Prenatal Counseling throughout Pregnancy: Effects on Physical Activity Level, Perceived Barriers, and Perinatal Health Outcomes: A Quasi-Experimental Study

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
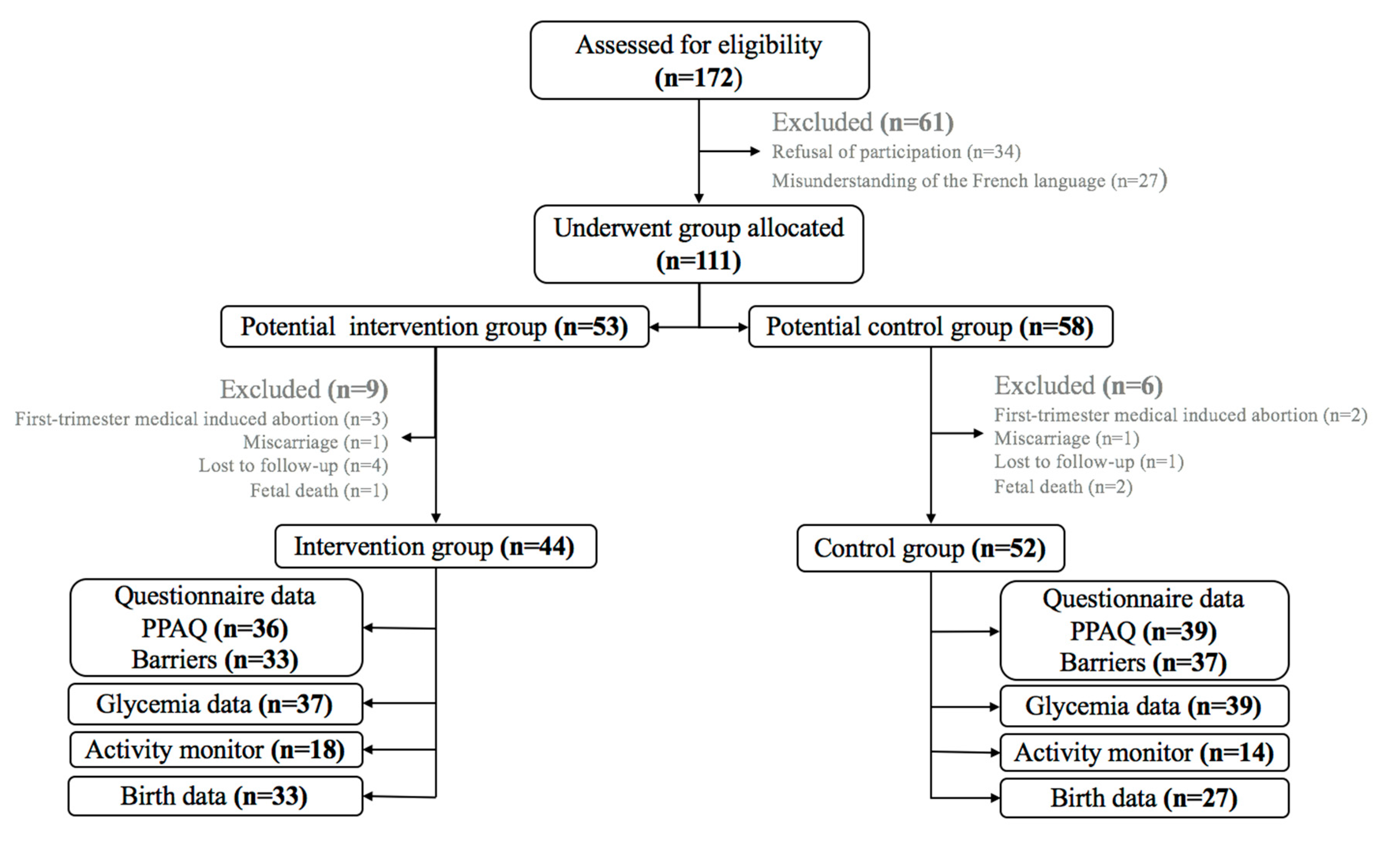
2.2. Participants and Ethics
2.3. Recruitment and Randomization
2.4. Physical Activity Intervention
2.5. Control Group
3. Data Collection
3.1. Physical Activity Behavior
3.2. Perceived Barriers to Physical Activity
3.3. Outcomes
4. Statistical Analysis
5. Results
5.1. Barriers to PA
5.2. Self-Reported Physical Activity
5.3. Measured Physical Activity
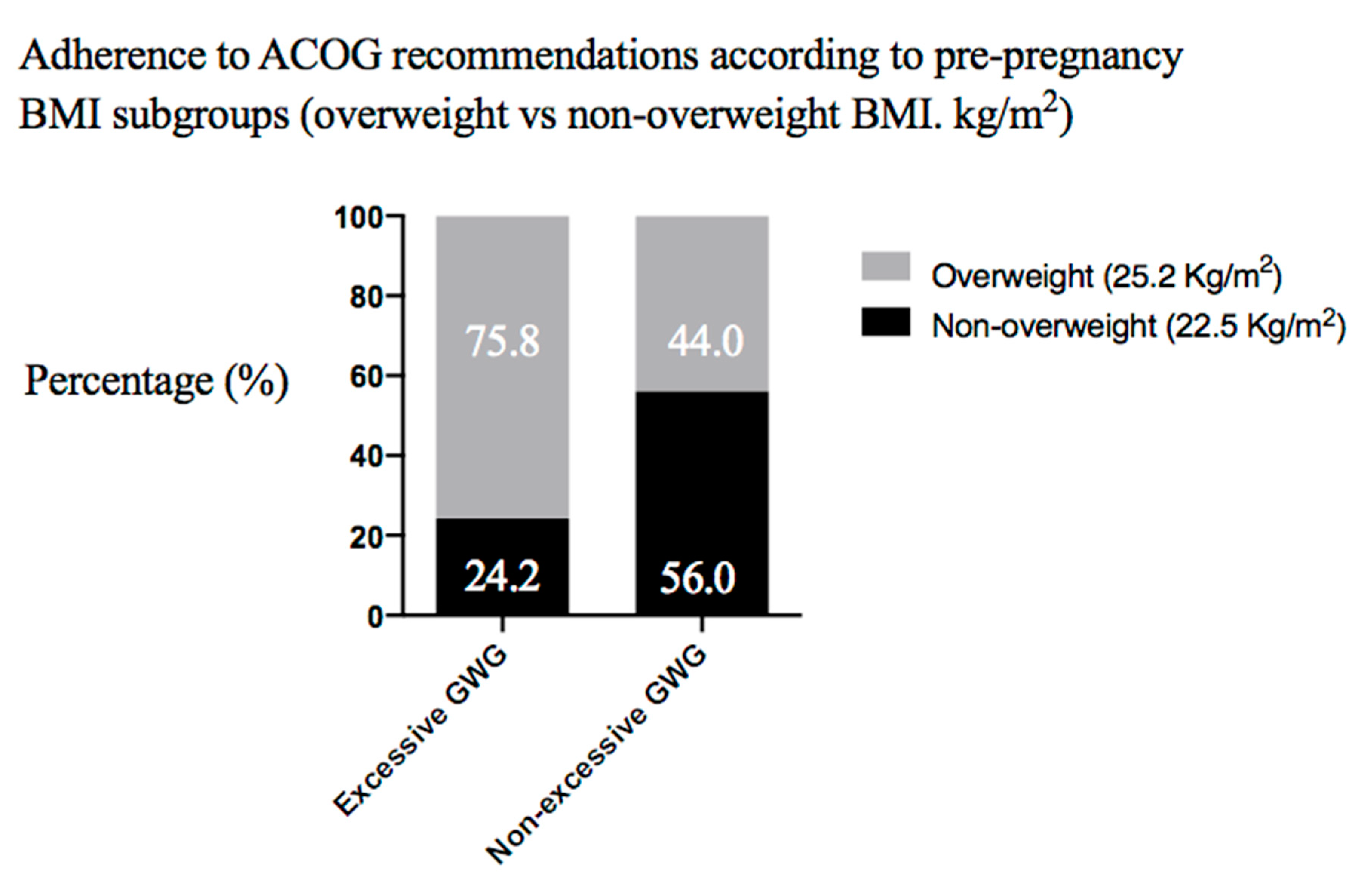
5.4. Maternal Outcomes
5.5. Neonatal Outcomes
6. Discussion
Limitations and Strengths of the Study
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- May, L.E.; Suminski, R.R.; Linklater, E.R.; Jahnke, S.; Glaros, A.G. Exercise during pregnancy: The role of obstetric providers. J. Am. Osteopath. Assoc. 2013, 113, 612–619. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Stengel, M.R.; Kraschnewski, J.L.; Hwang, S.W.; Kjerulff, K.H.; Chuang, C.H. “What my doctor didn’t tell me”: Examining health care provider advice to overweight and obese pregnant women on gestational weight gain and physical activity. Womens Health Issues Off. Publ. Jacobs. Inst. Womens Health 2012, 22, e535–e540. [Google Scholar] [CrossRef] [PubMed]
- Currie, S.; Sinclair, M.; Liddle, D.S.; Nevill, A.; Murphy, M.H. Application of objective physical activity measurement in an antenatal physical activity consultation intervention: A randomised controlled trial. BMC Public Health 2015, 15, 1259. [Google Scholar] [CrossRef] [PubMed]
- Connelly, M.; Brown, H.; van der Pligt, P.; Teychenne, M. Modifiable barriers to leisure-time physical activity during pregnancy: A qualitative study investigating first time mother’s views and experiences. BMC Pregnancy Childbirth 2015, 15, 100. [Google Scholar] [CrossRef]
- Atallah, A.; Pitot, S.; Savin, J.; Moussinga, N.; Laure, P. Physical activity carried out in a general population of Guadeloupe (FWI), determining factors: Results from APHYGUAD study. Sci. Sports 2012, 27, 160–168. [Google Scholar] [CrossRef]
- Carrère, P.; Fagour, C.; Sportouch, D.; Gane-Troplent, F.; Hélène-Pelage, J.; Lang, T.; Inamo, J. Diabetes mellitus and obesity in the French Caribbean: A special vulnerability for women? Women Health 2018, 58, 145–159. [Google Scholar] [CrossRef]
- da Silva Ricardo, L.I.; Evenson, K.R.; Hallal, P.C. Leisure-Time Physical Activity in Pregnancy and Maternal-Child Health: A Systematic Review and Meta-Analysis of Randomized Controlled Trials and Cohort Studies. Sports Med. 2016. [Google Scholar] [CrossRef]
- de Jersey, S.J.; Nicholson, J.M.; Callaway, L.K.; Daniels, L.A. An observational study of nutrition and physical activity behaviours, knowledge, and advice in pregnancy. BMC Pregnancy Childbirth 2013, 13, 115. [Google Scholar] [CrossRef]
- ACOG Committee Opinion. No. 650: Physical Activity and Exercise during Pregnancy and the Postpartum Period. Obstet Gynecol. 2015, 126, e135–e142. [Google Scholar] [CrossRef] [PubMed]
- Birsner, M.L.; Gyamfi-Bannerman, C. Physical Activity and Exercise during Pregnancy and the Postpartum Period: ACOG Committee Opinion, Number 804. Obstet Gynecol. 2020, 135, e178–e188. [Google Scholar]
- Chandonnet, N.; Saey, D.; Alméras, N.; Marc, I. French Pregnancy Physical Activity Questionnaire Compared with an Accelerometer Cut Point to Classify Physical Activity among Pregnant Obese Women. PLoS ONE 2012, 7, e38818. [Google Scholar] [CrossRef] [PubMed]
- Boeselt, T.; Spielmanns, M.; Nell, C.; Storre, J.H.; Windisch, W.; Magerhans, L.; Beutel, B.; Kenn, K.; Greulich, T.; Alter, P.; et al. Validity and Usability of Physical Activity Monitoring in Patients with Chronic Obstructive Pulmonary Disease (COPD). PLoS ONE 2016, 11, e0157229. [Google Scholar] [CrossRef] [PubMed]
- Bell, R.; Tennant, P.W.G.; McParlin, C.; Pearce, M.S.; Adamson, A.J.; Rankin, J.; Robson, S.C. Measuring physical activity in pregnancy: A comparison of accelerometry and self-completion questionnaires in overweight and obese women. Eur. J. Obstet. Gynecol. Reprod Biol. 2013, 170, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. Compendium of Physical Activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [PubMed]
- Evenson, K.R.; Moos, M.-K.; Carrier, K.; Siega-Riz, A.M. Perceived Barriers to Physical Activity among Pregnant Women. Matern. Child Health J. 2009, 13, 364–375. [Google Scholar] [CrossRef]
- Gaston, A.; Cramp, A. Exercise during pregnancy: A review of patterns and determinants. J. Sci. Med. Sport 2011, 14, 299–305. [Google Scholar] [CrossRef]
- Coll, C.V.N.; Domingues, M.R.; Gonçalves, H.; Bertoldi, A.D. Perceived barriers to leisure-time physical activity during pregnancy: A literature review of quantitative and qualitative evidence. J. Sci. Med. Sport 2017, 20, 17–25. [Google Scholar] [CrossRef]
- Thompson, E.L.; Vamos, C.A.; Daley, E.M. Physical activity during pregnancy and the role of theory in promoting positive behavior change: A systematic review. J. Sport Health Sci. 2017, 6, 198–206. [Google Scholar] [CrossRef]
- Harrison Taylor, N.F.; Shields, N.; Frawley, H.C. Attitudes, barriers and enablers to physical activity in pregnant women: A systematic review. J. Physiother. 2018, 64, 24–32. [Google Scholar] [CrossRef]
- Haakstad, L.A.H.; Vistad, I.; Sagedal, L.R.; Lohne-Seiler, H.; Torstveit, M.K. How does a lifestyle intervention during pregnancy influence perceived barriers to leisure-time physical activity? The Norwegian fit for delivery study, a randomized controlled trial. BMC Pregnancy Childbirth 2018, 18, 127. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists. ACOG Committee opinion No. 548: Weight gain during pregnancy. Obstet Gynecol. 2013, 121, 210–212. [Google Scholar] [CrossRef] [PubMed]
- International Association of Diabetes and Pregnancy Study Groups Consensus Panel; Metzger, B.E.; Gabbe, S.G.; Persson, B.; Buchanan, T.A.; Catalano, P.A.; Damm, P.; Dyer, A.R.; de Leiva, A.; Hod, M.; et al. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 2010, 33, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Jelsma, J.G.M.; van Leeuwen, K.M.; Oostdam, N.; Bunn, C.; Simmons, D.; Desoye, G.; Corcoy, R.; Adelantado, J.M.; Kautzky-Willer, A.; Harreiter, J.; et al. Beliefs, Barriers, and Preferences of European Overweight Women to Adopt a Healthier Lifestyle in Pregnancy to Minimize Risk of Developing Gestational Diabetes Mellitus: An Explorative Study. J. Pregnancy 2016, 2016, 3435791. [Google Scholar] [CrossRef] [PubMed]
- Melton, B.F.; Bland, H.W.; Marshall, E.S.; Bigham, L.E. The Effectiveness of a Physical Activity Educational Campaign in a Rural Obstetrics and Gynecology Office. Matern. Child Health J. 2016, 20, 2112–2120. [Google Scholar] [CrossRef]
- Santos Abreu, S.; Moreira, C.; Santos, R.; Ferreira, M.; Alves, O.; Moreira, P.; Mota, J. Physical Activity Patterns during Pregnancy in a Sample of Portuguese Women: A Longitudinal Prospective Study. Iran. Red Crescent Med. J. 2016, 18, e22455. [Google Scholar] [CrossRef]
- Huberty Buman, M.P.; Leiferman, J.A.; Bushar, J.; Adams, M.A. Trajectories of objectively-measured physical activity and sedentary time over the course of pregnancy in women self-identified as inactive. Prev. Med. Rep. 2016, 3, 353–360. [Google Scholar] [CrossRef]
- Fazzi, C.; Saunders, D.H.; Linton, K.; Norman, J.E.; Reynolds, R.M. Sedentary behaviours during pregnancy: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 32. [Google Scholar] [CrossRef]
- Hesketh, K.R.; Evenson, K.R.; Stroo, M.; Clancy, S.M.; Østbye, T.; Benjamin-Neelon, S.E. Physical activity and sedentary behavior during pregnancy and postpartum, measured using hip and wrist-worn accelerometers. Prev. Med. Rep. 2018, 10, 337–345. [Google Scholar] [CrossRef]
- Aittasalo Raitanen, J.; Kinnunen, T.I.; Ojala, K.; Kolu, P.; Luoto, R. Is intensive counseling in maternity care feasible and effective in promoting physical activity among women at risk for gestational diabetes? Secondary analysis of a cluster randomized NELLI study in Finland. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 104. [Google Scholar] [CrossRef]
- Samura, T.; Steer, J.; Michelis, L.D.; Carroll, L.; Holland, E.; Perkins, R. Factors Associated With Excessive Gestational Weight Gain: Review of Current Literature. Glob. Adv. Health Med. 2016, 5, 87–93. [Google Scholar] [CrossRef]
- Lopez-Cepero, A.; Leung, K.; Moore Simas, T.; Rosal, M.C. Association between Obstetric Provider’s Advice and Gestational Weight Gain. Matern. Child Health J. 2018, 22, 1127–1134. [Google Scholar] [CrossRef] [PubMed]
- Kunath, J.; Günther, J.; Rauh, K.; Hoffmann, J.; Stecher, L.; Rosenfeld, E.; Kick, L.; Ulm, K.; Hauner, H. Effects of a lifestyle intervention during pregnancy to prevent excessive gestational weight gain in routine care—The cluster-randomised GeliS trial. BMC Med. 2019, 17, 5. [Google Scholar] [CrossRef] [PubMed]
- Davenport, M.H.; Meah, V.L.; Ruchat, S.-M.; Davies, G.A.; Skow, R.J.; Barrowman, N.; Adamo, K.B.; Poitras, V.J.; E Gray, C.; Garcia, A.J.; et al. Impact of prenatal exercise on neonatal and childhood outcomes: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1386–1396. [Google Scholar] [CrossRef] [PubMed]
- McGee, L.D.; Cignetti, C.A.; Sutton, A.; Harper, L.; Dubose, C.; Gould, S. Exercise During Pregnancy: Obstetricians’ Beliefs and Recommendations Compared to American Congress of Obstetricians and Gynecologists’ 2015 Guidelines. Cureus 2018, 10, e3204. [Google Scholar] [CrossRef]
- Chan, C.W.H.; Au Yeung, E.; Law, B.M.H. Effectiveness of Physical Activity Interventions on Pregnancy-Related Outcomes among Pregnant Women: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 1840. [Google Scholar] [CrossRef] [PubMed]
- Bø, K.; Artal, R.; Barakat, R.; Brown, W.; Davies, G.A.L.; Dooley, M.; Evenson, K.R.; Haakstad, L.A.H.; Henriksson-Larsen, K.; Kayser, B.; et al. Exercise and pregnancy in recreational and elite athletes: 2016 evidence summary from the IOC expert group meeting, Lausanne. Part 1-exercise in women planning pregnancy and those who are pregnant. Br. J. Sports Med. 2016, 50, 571–589. [Google Scholar] [CrossRef]
- Bø, K.; Artal, R.; Barakat, R.; Brown, W.J.; Davies, G.A.L.; Dooley, M.; Evenson, K.R.; Haakstad, L.A.; Kayser, B.; I Kinnunen, T.; et al. Exercise and pregnancy in recreational and elite athletes: 2016/2017 evidence summary from the IOC expert group meeting, Lausanne. Part 5. Recommendations for health professionals and active women. Br. J. Sports Med. 2018, 52, 1080–1085. [Google Scholar] [CrossRef]
- Kinnunen Aittasalo, M.; Koponen, P.; Ojala, K.; Mansikkamäki, K.; Weiderpass, E.; Fogelholm, M.; Luoto, R. Feasibility of a controlled trial aiming to prevent excessive pregnancy-related weight gain in primary health care. BMC Pregnancy Childbirth 2008, 8, 37. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study Participants | Subgroup of Participants with Activity Monitoring | |||||||
|---|---|---|---|---|---|---|---|---|
| All, n = 96 | Intervention (n = 44) | Control (n = 52) | p | All, n = 32 | Intervention (n = 18) | Control (n = 14) | p | |
| Age, years | 29.0 ± 6.7 | 29.4 ± 6.4 | 28.7 ± 6.8 | 0.6 | 28.3 ± 6.1 | 28.8 ± 5.7 | 27.6 ± 6.9 | 0.2 |
| Height, m | 1.64 ± 0.06 | 1.63 ± 0.06 | 1.64 ± 0.06 | 0.4 | 1.64 ± 0.05 | 1.64 ± 0.05 | 1.63 ± 0.06 | 0.3 |
| Gestational age at entry, weeks | 11.9 ± 2.4 | 11.3 ± 2.4 | 12.4 ± 2.2 | 0.02 | 11.8 ± 2.1 | 11.2 ± 2.4 | 12.6 ± 1.5 | 0.06 |
| Pre-pregnancy weight, kg | 72.3 ± 17.4 | 71.7 ± 20.3 | 72.8 ± 14.6 | 0.7 | 71.8 ± 17.2 | 71.6 ± 18.0 | 72.1 ± 16.9 | 0.4 |
| Pre-pregnancy BMI, kg/m2 | 26.7 ± 5.8 | (n = 41) 26.6 ± 6.2 | (n = 45) 26.9 ± 5.5 | 0.4 | 25.9 ± 7.5 | (n = 17) 25.1 ± 8.6 | 26.9 ± 6.0 | 0.4 |
| Pre-pregnancy BMI category, n (%) -BMI < 18.5 kg/m2 | 6/86 (7.0) [0.0–29.4] | 2/41 (4.9) [0.0–11.6] | 4/45 (8.9) [0.0–17.3] | 0.7 | 3/31 (9.7) [0.0–20.3] | 1/17 (5.9) [0.0–17.4] | 2/14 (14.3) [0.0–33.3] | 0.7 |
| -BMI 18.5–24.9 kg/m2 | 31/86 (36.0) [18.8–53.2] | 17/41 (41.5) [26.2–56.8] | 14/45 (31.1) [17.4–44.8] | 9/31 (29.0) [12.8–45.2] | 6/17 (35.3) [11.9–58.7] | 3/14 (21.4) [0.0–43.7] | ||
| -BMI 25.0–29.9 kg/m2 | 22/86 (25.6) [6.9–44.3] | 10/41 (24.4) [11.1–37.7] | 12/45 (26.7) [13.6–39.8] | 9/31 (29.0) [12.8–45.2] | 5/17 (29.4) [7.1–51.7] | 4/14 (28.6) [4.0–53.2] | ||
| -BMI 30.0–40.0 kg/m2 | 27/86 (31.4) (13.6–49.2) | 12/41 (29.3) (15.2–43.4) | 15/45 (33.3) [19.4–47.2] | 10/31 (32.3) [15.6–49.0] | 5/17 (29.4) [7.1–51.7] | 5/14 (35.7) [9.7–61.7] | ||
| Marital status, n (%) -Single | 29/79 (36.7) [26.0–47.4] | 9/39 (23.1) [9.7–36.5] | 20/40 (50.0) [34.3–65.7] | 0.01 | 9/29 (31.0) [13.9–48.1] | 2/17 (11.8) [0.0–27.6] | 7/12 (58.3) [29.2–87.4] | 0.01 |
| -Living with partner/married | 50/79 (63.3) [52.6–74.0] | 30/39 (76.9) [63.5–90.3] | 20/40 (50.0) [34.3–65.7] | 20/29 (69.0) [51.9–86.1] | 15/17 (88.2) [72.4–100.0] | 5/12 (41.7) [12.6–70.8] | ||
| Educational level, n (%) -Higher Education | 32/79 (40.5) [29.6–51.4] | 20/39 (51.3) [35.4–67.2] | 12/40 (30.0) [15.6–44.4] | 0.02 | 15/29 (51.7) [33.2–70.2] | 12/17 (70.6) [48.3–92.9] | 3/12 (25.0) [0.0–50.6] | 0.04 |
| -Secondary | 19/79 (24.1) [14.6–33.6] | 11/39 (28.2) [13.9–42.5] | 8/40 (20.0) [7.4–32.6] | 4/29 (13.8) [1.0–26.5] | 2/17 (11.8) [0.0–27.6] | 2/12 (16.7) [0.0–38.7] | ||
| -Before secondary | 28/79 (35.4) [24.8–46.0] | 8/39 (28.6) [14.2–43.0] | 20/40 (50.0) [34.3–65.7] | 10/29 (34.5) [17.6–53.1] | 3/17 (17.6) [0.0–36.3] | 7/12 (58.3) [29.2–87.4] | ||
| Intervention | Control | |||||
|---|---|---|---|---|---|---|
| First Trimester | Second Trimester | Third Trimester | First Trimester | Second Trimester | Third Trimester | |
| Intrapersonal | ||||||
| Negatively related | ||||||
| Weight related to pregnancy | 1 (3.0) | 4 (12.1) * | 10 (31.3) | 3 (8.1) | 12 (32.4) | 17 (45.9) |
| Insecurity related to practice | 11 (33.3) * | 9 (27.3) * | 9 (28.1) * | 22 (59.5) | 22 (59.5) | 21 (56.8) |
| Fatigue after work | 14 (42.4) * | 13 (39.4) | 16 (50.0) | 24 (64.9) | 20 (54.1) | 22 (59.5) |
| Positively related | ||||||
| Being motivated | 28 (84.8) | 27 (81.8) * | 26 (81.3) * | 25 (67.6) | 20 (54.1) | 17 (45.9) |
| Interpersonal | ||||||
| Negatively related | ||||||
| Lack of information about benefits and risks, n (%) | 7 (21.2) | 4 (12.1) * | 1 (3.1) ** | 7 (18.9) | 14 (37.8) | 12 (32.4) |
| Lack of friendly support | 6 (18.2) * | 7 (21.2) * | 7 (21.9) | 15 (40.5) | 17 (45.9) | 15 (40.5) |
| Environment | ||||||
| Negatively related | ||||||
| Lack of sports facilities | 6 (18.2) * | 7 (21.2) * | 15 (46.9) | 15 (40.5) | 15 (40.5) | 17 (45.9) |
| First Trimester | Second Trimester | Third Trimester | Trimester Effect | |
|---|---|---|---|---|
| Total MET-h/week | 274.3 (177.9–400.5) | 191.4 (131.3–259.17) | 115.5 (92.4–169.2) | * |
| By intensity | ||||
| Sedentary | 66.6 (43.5–91.7) | 49.7 (35.0–76.2) | 43.5 (18.8–69.1) | * |
| Light | 112.8 (74.6–162.7) | 79.8 (39.6–117.6) | 52.6 (23.1–72.6) | * |
| Moderate | 76.7 (33.2–146.0) | 48.5 (18.6–84.6) | 19.2 (7.0–39.3) | * |
| Vigorous | 1.6 (0.0–4.8) | 0.0 (0.0–1.6) | 0.0 (0.0–0.0) | * |
| By type | ||||
| Household/caregiving | 116.9 (72.4–171.5) | 79.1 (38.8–122.4) | 48.3 (23.0–73.4) | * |
| Occupational | 62.1 (0.0–111.1) | 0.0 (0.0–63.5) | 0.0 (0.0–0.0) | * |
| Sports/Exercise | 14.1 (5.9–29.8) | 8.8 (2.5–21.5) | 6.1 (0.8–13.1) | * |
| Intervention | Control | |||||
|---|---|---|---|---|---|---|
| First Trimester | Second Trimester | Third Trimester | First Trimester | Second Trimester | Third Trimester | |
| Total MET-h/week | 275.9 (198.3–421.6) | 170.6 (130.2–254.4) | 128.3 (96.3–183.7) | 274.3 (160.4–390.9) | 196.7 (144.4–259.7) | 98.9 (78.5–152.2) |
| By intensity | ||||||
| Sedentary | 70.0 (48.0–92.2) | 49.7 (35.7–76.2) | 64.7 (36.4–78.7) * | 56.1 (37.8–88.1) | 50.7 (30.3–75.8) | 22.7 (9.4–49.8) |
| Light | 104.3 (66.2–170.2) | 73.2 (30.1–125.0) | 52.1 (20.4–73.2) | 122.3 (80.5–156.3) | 88.2 (62.1–110.9) | 52.6 (27.6–70.0) |
| Moderate | 89.3 (30.4–168.4) | 45.7 (18.5–86.0) | 18.5 (3.4–33.2) | 66.3 (35.4–128.2) | 53.7 (19.3–84.6) | 20.0 (10.4–43.5) |
| Vigorous | 1.6 (0.0–4.8) | 0 (0–1.6) | 0 (0–0) | 1.6 (0–5.2) | 0 (0–1.6) | 0 (0–0) |
| By type | ||||||
| Household/caregiving | 126.4 (74.4–180.6) | 74.6 (28.7–129.5) | 36.1 (18.5–71.2) | 94.8 (67.6–160.1) | 87.6 (48.1–120.2) | 53.5 (29.6–74.7) |
| Occupational | 65.4 (6.2–112.0) | 0 (0–68.4) | 0 (0–0) | 35.8 (0–111.1) | 0 (0–57.8) | 0 (0–0) |
| Sports/Exercise | 14.2 (5.6–24.7) | 8.5 (3.4–13.8) | 7.9 (0.4–13.2) | 13.3 (6.4–31.4) | 8.8 (1.7–22.5) | 6.0 (0.8–12.9) |
| Intervention | Control | ||||||
|---|---|---|---|---|---|---|---|
| First Trimester | Second Trimester | Third Trimester | First Trimester | Second Trimester | Third Trimester | p | |
| Number of steps/hours | 477 ± 61 | 408 ± 53 | 335 ± 31 | 575 ± 69 | 483 ± 60 | 378 ± 35 | >0.5 |
| Intervention | Control | OR (95%CI) Intervention/Control | p | |
|---|---|---|---|---|
| Excessive GWG n (%) | 16 (40.0) | 17 (39.5) | 1.02 (0.42–2.45) | 0.5 |
| GDM n (%) | 8 (21.6) | 4 (10.3) | 2.41 (0.66–8.83) | 0.1 |
| Fasting plasma glucose (g/l) | Group: 0.04; Time: 0.6 Group*time: 0.3 | |||
| Trimester 1 | 0.77 ± 0.05 | 0.76 ± 0.06 | ||
| Trimester 2 | 0.80 ± 0.08 | 0.76 ± 0.06 | ||
| Trimester 3 | 0.79 ± 0.09 | 0.76 ± 0.06 | ||
| OGTT (g/l) | Group: 0.5; Time: <0.001 Group*time: 0.3 | |||
| T0 | 0.80 ± 0.08 1.23 ± 0.29 | 0.76 ± 0.06 1.25 ± 0.23 | ||
| T60 | ||||
| T120 | 1.15 ± 0.28 | 1.10 ± 0.20 | ||
| Area under the curve (AUC) | 204 ± 42 | 201 ± 32 | 0.7 | |
| Maternal hypertension during labor, n/% | 7 (16.3) | 9 (21.4) | 0.71 (0.23–2.13) | 0.3 |
| Cesarean | 7 (15.9) | 6 (12.5) | 0.75 (0.23–2.44) | 0.4 |
| Intervention | Control | OR (95%CI) Intervention/Control | p | |
|---|---|---|---|---|
| Gestational age at delivery (WA) | 39.4 (39.4–41.1) | 39.4 (39.4–39.4) | 0.7 | |
| Preterm birth, n (%) | 2 (4.5) | 3 (6.1) | 1.37 (0.21–8.60) | 0.5 |
| Weight, kilograms | Group: 0.1; Age effect: <0.001 Group *age effect: 0.9 | |||
| Birth | 3.09 ± 0.41 | 3.23 ± 0.47 | ||
| First month | 4.08 ± 0.54 | 4.27 ± 0.64 | ||
| Second month | 5.25 ± 0.74 | 5.43 ± 0.73 | ||
| Length, meter | Group: 0.1; Age effect: <0.001 Group *age effect: 0.1 | |||
| Birth | 49.6 ± 2.24 | 50.0 ± 1.96 | ||
| First month | 53.0 ± 2.54 | 53.8 ± 3.24 | ||
| Second month | 56.8 ± 2.27 | 58.3 ± 3.62 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruart, S.; Sinnapah, S.; Hue, O.; Janky, E.; Antoine-Jonville, S. Prenatal Counseling throughout Pregnancy: Effects on Physical Activity Level, Perceived Barriers, and Perinatal Health Outcomes: A Quasi-Experimental Study. Int. J. Environ. Res. Public Health 2020, 17, 8887. https://doi.org/10.3390/ijerph17238887
Ruart S, Sinnapah S, Hue O, Janky E, Antoine-Jonville S. Prenatal Counseling throughout Pregnancy: Effects on Physical Activity Level, Perceived Barriers, and Perinatal Health Outcomes: A Quasi-Experimental Study. International Journal of Environmental Research and Public Health. 2020; 17(23):8887. https://doi.org/10.3390/ijerph17238887
Chicago/Turabian StyleRuart, Shelly, Stéphane Sinnapah, Olivier Hue, Eustase Janky, and Sophie Antoine-Jonville. 2020. "Prenatal Counseling throughout Pregnancy: Effects on Physical Activity Level, Perceived Barriers, and Perinatal Health Outcomes: A Quasi-Experimental Study" International Journal of Environmental Research and Public Health 17, no. 23: 8887. https://doi.org/10.3390/ijerph17238887
APA StyleRuart, S., Sinnapah, S., Hue, O., Janky, E., & Antoine-Jonville, S. (2020). Prenatal Counseling throughout Pregnancy: Effects on Physical Activity Level, Perceived Barriers, and Perinatal Health Outcomes: A Quasi-Experimental Study. International Journal of Environmental Research and Public Health, 17(23), 8887. https://doi.org/10.3390/ijerph17238887