
What’s New in the Treatment of Non-Alcoholic Fatty Liver Disease (NAFLD)

 , ,
, , 
Abstract
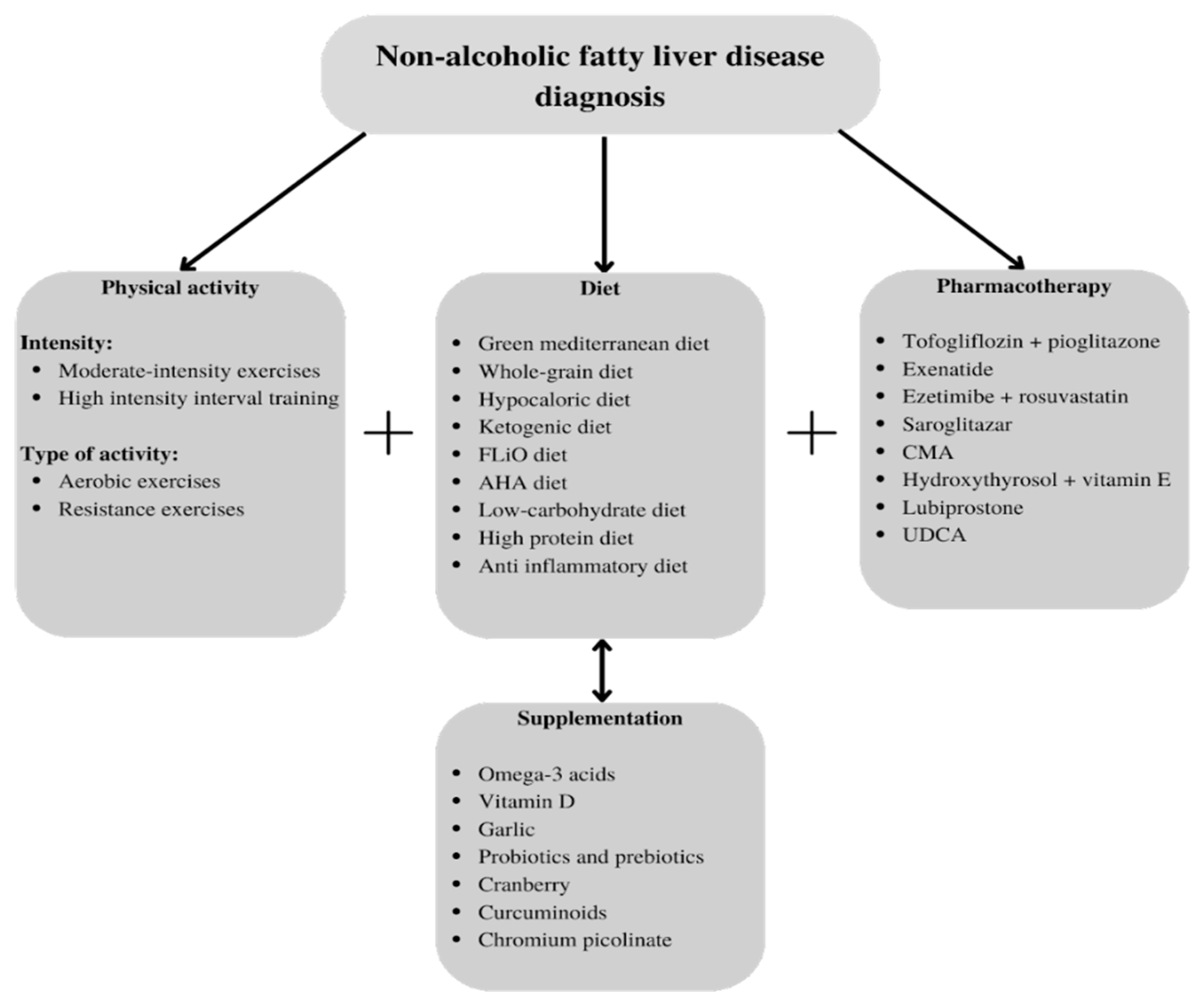
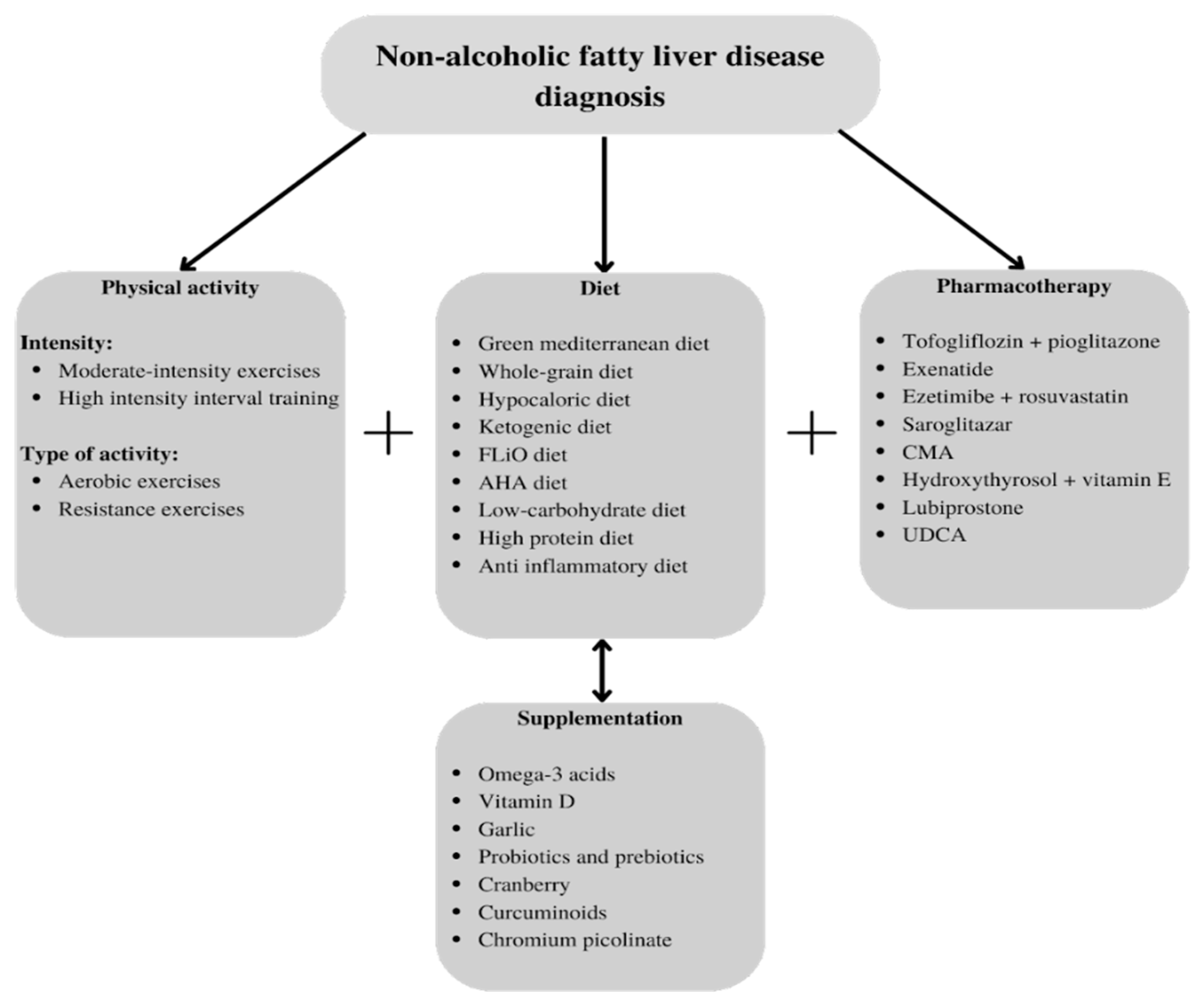
:1. Introduction
2. Materials and Methods
3. Results
3.1. Diet and Supplementation
3.2. Physical Activity
3.3. Pharmacotherapy
3.4. Surgeries and Overtures
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pervez, M.A.; Khan, D.A.; Mirza, S.A.; Slehria, A.U.R.; Nisar, U.; Aamir, M. Comparison of Delta-Tocotrienol and Alpha-Tocopherol Effects on Hepatic Steatosis and Inflammatory Biomarkers in Patients with Non-Alcoholic Fatty Liver Disease: A Randomized Double-Blind Active-Controlled Trial. Complement. Ther. Med. 2022, 70, 102866. [Google Scholar] [CrossRef] [PubMed]
- Kosmalski, M.; Ziółkowska, S.; Czarny, P.; Szemraj, J.; Pietras, T. The Coexistence of Nonalcoholic Fatty Liver Disease and Type 2 Diabetes Mellitus. J. Clin. Med. 2022, 11, 1375. [Google Scholar] [CrossRef] [PubMed]
- Tanase, D.M.; Gosav, E.M.; Costea, C.F.; Ciocoiu, M.; Lacatusu, C.M.; Maranduca, M.A.; Ouatu, A.; Floria, M. The Intricate Relationship between Type 2 Diabetes Mellitus (T2DM), Insulin Resistance (IR), and Nonalcoholic Fatty Liver Disease (NAFLD). J. Diabetes Res. 2020, 2020, 3920196. [Google Scholar] [CrossRef]
- Pantic, I.; Lugonja, S.; Rajovic, N.; Dumic, I.; Milovanovic, T. Colonic Diverticulosis and Non-Alcoholic Fatty Liver Disease: Is There a Connection? Medicina 2021, 58, 38. [Google Scholar] [CrossRef] [PubMed]
- Osorio-Conles, Ó.; Vega-Beyhart, A.; Ibarzabal, A.; Balibrea, J.M.; Graupera, I.; Rimola, J.; Vidal, J.; de Hollanda, A. A Distinctive NAFLD Signature in Adipose Tissue from Women with Severe Obesity. Int. J. Mol. Sci. 2021, 22, 10541. [Google Scholar] [CrossRef] [PubMed]
- Fahed, G.; Aoun, L.; Bou Zerdan, M.; Allam, S.; Bou Zerdan, M.; Bouferraa, Y.; Assi, H.I. Metabolic Syndrome: Updates on Pathophysiology and Management in 2021. Int. J. Mol. Sci. 2022, 23, 786. [Google Scholar] [CrossRef]
- Yamamura, S.; Eslam, M.; Kawaguchi, T.; Tsutsumi, T.; Nakano, D.; Yoshinaga, S.; Takahashi, H.; Anzai, K.; George, J.; Torimura, T. MAFLD Identifies Patients with Significant Hepatic Fibrosis Better than NAFLD. Liver Int. 2020, 40, 3018–3030. [Google Scholar] [CrossRef]
- Tang, A.; Ng, C.H.; Phang, P.H.; Chan, K.E.; Chin, Y.H.; Fu, C.E.; Zeng, R.W.; Xiao, J.; Tan, D.J.H.; Quek, J.; et al. Comparative Burden of Metabolic Dysfunction in Lean NAFLD vs Non-Lean NAFLD—A Systematic Review and Meta-Analysis. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2022, in press. [CrossRef]
- Calabrese, F.M.; Disciglio, V.; Franco, I.; Sorino, P.; Bonfiglio, C.; Bianco, A.; Campanella, A.; Lippolis, T.; Pesole, P.L.; Polignano, M.; et al. A Low Glycemic Index Mediterranean Diet Combined with Aerobic Physical Activity Rearranges the Gut Microbiota Signature in NAFLD Patients. Nutrients 2022, 14, 1773. [Google Scholar] [CrossRef]
- Newsome, P.N.; Sasso, M.; Deeks, J.J.; Paredes, A.; Boursier, J.; Chan, W.-K.; Yilmaz, Y.; Czernichow, S.; Zheng, M.-H.; Wong, V.W.-S.; et al. FibroScan-AST (FAST) Score for the Non-Invasive Identification of Patients with Non-Alcoholic Steatohepatitis with Significant Activity and Fibrosis: A Prospective Derivation and Global Validation Study. Lancet Gastroenterol. Hepatol. 2020, 5, 362–373. [Google Scholar] [CrossRef] [Green Version]
- Polyzos, S.A.; Mousiolis, A.; Mintziori, G.; Goulis, D.G. Nonalcoholic Fatty Liver Disease in Males with Low Testosterone Concentrations. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 1571–1577. [Google Scholar] [CrossRef] [PubMed]
- Pacheco, L.S.; Bradley, R.D.; Anderson, C.A.M.; Allison, M.A. Changes in Biomarkers of Non-Alcoholic Fatty Liver Disease (NAFLD) upon Access to Avocados in Hispanic/Latino Adults: Secondary Data Analysis of a Cluster Randomized Controlled Trial. Nutrients 2022, 14, 2744. [Google Scholar] [CrossRef] [PubMed]
- Ye, X.; Li, J.; Wang, H.; Wu, J. Pentraxin 3 and the TyG Index as Two Novel Markers to Diagnose NAFLD in Children. Dis. Markers 2021, 2021, 8833287. [Google Scholar] [CrossRef] [PubMed]
- Powell, E.E.; Wong, V.W.-S.; Rinella, M. Non-Alcoholic Fatty Liver Disease. Lancet 2021, 397, 2212–2224. [Google Scholar] [CrossRef] [PubMed]
- Caussy, C.; Aubin, A.; Loomba, R. The Relationship Between Type 2 Diabetes, NAFLD, and Cardiovascular Risk. Curr. Diabetes Rep. 2021, 21, 15. [Google Scholar] [CrossRef]
- Byrne, C.D.; Targher, G. NAFLD as a Driver of Chronic Kidney Disease. J. Hepatol. 2020, 72, 785–801. [Google Scholar] [CrossRef] [Green Version]
- Tao, G.; Zhang, G.; Chen, W.; Yang, C.; Xue, Y.; Song, G.; Qin, S. A Randomized, Placebo-controlled Clinical Trial of Hydrogen/Oxygen Inhalation for Non-alcoholic Fatty Liver Disease. J. Cell. Mol. Med. 2022, 26, 4113–4123. [Google Scholar] [CrossRef] [PubMed]
- Cheng, R.; Wang, L.; Le, S.; Yang, Y.; Zhao, C.; Zhang, X.; Yang, X.; Xu, T.; Xu, L.; Wiklund, P.; et al. A Randomized Controlled Trial for Response of Microbiome Network to Exercise and Diet Intervention in Patients with Nonalcoholic Fatty Liver Disease. Nat. Commun. 2022, 13, 2555. [Google Scholar] [CrossRef]
- Francque, S.M.; Marchesini, G.; Kautz, A.; Walmsley, M.; Dorner, R.; Lazarus, J.V.; Zelber-Sagi, S.; Hallsworth, K.; Busetto, L.; Frühbeck, G.; et al. Non-Alcoholic Fatty Liver Disease: A Patient Guideline. JHEP Rep. Innov. Hepatol. 2021, 3, 100322. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Ristic-Medic, D.; Kovacic, M.; Takic, M.; Arsic, A.; Petrovic, S.; Paunovic, M.; Jovicic, M.; Vucic, V. Calorie-Restricted Mediterranean and Low-Fat Diets Affect Fatty Acid Status in Individuals with Nonalcoholic Fatty Liver Disease. Nutrients 2020, 13, 15. [Google Scholar] [CrossRef]
- Cunha, G.M.; Guzman, G.; Correa De Mello, L.L.; Trein, B.; Spina, L.; Bussade, I.; Marques Prata, J.; Sajoux, I.; Countinho, W. Efficacy of a 2-Month Very Low-Calorie Ketogenic Diet (VLCKD) Compared to a Standard Low-Calorie Diet in Reducing Visceral and Liver Fat Accumulation in Patients With Obesity. Front. Endocrinol. 2020, 11, 607. [Google Scholar] [CrossRef]
- Crabtree, C.; Kackley, M.; Buga, A.; Fell, B.; LaFountain, R.; Hyde, P.; Sapper, T.; Kraemer, W.; Scandling, D.; Simonetti, O.; et al. Comparison of Ketogenic Diets with and without Ketone Salts versus a Low-Fat Diet: Liver Fat Responses in Overweight Adults. Nutrients 2021, 13, 966. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.L.; Johal, J.; Ong, K.W.; Han, C.Y.; Chan, Y.H.; Lee, Y.M.; Loo, W.M. Lifestyle Intervention Enabled by Mobile Technology on Weight Loss in Patients With Nonalcoholic Fatty Liver Disease: Randomized Controlled Trial. JMIR mHealth uHealth 2020, 8, e14802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yaskolka Meir, A.; Keller, M.; Müller, L.; Bernhart, S.H.; Tsaban, G.; Zelicha, H.; Rinott, E.; Kaplan, A.; Gepner, Y.; Shelef, I.; et al. Effects of Lifestyle Interventions on Epigenetic Signatures of Liver Fat: Central Randomized Controlled Trial. Liver Int. 2021, 41, 2101–2111. [Google Scholar] [CrossRef] [PubMed]
- Montemayor, S.; Mascaró, C.M.; Ugarriza, L.; Casares, M.; Llompart, I.; Abete, I.; Zulet, M.Á.; Martínez, J.A.; Tur, J.A.; Bouzas, C. Adherence to Mediterranean Diet and NAFLD in Patients with Metabolic Syndrome: The FLIPAN Study. Nutrients 2022, 14, 3186. [Google Scholar] [CrossRef]
- Campanella, A.; Iacovazzi, P.A.; Misciagna, G.; Bonfiglio, C.; Mirizzi, A.; Franco, I.; Bianco, A.; Sorino, P.; Caruso, M.G.; Cisternino, A.M.; et al. The Effect of Three Mediterranean Diets on Remnant Cholesterol and Non-Alcoholic Fatty Liver Disease: A Secondary Analysis. Nutrients 2020, 12, 1674. [Google Scholar] [CrossRef] [PubMed]
- Haigh, L.; Kirk, C.; El Gendy, K.; Gallacher, J.; Errington, L.; Mathers, J.C.; Anstee, Q.M. The Effectiveness and Acceptability of Mediterranean Diet and Calorie Restriction in Non-Alcoholic Fatty Liver Disease (NAFLD): A Systematic Review and Meta-Analysis. Clin. Nutr. 2022, 41, 1913–1931. [Google Scholar] [CrossRef]
- George, E.S.; Reddy, A.; Nicoll, A.J.; Ryan, M.C.; Itsiopoulos, C.; Abbott, G.; Johnson, N.A.; Sood, S.; Roberts, S.K.; Tierney, A.C. Impact of a Mediterranean Diet on Hepatic and Metabolic Outcomes in non-alcoholic Fatty Liver Disease: The MEDINA Randomised Controlled Trial. Liver Int. 2022, 42, 1308–1322. [Google Scholar] [CrossRef]
- Scragg, J.; Avery, L.; Cassidy, S.; Taylor, G.; Haigh, L.; Boyle, M.; Trenell, M.I.; Anstee, Q.M.; McPherson, S.; Hallsworth, K. Feasibility of a Very Low Calorie Diet to Achieve a Sustainable 10% Weight Loss in Patients With Nonalcoholic Fatty Liver Disease. Clin. Transl. Gastroenterol. 2020, 11, e00231. [Google Scholar] [CrossRef]
- Franco, I.; Bianco, A.; Mirizzi, A.; Campanella, A.; Bonfiglio, C.; Sorino, P.; Notarnicola, M.; Tutino, V.; Cozzolongo, R.; Giannuzzi, V.; et al. Physical Activity and Low Glycemic Index Mediterranean Diet: Main and Modification Effects on NAFLD Score. Results from a Randomized Clinical Trial. Nutrients 2020, 13, 66. [Google Scholar] [CrossRef]
- Xu, C.; Markova, M.; Seebeck, N.; Loft, A.; Hornemann, S.; Gantert, T.; Kabisch, S.; Herz, K.; Loske, J.; Ost, M.; et al. High-protein Diet More Effectively Reduces Hepatic Fat than Low-protein Diet despite Lower Autophagy and FGF21 Levels. Liver Int. 2020, 40, 2982–2997. [Google Scholar] [CrossRef]
- Haidari, F.; Hojhabrimanesh, A.; Helli, B.; Seyedian, S.-S.; Ahmadi-Angali, K. An Energy-Restricted High-Protein Diet Supplemented with β-Cryptoxanthin Alleviated Oxidative Stress and Inflammation in Nonalcoholic Fatty Liver Disease: A Randomized Controlled Trial. Nutr. Res. 2020, 73, 15–26. [Google Scholar] [CrossRef]
- Dorosti, M.; Jafary Heidarloo, A.; Bakhshimoghaddam, F.; Alizadeh, M. Whole-Grain Consumption and Its Effects on Hepatic Steatosis and Liver Enzymes in Patients with Non-Alcoholic Fatty Liver Disease: A Randomised Controlled Clinical Trial. Br. J. Nutr. 2020, 123, 328–336. [Google Scholar] [CrossRef] [PubMed]
- Kabisch, S.; Honsek, C.; Kemper, M.; Gerbracht, C.; Meyer, N.M.T.; Arafat, A.M.; Birkenfeld, A.L.; Machann, J.; Dambeck, U.; Osterhoff, M.A.; et al. Effects of Insoluble Cereal Fibre on Body Fat Distribution in the Optimal Fibre Trial. Mol. Nutr. Food Res. 2021, 65, 2000991. [Google Scholar] [CrossRef] [PubMed]
- Marin-Alejandre, B.A.; Cantero, I.; Perez-Diaz-del-Campo, N.; Monreal, J.I.; Elorz, M.; Herrero, J.I.; Benito-Boillos, A.; Quiroga, J.; Martinez-Echeverria, A.; Uriz-Otano, J.I.; et al. Effects of Two Personalized Dietary Strategies during a 2-year Intervention in Subjects with Nonalcoholic Fatty Liver Disease: A Randomized Trial. Liver Int. 2021, 41, 1532–1544. [Google Scholar] [CrossRef] [PubMed]
- Mohamad Nor, M.H.; Ayob, N.; Mokhtar, N.M.; Raja Ali, R.A.; Tan, G.C.; Wong, Z.; Shafiee, N.H.; Wong, Y.P.; Mustangin, M.; Nawawi, K.N.M. The Effect of Probiotics (MCP® BCMC® Strains) on Hepatic Steatosis, Small Intestinal Mucosal Immune Function, and Intestinal Barrier in Patients with Non-Alcoholic Fatty Liver Disease. Nutrients 2021, 13, 3192. [Google Scholar] [CrossRef]
- Sangouni, A.A.; Orang, Z.; Mozaffari-Khosravi, H. Effect of Omega-3 Supplementation on Fatty Liver and Visceral Adiposity Indices in Diabetic Patients with Non-Alcoholic Fatty Liver Disease: A Randomized Controlled Trial. Clin. Nutr. ESPEN 2021, 44, 130–135. [Google Scholar] [CrossRef]
- Green, C.J.; Pramfalk, C.; Charlton, C.A.; Gunn, P.J.; Cornfield, T.; Pavlides, M.; Karpe, F.; Hodson, L. Hepatic de Novo Lipogenesis Is Suppressed and Fat Oxidation Is Increased by Omega-3 Fatty Acids at the Expense of Glucose Metabolism. BMJ Open Diabetes Res. Care 2020, 8, e000871. [Google Scholar] [CrossRef] [Green Version]
- Cansanção, K.; Citelli, M.; Carvalho Leite, N.; López de las Hazas, M.-C.; Dávalos, A.; Tavares do Carmo, M.d.G.; Peres, W.A.F. Impact of Long-Term Supplementation with Fish Oil in Individuals with Non-Alcoholic Fatty Liver Disease: A Double Blind Randomized Placebo Controlled Clinical Trial. Nutrients 2020, 12, 3372. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.-F.; Wang, C.; Yang, T.; Ma, W.-J.; Zhai, J.; Zhao, T.; Xu, T.-C.; Li, J.; Liu, H.; Sinclair, A.J.; et al. Concentrated Fish Oil Ameliorates Non-Alcoholic Fatty Liver Disease by Regulating Fibroblast Growth Factor 21-Adiponectin Axis. Nutrition 2022, 99–100, 111659. [Google Scholar] [CrossRef] [PubMed]
- Song, L.; Zhao, X.G.; Ouyang, P.L.; Guan, Q.; Yang, L.; Peng, F.; Du, H.; Yin, F.; Yan, W.; Yu, W.J.; et al. Combined Effect of n -3 Fatty Acids and Phytosterol Esters on Alleviating Hepatic Steatosis in Non-Alcoholic Fatty Liver Disease Subjects: A Double-Blind Placebo-Controlled Clinical Trial. Br. J. Nutr. 2020, 123, 1148–1158. [Google Scholar] [CrossRef] [PubMed]
- Behrouz, V.; Aryaeian, N.; Zahedi, M.J.; Jazayeri, S. Effects of Probiotic and Prebiotic Supplementation on Metabolic Parameters, Liver Aminotransferases, and Systemic Inflammation in Nonalcoholic Fatty Liver Disease: A Randomized Clinical Trial. J. Food Sci. 2020, 85, 3611–3617. [Google Scholar] [CrossRef]
- Scorletti, E.; Afolabi, P.R.; Miles, E.A.; Smith, D.E.; Almehmadi, A.; Alshathry, A.; Childs, C.E.; Del Fabbro, S.; Bilson, J.; Moyses, H.E.; et al. Synbiotics Alter Fecal Microbiomes, But Not Liver Fat or Fibrosis, in a Randomized Trial of Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology 2020, 158, 1597–1610.e7. [Google Scholar] [CrossRef] [PubMed]
- Xue, L.; Deng, Z.; Luo, W.; He, X.; Chen, Y. Effect of Fecal Microbiota Transplantation on Non-Alcoholic Fatty Liver Disease: A Randomized Clinical Trial. Front. Cell. Infect. Microbiol. 2022, 12, 759306. [Google Scholar] [CrossRef]
- Yaghooti, H.; Ghanavati, F.; Seyedian, S.S.; Cheraghian, B.; Mohammadtaghvaei, N. The Efficacy of Calcitriol Treatment in Non-Alcoholic Fatty Liver Patients with Different Genotypes of Vitamin D Receptor FokI Polymorphism. BMC Pharmacol. Toxicol. 2021, 22, 18. [Google Scholar] [CrossRef]
- Mahmoudi, L.; Asadi, S.; Al-Mousavi, Z.; Niknam, R. A Randomized Controlled Clinical Trial Comparing Calcitriol versus Cholecalciferol Supplementation to Reduce Insulin Resistance in Patients with Non-Alcoholic Fatty Liver Disease. Clin. Nutr. 2021, 40, 2999–3005. [Google Scholar] [CrossRef]
- Zanko, V.L.; Domislovic, V.; Trkulja, V.; Krznaric-Zrnic, I.; Turk-Wensveen, T.; Krznaric, Z.; Kanizaj, T.F.; Radic-Kristo, D.; Bilic-Zulle, L.; Orlic, L.; et al. Vitamin D for Treatment of Non-alcoholic Fatty Liver Disease Detected by Transient Elastography: A Randomized, Double-blind, Placebo-controlled Trial. Diabetes Obes. Metab. 2020, 22, 2097–2106. [Google Scholar] [CrossRef]
- Rahimpour, Z.; Hoseini, R.; Behpour, N. Alterations of Liver Enzymes and Lipid Profile in Response to Exhaustive Eccentric Exercise: Vitamin D Supplementation Trial in Overweight Females with Non-Alcoholic Fatty Liver Disease. BMC Gastroenterol. 2022, 22, 372. [Google Scholar] [CrossRef]
- Tutunchi, H.; Ostadrahimi, A.; Saghafi-Asl, M.; Hosseinzadeh-Attar, M.-J.; Shakeri, A.; Asghari-Jafarabadi, M.; Roshanravan, N.; Farrin, N.; Naemi, M.; Hasankhani, M. Oleoylethanolamide Supplementation in Obese Patients Newly Diagnosed with Non-Alcoholic Fatty Liver Disease: Effects on Metabolic Parameters, Anthropometric Indices, and Expression of PPAR-α, UCP1, and UCP2 Genes. Pharmacol. Res. 2020, 156, 104770. [Google Scholar] [CrossRef]
- Medina-Urrutia, A.; Lopez-Uribe, A.R.; El Hafidi, M.; González-Salazar, M.d.C.; Posadas-Sánchez, R.; Jorge-Galarza, E.; del Valle-Mondragón, L.; Juárez-Rojas, J.G. Chia (Salvia Hispanica)-Supplemented Diet Ameliorates Non-Alcoholic Fatty Liver Disease and Its Metabolic Abnormalities in Humans. Lipids Health Dis. 2020, 19, 96. [Google Scholar] [CrossRef] [PubMed]
- Sangouni, A.A.; Azar, M.R.M.H.; Alizadeh, M. Effect of Garlic Powder Supplementation on Hepatic Steatosis, Liver Enzymes and Lipid Profile in Patients with Non-Alcoholic Fatty Liver Disease: A Double-Blind Randomised Controlled Clinical Trial. Br. J. Nutr. 2020, 124, 450–456. [Google Scholar] [CrossRef] [Green Version]
- Sangouni, A.A.; Alizadeh, M.; Jamalzehi, A.; Parastouei, K. Effects of Garlic Powder Supplementation on Metabolic Syndrome Components, Insulin Resistance, Fatty Liver Index, and Appetite in Subjects with Metabolic Syndrome: A Randomized Clinical Trial. Phytother. Res. 2021, 35, 4433–4441. [Google Scholar] [CrossRef] [PubMed]
- Kruse, M.; Kemper, M.; Gancheva, S.; Osterhoff, M.; Dannenberger, D.; Markgraf, D.; Machann, J.; Hierholzer, J.; Roden, M.; Pfeiffer, A.F.H. Dietary Rapeseed Oil Supplementation Reduces Hepatic Steatosis in Obese Men—A Randomized Controlled Trial. Mol. Nutr. Food Res. 2020, 64, 2000419. [Google Scholar] [CrossRef] [PubMed]
- Atefi, M.; Entezari, M.H.; Vahedi, H.; Hassanzadeh, A. Sesame Oil Ameliorates Alanine Aminotransferase, Aspartate Aminotransferase, and Fatty Liver Grade in Women with Nonalcoholic Fatty Liver Disease Undergoing Low-Calorie Diet: A Randomized Double-Blind Controlled Trial. Int. J. Clin. Pract. 2022, 2022, 4982080. [Google Scholar] [CrossRef] [PubMed]
- Masnadi Shirazi, K.; Shirinpour, E.; Masnadi Shirazi, A.; Nikniaz, Z. Effect of Cranberry Supplementation on Liver Enzymes and Cardiometabolic Risk Factors in Patients with NAFLD: A Randomized Clinical Trial. BMC Complement. Med. Ther. 2021, 21, 283. [Google Scholar] [CrossRef]
- Hormoznejad, R.; Mohammad Shahi, M.; Rahim, F.; Helli, B.; Alavinejad, P.; Sharhani, A. Combined Cranberry Supplementation and Weight Loss Diet in Non-Alcoholic Fatty Liver Disease: A Double-Blind Placebo-Controlled Randomized Clinical Trial. Int. J. Food Sci. Nutr. 2020, 71, 991–1000. [Google Scholar] [CrossRef]
- Goodarzi, R.; Jafarirad, S.; Mohammadtaghvaei, N.; Dastoorpoor, M.; Alavinejad, P. The Effect of Pomegranate Extract on Anthropometric Indices, Serum Lipids, Glycemic Indicators, and Blood Pressure in Patients with Nonalcoholic Fatty Liver Disease: A Randomized Double-blind Clinical Trial. Phytother. Res. 2021, 35, 5871–5882. [Google Scholar] [CrossRef] [PubMed]
- Namkhah, Z.; Naeini, F.; Rezayat, S.M.; Yaseri, M.; Mansouri, S.; Hosseinzadeh-Attar, M.J. Does Naringenin Supplementation Improve Lipid Profile, Severity of Hepatic Steatosis and Probability of Liver Fibrosis in Overweight/Obese Patients with NAFLD? A Randomised, Double-blind, Placebo-controlled, Clinical Trial. Int. J. Clin. Pract. 2021, 75, e14852. [Google Scholar] [CrossRef] [PubMed]
- Yari, Z.; Cheraghpour, M.; Alavian, S.M.; Hedayati, M.; Eini-Zinab, H.; Hekmatdoost, A. The Efficacy of Flaxseed and Hesperidin on Non-Alcoholic Fatty Liver Disease: An Open-Labeled Randomized Controlled Trial. Eur. J. Clin. Nutr. 2021, 75, 99–111. [Google Scholar] [CrossRef]
- Saberi-Karimian, M.; Keshvari, M.; Ghayour-Mobarhan, M.; Salehizadeh, L.; Rahmani, S.; Behnam, B.; Jamialahmadi, T.; Asgary, S.; Sahebkar, A. Effects of Curcuminoids on Inflammatory Status in Patients with Non-Alcoholic Fatty Liver Disease: A Randomized Controlled Trial. Complement. Ther. Med. 2020, 49, 102322. [Google Scholar] [CrossRef]
- Mirhafez, S.R.; Azimi-Nezhad, M.; Dehabeh, M.; Hariri, M.; Naderan, R.D.; Movahedi, A.; Abdalla, M.; Sathyapalan, T.; Sahebkar, A. The Effect of Curcumin Phytosome on the Treatment of Patients with Non-Alcoholic Fatty Liver Disease: A Double-Blind, Randomized, Placebo-Controlled Trial. In Pharmacological Properties of Plant-Derived Natural Products and Implications for Human Health; Barreto, G.E., Sahebkar, A., Eds.; Advances in Experimental Medicine and Biology; Springer International Publishing: Cham, Switzerland, 2021; Volume 1308, pp. 25–35. ISBN 978-3-030-64871-8. [Google Scholar]
- Cicero, A.F.G.; Sahebkar, A.; Fogacci, F.; Bove, M.; Giovannini, M.; Borghi, C. Effects of Phytosomal Curcumin on Anthropometric Parameters, Insulin Resistance, Cortisolemia and Non-Alcoholic Fatty Liver Disease Indices: A Double-Blind, Placebo-Controlled Clinical Trial. Eur. J. Nutr. 2020, 59, 477–483. [Google Scholar] [CrossRef] [Green Version]
- Kelardeh, B.M.; Rahmati-Ahmadabad, S.; Farzanegi, P.; Helalizadeh, M.; Azarbayjani, M.-A. Effects of Non-Linear Resistance Training and Curcumin Supplementation on the Liver Biochemical Markers Levels and Structure in Older Women with Non-Alcoholic Fatty Liver Disease. J. Bodyw. Mov. Ther. 2020, 24, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Tutunchi, H.; Ostadrahimi, A.; Saghafi-Asl, M.; Roshanravan, N.; Shakeri-Bavil, A.; Asghari-Jafarabadi, M.; Farrin, N.; Mobasseri, M. Expression of NF-κB, IL-6, and IL-10 Genes, Body Composition, and Hepatic Fibrosis in Obese Patients with NAFLD—Combined Effects of Oleoylethanolamide Supplementation and Calorie Restriction: A Triple-blind Randomized Controlled Clinical Trial. J. Cell. Physiol. 2021, 236, 417–426. [Google Scholar] [CrossRef] [PubMed]
- Amerikanou, C.; Kanoni, S.; Kaliora, A.C.; Barone, A.; Bjelan, M.; D’Auria, G.; Gioxari, A.; Gosalbes, M.J.; Mouchti, S.; Stathopoulou, M.G.; et al. Effect of Mastiha Supplementation on NAFLD: The MAST4HEALTH Randomised, Controlled Trial. Mol. Nutr. Food Res. 2021, 65, 2001178. [Google Scholar] [CrossRef]
- Amerikanou, C.; Papada, E.; Gioxari, A.; Smyrnioudis, I.; Kleftaki, S.-A.; Valsamidou, E.; Bruns, V.; Banerjee, R.; Trivella, M.G.; Milic, N.; et al. Mastiha Has Efficacy in Immune-Mediated Inflammatory Diseases through a MicroRNA-155 Th17 Dependent Action. Pharmacol. Res. 2021, 171, 105753. [Google Scholar] [CrossRef]
- Kanoni, S.; Kumar, S.; Amerikanou, C.; Kurth, M.J.; Stathopoulou, M.G.; Bourgeois, S.; Masson, C.; Kannt, A.; Cesarini, L.; Kontoe, M.-S.; et al. Nutrigenetic Interactions Might Modulate the Antioxidant and Anti-Inflammatory Status in Mastiha-Supplemented Patients With NAFLD. Front. Immunol. 2021, 12, 683028. [Google Scholar] [CrossRef] [PubMed]
- Izadi, F.; Farrokhzad, A.; Tamizifar, B.; Tarrahi, M.J.; Entezari, M.H. Effect of Sour Tea Supplementation on Liver Enzymes, Lipid Profile, Blood Pressure, and Antioxidant Status in Patients with Non-alcoholic Fatty Liver Disease: A Double-blind Randomized Controlled Clinical Trial. Phytother. Res. 2021, 35, 477–485. [Google Scholar] [CrossRef]
- Hosseinabadi, S.; Rafraf, M.; Asghari, S.; Asghari-Jafarabadi, M.; Vojouhi, S. Effect of Green Coffee Extract Supplementation on Serum Adiponectin Concentration and Lipid Profile in Patients with Non-Alcoholic Fatty Liver Disease: A Randomized, Controlled Trial. Complement. Ther. Med. 2020, 49, 102290. [Google Scholar] [CrossRef]
- Pervez, M.A.; Khan, D.A.; Slehria, A.U.R.; Ijaz, A. Delta-Tocotrienol Supplementation Improves Biochemical Markers of Hepatocellular Injury and Steatosis in Patients with Nonalcoholic Fatty Liver Disease: A Randomized, Placebo-Controlled Trial. Complement. Ther. Med. 2020, 52, 102494. [Google Scholar] [CrossRef]
- Majnooni, M.B.; Ataee, M.; Bahrami, G.; Heydarpour, F.; Aneva, I.Y.; Farzaei, M.H.; Ahmadi-Juoibari, T. The Effects of Co-administration of Artichoke Leaf Extract Supplementation with Metformin and Vitamin E in Patients with Nonalcoholic Fatty Liver Disease: A Randomized Clinical Trial. Phytother. Res. 2021, 35, 6324–6334. [Google Scholar] [CrossRef]
- Soleimani, D.; Rezaie, M.; Rajabzadeh, F.; Gholizadeh Navashenaq, J.; Abbaspour, M.; Miryan, M.; Razmpour, F.; Ranjbar, G.; Rezvani, R.; Jarahi, L.; et al. Protective Effects of Propolis on Hepatic Steatosis and Fibrosis among Patients with Nonalcoholic Fatty Liver Disease (NAFLD) Evaluated by Real-time Two-dimensional Shear Wave Elastography: A Randomized Clinical Trial. Phytother. Res. 2021, 35, 1669–1679. [Google Scholar] [CrossRef] [PubMed]
- Kazemi, S.; Shidfar, F.; Ehsani, S.; Adibi, P.; Janani, L.; Eslami, O. The Effects of Sumac (Rhus coriaria L.) Powder Supplementation in Patients with Non-Alcoholic Fatty Liver Disease: A Randomized Controlled Trial. Complement. Ther. Clin. Pract. 2020, 41, 101259. [Google Scholar] [CrossRef] [PubMed]
- Jinato, T.; Chayanupatkul, M.; Dissayabutra, T.; Chutaputti, A.; Tangkijvanich, P.; Chuaypen, N. Litchi-Derived Polyphenol Alleviates Liver Steatosis and Gut Dysbiosis in Patients with Non-Alcoholic Fatty Liver Disease: A Randomized Double-Blinded, Placebo-Controlled Study. Nutrients 2022, 14, 2921. [Google Scholar] [CrossRef]
- Ferro, Y.; Pujia, R.; Mazza, E.; Lascala, L.; Lodari, O.; Maurotti, S.; Pujia, A.; Montalcini, T. A New Nutraceutical (Livogen Plus®) Improves Liver Steatosis in Adults with Non-Alcoholic Fatty Liver Disease. J. Transl. Med. 2022, 20, 377. [Google Scholar] [CrossRef]
- Ferro, Y.; Montalcini, T.; Mazza, E.; Foti, D.; Angotti, E.; Gliozzi, M.; Nucera, S.; Paone, S.; Bombardelli, E.; Aversa, I.; et al. Randomized Clinical Trial: Bergamot Citrus and Wild Cardoon Reduce Liver Steatosis and Body Weight in Non-Diabetic Individuals Aged Over 50 Years. Front. Endocrinol. 2020, 11, 494. [Google Scholar] [CrossRef] [PubMed]
- Fathi, M.; Alavinejad, P.; Haidari, Z.; Amani, R. The Effects of Zinc Supplementation on Metabolic Profile and Oxidative Stress in Overweight/Obese Patients with Non-Alcoholic Fatty Liver Disease: A Randomized, Double-Blind, Placebo-Controlled Trial. J. Trace Elem. Med. Biol. 2020, 62, 126635. [Google Scholar] [CrossRef] [PubMed]
- Fathi, M.; Alavinejad, P.; Haidari, Z.; Amani, R. The Effect of Zinc Supplementation on Steatosis Severity and Liver Function Enzymes in Overweight/Obese Patients with Mild to Moderate Non-Alcoholic Fatty Liver Following Calorie-Restricted Diet: A Double-Blind, Randomized Placebo-Controlled Trial. Biol. Trace Elem. Res. 2020, 197, 394–404. [Google Scholar] [CrossRef]
- Kavianipour, F.; Aryaeian, N.; Mokhtare, M.; Mirnasrollahiparsa, R.; Jannani, L.; Agah, S.; Fallah, S.; Moradi, N. The Effect of Saffron Supplementation on Some Inflammatory and Oxidative Markers, Leptin, Adiponectin, and Body Composition in Patients with Nonalcoholic Fatty Liver Disease: A Double-blind Randomized Clinical Trial. Phytother. Res. 2020, 34, 3367–3378. [Google Scholar] [CrossRef]
- Moradi, F.; Kooshki, F.; Nokhostin, F.; Khoshbaten, M.; Bazyar, H.; Pourghassem Gargari, B. A Pilot Study of the Effects of Chromium Picolinate Supplementation on Serum Fetuin-A, Metabolic and Inflammatory Factors in Patients with Nonalcoholic Fatty Liver Disease: A Double-Blind, Placebo-Controlled Trial. J. Trace Elem. Med. Biol. 2021, 63, 126659. [Google Scholar] [CrossRef]
- Cohen, C.C.; Li, K.W.; Alazraki, A.L.; Beysen, C.; Carrier, C.A.; Cleeton, R.L.; Dandan, M.; Figueroa, J.; Knight-Scott, J.; Knott, C.J.; et al. Dietary Sugar Restriction Reduces Hepatic de Novo Lipogenesis in Adolescent Boys with Fatty Liver Disease. J. Clin. Investig. 2021, 131, e150996. [Google Scholar] [CrossRef] [PubMed]
- Medrano, M.; Arenaza, L.; Migueles, J.H.; Rodríguez-Vigil, B.; Ruiz, J.R.; Labayen, I. Associations of Physical Activity and Fitness with Hepatic Steatosis, Liver Enzymes, and Insulin Resistance in Children with Overweight/Obesity. Pediatr. Diabetes 2020, 21, 565–574. [Google Scholar] [CrossRef] [PubMed]
- Mascaró, C.M.; Bouzas, C.; Montemayor, S.; Casares, M.; Llompart, I.; Ugarriza, L.; Borràs, P.-A.; Martínez, J.A.; Tur, J.A. Effect of a Six-Month Lifestyle Intervention on the Physical Activity and Fitness Status of Adults with NAFLD and Metabolic Syndrome. Nutrients 2022, 14, 1813. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, A.; Abe, K.; Fujita, M.; Hayashi, M.; Okai, K.; Ohira, H. Simple Resistance Exercise Decreases Cytokeratin 18 and Fibroblast Growth Factor 21 Levels in Patients with Nonalcoholic Fatty Liver Disease: A Retrospective Clinical Study. Medicine 2020, 99, e20399. [Google Scholar] [CrossRef]
- Babu, A.F.; Csader, S.; Männistö, V.; Tauriainen, M.-M.; Pentikäinen, H.; Savonen, K.; Klåvus, A.; Koistinen, V.; Hanhineva, K.; Schwab, U. Effects of Exercise on NAFLD Using Non-Targeted Metabolomics in Adipose Tissue, Plasma, Urine, and Stool. Sci. Rep. 2022, 12, 6485. [Google Scholar] [CrossRef]
- Saldiran, T.Ç.; Mutluay, F.K.; Yağci, İ.; Yilmaz, Y. Impact of Aerobic Training with and without Whole-Body Vibration Training on Metabolic Features and Quality of Life in Non-Alcoholic Fatty Liver Disease Patients. Ann. Endocrinol. 2020, 81, 493–499. [Google Scholar] [CrossRef]
- Charatcharoenwitthaya, P.; Kuljiratitikal, K.; Aksornchanya, O.; Chaiyasoot, K.; Bandidniyamanon, W.; Charatcharoenwitthaya, N. Moderate-Intensity Aerobic vs Resistance Exercise and Dietary Modification in Patients With Nonalcoholic Fatty Liver Disease: A Randomized Clinical Trial. Clin. Transl. Gastroenterol. 2021, 12, e00316. [Google Scholar] [CrossRef]
- Draz, R.S.; Serry, Z.M.; Rahmy, A.F.; El Bardesi, M.S.; Taha, M.M. Electroacupuncture Versus Aerobic Interval Training on Liver Functions in Patients with Nonalcoholic Fatty Liver. J. Altern. Complement. Med. 2020, 26, 51–57. [Google Scholar] [CrossRef]
- Iwanaga, S.; Hashida, R.; Takano, Y.; Bekki, M.; Nakano, D.; Omoto, M.; Nago, T.; Kawaguchi, T.; Matsuse, H.; Torimura, T.; et al. Hybrid Training System Improves Insulin Resistance in Patients with Nonalcoholic Fatty Liver Disease: A Randomized Controlled Pilot Study. Tohoku J. Exp. Med. 2020, 252, 23–32. [Google Scholar] [CrossRef]
- Abdelbasset, W.K.; Tantawy, S.A.; Kamel, D.M.; Alqahtani, B.A.; Elnegamy, T.E.; Soliman, G.S.; Ibrahim, A.A. Effects of High-Intensity Interval and Moderate-Intensity Continuous Aerobic Exercise on Diabetic Obese Patients with Nonalcoholic Fatty Liver Disease: A Comparative Randomized Controlled Trial. Medicine 2020, 99, e19471. [Google Scholar] [CrossRef]
- Whyte, M.B.; Shojaee-Moradie, F.; Sharaf, S.E.; Cuthbertson, D.J.; Kemp, G.J.; Barrett, M.; Jackson, N.C.; Herring, R.A.; Wright, J.; Thomas, E.L.; et al. HDL-ApoA-I Kinetics in Response to 16 Wk of Exercise Training in Men with Nonalcoholic Fatty Liver Disease. Am. J. Physiol. Endocrinol. Metab. 2020, 318, E839–E847. [Google Scholar] [CrossRef] [PubMed]
- Milovanovic, T.; Pantic, I.; Dragasevic, S.; Lugonja, S.; Dumic, I.; Rajilic-Stojanovic, M. The Interrelationship Among Non-Alcoholic Fatty Liver Disease, Colonic Diverticulosis and Metabolic Syndrome. J. Gastrointestin. Liver Dis. 2021, 30, 274–282. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.; Lee, H.; Ji, S.; Yoon, S.H.; Cho, J.; Chung, J. Pharmacokinetics and Pharmacodynamics of Ursodeoxycholic Acid in an Overweight Population With Abnormal Liver Function. Clin. Pharmacol. Drug Dev. 2021, 10, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Mosca, A.; Crudele, A.; Smeriglio, A.; Braghini, M.R.; Panera, N.; Comparcola, D.; Alterio, A.; Sartorelli, M.R.; Tozzi, G.; Raponi, M.; et al. Antioxidant Activity of Hydroxytyrosol and Vitamin E Reduces Systemic Inflammation in Children with Paediatric NAFLD. Dig. Liver Dis. 2021, 53, 1154–1158. [Google Scholar] [CrossRef] [PubMed]
- Kedarisetty, C.K.; Bhardwaj, A.; Kumar, G.; Rastogi, A.; Bihari, C.; Kumar, M.; Sarin, S.K. Efficacy of Combining Pentoxiphylline and Vitamin E versus Vitamin E Alone in Non-Alcoholic Steatohepatitis— A Randomized Pilot Study. Indian J. Gastroenterol. 2021, 40, 41–49. [Google Scholar] [CrossRef]
- Civelek, M.; Podszun, M.C. Genetic Factors Associated with Response to Vitamin E Treatment in NAFLD. Antioxidants 2022, 11, 1284. [Google Scholar] [CrossRef]
- Panera, N.; Braghini, M.R.; Crudele, A.; Smeriglio, A.; Bianchi, M.; Condorelli, A.G.; Nobili, R.; Conti, L.A.; De Stefanis, C.; Lioci, G.; et al. Combination Treatment with Hydroxytyrosol and Vitamin E Improves NAFLD-Related Fibrosis. Nutrients 2022, 14, 3791. [Google Scholar] [CrossRef]
- Zeybel, M.; Altay, O.; Arif, M.; Li, X.; Yang, H.; Fredolini, C.; Akyildiz, M.; Saglam, B.; Gonenli, M.G.; Ural, D.; et al. Combined Metabolic Activators Therapy Ameliorates Liver Fat in Nonalcoholic Fatty Liver Disease Patients. Mol. Syst. Biol. 2021, 17, e10459. [Google Scholar] [CrossRef]
- Saneian, H.; Khalilian, L.; Heidari-Beni, M.; Khademian, M.; Famouri, F.; Nasri, P.; Hassanzadeh, A.; Kelishadi, R. Effect of L-Carnitine Supplementation on Children and Adolescents with Nonalcoholic Fatty Liver Disease (NAFLD): A Randomized, Triple-Blind, Placebo-Controlled Clinical Trial. J. Pediatr. Endocrinol. Metab. 2021, 34, 897–904. [Google Scholar] [CrossRef]
- Sangouni, A.A.; Sasanfar, B.; Ghadiri-Anari, A.; Hosseinzadeh, M. Effect of L-Carnitine Supplementation on Liver Fat Content and Cardiometabolic Indices in Overweight/Obese Women with Polycystic Ovary Syndrome: A Randomized Controlled Trial. Clin. Nutr. ESPEN 2021, 46, 54–59. [Google Scholar] [CrossRef]
- Harrison, S.A.; Baum, S.J.; Gunn, N.T.; Younes, Z.H.; Kohli, A.; Patil, R.; Koziel, M.J.; Chera, H.; Zhao, J.; Chakravarthy, M.V. Safety, Tolerability, and Biologic Activity of AXA1125 and AXA1957 in Subjects With Nonalcoholic Fatty Liver Disease. Am. J. Gastroenterol. 2021, 116, 2399–2409. [Google Scholar] [CrossRef]
- Kinoshita, T.; Shimoda, M.; Nakashima, K.; Fushimi, Y.; Hirata, Y.; Tanabe, A.; Tatsumi, F.; Hirukawa, H.; Sanada, J.; Kohara, K.; et al. Comparison of the Effects of Three Kinds of Glucose-lowering Drugs on Non-alcoholic Fatty Liver Disease in Patients with Type 2 Diabetes: A Randomized, Open-label, Three-arm, Active Control Study. J. Diabetes Investig. 2020, 11, 1612–1622. [Google Scholar] [CrossRef]
- Yoneda, M.; Honda, Y.; Ogawa, Y.; Kessoku, T.; Kobayashi, T.; Imajo, K.; Ozaki, A.; Nogami, A.; Taguri, M.; Yamanaka, T.; et al. Comparing the Effects of Tofogliflozin and Pioglitazone in Non-Alcoholic Fatty Liver Disease Patients with Type 2 Diabetes Mellitus (ToPiND Study): A Randomized Prospective Open-Label Controlled Trial. BMJ Open Diabetes Res. Care 2021, 9, e001990. [Google Scholar] [CrossRef]
- Takahashi, H.; Kessoku, T.; Kawanaka, M.; Nonaka, M.; Hyogo, H.; Fujii, H.; Nakajima, T.; Imajo, K.; Tanaka, K.; Kubotsu, Y.; et al. Ipragliflozin Improves the Hepatic Outcomes of Patients With Diabetes with NAFLD. Hepatol. Commun. 2022, 6, 120–132. [Google Scholar] [CrossRef]
- Phrueksotsai, S.; Pinyopornpanish, K.; Euathrongchit, J.; Leerapun, A.; Phrommintikul, A.; Buranapin, S.; Chattipakorn, N.; Thongsawat, S. The Effects of Dapagliflozin on Hepatic and Visceral Fat in Type 2 Diabetes Patients with Non-alcoholic Fatty Liver Disease. J. Gastroenterol. Hepatol. 2021, 36, 2952–2959. [Google Scholar] [CrossRef]
- Taheri, H.; Malek, M.; Ismail-Beigi, F.; Zamani, F.; Sohrabi, M.; Babaei, M.R.; Khamseh, M.E. Effect of Empagliflozin on Liver Steatosis and Fibrosis in Patients with Non-Alcoholic Fatty Liver Disease Without Diabetes: A Randomized, Double-Blind, Placebo-Controlled Trial. Adv. Ther. 2020, 37, 4697–4708. [Google Scholar] [CrossRef]
- Kahl, S.; Gancheva, S.; Straßburger, K.; Herder, C.; Machann, J.; Katsuyama, H.; Kabisch, S.; Henkel, E.; Kopf, S.; Lagerpusch, M.; et al. Empagliflozin Effectively Lowers Liver Fat Content in Well-Controlled Type 2 Diabetes: A Randomized, Double-Blind, Phase 4, Placebo-Controlled Trial. Diabetes Care 2020, 43, 298–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, K.Y.; Nakamura, A.; Omori, K.; Takase, T.; Miya, A.; Yamamoto, K.; Nomoto, H.; Kameda, H.; Taneda, S.; Kurihara, Y.; et al. Favorable Effect of Sodium–Glucose Cotransporter 2 Inhibitor, Dapagliflozin, on Non-alcoholic Fatty Liver Disease Compared with Pioglitazone. J. Diabetes Investig. 2021, 12, 1272–1277. [Google Scholar] [CrossRef] [PubMed]
- Della Pepa, G.; Russo, M.; Vitale, M.; Carli, F.; Vetrani, C.; Masulli, M.; Riccardi, G.; Vaccaro, O.; Gastaldelli, A.; Rivellese, A.A.; et al. Pioglitazone Even at Low Dosage Improves NAFLD in Type 2 Diabetes: Clinical and Pathophysiological Insights from a Subgroup of the TOSCA.IT Randomised Trial. Diabetes Res. Clin. Pract. 2021, 178, 108984. [Google Scholar] [CrossRef] [PubMed]
- Yan, H.; Wu, W.; Chang, X.; Xia, M.; Ma, S.; Wang, L.; Gao, J. Gender Differences in the Efficacy of Pioglitazone Treatment in Nonalcoholic Fatty Liver Disease Patients with Abnormal Glucose Metabolism. Biol. Sex Differ. 2021, 12, 1. [Google Scholar] [CrossRef] [PubMed]
- Yoneda, M.; Kobayashi, T.; Honda, Y.; Ogawa, Y.; Kessoku, T.; Imajo, K.; Nogami, A.; Taguri, M.; Kirikoshi, H.; Saito, S.; et al. Combination of Tofogliflozin and Pioglitazone for NAFLD: Extension to the ToPiND Randomized Controlled Trial. Hepatol. Commun. 2022, 6, 2273–2285. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Zhao, B.; Sun, H.; You, H.; Qu, S. Effects of Sitagliptin on Intrahepatic Lipid Content in Patients with Non-Alcoholic Fatty Liver Disease. Front. Endocrinol. 2022, 13, 866189. [Google Scholar] [CrossRef] [PubMed]
- Seo, H.-Y.; Lee, S.-H.; Han, E.; Hwang, J.S.; Han, S.; Kim, M.K.; Jang, B.K. Evogliptin Directly Inhibits Inflammatory and Fibrotic Signaling in Isolated Liver Cells. Int. J. Mol. Sci. 2022, 23, 11636. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Yan, H.; Xia, M.; Zhao, L.; Lv, M.; Zhao, N.; Rao, S.; Yao, X.; Wu, W.; Pan, B.; et al. Efficacy of Exenatide and Insulin Glargine on Nonalcoholic Fatty Liver Disease in Patients with Type 2 Diabetes. Diabetes Metab. Res. Rev. 2020, 36, e3292. [Google Scholar] [CrossRef]
- Flint, A.; Andersen, G.; Hockings, P.; Johansson, L.; Morsing, A.; Palle, M.S.; Vogl, T.; Loomba, R.; Plum-Mörschel, L. Randomised Clinical Trial: Semaglutide versus Placebo Reduced Liver Steatosis but Not Liver Stiffness in Subjects with Non-alcoholic Fatty Liver Disease Assessed by Magnetic Resonance Imaging. Aliment. Pharmacol. Ther. 2021, 54, 1150–1161. [Google Scholar] [CrossRef]
- Kuchay, M.S.; Krishan, S.; Mishra, S.K.; Choudhary, N.S.; Singh, M.K.; Wasir, J.S.; Kaur, P.; Gill, H.K.; Bano, T.; Farooqui, K.J.; et al. Effect of Dulaglutide on Liver Fat in Patients with Type 2 Diabetes and NAFLD: Randomised Controlled Trial (D-LIFT Trial). Diabetologia 2020, 63, 2434–2445. [Google Scholar] [CrossRef]
- Xiao, Y.; Liu, Y.; Zhao, L.; Zhou, Y. Effect of 5:2 Fasting Diet on Liver Fat Content in Patients with Type 2 Diabetic with Nonalcoholic Fatty Liver Disease. Metab. Syndr. Relat. Disord. 2022, 20, 459–465. [Google Scholar] [CrossRef]
- Zhang, L.-Y.; Qu, X.-N.; Sun, Z.-Y.; Zhang, Y. Effect of Liraglutide Therapy on Serum Fetuin A in Patients with Type 2 Diabetes and Non-Alcoholic Fatty Liver Disease. Clin. Res. Hepatol. Gastroenterol. 2020, 44, 674–680. [Google Scholar] [CrossRef]
- Guo, W.; Tian, W.; Lin, L.; Xu, X. Liraglutide or Insulin Glargine Treatments Improves Hepatic Fat in Obese Patients with Type 2 Diabetes and Nonalcoholic Fatty Liver Disease in Twenty-Six Weeks: A Randomized Placebo-Controlled Trial. Diabetes Res. Clin. Pract. 2020, 170, 108487. [Google Scholar] [CrossRef]
- Harreiter, J.; Just, I.; Leutner, M.; Bastian, M.; Brath, H.; Schelkshorn, C.; Klepochova, R.; Krššák, M.; Kautzky-Willer, A. Combined exenatide and dapagliflozin Has No Additive Effects on Reduction of Hepatocellular Lipids despite Better Glycaemic Control in Patients with Type 2 Diabetes Mellitus Treated with Metformin: EXENDA, a 24-week, Prospective, Randomized, Placebo-controlled Pilot Trial. Diabetes Obes. Metab. 2021, 23, 1129–1139. [Google Scholar] [CrossRef]
- Gastaldelli, A.; Repetto, E.; Guja, C.; Hardy, E.; Han, J.; Jabbour, S.A.; Ferrannini, E. Exenatide and Dapagliflozin Combination Improves Markers of Liver Steatosis and Fibrosis in Patients with Type 2 Diabetes. Diabetes Obes. Metab. 2020, 22, 393–403. [Google Scholar] [CrossRef] [Green Version]
- Cho, Y.; Rhee, H.; Kim, Y.; Lee, M.; Lee, B.-W.; Kang, E.S.; Cha, B.-S.; Choi, J.-Y.; Lee, Y. Ezetimibe Combination Therapy with Statin for Non-Alcoholic Fatty Liver Disease: An Open-Label Randomized Controlled Trial (ESSENTIAL Study). BMC Med. 2022, 20, 93. [Google Scholar] [CrossRef]
- Nakajima, A.; Eguchi, Y.; Yoneda, M.; Imajo, K.; Tamaki, N.; Suganami, H.; Nojima, T.; Tanigawa, R.; Iizuka, M.; Iida, Y.; et al. Randomised Clinical Trial: Pemafibrate, a Novel Selective Peroxisome Proliferator-activated Receptor α Modulator (SPPARMα), versus Placebo in Patients with Non-alcoholic Fatty Liver Disease. Aliment. Pharmacol. Ther. 2021, 54, 1263–1277. [Google Scholar] [CrossRef] [PubMed]
- Gawrieh, S.; Noureddin, M.; Loo, N.; Mohseni, R.; Awasty, V.; Cusi, K.; Kowdley, K.V.; Lai, M.; Schiff, E.; Parmar, D.; et al. Saroglitazar, a PPAR-α/γ Agonist, for Treatment of NAFLD: A Randomized Controlled Double-Blind Phase 2 Trial. Hepatology 2021, 74, 1809–1824. [Google Scholar] [CrossRef]
- Nadinskaia, M.; Maevskaya, M.; Ivashkin, V.; Kodzoeva, K.; Pirogova, I.; Chesnokov, E.; Nersesov, A.; Kaibullayeva, J.; Konysbekova, A.; Raissova, A.; et al. Ursodeoxycholic Acid as a Means of Preventing Atherosclerosis, Steatosis and Liver Fibrosis in Patients with Nonalcoholic Fatty Liver Disease. World J. Gastroenterol. 2021, 27, 959–975. [Google Scholar] [CrossRef] [PubMed]
- Xue, J.; Liang, S.; Ma, J.; Xiao, Y. Effect of Growth Hormone Therapy on Liver Enzyme and Other Cardiometabolic Risk Factors in Boys with Obesity and Nonalcoholic Fatty Liver Disease. BMC Endocr. Disord. 2022, 22, 49. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.S.; Weiss, J.J.; Fourman, L.T.; Buckless, C.; Branch, K.L.; Lee, H.; Torriani, M.; Misra, M.; Stanley, T.L. Effect of Recombinant Human Growth Hormone on Liver Fat Content in Young Adults with Nonalcoholic Fatty Liver Disease. Clin. Endocrinol. 2021, 94, 183–192. [Google Scholar] [CrossRef] [PubMed]
- Bahrami, M.; Cheraghpour, M.; Jafarirad, S.; Alavinejad, P.; Asadi, F.; Hekmatdoost, A.; Mohammadi, M.; Yari, Z. The Effect of Melatonin on Treatment of Patients with Non-Alcoholic Fatty Liver Disease: A Randomized Double Blind Clinical Trial. Complement. Ther. Med. 2020, 52, 102452. [Google Scholar] [CrossRef] [PubMed]
- Loomba, R.; Mohseni, R.; Lucas, K.J.; Gutierrez, J.A.; Perry, R.G.; Trotter, J.F.; Rahimi, R.S.; Harrison, S.A.; Ajmera, V.; Wayne, J.D.; et al. TVB-2640 (FASN Inhibitor) for the Treatment of Nonalcoholic Steatohepatitis: FASCINATE-1, a Randomized, Placebo-Controlled Phase 2a Trial. Gastroenterology 2021, 161, 1475–1486. [Google Scholar] [CrossRef]
- Syed-Abdul, M.M.; Parks, E.J.; Gaballah, A.H.; Bingham, K.; Hammoud, G.M.; Kemble, G.; Buckley, D.; McCulloch, W.; Manrique-Acevedo, C. Fatty Acid Synthase Inhibitor TVB-2640 Reduces Hepatic de Novo Lipogenesis in Males with Metabolic Abnormalities. Hepatology 2020, 72, 103–118. [Google Scholar] [CrossRef] [PubMed]
- Beysen, C.; Schroeder, P.; Wu, E.; Brevard, J.; Ribadeneira, M.; Lu, W.; Dole, K.; O’Reilly, T.; Morrow, L.; Hompesch, M.; et al. Inhibition of Fatty Acid Synthase with FT-4101 Safely Reduces Hepatic de Novo Lipogenesis and Steatosis in Obese Subjects with Non-alcoholic Fatty Liver Disease: Results from Two Early-phase Randomized Trials. Diabetes Obes. Metab. 2021, 23, 700–710. [Google Scholar] [CrossRef]
- Fouqueray, P.; Bolze, S.; Dubourg, J.; Hallakou-Bozec, S.; Theurey, P.; Grouin, J.-M.; Chevalier, C.; Gluais-Dagorn, P.; Moller, D.E.; Cusi, K. Pharmacodynamic Effects of Direct AMP Kinase Activation in Humans with Insulin Resistance and Non-Alcoholic Fatty Liver Disease: A Phase 1b Study. Cell Rep. Med. 2021, 2, 100474. [Google Scholar] [CrossRef]
- Gutierrez, J.A.; Liu, W.; Perez, S.; Xing, G.; Sonnenberg, G.; Kou, K.; Blatnik, M.; Allen, R.; Weng, Y.; Vera, N.B.; et al. Pharmacologic Inhibition of Ketohexokinase Prevents Fructose-Induced Metabolic Dysfunction. Mol. Metab. 2021, 48, 101196. [Google Scholar] [CrossRef] [PubMed]
- Kazierad, D.J.; Chidsey, K.; Somayaji, V.R.; Bergman, A.J.; Birnbaum, M.J.; Calle, R.A. Inhibition of Ketohexokinase in Adults with NAFLD Reduces Liver Fat and Inflammatory Markers: A Randomized Phase 2 Trial. Med 2021, 2, 800–813.e3. [Google Scholar] [CrossRef]
- Shih, P.-H.; Shiue, S.-J.; Chen, C.-N.; Cheng, S.-W.; Lin, H.-Y.; Wu, L.-W.; Wu, M.-S. Fucoidan and Fucoxanthin Attenuate Hepatic Steatosis and Inflammation of NAFLD through Modulation of Leptin/Adiponectin Axis. Mar. Drugs 2021, 19, 148. [Google Scholar] [CrossRef] [PubMed]
- Kessoku, T.; Imajo, K.; Kobayashi, T.; Ozaki, A.; Iwaki, M.; Honda, Y.; Kato, T.; Ogawa, Y.; Tomeno, W.; Kato, S.; et al. Lubiprostone in Patients with Non-Alcoholic Fatty Liver Disease: A Randomised, Double-Blind, Placebo-Controlled, Phase 2a Trial. Lancet Gastroenterol. Hepatol. 2020, 5, 996–1007. [Google Scholar] [CrossRef]
- Yasukawa, K.; Shimizu, A.; Yokoyama, T.; Kubota, K.; Notake, T.; Seki, H.; Kobayashi, A.; Soejima, Y. Preventive Effect of High-Dose Digestive Enzyme Management on Development of Nonalcoholic Fatty Liver Disease after Pancreaticoduodenectomy: A Randomized Controlled Clinical Trial. J. Am. Coll. Surg. 2020, 231, 658–669. [Google Scholar] [CrossRef] [PubMed]
- Safadi, R.; Braun, M.; Francis, A.; Milgrom, Y.; Massarwa, M.; Hakimian, D.; Hazou, W.; Issachar, A.; Harpaz, Z.; Farbstein, M.; et al. Randomised Clinical Trial: A Phase 2 Double-blind Study of Namodenoson in Non-alcoholic Fatty Liver Disease and Steatohepatitis. Aliment. Pharmacol. Ther. 2021, 54, 1405–1415. [Google Scholar] [CrossRef]
- Traussnigg, S.; Halilbasic, E.; Hofer, H.; Munda, P.; Stojakovic, T.; Fauler, G.; Kashofer, K.; Krssak, M.; Wolzt, M.; Trauner, M. Open-Label Phase II Study Evaluating Safety and Efficacy of the Non-Steroidal Farnesoid X Receptor Agonist PX-104 in Non-Alcoholic Fatty Liver Disease. Wien. Klin. Wochenschr. 2021, 133, 441–451. [Google Scholar] [CrossRef]
- Climax, J.; Newsome, P.N.; Hamza, M.; Weissbach, M.; Coughlan, D.; Sattar, N.; McGuire, D.K.; Bhatt, D.L. Effects of Epeleuton, a Novel Synthetic Second-Generation N-3 Fatty Acid, on Non-Alcoholic Fatty Liver Disease, Triglycerides, Glycemic Control, and Cardiometabolic and Inflammatory Markers. J. Am. Heart Assoc. 2020, 9, e016334. [Google Scholar] [CrossRef] [PubMed]
- Loomba, R.; Morgan, E.; Watts, L.; Xia, S.; Hannan, L.A.; Geary, R.S.; Baker, B.F.; Bhanot, S. Novel Antisense Inhibition of Diacylglycerol O-Acyltransferase 2 for Treatment of Non-Alcoholic Fatty Liver Disease: A Multicentre, Double-Blind, Randomised, Placebo-Controlled Phase 2 Trial. Lancet Gastroenterol. Hepatol. 2020, 5, 829–838. [Google Scholar] [CrossRef] [PubMed]
- Hou, X.; Yin, S.; Ren, R.; Liu, S.; Yong, L.; Liu, Y.; Li, Y.; Zheng, M.; Kunos, G.; Gao, B.; et al. Myeloid-Cell–Specific IL-6 Signaling Promotes MicroRNA-223-Enriched Exosome Production to Attenuate NAFLD-Associated Fibrosis. Hepatology 2021, 74, 116–132. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Xu, Z.; Wang, Q.; Shu, S. Danshao Shugan Granule Therapy for Non-Alcoholic Fatty Liver Disease. Lipids Health Dis. 2022, 21, 76. [Google Scholar] [CrossRef] [PubMed]
- Taha, M.M.; Aneis, Y.M.; Mohamady, H.M.; Alrasheedy, S.A.; Elsayed, S.H. Effect of Focused Ultrasound Cavitation Augmented with Aerobic Exercise on Abdominal and Intrahepatic Fat in Patients with Non-Alcoholic Fatty Liver Disease: A Randomized Controlled Trial. PLoS ONE 2021, 16, e0250337. [Google Scholar] [CrossRef]
- Mingrone, G.; van Baar, A.C.; Devière, J.; Hopkins, D.; Moura, E.; Cercato, C.; Rajagopalan, H.; Lopez-Talavera, J.C.; White, K.; Bhambhani, V.; et al. Safety and Efficacy of Hydrothermal Duodenal Mucosal Resurfacing in Patients with Type 2 Diabetes: The Randomised, Double-Blind, Sham-Controlled, Multicentre REVITA-2 Feasibility Trial. Gut 2022, 71, 254–264. [Google Scholar] [CrossRef] [PubMed]
- Nakao, Y.; Amrollahi, P.; Parthasarathy, G.; Mauer, A.S.; Sehrawat, T.S.; Vanderboom, P.; Nair, K.S.; Nakao, K.; Allen, A.M.; Hu, T.Y.; et al. Circulating Extracellular Vesicles Are a Biomarker for NAFLD Resolution and Response to Weight Loss Surgery. Nanomed. Nanotechnol. Biol. Med. 2021, 36, 102430. [Google Scholar] [CrossRef]
- Barros, F.; Fonseca, A.B.M. Bariatric Surgery during the Evolution of Fatty Liver–A Randomized Clinical Trial Comparing Gastric Bypass and Sleeve Gastrectomy Based on Transient Elastography. Clin. Obes. 2020, 10, e12393. [Google Scholar] [CrossRef]
- Dong, C.; Zhang, C.-R.; Xue, B.-Y.; Miu, W.-F.; Fang, N.-Y.; Li, K.; Ou, Z.-J.; Xu, Y.-Q. Electroacupuncture combined with lifestyle control on obese nonalcoholic fatty liver disease: A randomized controlled trial. Zhongguo Zhen Jiu Chin. Acupunct. Moxibustion 2020, 40, 129–134. [Google Scholar] [CrossRef]

{kind=link}
| Author | Diet | Duration | Results |
|---|---|---|---|
| Tutunchi et al. [50] | oleoyl ethanol amide | 12 weeks, 125 mg twice a day | weight ↓, TG ↓, LDL ↓, ALT ↓, AST ↓, BMI ↓, PPAR-α ↑, UCP1 ↑, UCP2 ↑ |
| Medina-Urrutia et al. [51] | chia | 8 weeks of 25 g/day | BMI ↓, girth of waist ↓, visceral abdominal fat ↓ |
| Sangouni et al. [52] | garlic powder | 12 weeks, 4 tablets, with 400 mg/day | liver fat ↓, improvement of hepatic enzymes and lipid profile |
| Sangouni et al. [53] | garlic powder | 3 months, 1600 mg/day | improvement in insulin resistance and fatty liver index |
| Kruse et al. [54] | rapeseed oil in combination with an isocaloric diet | 8 weeks, 50 g/day | liver fat ↓, free fatty acids ↓, IL-6 ↑ |
| Atefi et al. [55] | sesame oil with hypocaloric diet | 12 weeks, 30 g/day | liver fat ↓, liver enzymes ↓, anthropometric parameters ↓ |
| Masnadi Shirazi et al. [56] | cranberry extract | 6 months, 144 mg/day | ALP ↓, total cholesterol ↓, TG ↓, improvements in insulin resistance, liver steatosis ↓ |
| Hormoznejad et al. [57] | cranberry extract with weight loss diet | 12 weeks, 144 mg twice a day | ALT ↓, improvement in insulin resistance |
| Goodarzi et al. [58] | pomegranate extract | 12 weeks, 225 mg of dried pomegranate twice a day | total cholesterol ↓, TG ↓, LDL/HDL ratio ↓, fasting blood glucose ↓, improvement in insulin resistance, diastolic blood pressure ↓, weight ↓, BMI ↓, waist circumference ↓, HDL ↑ |
| Namkhah et al. [59] | naringenin | 4 weeks, 200 mg/day | weight ↓, BMI ↓, improvement in the lipid profile, improvement in NAFLD state |
| Yari et al. [60] | hesperidin flaxseed | 12 weeks, 500 mg twice a day 12 weeks, 30 g/day | TG ↓, LDL ↓, liver steatosis ↓, TNF-α ↓, hs-CRP ↓ HDL ↑, NF-kB ↓, alleviation of liver fibrosis |
| Saberi-Karimian et al. [61] | curcumine–piperine complex | 8 weeks 500 mg/day | TNF-α ↓, MCP-1 ↓, EGF ↓ |
| Mirhafez et al. [62] | curcumin | 2 months, 250 mg/day | liver fat ↓, improvements in liver enzymes and lipid profile |
| Cicero et al. [63] | curcumin | 8 weeks, 800 mg twice a day | improvement in fasting plasma insulin, HOMA-IR ↓, waist circumference ↓, blood pressure ↓, TG ↓, HDL↑, liver transaminases ↓, liver steatosis ↓, cortisol ↓ |
| Moradi Kelardeh et al. [64] | resistance training with curcumin | 12 weeks, 80 mg/day | ALT ↓, AST ↓ |
| Tutunchi et al. [65] | oleoyl ethanol amide | 12 weeks, 125 mg twice a day | NF-κB ↓, IL-6 ↓, IL-10 ↑, fat ↓ |
| Amerikanou et al. [66] | mastiha | 6 months, 0.35 g three times a day | improvement in lipid levels, improvement in liver fibrosis |
| Amerikanou et al. [67] | mastiha | 6 months, 2.8 g/day | increase in miR-155 was prevented by mastiha, |
| Kanoni et al. [68] | mastiha | 6 months, 2.1 g/day | total antioxidant status ↑ |
| Izadi et al. [69] | sour tee | 8 weeks, 450 mg/day | ALT ↓, AST ↓, TG ↓, diastolic blood pressure ↓, improvement in antioxidant factors |
| Hosseinabadi et al. [70] | green coffee extract | 8 weeks, 400 mg/day | HDL-levels ↑, BMI ↓, weight ↓, improvement in lipid profile, weight ↓ |
| Pervez et al. [71] | delta-tocotrienol | 24 weeks, 300 mg twice a day | hepatic steatosis ↓, HOMA-IR ↓, hs-CRP ↓, ALT ↓, AST ↓ |
| Pervez et al. [1] | delta-tocotrienol | 48 weeks, 300 mg twice a day | hepatic steatosis ↓, HOMA-IR ↓, serum malondialdehyde ↓ |
| Majnooni et al. [72] | artichoke leaf extract in co-administration with metformin and vitamin E | 12 weeks, 400 mg twice a day | ALT ↓, AST ↓, improvement in fatty liver grades |
| Soleimani et al. [73] | propolis | 4 months, 250 mg twice a day | liver fat ↓, fibrosis ↓ |
| Kazemi et al. [74] | sumac | 12 weeks, 2000 mg/day | HOMA-IR ↓, improvement in insulin sensitivity index, fasting glucose level ↓, HbA1c ↓, hs-CRP ↓ |
| Jinato et al. [75] | litchi extract | 24 weeks, 200 mg/day | improvement in liver steatosis, alteration in intestinal microbiota |
| Author | Type of Study | Intervention Group | Diet | Duration | Results |
|---|---|---|---|---|---|
| Montemayor et al. [26] | Multi-center prospective randomized trial | 57 patients diagnosed with NAFLD using MRI and MetS, according to the International Diabetes Federation (IDF) | Mediterranean diet (high adherence) in connection with physical activity promotion and 25–30% reduction in baseline calorie intake | 6 months | ↑: HDL-c (NS) ↓: BMI (S), BW (S), WC (S), SBP (S), DBP (S), HFC (S), glucose level (NS), TG (S), HOMA-IR (NS), AST (NS), ALT (NS), GGT (S) |
| Cohen et al. [82] | RCT | 16 adolescent patients with an NAFLD diagnosis proven by biopsy | Low-free-sugar diet | 8 weeks | ↓: Hepatic DNL (S), HFC (NS), fasting insulin (NS), ALT (S) |
| Dorosti et al. [34] | RCT | 47 patients with NAFLD diagnosed by ultrasonography and liver fat content | Whole-grain diet | 12 weeks | ↑: HDL (S) ↓: Ultrasound fatty liver grade (S), ALT (S), AST (S), GGT (S), TC (S), LDL (S), TG (NS), SBP (NS), DBP (NS), serum insulin (S), HOMA-IR (S) |
| Moradi et al. [81] | RCT | 23 patients with NAFLD diagnosed by ultrasound | Chromium picolinate, 400 μg/day supplementation | 3 months | ↑: QUICKI (S) ↓: TG (S), AIP (S), VLDL-c (S), HOMA-IR (S), hs-CRP (S), IL-6 (S), TNF-α (S), fetuin-A (S) |
| Medina-Urrutia et al. [51] | Single-arm experimental design study | 25 patients with NAFLD diagnosed by computer tomography | Milled Salvia hispanica (chia) at a dose of 25 g/day, supplemented in an isocaloric diet | 8 weeks | ↓: TC (S), non-HDL-c (S), FFA (S), BW (S), BMI (S), WC (S), SAT (S), VAT (S) |
| Hormoznejad et al. [57] | RCT | 25 patients with NAFLD diagnosed by ultrasound | Weight loss diet plus cranberry supplementation, 2 tablets each containing 144 mg of Vaccinium macrocarpon extract | 12 weeks | ↑: Muscle mass (S) ↓: BW (S), body fat (S), BMI (S), WC (S), ALT (S), AST (NS), GGT (NS), insulin (S), HOMA-IR (S), TG (NS), TC (NS), LDL-c (NS) |
| Sangouni et al. [52] | RCT | 45 patients with fatty liver grade 1 to 3 based on ultrasound | Garlic powder supplementation—400 mg 4 times a day | 12 weeks | ↓: Hepatic steatosis (S), ALT (S), AST (S), GGT (S), TG (S), HDL (S), LDL (S) |
| Soleimani et al. [73] | RCT | 27 patients with hepatic steatosis diagnosed by elastography | Propolis, 250 mg twice/day | 4 months | ↓: Liver stiffness (S), hs-CRP (S), BW (NS), TG (NS), TC (NS) |
| Study | Type of Study | Intervention Group | Medication | Duration | Results | Safety |
|---|---|---|---|---|---|---|
| Phrueksotsai et al. [106] | RCT | 18 patients with DM2 and hepatic steatosis confirmed by abdominal ultrasonography or CT | Dapagliflozin, 10 mg per day | 12 weeks | ↑: HDL (NS), adiponectin (S) ↓: HFC (S), weight (S), BMI (S), body fat (S), ALT (S), HbA1c (S), HOMA-IR (NS), uric acid (NS), LDL (NS) | Lack of significant adverse effects |
| Yoneda et al. [104] | Randomized, prospective, open-label controlled trial | 21 patients with DM2 and NAFLD measured by hepatic fat fraction of at least 10%, as assessed based on the MRI-proton density fat fraction | Tofogliflozin, 20 mg per day | 24 weeks | ↑: HDL (S), ketone bodies (S) ↓: HFC (S), BW (S), ALT (S), AST (S), GGT (S), liver stiffness—MRE-LSM (NS), HbA1c (S), uric acid (S), oxidative stress (S), hepatocyte apoptosis—CK-18 fragment M30 antigen (S) | One case of urinary tract infection, lack of life-threatening events |
| Taheri et al. [107] | RCT | 43 patients with an NAFLD diagnosis based on previous ultrasound imaging or liver function test without diabetes comorbidity | Empagliflozin, 10 mg/day | 24 weeks | ↓: liver stiffness (S), liver steatosis (S), AST (S), ALT (S), fasting insulin (S), BW (S), BMI (S), WC (S) | Lack of major adverse effects |
| Takahashi et al. [105] | RCT | 25 patients with DM and NAFLD diagnosed by liver biopsy | Ipragliflozin, 50 mg/day | 72 weeks | ↓: HbA1c (S), BMI (S), fasting glucose (S), VAT(S), SAT (S), AST (S), ALT (S), GGT (S), type IV collagen 7s—marker of fibrosis (S), liver fibrosis reduction by at least one stage (S) | Mild to moderate adverse effects reported by 22.2% of participants |
| Yoneda et al. [104] | Randomized, prospective, open-label controlled trial | 19 patients with DM2 and NAFLD measured by hepatic fat fraction of at least 10%, as assessed based on the MRI-proton density fat fraction | Pioglitazone, 15–30 mg per day | 24 weeks | ↑: BW (S), HDL (S), adiponectin (S) ↓: HFC (S), ALT (S), AST (S), GGT (S), alkaline phosphatase levels (S), liver stiffness—MRE-LSM (S), HbA1c (S), TG (S), oxidative stress (NS), hepatocyte apoptosis—CK-18 fragment M30 antigen (S) | Adverse effects: edema and weight gain, lack of life-threatening events |
| Wang et al. [113] | A prospective comparative study | 14 patients with DM2 comorbidity with ab NAFLD diagnosis based on fulfillment of diagnostic criteria | Sitagliptin, 100 mg/day | 24 weeks | ↓: HFC (NS), HbA1c (S), FPG (S), WC (S), BMI (S) | Well tolerated |
| Liu et al. [115] | RCT | 38 patients with NAFLD measured by proton MRS and newly diagnosed DM2 | Exenatide s.c. 5 μg twice daily for 4 weeks followed by 10 μg twice daily for 20 weeks | 24 weeks | ↓: HFC (S), FIB-4 (S), VAT (S), SAT (S), ALT, AST, GGT, TC (S), TG (S) LDL-c (S), FFA (S), WC (S), BW (S), BMI (S), SBP (S), DBP (S) | Hypoglycemic events, lack of major adverse effects |
| Flint et al. [116] | RCT | 34 patients with NAFLD measured by MRI-PDFF | Semaglutide s.c. 0.4 mg/day | 72 weeks | ↓: liver steatosis (S), hepatic fat volume (S), total liver volume (S), VAT (S), SAT (S), BW (S), HbA1c (S), ALT (S), AST (S), GGT (S), SBP (S), hs-CRP (S), TG (S) | Reported adverse reactions were similar in the treatment group and placebo; gastrointestinal effects and serious adverse effects reported by 12.1% of subjects |
| Guo et al. [120] | RCT | Patients with DM2 and NAFLD indicated by hepatic steatosis upon imaging or histology | Liraglutide s.c. at onset 0.6 mg/day, increased weekly with forced titration to 1.8 mg plus metformin at 2 g/day | 26 weeks | ↓: HFC (S), SAT (S), VAT (S), AST (S), ALT (S), HOMA-IR (S), BW (S), WC (S), BMI (S), HbA1c (NS), FBG (NS) | Events of mild hypoglycemia, nausea, diarrhea and vomiting |
| Liu et al. [115] | RCT | 38 patients with NAFLD measured by proton MRS and newly diagnosed DM2 | Insulin glargine (Lantus) at doses needed to achieve below 7.0 mmol/L of FPG | 24 weeks | ↓: HFC (S), VAT (NS), ALT (S), GGT (S), HbA1c (S), TG (S), FFA (S), WC (S), FCP (S) | Hypoglycemic events, lack of major adverse effects |
| Nakajima et al. [124] | RCT | 58 patients with MRI-PDFF proven elevated liver fat content | Pemafibrate, 0.2 mg twice a day | 72 weeks | ↓: MRE-based liver stiffness (S), HFC (NS), ALT (S), GGT (S), ALP (S), LDL-c (S), TC (S), TG (S), HDL-c (S) | Therapy well tolerated, mild and moderate severity adverse effects |
| Cho et al. [123] | RCT | 34 patients with liver steatosis proven by ultrasound with or without DM2 | Ezetimibe 10 mg/day plus rosuvastatin 5 mg/day | 24 weeks | ↓: HFC (S), CAP (S), BMI (S), WC (S), LDL-c (S), TG (S), CRP (S) | Lack of significant adverse effects |
| Nadinskaia et al. [126] | Open-label, multicenter, international noncomparative trial | 74 patients with NAFLD diagnosed by ultrasound | Ursodeoxycholic acid 15 mg/kg/day | 6 months | ↑: HDL (S)—only in women’s group ↓: BW (S), FLI (S), TC (S), LDL (S), TG (S), CIMT (S), 10-year ASCVD risk (S—for women, NS—for men), ALT (S for man and women), ALT (S for man), AST (S for men), GGT (S for men) | No data |
| Pan et al. [128] | Randomized open label trial | young people with ≥5% hepatic fat fraction on proton magnetic resonance spectroscopy | Somatropin at a starting dose of 0.5 mg/day with further titration to IGF-1 z-score | 24 weeks | ↓: HFF (S), BMI (S), ALT (NS), AST (NS), GGT (NS) | Lack of treatment-related reasons to discontinue the study |
| Climax et al. [141] | RCT | 33 patients with NAFLD diagnosed by imaging or histology | Epeleuton at a dose of 1 g twice a day | 16 weeks | ↓: HFC (NS), ALT (NS), HOMA-IR (S), Adipo-IR (S), HbA1c (S), FPG (S), TG (S), TC (S), VLDL-c (S), RLP-c (S), non–HDL-C (NS), circulating inflammatory markers (S) | 45.5% of responders reported adverse events connected with treatment being mild to moderate in severity but probably not related to epeleuton, lack of serious adverse effects |
| Zeybel et al. [99] | Randomized, placebo-controlled phase 2 study | 20 overweight patients with NAFLD diagnosis—liver fat was determined by MRI-PDFF | Combined metabolic activators (CMAs) containing 3.73 g L-carnitine tartrate, 1 g nicotinamide riboside, 12.35 g serine and 2.55 g N-acetyl-l-cysteine)—one dose for first 14 days, followed by 2 doses up to the end of the study | 10 weeks | ↓: HFC (S), ALT (S), AST (S), uric acid (S), creatinine (S), SBP (S), inflammatory protein markers (S) | 12 of 20 subjects reported mild–moderate adverse symptoms, but they decided to be followed up in the study |
| Harrison et al. [102] | Randomized clinical study | 29 patients with NAFLD diagnosis indicated by CT, MR and AST level, including 12 patients with diabetes comorbidity | AXA1125 24 g twice daily | 16 weeks | ↓: HFC (S), HOMA-IR (NS), ALT (NS), liver fibrosis (NS), apoptosis marker—K-18 M65 (S—after 8 weeks, NS—at the endpoint), cT1—imaging marker of inflammation and fibrosis (S) | Mild or moderate adverse effects, 1 subject resigned from the study |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kosmalski, M.; Frankowski, R.; Ziółkowska, S.; Różycka-Kosmalska, M.; Pietras, T. What’s New in the Treatment of Non-Alcoholic Fatty Liver Disease (NAFLD). J. Clin. Med. 2023, 12, 1852. https://doi.org/10.3390/jcm12051852
Kosmalski M, Frankowski R, Ziółkowska S, Różycka-Kosmalska M, Pietras T. What’s New in the Treatment of Non-Alcoholic Fatty Liver Disease (NAFLD). Journal of Clinical Medicine. 2023; 12(5):1852. https://doi.org/10.3390/jcm12051852
Chicago/Turabian StyleKosmalski, Marcin, Rafał Frankowski, Sylwia Ziółkowska, Monika Różycka-Kosmalska, and Tadeusz Pietras. 2023. "What’s New in the Treatment of Non-Alcoholic Fatty Liver Disease (NAFLD)" Journal of Clinical Medicine 12, no. 5: 1852. https://doi.org/10.3390/jcm12051852
APA StyleKosmalski, M., Frankowski, R., Ziółkowska, S., Różycka-Kosmalska, M., & Pietras, T. (2023). What’s New in the Treatment of Non-Alcoholic Fatty Liver Disease (NAFLD). Journal of Clinical Medicine, 12(5), 1852. https://doi.org/10.3390/jcm12051852