
Long-Term Survival among Patients Hospitalized for COVID-19 during the First Three Epidemic Waves: An Observational Study in a Northern Italy Hospital

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Statistical Analysis
3. Results
3.1. Demographic and Clinicopathological Differences among COVID-19 Patients Hospitalized during the First Three Waves
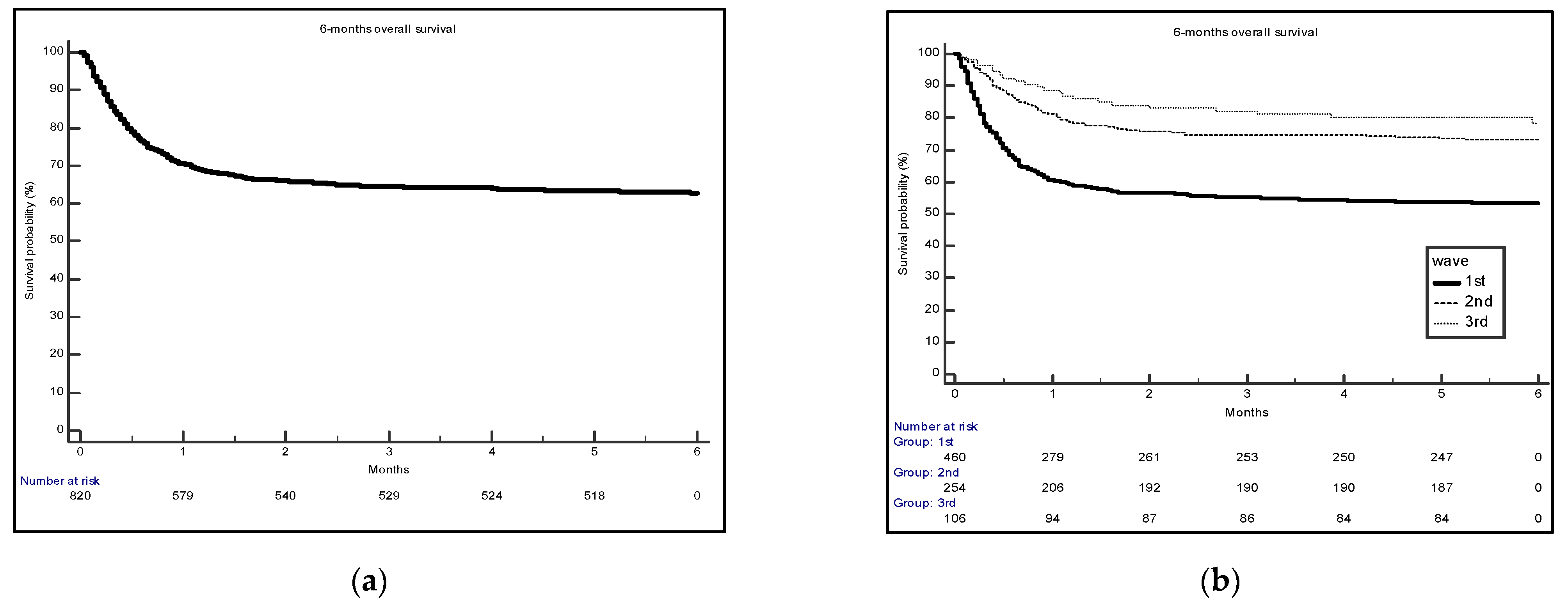
3.2. Survival Analysis of COVID-19 Patients Hospitalized during the First Three Waves
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhou, H.; Ni, W.J.; Huang, W.; Wang, Z.; Cai, M.; Sun, Y.C. Advances in pathogenesis, progression, potential targets and targeted therapeutic strategies in SARS-CoV-2-Induced COVID-19. Front Immunol. 2022, 13, 834942. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the Coronavirus Disease 2019 (COVID-19) outbreak in China: Summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Casals, M.; Brito-Zerón, P.; Mariette, X. Systemic and organ-specific immune-related manifestations of COVID-19. Nat. Rev. Rheumatol. 2021, 6, 315–332. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.; Peng, F.; Xu, B.; Zhao, J.; Liu, H.; Peng, J.; Li, Q.; Jiang, C.; Zhou, Y.; Liu, S.; et al. Risk factors of critical & mortal COVID-19 cases: A systematic literature review and meta-analysis. J. Infect. 2020, 2, e16–e25. [Google Scholar] [CrossRef]
- Betti, M.; Bertolotti, M.; Ferrante, D.; Roveta, A.; Pelazza, C.; Giacchero, F.; Penpa, S.; Massarino, C.; Bolgeo, T.; Cassinari, A.; et al. Baseline clinical characteristics and prognostic factors in hospitalized COVID-19 patients aged ≤ 65 years: A retrospective observational study. PLoS ONE. 2021, 3, e0248829. [Google Scholar] [CrossRef]
- Vinceti, M.; Filippini, T.; Rothman, K.J.; Di Federico, S.; Orsini, N. SARS-CoV-2 infection incidence during the first and second COVID-19 waves in Italy. Environ. Res. 2021, 197, 111097. [Google Scholar] [CrossRef] [PubMed]
- Dorrucci, M.; Minelli, G.; Boros, S.; Manno, V.; Prati, S.; Battaglini, M.; Corsetti, G.; Andrianou, X.; Riccardo, F.; Fabiani, M.; et al. Excess mortality in Italy during the COVID-19 pandemic: Assessing the differences between the first and the second wave, year 2020. Front. Public. Health. 2021, 9, 669209. [Google Scholar] [CrossRef] [PubMed]
- Giacomelli, A.; Ridolfo, A.L.; Pezzati, L.; Oreni, L.; Carrozzo, G.; Beltrami, M.; Poloni, A.; Caloni, B.; Lazzarin, S.; Colombo, M.; et al. Mortality rates among COVID-19 patients hospitalised during the first three waves of the epidemic in Milan, Italy: A prospective observational study. PLoS ONE. 2022, 4, e0263548. [Google Scholar] [CrossRef] [PubMed]
- Bassi, F.; Doria, M. Diffusion of COVID-19 among children and adolescents during the second and third waves of the pandemic in Italy. Eur. J. Pediatr. 2022, 181, 1619–1632. [Google Scholar] [CrossRef] [PubMed]
- Magnani, C.; Azzolina, D.; Gallo, E.; Ferrante, D.; Gregori, D. How Large Was the Mortality Increase Directly and Indirectly Caused by the COVID-19 Epidemic? An Analysis on All-Causes Mortality Data in Italy. Int. J. Environ. Res. Public Health. 2020, 17, 3452. [Google Scholar] [CrossRef]
- Onder, G.; Rezza, G.; Brusaferro, S. Case-Fatality Rate and Characteristics of Patients Dying in Relation to COVID-19 in Italy. JAMA 2020, 323, 1775–1776. [Google Scholar] [CrossRef] [PubMed]
- Grande, E.; Fedeli, U.; Pappagallo, M.; Crialesi, R.; Marchetti, S.; Minelli, G.; Iavarone, I.; Frova, L.; Onder, G.; Grippo, F. Variation in Cause-Specific Mortality Rates in Italy during the First Wave of the COVID-19 Pandemic: A Study Based on Nationwide Data. Int. J. Environ. Res. Public Health 2022, 19, 805. [Google Scholar] [CrossRef] [PubMed]
- Bellan, M.; Patti, G.; Hayden, E.; Azzolina, D.; Pirisi, M.; Acquaviva, A.; Aimaretti, G.; Aluffi Valletti, P.; Angilletta, R.; Arioli, R.; et al. Fatality rate and predictors of mortality in an Italian cohort of hospitalized COVID-19 patients. Sci. Rep. 2020, 10, 20731. [Google Scholar] [CrossRef] [PubMed]
- Bellan, M.; Azzolina, D.; Hayden, E.; Gaidano, G.; Pirisi, M.; Acquaviva, A.; Aimaretti, G.; Aluffi Valletti, P.; Angilletta, R.; Arioli, R.; et al. Simple Parameters from Complete Blood Count Predict In-Hospital Mortality in COVID-19. Dis. Markers. 2021, 2021, 8863053. [Google Scholar] [CrossRef]
- World Health Organization. Laboratory Testing for Coronavirus Disease 2019 (COVID-19) in Suspected Human Cases; Interim Guidance; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Istituto Superiore di Sanità, Epidemia COVID-19 Aggiornamento Nazionale 4 agosto 2021 ore 12:00. Available online: https://www.epicentro.iss.it/coronavirus/bollettino/Bollettino-sorveglianza-integrata-COVID-19_4-agosto-2021.pdf (accessed on 6 August 2021).
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- World Health Organization. Clinical Management of Severe Acute Respiratory Infection When Novel Coronavirus (2019-nCoV) Infection is Suspected Interim Guidance 28 January 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Harvey, L.A. REDCap: Web-based software for all types of data storage and collection. Spinal Cord. 2018, 56, 625. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Carbonell, R.; Urgelés, S.; Rodríguez, A.; Bodí, M.; Martín-Loeches, I.; Solé-Violán, J.; Díaz, E.; Gómez, J.; Trefler, S.; Vallverdú, M.; et al. Mortality comparison between the first and second/third waves among 3795 critical COVID-19 patients with pneumonia admitted to the ICU: A multicentre retrospective cohort study. Lancet Reg. Health Eur. 2021, 11, 100243. [Google Scholar] [CrossRef] [PubMed]
- Xia, Y.; Ma, H.; Buckeridge, D.L.; Brisson, M.; Sander, B.; Chan, A.; Verma, A.; Ganser, I.; Kronfli, N.; Mishra, S.; et al. Mortality trends and length of stays among hospitalized patients with COVID-19 in Ontario and Québec (Canada): A population-based cohort study of the first three epidemic waves. Int. J. Infect. Dis. 2022, 121, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Zuccaro, V.; Colaneri, M.; Asperges, E.; Valsecchi, P.; Sambo, M.; Maiocchi, L.; Sacchi, P.; Muzzi, A.; Musella, V.; Cutti, S.; et al. Mortality due to COVID-19 during the pandemic: A comparison of first, second and third SMAtteo COVID-19 REgistry (SMACORE). Heliyon 2022, 8, e08895. [Google Scholar] [CrossRef] [PubMed]
- Blanca, D.; Nicolosi, S.; Bandera, A.; Blasi, F.; Mantero, M.; Hu, C.; de Amicis, M.M.; Lucchi, T.; Schinco, G.; Peyvandi, F.; et al. Comparison between the first and second COVID-19 waves in Internal Medicine wards in Milan, Italy: A retrospective observational study. Intern. Emerg. Med. 2022, 15, 2219–2228. [Google Scholar] [CrossRef] [PubMed]
- Caramello, V.; Catalano, A.; Macciotta, A.; Dansero, L.; Sacerdote, C.; Costa, G.; Aprà, F.; Tua, A.; Boccuzzi, A.; Ricceri, F. Improvements throughout the three waves of COVID-19 pandemic: Results from 4 million inhabitants of North-West Italy. J. Clin. Med. 2022, 11, 4304. [Google Scholar] [CrossRef]
- Parra-Bracamonte, G.M.; Lopez-Villalobos, N.; Parra-Bracamonte, F.E. Clinical characteristics and risk factors for mortality of patients with COVID-19 in a large data set from Mexico. Ann. Epidemiol. 2020, 52, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Leidi, F.; Boari, G.E.M.; Scarano, O.; Mangili, B.; Gorla, G.; Corbani, A.; Accordini, B.; Napoli, F.; Ghidelli, C.; Archenti, G.; et al. Comparison of the characteristics, morbidity and mortality of COVID-19 between first and second/third wave in a hospital setting in Lombardy: A retrospective cohort study. Intern. Emerg. Med. 2022, 17, 1941–1949. [Google Scholar] [CrossRef]
- Minnai, F.; De Bellis, G.; Dragani, T.A.; Colombo, F. COVID-19 mortality in Italy varies by patient age, sex and pandemic wave. Sci. Rep. 2022, 12, 4604. [Google Scholar] [CrossRef]
- Meschiari, M.; Cozzi-Lepri, A.; Tonelli, R.; Bacca, E.; Menozzi, M.; Franceschini, E.; Cuomo, G.; Bedini, A.; Volpi, S.; Milic, J.; et al. First and second waves among hospitalised patients with COVID-19 with severe pneumonia: A comparison of 28-day mortality over the 1-year pandemic in a tertiary university hospital in Italy. BMJ Open 2022, 12, e054069. [Google Scholar] [CrossRef] [PubMed]
- Palmieri, L.; Palmer, K.; Lo Noce, C.; Meli, P.; Giuliano, M.; Floridia, M.; Tamburo de Bella, M.; Piccioli, A.; Brusaferro, S.; Onder, G.; et al. Differences in the clinical characteristics of COVID-19 patients who died in hospital during different phases of the pandemic: National data from Italy. Aging Clin. Exp. Res. 2021, 33, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Borghesi, A.; Golemi, S.; Carapella, N.; Zigliani, A.; Farina, D.; Maroldi, R. Lombardy, Northern Italy: COVID-19 second wave less severe and deadly than the first? A preliminary investigation. Infect. Dis. (Lond). 2021, 53, 370–375. [Google Scholar] [CrossRef] [PubMed]
- Toyoshima, Y.; Nemoto, K.; Matsumoto, S.; Nakamura, Y.; Kiyotani, K. SARS-CoV-2 genomic variations associated with mortality rate of COVID-19. J. Hum. Genet. 2020, 65, 1075–1082. [Google Scholar] [CrossRef] [PubMed]
- Patone, M.; Thomas, K.; Hatch, R.; Tan, P.S.; Coupland, C.; Liao, W.; Mouncey, P.; Harrison, D.; Rowan, K.; Horby, P.; et al. Mortality and critical care unit admission associated with the SARS-CoV-2 lineage B.1.1.7 in England: An observational cohort study. Lancet Infect. Dis. 2021, 21, 1518–1528. [Google Scholar] [CrossRef]

{kind=link}
| Characteristics | Total N = 825 | 1th Wave (24 February–13 April 2020) N = 464 | 2nd Wave (14 September–2 November 2020) N = 255 | 3rd Wave (15 February–6 April 2021) N = 106 | p-Value |
|---|---|---|---|---|---|
| Sex, N (%) | |||||
| Male | 501 (60.7) | 287 (61.9) | 152 (59.6) | 62 (58.5) | 0.74 |
| Female | 324 (39.3) | 177 (38.1) | 103 (40.4) | 44 (41.5) | |
| Age, N (%) | |||||
| <65 | 291 (35.3) | 146 (31.5) | 105 (41.2) | 40 (37.7) | 0.03 |
| ≥65 | 534 (64.7) | 318 (68.5) | 150 (58.8) | 66 (62.3) | |
| Comorbidities, N (%) | |||||
| 0–1 | 336 (40.7) | 184 (39.7) | 112 (43.9) | 40 (37.7) | 0.43 |
| ≥2 | 489 (59.3) | 280 (60.3) | 143 (56.1) | 66 (62.3) | |
| Duration of hospitalization (days), median (IQR) 1 | 11 (5–21) | 9 (4–18) | 14 (6–24) | 17 (10–26) | 0.0001 |
| COVID-19 complications, N (%) | |||||
| No | 252 (30.5) | 148 (31.9) | 72 (28.2) | 32 (30.2) | 0.45 |
| Yes | 546 (66.2) | 295 (63.6) | 177 (69.4) | 74 (69.8) | |
| Missing | 27 (3.3) | 21 (4.5) | 6 (2.4) | 0 | |
| Disease severity, N (%) | <0.0001 | ||||
| Mild/moderate | 349 (42.3) | 161 (34.7) | 140 (54.9) | 48 (45.3) | |
| Severe/critical | 358 (43.4) | 225 (48.5) | 86 (33.7) | 47 (44.3) | |
| Missing | 118 (14.3) | 78 (16.8) | 29 (11.4) | 11 (10.4) | |
| Charlson Comorbidity Index, median (IQR)1 | 4 (2–5) | 4 (3–6) | 3 (2–5) | 4 (2–5) | 0.0002 |
| Oxygen therapy, N (%) | |||||
| No | 179 (21.7) | 84 (18.1) | 73 (28.6) | 22 (20.8) | 0.002 |
| Yes | 640 (77.6) | 380 (81.9) | 176 (69.0) | 84 (79.2) | |
| Missing | 6 (0.7) | 0 | 6 (2.4) | 0 | |
| Invasive Mechanical ventilation, N (%) | |||||
| No | 722 (87.5) | 387 (83.4) | 236 (92.5) | 99 (93.4) | <0.0001 |
| Yes | 97 (11.8) | 77 (16.6) | 13 (5.1) | 7 (6.6) | |
| Missing | 6 (0.7) | 0 | 6 (2.4) | 0 |
| Characteristics | Total N = 825 | 1th Wave (24 February–13 April 2020) N = 464 | 2nd Wave (14 September–2 November 2020) N = 255 | 3rd Wave (15 February–6 April 2021) N = 106 | p-Value |
|---|---|---|---|---|---|
| Death events by the end of follow-up, N (%) | 309 (37.5) | 218 (47.0) | 69 (27.0) | 22 (20.7) | <0.0001 |
| Death events during hospitalization at the Alessandria’s hub hospital, N (%) | 186 (22.5) | 132 (28.5) | 42 (16.5) | 12 (11.3) | <0.0001 |
| Age at death (years), median (IQR) 1 | 81 (74–86) | 80 (73–85) | 84 (77–89) | 78 (74–83) | 0.02 |
| Cause of death N (%) | |||||
| COVID-19 pneumonia | 190 (61.5) | 133 (61.0) | 47 (68.1) | 10 (45.4) | 0.006 |
| Distress respiratory syndrome | 60 (19.4) | 49 (22.5) | 7 (10.1) | 4 (18.2) | |
| Other | 43 (13.9) | 24 (5.2) | 11 (15.9) | 8 (36.4) | |
| Missing | 16 (5.2) | 12 (2.6) | 4 (5.8) | 0 |
| Characteristics | N. Deaths 1 | Person-Months 1 | Univariable Model | Multivariable Model 2 |
|---|---|---|---|---|
| HR 3 (95% CI) | HR 3 (95% CI) | |||
| Wave | ||||
| 1st | 172 | 1382 | 1 | 1 |
| 2nd | 60 | 1019 | 0.48 (0.36–0.63) | 0.65 (0.48–0.88) |
| 3rd | 21 | 460 | 0.35 (0.23–0.55) | 0.44 (0.28–0.70) |
| Sex | ||||
| Male | 152 | 1719 | 1 | 1 |
| Female | 101 | 1143 | 0.88 (0.70–1.12) | 1.03 (0.80–1.34) |
| Age | ||||
| <65 | 26 | 1347 | 1 | 1 |
| ≥5 | 227 | 1515 | 6.87 (4.71–10.02) | 3.40 (2.20–5.24) |
| Comorbidities | ||||
| 0–1 | 52 | 1407 | 1 | 1 |
| ≥2 | 201 | 1455 | 3.31 (2.50–4.39) | 1.28 (0.91–1.80) |
| Disease severity | ||||
| Mild/moderate | 82 | 1652 | 1 | 1 |
| Severe/critical | 171 | 1210 | 2.46 (1.90–3.20) | 1.87 (1.43–2.45) |
| Charlson Comorbidity Index | 253 | 2862 | 1.26 (1.22–1.31) | 1.21 (1.15–1.27) |
| Oxygen therapy | ||||
| No | 40 | 632 | 1 | 1 |
| Yes | 213 | 2230 | 1.75 (1.27–2.39) | 2.30 (1.61–3.30) |
| Invasive Mechanical ventilation | ||||
| No | 208 | 2626 | 1 | 1 |
| Yes | 45 | 236 | 1.93 (1.44–2.58) | 1.16 (0.82–1.65) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bertolotti, M.; Betti, M.; Giacchero, F.; Grasso, C.; Franceschetti, G.; Carotenuto, M.; Odone, A.; Pacileo, G.; Ferrante, D.; Maconi, A. Long-Term Survival among Patients Hospitalized for COVID-19 during the First Three Epidemic Waves: An Observational Study in a Northern Italy Hospital. Int. J. Environ. Res. Public Health 2022, 19, 15298. https://doi.org/10.3390/ijerph192215298
Bertolotti M, Betti M, Giacchero F, Grasso C, Franceschetti G, Carotenuto M, Odone A, Pacileo G, Ferrante D, Maconi A. Long-Term Survival among Patients Hospitalized for COVID-19 during the First Three Epidemic Waves: An Observational Study in a Northern Italy Hospital. International Journal of Environmental Research and Public Health. 2022; 19(22):15298. https://doi.org/10.3390/ijerph192215298
Chicago/Turabian StyleBertolotti, Marinella, Marta Betti, Fabio Giacchero, Chiara Grasso, Genny Franceschetti, Margherita Carotenuto, Anna Odone, Guglielmo Pacileo, Daniela Ferrante, and Antonio Maconi. 2022. "Long-Term Survival among Patients Hospitalized for COVID-19 during the First Three Epidemic Waves: An Observational Study in a Northern Italy Hospital" International Journal of Environmental Research and Public Health 19, no. 22: 15298. https://doi.org/10.3390/ijerph192215298
APA StyleBertolotti, M., Betti, M., Giacchero, F., Grasso, C., Franceschetti, G., Carotenuto, M., Odone, A., Pacileo, G., Ferrante, D., & Maconi, A. (2022). Long-Term Survival among Patients Hospitalized for COVID-19 during the First Three Epidemic Waves: An Observational Study in a Northern Italy Hospital. International Journal of Environmental Research and Public Health, 19(22), 15298. https://doi.org/10.3390/ijerph192215298