An Empirical Study on Patients’ Acceptance of Physician-Patient Interaction in Online Health Communities


Abstract
1. Introduction
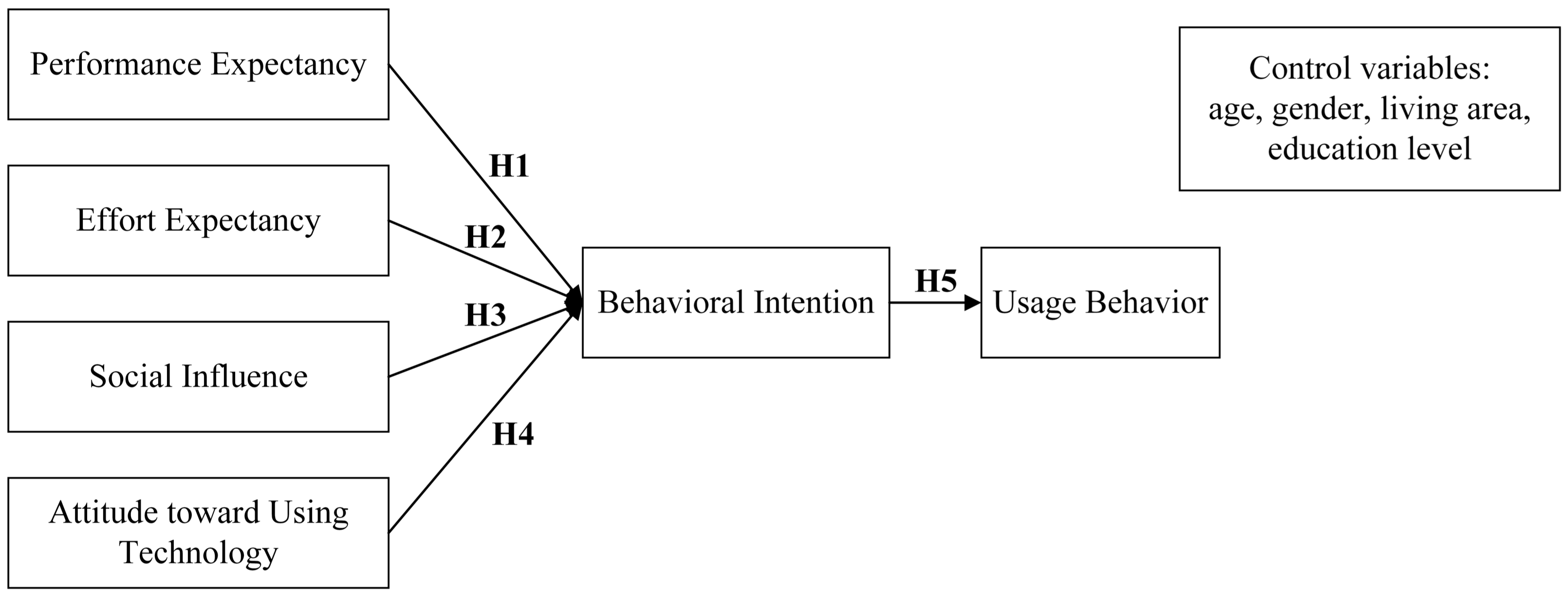
2. Research Model and Hypotheses
2.1. Online Health Communities
2.2. Unified Theory of Acceptance and Use of Technology
2.3. Physician—Patient Interaction
2.4. Research Hypotheses
3. Materials and Methods
3.1. Instrument Development
3.2. Data Collection and Respondent Profile
4. Results
4.1. Data Analysis
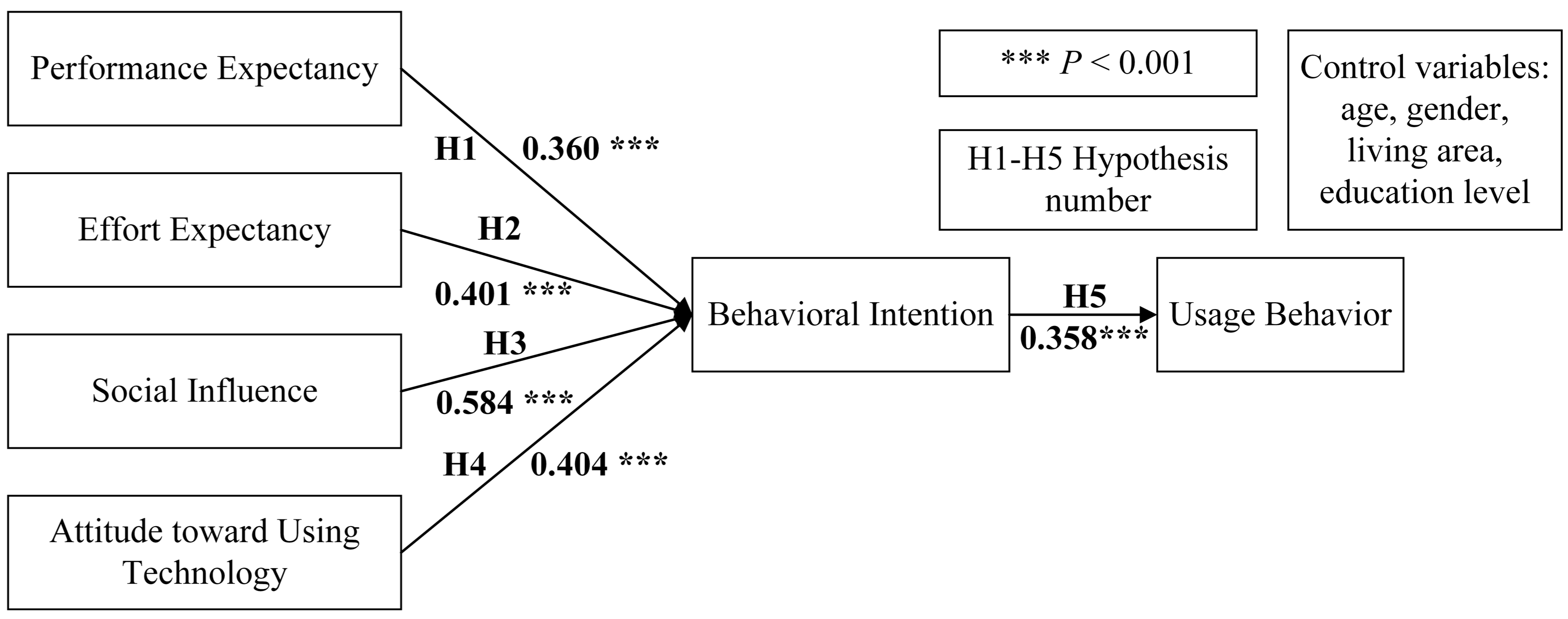
4.2. Hypothesis Testing
5. Discussion
5.1. Principal Results
5.2. Limitations and Potentials
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Yan, Z.; Wang, T.; Chen, Y.; Zhang, H. Knowledge sharing in online health communities: A social exchange theory perspective. Inf. Manag. 2016, 53, 643–653. [Google Scholar] [CrossRef]
- Bronstein, J. An examination of social and informational support behavior codes on the Internet: The case of online health communities. Libr. Inf. Sci. Res. 2017, 1, 63–68. [Google Scholar] [CrossRef]
- Yang, H.; Guo, X.; Wu, T. Exploring the influence of the online physician service delivery process on patient satisfaction. Decis. Support. Syst. 2015, 78, 113–121. [Google Scholar] [CrossRef]
- Zhao, J.; Ha, S.; Widdows, R. Building trusting relationships in online health communities. Cyberpsychol. Behav. Soc. N 2013, 16, 650–657. [Google Scholar] [CrossRef]
- Berger, M.; Wagner, T.H.; Baker, L.C. Internet use and stigmatized illness. Soc. Sci. Med. 2005, 61, 1821–1827. [Google Scholar] [CrossRef]
- Yan, L.; Tan, Y. Feeling blue? Go online: An empirical study of social support among patients. Inf. Syst. Res. 2014, 25, 690–709. [Google Scholar] [CrossRef]
- Wu, H.; Lu, N. Online written consultation, telephone consultation and offline appointment: An examination of the channel effect in online health communities. Int. J. Med. Inf. 2017, 107, 107–119. [Google Scholar] [CrossRef]
- Venkatesh, V.; Morris, M.G.; Davis, G.B.; Davis, F.D. User acceptance of information technology: Toward a unified view. MIS Q. 2003, 27, 425–478. [Google Scholar] [CrossRef]
- Chang, I.C.; Hsu, H.M. Predicting medical staff intention to use an online reporting system with modified unified theory of acceptance and use of technology. Telemed. J. E-Health 2012, 18, 67–73. [Google Scholar] [CrossRef]
- Hennemann, S.; Witthöft, M.; Bethge, M.; Spanier, K.; Beutel, M.E.; Zwerenz, R. Acceptance and barriers to access of occupational e-mental health: Cross-sectional findings from a health-risk population of employees. Int. Arch. Occup. Environ. Health 2018, 91, 305–316. [Google Scholar] [CrossRef]
- Veer, A.J.; Peeters, J.M.; Brabers, A.E.; Schellevis, F.G.; Rademakers, J.J.; Francke, A.L. Determinants of the intention to use e-health by community dwelling older people. BMC. Health Serv. Res. 2015, 15, 103. [Google Scholar]
- Kaba, B.; Touré, B. Understanding information and communication technology behavioral intention to use: Applying the UTAUT model to social networking site adoption by young people in a least developed country. J. Assoc. Inf. Sci. Tech. 2014, 65, 1662–1674. [Google Scholar] [CrossRef]
- Jiang, S.; Street, R.L. Pathway linking Internet health information seeking to better health: A moderated mediation study. Health Commun. 2017, 32, 1024–1031. [Google Scholar] [CrossRef]
- Lamberg, L. Online empathy for mood disorders. JAMA 2003, 289, 3073–3077. [Google Scholar]
- Wu, B. Patient continued use of online health care communities: Web mining of patient-doctor communication. J. Med. Internet Res. 2018, 20, e126. [Google Scholar] [CrossRef]
- Murray, E.; Lo, B.; Pollack, L.; Donelan, K.; Catania, J.; White, M.; Zapert, K.; Turner, R. The impact of health information on the internet on the physician-patient relationship: Patient perceptions. Arch. Intern. Med. 2003, 163, 1727–1734. [Google Scholar] [CrossRef]
- Sillence, E. Giving and receiving peer advice in an online breast cancer support group. Cyberpsychol. Beheav. Soc. Netw. 2013, 16, 480–485. [Google Scholar] [CrossRef]
- Cacciatore, M.A.; Anderson, A.A.; Choi, D.H.; Brossard, D.; Scheufele, D.A.; Liang, X.; Ladwig, P.J.; Xenos, M.; Dudo, A. Coverage of emerging technologies: A comparison between print and online media. New Media Soc. 2012, 14, 1039–1059. [Google Scholar] [CrossRef]
- Mäntymäki, M.; Salo, J. Purchasing behavior in social virtual worlds: An examination of Habbo Hotel. Int. J. Inf. Manag. 2013, 33, 282–290. [Google Scholar] [CrossRef]
- Dermentzi, E.; Papagiannidis, S. UK public’s intention to engage with academia via online technologies. Behav. Inf. Technol. 2018, 37, 120–132. [Google Scholar] [CrossRef]
- Sun, J.; Lu, J. An empirical study on user acceptance of healthcare website. Int. J. Netw. Virtual Organ. 2014, 14, 57–73. [Google Scholar] [CrossRef]
- Laugesen, J.; Hassanein, K.; Yuan, Y. The impact of internet health information on patient compliance: A research model and an empirical study. J. Med. Internet Res. 2015, 17, e143. [Google Scholar] [CrossRef] [PubMed]
- Heritage, J.; Maynard, D.W. Problems and prospects in the study of physician-patient interaction: 30 years of research. Annu. Rev. Sociol. 2006, 32, 351–374. [Google Scholar] [CrossRef]
- Roter, D.L. Patient participation in the patient-provider interaction: The effects of patient question asking on the quality of interaction, satisfaction and compliance. Health Educ. Monogr. 1977, 5, 281–315. [Google Scholar] [CrossRef] [PubMed]
- Ong, L.M.; De Haes, J.C.; Hoos, A.M.; Lammes, F.B. Doctor-patient communication: A review of the literature. Soc. Sci. Med. 1995, 40, 903–918. [Google Scholar] [CrossRef]
- Rottmann, N.; Helmes, A.W.; Vogel, B.A. Patients’ needs and experiences at breast cancer diagnosis: How perceived threat influences the physician-patient interaction. J. Psychosoc. Oncol. 2010, 28, 157–172. [Google Scholar] [CrossRef]
- Bu, X.Q.; You, L.M.; Li, Y.; Liu, K.; Zheng, J.; Yan, T.B.; Chen, S.X.; Zhang, L.F. Psychometric properties of the kessler 10 scale in Chinese parents of children with cancer. Cancer Nurs. 2017, 40, 297–304. [Google Scholar] [CrossRef]
- Xiao, Y.Y.; Li, T.; Xiao, L.; Wang, S.W.; Wang, S.Q.; Wang, H.X.; Wang, B.B.; Gao, Y.L. The Chinese version of instrument of professional attitude for student nurses (ISAPN): Assessment of reliability and validity. Nurse Educ. Today 2016, 49, 79–83. [Google Scholar] [CrossRef]
- Huh, J.; Kwon, B.C.; Kim, S.H.; Lee, S.; Choo, J.; Kim, J.; Choi, M.J.; Yi, J.S. Personas in online health communities. J. Biomed. Inf. 2016, 63, 212–225. [Google Scholar] [CrossRef]
- Spaderna, H.; Sieverding, M. Who makes use of internet-delivered health information? The role of gender role self-concept in young men and women. Psychol. Health Med. 2015, 20, 247–253. [Google Scholar] [CrossRef]
- Buysse, H.E.; Coorevits, P.; Van Maele, G.; Hutse, A.; Kaufman, J.; Ruige, J.; De Moor, G.J. Introducing telemonitoring for diabetic patients: Development of a telemonitoring ‘Health Effect and Readiness’ questionnaire. Int. J. Med. Inf. 2010, 79, 576–584. [Google Scholar] [CrossRef] [PubMed]
- Biasutti, M.; Frate, S. A validity and reliability study of the attitudes toward sustainable development scale. Environ. Educ. Res. 2017, 23, 214–230. [Google Scholar] [CrossRef]
- Erdogan, M.; Ok, A.; Marcinkowski, T.J. Development and validation of children’s responsible environmental behavior scale. Environ. Educ. Res. 2012, 18, 507–540. [Google Scholar] [CrossRef]
- Kaiser, H.F. A second generation little jiffy. Psychometrika 1970, 35, 401–415. [Google Scholar] [CrossRef]
- Kurtuldu, M.K.; Bulut, D. Development of a self-efficacy scale toward piano lessons. Educ. Sci. Theory Pract. 2017, 17, 835–857. [Google Scholar] [CrossRef]
- Wu, W.; Tang, F.; Dong, X.; Liu, C. Different identifications cause different types of voice: A role identity approach to the relations between organizational socialization and voice. Asia Pac. J. Manag. 2015, 32, 251–287. [Google Scholar] [CrossRef]
- Sardeshmukh, S.R.; Vandenberg, R.J. Integrating moderation and mediation: A structural equation modeling approach. Organ. Res. Methods 2017, 20, 721–745. [Google Scholar] [CrossRef]
- Lee, Y.J.; Hosanagar, K.; Tan, Y. Do I follow my friends or the crowd? Information cascades in online movie ratings. Manag. Sci. 2015, 61, 2241–2258. [Google Scholar] [CrossRef]
- Li, D.; Luo, Z.; Ding, Y.; Sun, G.Z.; Sun, G.Z.; Dai, X.; Du, J.; Zhang, J.; Kong, S. User-level microblogging recommendation incorporating social influence. J. Assoc. Inf. Sci. Tech. 2017, 68, 553–568. [Google Scholar] [CrossRef]
- Luo, P.; Chen, K.; Wu, C. Measuring social influence for firm-level financial performance. Electron. Commer. Res. Appl. 2016, 20, 15–29. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Constructs | Items |
|---|---|
| Performance expectancy (PE) [8,21] | 1. I would find the physician–patient interaction in an online health community useful for my health. 2. Conducting an interaction with physicians in an online health community can improve my life quality. 3. Conducting an interaction with physicians in an online health community increases my ability for self-care. 4. Conducting an interaction with physicians in an online health community makes me become healthier. |
| Effort expectancy (EE) [8,21] | 1. Physician–patient interaction in an online health community would be clear and understandable. 2. It would be easy for me to become skillful at physician–patient interaction in an online health community. 3. I would find the physician–patient interaction in an online health community easy to maintain. 4. Learning to conduct the physician–patient interaction in an online health community is easy for me. |
| Social influence (SI) [8,21] | 1. People who influence my behavior think that I should conduct an interaction with physicians in ab online health community. 2. People who are important to me think that I should conduct an interaction with physicians in an online health community. 3. I will feel uneasy if my friends conduct an interaction with physicians in an online health community but I do not. |
| Attitude toward using technology (AUT) [8,21] | 1. Physician–patient interaction in an online health community is a bad/good thing. 2. Physician–patient interaction in an online health community makes healthcare more easily to understand. 3. Physician–patient interaction in an online health community is useful. 4. I like to conduct interactions with physicians in an online health community. |
| Usage behavior (UB) [8,21] | 1. Recently, I plan to conduct an interaction with physicians in ab online health community. 2. I’m willing to conduct an interaction with physicians in ab online health community if available. 3. I think I will be willing to conduct an interaction with physicians in an online health community if I have known some. 4. I will conduct an interaction with physicians in an online health community in the future. |
| Characteristic | Number | Percentage | |
|---|---|---|---|
| (1) Age | <20 | 18 | 4.76% |
| 21–29 | 119 | 31.48% | |
| 30–39 | 109 | 28.84% | |
| 40–49 | 81 | 21.43% | |
| 50–59 | 45 | 11.90% | |
| 60 and above | 6 | 1.59% | |
| (2) Gender | Male | 172 | 45.50% |
| Female | 206 | 54.50% | |
| (3) Living area | Urban | 247 | 65.34% |
| Rural | 131 | 34.66% | |
| (4) Education level | Junior middle school and below | 9 | 2.38% |
| High school | 50 | 13.23% | |
| Junior college | 98 | 25.93% | |
| Bachelor’s degree | 183 | 48.41% | |
| Master’s degree | 33 | 8.73% | |
| Doctor’s degree | 5 | 1.32% | |
| Model Factors | Fit Indices 1 | ||||||
|---|---|---|---|---|---|---|---|
| χ2 | df | χ2/df | RMSEA | CFI | IFI | TLI | |
| Model 1 (six factors) | 378.828 | 215 | 1.762 | 0.045 | 0.958 | 0.959 | 0.951 |
| Model 2 (five factors) | 397.607 | 220 | 1.807 | 0.046 | 0.955 | 0.955 | 0.948 |
| Model 3 (four factors) | 445.161 | 224 | 1.987 | 0.051 | 0.944 | 0.944 | 0.936 |
| Model 4 (three factors) | 448.448 | 227 | 1.976 | 0.051 | 0.944 | 0.944 | 0.937 |
| Model 5 (two factors) | 488.376 | 229 | 2.133 | 0.055 | 0.934 | 0.934 | 0.927 |
| Model 6 (one factor) | 489.045 | 230 | 2.126 | 0.055 | 0.934 | 0.934 | 0.927 |
| Effects 1 | Path coefficients (SD) | P |
|---|---|---|
| PE → BI | 0.351 (0.128) | 0.003 |
| EE → BI | 0.392 (0.092) | 0.000 |
| SI → BI | 0.570 (0.115) | 0.000 |
| AUT → BI | 0.400 (0.112) | 0.001 |
| BI → UB | 0.165 (0.045) | 0.000 |
| PE → UB | 0.058 (0.024) | 0.002 |
| EE → UB | 0.065 (0.021) | 0.000 |
| SI → UB | 0.094 (0.033) | 0.000 |
| AUT → UB | 0.066 (0.025) | 0.000 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, X.; Zhang, R.; Zhu, X. An Empirical Study on Patients’ Acceptance of Physician-Patient Interaction in Online Health Communities. Int. J. Environ. Res. Public Health 2019, 16, 5084. https://doi.org/10.3390/ijerph16245084
Lu X, Zhang R, Zhu X. An Empirical Study on Patients’ Acceptance of Physician-Patient Interaction in Online Health Communities. International Journal of Environmental Research and Public Health. 2019; 16(24):5084. https://doi.org/10.3390/ijerph16245084
Chicago/Turabian StyleLu, Xinyi, Runtong Zhang, and Xiaomin Zhu. 2019. "An Empirical Study on Patients’ Acceptance of Physician-Patient Interaction in Online Health Communities" International Journal of Environmental Research and Public Health 16, no. 24: 5084. https://doi.org/10.3390/ijerph16245084
APA StyleLu, X., Zhang, R., & Zhu, X. (2019). An Empirical Study on Patients’ Acceptance of Physician-Patient Interaction in Online Health Communities. International Journal of Environmental Research and Public Health, 16(24), 5084. https://doi.org/10.3390/ijerph16245084