2020). Conservative Treatment for Acute Ankle Sprain: A Systematic Review. Journal of Clinical Medicine, 9(10), 3128. https://doi.org/10.3390/jcm9103128