
Evaluating the Impact of Post-Transplant Cyclophosphamide and Anti-Thymocyte Globulin on CMV Reactivation Following Allogeneic Hematopoietic Stem Cell Transplantation: A Systematic Literature Review

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
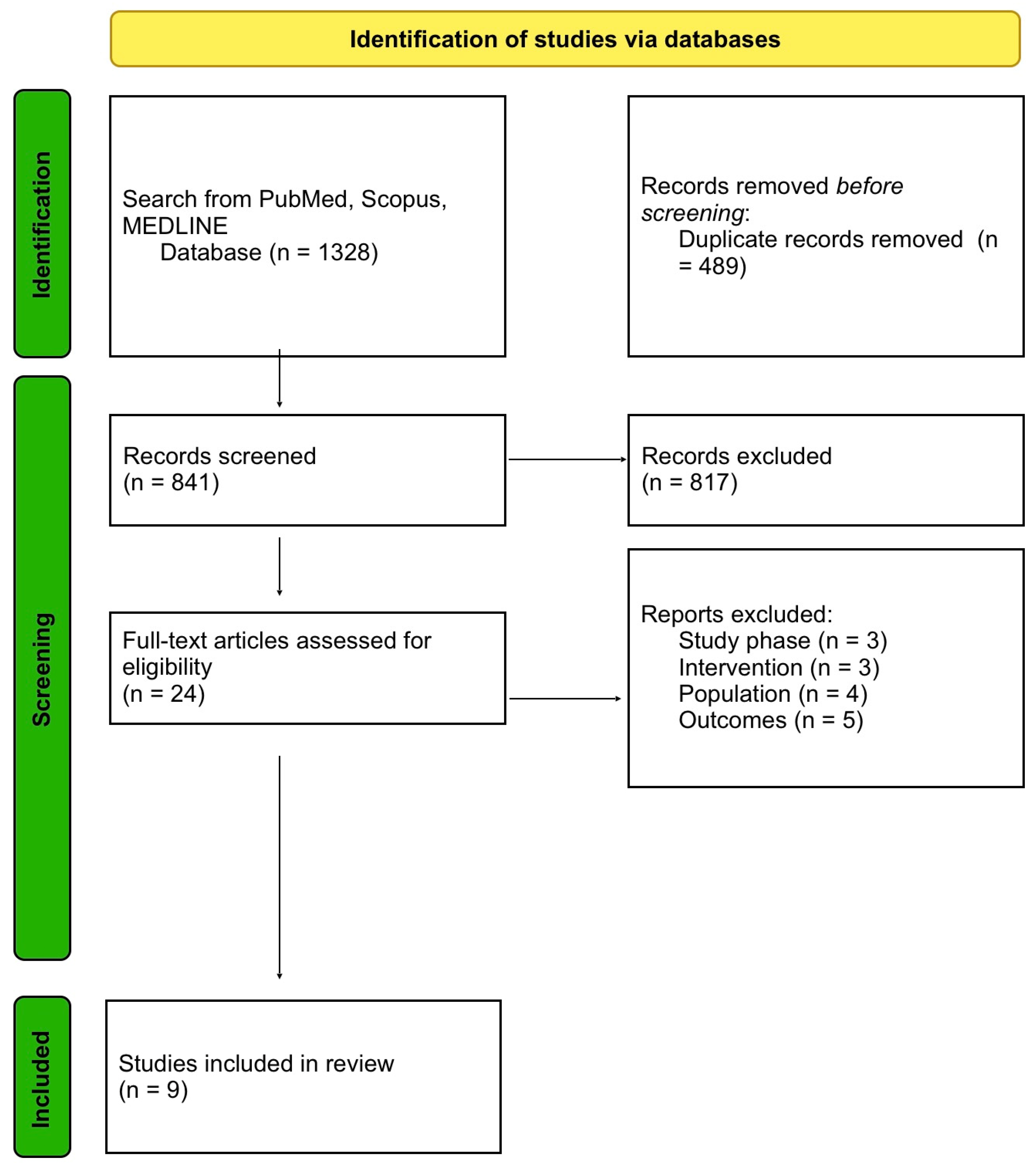
2.1. Systematic Literature Review
2.2. Data Presentation, Extraction, and Endpoints
3. Results
3.1. Systematic Literature Review
3.2. Outcomes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AML | acute myeloid leukaemia |
| ALL | acute lymphoblastic leukaemia |
| allo-HCT | allogeneic hematopoietic stem cell transplantation |
| ATG | anti-thymocyte globulin |
| BM | bone marrow |
| BMT | bone marrow transplantation |
| CIs | confidence intervals |
| CIBMTR | Center for International Blood and Marrow Transplant Research |
| CML | chronic myeloid leukaemia |
| CMV | cytomegalovirus clinically significant CMV infections |
| CS-CMVis | clinically significant CMV infections |
| EBMT | European Group for Bone and Marrow Transplantation |
| GvHD | graft-versus-host disease |
| aGvHD | acute graft-versus-host disease |
| cGvHD | chronic graft-versus-host disease |
| GvL | graft-versus-leukaemia |
| HL | Hodgkin lymphoma |
| NHL | non-Hodgkin lymphoma |
| HRs | hazard ratios |
| MAC | myeloablative conditioning |
| MDS | myelodysplastic syndrome |
| MDS-MPN | myelodysplastic syndrome-myeloproliferative neoplasm |
| MM | multiple myeloma |
| MMF | mycophenolate mofetil |
| MRD | matched related donor |
| MMRD | mismatched related donor |
| MUD | matched unrelated donor |
| MMUD | mismatched unrelated donor |
| MPNs | myeloproliferative neoplasms |
| MTX | methotrexate |
| NMA | nonmyeloablative conditioning |
| NR | not reported |
| NRM | non-relapse mortality |
| NS | not significant |
| OS | overall survival |
| PBSC | peripheral blood stem cells |
| PMF | primary myelofibrosis |
| PTCy | post-transplantation cyclophosphamide |
| RIC | reduced-intensity conditioning |
| SD | standard deviation |
| Tac | tacrolimus |
| TCD | T-cell depletion |
| TRM | transplant-related mortality |
References
- Copelan, E.A. Hematopoietic Stem-Cell Transplantation. N. Engl. J. Med. 2006, 354, 1813–1826. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, M.M.; Gale, R.P.; Sondel, P.M.; Goldman, J.M.; Kersey, J.; Kolb, H.J.; Rimm, A.A.; Ringden, O.; Rozman, C.; Speck, B.; et al. Graft-Versus-Leukemia Reactions After Bone Marrow Transplantation. Blood 1990, 75, 555–562. [Google Scholar] [CrossRef] [PubMed]
- Glucksberg, H.; Storb, R.; Fefer, A.; Buckner, C.D.; Neiman, P.E.; Clift, R.A.; Lerner, K.G.; Thomas, E.D. Clinical Manifestations of Graft-versus-Host Disease in Human Recipients of Marrow from HL-A-Matched Sibling Donors. Transplantation 1974, 18, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Klein, J.; Haagenson, M.; Baxter-Lowe, L.A.; Confer, D.L.; Eapen, M.; Fernandez-Vina, M.; Flomenberg, N.; Horowitz, M.; Hurley, C.K.; et al. High-Resolution Donor-Recipient HLA Matching Contributes to the Success of Unrelated Donor Marrow Transplantation. Blood 2007, 110, 4576–4583. [Google Scholar] [CrossRef] [PubMed]
- Woolfrey, A.; Klein, J.P.; Haagenson, M.; Spellman, S.; Petersdorf, E.; Oudshoorn, M.; Gajewski, J.; Hale, G.A.; Horan, J.; Battiwalla, M.; et al. HLA-C Antigen Mismatch Is Associated with Worse Outcome in Unrelated Donor Peripheral Blood Stem Cell Transplantation. Biol. Blood Marrow Transpl. 2011, 17, 885–892. [Google Scholar] [CrossRef] [PubMed]
- Maiers, M.; Gragert, L.; Klitz, W. High-Resolution HLA Alleles and Haplotypes in the United States Population. Hum. Immunol. 2007, 68, 779–788. [Google Scholar] [CrossRef]
- Gragert, L.; Eapen, M.; Williams, E.; Freeman, J.; Spellman, S.; Baitty, R.; Hartzman, R.; Rizzo, J.D.; Horowitz, M.; Confer, D.; et al. HLA Match Likelihoods for Hematopoietic Stem-Cell Grafts in the U.S. Registry. N. Engl. J. Med. 2014, 371, 339–348. [Google Scholar] [CrossRef]
- Barker, J.N.; Boughan, K.; Dahi, P.B.; Devlin, S.M.; Maloy, M.A.; Naputo, K.; Mazis, C.M.; Davis, E.; Nhaissi, M.; Wells, D.; et al. Racial Disparities in Access to HLA-Matched Unrelated Donor Transplants: A Prospective 1312-Patient Analysis. Blood Adv. 2019, 3, 939–944. [Google Scholar] [CrossRef]
- D’Souza, A.; Fretham, C.; Lee, S.J.; Arora, M.; Brunner, J.; Chhabra, S.; Devine, S.; Eapen, M.; Hamadani, M.; Hari, P.; et al. Current Use of and Trends in Hematopoietic Cell Transplantation in the United States. Biol. Blood Marrow Transpl. 2020, 26, e177–e182. [Google Scholar] [CrossRef]
- Dybko, J.; Giordano, U.; Pilch, J.; Mizera, J.; Borkowski, A.; Mordak-Domagała, M. Comparison of Different Rabbit Anti-Thymocyte Globulin Formulations in the Prophylaxis of Graft-versus-Host Disease: A Systematic Review. J. Clin. Med. 2023, 12, 5449. [Google Scholar] [CrossRef]
- Roberto, A.; Castagna, L.; Zanon, V.; Bramanti, S.; Crocchiolo, R.; McLaren, J.E.; Gandolfi, S.; Tentorio, P.; Sarina, B.; Timofeeva, I.; et al. Role of Naive-Derived T Memory Stem Cells in T-Cell Reconstitution Following Allogeneic Transplantation. Blood 2015, 125, 2855–2864. [Google Scholar] [CrossRef] [PubMed]
- Kanakry, C.G.; O’Donnell, P.V.; Furlong, T.; De Lima, M.J.; Wei, W.; Medeot, M.; Mielcarek, M.; Champlin, R.E.; Jones, R.J.; Thall, P.F.; et al. Multi-Institutional Study of Post-Transplantation Cyclophosphamide as Single-Agent Graft-versus-Host Disease Prophylaxis after Allogeneic Bone Marrow Transplantation Using Myeloablative Busulfan and Fludarabine Conditioning. J. Clin. Oncol. 2014, 32, 3497–3505. [Google Scholar] [CrossRef] [PubMed]
- Wachsmuth, L.P.; Patterson, M.T.; Eckhaus, M.A.; Venzon, D.J.; Gress, R.E.; Kanakry, C.G. Post-Transplantation Cyclophosphamide Prevents Graft-versus-Host Disease by Inducing Alloreactive T Cell Dysfunction and Suppression. J. Clin. Investig. 2019, 129, 2357–2373. [Google Scholar] [CrossRef] [PubMed]
- EBMT 2023—Program. Available online: https://ebmt2023.abstractserver.com/program/#/details/persons/446 (accessed on 24 July 2023).
- Spyridonidis, A. How Much Immunosuppression Do We Need? Blood 2017, 129, 1241–1243. [Google Scholar] [CrossRef]
- Mielcarek, M.; Furlong, T.; O’Donnell, P.V.; Storer, B.E.; McCune, J.S.; Storb, R.; Carpenter, P.A.; Flowers, M.E.D.; Appelbaum, F.R.; Martin, P.J. Posttransplantation Cyclophosphamide for Prevention of Graft-versus-Host Disease after HLA-Matched Mobilized Blood Cell Transplantation. Blood 2016, 127, 1502–1508. [Google Scholar] [CrossRef]
- Luznik, L.; Bolaños-Meade, J.; Zahurak, M.; Chen, A.R.; Smith, B.D.; Brodsky, R.; Huff, C.A.; Borrello, I.; Matsui, W.; Powell, J.D.; et al. High-Dose Cyclophosphamide as Single-Agent, Short-Course Prophylaxis of Graft-versus-Host Disease. Blood 2010, 115, 3224–3230. [Google Scholar] [CrossRef]
- Kasamon, Y.L.; Ambinder, R.F.; Fuchs, E.J.; Zahurak, M.; Rosner, G.L.; Bolaños-Meade, J.; Levis, M.J.; Gladstone, D.E.; Huff, C.A.; Swinnen, L.J.; et al. Prospective Study of Nonmyeloablative, HLA-Mismatched Unrelated BMT with High-Dose Posttransplantation Cyclophosphamide. Blood Adv. 2017, 1, 288–292. [Google Scholar] [CrossRef]
- Jorge, A.S.; Suárez-Lledó, M.; Pereira, A.; Gutierrez, G.; Fernández-Avilés, F.; Rosiñol, L.; Llobet, N.; Solano, T.; Urbano-Ispízua, Á.; Rovira, M.; et al. Single Antigen-Mismatched Unrelated Hematopoietic Stem Cell Transplantation Using High-Dose Post-Transplantation Cyclophosphamide Is a Suitable Alternative for Patients Lacking HLA-Matched Donors. Biol. Blood Marrow Transpl. 2018, 24, 1196–1202. [Google Scholar] [CrossRef]
- Mehta, R.S.; Saliba, R.M.; Chen, J.; Rondon, G.; Hammerstrom, A.E.; Alousi, A.; Qazilbash, M.; Bashir, Q.; Ahmed, S.; Popat, U.; et al. Post-Transplantation Cyclophosphamide versus Conventional Graft-versus-Host Disease Prophylaxis in Mismatched Unrelated Donor Haematopoietic Cell Transplantation. Br. J. Haematol. 2016, 173, 444–455. [Google Scholar] [CrossRef]
- Bonifazi, F.; Rubio, M.T.; Bacigalupo, A.; Boelens, J.J.; Finke, J.; Greinix, H.; Mohty, M.; Nagler, A.; Passweg, J.; Rambaldi, A.; et al. Rabbit ATG/ATLG in Preventing Graft-versus-Host Disease after Allogeneic Stem Cell Transplantation: Consensus-Based Recommendations by an International Expert Panel. Bone Marrow Transpl. 2020, 55, 1093–1102. [Google Scholar] [CrossRef]
- McCurdy, S.R.; Luznik, L. Post-Transplantation Cyclophosphamide for Chimerism-Based Tolerance. Bone Marrow Transpl. 2019, 54, 769–774. [Google Scholar] [CrossRef] [PubMed]
- Luznik, L.; Pasquini, M.C.; Logan, B.; Soiffer, R.J.; Wu, J.; Devine, S.M.; Geller, N.; Giralt, S.; Heslop, H.E.; Horowitz, M.M.; et al. Randomized Phase III BMT CTN Trial of Calcineurin Inhibitor-Free Chronic Graft-Versus-Host Disease Interventions in Myeloablative Hematopoietic Cell Transplantation for Hematologic Malignancies. J. Clin. Oncol. 2022, 40, 356–368. [Google Scholar] [CrossRef] [PubMed]
- Carnevale-Schianca, F.; Caravelli, D.; Gallo, S.; Coha, V.; D’Ambrosio, L.; Vassallo, E.; Fizzotti, M.; Nesi, F.; Gioeni, L.; Berger, M.; et al. Post-Transplant Cyclophosphamide and Tacrolimus-Mycophenolate Mofetil Combination Prevents Graft-versus-Host Disease in Allogeneic Peripheral Blood Hematopoietic Cell Transplantation from HLA-Matched Donors. Biol. Blood Marrow Transpl. 2017, 23, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Greco, R.; Lorentino, F.; Morelli, M.; Giglio, F.; Mannina, D.; Assanelli, A.; Mastaglio, S.; Dalto, S.; Perini, T.; Lazzari, L.; et al. Posttransplantation Cyclophosphamide and Sirolimus for Prevention of GVHD after HLA-Matched PBSC Transplantation. Blood 2016, 128, 1528–1531. [Google Scholar] [CrossRef] [PubMed]
- Moiseev, I.S.; Pirogova, O.V.; Alyanski, A.L.; Babenko, E.V.; Gindina, T.L.; Darskaya, E.I.; Slesarchuk, O.A.; Bondarenko, S.N.; Afanasyev, B.V. Graft-versus-Host Disease Prophylaxis in Unrelated Peripheral Blood Stem Cell Transplantation with Post-Transplantation Cyclophosphamide, Tacrolimus, and Mycophenolate Mofetil. Biol. Blood Marrow Transpl. 2016, 22, 1037–1042. [Google Scholar] [CrossRef] [PubMed]
- Holtick, U.; Chemnitz, J.M.; Shimabukuro-Vornhagen, A.; Theurich, S.; Chakupurakal, G.; Krause, A.; Fiedler, A.; Luznik, L.; Hellmich, M.; Wolf, D.; et al. OCTET-CY: A Phase II Study to Investigate the Efficacy of Post-Transplant Cyclophosphamide as Sole Graft-versus-Host Prophylaxis after Allogeneic Peripheral Blood Stem Cell Transplantation. Eur. J. Haematol. 2016, 96, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Bradstock, K.F.; Bilmon, I.; Kwan, J.; Micklethwaite, K.; Blyth, E.; Deren, S.; Bayley, A.; Gebski, V.; Gottlieb, D. Single-Agent High-Dose Cyclophosphamide for Graft-versus-Host Disease Prophylaxis in Human Leukocyte Antigen-Matched Reduced-Intensity Peripheral Blood Stem Cell Transplantation Results in an Unacceptably High Rate of Severe Acute Graft-versus-Host Disease. Biol. Blood Marrow Transpl. 2015, 21, 941–944. [Google Scholar] [CrossRef]
- Tang, L.; Liu, Z.; Li, T.; Dong, T.; Wu, Q.; Niu, T.; Liu, T.; Ji, J. Post-Transplant Cyclophosphamide versus Anti-Thymocyte Globulin in Allogeneic Hematopoietic Stem Cell Transplantation from Unrelated Donors: A Systematic Review and Meta-Analysis. Front. Oncol. 2023, 13, 1071268. [Google Scholar] [CrossRef]
- Esquirol, A.; Pascual, M.J.; Kwon, M.; Pérez, A.; Parody, R.; Ferra, C.; Garcia Cadenas, I.; Herruzo, B.; Dorado, N.; Hernani, R.; et al. Severe Infections and Infection-Related Mortality in a Large Series of Haploidentical Hematopoietic Stem Cell Transplantation with Post-Transplant Cyclophosphamide. Bone Marrow Transpl. 2021, 56, 2432–2444. [Google Scholar] [CrossRef]
- Bacigalupo, A.; Lamparelli, T.; Bruzzi, P.; Guidi, S.; Alessandrino, P.E.; Di Bartolomeo, P.; Oneto, R.; Bruno, B.; Barbanti, M.; Sacchi, N.; et al. Antithymocyte Globulin for Graft-versus-Host Disease Prophylaxis in Transplants from Unrelated Donors: 2 Randomized Studies from Gruppo Italiano Trapianti Midollo Osseo (GITMO). Blood 2001, 98, 2942–2947. [Google Scholar] [CrossRef]
- Finke, J.; Bethge, W.A.; Schmoor, C.; Ottinger, H.D.; Stelljes, M.; Zander, A.R.; Volin, L.; Ruutu, T.; Heim, D.A.; Schwerdtfeger, R.; et al. Standard Graft-versus-Host Disease Prophylaxis with or without Anti-T-Cell Globulin in Haematopoietic Cell Transplantation from Matched Unrelated Donors: A Randomised, Open-Label, Multicentre Phase 3 Trial. Lancet Oncol. 2009, 10, 855–864. [Google Scholar] [CrossRef] [PubMed]
- Mikulska, M.; Bartalucci, C.; Raiola, A.M.; Oltolini, C. Does PTCY Increase the Risk of Infections? Blood Rev. 2023, 62, 101092. [Google Scholar] [CrossRef] [PubMed]
- Stern, L.; Withers, B.; Avdic, S.; Gottlieb, D.; Abendroth, A.; Blyth, E.; Slobedman, B. Human Cytomegalovirus Latency and Reactivation in Allogeneic Hematopoietic Stem Cell Transplant Recipients. Front. Microbiol. 2019, 10, 01186. [Google Scholar] [CrossRef] [PubMed]
- Green, M.L.; Leisenring, W.; Stachel, D.; Pergam, S.A.; Sandmaier, B.M.; Wald, A.; Corey, L.; Boeckh, M. Efficacy of a Viral Load-Based, Risk-Adapted, Preemptive Treatment Strategy for Prevention of Cytomegalovirus Disease after Hematopoietic Cell Transplantation. Biol. Blood Marrow Transpl. 2012, 18, 1687–1699. [Google Scholar] [CrossRef] [PubMed]
- Nishihori, T.; Shaheen, M.; El-Asmar, J.; Aljurf, M.; Kharfan-Dabaja, M.A. Therapeutic Strategies for Cytomegalovirus in Allogeneic Hematopoietic Cell Transplantation. Immunotherapy 2015, 7, 1059–1071. [Google Scholar] [CrossRef]
- Teira, P.; Battiwalla, M.; Ramanathan, M.; Barrett, A.J.; Ahn, K.W.; Chen, M.; Green, J.S.; Saad, A.; Antin, J.H.; Savani, B.N.; et al. Early Cytomegalovirus Reactivation Remains Associated with Increased Transplant-Related Mortality in the Current Era: A CIBMTR Analysis. Blood 2016, 127, 2427–2438. [Google Scholar] [CrossRef] [PubMed]
- Green, M.L.; Leisenring, W.M.; Xie, H.; Walter, R.B.; Mielcarek, M.; Sandmaier, B.M.; Riddell, S.R.; Boeckh, M. CMV Reactivation after Allogeneic HCT and Relapse Risk: Evidence for Early Protection in Acute Myeloid Leukemia. Blood 2013, 122, 1316–1324. [Google Scholar] [CrossRef] [PubMed]
- Elmaagacli, A.H.; Steckel, N.K.; Koldehoff, M.; Hegerfeldt, Y.; Trenschel, R.; Ditschkowski, M.; Christoph, S.; Gromke, T.; Kordelas, L.; Ottinger, H.D.; et al. Early Human Cytomegalovirus Replication after Transplantation Is Associated with a Decreased Relapse Risk: Evidence for a Putative Virus-versus-Leukemia Effect in Acute Myeloid Leukemia Patients. Blood 2011, 118, 1402–1412. [Google Scholar] [CrossRef]
- Foley, B.; Cooley, S.; Verneris, M.R.; Pitt, M.; Curtsinger, J.; Luo, X.; Lopez-Vergès, S.; Lanier, L.L.; Weisdorf, D.; Miller, J.S. Cytomegalovirus Reactivation after Allogeneic Transplantation Promotes a Lasting Increase in Educated NKG2C+ Natural Killer Cells with Potent Function. Blood 2012, 119, 2665–2674. [Google Scholar] [CrossRef]
- Modi, D.; Kondrat, K.; Kim, S.; Deol, A.; Ayash, L.; Ratanatharathorn, V.; Uberti, J.P. Post-Transplant Cyclophosphamide Versus Thymoglobulin in HLA-Mismatched Unrelated Donor Transplant for Acute Myelogenous Leukemia and Myelodysplastic Syndrome. Transpl. Cell. Ther. 2021, 27, 760–767. [Google Scholar] [CrossRef]
- Jimenez, A.J.; Komanduri, K.; Brown, S.; Wang, T.; Pereira, D.; Goodman, M.; Beitinjaneh, A.; Lekakis, L.; Chinapen, S.; Devlin, S.; et al. Improved GRFS after Posttransplant Cyclophosphamide-Based vs. ATG-Based HLA-Mismatched Unrelated Donor Transplant. Blood Adv. 2022, 6, 4491–4500. [Google Scholar] [CrossRef]
- Massoud, R.; Gagelmann, N.; Fritzsche-Friedland, U.; Zeck, G.; Heidenreich, S.; Wolschke, C.; Ayuk, F.; Christopeit, M.; Kröger, N. Comparison of Immune Reconstitution between Anti-T-Lymphocyte Globulin and Posttransplant Cyclophosphamide as Acute Graft-versus-Host Disease Prophylaxis in Allogeneic Myeloablative Peripheral Blood Stem Cell Transplantation. Haematologica 2022, 107, 857–867. [Google Scholar] [CrossRef]
- Dybko, J.; Sobczyk-Kruszelnicka, M.; Makuch, S.; Agrawal, S.; Dudek, K.; Giebel, S.; Gil, L. The Benefits of the Post-Transplant Cyclophosphamide in Both Haploidentical and Mismatched Unrelated Donor Setting in Allogeneic Stem Cells Transplantation. Int. J. Mol. Sci. 2023, 24, 5764. [Google Scholar] [CrossRef] [PubMed]
- Retière, C.; Willem, C.; Guillaume, T.; Vié, H.; Gautreau-Rolland, L.; Scotet, E.; Saulquin, X.; Gagne, K.; Béné, M.C.; Imbert, B.M.; et al. Impact on Early Outcomes and Immune Reconstitution of High-Dose Post-Transplant Cyclophosphamide vs. Anti-Thymocyte Globulin after Reduced Intensity Conditioning Peripheral Blood Stem Cell Allogeneic Transplantation. Oncotarget 2018, 9, 11451–11464. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.S.; Saliba, R.M.; Rondon, G.; Al-Atrash, G.; Bashir, Q.; Hosing, C.M.; Kebriaei, P.; Khouri, I.; Nieto, Y.; Oran, B.; et al. Post-Transplantation Cyclophosphamide Versus Tacrolimus and Methotrexate Graft-Versus-Host Disease Prophylaxis for HLA-Matched Donor Transplantation. Transpl. Cell. Ther. 2022, 28, 695.e1–695.e10. [Google Scholar] [CrossRef] [PubMed]
- Camargo, J.F.; Ebisu, Y.; Jimenez-Jimenez, A.; Natori, Y.; Moroz, I.; Morris, M.I.; Alencar, M.; Anderson, A.D.; Lekakis, L.; Beitinjaneh, A.; et al. Lower Incidence of Cytomegalovirus Reactivation Following Post-Transplantation Cyclophosphamide HLA-Mismatched Unrelated Donor Transplantation. Transpl. Cell. Ther. 2021, 27, 1017.e1–1017.e7. [Google Scholar] [CrossRef] [PubMed]
- Bailén, R.; Kwon, M.; Pascual-Cascón, M.J.; Ferrà, C.; Sanz, J.; Gallardo-Morillo, A.; García-Sola, A.; Torrent, A.; Jiménez-Lorenzo, M.J.; Piñana, J.L.; et al. Post-transplant cyclophosphamide for GVHD prophylaxis compared to ATG-based prophylaxis in unrelated donor transplantation. Ann. Hematol. 2021, 100, 541–553. [Google Scholar] [CrossRef] [PubMed]
- Goldsmith, S.R.; Abid, M.B.; Auletta, J.J.; Bashey, A.; Beitinjaneh, A.; Castillo, P.; Chemaly, R.F.; Chen, M.; Ciurea, S.; Dandoy, C.E.; et al. Posttransplant Cyclophosphamide Is Associated with Increased Cytomegalovirus Infection: A CIBMTR Analysis. Blood 2021, 137, 3291–3305. [Google Scholar] [CrossRef] [PubMed]
- Battipaglia, G.; Labopin, M.; Hamladji, R.M.; Blaise, D.; Chevallier, P.; Brissot, E.; Gerbitz, A.; Socié, G.; Afanasyev, B.; Ciceri, F.; et al. Post-Transplantation Cyclophosphamide versus Antithymocyte Globulin in Patients with Acute Myeloid Leukemia Undergoing Allogeneic Stem Cell Transplantation from HLA-Identical Sibling Donors: A Retrospective Analysis from the Acute Leukemia Working Party of the European Society for Blood and Marrow Transplantation. Cancer 2021, 127, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Little, J.S.; Duléry, R.; Shapiro, R.M.; Aleissa, M.M.; Zhou, G.; Koreth, J.; Antin, J.H.; Cutler, C.; Nikiforow, S.; Romee, R.; et al. Opportunistic Infections in Patients Receiving Post-Transplant Cyclophosphamide: Impact of Haploidentical Versus Unrelated Donor Allograft. Transpl. Cell. Ther. 2023, in press.
- Spyridonidis, A.; Labopin, M.; Brissot, E.; Moiseev, I.; Cornelissen, J.; Choi, G.; Ciceri, F.; Vydra, J.; Reményi, P.; Rovira, M.; et al. Should anti-thymocyte globulin be added in post-transplant cyclophosphamide based matched unrelated donor peripheral blood stem cell transplantation for acute myeloid leukemia? A study on behalf of the Acute Leukemia Working Party of the EBMT. Bone Marrow Transpl. 2022, 57, 1774–1780. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Yang, J.; Cai, Y.; Huang, C.; Xu, X.; Qiu, H.; Niu, J.; Zhou, K.; Zhang, Y.; Xia, X.; et al. Low-dose anti-thymocyte globulin plus low-dose post-transplant cyclophosphamide-based regimen for prevention of graft-versus-host disease after haploidentical peripheral blood stem cell transplants: A large sample, long-term follow-up retrospective study. Front. Immunol. 2023, 26, 1252879. [Google Scholar] [CrossRef] [PubMed]
- Zu, Y.; Li, Z.; Gui, R.; Liu, Y.; Zhang, Y.; Yu, F.; Zhao, H.; Fu, Y.; Zhan, X.; Wang, Z.; et al. Low-dose post-transplant cyclophosphamide with low-dose antithymocyte globulin for prevention of graft-versus-host disease in first complete remission undergoing 10/10 HLA-matched unrelated donor peripheral blood stem cell transplants: A multicentre, randomized controlled trial. Bone Marrow Transpl. 2022, 57, 1573–1580. [Google Scholar] [CrossRef]
- Battipaglia, G.; Labopin, M.; Blaise, D.; Diez-Martin, J.L.; Bazarbachi, A.; Vitek, A.; Chevallier, P.; Castagna, L.; Grillo, G.; Daguindau, E.; et al. Impact of the Addition of Antithymocyte Globulin to Post-Transplantation Cyclophosphamide in Haploidentical Transplantation with Peripheral Blood Compared to Post-Transplantation Cyclophosphamide Alone in Acute Myelogenous Leukemia: A Retrospective Study on Behalf of the Acute Leukemia Working Party of the European Society for Blood and Marrow Transplantation. Transpl. Cell. Ther. 2022, 28, 587.e1–587.e7. [Google Scholar] [CrossRef]
- El-Cheikh, J.; Devillier, R.; Dulery, R.; Massoud, R.; Al Chami, F.; Ghaoui, N.; Moukalled, N.; Pagliardini, T.; Marino, F.; Malard, F.; et al. Impact of Adding Antithymocyte Globulin to Posttransplantation Cyclophosphamide in Haploidentical Stem-Cell Transplantation. Clin. Lymphoma Myeloma Leuk. 2020, 20, 617–623. [Google Scholar] [CrossRef]
- Law, A.D.; Salas, M.Q.; Lam, W.; Michelis, F.V.; Thyagu, S.; Kim, D.D.H.; Lipton, J.H.; Kumar, R.; Messner, H.; Viswabandya, A. Reduced-Intensity Conditioning and Dual T Lymphocyte Suppression with Antithymocyte Globulin and Post-Transplant Cyclophosphamide as Graft-versus-Host Disease Prophylaxis in Haploidentical Hematopoietic Stem Cell Transplants for Hematological Malignancies. Biol. Blood Marrow Transpl. 2018, 24, 2259–2264. [Google Scholar] [CrossRef]


{kind=link}
| Modi et al., 2021, [41], n = 76 | Jimenez et al., 2022, [42], n = 128 | Massoud et al., 2022, [43], n = 599 | Dybko et al., 2023, [44], n = 145 | Retière et al., 2018, [45], n = 45 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Characteristic | ATG | PTCy | ATG | PTCy | ATG | PTCy | ATG + CsA + Mtx | PTCy + TAK+ MMF | ATG | PTCy |
| Number of patients | n = 51 | n = 25 | n = 46 | n = 82 | n = 476 | n = 123 | n = 35 | n = 110 | n = 15 | n = 30 |
| Age (years) median (range) | 53 (22–80) | 62 (31–76) | 55 (21–72) | 60 (21–75) | 50 (SD = 14) | 50 (SD = 13) | <60 years 91.4% >60 8.6% | <60 years 80.9% >60 19.1% | 65 (32–72) | 62 (24–72) |
| Sex, (%) (M)ale (F)emale | M: n = 27 (53%) F: n = 24 (47%) | M: n = 13 (52%) F: n = 12 (48%) | M: n = 24 (52%) F: n = 22 (48%) | M: n = 45 (55%) F: n = 37 (45%) | M: n = 294 (52%) F: n = 182 (48%) | M: n = 75 (60%) F: n = 48 (40%) | M: n = 18 (51.4%) F: n = 17 (48.6%) | M: n = 56 (50.9%) F: n = 54 (49.1%) | M: n = 8 (53%) F: n = 7 (47%) | M: n = 23 (77%) F: n = 7 (23%) |
| Follow-up median (range) | 5.27 years | 1.13 years | 45.7 months (3.7–106) | 27 months (6.6–58.7) | 16 months (1–169) | 16 months (1–169) | NR | NR | 24 months | 24 months |
| Diagnosis | AML: n = 40 (78%) MDS: n = 11 (22%) | AML: n = 19 (76%) MDS: n= 6 (24%) | NR | NR | ALL: n = 27 (6%) AML: n = 206 (43%) CML: n = 16 (3%) MDS: n = 43 (9%) MDS-MPN: n = 6 (1%) HL: n = 4 (1%) NHL: n = 75 (16%) MM: n = 64 (13%) PMF: n = 12 (3%) Other AL: n = 3 (1%) | ALL: n = 35 (29%) AML: n = 23 (19%) CML: n = 1 (1%) MDS: n = 2 (2%) MDS-MPN: n = 4 (3%) HL: n = 2 (2%) NHL: n = 13 (11%) MM: n = 38 (31%) PMF: n = 2 (2%) Other AL: n = 3 (2%) | AML + MDS n = 14 (40%) ALL n = 7 (20%) HL + NHL + MM n = 11 (31.4%) OMF, CML, SAA n = 3 (8.6%) | AML + MDS n = 52 (47.3%) ALL n = 15 (13.6%) HL + NHL + MM n = 31 (28.2%) OMF, CML, SAA n = 12 (10.9%) | MDS: n = 3 (20%) AML: n = 7 (35%) ALL: n = 2 (13%) Lymphoma n = 0 (0%) Hodgkin disease: n = 2 (13%) MF: n = 0 (0%) CLL: n = 0 (0%) CML: n = 1 (7%) | MDS: n = 4 (13%) AML: n = 11 (37%) ALL: n = 2 (7%) Lymphoma n = 1 (3%) Hodgkin disease: n = 3 (10%) MF: n = 7 (23%) CLL: n = 1 (3%) CML: n = 1 (3%) |
| Mehta et al., 2022, [46], n= 552 | Camargo et al., 2021, [47], n = 78 | Bailén et al., 2021, [48], n = 132 | Moiseev et al., 2016, [26], n = 211 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Characteristic | ATG + Tac/MTX | PTCy | ATG MMUD | PTCy MMUD | PTCy haplo | ATG + MTX + CsA | PTCy | ATG | PTCy |
| Number of patients | n = 306 | n = 246 | n = 37 | n = 22 | n = 19 | n = 60 | n = 72 | n = 125 | n = 86 |
| Age (years) median (range) | 29 (18–59) | 29 (18–60) | 54 (39–63) | 60 (50–62) | 48 (46–59) | 42 (31–55) | 44 (18–72) | 31 (18–62) | 34 (18–59) |
| Sex, (%) (M)ale (F)emale | NR | NR | M: n = 15 (41%) F: n = 22 (59%) | M: n = 9 (41%) F: n = 13 (59%) | M: n = 10 (53%) F: n = 9 (47%) | M: n = 37 (62%) F: n = 23 (38%) | M: n = 42 (57%) F: n = 30 (43%) | NR | NR |
| Follow-up median (range) | 53 (16–79) | 29 (3–64) | 259 days (98–531) | 228 days (155–370) | 217 days (148–368) | 78 months (12–125) | 26 months (6–65) | 17 months (1–64) | 12 months (4–30) |
| Diagnosis | AML/MDS n = 158 (52%) ALL n = 63 (21%) Chronic lymphoid malignancies n = 63 (21%) Chronic myeloid malignancies 1 n = 22 (7%) | AML/MDS n = 184 (75%) ALL n = 10 (4%) Chronic lymphoid malignancies n = 15 (6%) Chronic myeloid malignancies 1 n= 37 (15%) | AL: n = 19 (51%) Lymphoma: N = 5 (14%) MDS/MPN: n = 10 (27%) Other: n = 3 (8%) | AL: n = 16 (73%) Lymphoma: n = 2 (9%) MDS/MPN: n = 3 (14%) Other: n = 1 (5%) | AL: n = 9 (47%) Lymphoma: n = 4 (21%) MDS/MPN: n = 2 (11%) Other: n = 4 (21%) | AML/MDS: n = 35 (58%) ALL: n = 13 (22%) NHL/CLL: n = 8 (13%) Others n = 4 (7%) | AML/MDS: n = 47 (65%) ALL: n = 18 (25%) NHL/CLL: n = 2 (3%) Others n = 5 (7%) | AML: n = 83 (66%) ALL: n = 42 (34%) | AML: n = 52 (60%) ALL: n = 34 (40%) |
| Modi et al., 2021, [41], n = 76 | Jimenez et al., 2022, [42], n = 128 | Massoud et al., 2022, [43], n = 599 | Dybko et al., 2023, [44], n = 145 | Retière et al., 2018, [45], n = 45 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Characteristic | ATG | PTCy | ATG | PTCy | ATG | PTCy | ATG + CsA + Mtx | PTCy + TAK+ MMF | ATG | PTCy |
| Number of patients | n = 51 | n = 25 | n = 46 | n = 82 | n = 476 | n = 123 | n = 35 | n = 110 | n = 15 | n = 30 |
| Conditioning | MAC: n = 30 RIC: n = 21 | MAC: n = 5 RIC: n = 20 | Busulfan based n = 18 (39%) Fludrabine/Cy/TBI-200 n = 5 (11%) Melphalan based n = 16 (35%) TBI based n = 7 (15%) p = 0.1 | Busulfan based n = 25 (31%) Fludrabine/Cy/TBI-200 n = 22 (27%) Melphalan based n = 28 (34%) TBI based n = 7 (9%) p = 0.1 | Busulfan based n = 256 (54%) TBI based n = 130 (27%) Other n = 90 (19%) p < 0.001 | Busulfan based n = 29 (24%) TBI based n = 55 (45%) Other n = 39 (32%) p < 0.001 | RIC n = 2 (5.7%) MAC n = 30 (85.7%) NMA n = 3 (8.6%) | RIC n = 19 (17.3%) MAC n = 72 (65.5%) NMA n = 19 (17.3%) | RIC: n = 15 (100%) Clofarabine-based n = 15 (50%) Fludarabine-based n = 15 (50%) | RIC: n = 30 (100%) Clofarabine-based n = 10 (66%) Fludarabine-based n = 5 (33%) |
| Stem cell source, % | Bone marrow: n = 2 (4%) Peripheral blood: n = 49 (96%) | Bone marrow: n = 1 (4%) Peripheral blood: n = 24 (96%) | Bone marrow: n = 53 (41%) Peripheral blood: n = 75 (59%) | Bone marrow: n = 41 (50%) Peripheral blood: n = 41 (50%) | Peripheral blood: n = 476 (100%) | Peripheral blood: n = 123 (100%) | Peripheral blood: n = 35 (100%) | Peripheral blood: n = 110 (100%) | Peripheral blood: n = 15 (100%) | Peripheral blood: n = 30 (100%) |
| Donor | MMUD | MMUD | MMUD | MMUD | MRD n = 74 (16%) MMRD n = 3 (1%) MUD n = 303 (64%) MMUD n = 96 (20%) | MRD n = 31 (25%) MMRD n = 14 (11%) MUD n = 57 (46%) MMUD n = 21 (17%) | haploidentical n = 0 (0%) MMUD n = 35 (100%) | haploidentical n = 93 (84,5%) MMUD n = 17 (15.5%) | MUD n = 6 (40%) MRD n = 8 (53%) MMUD n = 1 (7%) | Haploidentical n = 20 (66%) MUD n = 6 (20%) MRD n = 4 (14%) |
| aGvHD grades II-IV | 52.9% (p = 0.01) | 24.4% (p = 0.01) | NR | NR | 36% (p = 0.005) | 40% (p = 0.005) | n = 11 (31.4%) p = 0.005 | n = 19 (17.2%) p = 0.005 | n = 7 (47%) | n = 14 (47%) |
| aGvHD grades III–IV | 19.6% (p = 0.38) | 12% (p = 0.38) | 31% (p = 0.03) | 15% (p = 0.03) | 15% (p = 0.005) | 12% (p = 0.005) | n = 7 (20.0%) p = 0.005 | 5 (4.5%) p = 0.005 | n = 3 (20%) | n =3 (10%) |
| cGvHD overall | 49% (p = 0.006) | 16% (p = 0.006) | 22% (p = 0.03) | 9% (p = 0.03) | 15% (p = 0.005) | 27% (p = 0.005) | n = 3 (8.6%) p = 0.005 | n = 20 (18.2%) p = 0.005 | NR | NR |
| CD34 dose, median (range) | 6.61 (1.2–25.58) p = 0.299 | 7.87 (2.21–20.75) p = 0.299 | 2.38 (0.18–9.0) p > 0.9 | 2.34 (0.08–10.8) p > 0.9 | 11.55 (SD = 64) | 7.18 (SD = 2) | NR | NR | 6.59 (4.57–10.02) p = NS | 8 (3.9–22) p = NS |
| HLA matching (%) | 7/8 (100%) | 7/8 (100%) | <7/8 n = 1 (2%) 7/8 n = 45 (98%) p < 0.001 | <7/8 n = 25 (30%) 7/8 n = 57 (70%) p < 0.001 | 10/10 n = 377 (SD = 79) <10/10 n = 99 (SD = 21) | 10/10 n = 88 (SD = 72) <10/10 n = 35 (SD = 29) | NR | NR | NR | NR |
| Overall survival | 1 year 57% p = 0.136 | 1 year 70% p = 0.136 | 1 year 0.45 2 years 0.29 p < 0.001 | 1 year 0.75 2 years 0.66 p < 0.001 | 3 years 65% p = 0.663 | 3 years 58% p = 0.663 | 5 years 32.4% p = 0.03 | 5 years 51.1% p = 0.03 | 1 year 73% 2 years 73% p = NS | 1 year 90% 2 years 79% p = NS |
| Mehta et al., 2022, [46], n = 552 | Camargo et al., 2021, [47], n = 78 | Bailén et al., 2021, [48], n = 132 | Moiseev et al., 2016, [26], n = 211 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Characteristic | ATG + Tac/MTX | PTCy | ATG MMUD | PTCy MMUD | PTCy haplo | ATG + MTX + CsA | PTCy | ATG | PTCy |
| Number of patients | n = 306 | n = 246 | n = 37 | n = 22 | n = 19 | n = 60 | n = 72 | n = 125 | n = 86 |
| Conditioning | MAC n = 196 (64%) RIC n = 110 (36%) | MAC n = 148 (60%) RIC n = 98 (40%) | MAC: n = 8 (22%) RIC: n = 29 (78%) | MAC: n = 3 (14%) RIC: n = 19 (86%) | MAC: n = 1 (5%) RIC: n = 18 (95%) | MAC: n = 41 (68%) RIC: n = 19 (32%) | MAC: n = 45 (63%) RIC: n = 27 (37%) | MAC: n = 32 (26%) RIC: n = 93 (74%) | MAC: n = 21 (24%) RIC: n = 65 (76%) |
| Stem cell source, % | Peripheral blood n = 195 (64%) Bone marrow n = 111 (36%) | Peripheral blood n = 190 (77%) Bone marrow n = 56 (23%) | Bone marrow: n = 10 (27%) Peripheral blood: n = 27 (73%) | Bone marrow: n = 20 (91%) Peripheral blood: n = 2 (9%) | Bone marrow: n = 2 (11%) Peripheral blood: n = 17 (89%) | Bone marrow: n = 5 (8%) Peripheral blood: n = 55 (92%) | Bone marrow: n = 16 (22%) Peripheral blood: n = 56 (78%) | Peripheral blood: n = 125 (100%) | Peripheral blood: n = 86 (100%) |
| Donor | MUD | MUD | MMUD | MMUD | haploidentical | MUD n = 49 (82%) MMUD n = 11 (18%) | MUD n = 63 (87%) MMUD n = 9 (13%) | MUD n = 106 (85%) MMUD n = 19 (15%) | MUD n = 68 (79%) MMUD n = 18 (21%) |
| aGvHD grades II-IV | 180-day 42% p = 0.03 | 180-day 52% p = 0.03 | n = 12 (32%) p = 0.39 | n = 4 (18%) p = 0.39 | n = 7 (37%) p = 0.39 | day +100: 67% p = 0.008 | day +100: 46% p = 0.008 | 45% p = 0.00003 | 19% p = 0.00003 |
| aGvHD grades III-IV | 9% p = 0.5 | 8% p = 0.5 | n = 1 (3%) p = 0.14 | n = 3 (14%) p = 0.14 | n = 0 (0%) | day +100: 34% p = 0.003 | day +100: 3% p = 0.003 | 27% p < 0.0001 | 4% p < 0.0001 |
| cGvHD overall | 3-year 19% p = 0.5 | 3-year 18% p = 0.5 | NR | NR | NR | 37% p = 0.75 | 37% p = 0.75 | 65% p < 0.0001 | 16% p < 0.0001 |
| CD34 dose, median (range) | NR | NR | 6.1 (2.8–8.4) p < 0.0001 | 2.0 (1.5–3.4) p < 0.0001 | 8.9 (6.7–14) p < 0.0001 | 4.7 (4–6) p = 0.786 | 5.2 (3.2–7) p = 0.786 | 5.9 (SD 1.5) | 6.0 (SD 1.5) |
| HLA matching (%) | NR | NR | NR | NR | NR | 10/10 n = 49 (82%) 8/8 n = 0 (0%) 9/10 n = 11 (18%) | 10/10 n = 55 (76%) 8/8 n = 8 (11%) 9/10 n = 9 (13%) | 10/10 n = 106 (85%) 8–9/10 n = 19 (15%) | 10/10 n = 68 (79%) 8–9/10 n = 18 (21%) |
| Overall survival | 3 years 55% p = 0.05 | 3 years 61% p = 0.05 | NR | NR | NR | 2 years 58% p = 0.475 | 2 years 60% p = 0.475 | 69% p = 0.0007 | 40% p = 0.0007 |
| Modi et al., 2021, [41], n = 76 | Jimenez et al., 2022, [42], n = 128 | Massoud et al., 2022, [43], n = 599 | Dybko et al., 2023, [44], n = 145 | Retière et al., 2018, [45], n = 45 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Characteristic | ATG | PTCy | ATG | PTCy | ATG | PTCy | ATG + CsA + Mtx | PTCy + TAK+ MMF | ATG | PTCy |
| Number of patients | n = 51 | n = 25 | n = 46 | n = 82 | n = 476 | n = 123 | n = 35 | n = 110 | n = 15 | n = 30 |
| CMV prophylaxis | NR | NR | letermovir | letermovir | acyclovir | acyclovir | NR | NR | NR | NR |
| (D)onor/(R)ecipient CMV status | D+/R+ n = 21 (41%) D+/R− n = 9 (18%) D−/R+ n = 20 (39%) D−/R− n = 1 (2%) p > 0.99 | D + /R+ n = 11 (44%) D + /R− n = 4 (16%) D−/R+ n = 9 (36%) D−/R− n = 1 (4%) p > 0.99 | R+ n = 37 (80%) | R+ n = 55 (67%) | D+/R+ n = 194 (41%) D+/R− n = 68 (14%) D−/R+ n = 62 (13%) D−/R− n = 151 (32%) | D+/R+ n = 58 (47%) D+/R− n = 15 (12%) D−/R+ n = 9 (7%) D−/R− n = 41 (34%) | R+ n = 29 (82.9%) | R+ n = 90 (81.8%) | NR | NR |
| CMV reactivation overall | 42% p = 0.07 | 20% p = 0.07 | NR | NR | n = 214 (46%) | n = 60 (50%) | n = 24 (68.8%) p = 0.022 | n = 51 (46.4%) p = 0.022 | n = 6 (40%) p = NS | n = 8 (27%) p = NS |
| CS-CMVi | n = 3 (6%) p = 0.07 | n = 0 p = 0.07 | 57% p = 0.1 | 30% p = 0.1 | NR | NR | NR | NR | NR | NR |
| Median time to CMV reactivation (days) | 29 days p = 0.02 | 39 days p = 0.02 | NR | NR | NR | NR | NR | NR | NR | NR |
| Mehta et al., 2022, [46], n = 552 | Camargo et al., 2021, [47], n = 78 | Bailén et al., 2021, [48], n = 132 | Moiseev et al., 2016, [26], n = 211 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Characteristic | ATG + Tac/MTX | PTCy | ATG MMUD | PTCy MMUD | PTCy haplo | ATG + MTX + CsA | PTCy | ATG | PTCy |
| Number of patients | n = 306 | n = 246 | n = 37 | n = 22 | n = 19 | n = 60 | n = 72 | n = 125 | n = 86 |
| CMV prophylaxis | NR | NR | Acyclovir n = 33 (89%) Acyclovir/Letermovir: n = 4 (11%) p = 0.007 | Acyclovir n = 12 (55%) Acyclovir/Letermovir n = 10 (45%) p = 0.007 | Acyclovir n = 16 (84%) Acyclovir/Letermovir n = 3 (16%) p = 0.007 | Acyclovir | Acyclovir | NR | NR |
| (D)onor/(R)ecipient CMV status | R+ n = 259 (84%) R− n = 46 (15%) Missing: n = 1 | R+ n = 172 (70%) R− n = 74 (30%) Missing: n = 0 | D+/R− n = 2 (5%) p = 0.85 D+/R+ n = 19 (51%) p = 0.84 D−/R+ n = 15 (41%) p = 0.87 D−/R− n = 1 (3%) p = 0.06 | D+/R− n = 2 (9%) p = 0.85 D+/R+ n = 10 (45%) p = 0.84 D−/R+ n = 10 (45%) p = 0.87 D−/R− n = 0 (0%) p = 0.06 | D+/R− n = 1 (5%) p = 0.85 D+/R+ n = 8 (42%) p = 0.84 D−/R+ n = 7 (37%) p = 0.87 D−/R− n = 3 (16%) p = 0.06 | D+/R− n = 4 (7%) D−/R+ n = 32 (53%) No serodiscordance n = 24 (40%) p = 0.533 | D+/R− n = 3 (4%) D−/R+ n = 37 (52%) No serodiscordance n = 32 (44%) p = 0.533 | NR | NR |
| CMV reactivation overall | 35% p = 0.002 | 24% p = 0.002 | 100-day 77% p = 0.02 200-day 86% p = 0.049 | 100-day 41% p = 0.02 200-day 64% p = 0.049 | 100-day 63% p = 0.02 200-day 68% p = 0.049 | n = 37 (51%) p = 0.191 | n = 24 (40%) p = 0.191 | n = 75 (60%) p = 0.045 | n = 40 (46.5%) p = 0.045 |
| CS-CMVi | NR | NR | 100-day 54% p = 0.01 200-day 58% p = 0.03 | 100-day 14% p = 0.01 200-day 25% p = 0.03 | 100-day 53% p = 0.01 200-day 53% p = 0.03 | NR | NR | n = 41 (32.8%) p = 0.177 | n = 21 (24.4%) p = 0.177 |
| Median time to CMV reactivation (days) | NR | NR | NR | NR | NR | NR | NR | NR | NR |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dybko, J.; Giordano, U.; Pilch, J.; Mizera, J.; Borkowski, A.; Dereń-Wagemann, I. Evaluating the Impact of Post-Transplant Cyclophosphamide and Anti-Thymocyte Globulin on CMV Reactivation Following Allogeneic Hematopoietic Stem Cell Transplantation: A Systematic Literature Review. J. Clin. Med. 2023, 12, 7765. https://doi.org/10.3390/jcm12247765
Dybko J, Giordano U, Pilch J, Mizera J, Borkowski A, Dereń-Wagemann I. Evaluating the Impact of Post-Transplant Cyclophosphamide and Anti-Thymocyte Globulin on CMV Reactivation Following Allogeneic Hematopoietic Stem Cell Transplantation: A Systematic Literature Review. Journal of Clinical Medicine. 2023; 12(24):7765. https://doi.org/10.3390/jcm12247765
Chicago/Turabian StyleDybko, Jarosław, Ugo Giordano, Justyna Pilch, Jakub Mizera, Artur Borkowski, and Izabela Dereń-Wagemann. 2023. "Evaluating the Impact of Post-Transplant Cyclophosphamide and Anti-Thymocyte Globulin on CMV Reactivation Following Allogeneic Hematopoietic Stem Cell Transplantation: A Systematic Literature Review" Journal of Clinical Medicine 12, no. 24: 7765. https://doi.org/10.3390/jcm12247765
APA StyleDybko, J., Giordano, U., Pilch, J., Mizera, J., Borkowski, A., & Dereń-Wagemann, I. (2023). Evaluating the Impact of Post-Transplant Cyclophosphamide and Anti-Thymocyte Globulin on CMV Reactivation Following Allogeneic Hematopoietic Stem Cell Transplantation: A Systematic Literature Review. Journal of Clinical Medicine, 12(24), 7765. https://doi.org/10.3390/jcm12247765