
Transfusion Burden in Allogeneic Hematopoietic Stem Cell Transplantation over Time: Experience from a Single Institution
 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Material and Methods
2.1. Patient Characteristics and Transplantation Modalities
2.2. Transfusion Protocol
2.3. Statistical Analysis
3. Results
3.1. Patient and Transplantation Characteristics
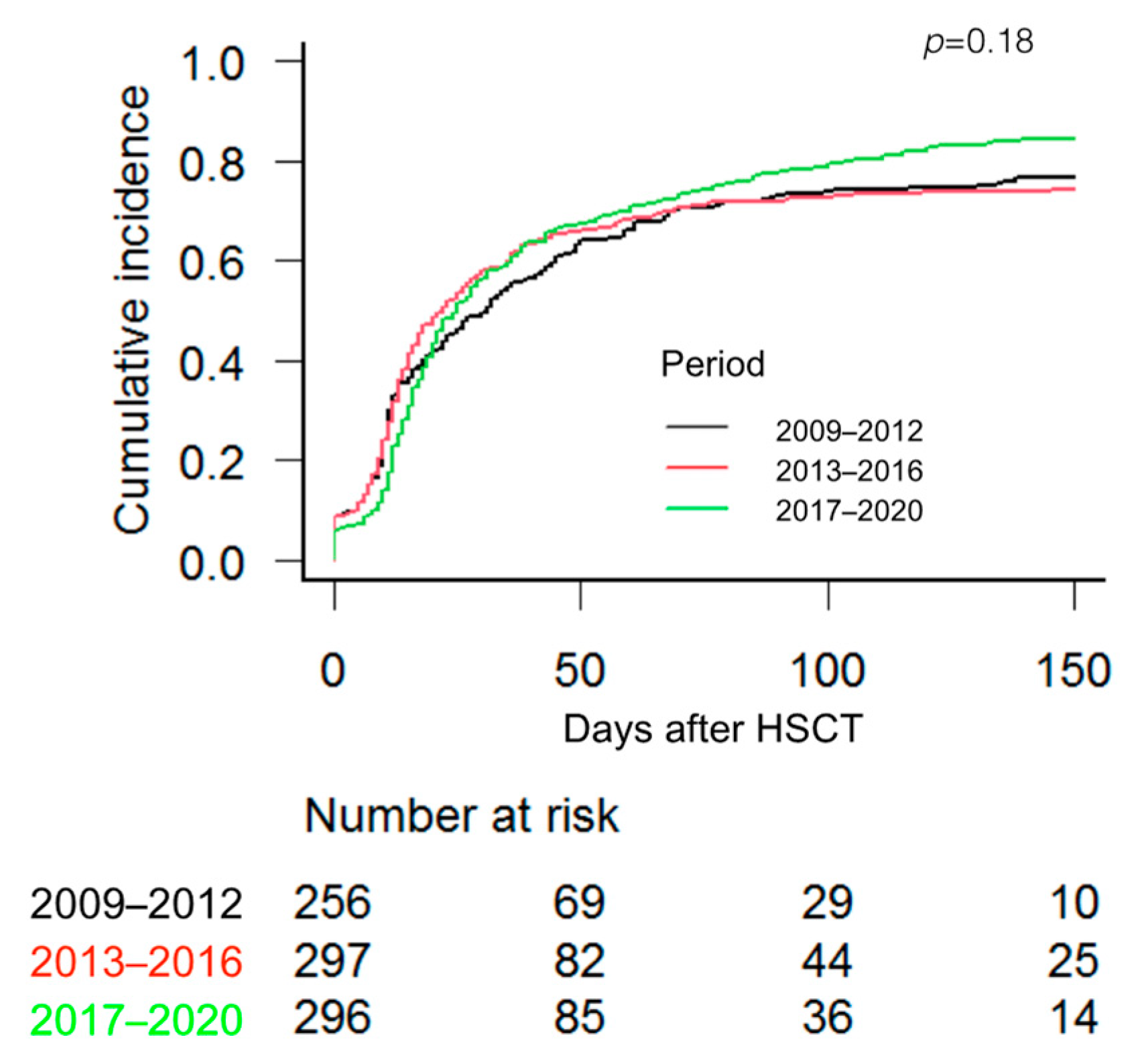
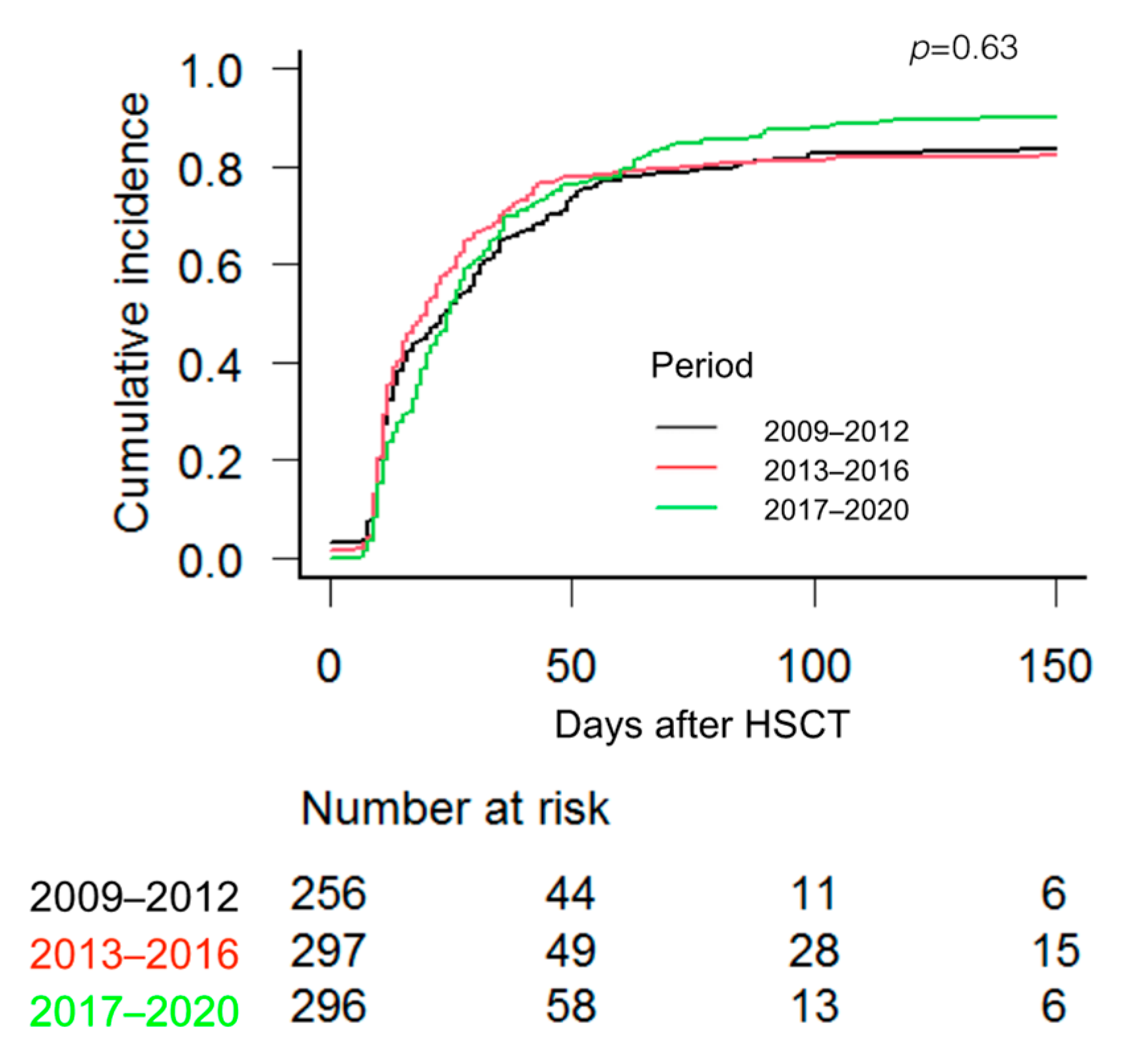
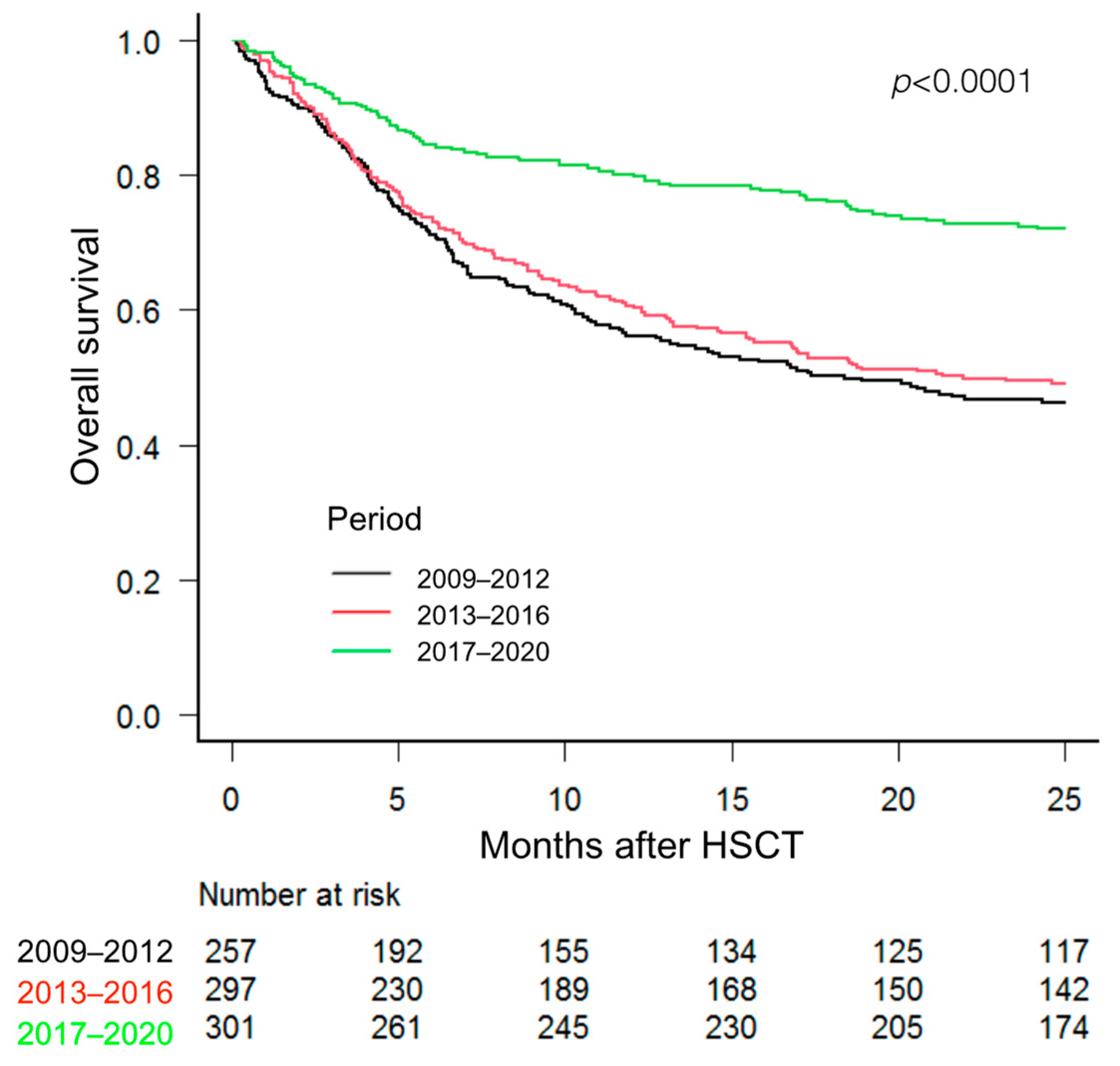
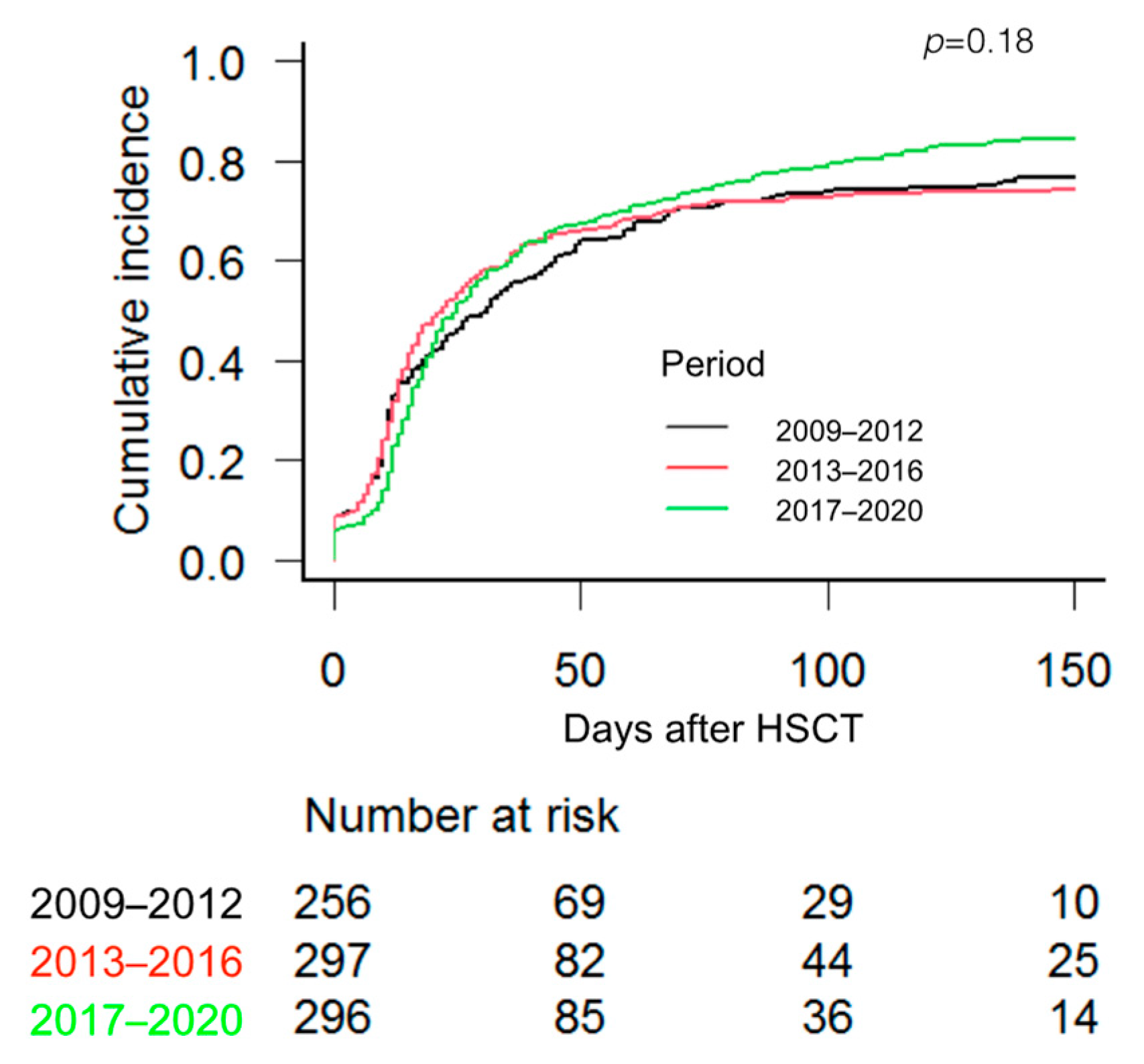
3.2. Transfusion Outcome
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cohn, C.S. Transfusion support issues in hematopoietic stem cell transplantation. Cancer Control 2015, 22, 52–59. [Google Scholar] [CrossRef]
- Elemary, M.; Seghatchian, J.; Stakiw, J.; Bosch, M.; Sabry, W. Goubran Transfusion challenges in hematology oncology and hematopoietic stem cell transplant-Literature review and local experience. Transfus. Apher. Sci. 2017, 56, 317–321. [Google Scholar] [CrossRef] [PubMed]
- Gastecki, K.; Shanley, R.; Welbig, J.; Cohn, C.; Brunstein, C.G. Red blood cell product utilization in patients undergoing allogeneic stem cell transplantation. Transfusion 2019, 59, 2301–2307. [Google Scholar] [CrossRef]
- Dahl, D.; Hahn, A.; Koenecke, C.; Heuft, H.G.; Dammann, E.; Stadler, M.; Buchholz, S.; Krauter, J.; Eder, M.; Sykora, K.W.; et al. Prolonged isolated red blood cell transfusion requirement after allogeneic blood stem cell transplantation: Identification of patients at risk. Transfusion 2010, 50, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Jekarl, D.W.; Kim, J.K.; Han, J.H.; Lee, H.; Yoo, J.; Lim, J.; Kim, Y. Transfusion support in hematopoietic stem cell transplantation. Blood Res. 2023, 58, 1–7. [Google Scholar] [CrossRef]
- Solves, P.; Lozano, M.; Zhiburt, E.; Anguita Velasco, J.; Maria Pérez-Corral, A.; Monsalvo-Saornil, S.; Yamazaki, S.; Okazaki, H.; Selleng, K.; Aurich, K.; et al. International Forum on Transfusion Practices in Haematopoietic Stem-Cell Transplantation: Summary. Vox Sang. 2021, 116, 609–612. [Google Scholar] [CrossRef] [PubMed]
- Stanworth, S.J.; Hyde, C.; Heddle, N.; Rebulla, P.; Brunskill, S.; Murphy, M.F. Prophylactic platelet transfusion for haemorrhage after chemotherapy and stem cell transplantation. Cochrane Database. Syst. Rev. 2004, 4, CD004269. [Google Scholar] [CrossRef]
- Solh, M.; Morgan, S.; McCullough, J.; Shanley, R.; Weisdorf, D.J. Blood transfusions and pulmonary complications after hematopoietic cell transplantation. Transfusion 2016, 56, 653–661. [Google Scholar] [CrossRef]
- Moscardó, F.; Sanz, J.; Carbonell, F.; Sanz, M.A.; Larrea, L.; Montesinos, P.; Lorenzo, I.; Vera, B.; Boluda, B.; Salazar, C.; et al. Effect of CD8⁺ cell content on umbilical cord blood transplantation in adults with hematological malignancies. Biol. Blood Marrow. Transpl. 2014, 20, 1744–1750. [Google Scholar] [CrossRef] [PubMed]
- De La Serna, J.; Sanz, J.; Bermúdez, A.; Cabrero, M.; Serrano, D.; Vallejo, C.; Gómez, V.; Moraleda, J.M.; Perez, S.G.; Caballero, M.D.; et al. Toxicity and efficacy of busulfan and fludarabine myeloablative conditioning for HLA-identical sibling allogeneic hematopoietic cell transplantation in AML and MDS. Bone Marrow Transpl. 2016, 51, 961–966. [Google Scholar] [CrossRef]
- Montoro, J.; Piñana, J.L.; Hernández-Boluda, J.C.; Hernani, R.; Lorenzo, I.; Pérez, A.; Guerreiro, M.; Balaguer-Rosello, A.; Sanz, G.F.; Carretero, C.; et al. Uniform graft-versus-host disease prophylaxis with posttransplant cyclophosphamide, sirolimus, and mycophenolate mofetil following hematopoietic stem cell transplantation from haploidentical, matched sibling and unrelated donors. Bone Marrow Transpl. 2020, 55, 2147–2159. [Google Scholar] [CrossRef]
- Lazzari, L.; Balaguer-Roselló, A.; Montoro, J.; Greco, R.; Hernani, R.; Lupo-Stanghellini, M.T.; Villalba, M.; Giglio, F.; Facal, A.; Lorentino, F.; et al. Post-transplant cyclophosphamide and sirolimus based graft-versus-host disease prophylaxis after allogeneic stem cell transplantation for acute myeloid leukemia. Bone Marrow Transpl. 2022, 57, 1389–1398. [Google Scholar] [CrossRef]
- Gajewski, J.L.; Johnson, V.V.; Sandler, S.G.; Sayegh, A.; Klumpp, T.R. A review of transfusion practice before, during, and after hematopoietic progenitor cell transplantation. Blood 2008, 112, 3036–3047. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transpl. 2013, 8, 452–458. [Google Scholar] [CrossRef]
- Solh, M.; Brunstein, C.; Morgan, S.; Weisdorf, D. Platelet and red blood cell utilization and transfusion independence in umbilical cord blood and allogeneic peripheral blood hematopoietic cell transplants. Biol. Blood Marrow Transpl. 2011, 17, 710–716. [Google Scholar] [CrossRef]
- Tomonari, A.; Takahashi, S.; Ooi, J.; Tsukada, N.; Konuma, T.; Kobayashi, T.; Sato, A.; Iseki, T.; Yamaguchi, T.; Tojo, A.; et al. Impact of ABO incompatibility on engraftment and transfusion outcome after unrelated cord blood transplantation: A single institute experience in japan. Bone Marrow Transpl. 2007, 40, 523–528. [Google Scholar] [CrossRef]
- Solves, P.; Carpio, N.; Carretero, C.; Lorenzo, J.I.; Sanz, J.; Gómez, I.; López-Chuliá, F.; Arilla, M.J.; Regadera, A.I.; Montesinos, P.; et al. ABO incompatibility does not influence transfusion requirements in patients undergoing single-unit umbilical cord blood transplantation. Bone Marrow Transpl. 2017, 52, 394–399. [Google Scholar] [CrossRef] [PubMed]
- Le Viellez, A.; P’Ng, S.; Buffery, S.; Wright, M.; Cooney, J.; Cannell, P.; Purtill, D. Red cell and platelet transfusion burden following myeloablative allogeneic haematopoietic stem cell transplantation. Intern. Med. J. 2015, 45, 1286–1292. [Google Scholar] [CrossRef]
- Griffith, L.M.; VanRaden, M.; Barrett, A.J.; Childs, R.W.; Fowler, D.H.; Kang, E.M.; Tisdale, J.F.; Klein, H.G.; Stroncek, D.F. Transfusion support for matched sibling allogeneic hematopoietic stem cell transplantation (1993–2010): Factors that predict intensity and time to transfusion independence. Transfusion 2019, 59, 303–315. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Xiao, Y.; Ran, Q.; Liu, Y.; Duan, Q.; Duan, H.; Ye, X.; Li, Z. Clinical observation of factors in the efficacy of blood component transfusión in patients following hematopoietic stem cell transplantation. PLoS ONE 2012, 7, e36912. [Google Scholar] [CrossRef]
- Wang, Z.; Sorror, M.L.; Leisenring, W.; Schoch, G.; Maloney, D.G.; Sandmaier, B.M.; Storb, R. The impact of donor type and ABO incompatibility on transfusion requirements after nonmyeloablative hematopoietic cell Transplantation. Br. J. Haematol. 2010, 149, 101–110. [Google Scholar] [CrossRef]
- Marco-Ayala, J.; Sanz, J.; Gómez-Seguí, I.; Balaguer-Rosello, A.; Montoro, J.; Guerreiro, M.; Chorao, P.; Facal, A.; Villalba, M.; Ángel Sanz, M.; et al. Impact of posttransplant cyclophosphamide on transfusion requirements in hla matched sibling peripheral blood stem cell transplantation. Transplant. Cell Ther. 2023, 13, S2666–S6367. [Google Scholar] [CrossRef]
- Desjonqueres, A.; Illiaquer, M.; Duquesne, A.; Le Bris, Y.; Peterlin, P.; Guillaume, T.; Delaunay, J.; Rialland, F.; Moreau, P.; Béné, M.C.; et al. Longer delay of hematological recovery and increased transfusion needs after haploidentical compared to non-haploidentical stem cell transplantation. Bone Marrow Transpl. 2016, 51, 1150–1152. [Google Scholar] [CrossRef] [PubMed]
- Yuan, S.; Yang, D.; Nakamura, R.; Zhuang, L.; Al Malki, M.M.; Karanes, C.; Wang, S. Red blood cell and platelet transfusion support in the first 30 and 100 days after allogeneic hematopoietic cell transplant. Transfusion 2020, 60, 2225–2242. [Google Scholar] [CrossRef]
- Solves, P.; Sanz, J.; Gómez, I.; de la Puerta, R.; Arnao, M.; Montoro, J.; Piñana, J.L.; Carretero, C.; Balaguer, A.; Guerreiro, M.; et al. Comparison of transfusion requirements in adult patients undergoing Haploidentical or single-unit umbilical cord blood stem cell transplantation. Eur. J. Haematol. 2019, 103, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Gooptu, M.; Antin, J.H. GVHD prophylaxis 2020. Front. Immunol. 2021, 12, 605726. [Google Scholar] [CrossRef] [PubMed]
- Tay, J.; Allan, D.S.; Chatelain, E.; Coyle, D.; Elemary, M.; Fulford, A.; Petrcich, W.; Ramsay, T.; Walker, I.; Xenocostas, A.; et al. Liberal Versus Restrictive Red Blood Cell Transfusion Thresholds in Hematopoietic Cell Transplantation: A Randomized, Open Label, Phase III, Noninferiority Trial. D. J. Clin. Oncol. 2020, 38, 1463–1473. [Google Scholar] [CrossRef] [PubMed]
- Avdic, A.; Tucker, S.; Evans, R.; Smith, A.; Zimmerman, M.B. Comparing the ratio of mean red blood cell transfusion episode rate of 1 unit versus 2 units in hematopoietic stem cell transplant patients. Transfusion 2016, 56, 2346–2351. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Characteristics | 2009–2012 | 2013–2016 | 2017–2020 | p |
|---|---|---|---|---|
| Patients, n (%) | 257 (30) | 297 (35) | 301 (35) | |
| Recipient age in years, median (range) | 46 (16–66) | 46.5 (16–70) | 50.5 (15–71) | 0.0007 |
| Sex, n (%) | 0.7 | |||
| Male | 151 (59) | 168 (57) | 178 (59) | |
| Female | 106 (41) | 129 (43) | 123 (41) | |
| Diagnosis, n (%) | 0.08 | |||
| Acute myeloid leukaemia | 115 (45) | 131 (44) | 140 (47) | |
| Acute lymphoblastic leukaemia | 45 (17) | 59 (20) | 47 (16) | |
| Chronic lymphoproliferative disorders | 38 (15) | 54 (18) | 37 (12) | |
| Multiple myeloma | 8 (3) | 11 (4) | 22 (7) | |
| Myelodysplastic syndrome | 16 (6) | 23 (7) | 22(7) | |
| Myeloproliferative disorders | 12 (5) | 7 (2) | 17 (6) | |
| Chronic myeloid leukaemia | 7 (3) | 5 (1) | 6 (2) | |
| Aplastic anaemia | 13 (5) | 7 (2) | 9 (3) | |
| Others | 3 (1) | 0 | 1 (0) | |
| Donor type, n (%) | <0.0001 | |||
| MRD | 120 (47) | 131 (44) | 107 (35) | |
| MUD | 14 (5) | 26 (9) | 94 (31) | |
| Haplo-HSCT | 7 (3) | 49 (16) | 84 (29) | |
| UCBT | 116 (45) | 91 (31) | 16 (5) | |
| Disease status at transplantation, n (%) | 0.3 | |||
| Early | 118 (46) | 151 (51) | 150 (50) | |
| Intermediate | 69 (27) | 68 (23) | 81 (27) | |
| Advanced | 54 (21) | 71 (24) | 60 (20) | |
| Not applicable | 16 (6) | 7 (2) | 10 (3) | |
| Stem cell source, n (%) | <0.0001 | |||
| Bone marrow | 2 (1) | 4 (2) | 26 (9) | |
| Peripheral blood | 139 (45) | 202 (68) | 259 (86) | |
| Umbilical cord blood | 116 (54) | 91 (30) | 16 (5) | |
| CD34+ × 106/kg, median (range) | 2.5 (0.04–14.4) | 4.4 (0.08–15.5) | 7.1 (0.1–25.9) | <0.0001 |
| Conditioning regimen, n (%) | 0.035 | |||
| Myeloablative | 146 (57) | 163 (55) | 141 (47) | |
| Reduced-intensity conditioning | 111 (43) | 134 (45) | 160 (53) | |
| GVHD prophylaxis, n (%) | <0.0001 | |||
| CsA + MTX | 118 (46) | 129 (43) | 3 (1) | |
| CsA + corticosteroids | 94 (37) | 83 (28) | 10 (3) | |
| CsA + MMF | 37 (14) | 28 (9) | 11 (4) | |
| PT-Cy + CsA + MMF | 1 (0) | 45 (15) | 15 (5) | |
| PT-Cy + MTX + sirolimus | 0 | 0 | 259 (86) | |
| Other | 7 (3) | 12 (4) | 3 (1) | |
| Transplant order, n (%) | ||||
| 1 | 201 (78) | 222 (75) | 227 (75) | |
| 2 | 55 (21) | 70 (24) | 66 (22) | |
| 3 | 1 (0) | 5 (1) | 8 (3) | |
| ABO compatibility, n (%) | 0.06 | |||
| Identical | 129 (50) | 180 (61) | 172 (57) | |
| Minor incompatibility | 54 (21) | 60 (20) | 66 (22) | |
| Major incompatibility | 62 (24) | 45 (15) | 45 (15) | |
| Bidirectional incompatibility | 12 (5) | 12 (4) | 18 (6) | |
| Days until neutrophils > 0.5 × 109/L, median (range) | 14 (5–55) | 14 (7–39) | 17 (7–39) | <0.0001 |
| Days until platelets > 20 × 109/L, median (range) | 23 (9–208) | 20 (8–319) | 28 (11–263) | <0.0001 |
| 2009–2012 | 2013–2016 | 2017–2020 | p | |
|---|---|---|---|---|
| MRD | ||||
| Patients, n (%) | 120 (34) | 131 (36) | 107 (30) | |
| RCB transfusion independence | 0.06 | |||
| Days, median (range) | 10.5 (0–153) | 11.5 (0–310) | 17.5 (0–190) | |
| CuI at 100 days, % (95% CI) | 85 (78–91) | 85 (78–90) | 79 (70–86) | |
| PLT transfusion independence | 0.0001 | |||
| Days, median (range) | 11 (0–80) | 11 (0–110) | 19 (7–155) | |
| CuI at 100 days, % (95% CI) | 94 (87–97) | 94 (88–97) | 87 (79–92) | |
| RBC units at day +30, median (range) | 2 (0–21) | 3 (0–24) | 4 (0–38) | <0.0001 |
| RBC units, day 31–90 *, median (range) | 4 (2–53) | 6 (2–49) | 4 (1–30) | 0.5 |
| PLT units at day +30, median (range) | 3 (0–55) | 3 (0–70) | 5 (1–39) | 0.002 |
| PLT units, day 31–90 *, median (range) | 19 (1–99) | 14 (1–83) | 14 (1–85) | 0.12 |
| MUD | ||||
| Patients, n (%) | 14 (11) | 26 (19) | 94 (70) | |
| RCB transfusion independence | 0.61 | |||
| Days, median (range) | 25.5 (0–149) | 12 (0–100) | 26 (0–260) | |
| CuI at 100 days, % (95% CI) | 78 (40–93) | 80 (57–92) | 84 (75–90) | |
| PLT transfusion independence | 0.23 | |||
| Days, median (range) | 18 (6–22) | 22 (6–173) | 25 (3–210) | |
| CuI at 100 days, % (95% CI) | 85 (53–96) | 88 (68–96) | 90 (81–95) | |
| RBC units at day +30, median (range) | 5 (0–23) | 4 (0–21) | 4 (0–23) | 0.31 |
| RBC units, day 31–90 *, median (range) | 4 (2–12) | 5 (2–16) | 5 (1–85) | 0.8 |
| PLT units at day +30, median (range) | 10 (5–70) | 6 (1–48) | 7 (2–69) | 0.12 |
| PLT units, day 31–90 *, median (range) | 6 (1–23) | 2 (1–57) | 10 (2–49) | 0.07 |
| Haploidentical | ||||
| Patients, n (%) | 7 (5) | 49 (35) | 84 (60) | |
| RCB transfusion independence | 0.097 | |||
| Days, median (range) | 29.5 (10–48) | 25.5 (0–290) | 21 (0–255) | |
| CuI at 100 days, % (95% CI) | 28 (4–61) | 67 (51–78) | 74 (63–82) | |
| PLT transfusion independence | 0.12 | |||
| Days, median (range) | 23 (6–35) | 26 (22–72) | 28 (0–169) | |
| CuI at 100 days, % (95% CI) | 28 (4–61) | 67 (52–78) | 84 (73–90) | |
| RBC units at day +30, median (range) | 10 (5–18) | 6 (0–23) | 5 (0–18) | 0.08 |
| RBC units, day 31–90 *, median (range) | 2 (2–2) | 6 (2–12) | 6 (0–79) | 0.15 |
| PLT units at day +30, median (range) | 14 (10–38) | 11 (3–30) | 8 (2–28) | 0.13 |
| PLT units, day 31–90 *, median (range) | 11 (1–12) | 10 (2–41) | 10 (2–124) | 0.3 |
| UCBT | ||||
| Patients, n (%) | 116 (52) | 91 (41) | 16 (7) | |
| RCB transfusion independence | 0.17 | |||
| Days, median (range) | 33 (0–240) | 28 (0–183) | 33 (0–200) | |
| CuI at 100 days, % (95% CI) | 63 (53–71) | 54 (44–64) | 73 (40–90) | |
| Platelet transfusion independence | 0.001 | |||
| Days, median (range) | 35 (0–175) | 34 (0–180) | 34 (0–60) | |
| CuI at 100 days, % (95% CI) | 73 (64–81) | 67 (56–75) | 93 (61–99) | |
| RBC units at day +30, median (range) | 6 (0–18) | 6 (0–39) | 5 (3–12) | 0.4 |
| RBC units, day 31–90 *, median (range) | 6 (3–29) | 6 (3–53) | 6 (3–12) | 0.8 |
| PLT units at day +30, median (range) | 16 (0–59) | 15 (0–85) | 11 (0–30) | 0.19 |
| PLT units, day 31–90 *, median (range) | 8 (1–98) | 6 (1–300) | 4 (1–50) | 0.48 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Solves, P.; Marco-Ayala, J.; Sanz, M.Á.; Gómez-Seguí, I.; Balaguer-Roselló, A.; Facal, A.; Villalba, M.; Montoro, J.; Sanz, G.; de la Rubia, J.; et al. Transfusion Burden in Allogeneic Hematopoietic Stem Cell Transplantation over Time: Experience from a Single Institution. J. Clin. Med. 2023, 12, 3467. https://doi.org/10.3390/jcm12103467
Solves P, Marco-Ayala J, Sanz MÁ, Gómez-Seguí I, Balaguer-Roselló A, Facal A, Villalba M, Montoro J, Sanz G, de la Rubia J, et al. Transfusion Burden in Allogeneic Hematopoietic Stem Cell Transplantation over Time: Experience from a Single Institution. Journal of Clinical Medicine. 2023; 12(10):3467. https://doi.org/10.3390/jcm12103467
Chicago/Turabian StyleSolves, Pilar, Javier Marco-Ayala, Miguel Ángel Sanz, Inés Gómez-Seguí, Aitana Balaguer-Roselló, Ana Facal, Marta Villalba, Juan Montoro, Guillermo Sanz, Javier de la Rubia, and et al. 2023. "Transfusion Burden in Allogeneic Hematopoietic Stem Cell Transplantation over Time: Experience from a Single Institution" Journal of Clinical Medicine 12, no. 10: 3467. https://doi.org/10.3390/jcm12103467