Feasibility and Clinical Usefulness of the Unified Protocol in Online Group Format for Bariatric Surgery Candidates: Study Protocol for a Multiple Baseline Experimental Design




Abstract
1. Introduction
2. Materials and Methods
2.1. Sample and Recruitment
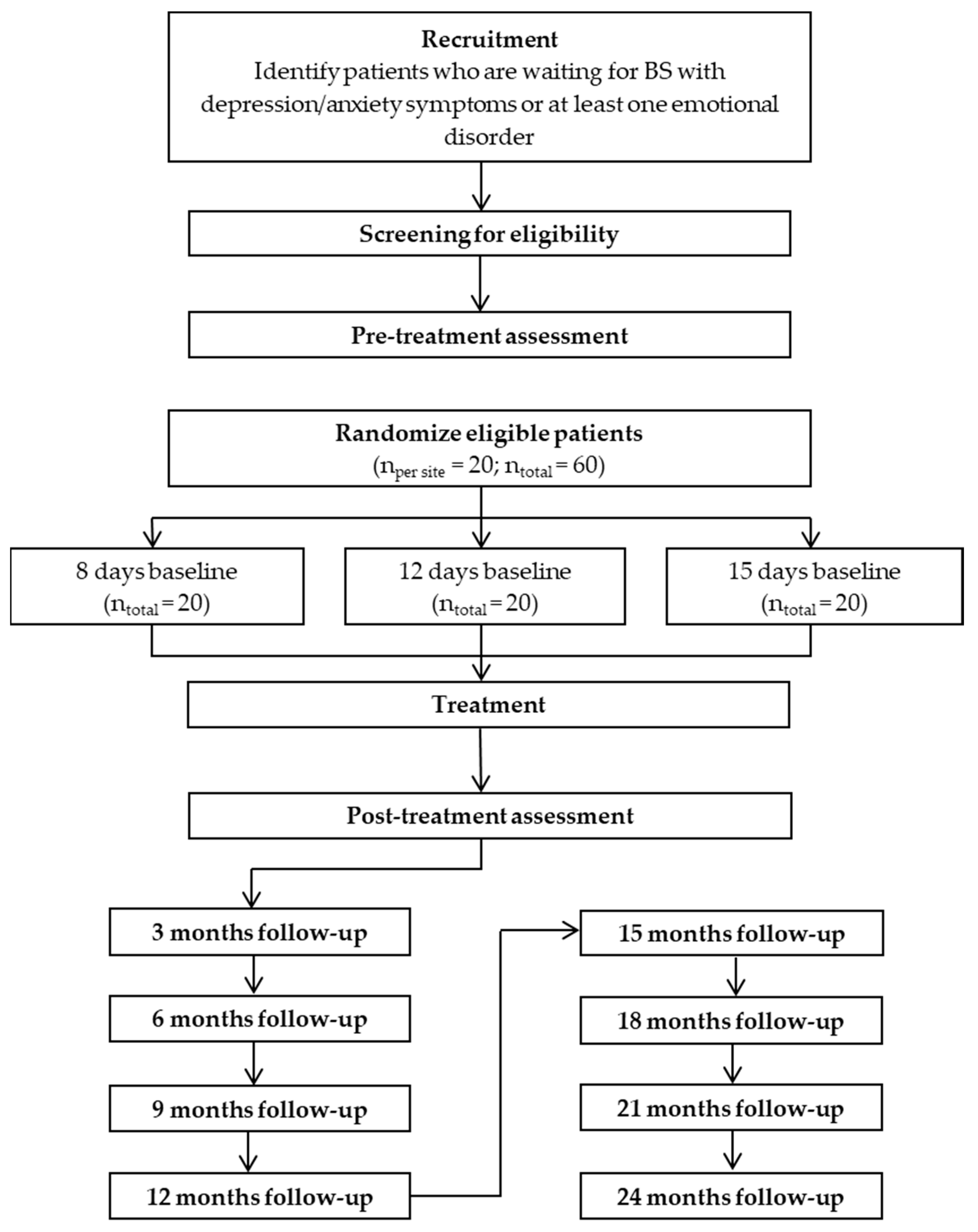
2.2. Procedure
2.3. Eligibility Criteria
2.4. Ethics
2.5. Measures
2.5.1. Primary Outcomes
2.5.2. Secondary Outcomes
2.5.3. Baseline Assessment
2.5.4. Assessment during Treatment
2.6. Data Analysis
3. Expected Results
4. Discussion
- It can allow clinicians to use a single treatment for those candidates who present different EDs, with comorbidity, and also with subclinical symptoms or unspecified disorders [15].
- In other public health systems similar to the Spanish one, where onsite specific CBT is the most common delivery format, and therapy sessions occur at long intervals (e.g., more than a month) due to waiting lists, a UP online group intervention can help to increase the frequency of sessions and reduce costs because there are more patients treated simultaneously (five to eight patients in the same group), which can facilitate better patient care.
- Thanks to the online format, this intervention will facilitate access to psychological interventions in those candidates who face mobility challenges due to their obesity condition [31]. This innovative approach would be in line with the goals of the World Health Organization proposed in the mental health action plan to use electronic technologies to expand the delivery of mental health care [83].
- The fact of receiving quarterly follow-ups up to two years after treatment allows guaranteeing the prevention of relapses and maintaining the results, especially beyond the year and a half or two years, which is the moment in which the literature recognizes that pre-BS problems tend to reappear [42].
- Furthermore, this advantage offered by long term relapse prevention follow-ups leads to a condition of reduced healthcare costs that are associated with the care of comorbid health problems in this type of patients [3].
- And finally, it is known that group therapy provides benefits to the patient that are not obtained with individual treatment, such as reducing isolation, facilitating social support, and learning from the experiences of others [33], which could improve its efficiency.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Yumuk, V.; Tsigos, C.; Fried, M.; Schindler, K.; Busetto, L.; Micic, D.; Toplak, H. European Guidelines for Obesity Management in Adults. Obes. Facts 2015, 8, 402–424. [Google Scholar] [CrossRef] [PubMed]
- Oltmanns, J.R.; Rivera, J.; Cole, J.; Merchant, A.; Steiner, J.P. Personality psychopathology: Longitudinal prediction of change in body mass index and weight post-bariatric surgery. Health Psychol. 2020, 39, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Hernáez, A.; Zomeño, M.D.; Dégano, I.R.; Pérez-Fernández, S.; Goday, A.; Vila, J.; Civeira, F.; Moure, R.; Marrugat, J. Exceso de peso en España: Situacioón actual, proyecciones para 2030 y sobrecoste directo estimado para el Sistema Nacional de Salud [Excess Weight in Spain: Current Situation, Projections for 2030, and Estimated Direct Extra Cost for the Spanish Health Sy. Span. J. Cardiol. 2019, 72, 916–924. [Google Scholar] [CrossRef]
- Castaneda, D.; Popov, V.B.; Wander, P.; Thompson, C.C. Risk of Suicide and Self-harm Is Increased After Bariatric Surgery—A Systematic Review and Meta-analysis. Obes. Surg. 2019, 29, 322–333. [Google Scholar] [CrossRef]
- De Luca, M.; Angrisani, L.; Himpens, J.; Busetto, L.; Scopinaro, N.; Weiner, R.; Sartori, A.; Stier, C.; Lakdawala, M.; Bhasker, A.G.; et al. Indications for Surgery for Obesity and Weight-Related Diseases: Position Statements from the International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO). Obes. Surg. 2016, 26, 1659–1696. [Google Scholar] [CrossRef]
- OECD/European Union. Health at a Glance: Europe 2018: State of Health in the EU Cycle; OECD Publishing, Paris/European Union: Brussels, Belgium, 2018. [Google Scholar] [CrossRef]
- Spirou, D.; Raman, J.; Smith, E. Psychological outcomes following surgical and endoscopic bariatric procedures: A systematic review. Obes. Rev. 2020, e12998. [Google Scholar] [CrossRef]
- Dixon, J.B.; Dixon, M.E.; O’Brien, P.E. Depression in Association With Severe Obesity. Arch. Intern. Med. 2003, 163, 2058. [Google Scholar] [CrossRef]
- OECD. The Heavy Burden of Obesity: The Economics of Prevention, OECD Health Policy Studies 2019; OECD: Paris, France, 2019. [Google Scholar] [CrossRef]
- Jumbe, S.; Hamlet, C.; Meyrick, J. Psychological Aspects of Bariatric Surgery as a Treatment for Obesity. Curr. Obes. Rep. 2017, 6, 71–78. [Google Scholar] [CrossRef]
- Lauren, A.D.; Sijercic, I.; Cassin, S.E. Preoperative and post-operative psychosocial interventions for bariatric surgery patients: A systematic review. Obes. Rev. 2020, e12926. [Google Scholar] [CrossRef]
- Sarwer, D.B.; Heinberg, L.J. A Review of the Psychosocial Aspects of Clinically Severe Obesity and Bariatric Surgery. Am. Psychol. Assoc. 2020, 75, 252–264. [Google Scholar] [CrossRef]
- Geller, S.; Dahan, S.; Levy, S.; Goldzweig, G.; Hamdan, S.; Abu-Abeid, S. Body Image and Emotional Eating as Predictors of Psychological Distress Following Bariatric Surgery. Obes. Surg. 2019. [Google Scholar] [CrossRef] [PubMed]
- Institute for Health Metrics and Evaluation. Global Health Data Exchange. Available online: http://ghdx.healthdata.org/gbd-results-tool (accessed on 5 May 2020).
- Barlow, D.H.; Farchione, T.J.; Sauer-Zavala, S.; Murray-Latin, H.; Ellard, K.K.; Bullis, J.R.; Bentley, K.H.; Boettcher, H.T.; Cassiello-Robbins, C. Unified Protocol for Transdiagnostic Treatment of Emotional Disorders: Therapist Guide, 2nd ed.; Oxford University Press: New York, NY, USA, 2018. [Google Scholar]
- Lim, R.B.C.; Zhang, M.W.B.; Ho, R.C.M. Prevalence of all-cause mortality and suicide among bariatric surgery cohorts: A meta-analysis. Int. J. Environ. Res. Public Health 2018, 15, 1519. [Google Scholar] [CrossRef] [PubMed]
- Barlow, D.H.; Farchione, T.J.; Bullis, J.R.; Gallagher, M.W.; Murray-Latin, H.; Sauer-Zavala, S.; Bentley, K.H.; Thompson-Hollands, J.; Conklin, L.R.; Boswell, J.F.; et al. The unified protocol for transdiagnostic treatment of Emotional Disorders compared with diagnosis-specific protocols for anxiety disorders: A randomized clinical trial. JAMA Psychiatry 2017, 74, 875–884. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.; Campbell, L.; Lehman, C.; Grisham, J.; Mancill, R. Current and Lifetime Comorbidity of the DSM-IV Anxiety and Mood Disorders in a Large Clinical Sample. J. Abnorm. Psychol. 2001, 110, 585–599. [Google Scholar] [CrossRef] [PubMed]
- McManus, F.; Shafran, R.; Cooper, Z. What does a ’transdiagnostic approach have to offer the treatment of anxiety disorders? Br. J. Clin. Psychol. 2010, 49, 491–505. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.A.; Barlow, D.H. A proposal for a dimensional classification system based on the shared features of the DSM-IV Anxiety and Mood Disorders: Implications for Assessment and Treatment. Psychol. Assess. 2009, 21, 256–271. [Google Scholar] [CrossRef]
- Sauer-Zavala, S.; Cassiello-Robbins, C.; Conklin, L.R.; Bullis, J.R.; Thompson-Hollands, J.; Kennedy, K.A. Isolating the Unique Effects of the Unified Protocol Treatment Modules Using Single Case Experimental Design. Behav. Modif. 2017, 41, 286–307. [Google Scholar] [CrossRef]
- Sauer-Zavala, S.; Cassiello-Robbins, C.; Ametaj, A.A.; Wilner, J.G.; Pagan, D. Transdiagnostic Treatment Personalization: The Feasibility of Ordering Unified Protocol Modules According to Patient Strengths and Weaknesses. Behav. Modif. 2019, 43, 518–543. [Google Scholar] [CrossRef]
- Sakiris, N.; Berle, D. A systematic review and meta-analysis of the Unified Protocol as a transdiagnostic emotion regulation based intervention. Clin. Psychol. Rev. 2019, 72, 1017–1051. [Google Scholar] [CrossRef]
- Weihs, K.L.; McConnell, M.H.; Wiley, J.F.; Crespi, C.M.; Sauer-Zavala, S.; Stanton, A.L. A Preventive Intervention to Modify Depression Risk Targets after Breast Cancer Diagnosis: Design and Single-Arm Pilot Study. Psychooncology 2019, 28, 880–887. [Google Scholar] [CrossRef]
- Parsons, J.T.; Rendina, H.J.; Moody, R.L.; Gurung, S.; Starks, T.J.; Pachankis, J.E. Feasibility of an Emotion Regulation Intervention to Improve Mental Health and Reduce HIV Transmission Risk Behaviors for HIV-Positive Gay and Bisexual Men with Sexual Compulsivity. Aids Behav. 2017, 21, 1540–1549. [Google Scholar] [CrossRef] [PubMed]
- Johari-Fard, R.; Ghafourpour, R. The effectiveness of Unified Treatment approach on quality of life and symptoms of patients with irritable bowel syndrome referred to gastrointestinal clinics. Int. J. BodyMind Cult. 2015, 2, 85–94. [Google Scholar]
- Andersson, G. Internet-Delivered Psychological Treatments. Annu. Rev. Clin. Psychol. 2016, 12, 157–179. [Google Scholar] [CrossRef] [PubMed]
- Andersson, G. Using the Internet to provide cognitive behaviour therapy. Behav. Res. Ther. 2009, 47, 175–180. [Google Scholar] [CrossRef]
- Andrews, G.; Cuijpers, P.; Craske, M.G.; McEvoy, P.; Titov, N. Computer therapy for the anxiety and depressive disorders is effective, acceptable and practical health care: A meta-analysis. PLoS ONE 2010, 5. [Google Scholar] [CrossRef]
- Andreu-pejó, L.; Martínez-borba, V.; Suso-ribera, C.; Osma, J. Can we predict the evolution of depressive symptoms, adjustment, and perceived social support of pregnant women from their personality characteristics? A technology-supported longitudinal study. Int. J. Environ. Res. Public Health 2020, 17, 3439. [Google Scholar] [CrossRef]
- King, W.C.; Engel, S.G.; Elder, K.A.; Chapman, W.H.; Eid, G.M.; Wolfe, B.M.; Belle, S.H. Walking capacity of bariatric surgery candidates. Surg. Obes. Relat. Dis. 2012, 8, 48–59. [Google Scholar] [CrossRef][Green Version]
- Wind, T.R.; Rijkeboer, M.; Andersson, G.; Riper, H. The COVID-19 pandemic: The ‘black swan’ for mental health care and a turning point for e-health. Internet Interv. 2020, 20, 100317. [Google Scholar] [CrossRef]
- Yalom, I.D.; Leszcz, M. The Theory and Practice of Group Therapy, 5th ed.; IUP: New York, NY, USA, 2005. [Google Scholar]
- Kratochwill, T.R.; Hitchcock, J.H.; Horner, R.H.; Levin, J.R.; Odom, S.L.; Rindskopf, D.M.; Shadish, W.R. Single-Case Intervention Research Design Standards. Remed. Spec. Educ. 2012, 34, 26–38. [Google Scholar] [CrossRef]
- Hawkins, N.G.; Sanson-Fisher, R.W.; Shakeshaft, A.; D’Este, C.; Green, L.W. The multiple baseline design for evaluating population-based research. Am. J. Prev. Med. 2007, 33, 162–168. [Google Scholar] [CrossRef]
- Barlow, D.H.; Nock, M.K.; Hersen, M. Single Case Experimental Designs: Strategies for Studying Behavior Change, 3rd ed.; Allyn & Bacon: Boston, MA, USA, 2009. [Google Scholar]
- Barlow, H.D.; Durand, V.M.; Hofmann, S.G. Abnormal Psychology: An Integrative Approach, 8th ed.; Cengage Learning: Boston, MA, USA, 2018. [Google Scholar]
- Kratochwill, T.R.; Hitchcock, J.; Horner, R.H.; Levin, J.R.; Odom, S.L.; Rindskopf, D.M.; Shadish, W.R. Single-Case Design Technical Documentation. What Work. Clear. House 2010. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Bell, M.L.; Whitehead, A.L.; Julious, S.A. Guidance for using pilot studies to inform the design of intervention trials with continuous outcomes. Clin. Epidemiol. 2018, 10, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Cassin, S.; Sockalingam, S.; Du, C.; Wnuk, S.; Hawa, R.; Parikh, S.V. A pilot randomized controlled trial of telephone-based cognitive behavioural therapy for preoperative bariatric surgery patients. Behav. Res. Ther. 2016, 80, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Sockalingam, S.; Leung, S.E.; Hawa, R.; Wnuk, S.; Parikh, S.V.; Jackson, T.; Cassin, S.E. Telephone-based cognitive behavioural therapy for female patients 1-year post-bariatric surgery: A pilot study. Obes. Res. Clin. Pract. 2019, 13, 499–504. [Google Scholar] [CrossRef]
- Andersson, G.; Cuijpers, P. Internet-based and other computerized psychological treatments for adult depression: A meta-analysis. Cogn. Behav. Ther. 2009, 38, 196–205. [Google Scholar] [CrossRef]
- Martín, E.; Ruiz-Tovar, J.; Sánchez, R. Vía Clínica de Cirugía Bariátrica 2017; Im3mediA comunicación: Albacete, Spain, 2017. [Google Scholar]
- Qualtrics (Version 2.16); Qualtrics software: Provo, UT, USA, 2017.
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for the Beck Depression Inventory-II; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Sanz, J.; Perdigón, A.L.; Vázquez, C. The Spanish adaptation of the Beck’s Depression Inventory-II (BDI-II): Psychometric properties in the general population. Clin. Salud 2003, 14, 249–280. [Google Scholar]
- Beck, A.T.; Steer, R. Beck Anxiety Inventory Manual; Psychological Corporation: San Antonio, TX, USA, 1993. [Google Scholar]
- Magán, I.; Sanz, J.; García-Vera, M.P. Psychometric properties of a Spanish version of the Beck Anxiety Inventory (BAI) in general population. Span. J. Psychol. 2008, 11, 626–640. [Google Scholar] [CrossRef]
- Sheehan, D.V. Mini International Neuropsychiatric Interview 7.0. (MINI 7.0); Medical Outcomes Systems: Jacksonville, FL, USA, 2015. [Google Scholar]
- Ministerio de Justicia. Real Decreto 1720/2008, de 19 de Enero, Para la Aprobación de la Ley Orgánica 15/1999 de Protección de Datos de Carácter Personal. Boletín Oficial del Estado, 19 January 2008; pp. 4103–4136.
- Asociación Medica Mundial Declaración de Helsinki. Principios éticos Para las Investigaciones Con Seres Humanos. In Proceedings of the 59th Asamblea General, Seúl, Korea, 18 October 2008.
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Personal. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef]
- Sandín, B.; Chorot, P.; Lostao, L.; Joiner, T.E.; Santed, M.A.; Valiente, R.M. Escalas PANAS de Afecto Positivo y Negativo: Validación factorial y convergencia transcultural. Psicothema 1999, 11, 37–51. [Google Scholar]
- Costa, P.T.; McCrae, R.R. Revised NEO Personality Inventory (NEO-PI-R) and NEO Five-Factor Inventory (NEO-FFI); TEA Ediciones: Madrid, Spain, 1999. [Google Scholar]
- Mezzich, J.E.; Ruipérez, M.A.; Pérez, C.; Yoon, G.; Liu, J.; Mahmud, S. The Spanish Version of the Quiality of Life Index. J. Nerv. Ment. Dis. 2000, 188, 301–305. [Google Scholar] [CrossRef]
- Brooks, R. EuroQol: The current state of play. Health Policy 1996, 37, 53–72. [Google Scholar] [CrossRef]
- Badia, X.; Roset, M.; Montserrat, S.; Herdman, M.; Segura, A. La versión española del EuroQol: Descripción y aplicaciones EuroQol Spanish Version: Description and Aplications. Clin. Med. 1999, 112, 79–86. [Google Scholar]
- Echeburúa, E.; Corral, P.; Fernández-Montalvo, J. Maladjustment Inventory (MI): Psychometric properties in clinical contexts. Análisis Modif. Conducta 2000, 26, 325–340. [Google Scholar]
- Gratz, K.L.; Roemer, L. Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the difficulties in emotion regulation scale. J. Psychopathol. Behav. Assess. 2004, 26, 41–54. [Google Scholar] [CrossRef]
- Hervás, G.; Jódar, R. The Spanish version of the Difficulties in Emotion Regulation Scale. Clin. Salud 2008, 19, 139–156. [Google Scholar]
- Gámez, W.; Chmielewski, M.; Kotov, R.; Ruggero, C.; Suzuki, N.; Watson, D. The Brief Experiential Avoidance Questionnaire: Development and initial validation. Psychol. Assess. 2014, 26, 35–45. [Google Scholar] [CrossRef]
- Vázquez-Morejón, R.; León, J.M.; Martín, A.; Vazquez, A.J. Validation of a spanish version of the brief experiential avoidance questionnaire (BEAQ) in clinical population. Psicothema 2019, 31, 335–340. [Google Scholar] [CrossRef]
- Cardaciotto, L.; Herbert, J.D.; Forman, E.M.; Moitra, E.; Farrow, V. The assessment of present-moment awareness and acceptance: The Philadelphia Mindfulness Scale. Assessment 2008, 15, 204–223. [Google Scholar] [CrossRef]
- Tejedor, R.; Feliu-Soler, A.; Pascual, J.C.; Cebolla, A.; Portella, M.J.; Trujols, J.; Soriano, J.; Pérez, V.; Soler, J. Psychometric properties of the Spanish version of the Philadelphia Mindfulness Scale. Rev. Psiquiatr. Salud Ment. 2014, 7, 157–165. [Google Scholar] [CrossRef]
- Gross, J.J.; John, O.P. Individual differences in two emo- tion regulation processes: Implications for affect, relationships, and well-being. J. Personal. Soc. Psychol. 2003, 85, 348–362. [Google Scholar] [CrossRef]
- Cabello, R.; Salguero, J.M.; Fernández-Berrocal, P.; Gross, J.J. A Spanish adaptation of the Emotion Regulation Questionnaire. Eur. J. Psychol. Assess. 2013, 29, 234–240. [Google Scholar] [CrossRef]
- Henderson, M.; Freeman, C.P.L. A self-rating scale for bulimia the ‘bite’. Br. J. Psychiatry 1987, 150, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Moya, T.R.; Bersabé, R.; Jiménez, M. Fiabilidad y validez del test de investigación bulímica de Edimburgo (BITE) en una muestra de adolescentes españoles; Reliability and validity of the Bulimic Investigatory Test Edinburgh (BITE) in a sample of Spanish adolescents. Psicol. Conduct. 2004, 12, 447–461. [Google Scholar]
- Cooper, P.J.; Taylor, M.J.; Cooper, Z.; Fairburn, C.G. The development and validation of the Body Shape Questionnaire. Int. J. Eat. Disord. 1987, 6, 485–494. [Google Scholar] [CrossRef]
- Raich, R.M.; Mora, M.; Soler, A.; Avila, C.; Clos, I.; Zapater, L. Adaptación de un instrumento de evaluación de la insatisfacción corporal; Adaptation of a body dissatisfaction assessment instrument. Clin. Health 1996, 7, 51–66. [Google Scholar]
- Arnow, B.; Kenardy, J.; Agras, W. The Emotional Eating Scale: The development of a measure to assess coping with negative affect by eating. Int. J. Eat. Disord. 1995, 18, 79–90. [Google Scholar] [CrossRef]
- Suso-Ribera, C.; Castilla, D.; Zaragozá, I.; Ribera-Canudas, M.V.; Botella, C.; García-Palacios, A. Validity, Reliability, Feasibility, and Usefulness of Pain Monitor, a Multidimensional Smartphone App for Daily Monitoring of Adults with Heterogeneous Chronic Pain. Clin. J. Pain 2018, 34, 900–908. [Google Scholar] [CrossRef]
- Norman, S.B.; Cissel, S.H.; Means-Christensen, A.J.; Stein, M.B. Development and validation of an Overall Anxiety Severity and Impairment Scale. Depress. Anxiety 2006, 23, 245–249. [Google Scholar] [CrossRef]
- Bentley, K.H.; Gallagher, M.W.; Carl, J.R.; Barlow, D.H. Development and validation of the Overall Depression Severity and Impairment Scale. Psychol. Assess. 2014, 26, 815–830. [Google Scholar] [CrossRef]
- Osma, J.; Quilez-Orden, A.; Suso-Ribera, C.; Peris-Baquero, O.; Norman, S.B.; Bentley, K.H.; Sauer-Zavala, S. Psychometric properties and validation of the Spanish versions of the overall anxiety and depression severity and impairment scales. J. Affect. Disord. 2019, 252, 9–18. [Google Scholar] [CrossRef]
- Barlow, D.; Sauer-Zavala, S.; Farchione, T.; Murray, H.; Ellard, K.; Bullis, J.; Castellano-Robbins, C. The Unified Protocol for Transdiagnostic Treatment of Emotional Disorders: Client Workbook, 2nd ed.; Oxford University Press: New York, NY, USA, 2018. [Google Scholar]
- IBM Corp. IBM SPSS Statistics for Windows; Version 22.0 2013; IBM: Armonk, NY, USA, 2013. [Google Scholar]
- Jacobson, N.S.; Truax, P. Clinical significance: A statistical approach to defining meaningful change in psychotherapy research. J. Consult. Clin. Psychol. 1991, 59, 12–19. [Google Scholar] [CrossRef]
- De Andrés Pizarro, J. El análisis de estudios cualitativo. Aten. Primaria 2000, 25, 42–46. [Google Scholar] [CrossRef][Green Version]
- Shamseer, L.; Sampson, M.; Bukutu, C.; Schmid, C.H.; Nikles, J.; Tate, R.; Johnston, B.C.; Zucker, D.; Shadish, W.R.; Kravitz, R.; et al. Consort extension for reporting N-of-1 trials (CENT) 2015: Explanation and elaboration. J. Clin. Epidemiol. 2016, 76, 18–46. [Google Scholar] [CrossRef]
- Welbourn, R.; Dixon, J.; Barth, J.H.; Finer, N.; Hughes, C.A.; le Roux, C.W.; Wass, J. NICE-Accredited Commissioning Guidance for Weight Assessment and Management Clinics: A Model for a Specialist Multidisciplinary Team Approach for People with Severe Obesity. Obes. Surg. 2016, 26, 649–659. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Mental Health Action Plan 2013–2020; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Renjilian, D.A.; Perri, M.G.; Nezu, A.M.; McKelvey, W.F.; Shermer, R.L.; Anton, S.D. Individual versus group therapy for obesity: Effects of matching participants to their treatment preferences. J. Consult. Clin. Psychol. 2001, 69, 717–721. [Google Scholar] [CrossRef] [PubMed]
- Osma, J.; Suso-Ribera, C.; Peris-Baquero, O.; Gil-Lacruz, M.; Pérez-Ayerra, L.; Ferreres-Galan, V.; Torres-Alfosea, M.A.; López-Escriche, M.; Domínguez, O. What format of treatment do patients with emotional disorders prefer and why? Implications for public mental health settings and policies. PLoS ONE 2019, 14, e0218117. [Google Scholar] [CrossRef] [PubMed]
- Osma, J.; Sánchez-Gómez, A.; Peris-Baquero, O. Applying the unified protocol to a single case of major depression with schizoid and depressive personality traits. Psicothema 2018, 30, 364–369. [Google Scholar] [CrossRef]


{kind=link}
| Inclusion Criteria |
|
|
|
|
|
|
|
|
| Contraindications |
| Relative |
|
|
|
|
|
|
|
| Absolute |
|
|
|
|
| Session Number | Content |
|---|---|
| Session 1 | Setting Goals and Maintaining Motivation |
| Session 2 | Understanding your Emotions: What is an Emotion? |
| Session 3 | Understanding your Emotions: Following the ARC (Antecedent, Response, Consequence) |
| Session 4 | Mindful Emotion Awareness—I |
| Session 5 | Mindful Emotion Awareness—II |
| Session 6 | Cognitive Flexibility—I |
| Session 7 | Cognitive Flexibility—II |
| Session 8 | Countering Emotional Behaviors |
| Session 9 | Understanding and Confronting Physical Sensations |
| Session 10 | Putting it into Practice: Emotion Exposures—I |
| Session 11 | Putting it into Practice: Emotion Exposures—II |
| Session 12 | Recognizing Accomplishments and Looking to the Future |
| Measures | Pre-Treatment | Baseline | Treatment | Post-Treatment | Follow-Ups 1 |
|---|---|---|---|---|---|
| Demographic characteristics | X | ||||
| MINI | X | X | X | ||
| BDI-II | X | X | X | ||
| BAI | X | X | X | ||
| BMI | X | X | X | X | X |
| PANAS | X | X | X | ||
| NEO-FFI | X | X | X | ||
| QLI | X | X | X | ||
| EuroQol | X | X | X | ||
| MI | X | X | X | ||
| DERS | X | X | X | ||
| BEAQ | X | X | X | ||
| PHLMS | X | X | X | ||
| ERQ | X | X | X | ||
| Surgical Complications | X | ||||
| BITE | X | X | X | ||
| BSQ | X | X | X | ||
| EES | X | X | X | ||
| OASIS | X | ||||
| ODSIS | X | ||||
| OESIS | X | ||||
| PESIS | X | ||||
| STQ | X | X | |||
| Baseline assessment battery 2 | X | ||||
| Assessment battery during treatment 3 | X |
| Clinical Usefulness of the UP for Bariatric Surgery Candidates |
| Group Results: |
|
| Individual Results: |
|
|
| In both cases, the expected directions for the different variables are: |
|
|
| Feasibility of the UP for Bariatric Surgery Candidates |
|
|
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quilez-Orden, A.; Ferreres-Galán, V.; Osma, J. Feasibility and Clinical Usefulness of the Unified Protocol in Online Group Format for Bariatric Surgery Candidates: Study Protocol for a Multiple Baseline Experimental Design. Int. J. Environ. Res. Public Health 2020, 17, 6155. https://doi.org/10.3390/ijerph17176155
Quilez-Orden A, Ferreres-Galán V, Osma J. Feasibility and Clinical Usefulness of the Unified Protocol in Online Group Format for Bariatric Surgery Candidates: Study Protocol for a Multiple Baseline Experimental Design. International Journal of Environmental Research and Public Health. 2020; 17(17):6155. https://doi.org/10.3390/ijerph17176155
Chicago/Turabian StyleQuilez-Orden, Alba, Vanesa Ferreres-Galán, and Jorge Osma. 2020. "Feasibility and Clinical Usefulness of the Unified Protocol in Online Group Format for Bariatric Surgery Candidates: Study Protocol for a Multiple Baseline Experimental Design" International Journal of Environmental Research and Public Health 17, no. 17: 6155. https://doi.org/10.3390/ijerph17176155
APA StyleQuilez-Orden, A., Ferreres-Galán, V., & Osma, J. (2020). Feasibility and Clinical Usefulness of the Unified Protocol in Online Group Format for Bariatric Surgery Candidates: Study Protocol for a Multiple Baseline Experimental Design. International Journal of Environmental Research and Public Health, 17(17), 6155. https://doi.org/10.3390/ijerph17176155