Hospitalized Patients Accessing Information on Prescribed Medications from the Bedside Terminal: A Cross-Sectional Study

 and
and
Abstract
1. Introduction
2. Materials and Methods
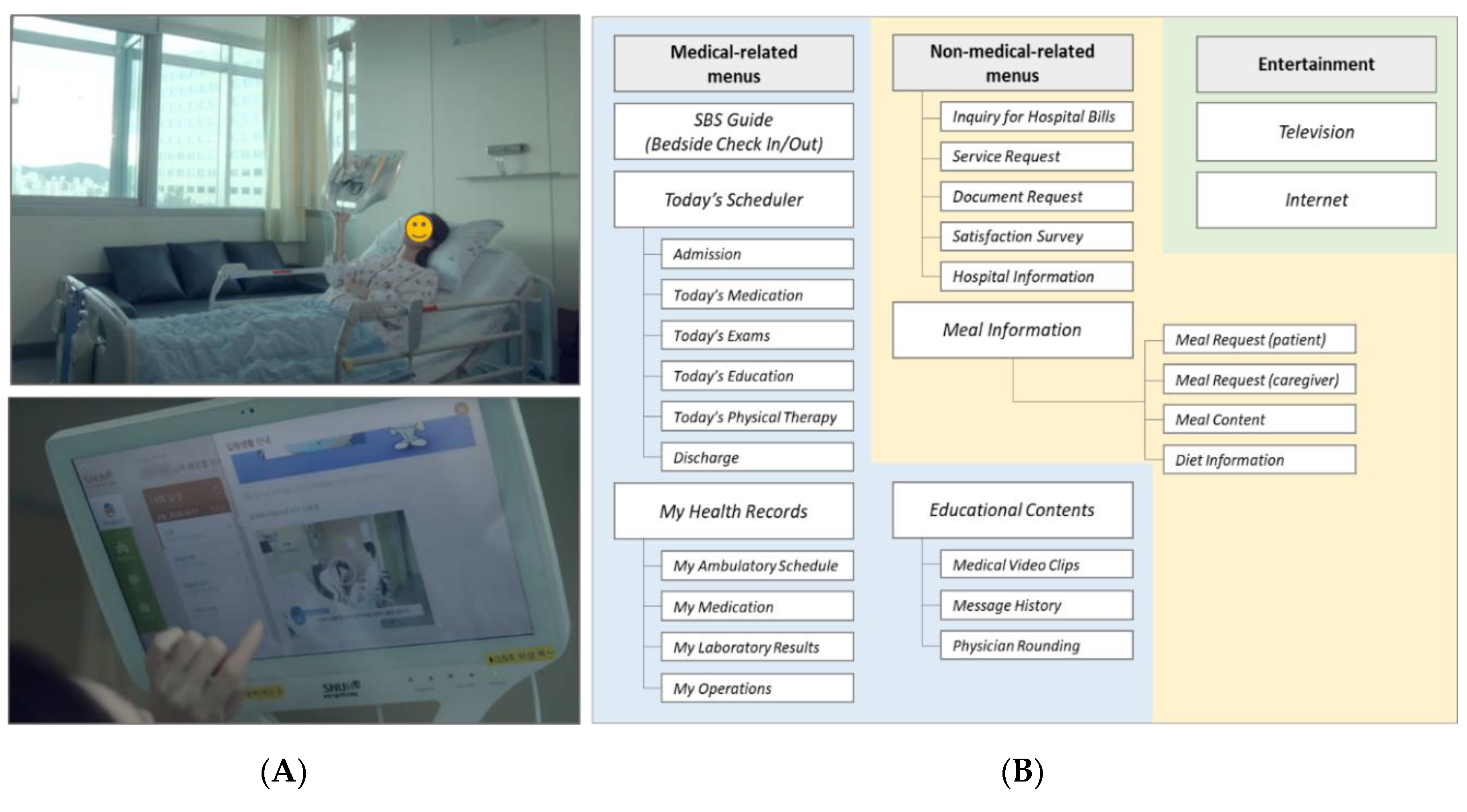
2.1. Study Site and the Smart Bedside Station (SBS)
2.2. Study Process
2.2.1. Analysis of the SBS Access Data
2.2.2. Root Cause Analysis
2.3. Data Analysis
2.4. Ethical Board Approval
3. Results
3.1. SBS Usage Patterns
3.2. Associated Factors for Accessing Today’s Medication
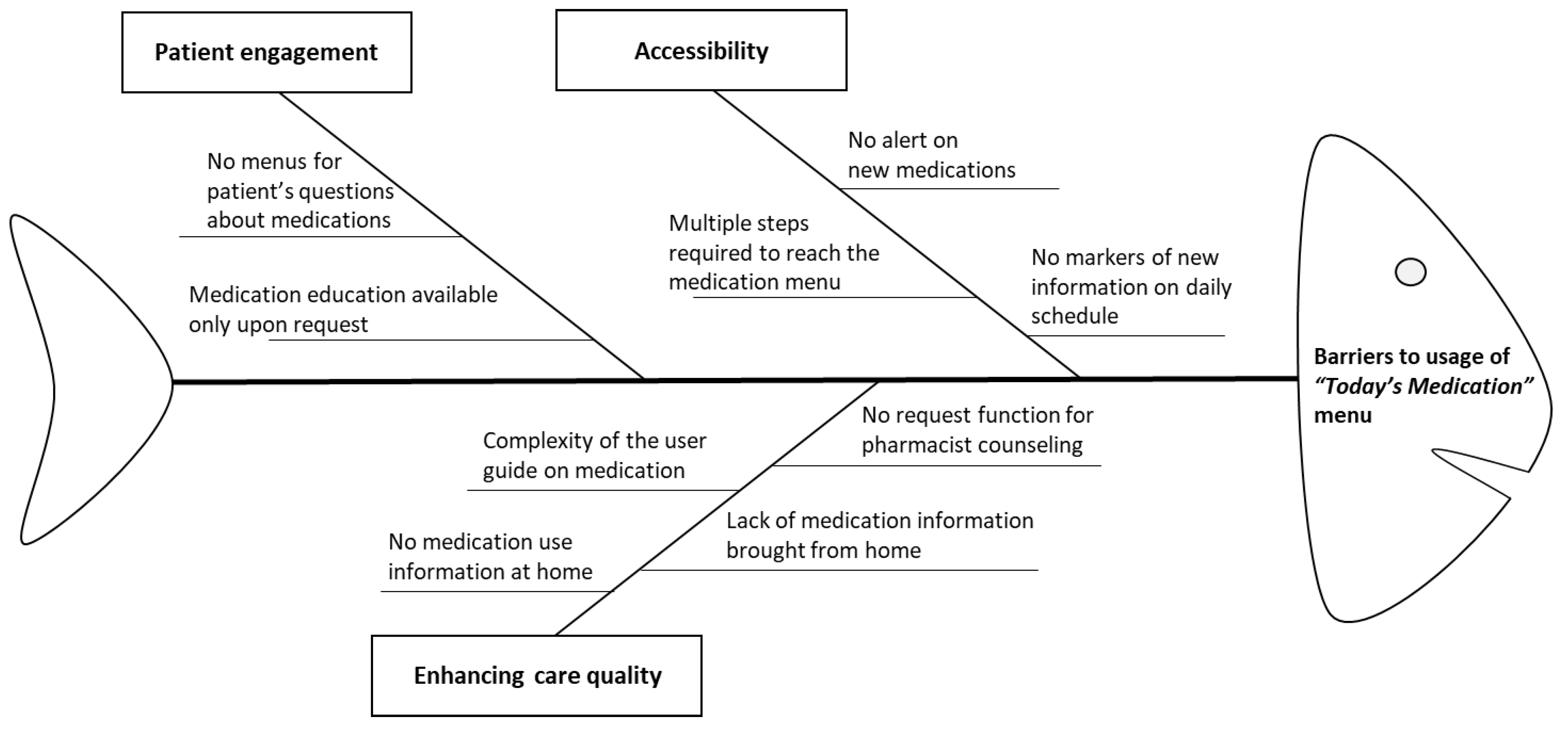
3.3. Root Cause Analysis Using a Fishbone Diagram
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Health Information Technology: Improving the Nation′s Health Care. Available online: https://www.healthit.gov/video/health-information-technology-improving-nations-health-care (accessed on 2 November 2019).
- Sheth, A.; Jaimini, U.; Thirunarayan, K.; Banerjee, T. Augmented personalized health: How smart data with IoTs and AI is about to change healthcare. In Proceedings of the 2017 IEEE 3rd International Forum on Research and Technologies for Society and Industry (RTSI), Modena, Italy, 11–13 September 2017. [Google Scholar] [CrossRef]
- Banerjee, T.; Sheth, A. IoT Quality Control for Data and Application Needs. IEEE Intell. Syst. 2017, 32, 68–73. [Google Scholar] [CrossRef]
- SCH: kHealth: Semantic Multisensory Mobile Approach to Personalized Asthma Care. Available online: https://grantome.com/grant/NIH/R01-HD087132-02#panel-abstract-body (accessed on 3 July 2020).
- Strickland, E. IBM Watson, heal thyself: How IBM overpromised and underdelivered on AI health care. IEEE Spectr. 2019, 56, 24–31. [Google Scholar] [CrossRef]
- Tang, C.; Lorenzi, N.; Harle, C.A.; Zhou, X.; Chen, Y. Interactive systems for patient-centered care to enhance patient engagement. J. Am. Med. Inform. Assoc. 2016, 23, 2–4. [Google Scholar] [CrossRef] [PubMed]
- Wager, K.A.; Lee, F.W.; Glaser, J.P. Health Care Information Systems: A Practical Approach for Health Care Management, 2nd ed.; Jossey-Bass: San Francisco, CA, USA, 2017. [Google Scholar]
- Caligtan, C.A.; Carroll, D.L.; Hurley, A.C.; Gersh-Zaremski, R.; Dykes, P.C. Bedside information technology to support patient-centered care. Int. J. Med. Inform. 2012, 81, 442–451. [Google Scholar] [CrossRef] [PubMed]
- Dalal, A.K.; Dykes, P.C.; Collins, S.; Lehmann, L.S.; Ohashi, K.; Rozenblum, R.; Stade, D.; McNally, K.; Morrison, C.R.; Ravindran, S.; et al. A web-based, patient-centered toolkit to engage patients and caregivers in the acute care setting: A preliminary evaluation. J. Am. Med. Inform. Assoc. 2015, 23, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century; National Academies Press: Washington, DC, USA, 2001. [Google Scholar] [CrossRef]
- The Eight Principles of Patient-Centered Care. Available online: https://www.oneviewhealthcare.com/the-eight-principles-of-patient-centered-care (accessed on 3 December 2019).
- Kruse, C.S.; Bolton, K.; Freriks, G. The effect of patient portals on quality outcomes and its implications to meaningful use: A systematic review. J. Med. Internet Res. 2015, 17, e44. [Google Scholar] [CrossRef] [PubMed]
- What Is a Patient Portal? Available online: https://www.healthit.gov/faq/what-patient-portal (accessed on 20 December 2019).
- Kelly, M.M.; Coller, R.J.; Hoonakker, P.L. Inpatient portals for hospitalized patients and caregivers: A systematic review. J. Hosp. Med. 2018, 13, 405–412. [Google Scholar] [CrossRef]
- Robinson, J.R.; Davis, S.E.; Cronin, R.M.; Jackson, G.P. Use of a patient portal during hospital admissions to surgical services. AMIA Annu. Symp. Proc. 2016, 2016, 1967–1976. [Google Scholar]
- McAlearney, A.S.; Sieck, C.J.; Hefner, J.L.; Aldrich, A.M.; Walker, D.M.; Rizer, M.K.; Moffatt-Bruce, S.D.; Huerta, T.R. High Touch and High Tech (HT2) proposal: Transforming patient engagement throughout the continuum of care by engaging patients with portal technology at the bedside. JMIR Res. Protoc. 2016, 5, e221. [Google Scholar] [CrossRef]
- Bansilal, S.; Castellano, J.M.; Garrido, E.; Wei, H.G.; Freeman, A.; Spettell, C.; Garcia-Alonso, F.; Lizano, I.; Arnold, R.J.G.; Rajda, J.; et al. Assessing the impact of medication adherence on long-term cardiovascular outcomes. J. Am. Coll. Cardiol. 2016, 68, 789–801. [Google Scholar] [CrossRef]
- Harnett, J.; Wiederkehr, D.; Gerber, R.; Gruben, D.; Bourret, J.; Koenig, A. Primary nonadherence, associated clinical outcomes, and health care resource use among patients with rheumatoid arthritis prescribed treatment with injectable biologic disease-modifying antirheumatic drugs. J. Manag. Care Spec. Pharm. 2016, 22, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Kangovi, S.; Mitra, N.; Grande, D.; White, M.L.; McCollum, S.; Sellman, J.; Shannon, R.P.; Long, J.A. Patient-centered community health worker intervention to improve posthospital outcomes: A randomized clinical trial. JAMA Intern. Med. 2014, 174, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Martínez Nicolás, I.; Lê Cook, B.; Flores, M.; Del Olmo Rodriguez, M.; Hernández Rodríguez, C.; Llamas Sillero, P.; Baca-Garcia, E. The impact of a comprehensive electronic patient portal on the health service use: An interrupted time-series analysis. Eur. J. Public Health 2018, 29, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Yoo, S.; Lee, K.-H.; Baek, H.; Ryu, B.; Chung, E.; Kim, K.; Yi, J.C.; Park, S.B.; Hwang, H. Development and user research of a smart bedside station system toward patient-centered healthcare system. J. Med. Syst. 2015, 39, 86. [Google Scholar] [CrossRef] [PubMed]
- Ryu, B.; Kim, S.; Lee, K.-H.; Hwang, H.; Yoo, S. Inpatient satisfaction and usage patterns of personalized smart bedside station system for patient-centered service at a tertiary university hospital. Int. J. Med. Inform. 2016, 95, 35–42. [Google Scholar] [CrossRef]
- Cho, M.; Park, Y. Utilization of and satisfaction with smart bedside station system as a patient-centered healthcare system. J. Muscle Jt Health 2017, 24, 89–100. [Google Scholar] [CrossRef]
- Sooyoung Yoo, H.H.; Jheon, S. Hospital information systems: Experience at the fully digitized Seoul National University Bundang Hospital. J. Thorac. Dis. 2016, 8 (Suppl. 8), S637. [Google Scholar]
- Berkman, N.D.; Davis, T.C.; McCormack, L. Health literacy: What is it? J. Health Commun. 2010, 15 (Suppl. 2), 9–19. [Google Scholar] [CrossRef]
- Frisch, A.-L.; Camerini, L.; Diviani, N.; Schulz, P.J. Defining and measuring health literacy: How can we profit from other literacy domains? Health Promot. Int. 2012, 27, 117–126. [Google Scholar] [CrossRef]
- Liu, Y.-B.; Liu, L.; Li, Y.-F.; Chen, Y.-L. Relationship between health literacy, health-related behaviors and health status: A survey of elderly Chinese. Int. J. Environ. Res. Public Health 2015, 12, 9714–9725. [Google Scholar] [CrossRef] [PubMed]
- Howard, D.H.; Gazmararian, J.; Parker, R.M. The impact of low health literacy on the medical costs of Medicare managed care enrollees. Am. J. Med. 2005, 118, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Xie, B. Effects of an eHealth literacy intervention for older adults. J. Med. Internet Res. 2011, 13, e90. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Guidelines on Hand Hygiene in Health Care: First Global Patient Safety Challenge Clean Care Is Safer Care; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Grossman, L.V.; Masterson Creber, R.M.; Benda, N.C.; Wright, D.; Vawdrey, D.K.; Ancker, J.S. Interventions to increase patient portal use in vulnerable populations: A systematic review. J. Am. Med. Inform. Assoc. 2019, 26, 855–870. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Mean (SD) | N (%) |
|---|---|---|
| Age, mean ± SD | 55.78 ± 21.35 | |
| Under 20 | 2966 (8.03) | |
| 20–39 | 4810 (13.02) | |
| 40–64 | 14,444 (39.11) | |
| Over 65 | 14,711 (39.83) | |
| Gender (men) | 18,492 (50.07) | |
| Length of stay, mean ± SD | 11.76 ± 17.82 | |
| Department of hospitalization | ||
| Surgery | 13,075 (35.40) | |
| Internal medicine | 12,991 (35.18) | |
| Obstetrics and gynecology | 2889 (7.82) | |
| Urology | 1933 (5.23) | |
| Pediatric | 1656 (4.48) | |
| Others | 4387 (11.88) | |
| Education level * | ||
| Less than elementary school | 5184 (16.07) | |
| Middle to high school education | 13,571 (42.07) | |
| College education or above | 13,503 (41.86) | |
| Job type * | ||
| No job | 9254 (28.69) | |
| Professionals | 2451 (7.60) | |
| Business owners | 3509 (10.88) | |
| Company workers | 4890 (15.16) | |
| Housewives | 8126 (25.19) | |
| Students | 1411 (4.37) | |
| Military service | 200 (0.62) | |
| Others a | 2416 (7.49) |
| Characteristics | Total SBS Use (n = 34,189) | N (%) | |
|---|---|---|---|
| Accessed a (n = 13,732) | Did Not Access (n = 20,457) | ||
| Age, mean ± SD | 50.79 ± 21.04 | 59.65 ± 20.43 | |
| Under 20 | 2668 | 1290 (48.35) | 1378 (51.65) |
| 20–39 | 4268 | 2547 (59.68) | 1721 (40.32) |
| 40–64 | 13,491 | 6007 (44.53) | 7484 (55.47) |
| Over 65 | 13,762 | 3888 (28.25) | 9874 (71.75) |
| Gender (men) | 17,230 | 6784 (49.40) | 10,446 (51.06) |
| Department of hospitalization | |||
| Surgery | 12,410 | 4999 (40.28) | 7411 (59.72) |
| Internal medicine | 12,146 | 4276 (35.21) | 7870 (64.79) |
| Obstetrics and gynecology | 2672 | 1427 (53.41) | 1245 (46.59) |
| Urology | 1884 | 831 (44.11) | 1053 (55.89) |
| Pediatric | 1512 | 735 (48.61) | 777 (51.39) |
| Others | 3565 | 1464 (41.07) | 2101 (58.93) |
| Education level * | |||
| Less than elementary school | 4827 | 1445 (29.94) | 3382 (70.06) |
| Middle to high school education | 12,651 | 4600 (36.36) | 8051 (63.64) |
| College education or above | 12,383 | 6004 (48.49) | 6379 (51.51) |
| Job type * | |||
| No job | 8614 | 2670 (31.00) | 5944 (69.00) |
| Professionals | 2275 | 1137 (49.98) | 1138 (50.02) |
| Business owners | 3292 | 1322 (40.16) | 1970 (59.84) |
| Company workers | 4576 | 2460 (53.76) | 2116 (46.24) |
| Housewives | 7497 | 2822 (37.64) | 4675 (62.36) |
| Students | 1230 | 662 (53.82) | 568 (46.18) |
| Military service | 166 | 98 (59.04) | 68 (40.96) |
| Others b | 2210 | 875 (39.59) | 1335 (60.41) |
| Characteristics | Adjusted OR | 95% CI |
|---|---|---|
| Gender | ||
| Women | 1.00 (reference) | |
| Men | 0.983 | 0.925–1.044 |
| Age | ||
| Over 65 | 1.00 (reference) | |
| Under 20 | 1.856 * | 1.478–2.331 |
| 20–39 | 2.631 * | 2.409–2.874 |
| 40–64 | 1.714 * | 1.612–1.823 |
| Education level | ||
| Less than elementary school | 1.00 (reference) | |
| Above graduate education | 1.543 * | 1.419–1.677 |
| Middle to high school education | 1.153 * | 1.067–1.247 |
| Job type | ||
| No job | 1.00 (reference) | |
| Professionals | 1.247 * | 1.125–1.382 |
| Business owners | 1.088 | 0.995–1.190 |
| Company workers | 1.418 * | 1.303–1.544 |
| Housewives | 1.055 | 0.974–1.143 |
| Students | 1.617 * | 1.324–1.974 |
| Military service | 1.724 * | 1.249–2.379 |
| Others a | 1.103 | 0.996–1.221 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, J.; Kim, S.; Shin, S.; Yoo, H.; Park, G.H.; Jeon, E.; Lee, E.; Lee, H.-Y.; Lee, E. Hospitalized Patients Accessing Information on Prescribed Medications from the Bedside Terminal: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 4850. https://doi.org/10.3390/ijerph17134850
Cho J, Kim S, Shin S, Yoo H, Park GH, Jeon E, Lee E, Lee H-Y, Lee E. Hospitalized Patients Accessing Information on Prescribed Medications from the Bedside Terminal: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2020; 17(13):4850. https://doi.org/10.3390/ijerph17134850
Chicago/Turabian StyleCho, Jungwon, Seungyeon Kim, Sangyoon Shin, Hyejin Yoo, Gi Hyue Park, Eunha Jeon, Eunsook Lee, Ho-Young Lee, and Euni Lee. 2020. "Hospitalized Patients Accessing Information on Prescribed Medications from the Bedside Terminal: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 17, no. 13: 4850. https://doi.org/10.3390/ijerph17134850
APA StyleCho, J., Kim, S., Shin, S., Yoo, H., Park, G. H., Jeon, E., Lee, E., Lee, H.-Y., & Lee, E. (2020). Hospitalized Patients Accessing Information on Prescribed Medications from the Bedside Terminal: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 17(13), 4850. https://doi.org/10.3390/ijerph17134850