
Chemokine/Cytokine Levels Correlate with Organ Involvement in PR3-ANCA-Associated Vasculitis

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Cytokine Array
2.3. Assessment of Organ Involvement of the Disease
2.4. Statistics
3. Results
3.1. Patients’ Characteristics
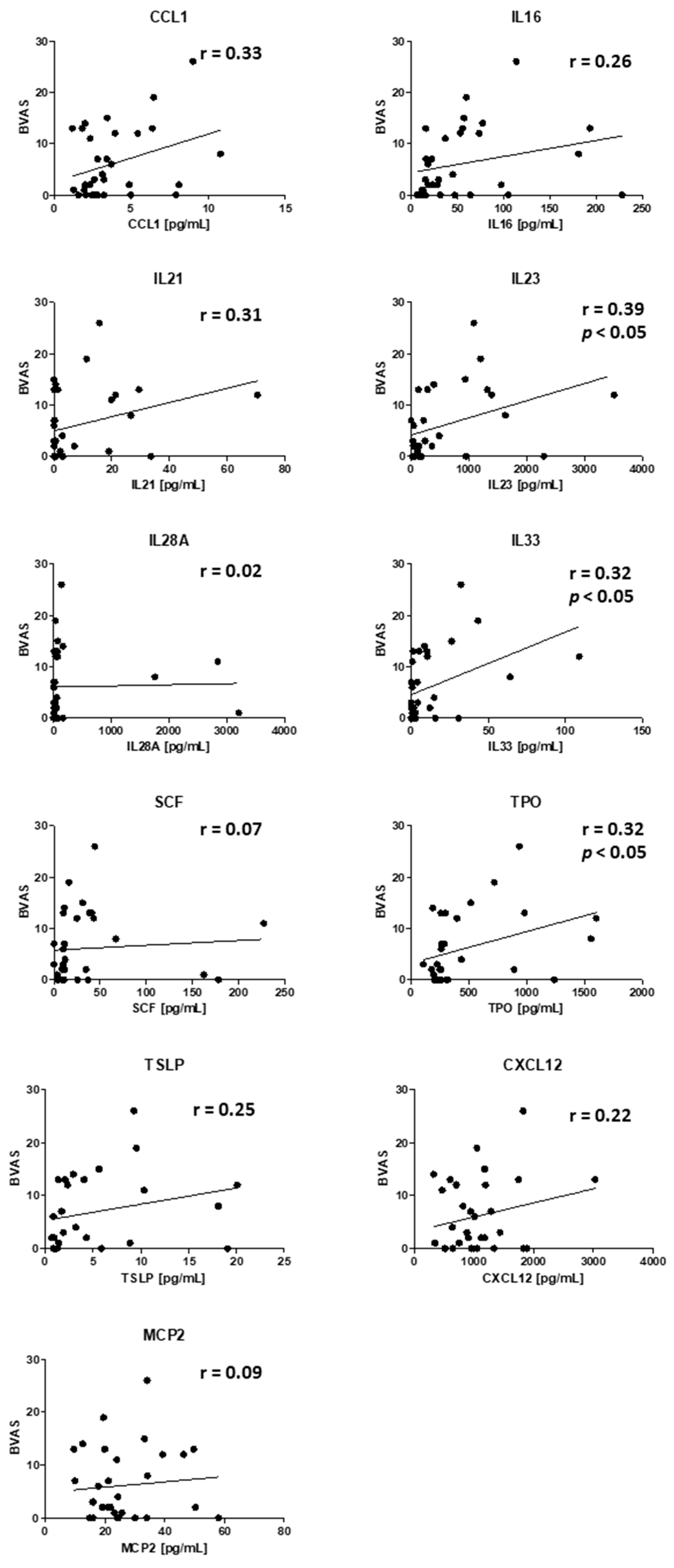
3.2. Correlations of Plasma Cytokines and Disease Activity
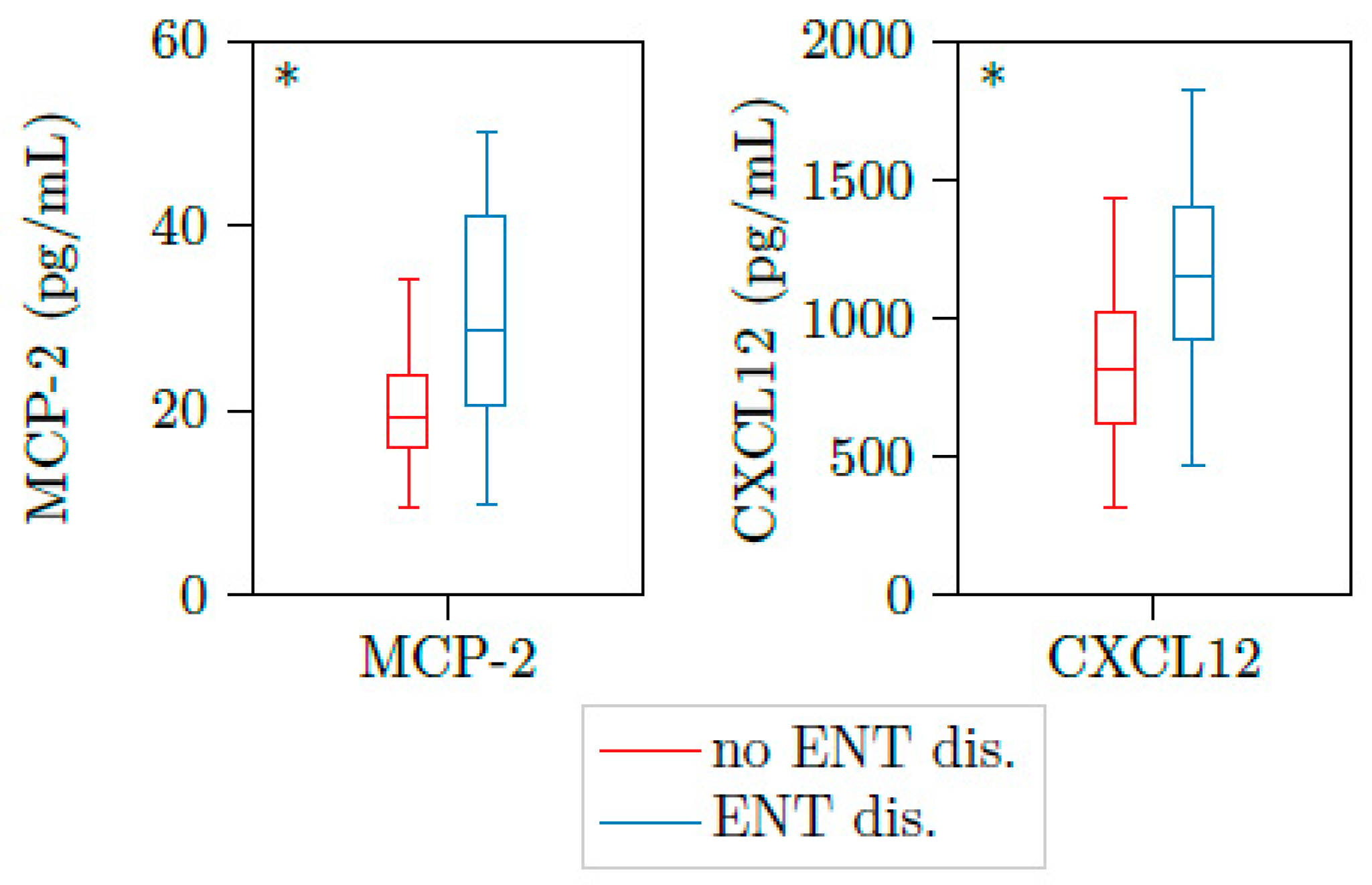
3.3. Correlations of Plasma Cytokines and Ear/Nose/Throat Activity
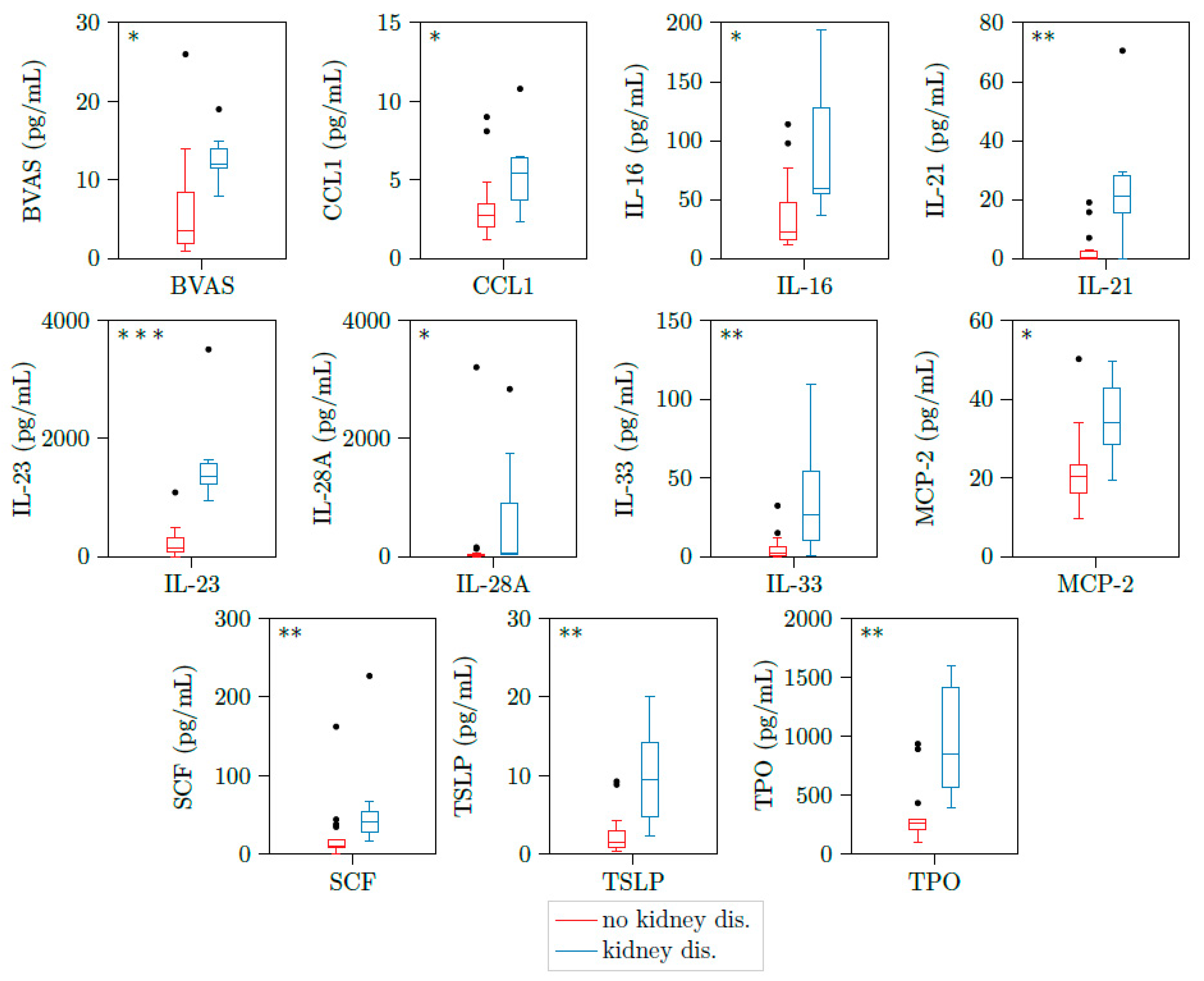
3.4. Correlations of Plasma Cytokines and Kidney Involvement
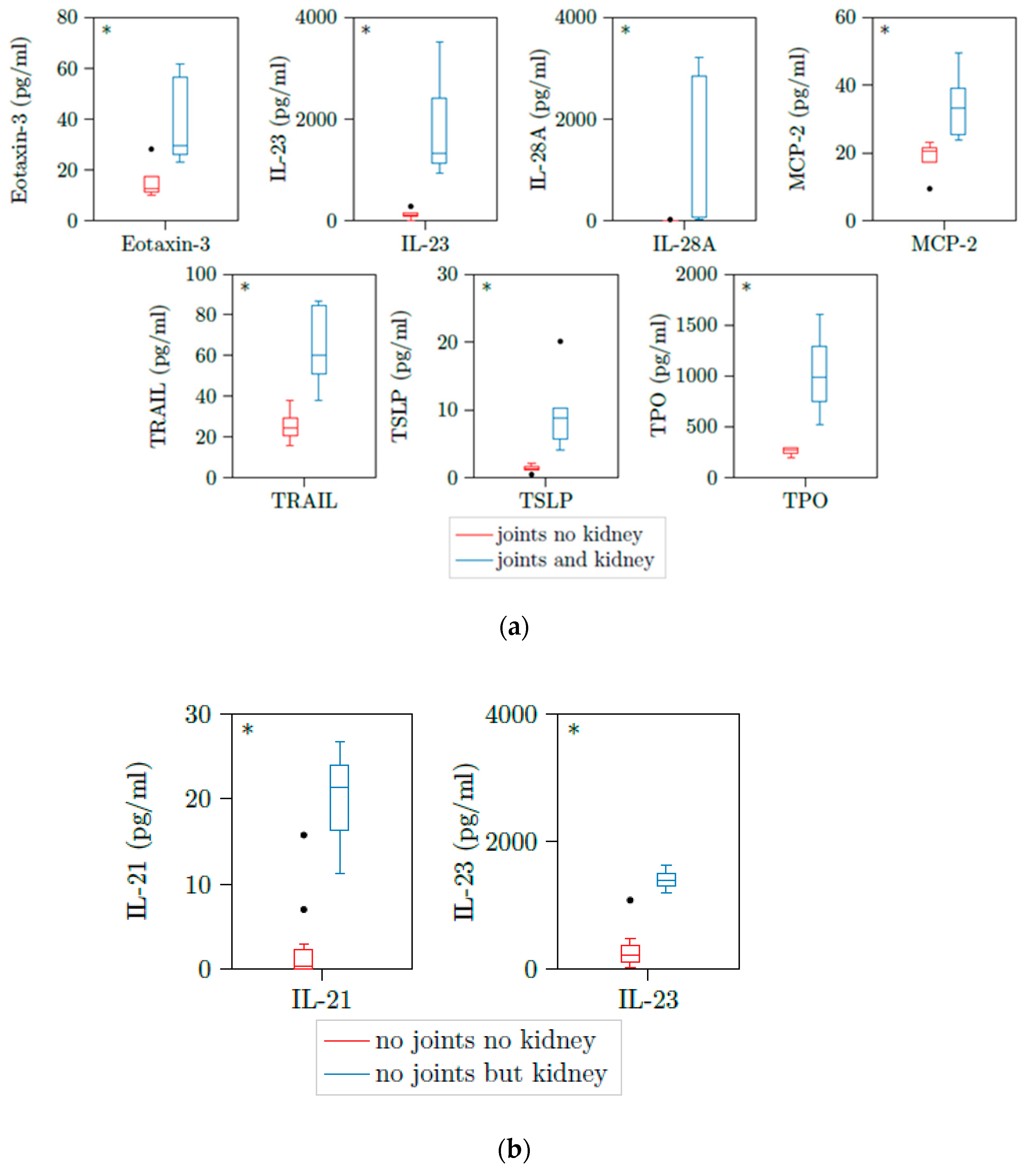
3.5. Correlations of Plasma Cytokines and Joint and Lung Activity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hoffman, G.S.; Kerr, G.S.; Leavitt, R.Y.; Hallahan, C.W.; Lebovics, R.S.; Travis, W.D.; Rottem, M.; Fauci, A.S. Wegener Granulomatosis: An Analysis of 158 Patients. Ann. Intern. Med. 1992, 116, 488–498. [Google Scholar] [CrossRef]
- Greco, A.; Marinelli, C.; Fusconi, M.; Macri, G.; Gallo, A.; De Virgilio, A.; Zambetti, G.; de Vincentiis, M. Clinic manifestations in granulomatosis with polyangiitis. Int. J. Immunopathol. Pharmacol. 2016, 29, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Falk, R.J.; Jennette, J.C. Anti-Neutrophil Cytoplasmic Autoantibodies with Specificity for Myeloperoxidase in Patients with Systemic Vasculitis and Idiopathic Necrotizing and Crescentic Glomerulonephritis. N. Engl. J. Med. 1988, 318, 1651–1657. [Google Scholar] [CrossRef] [PubMed]
- Jennette, J.C.; Falk, R.J. Antineutrophil Cytoplasmic Autoantibodies and Associated Diseases: A Review. Am. J. Kidney Dis. 1990, 15, 517–529. [Google Scholar] [CrossRef]
- Jennette, J.C.; Falk, R.J.; Bacon, P.A.; Basu, N.; Cid, M.C.; Ferrario, F.; Flores-Suarez, L.F.; Gross, W.L.; Guillevin, L.; Hagen, E.C.; et al. Revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheumatol. 2013, 65, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Birck, R.; Schmitt, W.H.; Kaelsch, I.A.; van der Woude, F.J. Serial ANCA Determinations for Monitoring Disease Activity in Patients With ANCA-Associated Vasculitis: Systematic Review. Am. J. Kidney Dis. 2006, 47, 15–23. [Google Scholar] [CrossRef]
- Boomsma, M.M.; Stegeman, C.A.; van der Leij, M.J.; Oost, W.; Hermans, J.; Kallenberg, C.G.M.; Limburg, P.C.; Tervaert, J.W.C. Prediction of relapses in Wegener’s granulomatosis by measurement of antineutrophil cytoplasmic antibody levels: A prospective study. Arthritis Rheumatol. 2000, 43, 2025–2033. [Google Scholar] [CrossRef]
- Tomasson, G.; Grayson, P.C.; Mahr, A.; LaValley, M.; Merkel, P.A. Value of ANCA measurements during remission to predict a relapse of ANCA-associated vasculitis—A meta-analysis. Rheumatology 2011, 51, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Jennette, J.C.; Nachman, P.H. ANCA Glomerulonephritis and Vasculitis. Clin. J. Am. Soc. Nephrol. 2017, 12, 1680–1691. [Google Scholar] [CrossRef] [PubMed]
- Kronbichler, A.; Shin, J.I.; Lee, K.H.; Nakagomi, D.; Quintana, L.F.; Busch, M.; Craven, A.; Luqmani, R.A.; Merkel, P.A.; Mayer, G.; et al. Clinical associations of renal involvement in ANCA-associated vasculitis. Autoimmun. Rev. 2020, 19, 102495. [Google Scholar] [CrossRef] [PubMed]
- Salama, A.D.; Little, M.A. Animal models of antineutrophil cytoplasm antibody-associated vasculitis. Curr. Opin. Rheumatol. 2012, 24, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Xiao, H.; Heeringa, P.; Hu, P.; Liu, Z.; Zhao, M.; Aratani, Y.; Maeda, N.; Falk, R.J.; Jennette, J.C. Antineutrophil cytoplasmic autoantibodies specific for myeloperoxidase cause glomerulonephritis and vasculitis in mice. J. Clin. Investig. 2002, 110, 955–963. [Google Scholar] [CrossRef] [PubMed]
- Sinico, R.A.; di Toma, L.; Radice, A. Renal involvement in anti-neutrophil cytoplasmic autoantibody associated vasculitis. Autoimmun. Rev. 2013, 12, 477–482. [Google Scholar] [CrossRef] [PubMed]
- Poggio, E.D.; McClelland, R.L.; Blank, K.N.; Hansen, S.; Bansal, S.; Bomback, A.S.; Canetta, P.A.; Khairallah, P.; Kiryluk, K.; Lecker, S.H.; et al. Systematic Review and Meta-Analysis of Native Kidney Biopsy Complications. Clin. J. Am. Soc. Nephrol. 2020, 15, 1595–1602. [Google Scholar] [CrossRef]
- O’Brien, E.C.; White, C.A.; Wyse, J.; Leacy, E.; Porter, R.K.; Little, M.A.; Hickey, F.B. Pro-inflammatory Stimulation of Monocytes by ANCA Is Linked to Changes in Cellular Metabolism. Front. Med. 2020, 7, 553. [Google Scholar] [CrossRef] [PubMed]
- Brix, S.R.; Stege, G.; Disteldorf, E.; Hoxha, E.; Krebs, C.; Krohn, S.; Otto, B.; Klätschke, K.; Herden, E.; Heymann, F.; et al. CC Chemokine Ligand 18 in ANCA-Associated Crescentic GN. J. Am. Soc. Nephrol. 2015, 26, 2105–2117. [Google Scholar] [CrossRef] [PubMed]
- Fagin, U.; Csernok, E.; Müller, A.; Pitann, S.; Fazio, J.; Krause, K.; Bremer, P.; Wipfler-Freissmuth, E.; Moosig, F.; Gross, W.L.; et al. Distinct proteinase 3-induced cytokine patterns in Wegener’s granulomatosis, Churg-Strauss syndrome, and healthy controls. Clin. Exp. Rheumatol. 2011, 29, 57–62. [Google Scholar]
- Gou, S.-J.; Yuan, J.; Chen, M.; Yu, F.; Zhao, M.-H. Circulating complement activation in patients with anti-neutrophil cytoplasmic antibody-associated vascu-litis. Kidney Int. 2013, 83, 129–137. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, E.C.; Abdulahad, W.H.; Rutgers, A.; Huitema, M.G.; O’Reilly, V.P.; Coughlan, A.M.; Harrington, M.; Heeringa, P.; Little, M.A.; Hickey, F.B. Intermediate monocytes in ANCA vasculitis: Increased surface expression of ANCA autoantigens and IL-1β secretion in response to anti-MPO antibodies. Sci. Rep. 2015, 5, srep11888. [Google Scholar] [CrossRef]
- Kiessler, P.C. Probability & statistics for engineers & scientists. Am. Stat. 2006, 60, 343. [Google Scholar]
- Shapiro, S.S.; Wilk, M.B. An analysis of variance test for normality (complete samples). Biometrika 1965, 52, 591–611. [Google Scholar] [CrossRef]
- Levene, H. Contributions to Probability and Statistics: Essays in Honor of Harold Hotelling; Stanford University Press: Palo Alto, CA, USA, 1960. [Google Scholar]
- Welch, B.L. The generalization of “Student’s” problem when several different population variances are involved. Biometrika 1947, 34, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Mann, H.B.; Whitney, D.R. On a Test of Whether one of Two Random Variables is Stochastically Larger than the Other. Ann. Math. Stat. 1947, 18, 50–60. [Google Scholar] [CrossRef]
- Hogan, P.C.P.; O’Connell, R.M.; Scollard, S.; Browne, E.; Hackett, E.E.; Feighery, C. Biomarkers Predict Relapse in Granulomatosis with Polyangiitis. J. Biomark. 2014, 2014, 1–4. [Google Scholar] [CrossRef]
- Bader, L.; Koldingsnes, W.; Nossent, J. B-lymphocyte activating factor levels are increased in patients with Wegener’s granulomatosis and inversely correlated with ANCA titer. Clin. Rheumatol. 2010, 29, 1031–1035. [Google Scholar] [CrossRef]
- Hoffmann, J.C.; Patschan, D.; Dihazi, H.; Müller, C.; Schwarze, K.; Henze, E.; Ritter, O.; Müller, G.A.; Patschan, S. Cytokine profiling in anti neutrophil cytoplasmic antibody-associated vasculitis: A cross-sectional cohort study. Rheumatol. Int. 2019, 39, 1907–1917. [Google Scholar] [CrossRef] [PubMed]
- Natori, Y.; Sekiguchi, M.; Ou, Z. Gene expression of CC chemokines in experimental crescentic glomerulonephritis (CGN). Clin. Exp. Immunol. 1997, 109, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Wohlfahrtova, M.; Tycova, I.; Honsova, E.; Lodererova, A.; Viklicky, O. Molecular Patterns of Subclinical and Clinical Rejection of Kidney Allograft: Quantity Matters. Kidney Blood Press. Res. 2015, 40, 244–257. [Google Scholar] [CrossRef] [PubMed]
- Lai, P.C.; Smith, J.; Bhangal, G.; Chaudhry, K.A.; Chaudhry, A.N.; Keith, J.C., Jr.; Tam, F.W.K.; Pusey, C.D.; Cook, H.T. Interleukin-11 reduces renal injury and glomerular NF-kappa B activity in murine experimental glomeru-lonephritis. Nephron Exp. Nephrol. 2005, 101, e146–e154. [Google Scholar] [CrossRef] [PubMed]
- Magno, A.L.; Herat, L.Y.; Carnagarin, R.; Schlaich, M.P.; Matthews, V.B. Current Knowledge of IL-6 Cytokine Family Members in Acute and Chronic Kidney Disease. Biomedicines 2019, 7, 19. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.H.; Chung, J.-J.; Akilesh, S.; Koziell, A.; Jain, S.; Hodgin, J.B.; Miller, M.J.; Stappenbeck, T.S.; Miner, J.H.; Shaw, A.S. B cell–derived IL-4 acts on podocytes to induce proteinuria and foot process effacement. JCI Insight 2017, 2. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Chen, L.; Yao, G.; Yang, W.; Yang, K.; Xiong, C. Novel Blood Cytokine-Based Model for Predicting Severe Acute Kidney Injury and Poor Outcomes After Cardiac Surgery. J. Am. Hear. Assoc. 2020, 9, e018004. [Google Scholar] [CrossRef]
- Pawlik, K.K.; Bohdziewicz, A.; Chrabąszcz, M.; Stochmal, A.; Sikora, M.; Alda-Malicka, R.; Czuwara, J.; Rudnicka, L. Biomarkers of disease activity in systemic sclerosis. Wiad. Lek. 2020, 73, 2300–2305. [Google Scholar] [CrossRef]
- Hladinova, Z.; Hruskova, Z.; Svobodova, B.; Malickova, K.; Lanska, V.; Konopásek, P.; Jancova, E.; Rysava, R.; Edelstein, C.L.; Tesar, V. Increased Levels of Soluble ST2 in Patients with Active Newly Diagnosed ANCA-Associated Vasculitis. Mediat. Inflamm. 2015, 2015, 1–5. [Google Scholar] [CrossRef]
- Nogueira, E.; Hamour, S.; Sawant, D.; Henderson, S.; Mansfield, N.; Chavele, K.-M.; Pusey, C.D.; Salama, A.D. Serum IL-17 and IL-23 levels and autoantigen-specific Th17 cells are elevated in patients with AN-CA-associated vasculitis. Nephrol. Dial. Transplant. 2010, 25, 2209–2217. [Google Scholar] [CrossRef] [PubMed]
- Bilgic, H.; Ytterberg, S.R.; Amin, S.; McNallan, K.T.; Wilson, J.C.; Koeuth, T.; Ellingson, S.; Newman, B.; Bauer, J.W.; Peterson, E.J.; et al. Interleukin-6 and type I interferon-regulated genes and chemokines mark disease activity in dermatomyo-sitis. Arthritis Rheumatol. 2009, 60, 3436–3446. [Google Scholar] [CrossRef] [PubMed]
- El Kossi, M.M.H.; El Nahas, A.M. Stem cell factor and crescentic glomerulonephritis. Am. J. Kidney Dis. 2003, 41, 785–795. [Google Scholar] [CrossRef]
- El-Koraie, A.F.; Baddour, N.M.; Adam, A.G.; El Kashef, E.H.; El Nahas, A.M. Role of stem cell factor and mast cells in the progression of chronic glomerulonephritides. Kidney Int. 2001, 60, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Taneda, S.; Segerer, S.; Hudkins, K.L.; Cui, Y.; Wen, M.; Segerer, M.; Wener, M.H.; Khairallah, C.G.; Farr, A.G.; Alpers, C.E. Cryoglobulinemic Glomerulonephritis in Thymic Stromal Lymphopoietin Transgenic Mice. Am. J. Pathol. 2001, 159, 2355–2369. [Google Scholar] [CrossRef]
- Banas, M.C.; Banas, B.; Hudkins, K.L.; Wietecha, T.A.; Iyoda, M.; Bock, E.; Hauser, P.; Pippin, J.W.; Shankland, S.J.; Smith, K.D.; et al. TLR4 links podocytes with the innate immune system to mediate glomerular injury. J. Am. Soc. Nephrol. 2008, 19, 704–713. [Google Scholar] [CrossRef] [PubMed]
- Park, H.J.; Jung, S.M.; Song, J.J.; Park, Y. Platelet to lymphocyte ratio is associated with the current activity of ANCA-associated vasculitis at diag-nosis: A retrospective monocentric study. Rheumatol. Int. 2018, 38, 1865–1871. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, M.; Thomas, S.R.; Radford, K.; Dvorkin-Gheva, A.; Davydchenko, S.; Kjarsgaard, M.; Svenningsen, S.; Almas, S.; Felix, L.C.; Stearns, J.; et al. Sputum Antineutrophil Cytoplasmic Antibodies in Serum Antineutrophil Cytoplasmic Anti-body-Negative Eosinophilic Granulomatosis with Polyangiitis. Am. J. Respir. Crit. Care Med. 2019, 199, 158–170. [Google Scholar] [CrossRef] [PubMed]
- Radajewski, K.; Wierzchowska, M.; Grzanka, D.; Antosik, P.; Zdrenka, M.; Burduk, P. Tissue remodelling in chronic rhinosinusitis—Review of literature. Otolaryngol. Pol. 2019, 73, 1–4. [Google Scholar]
- Miyabe, Y.; Miyabe, C.; Iwai, Y.; Luster, A.D. Targeting the Chemokine System in Rheumatoid Arthritis and Vasculitis. JMA J. 2020, 3, 182–192. [Google Scholar] [CrossRef] [PubMed]
- Sakai, R.; Kondo, T.; Kurasawa, T.; Nishi, E.; Okuyama, A.; Chino, K.; Shibata, A.; Okada, Y.; Takei, H.; Nagasawa, H.; et al. Current clinical evidence of tocilizumab for the treatment of ANCA-associated vasculitis: A prospective case series for microscopic polyangiitis in a combination with corticosteroids and literature review. Clin. Rheumatol. 2017, 36, 2383–2392. [Google Scholar] [CrossRef] [PubMed]
- Seitz, M.; Reichenbach, S.; Bonel, H.M.; Adler, S.; Wermelinger, F.; Villiger, P.M. Rapid induction of remission in large vessel vasculitis by IL-6 blockade. A case series. Swiss Med. Wkly. 2011, 141, 13156. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Demographics | |
|---|---|
| Age; n = 17 | mean ± std. |
| age | 54.1 ± 13.0 |
| Gender | n |
| f/m | 8/9 |
| PR3-ANCA titer | mean ± std. |
| active disease | 331.4 ± 598.2 |
| remission | 141.3 ± 314.5 |
| BVAS | mean ± std. |
| active disease | 8.5 ± 6.4 |
| remission | 0.0 ± 0.0 |
| Comorbidities; n = 17 | n yes/no (% yes/no) |
| hypertension | 11/6 (64.7/35.3) |
| diabetes | 2/15 (11.8/88.2) |
| cardio vascular disease | 0/17 (0/100) |
| malignancies | 0/17 (0/100) |
| kidney transplantation | 0/17 (0/100) |
| dialysis | 2/15 (11.8/88.2) |
| Main organ involvement at initial presentation; n = 17 | n yes/no (% yes/no) |
| renal | 7/10 (41.2/58.8) |
| ear, nose and throat | 10/7 (58.8/41.2) |
| joint | 7/10 (41.2/58.8) |
| lung | 5/12 (29.4/70.6) |
| central nerve system | 6/11 (35.3/64.7) |
| Main organ involvement at follow up; n = 15 | n yes/no (% yes/no) |
| renal | 0/15 (0.0/100.0) |
| ear, nose and throat | 2/13 (13.3/86.7) |
| joint | 7/10 2/13 (13.3/86.7) |
| lung | 0/15 (0.0/100.0) |
| central nerve system | 2/13 (13.3/86.7) |
| Medication at initial presentation; n = 17 | n yes/no (% yes/no) |
| Steroids | 13/4 (76.5/23.5) |
| Cyclophosphamide | 3/14 (17.6/82.4) |
| Azathioprine | 5/12 (29.4/70.6) |
| Mycophenolate mofetil | 3/14 (17.6/82.4) |
| Methotrexate | 2/15 (11.8/88.2) |
| Cyclosporine | 0/17 (0/100) |
| Rituximab | 0/17 (0/100) |
| Plasmapheresis | 0/17 (0/100) |
| Medication at follow up; n = 15 | n yes/no (% yes/no) |
| Steroids | 11/4 (73.0/27.0) |
| Cyclophosphamide | 0/15 (0.0/100.0) |
| Azathioprine | 2/13 (13.3/82.7) |
| Mycophenolate mofetil | 2/13 (13.3/82.7) |
| Methotrexate | 1/14 (6.7/93.3) |
| Cyclosporine | 0/15 (0/100) |
| Rituximab | 0/15 (0/100) |
| Plasmapheresis | 0/15 (0/100) |
| Cytokine | Active Mean (min–max); n = 23 | Remission Mean (min–max); n = 9 | * = p < 0.05; *** = p < 0.001; n.s. = not significant |
|---|---|---|---|
| ANCA | 331.39 (0.00−2048.00) | 141.33 (0.00−1024.00) | n.s. |
| BVAS | 8.52 (1.00−26.00) | 0.00 (0.00−0.00) | |
| CCL1 | 4.02 (1.19−10.80) | 3.37 (1.57−7.91) | n.s. |
| CCL15 | 2712.58 (322.19−5778.18) | 2764.14 (1252.99−6326.59) | n.s. |
| CCL17 | 50.60 (0.00−123.75) | 59.96 (7.03−125.37) | n.s. |
| CCL21 | 55.15 (0.00−256.08) | 42.15 (6.42 v 157.79) | n.s. |
| CCL27 | 369.37 (17.98−757.08) | 413.92 (148.57−1152.58) | n.s. |
| CRP | 15.93 (0.30−145.00) | 1.81 (1.00−3.00) | n.s. |
| CXCL12 | 1063.73 (317.83−3026.04) | 1071.81 (511.06−1878.92) | n.s. |
| CXCL13 | 22.10 (1.89−97.34) | 13.17 (3.22−29.82) | n.s. |
| CXCL5 | 507.91 (53.44−1315.25) | 552.03 (50.23−1290.88) | n.s. |
| Eotaxin-2 | 423.54 (85.43−655.17) | 456.92 (174.48−735.23) | n.s. |
| Eotaxin-3 | 40.93 (7.39−195.33) | 40.55 (18.40−152.34) | n.s. |
| IL-16 | 54.65 (11.47−193.47) | 57.99 (6.75−228.25) | n.s. |
| IL-20 | 48.95 (0.78−254.13) | 42.65 (13.16−153.65) | n.s. |
| IL-21 | 9.97 (0.00−70.53) | 4.17 (0.00−33.62) | n.s. |
| IL-23 | 650.77 (0.00−3511.30) | 431.55 (26.03−2295.86) | n.s. |
| IL-28A | 371.64 (0.00−3208.29) | 36.91 (0.00−158.17) | n.s. |
| IL-33 | 15.44 (0.00−109.11) | 6.07 (0.00−30.86) | n.s. |
| MCP-2 | 25.54 (9.47−50.23) | 26.82 (14.72−58.03) | n.s. |
| MCP-4 | 32.15 (7.87−100.94) | 30.06 (9.29−84.76) | n.s. |
| SCF | 35.99 (0.00−226.84) | 30.96 (3.85−178.01) | n.s. |
| TPO | 514.48 (105.91−1602.86) | 361.96 (199.93−1238.14) | n.s. |
| TRAIL | 60.49 (10.34−176.74) | 72.63 (16.45−238.06) | n.s. |
| TSLP | 4.83 (0.36−20.09) | 3.40 (0.44−19.08) | n.s. |
| creatinine | 178.00 (33.00-802.00) | 113.50 (74.00−282.00) | n.s. |
| hemoglobin | 13.19 (11.00−15.80) | 12.85 (11.10−14.20) | n.s. |
| leucocytes | 8.53 (2.00−17.40) | 5.70 (4.30−7.40) | |
| thrombocytes | 245.05 (13.00−591.00) | 228.62 (75.00−341.00) | n.s. |
| Cytokine | Active (ENT Affected) Mean (min–max); n = 12 | Inactive (ENT Not Affected) Mean (min–max); n = 11 | * = p < 0.05; n.s. = not significant |
|---|---|---|---|
| ANCA | 392.17 (2.00−2048.00) | 265.09 (0.00−2048.00) | n.s. |
| BVAS | 10.17 (2.00−26.00) | 6.73 (1.00−19.00) | n.s. |
| CCL1 | 4.50 (1.84−9.01) | 3.50 (1.19−10.80) | n.s. |
| CCL15 | 2921.78 (322.19−4627.90) | 2484.36 (349.69−5778.18) | n.s. |
| CCL17 | 57.56 (0.00−123.75) | 43.01 (15.50−94.13) | n.s. |
| CCL21 | 58.58 (5.03−198.89) | 51.42 (0.00−256.08) | n.s. |
| CCL27 | 429.99 (17.98−757.08) | 303.23 (51.00−482.23) | n.s. |
| CRP | 13.93 (1.00−32.00) | 18.13 (0.30−145.00) | n.s. |
| CXCL12 | 1289.93 (466.15−3026.04) | 816.95 (317.83−1434.82) | |
| CXCL13 | 19.63 (1.89−83.24) | 24.80 (3.73−97.34) | n.s. |
| CXCL5 | 539.80 (187.10−1315.25) | 473.13 (53.44−1067.55) | n.s. |
| Eotaxin-2 | 475.61 (211.65−655.17) | 366.74 (85.43−538.32) | n.s. |
| Eotaxin-3 | 45.06 (10.21−120.52) | 36.42 (7.39−195.33) | n.s. |
| IL-16 | 60.17 (15.89−193.47) | 48.63 (11.47−181.22) | n.s. |
| IL-20 | 52.25 (1.92−153.98) | 45.35 (0.78−254.13) | n.s. |
| IL-21 | 13.70 (0.00−70.53) | 5.90 (0.00−26.68) | n.s. |
| IL-23 | 830.31 (0.00−3511.30) | 453.28 (32.49−1629.89) | n.s. |
| IL-28A | 271.77 (0.00−2838.47) | 480.58 (0.00−3208.29) | n.s. |
| IL-33 | 17.42 (0.00−109.11) | 13.28 (0.00−64.37) | n.s. |
| MCP-2 | 30.62 (9.89−50.23) | 20.00 (9.47−34.15) | |
| MCP-4 | 39.28 (12.66−100.94) | 24.37 (7.87−50.07) | n.s. |
| SCF | 40.69 (0.03−226.84) | 30.87 (0.00−162.36) | n.s. |
| TPO | 604.01 (249.50−1602.86) | 416.00 (105.91−1556.27) | n.s. |
| TRAIL | 68.12 (15.70−176.74) | 52.16 (10.34−134.17) | n.s. |
| TSLP | 5.08 (0.46−20.09) | 4.55 (0.36−18.09) | n.s. |
| creatinine | 183.11 (33.00−802.00) | 173.40 (63.00−662.00) | n.s. |
| hemoglobin | 13.30 (11.30−15.80) | 13.06 (11.00−15.10) | n.s. |
| leucocytes | 9.14 (4.00−17.20) | 7.86 (2.00−17.40) | n.s. |
| thrombocytes | 247.27 (166.00−348.00) | 242.60 (13.00−591.00) | n.s. |
| Cytokine | Active (Kidney Affected) Mean (min–max); n = 7 | Inactive (Kidney Not Affected) Mean (min–max); n = 16 | * = p < 0.05; ** = p < 0.01; *** = p < 0.001; n.s. = not significant |
|---|---|---|---|
| ANCA | 246.86 (0.00−1024.00) | 368.38 (0.00−2048.00) | n.s. |
| BVAS | 12.86 (8.00−19.00) | 6.62 (1.00−26.00) | |
| CCL1 | 5.55 (2.35−10.80) | 3.35 (1.19−9.01) | |
| CCL15 | 3456.04 (322.19−5778.18) | 2387.32 (349.69−3909.46) | n.s. |
| CCL17 | 63.32 (0.00−123.75) | 45.03 (15.50−101.86) | n.s. |
| CCL21 | 75.05 (5.03−256.08) | 46.45 (0.00−198.89) | n.s. |
| CCL27 | 398.45 (17.98−757.08) | 356.64 (51.00−719.80) | n.s. |
| CRP | 14.53 (2.00−32.00) | 16.49 (0.30−145.00) | n.s. |
| CXCL12 | 1202.39 (466.15−3026.04) | 1003.06 (317.83−1823.04) | n.s. |
| CXCL13 | 31.09 (3.39−97.34) | 18.17 (1.89−83.24) | n.s. |
| CXCL5 | 434.64 (252.89−653.00) | 539.97 (53.44−1315.25) | n.s. |
| Eotaxin-2 | 463.00 (148.80−655.17) | 406.28 (85.43−579.55) | n.s. |
| Eotaxin-3 | 62.83 (26.21−195.33) | 31.34 (7.39−120.52) | n.s. |
| IL-16 | 93.63 (36.87−193.47) | 37.59 (11.47−113.97) | |
| IL-20 | 71.76 (1.92−254.13) | 38.97 (0.78−153.98) | n.s. |
| IL-21 | 25.61 (0.00−70.53) | 3.12 (0.00−19.06) | |
| IL-23 | 1666.17 (936.37−3511.30) | 244.61 (0.00−1086.40) | |
| IL-28A | 691.58 (28.11−2838.47) | 231.66 (0.0−3208.29) | |
| IL-33 | 37.87 (0.86−109.11) | 5.62 (0.00−32.29) | |
| MCP-2 | 35.13 (19.40−49.68) | 21.34 (9.47−50.23) | |
| MCP-4 | 40.06 (18.87−68.22) | 28.69 (7.87−100.94) | n.s. |
| SCF | 64.33 (16.12−226.84) | 23.60 (0.00−162.36) | |
| TPO | 962.79 (397.49−1602.86) | 335.15 (105.91−936.12) | |
| TRAIL | 64.21 (10.34−134.17) | 58.86 (15.70−176.74) | n.s. |
| TSLP | 10.00 (2.31−20.09) | 2.56 (0.36−9.27) | |
| creatinine | 294.50 (90.00−802.00) | 146.93 (33.00−662.00) | n.s. |
| hemoglobin | 13.59 (11.30−15.80) | 12.99 (11.00−15.00) | n.s. |
| leucocytes | 10.67 (2.00−17.20) | 7.46 (4.00−17.40) | n.s. |
| thrombocytes | 277.00 (13.00−591.00) | 229.07 (148.00−320.00) | n.s. |
| Cytokine | Active (Joints No Kidney) Mean (min–max); n = 4 | Inactive (Joints and Kidney) Mean (min–max); n = 5 | * = p < 0.05; n.s. = not significant | Active (No Joints No Kidney) Mean (min–max); n = 10 | Inactive (No Joints But Kidney) Mean (min–max); n = 3 | * = p < 0.05; n.s. = not significant |
|---|---|---|---|---|---|---|
| ANCA | 534.00 (8.00–2048.00) | 332.80 (128.00−1024.00) | n.s. | 324.60 (0.00−2048.00) | 106.67 (0.00−256.00) | n.s. |
| BVAS | 8.50 (1.00–13.00) | 10.40 (1.00−15.00) | n.s. | 6.50 (2.00−26.00) | 13.00 (8.00−19.00) | n.s. |
| CCL1 | 1.94 (1.19–3.43) | 3.62 (1.96−6.39) | n.s. | 4.02 (2.01−9.01) | 7.57 (5.44−10.80) | n.s. |
| CCL15 | 2976.61 (2568.80–3315.45) | 2289.54 (322.19−4627.90) | n.s. | 2327.43 (641.91−3909.46) | 4364.76 (2905.70−5778.18) | n.s. |
| CCL17 | 26.20 (15.50–55.75) | 50.11 (0.00−111.88) | n.s. | 52.83 (23.63−101.86) | 80.42 (46.15−123.75) | n.s. |
| CCL21 | 17.33 (0.00–34.27) | 48.58 (5.03−97.60) | n.s. | 62.04 (19.52−198.89) | 106.35 (22.95−256.08) | n.s. |
| CCL27 | 342.61 (271.61–418.81) | 311.34 (17.98−757.08) | n.s. | 380.26 (148.97−719.80) | 427.81 (285.22−544.34) | n.s. |
| CRP | 13.00 (1.00–30.00) | 12.88 (0.30−32.00) | n.s. | 20.44 (1.00−145.00) | 12.00 (2.00−22.00) | n.s. |
| CXCL12 | 1007.10 (599.82–1743.66) | 1141.71 (340.77−3026.04) | n.s. | 1067.62 (317.83−1823.04) | 1016.31 (811.75−1188.45) | n.s. |
| CXCL13 | 31.48 (8.27–83.24) | 17.69 (3.73−50.68) | n.s. | 15.41 (1.89−37.34) | 44.29 (3.39−97.34) | n.s. |
| CXCL5 | 320.69 (53.44–616.89) | 566.66 (252.89−1067.55) | n.s. | 598.01 (265.18−1315.25) | 425.59 (263.14−653.00) | n.s. |
| Eotaxin-2 | 457.93 (385.44–512.80) | 506.24 (279.14−655.17) | n.s. | 403.04 (85.43−579.55) | 408.84 (148.80−591.91) | n.s. |
| Eotaxin-3 | 16.04 (10.21–28.20) | 39.47 (23.18−61.75) | 40.68 (9.52−120.52) | 88.54 (26.21−195.33) | n.s. | |
| IL-16 | 24.80 (11.47–55.82) | 70.72 (12.83−193.47) | n.s. | 47.12 (15.16−113.97) | 104.89 (59.74−181.22) | n.s. |
| IL-20 | 29.92 (11.49–60.34) | 36.54 (0.78−106.11) | n.s. | 48.89 (5.52−153.98) | 106.79 (24.76−254.13) | n.s. |
| IL-21 | 0.91 (0.00–2.25) | 27.80 (0.00−70.53) | n.s. | 2.73 (0.00−15.76) | 19.79 (11.34−26.68) | |
| IL-23 | 129.77 (0.00–283.89) | 1923.25 (936.37−3511.30) | 310.62 (32.49−1086.40) | 1409.08 (1202.54−1629.89) | ||
| IL-28A | 8.70 (0.00–25.75) | 1240.53 (30.44−3208.29) | 46.35 (2.35−154.89) | 615.55 (28.11−1752.20) | n.s. | |
| IL-33 | 2.37 (0.00–5.33) | 29.47 (0.66−109.11) | n.s. | 7.92 (0.00−32.29) | 39.47 (10.60−64.37) | n.s. |
| MCP-2 | 18.40 (9.47−23.15) | 34.33 (23.90−49.68) | 22.45 (9.89−50.23) | 33.28 (19.40−46.30) | n.s. | |
| MCP-4 | 15.91 (12.19−20.27) | 34.44 (18.87−68.22) | n.s. | 36.28 (7.87−100.94) | 43.84 (25.32−56.12) | n.s. |
| SCF | 13.02 (0.03–38.20) | 97.29 (24.81−226.84) | n.s. | 15.31 (0.00−44.29) | 42.06 (16.12−67.11) | n.s. |
| TPO | 259.73 (197.29−295.80) | 1034.02 (517.19−1602.86) | 372.78 (105.91−936.12) | 891.56 (397.49−1556.27) | n.s. | |
| TRAIL | 25.52 (15.70−37.82) | 64.03 (37.96−86.78) | 72.06 (21.12−176.74) | 63.11 (10.34−134.17) | n.s. | |
| TSLP | 1.32 (0.46−2.09) | 9.79 (4.04−20.09) | 2.60 (0.36−9.27) | 9.98 (2.31−18.09) | n.s. | |
| creatinine | 164.50 (76.00−311.00) | 534.67 (140.00−802.00) | n.s. | 85.56 (33.00−126.00) | 118.00 (90.00−146.00) | n.s. |
| hemoglobin | 12.65 (11.90−13.70) | 14.30 (11.50−15.80) | n.s. | 12.79 (11.00−15.00) | 12.83 (11.30−15.10) | n.s. |
| leucocytes | 10.43 (4.70−17.40) | 9.60 (5.70−15.40) | n.s. | 6.44 (4.00−11.10) | 10.80 (2.00−17.20) | n.s. |
| thrombocytes | 235.50 (170.00−320.00) | 253.20 (212.00−348.00) | n.s. | 228.62 (148.00−316.00) | 298.33 (13.00−591.00) | n.s. |
| Cytokine | Active (No Lung No Kidney) Mean (min–max); n = 12 | Inactive (No Lung But Kidney) Mean (min–max); n = 6 | * = p < 0.05; ** = p < 0.01; *** = p < 0.001; n.s. = not significant |
|---|---|---|---|
| ANCA | 317.50 (0.00−2048.00) | 266.67 (0.00−1024.00) | n.s. |
| BVAS | 4.92 (1.00−13.00) | 13.00 (8.00−19.00) | |
| CCL1 | 3.02 (1.19−8.10) | 5.82 (2.35−10.80) | |
| CCL15 | 2489.85 (349.69−3909.46) | 3663.79 (322.19−5778.18) | n.s. |
| CCL17 | 47.31 (15.50−101.86) | 71.40 (0.00−123.75) | n.s. |
| CCL21 | 36.44 (0.00−104.05) | 76.54 (5.03−256.08) | n.s. |
| CCL27 | 365.16 (51.00−719.80) | 413.19 (17.98−757.08) | n.s. |
| CRP | 8.94 (0.30−30.00) | 14.53 (2.00−32.00) | n.s. |
| CXCL12 | 1033.10 (340.77−1743.66) | 1286.24 (466.15−3026.04) | n.s. |
| CXCL13 | 18.39 (1.89−83.24) | 32.43 (3.39−97.34) | n.s. |
| CXCL5 | 488.43 (53.44−1067.55) | 445.46 (252.89−653.00) | n.s. |
| Eotaxin-2 | 405.71 (121.68−579.55) | 454.58 (148.80−655.17) | n.s. |
| Eotaxin-3 | 27.34 (7.39−69.56) | 63.89 (26.21−195.33) | n.s. |
| IL-16 | 29.17 (11.47−97.75) | 100.36 (36.87 − 193.47) | |
| IL-20 | 30.90 (0.78−95.20) | 74.97 (1.92−254.13) | n.s. |
| IL-21 | 2.55 (0.00−19.06) | 18.13 (0.00−29.46) | |
| IL-23 | 151.86 (0.00−361.18) | 1297.14 (936.37−629.89) | |
| IL-28A | 280.65 (0.00−3208.29) | 801.76 (28.11−2838.47) | |
| IL-33 | 2.84 (0.00−12.26) | 26.00 (0.86−64.37) | |
| MCP-2 | 21.21 (9.47−50.23) | 34.44 (19.40−49.68) | |
| MCP-4 | 24.78 (9.23−43.05) | 43.59 (25.32−68.22) | |
| SCF | 25.84 (0.03−162.36) | 70.91 (16.12−226.84) | |
| TPO | 305.82 (177.72−891.44) | 834.78 (397.49−1556.27) | |
| TRAIL | 58.21 (15.70−176.74) | 66.41 (10.34−134.17) | n.s. |
| TSLP | 2.11 (0.46−8.86) | 8.32 (2.31−18.09) | |
| creatinine | 174.45 (33.00−662.00) | 294.50 (90.00−802.00) | n.s. |
| hemoglobin | 13.26 (11.80−15.00) | 13.93 (11.30−15.80) | n.s. |
| leucocytes | 7.74 (4.00−17.40) | 10.90 (2.00−17.20) | n.s. |
| thrombocytes | 222.10 (166.00−320.00) | 280.50 (13.00−591.00) | n.s. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Müller-Deile, J.; Jaremenko, C.; Haller, H.; Schiffer, M.; Haubitz, M.; Christiansen, S.; Falk, C.; Schiffer, L. Chemokine/Cytokine Levels Correlate with Organ Involvement in PR3-ANCA-Associated Vasculitis. J. Clin. Med. 2021, 10, 2715. https://doi.org/10.3390/jcm10122715
Müller-Deile J, Jaremenko C, Haller H, Schiffer M, Haubitz M, Christiansen S, Falk C, Schiffer L. Chemokine/Cytokine Levels Correlate with Organ Involvement in PR3-ANCA-Associated Vasculitis. Journal of Clinical Medicine. 2021; 10(12):2715. https://doi.org/10.3390/jcm10122715
Chicago/Turabian StyleMüller-Deile, Janina, Christian Jaremenko, Hermann Haller, Mario Schiffer, Marion Haubitz, Silke Christiansen, Christine Falk, and Lena Schiffer. 2021. "Chemokine/Cytokine Levels Correlate with Organ Involvement in PR3-ANCA-Associated Vasculitis" Journal of Clinical Medicine 10, no. 12: 2715. https://doi.org/10.3390/jcm10122715
APA StyleMüller-Deile, J., Jaremenko, C., Haller, H., Schiffer, M., Haubitz, M., Christiansen, S., Falk, C., & Schiffer, L. (2021). Chemokine/Cytokine Levels Correlate with Organ Involvement in PR3-ANCA-Associated Vasculitis. Journal of Clinical Medicine, 10(12), 2715. https://doi.org/10.3390/jcm10122715