The Relationship Between Obesity Status and Body Image Dissatisfaction on Gross Motor Skill Development and Cardiorespiratory Fitness in Children Aged 6–12 Years Old

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
Participants
2.2. Anthropometric Measures
2.3. Cardiorespiratory Fitness Test
2.4. Body Image Perception
2.5. Gross Motor Skill Tests
2.5.1. Segmental Speed (2 Tests)
2.5.2. Agility (4 Tests)
2.5.3. Balance (2 Tests)
2.5.4. Reaction Time (1 Test)
2.5.5. Coordination (3 Tests)
2.5.6. Statistical Analysis
3. Results
4. Discussion
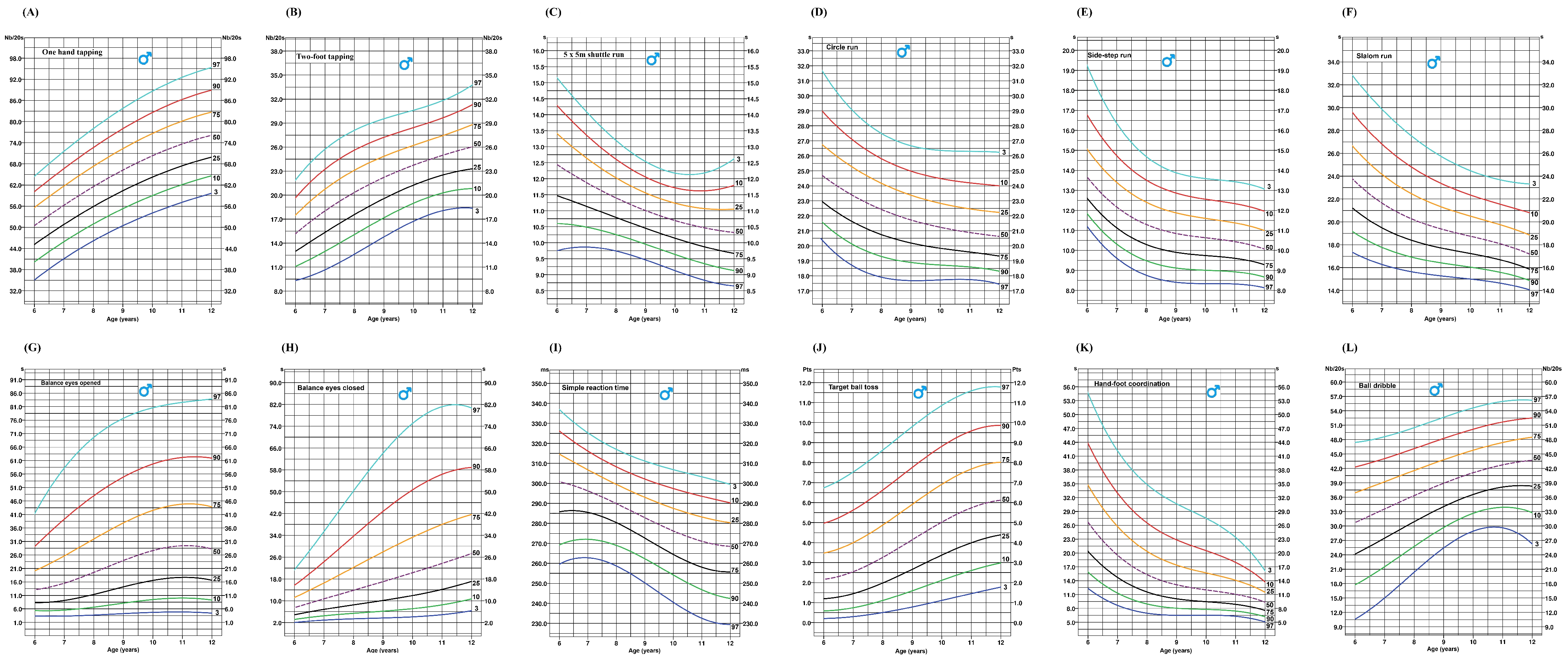
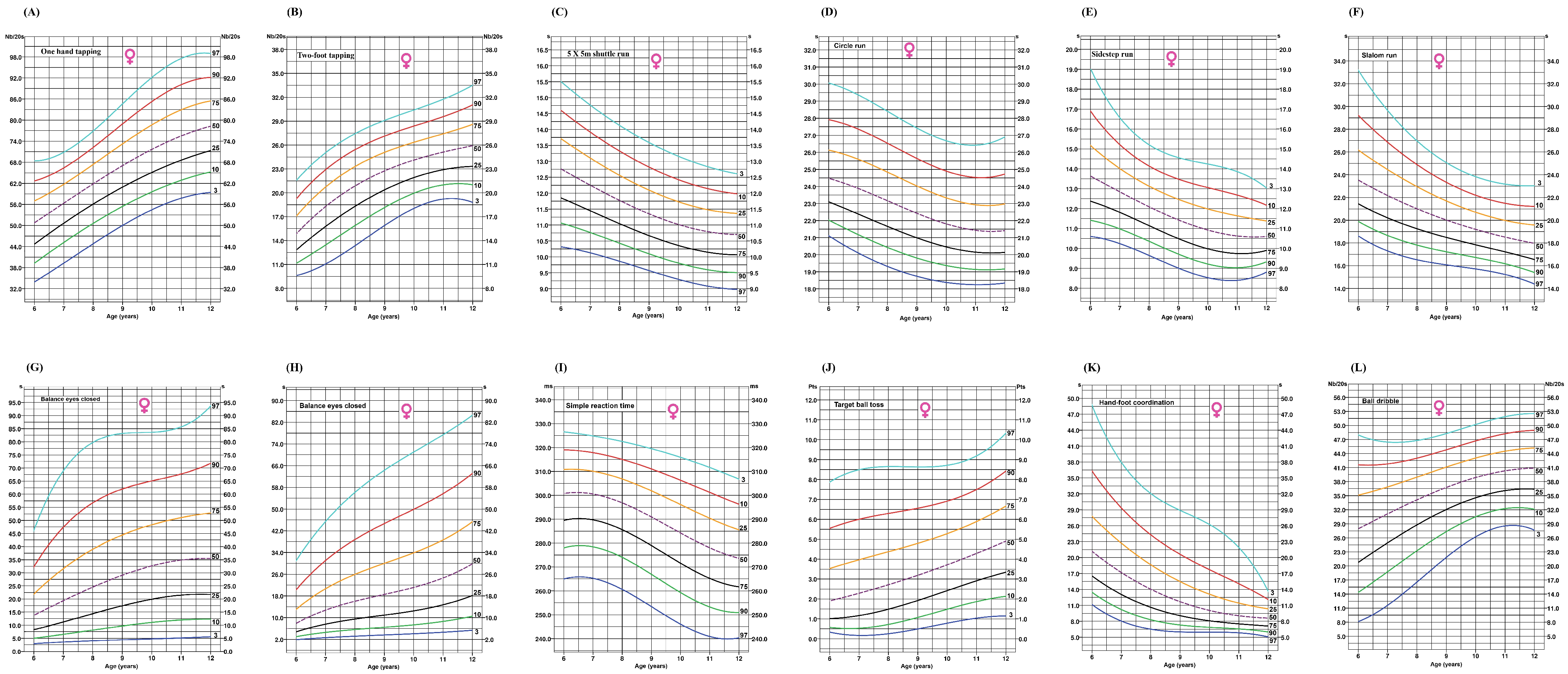
4.1. Reference Values for the Development of Gross Motor Skills in Children
4.2. Impact of Gross Motor Skills Development and Cardiorespiratory Fitness on Body Image Dissatisfaction
4.3. Relationship Between Obesity Status and Gross Motor Skills Competence
Strengths and Limits
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hardy, L.L.; Reinten-Reynolds, T.; Espinel, P.; Zask, A.; Okely, A.D. Prevalence and correlates of low fundamental movement skill competency in children. Pediatrics 2012, 130, e390–e398. [Google Scholar] [CrossRef] [PubMed]
- Janacsek, K.; Fiser, J.; Nemeth, D. The best time to acquire new skills: Age-related differences in implicit sequence learning across the human lifespan. Dev. Sci. 2012, 15, 496–505. [Google Scholar] [CrossRef]
- Missiuna, C.; Moll, S.; King, G.; Stewart, D.; Macdonald, K. Life experiences of young adults who have coordination difficulties. Can. J. Occup. Ther. 2008, 75, 157–166. [Google Scholar] [CrossRef]
- Losse, A.; Henderson, S.E.; Elliman, D.; Hall, D.; Knight, E.; Jongmans, M. Clumsiness in Children—Do They Grow Out of It? A 10-Year Follow-Up Study. Dev. Med. Child Neurol. 1991, 33, 55–68. [Google Scholar] [CrossRef]
- Rizzo, N.S.; Ruiz, J.R.; Hurtig-Wennlöf, A.; Ortega, F.B.; Sjöström, M. Relationship of physical activity, fitness, and fatness with clustered metabolic risk in children and adolescents: The European youth heart study. J. Pediatr. 2007, 150, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Stabelini Neto, A.; Sasaki, J.E.; Mascarenhas, L.P.; Boguszewski, M.C.S.; Bozza, R.; Ulbrich, A.Z.; da Silva, S.G.; de Campos, W. Physical activity, cardiorespiratory fitness, and metabolic syndrome in adolescents: A cross-sectional study. BMC Public Health 2011, 11, 674. [Google Scholar] [CrossRef]
- Viner, R.M.; Ozer, E.M.; Denny, S.; Marmot, M.; Resnick, M.; Fatusi, A.; Currie, C. Adolescence and the Social Determinants of Health. Lancet 2012, 379, 1641–1652. [Google Scholar] [CrossRef] [PubMed]
- Telama, R. Tracking of Physical Activity from Childhood to Adulthood: A Review. Obes. Facts 2009, 2, 187–195. [Google Scholar] [CrossRef]
- Yao, C.A.; Rhodes, R.E. Parental correlates in child and adolescent physical activity: A meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 10. [Google Scholar] [CrossRef]
- Mori, S.; Nakamoto, H.; Mizuochi, H.; Ikudome, S.; Gabbard, C. Influence of affordances in the home environment on motor development of young children in Japan. Child Dev. Res. 2013, 2013, 898406. [Google Scholar] [CrossRef]
- Shonkoff, J.P.; Boyce, W.T.; McEwen, B.S. Neuroscience, molecular biology, and the childhood roots of health disparities. JAMA 2009, 301, 2252–2259. [Google Scholar] [CrossRef] [PubMed]
- Barnett, L.M.; Lai, S.K.; Veldman, S.L.C.; Hardy, L.L.; Cliff, D.P.; Morgan, P.J.; Zask, A.; Lubans, D.R.; Shultz, S.P.; Ridgers, N.D.; et al. Correlates of gross motor competence in children and adolescents: A systematic review and meta-analysis. Sports Med. 2016, 46, 1663–1688. [Google Scholar] [CrossRef] [PubMed]
- Hands, B. Changes in motor skill and fitness measures among children with high and low motor competence: A five-year longitudinal study. J. Sci. Med. Sport 2008, 11, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Bryant, E.S.; Duncan, M.J.; Birch, S.L. Fundamental movement skills and weight status in British primary school children. Eur. J. Sport Sci. 2014, 14, 730–736. [Google Scholar] [CrossRef]
- Barros, W.M.A.; Silva, K.G.D.; Silva, R.K.P.; da Silva Souza, A.P.; da Silva, A.B.J.; Silva, M.R.M.; de Sousa Fernandes, M.S.; de Souza, S.L.; de Oliveira Nogueira Souza, V. Effects of overweight/obesity on motor performance in children: A systematic review. Front. Endocrinol. 2022, 12, 759165. [Google Scholar] [CrossRef]
- Cheng, J.; East, P.; Blanco, E.; Sim, E.K.; Castillo, M.; Lozoff, B.; Gahagan, S. Obesity leads to declines in motor skills across childhood. Child Care Health Dev. 2016, 42, 343–450. [Google Scholar] [CrossRef]
- Cliff, D.P.; Okely, A.D.; Morgan, P.J.; Jones, R.A.; Steele, J.R.; Baur, L.A. Proficiency deficiency: Mastery of fundamental movement skills and skill components in overweight and obese children. Obesity 2012, 20, 1024–1033. [Google Scholar] [CrossRef]
- Leone, M.; Bui, H.T.; Kalinova, E.; Bourget-Gaudreault, S.; Levesque, P.; Lemoyne, J.; Gagnon, D.; Larivière, G.; Léger, L.; Allisse, M. Updating normative cross-sectional values and secular trends in body mass, body height and body mass index among Québec children and adolescents. Can. J. Public Health 2023, 114, 629–641. [Google Scholar] [CrossRef]
- Malina, R.M. Top 10 research questions related to growth and maturation of relevance to physical activity, performance, and fitness. Res. Q. Exerc. Sport 2014, 85, 157–173. [Google Scholar] [CrossRef]
- D’Hondt, E.; Deforche, B.; De Bourdeaudhuij, I.; Lenoir, M. Childhood obesity affects fine motor skill performance under different postural constraints. Neurosci. Lett. 2008, 440, 72–75. [Google Scholar] [CrossRef]
- Calcaterra, V.; Marin, L.; Vandoni, M.; Rossi, V.; Pirazzi, A.; Grazi, R.; Patané, P.; Silvestro, G.S.; Pellino, V.C.; Albanese, I.; et al. Childhood obesity and incorrect body posture: Impact on physical activity and the therapeutic role of exercise. Int. J. Environ. Res. Public Health 2022, 19, 16728. [Google Scholar] [CrossRef] [PubMed]
- Deforche, B.I.; Hills, A.P.; Worringham, C.J.; Davies, P.S.; Murphy, A.J.; Bouckaert, J.J.; De Bourdeaudhuij, I.M. Balance and postural skills in normal-weight and overweight prepubertal boys. Int. J. Pediatr. Obes. 2009, 4, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, L.P.; Stodden, D.F.; Lopes, V.P. Developmental pathways of change in fitness and motor competence are related to overweight and obesity status at the end of primary school. J. Sci. Med. Sport 2016, 19, 87–92. [Google Scholar] [CrossRef]
- Thomas, F.; Bean, K.; Pannier, B.; Oppert, J.M.; Guize, L.; Benetos, A. Cardiovascular mortality in overweight subjects: The key role of associated risk factors. Hypertension 2005, 46, 654–659. [Google Scholar] [CrossRef]
- Venetsanou, F.; Kambas, A. Environmental factors affecting preschoolers’ motor development. Early Child. Educ. J. 2009, 37, 10. [Google Scholar] [CrossRef]
- Newell, K.M. Constraints on the Development of Coordination. In Motor Development in Children Aspects of Coordination and Control; Wade, M.G., Whiting, H.T.A., Eds.; Martinus Nijhoff: Leiden, The Netherlands, 1986. [Google Scholar] [CrossRef]
- Largo, R.H.; Fischer, J.E.; Rousson, V. Neuromotor development from kindergarten age to adolescence: Developmental course and variability. Swiss Med. Wkly. 2003, 133, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Vandorpe, B.; Vandendriessche, J.; Lefevre, J.; Pion, J.; Vaeyens, R.; Matthys, S.; Philippaerts, R.; Lenoir, M. The Körperkoordinations Test für Kinder: Reference values and suitability for 6-12-year-old children in Flanders. Scand. J. Med. Sci. Sports 2011, 21, 378–388. [Google Scholar] [CrossRef]
- D’Hondt, E.; Deforche, B.; Vaeyens, R.; Vandorpe, B.; Vandendriessche, J.; Pion, J.; Philippaerts, R.; de Bourdeaudhuij, I.; Lenoir, M. Gross motor coordination in relation to weight status and age in 5- to 12-year-old boys and girls: A cross-sectional study. Int. J. Pediatr. Obes. 2011, 6, e556–e564. [Google Scholar] [CrossRef]
- Lopes, L.; Santos, R.; Pereira, B.; Lopes, V.P. Associations between gross motor coordination and academic achievement in elementary school children. Hum. Mov. Sci. 2013, 32, 9–20. [Google Scholar] [CrossRef]
- Cash, T.F. (Ed.) Body Image: A Handbook of Theory, Research, and Clinical Practice; Guilford Press: New York, NY, USA, 2004; paperback edition. [Google Scholar]
- McLean, S.A.; Paxton, S.J. Body image in the context of eating disorders. Psychiatr. Clin. N. Am. 2019, 42, 145–156. [Google Scholar] [CrossRef]
- Quittkat, H.L.; Hartmann, A.S.; Düsing, R.; Buhlmann, U.; Vocks, S. Body dissatisfaction, importance of appearance, and body appreciation in men and women over the lifespan. Front. Psychiatry 2019, 10, 864. [Google Scholar] [CrossRef]
- Thompson, J.K.; Heinberg, L.J.; Altabe, M.; Tantleff-Dunn, S. Exacting Beauty: Theory, Assessment, and Treatment of Body Image Disturbance; American Psychological Association: Washington, DC, USA, 1999. [Google Scholar] [CrossRef]
- Andrew, R.; Tiggemann, M.; Clark, L. The protective role of body appreciation against media-induced body dissatisfaction. Body Image 2015, 15, 98–104. [Google Scholar] [CrossRef]
- Cash, T.F.; Smolak, L. (Eds.) Body Image: A Handbook of Science, Practice, and Prevention, 2nd ed.; Guilford Press: New York, NY, USA, 2012. [Google Scholar]
- Tylka, T.L. Positive psychology perspectives on body image. In Encyclopedia of Body Image and Human Appearance; Elsevier: Amsterdam, The Netherlands, 2012; pp. 657–663. [Google Scholar] [CrossRef]
- Wood-Barcalow, N.L.; Tylka, T.L.; Augustus-Horvath, C.L. “But I Like My Body”: Positive body image characteristics and a holistic model for young-adult women. Body Image 2010, 7, 106–116. [Google Scholar] [CrossRef]
- Garner, D.M. Eating Disorder Inventory-3; Psychological Assessment Ressources, Inc.: Lutz, FL, USA, 2004. [Google Scholar]
- Canpolat, B.I.; Orsel, S.; Akdemir, A.; Ozbay, M.H. The relationship between dieting and body image, body ideal, self-perception, and body mass index in Turkish adolescents. Int. J. Eat. Disord. 2005, 37, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Cooper, P.J.; Taylor, M.J. Body image disturbance in bulimia nervosa. Br. J. Psychiatry 1988, 153, 32–36. [Google Scholar] [CrossRef]
- Grabe, S.; Ward, L.M.; Hyde, J.S. The role of the media in body image concerns among women: A meta-analysis of experimental and correlational studies. Psychol. Bull. 2008, 134, 460–476. [Google Scholar] [CrossRef] [PubMed]
- Groesz, L.M.; Levine, M.P.; Murnen, S.K. The effect of experimental presentation of thin media images on body satisfaction: A meta-analytic review. Int. J. Eat. Disord. 2002, 31, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Heider, N.; Spruyt, A.; De Houwer, J. Body dissatisfaction revisited: On the importance of implicit beliefs about actual and ideal body image. Psychol. Belg. 2018, 57, 158. [Google Scholar] [CrossRef]
- Hill, M.L.; Masuda, A.; Latzman, R.D. Body image flexibility as a protective factor against disordered eating behavior for women with lower body mass index. Eat. Behav. 2013, 14, 336–341. [Google Scholar] [CrossRef]
- Mishina, K.; Kronström, K.; Heinonen, E.; Sourander, A. Body dissatisfaction and dieting among Finnish adolescents: A 20-year population-based time-trend study. Eur. Child Adolesc. Psychiatry 2024, 33, 2605–2614. [Google Scholar] [CrossRef]
- Strauman, T.J.; Vookles, J.; Berenstein, V.; Chaiken, S.; Higgins, E.T. Self-discrepancies and vulnerability to body dissatisfaction and disordered eating. J. Pers. Soc. Psychol. 1991, 61, 946–956. [Google Scholar] [CrossRef] [PubMed]
- Streatfeild, J.; Hickson, J.; Austin, S.B.; Hutcheson, R.; Kandel, J.S.; Lampert, J.G.; Myers, E.M.; Richmond, T.K.; Samnaliev, M.; Velasquez, K.; et al. Social and economic cost of eating disorders in the United States: Evidence to inform policy action. Int. J. Eat. Disord. 2021, 54, 851–868. [Google Scholar] [CrossRef]
- Crespo, C.; Kielpikowski, M.; Jose, P.E.; Pryor, J. Relationships between family connectedness and body satisfaction: A longitudinal study of adolescent girls and boys. J. Youth Adolesc. 2010, 39, 1392–1401. [Google Scholar] [CrossRef]
- Kostanski, M.; Gullone, E. Dieting and body image in the child’s world: Conceptualization and behavior. J. Genet. Psychol. 1999, 160, 488. [Google Scholar] [CrossRef]
- Stice, E.; Marti, C.N.; Durant, S. Risk factors for onset of eating disorders: Evidence of multiple risk pathways from an 8-year prospective study. Behav. Res. Ther. 2011, 49, 622–627. [Google Scholar] [CrossRef] [PubMed]
- Stice, E.; Bearman, S.K. Body-image and eating disturbances prospectively predict increases in depressive symptoms in adolescent girls: A growth curve analysis. Dev. Psychol. 2001, 37, 597–607. [Google Scholar] [CrossRef] [PubMed]
- Stice, E.; Shaw, H.E. Role of body dissatisfaction in the onset and maintenance of eating pathology. J. Psychosom. Res. 2002, 53, 985–993. [Google Scholar] [CrossRef]
- Yanover, T.; Thompson, J.K. Eating problems, body image disturbances, and academic achievement: Preliminary evaluation of the eating and body image disturbances academic interference scale. Int. J. Eat. Disord. 2008, 41, 184–187. [Google Scholar] [CrossRef]
- Al Sabbah, H.; Vereecken, C.A.; Elgar, F.J.; Nansel, T.; Aasvee, K.; Abdeen, Z.; Ojala, K.; Ahluwalia, N.; Maes, L. Body weight dissatisfaction and communication with parents among adolescents in 24 countries: International cross-sectional survey. BMC Public Health 2009, 9, 52. [Google Scholar] [CrossRef]
- Carter, A.; Forrest, J.I.; Kaida, A. Association between internet use and body dissatisfaction among young females: Cross-sectional analysis of the Canadian community health survey. J. Med. Internet Res. 2017, 19, e39. [Google Scholar] [CrossRef]
- Bucchianeri, M.; Neumark-Sztainer, D. Body dissatisfaction: An overlooked public health concern. J. Public Ment. Health 2014, 13, 64–69. [Google Scholar] [CrossRef]
- Neumark-Sztainer, D.; Goeden, C.; Story, M.; Wall, M. Associations between Body Satisfaction and Physical Activity in Adolescents: Implications for programs aimed at preventing a broad spectrum of weight-related disorders. Eat. Disord. 2004, 12, 125–137. [Google Scholar] [CrossRef] [PubMed]
- Presnell, K.; Bearman, S.K.; Stice, E. Risk factors for body dissatisfaction in adolescent boys and girls: A prospective study. Int. J. Eat. Disord. 2004, 36, 389–401. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.B.; Haynos, A.F.; Wall, M.M.; Chen, C.; Eisenberg, M.E.; Neumark-Sztainer, D. Fifteen-year prevalence, trajectories, and predictors of body dissatisfaction from adolescence to middle adulthood. Clin. Psychol. Sci. 2019, 7, 1403–1415. [Google Scholar] [CrossRef]
- D’Hondt, E.; Deforche, B.; Gentier, I.; De Bourdeaudhuij, I.; Vaeyens, R.; Philippaerts, R.; Lenoir, M. A longitudinal analysis of gross motor coordination in overweight and obese children versus normal-weight peers. Int. J. Obes. 2013, 37, 61–67. [Google Scholar] [CrossRef]
- Gentier, I.; D’Hondt, E.; Shultz, S.; Deforche, B.; Augustijn, M.; Hoorne, S.; Verlaecke, K.; De Bourdeaudhuij, I.; Lenoir, M. Fine and gross motor skills differ between healthy-weight and obese children. Res. Dev. Disabil. 2013, 34, 4043–4051. [Google Scholar] [CrossRef]
- Lopes, V.P.; Stodden, D.F.; Rodrigues, L.P. Weight status is associated with cross-sectional trajectories of motor co-ordination across childhood. Child Care Health Dev. 2014, 40, 891–899. [Google Scholar] [CrossRef]
- Wrotniak, B.H.; Epstein, L.H.; Dorn, J.M.; Jones, K.E.; Kondilis, V.A. The relationship between motor proficiency and physical activity in children. Pediatrics 2006, 118, e1758–e1765. [Google Scholar] [CrossRef]
- Ballarin, G.; Gallè, F.; Dinacci, L.; Liberti, F.; Cunti, A.; Valerio, G. Self-perception profile, body image perception and satisfaction in relation to body mass index: An Investigation in a Sample of Adolescents from the Campania Region, Italy. Children 2024, 11, 805. [Google Scholar] [CrossRef]
- Dion, J.; Hains, J.; Vachon, P.; Plouffe, J.; Laberge, L.; Perron, M.; McDuff, P.; Kalinova, E.; Leone, M. Correlates of body dissatisfaction in children. J. Pediatr. 2016, 171, 202–207. [Google Scholar] [CrossRef]
- King, J.E.; Jebeile, H.; Garnett, S.P.; Baur, L.A.; Paxton, S.J.; Gow, M.L. Physical activity based pediatric obesity treatment, depression, self-esteem and body image: A systematic review with meta-analysis. Ment. Health Phys. Act. 2020, 19, 100342. [Google Scholar] [CrossRef]
- Markey, C.N. Why body image is important to adolescent development. J. Youth Adolesc. 2010, 39, 1387–1391. [Google Scholar] [CrossRef] [PubMed]
- Weinberger, N.A.; Kersting, A.; Riedel-Heller, S.G.; Luck-Sikorski, C. Body Dissatisfaction in Individuals with obesity compared to normal-weight individuals: A systematic review and meta-analysis. Obes. Facts 2016, 9, 424–441. [Google Scholar] [CrossRef]
- Wardle, J.; Cooke, L. The impact of obesity on psychological well-being. Best Pract. Res. Clin. Endocrinol. Metab. 2005, 19, 421–440. [Google Scholar] [CrossRef] [PubMed]
- Colella, D.; Morano, M.; Robazza, C.; Bortoli, L. Body image, perceived physical ability, and motor performance in nonoverweight and overweight Italian children. Percept. Mot. Skills 2009, 108, 209–218. [Google Scholar] [CrossRef]
- Morano, M.; Colella, D.; Capranica, L. Body image, perceived and actual physical abilities in normal-weight and overweight boys involved in individual and team sports. J. Sports Sci. 2011, 29, 355–362. [Google Scholar] [CrossRef]
- Morano, M.; Colella, D.; Robazza, C.; Bortoli, L.; Capranica, L. Physical self-perception and motor performance in normal-weight, overweight and obese children. Scand. J. Med. Sci. Sports 2011, 21, 465–473. [Google Scholar] [CrossRef]
- Carlman, P.; Wagnsson, S.; Patriksson, G. Causes and consequences of dropping out from organized youth sports. Swed. J. Sports Res. 2013, 2, 26–54. [Google Scholar]
- Crane, J.; Temple, V. A systematic review of dropout from organized sport among children and youth. Eur. Phys. Educ. Rev. 2015, 21, 114–131. [Google Scholar] [CrossRef]
- Field, A.E.; Cheung, L.; Wolf, A.M.; Herzog, D.B.; Gortmaker, S.L.; Colditz, G.A. Exposure to the mass media and weight concerns among girls. Pediatrics 1999, 103, E36. [Google Scholar] [CrossRef]
- Foley Davelaar, C.M. Body image and its role in physical activity: A systematic review. Cureus 2021, 13, e13379. [Google Scholar] [CrossRef] [PubMed]
- Jensen, C.D.; Steele, R.G. Body dissatisfaction, weight criticism, and self-reported physical activity in preadolescent children. J. Pediatr. Psychol. 2009, 34, 822–826. [Google Scholar] [CrossRef]
- Lohman, T.G.; Roche, A.F.; Martorell, R. Anthropometric Standardization Reference Manual; Human Kinetics Books: Champaign, IL, USA, 1988. [Google Scholar]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [PubMed]
- Léger, L.A.; Mercier, D.; Gadoury, C.; Lambert, J. The multistage 20 metre shuttle run test for aerobic fitness. J. Sports Sci. 1988, 6, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Thompson, M.A.; Gray, J.J. Development and validation of a new body image assessment scale. J. Pers. Assess. 1995, 64, 258–269. [Google Scholar] [CrossRef]
- Barrow, H.M.; McGee, R.A. A Practical Approach to Measurement in Physical Education; Lea and Febiger: Washington, DC, USA, 1971. [Google Scholar]
- Fleishman, E.A. The Structure and Measurement of Physical Fitness; Prentice-Hall: Englewood Cliffs, NJ, USA, 1964. [Google Scholar]
- Strand, B.N.; Wilson, R. Assessing Sport Skills; Human Kinetics Publishers: Champaign, IL, USA, 1993. [Google Scholar]
- Hulteen, R.M.; Barnett, L.M.; True, L.; Lander, N.J.; Del Pozo Cruz, B.; Lonsdale, C. Validity and reliability evidence for motor competence assessments in children and adolescents: A systematic review. J. Sports Sci. 2020, 38, 1717–1798. [Google Scholar] [CrossRef]
- World Health Organization. WHO Child Growth Standards: Length/height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age: Methods and Development; World Health Organization: Geneva, Switzerland, 2006. Available online: https://www.who.int/tools/child-growth-standards/standards (accessed on 10 November 2024).
- Hoaglin, D.C.; Iglewicz, B. Fine tuning some resistant rules for outlier labeling. J. Am. Stat. Assoc. 1987, 82, 1147–1149. [Google Scholar] [CrossRef]
- Cole, T.J.; Green, P.J. Smoothing reference centile curves: The LMS method and penalized likelihood. Stat. Med. 1992, 11, 1305–1319. [Google Scholar] [CrossRef]
- Lowrey, G.H. Growth and Development of Children; Year Book Medical: Chicago, IL, USA, 1986. [Google Scholar]
- Pääsuke, M.; Ereline, J.; Gapeyeva, H.; Toots, M.; Toots, L. Comparison of twitch contractile properties of plantar flexor muscles in 9–10-year-old girls and boys. Pediatr. Exerc. Sci. 2003, 15, 324–332. [Google Scholar] [CrossRef]
- Tomazin, K.; Skof, B.; Dolenec, A.; Coh, M. Gender-related differences in maximum mechanical power output in short-term activities in children and adolescents. Coll. Antropol. 2008, 32, 821–828. [Google Scholar] [PubMed]
- Gosselin, V.; Leone, M.; Laberge, S. Socioeconomic and gender-based disparities in the motor competence of school-age children. J. Sports Sci. 2021, 39, 341–350. [Google Scholar] [CrossRef] [PubMed]
- Larson, J.C.; Mostofsky, S.H.; Goldberg, M.C.; Cutting, L.E.; Denckla, M.B.; Mahone, E.M. Effects of gender and age on motor exam in typically developing children. Dev. Neuropsychol. 2007, 32, 543–562. [Google Scholar] [CrossRef]
- Smits-Engelsman, B.; Coetzee, D.; Valtr, L.; Verbecque, E. Do girls have an advantage compared to boys when their motor skills are tested using the movement assessment battery for children, 2nd Edition? Children 2023, 10, 1159. [Google Scholar] [CrossRef]
- Statistics Canada, Census at School. Average Reaction Time, by Age and Dominant Hand. 2008. Available online: https://censusatschool.ca/data-results/2007-08/average-reaction-time/ (accessed on 6 February 2025).
- Pahlevanian, A.A.; Ahmadizadeh, Z. Relationship between gender and motor skills in preschoolers. Middle East J. Rehabil. Health Stud. 2014, 1, e20843. [Google Scholar] [CrossRef]
- Sheehan, D.P.; Lienhard, K.; Ammar, D. Reducing the object control skills gender gap in elementary school boys and girls. Adv. Phys. Educ. 2020, 10, 155–168. [Google Scholar] [CrossRef]
- Statistics Canada. Physical Activity and Screen Time Among Canadian Children and Youth, 2016 and 2017; Catalogue No. 82-625-X.; Statistics Canada: Toronto, ON, USA, 2019; ISSN 1920-9118. Available online: https://www150.statcan.gc.ca/n1/pub/82-625-x/2019001/article/00003-fra.htm (accessed on 6 February 2025).
- Hamlen, K.R. Re-examining gender differences in video game play: Time spent and feelings of success. J. Educ. Comput. Res. 2010, 43, 293–308. [Google Scholar] [CrossRef]
- Leone, M.; Levesque, P.; Bourget-Gaudreault, S.; Lemoyne, J.; Kalinova, E.; Comtois, A.S.; Bui, H.T.; Léger, L.; Frémont, P. Secular trends of cardiorespiratory fitness in children and adolescents over a 35-year period: Chronicle of a predicted foretold. Front. Public Health 2023, 10, 1056484. [Google Scholar] [CrossRef]
- Crane, J.R.; Naylor, P.J.; Cook, R.; Temple, V.A. Do perceptions of competence mediate the relationship between fundamental motor skill proficiency and physical activity levels of children in kindergarten? J. Phys. Act. Health 2015, 12, 954–961. [Google Scholar] [CrossRef]
- LeGear, M.; Greyling, L.; Sloan, E.; Bell, R.I.; Williams, B.L.; Naylor, P.J.; Temple, V.A. A window of opportunity? Motor skills and perceptions of competence of children in Kindergarten. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 29. [Google Scholar] [CrossRef]
- Slykerman, S.; Ridgers, N.D.; Stevenson, C.; Barnett, L.M. How important is young children’s actual and perceived movement skill competence to their physical activity? J. Sci. Med. Sport 2016, 19, 488–492. [Google Scholar] [CrossRef]
- Hausenblas, H.A.; Downs, D.S.; Fleming, D.S.; Connaughton, D.P. Body image in middle school children. Eat. Weight Disord. 2002, 7, 244–248. [Google Scholar] [CrossRef] [PubMed]
- Berk, L.E.; Meyers, A.B. Infants, Children, and Adolescents, Eighth ed.; Pearson: New York, NY, USA, 2016. [Google Scholar]
- Levine, L.E.; Munsch, J. Child Development: An Active Learning Approach, 4th ed.; SAGE: Thousand Oaks, CA, USA, 2022. [Google Scholar]
- Paxton, S.J.; Neumark-Sztainer, D.; Hannan, P.J.; Eisenberg, M.E. Body dissatisfaction prospectively predicts depressive mood and low self-esteem in adolescent girls and boys. J. Clin. Child Adolesc. Psychol. 2006, 35, 539–549. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Floody, P.; Soto-García, D.; Caamaño-Navarrete, F.; Carter-Thuillier, B.; Guzmán-Guzmán, I.P. Negative Physical Self-concept is associated to low cardiorespiratory fitness, negative lifestyle and poor mental health in chilean schoolchildren. Nutrients 2022, 14, 2771. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.L.; Damiano, S.R.; McLean, S.A.; Wertheim, E.H.; Paxton, S.J. Biopsychosocial correlates of body satisfaction in 7- to 8-year old children: A cross-sectional and prospective investigation. J. Eat. Disord. 2024, 12, 215. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Variables | Boys | n | Girls | n | p Values | Cohen’s d |
|---|---|---|---|---|---|---|
| Age (years) | 9.5 ± 1.7 | 1535 | 9.4 ± 1.8 | 1609 | 0.852 | 0.06 |
| BM (kg) | 33.0 ± 10.3 | 1280 | 33.8 ± 11.2 | 1302 | 0.061 | 0.07 |
| BH (cm) | 137.5 ± 11.6 | 1279 | 138.3 ± 12.8 | 1302 | 0.084 | 0.07 |
| BMI (kg/m2) | 17.1 ± 3.3 | 1278 | 17.3 ± 3.4 | 1302 | 0.322 | 0.06 |
| One-hand plate tapping (Nb/20 s) | 66.1 ± 11.8 | 1440 | 66.7 ± 12.8 | 1515 | 0.170 | 0.05 |
| Two-foot tapping (Nb/20 s) | 21.7 ± 0.4.9 | 1426 | 21.9 ± 4.8 | 1512 | 0.445 | 0.04 |
| 5 × 5 m shuttle run (s) | 11.1 ± 1.3 | 1421 | 11.4 ± 1.3 | 1524 | <0.001 | 0.23 |
| Circle run (s) | 22.1 ± 2.7 | 1441 | 22.7 ± 2.5 | 1538 | <0.001 | 0.24 |
| Sidestep run (s) | 11.3 ± 1.8 | 1440 | 11.7 ± 1.8 | 1510 | <0.001 | 0.23 |
| Slalom run (s) | 19.7 ± 3.3 | 1428 | 20.2 ± 3.0 | 548 | <0.001 | 0.16 |
| Balance eyes opened (s) | 23.1 ± 17.9 | 1439 | 27.1 ± 19.9 | 1497 | <0.001 | 0.21 |
| Balance eyes closed (s) | 17.7 ± 15.0 | 1366 | 20.0 ± 16.4 | 1428 | <0.001 | 0.15 |
| Simple reaction time (ms) | 282.3 ± 19.9 | 778 | 288.2 ± 19.5 | 809 | <0.001 | 0.30 |
| Target ball toss (pts) | 4.6 ± 2.9 | 1457 | 3.1 ± 2.3 | 1537 | <0.001 | 0.55 |
| Hand–foot coordination (s) | 14.5 ± 7.4 | 1359 | 12.6 ± 6.4 | 1464 | <0.001 | 0.28 |
| Ball dribble (Nb/20 s) | 38.3 ± 8.6 | 1445 | 35.6 ± 8.4 | 1528 | <0.001 | 0.32 |
| VO2peak (ml/kg/min) | 46.3 ± 4.5 | 979 | 44.8 ± 3.8 | 891 | <0.001 | 0.36 |
| Stages (number) | 3.5 ± 1.9 | 980 | 2.8 ± 1.5 | 891 | <0.001 | 0.40 |
| Variables | Satisfied | Dissatisfied | ||||||
|---|---|---|---|---|---|---|---|---|
| n | Mean ± SD | CI | n | Mean ± SD | CI | p Values | Cohen’s d ES | |
| Boys | ||||||||
| Age (years) | 481 | 9.8 ± 1.7 | 9.6–9.9 | 634 | 9.6 ± 1.7 | 9.5–9.7 | 0.091 | 0.03 |
| One-hand tapping (Nb/20 s) | 468 | 67.3 ± 11.9 | 66.3–68.4 | 622 | 65.9 ± 11.4 | 65.0–66.8 | 0.042 | 0.12 |
| Two-foot tapping (Nb/20 s) | 465 | 22.7 ± 4.8 | 22.3–23.2 | 614 | 21.6 ± 4.6 | 21.2–22.0 | <0.001 | 0.24 |
| 5 × 5 m shuttle run (s) | 450 | 11.1 ± 1.2 | 10.9–11.2 | 603 | 11.4 ± 1.3 | 11.3–11.5 | <0.001 | 0.24 |
| Circle run (s) | 468 | 21.8 ± 2.6 | 21.6–22.0 | 613 | 22.3 ± 2.6 | 22.1–22.5 | 0.002 | 0.19 |
| Sidestep run (s) | 462 | 11.1 ± 1.7 | 10.9–11.2 | 615 | 11.4 ± 1.7 | 11.2–11.5 | 0.003 | 0.18 |
| Slalom run (s) | 463 | 19.3 ± 2.2 | 19.0–19.6 | 611 | 19.8 ± 3.3 | 19.5–20.0 | 0.025 | 0.17 |
| Balance eyes opened (s) | 463 | 24.6 ± 18.4 | 22.9–26.2 | 620 | 21.3 ± 17.6 | 19.9–22.7 | 0.003 | 0.18 |
| Balance eyes closed (s) | 449 | 19.3 ± 15.4 | 17.9–20.8 | 599 | 17.9 ± 15.1 | 16.7–19.1 | 0.133 | 0.09 |
| Simple reaction time (ms) | 287 | 283 ± 20 | 280–285 | 427 | 282 ± 20 | 280–284 | 0.766 | 0.05 |
| Target ball toss (Pts) | 475 | 4.8 ± 3.0 | 4.5–5.1 | 621 | 4.5 ± 2.9 | 4.3–4.7 | 0.124 | 0.10 |
| Hand/foot coordination (s) | 443 | 13.5 ± 6.8 | 12.8–14.1 | 596 | 14.8 ± 7.3 | 14.2–15.3 | 0.004 | 0.18 |
| Ball dribble (Nb/20 s) | 460 | 39.3 ± 8.0 | 38.6–40.0 | 619 | 38.0 ± 8.9 | 37.3–38.7 | 0.012 | 0.15 |
| VO2peak (ml/kg/min) | 381 | 46.8 ± 4.5 | 46.3–47.2 | 528 | 46.0 ± 4.7 | 45.6–46.4 | 0.013 | 0.17 |
| Stages (number) | 381 | 3.8 ± 1.9 | 3.6–4.0 | 528 | 3.3 ± 1.9 | 3.2–3.5 | <0.001 | 0.26 |
| Girls | ||||||||
| Age (years) | 486 | 9.8 ± 1.7 | 9.7–10.0 | 657 | 9.7 ± 1.7 | 9.5–9.8 | 0.079 | 0.06 |
| One-hand tapping (Nb/20 s) | 470 | 68.4 ± 13.1 | 67.2–69.5 | 635 | 67.1 ± 12.4 | 66.1–68.1 | 0.102 | 0.10 |
| Two-foot tapping (Nb/20 s) | 466 | 22.8 ± 4.6 | 22.4–23.2 | 634 | 22.2 ± 4.4 | 21.9–22.5 | 0.027 | 0.13 |
| 5 × 5 m shuttle run (s) | 472 | 11.3 ± 1.2 | 11.2–11.4 | 628 | 11.6 ± 1.2 | 11.5–11.7 | <0.001 | 0.25 |
| Circle run (s) | 474 | 22.4 ± 2.4 | 22.2–22.6 | 636 | 22.6 ± 2.4 | 22.5–22.8 | 0.073 | 0.08 |
| Sidestep run (s) | 466 | 11.3 ± 1.7 | 11.2–11.5 | 624 | 11.7 ± 1.7 | 11.6–11.8 | <0.001 | 0.24 |
| Slalom run (s) | 467 | 19.7 ± 3.0 | 19.4–20.0 | 627 | 20.1 ± 2.9 | 19.9–20.4 | 0.022 | 0.14 |
| Balance eyes opened (s) | 466 | 29.7 ± 20.3 | 27.9–31.6 | 625 | 25.9 ± 19.8 | 24.3–27.4 | 0.002 | 0.19 |
| Balance eyes closed (s) | 450 | 23.5 ± 16.6 | 22.0–25.1 | 606 | 19.8 ± 16.3 | 18.5–21.1 | <0.001 | 0.23 |
| Simple reaction time (ms) | 305 | 287 ± 20 | 285–289 | 433 | 289 ± 20 | 287–291 | 0.131 | 0.10 |
| Target ball toss (Pts) | 476 | 3.3 ± 2.4 | 3.0–3.5 | 630 | 3.2 ± 2.4 | 3.0–3.3 | 0.505 | 0.04 |
| Hand/foot coordination (s) | 451 | 11.7 ± 5.8 | 11.1–12.2 | 620 | 12.0 ± 5.8 | 11.6–12.5 | 0.362 | 0.05 |
| Ball dribble (Nb/20 s) | 465 | 36.8 ± 7.7 | 36.1–37.5 | 628 | 35.8 ± 8.4 | 35.1–36.4 | 0.036 | 0.12 |
| VO2peak (ml/kg/min) | 346 | 44.9 ± 3.8 | 44.5–45.4 | 464 | 44.6 ± 3.8 | 44.3–45.0 | 0.261 | 0.08 |
| Stages (number) | 346 | 3.0 ± 1.5 | 2.8–3.1 | 464 | 2.8 ± 1.4 | 2.7–3.0 | 0.118 | 0.14 |
| Overall Body Image Dissatisfaction | ||||
|---|---|---|---|---|
| All Participants | Boys | Girls | ||
| n = 1076 | % | n = 1084 | % | |
| Satisfied | 465 | 43.2 | 463 | 42.7 |
| Want to be thinner | 341 | 31.7 | 511 | 47.1 |
| Want to be bigger | 270 | 25.1 | 110 | 10.2 |
| Body image dissatisfaction based on the desire to be thinner or bigger | ||||
| Dissatisfied | n = 611 | % | n = 620 | % |
| Want to be thinner | 341 | 44.2 | 511 | 82.3 |
| Want to be bigger | 270 | 55.8 | 110 | 17.7 |
| Body image dissatisfaction vs. BMI | ||||
| Typical BMI | n = 909 | % | n = 878 | % |
| Satisfied | 427 | 47.0 | 424 | 48.3 |
| Dissatisfied | 482 | 53.0 | 454 | 51.7 |
| Overweight | n = 108 | % | n = 146 | % |
| Satisfied | 27 | 25.0 | 30 | 20.6 |
| Dissatisfied | 81 | 75.0 | 116 | 79.4 |
| Obese | n = 59 | % | n = 59 | % |
| Satisfied | 11 | 18.6 | 9 | 15.3 |
| Dissatisfied | 48 | 81.4 | 50 | 84.7 |
| Body image dissatisfaction vs. socioeconomic status | ||||
| Mean | SD | Mean | SD | |
| Favorable | 1.51 | 0.50 | 1.61 | 0.49 |
| Unfavorable | 1.56 | 0.50 | 1.62 | 0.49 |
| p values (Student t-test) | 0.106 | 0.748 | ||
| Validation of self-assessment of body image | ||||
| r (n = 1119) | Kendall’s Tau-b | r (n = 1145) | Kendall’s Tau-b | |
| Independent rating | 0.558 | 0.474 | 0.624 | 0.542 |
| Overall Body Image Dissatisfaction | ||||
|---|---|---|---|---|
| Boys | 6 to 8 years old | 9 to 12 years old | ||
| n = 411 | % | n = 704 | % | |
| Satisfied | 162 | 39.4 | 319 | 45.3 |
| Want to be thinner | 122 | 29.7 | 231 | 32.8 |
| Want to be bigger | 127 | 30.9 | 154 | 21.9 |
| Body image dissatisfaction based on the desire to be thinner or bigger | ||||
| Dissatisfied | n = 249 | % | n = 385 | % |
| Want to be thinner | 122 | 49.0 | 231 | 60.0 |
| Want to be bigger | 127 | 51.0 | 154 | 40.0 |
| Body image dissatisfaction vs. BMI | ||||
| Typical BMI | n = 332 | % | n = 577 | % |
| Satisfied | 134 | 40.4 | 293 | 50.8 |
| Dissatisfied | 198 | 59.6 | 284 | 49.2 |
| Overweight | n = 30 | % | n = 78 | % |
| Satisfied | 11 | 36.7 | 16 | 20.5 |
| Dissatisfied | 19 | 63.3 | 62 | 79.5 |
| Obese | n = 22 | % | n = 37 | % |
| Satisfied | 7 | 31.8 | 4 | 10.8 |
| Dissatisfied | 15 | 68.2 | 33 | 89.2 |
| Body image dissatisfaction vs. socioeconomic status | ||||
| Mean | SD | Mean | SD | |
| Favorable | 1.62 | 0.49 | 1.58 | 0.49 |
| Unfavorable | 1.60 | 0.49 | 1.22 | 0.50 |
| p values (Student T-test) | 0.662 | 0.121 | ||
| Validation of self-assessment of body image | ||||
| r (n = 367) | Kendall’s Tau-b | r (n = 619) | Kendall’s Tau-b | |
| Independent rating | 0.505 | 0.420 | 0.581 | 0.496 |
| Overall Body Image Dissatisfaction | ||||
|---|---|---|---|---|
| Girls | 6 to 8 years old | 9 to 12 years old | ||
| n = 400 | % | n = 743 | % | |
| Satisfied | 152 | 38.0 | 334 | 45.0 |
| Want to be thinner | 190 | 47.5 | 348 | 46.8 |
| Want to be bigger | 58 | 14.5 | 61 | 8.2 |
| Body image dissatisfaction based on the desire to be thinner or bigger | ||||
| Dissatisfied | n = 248 | % | n = 409 | % |
| Want to be thinner | 190 | 76.6 | 348 | 85.1 |
| Want to be bigger | 58 | 23.4 | 61 | 14.9 |
| Body image dissatisfaction vs. BMI | ||||
| Typical BMI | n = 294 | % | n = 585 | % |
| Satisfied | 121 | 41.1 | 303 | 51.8 |
| Dissatisfied | 173 | 58.9 | 282 | 48.2 |
| Overweight | n = 47 | % | n = 99 | % |
| Satisfied | 14 | 29.8 | 16 | 16.2 |
| Dissatisfied | 33 | 70.2 | 83 | 83.8 |
| Obese | n = 20 | % | n = 39 | % |
| Satisfied | 4 | 20.0 | 5 | 12.8 |
| Dissatisfied | 16 | 80.0 | 34 | 87.2 |
| Body image dissatisfaction vs. socioeconomic status | ||||
| Mean | SD | Mean | SD | |
| Favorable | 1.56 | 0.50 | 1.57 | 0.50 |
| Unfavorable | 1.66 | 0.47 | 1.54 | 0.50 |
| p values (Student t-test) | 0.045 | 0.337 | ||
| Validation of self-assessment of body image | ||||
| r (n = 348) | Kendall’s Tau-b | r (n = 643) | Kendall’s Tau-b | |
| Independent rating | 0.547 | 0.477 | 0.651 | 0.565 |
| n | Typical | n | Overweight | n | Obese | p Values | Effect Size f | |
|---|---|---|---|---|---|---|---|---|
| Boys | ||||||||
| Age (years) | 1074 | 9.6 ± 1.7 | 124 | 9.9 ± 1.7 | 66 | 9.6 ± 1.8 | 0.193 | 0.08 |
| One-hand tapping (Nb/20 s) | 1019 | 66.3 ± 11.5 | 123 | 66.7 ± 12.1 | 62 | 65.0 ± 12.4 | 0.911 | 0.07 |
| Two-foot tapping (Nb/20 s) | 1017 | 22.1 ± 4.8 | 120 | 21.9 ± 4.8 | 61 | 20.6 ± 4.3 | 0.074 | 0.15 |
| 5 × 5 m shuttle run (s) | 993 | 11.2 ± 1.3 | 117 | 11.4 ± 1.2 | 62 | 11.8 ± 1.1 | 0.001 | 0.24 |
| Circle run (s) | 1015 | 22.1 ± 2.7 | 120 | 22.3 ± 2.4 | 62 | 22.6 ± 2.5 | 0.239 | 0.09 |
| Sidestep run (s) | 1009 | 11.2 ± 1.8 | 120 | 11.4 ± 1.5 | 61 | 12.0 ± 1.8 | 0.002 | 0.22 |
| Slalom run (s) | 999 | 19.7 ± 3.4 | 119 | 19.9 ± 3.1 | 62 | 20.5 ± 3.0 | 0.166 | 0.12 |
| Balance eyes opened (s) | 1012 | 23.9 ± 17.7 | 119 | 18.2 ± 17.7 | 62 | 12.9 ± 14.5 | <0.001 | 0.31 |
| Balance eyes closed (s) | 977 | 18.6 ± 15.1 | 113 | 17.3 ± 15.7 | 60 | 11.2 ± 12.6 | 0.001 | 0.24 |
| Simple reaction time (ms) | 638 | 283 ± 20 | 74 | 281 ± 21 | 42 | 279 ± 20 | 0.467 | 0.09 |
| Target ball toss (pts) | 1029 | 4.6 ± 3.0 | 121 | 4.7 ± 2.9 | 60 | 4.8 ± 2.8 | 0.719 | 0.03 |
| Hand–eye coordination (s) | 972 | 14.3 ± 7.2 | 114 | 14.1 ± 6.3 | 56 | 14.9 ± 7.3 | 0.827 | 0.06 |
| Ball dribble (Nb/20 s) | 1009 | 38.3 ± 8.7 | 123 | 38.8 ± 8.1 | 63 | 38.2 ± 8.1 | 0.808 | 0.08 |
| Stages (Nb) | 825 | 3.7 ± 1.9 | 105 | 2.7± 1.5 | 48 | 1.9 ± 0.9 | <0.001 | 0.61 |
| VO2peak (ml/kg/min) | 824 | 46.8 ± 4.4 | 105 | 44.2 ± 4.0 | 48 | 42.2 ± 3.9 | <0.001 | 0.53 |
| Girls | ||||||||
| Age (years) | 1059 | 9.6 ± 1.7 | 170 | 9.9 ± 1.7 | 64 | 9.8 ± 1.7 | 0.066 | 0.08 |
| One-hand tapping (Nb/20 s) | 1015 | 67.5 ± 12.7 | 162 | 66.6 ± 12.2 | 63 | 65.4 ± 12.1 | 0.350 | 0.08 |
| Two-foot tapping (Nb/20 s) | 1028 | 22.2 ± 4.8 | 162 | 22.1 ± 4.3 | 63 | 21.2 ± 4.0 | 0.210 | 0.11 |
| 5 × 5 m shuttle run (s) | 1015 | 11.5 ± 1.2 | 159 | 11.6 ± 1.1 | 57 | 12.0 ± 1.2 | 0.001 | 0.20 |
| Circle run (s) | 1024 | 22.6 ± 2.5 | 164 | 22.8 ± 2.2 | 62 | 23.7 ± 2.3 | 0.001 | 0.23 |
| Sidestep run (s) | 1002 | 11.6 ± 1.7 | 155 | 11.7 ± 1.5 | 62 | 12.3 ± 1.6 | 0.002 | 0.21 |
| Slalom run (s) | 1002 | 20.1 ± 3.1 | 160 | 20.2 ± 3.0 | 60 | 20.5 ± 2.7 | 0.552 | 0.06 |
| Balance eyes opened (s) | 998 | 28.5 ± 19.5 | 159 | 23.8 ± 20.3 | 61 | 16.7 ± 20.4 | <0.001 | 0.28 |
| Balance eyes closed (s) | 960 | 21.3 ± 16.4 | 153 | 17.9 ± 16.2 | 60 | 16.2 ± 15.3 | 0.007 | 0.15 |
| Simple reaction time (ms) | 621 | 288 ± 20 | 106 | 289 ± 20 | 42 | 289 ± 17 | 0.929 | 0.03 |
| Target ball toss (pts) | 1022 | 3.2 ± 2.4 | 163 | 3.3 ± 2.2 | 63 | 2.7 ± 2.4 | 0.323 | 0.12 |
| Hand–eye coordination (s) | 985 | 12.4 ± 6.2 | 161 | 12.1 ± 5.2 | 61 | 13.1 ± 6.4 | 0.552 | 0.08 |
| Ball dribble (Nb/20 s) | 1013 | 35.9 ± 8.4 | 161 | 36.2 ± 7.8 | 62 | 35.0 ± 7.0 | 0.616 | 0.07 |
| Stages (Nb) | 721 | 3.0 ± 1.5 | 126 | 2.3 ± 1.1 | 44 | 1.9 ± 0.9 | <0.001 | 0.44 |
| VO2peak (ml/kg/min) | 721 | 45.2 ± 3.7 | 126 | 43.0 ± 3.5 | 44 | 42.5 ± 3.4 | <0.001 | 0.36 |
| Variables | Satisfied | Dissatisfied | ||||||
|---|---|---|---|---|---|---|---|---|
| n | Mean ± SD | CI | n | Mean ± SD | CI | p Values | Cohen’s d ES | |
| Boys | ||||||||
| One-hand tapping (Nb/20 s) | 415 | 67.9 ± 11.5 | 66.8–69.0 | 473 | 65.6 ± 11.3 | 64.6–66.6 | 0.003 | 0.20 |
| Two-foot tapping (Nb/20 s) | 416 | 23.0 ± 4.7 | 22.5–23.4 | 468 | 21.7 ± 4.7 | 21.3–22.1 | <0.001 | 0.28 |
| 5 × 5 m shuttle run (s) | 403 | 11.0 ± 1.2 | 10.9–11.1 | 461 | 11.3 ± 1.3 | 11.3–11.5 | <0.001 | 0.24 |
| Circle run (s) | 418 | 21.8 ± 2.7 | 21.5–22.0 | 464 | 22.3 ± 2.7 | 22.1–22.6 | 0.003 | 0.19 |
| Sidestep run (s) | 412 | 11.0 ± 1.7 | 10.8–11.3 | 469 | 11.3 ± 1.7 | 11.1–11.4 | 0.010 | 0.18 |
| Slalom run (s) | 413 | 19.2 ± 3.3 | 18.9–19.6 | 464 | 19.7 ± 3.3 | 19.4–20.0 | 0.037 | 0.15 |
| Balance eyes opened (s) | 414 | 25.5 ± 18.4 | 23.7–27.3 | 473 | 23.0 ± 17.6 | 21.4–24.6 | 0.037 | 0.14 |
| Balance eyes closed (s) | 401 | 20.1 ± 15.6 | 18.6–21.6 | 458 | 18.6 ± 15.0 | 17.2–20.0 | 0.145 | 0.10 |
| Simple reaction time (ms) | 261 | 283 ± 20 | 280–285 | 328 | 282 ± 20 | 280–285 | 0.911 | 0.01 |
| Target ball toss (Pts) | 423 | 4.9 ± 3.0 | 4.6–5.2 | 475 | 4.5 ± 2.9 | 4.2–4.7 | 0.046 | 0.14 |
| Hand/foot coordination (s) | 396 | 13.1 ± 6.5 | 12.2–13.8 | 456 | 14.8 ± 7.5 | 14.1–15.5 | 0.001 | 0.24 |
| Ball dribble (Nb/20 s) | 410 | 39.7 ± 7.7 | 39.0–40.5 | 471 | 38.0 ± 9.0 | 37.1–38.8 | 0.002 | 0.20 |
| VO2peak (ml/kg/min) | 351 | 46.9 ± 4.5 | 46.5–47.4 | 417 | 46.8 ± 4.5 | 46.3–47.2 | 0.580 | 0.02 |
| Stages (number) | 351 | 3.9 ± 1.9 | 3.7–4.1 | 417 | 3.6 ± 1.9 | 3.4–3.8 | 0.012 | 0.16 |
| Girls | ||||||||
| One-hand tapping (Nb/20 s) | 411 | 69.0 ± 12.7 | 67.8–70.3 | 439 | 67.7 ± 12.2 | 66.5–68.8 | 0.108 | 0.10 |
| Two-foot tapping (Nb/20 s) | 413 | 23.1 ± 4.5 | 22.7–23.5 | 442 | 22.4 ± 4.4 | 22.0–22.8 | 0.027 | 0.16 |
| 5 × 5 m shuttle run (s) | 414 | 11.3 ± 1.2 | 11.2–11.4 | 437 | 11.5 ± 1.2 | 11.4–11.6 | 0.029 | 0.17 |
| Circle run (s) | 417 | 22.3 ± 2.4 | 22.1–22.6 | 441 | 22.5 ± 2.4 | 22.3–22.7 | 0.336 | 0.09 |
| Sidestep run (s) | 408 | 11.3 ± 1.6 | 11.1–11.4 | 432 | 11.5 ± 1.6 | 11.4–11.7 | 0.025 | 0.14 |
| Slalom run (s) | 412 | 19.6 ± 2.9 | 19.3–19.9 | 433 | 20.0 ± 2.9 | 19.7–20.3 | 0.042 | 0.14 |
| Balance eyes opened (s) | 410 | 30.6 ± 19.9 | 28.7–32.6 | 433 | 28.0 ± 19.3 | 26.2–29.8 | 0.050 | 0.13 |
| Balance eyes closed (s) | 396 | 24.3 ± 16.7 | 22.6–25.9 | 418 | 21.0 ± 16.2 | 19.4–22.5 | 0.004 | 0.20 |
| Simple reaction time (ms) | 275 | 286 ± 19 | 284–289 | 296 | 290 ± 20 | 287–292 | 0.042 | 0.21 |
| Target ball toss (Pts) | 417 | 3.3 ± 2.5 | 3.1–3.6 | 435 | 3.2 ± 2.4 | 3.0–3.4 | 0.419 | 0.04 |
| Hand/foot coordination (s) | 397 | 11.3 ± 5.6 | 10.8–11.9 | 430 | 11.9 ± 5.6 | 11.3–12.4 | 0.166 | 0.11 |
| Ball dribble (Nb/20 s) | 411 | 37.1 ± 7.7 | 36.3–37.8 | 434 | 36.0 ± 8.5 | 35.2–36.8 | 0.044 | 0.14 |
| VO2peak (ml/kg/min) | 315 | 45.1 ± 3.8 | 44.7–45.5 | 335 | 45.4 ± 3.6 | 45.0–45.8 | 0.337 | 0.08 |
| Stages (number) | 315 | 3.1 ± 1.5 | 2.9–3.3 | 335 | 3.0 ± 1.4 | 2.9–3.2 | 0.707 | 0.07 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Allisse, M.; Thibault, I.; Gagnon, D.; Kalinova, E.; Larivière, G.; Leone, M. The Relationship Between Obesity Status and Body Image Dissatisfaction on Gross Motor Skill Development and Cardiorespiratory Fitness in Children Aged 6–12 Years Old. Int. J. Environ. Res. Public Health 2025, 22, 417. https://doi.org/10.3390/ijerph22030417
Allisse M, Thibault I, Gagnon D, Kalinova E, Larivière G, Leone M. The Relationship Between Obesity Status and Body Image Dissatisfaction on Gross Motor Skill Development and Cardiorespiratory Fitness in Children Aged 6–12 Years Old. International Journal of Environmental Research and Public Health. 2025; 22(3):417. https://doi.org/10.3390/ijerph22030417
Chicago/Turabian StyleAllisse, Maxime, Isabelle Thibault, Dominic Gagnon, Emilia Kalinova, Georges Larivière, and Mario Leone. 2025. "The Relationship Between Obesity Status and Body Image Dissatisfaction on Gross Motor Skill Development and Cardiorespiratory Fitness in Children Aged 6–12 Years Old" International Journal of Environmental Research and Public Health 22, no. 3: 417. https://doi.org/10.3390/ijerph22030417
APA StyleAllisse, M., Thibault, I., Gagnon, D., Kalinova, E., Larivière, G., & Leone, M. (2025). The Relationship Between Obesity Status and Body Image Dissatisfaction on Gross Motor Skill Development and Cardiorespiratory Fitness in Children Aged 6–12 Years Old. International Journal of Environmental Research and Public Health, 22(3), 417. https://doi.org/10.3390/ijerph22030417