
The Impact of a Telehealth Intervention on Activity Profiles in Older Adults during the COVID-19 Pandemic: A Pilot Study


 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Intervention
2.3. Measures
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kvaavik, E.; Batty, G.D.; Ursin, G.; Huxley, R.; Gale, C.R. Influence of individual and combined health behaviors on total and cause-specific mortality in men and women: The United Kingdom health and lifestyle survey. Arch. Intern. Med. 2010, 170, 711–718. [Google Scholar] [CrossRef] [Green Version]
- Daskalopoulou, C.; Koukounari, A.; Ayuso-Mateos, J.L.; Prince, M.; Prina, A.M. Associations of Lifestyle Behaviour and Healthy Ageing in Five Latin American and the Caribbean Countries-A 10/66 Population-Based Cohort Study. Nutrients 2018, 10, 1593. [Google Scholar] [CrossRef] [Green Version]
- Harvey, J.A.; Chastin, S.F.; Skelton, D.A. Prevalence of sedentary behavior in older adults: A systematic review. Int. J. Environ. Res. Public Health 2013, 10, 6645–6661. [Google Scholar] [CrossRef]
- Bailey, L.; Ward, M.; DiCosimo, A.; Baunta, S.; Cunningham, C.; Romero-Ortuno, R.; Briggs, R. Physical and Mental Health of Older People while Cocooning during the COVID-19 Pandemic. QJM Int. J. Med. 2021, hcab015. [Google Scholar] [CrossRef]
- Browne, R.A.; Macêdo, G.A.; Cabral, L.L.; Oliveira, G.T.; Vivas, A.; Fontes, E.B.; Costa, E.C. Initial impact of the COVID-19 pandemic on physical activity and sedentary behavior in hypertensive older adults: An accelerometer-based analysis. Exp. Gerontol. 2020, 142, 111121. [Google Scholar] [CrossRef]
- Harrison, E.; Monroe-Lord, L.; Carson, A.D.; Jean-Baptiste, A.M.; Phoenix, J.; Jackson, P.; Richardson, M.L. COVID-19 pandemic-related changes in wellness behavior among older Americans. BMC Public Health 2021, 21, 755. [Google Scholar] [CrossRef] [PubMed]
- Cimperman, M.; Brenčič, M.M.; Trkman, P.; Stanonik, M.D.L. Older adults’ perceptions of home telehealth services. Telemed. Health 2013, 19, 786–790. [Google Scholar] [CrossRef]
- Jones, R.B.; Ashurst, E.J.; Atkey, J.; Duffy, B. Older people going online: Its value and before-after evaluation of volunteer support. J. Med. Internet Res. 2015, 17, e122. [Google Scholar] [CrossRef]
- Hunsaker, A.; Hargittai, E. A review of Internet use among older adults. New Media Soc. 2018, 20, 3937–3954. [Google Scholar] [CrossRef]
- Marcus, B.H.; Lewis, B.A.; Williams, D.M.; Dunsiger, S.; Jakicic, J.M.; Whiteley, J.A.; Parisi, A.F. A comparison of Internet and print-based physical activity interventions. Arch. Intern. Med. 2007, 167, 944–949. [Google Scholar] [CrossRef] [Green Version]
- Mohadis, H.M.; Ali, N.M.; Shahar, S.; Smeaton, A.F. Web-based physical activity interventions for older adults: A review. In Advances in Visual Informatics; Badioze Zaman, H., Ed.; IVIC 2015. Lecture Notes in Computer; Science, Springer: Cham, Switzerland, 2015; Volume 9429. [Google Scholar]
- Jonkman, N.H.; van Schooten, K.S.; Maier, A.B.; Pijnappels, M. eHealth interventions to promote objectively measured physical activity in community-dwelling older people. Maturitas 2018, 113, 32–39. [Google Scholar] [CrossRef]
- Doraiswamy, S.; Jithesh, A.; Mamtani, R.; Abraham, A.; Cheema, S. Telehealth Use in Geriatrics Care during the COVID-19 Pandemic-A Scoping Review and Evidence Synthesis. Int. J. Environ. Res. Public Health 2021, 18, 1755. [Google Scholar] [CrossRef]
- Defining Adult Overweight & Obesity. Available online: https://www.cdc.gov/obesity/adult/defining.html (accessed on 27 May 2021).
- The Physical Activity Readiness Questionnaire for Everyone. Available online: http://eparmedx.com/wp-content/uploads/2013/03/FINAL-FILLABLE-ParQ-Plus-Jan-20191.pdf (accessed on 27 May 2021).
- Iftakhar, S. Google Classroom: What Works and How? J. Educ. Soc. Sci. 2016, 3, 12–18. [Google Scholar]
- Riffin, C.; Kenien, C.; Ghesquiere, A.; Dorime, A.; Villanueva, C.; Gardner, D.; Reid, M.C. Community-based participatory research: Understanding a promising approach to addressing knowledge gaps in palliative care. Ann. Palliat. Med. 2016, 5, 218–224. [Google Scholar] [CrossRef] [Green Version]
- Wallerstein, N.B.; Duran, B. Using community-based participatory research to address health disparities. Health Promot. Pract. 2006, 7, 312–323. [Google Scholar] [CrossRef]
- Salimi, Y.; Shahandeh, K.; Malekafzali, H.; Loori, N.; Kheiltash, A.; Jamshidi, E.; Majdzadeh, R. Is Community-based Participatory Research (CBPR) Useful? A Systematic Review on Papers in a Decade. Int. J. Prev. Med. 2012, 3, 386–393. [Google Scholar]
- Exercise for Older Adults. Available online: http://file.lacounty.gov/SDSInter/dmh/216745_ExerciseforOlderAdultsHealthCareProviderManual.pdf (accessed on 27 May 2021).
- AgePage Healthy Eating After 50. Available online: https://order.nia.nih.gov/sites/default/files/2019-10/Healthy-Eating-2019-update-508.pdf (accessed on 27 May 2021).
- Exercise & Physical Activity. Available online: https://healthysd.gov/wp-content/uploads/2015/04/go4life-exercise-guide.pdf (accessed on 27 May 2021).
- Bernstein, M.; Munoz, N. Academy of Nutrition and Dietetics. Position of the Academy of Nutrition and Dietetics: Food and nutrition for older adults: Promoting health and wellness. J. Acad. Nutr. Diet. 2012, 112, 1255–1277. [Google Scholar] [CrossRef]
- Swann, C.; Rosenbaum, S.; Lawrence, A.; Vella, S.A.; McEwan, D.; Ekkekakis, P. Updating goal-setting theory in physical activity promotion: A critical conceptual review. Health Psychol. Rev. 2021, 15, 34–50. [Google Scholar] [CrossRef] [Green Version]
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R.; Tudor-Locke, C.; Leon, A.S. Compendium of Physical Activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [Green Version]
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; Leon, A.S. Compendium of physical activities: An update of activity codes and MET intensities. Med. Sci. Sports Exerc. 2000, 32, S498–S504. [Google Scholar] [CrossRef] [Green Version]
- Gomersall, S.R.; Olds, T.S.; Ridley, K. Development and evaluation of an adult use-of-time instrument with an energy expenditure focus. J. Sci. Med. Sport 2011, 14, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Foley, L.S.; Maddison, R.; Rush, E.; Olds, T.S.; Ridley, K.; Jiang, Y. Doubly labeled water validation of a computerized use-of-time recall in active young people. Metabolism 2013, 62, 163–169. [Google Scholar] [CrossRef]
- Gomersall, S.; Maher, C.; Norton, K.; Dollman, J.; Tomkinson, G.; Esterman, A.; Olds, T. Testing the activitystat hypothesis: A randomised controlled trial protocol. BMC Public Health 2012, 12, 851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brønd, J.C.; Arvidsson, D. Sampling frequency affects the processing of Actigraph raw acceleration data to activity counts. J. Appl. Physiol. 2016, 120, 362–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wennman, H.; Pietilä, A.; Rissanen, H.; Valkeinen, H.; Partonen, T.; Mäki-Opas, T.; Borodulin, K. Gender, age and socioeconomic variation in 24-hour physical activity by wrist-worn accelerometers: The FinHealth 2017 Survey. Sci. Rep. 2019, 9, 6534. [Google Scholar] [CrossRef] [Green Version]
- McGrath, R.; Vella, C.A.; Scruggs, P.W.; Peterson, M.D.; Williams, C.J.; Paul, D.R. The Impact of Low Accelerometer Wear Time on the Estimates and Application of Sedentary Behavior and Physical Activity Data in Adults. J. Phys. Act. Health 2017, 14, 919–924. [Google Scholar] [CrossRef]
- Tudor-Locke, C.; Camhi, S.M.; Troiano, R.P. A catalog of rules, variables, and definitions applied to accelerometer data in the National Health and Nutrition Examination Survey, 2003–2006. Prev. Chronic Dis. 2012, 9, E113. [Google Scholar] [CrossRef] [Green Version]
- Choi, L.; Liu, Z.; Matthews, C.E.; Buchowski, M.S. Validation of accelerometer wear and nonwear time classification algorithm. Med. Sci. Sports Exerc. 2011, 43, 357–364. [Google Scholar] [CrossRef] [Green Version]
- Montoye, A.H.; Clevenger, K.A.; Pfeiffer, K.A.; Nelson, M.B.; Bock, J.M.; Imboden, M.T.; Kaminsky, L.A. Development of cut-points for determining activity intensity from a wrist-worn ActiGraph accelerometer in free-living adults. J. Sports Sci. 2020, 38, 2569–2578. [Google Scholar] [CrossRef]
- Stockwell, S.; Trott, M.; Tully, M.; Shin, J.; Barnett, Y.; Butler, L.; Smith, L. Changes in physical activity and sedentary behaviours from before to during the COVID-19 pandemic lockdown: A systematic review. BMJ Open Sport Exerc. Med. 2021, 7, e000960. [Google Scholar] [CrossRef]
- Douthit, N.; KiBiswas, Sv.S.; Dwolatzky, T. Exposing some important barriers to health care access in the rural USA. Public Health 2015, 129, 611–620. [Google Scholar] [CrossRef]
- Andersson, G. Internet interventions: Past, present and future. Internet Interv. 2018, 12, 181–188. [Google Scholar] [CrossRef]
- Lam, K.; Lu, A.D.; Shi, Y.; Covinsky, K.E. Assessing Telemedicine Unreadiness Among Older Adults in the United States During the COVID-19 Pandemic. JAMA Intern. Med. 2020, 180, 1389–1391. [Google Scholar] [CrossRef] [PubMed]
- Colby, S.L.; Ortman, J.M. Projections of the Size and Composition of the US Population: 2014 to 2060. Available online: https://www.census.gov/content/dam/Census/library/publications/2015/demo/p25-1143.pdf (accessed on 27 May 2021).
- Julious, S.A. Sample size of 12 per group rule of thumb for a pilot study. Pharm. Stat. 2005, 4, 287–291. [Google Scholar] [CrossRef]

{kind=link}
| Super-Domain | Sub-Domain | Description | Examples |
|---|---|---|---|
| Sleep | - | Sleeping, napping | Day time nap |
| Physical Activity | - | Formal and informal exercise | Gym, sports |
| Work and Study | - | Occupational activity, study | Office work |
| - | Computer | Non-gaming computer use | Internet, email |
| Transport | - | Locomotion | Driving a car |
| - | Active transport | Non-motorized transport | Cycling, walking |
| - | Passive transport | Motorized transport | Riding a bus |
| Quiet Time | - | Non-social leisure time | Listen to music |
| - | Reading | Recreational reading | Reading an article |
| - | Other | Non-reading quiet time | Lying in bed |
| Self-Care | - | Eating, grooming | Eating dinner |
| - | Eating | Eating or drinking | Drinking coffee |
| - | Grooming | Grooming or ablutions | Showering |
| Social | - | Social and cultural activities | Talking |
| - | Communications | Communicating with others | Calls, text message |
| - | Socializing | Social interactions | Parties |
| Chores | - | Domestic tasks | Food prep |
| - | Indoor chores | Inside tasks | Vacuuming |
| - | Outdoor chores | Outdoor tasks | Gardening |
| Screen Time | - | Phone apps, television | Phone apps |
| - | Television or videogames | Watching television, movies | Watching movies |
| Variable | Value |
|---|---|
| Age (Years) | 70.6 ± 4.5 |
| Female (n (%)) | 10 (76.9) |
| Non-Hispanic White (n (%)) | 13 (100.0) |
| Completed Bachelor’s Degree or Higher (n (%)) | 9 (69.2) |
| Retired (n (%)) | 12 (92.3) |
| Current Smoker (n (%)) | 0 (0.0) |
| Excellent or Very Good Self-Rated Health (n (%)) | 10 (76.9) |
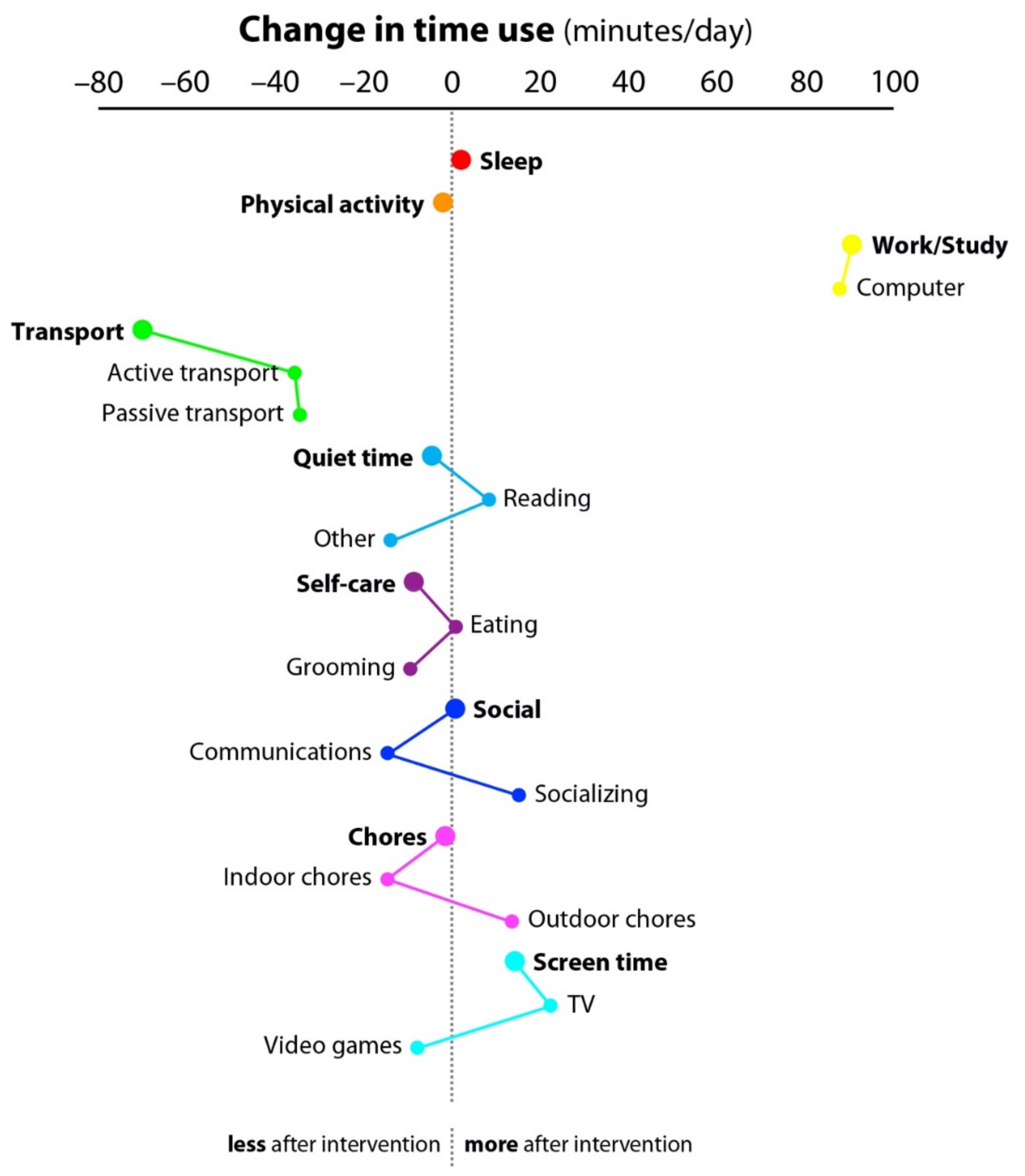
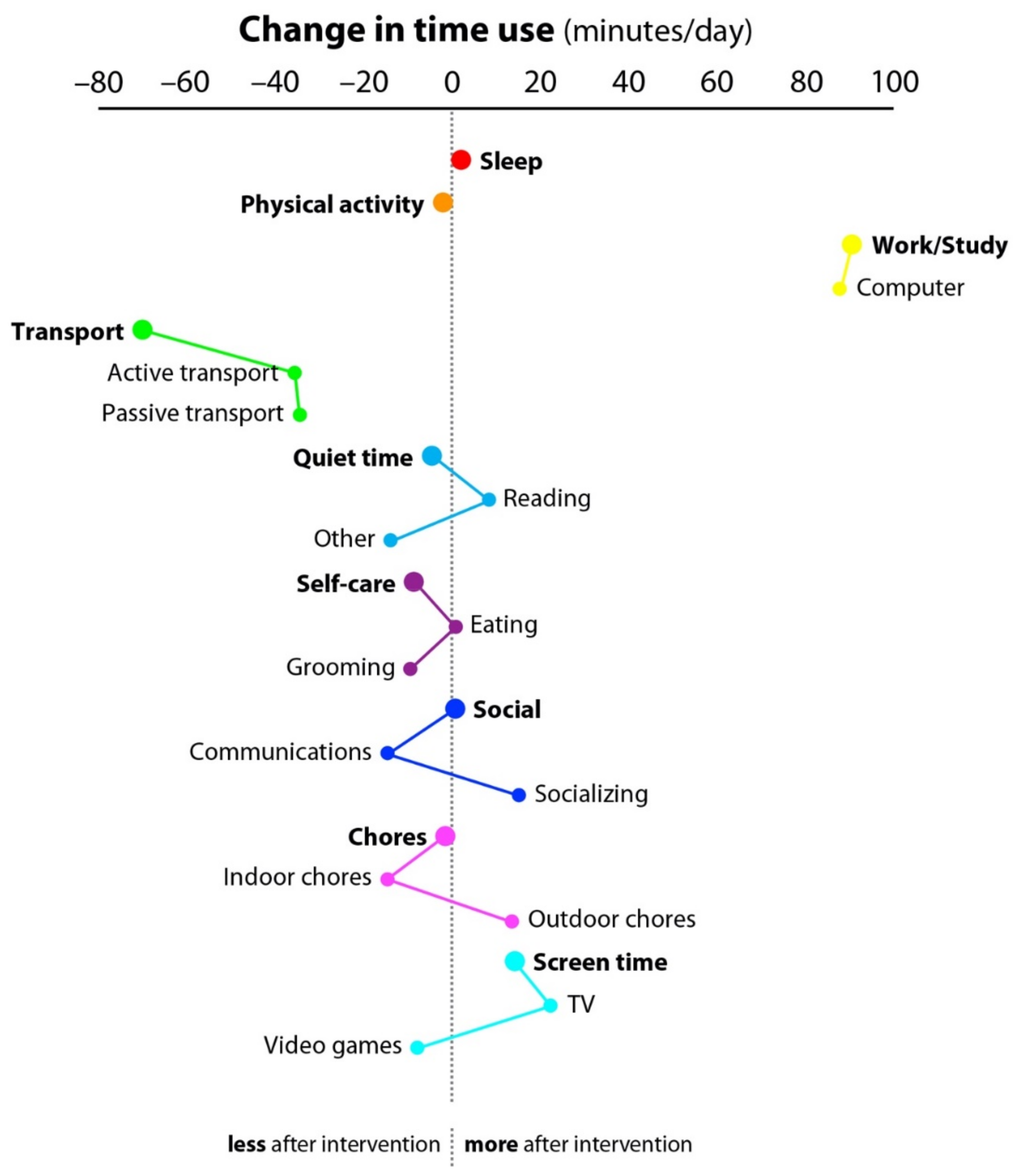
| Super-Domain | Sub-Domain | Baseline † | Post-Intervention † | Mean Change Minutes (95% CI) |
|---|---|---|---|---|
| Sleep | - | 487 ± 38 | 489 ± 37 | 2 (−32, 36) |
| Physical Activity | - | 22 ± 16 | 20 ± 29 | −2 (−21, 17) |
| Work and Study | - | 31 ± 29 | 122 ± 68 | 91 (45, 136) |
| - | Computer | 26 ± 30 | 114 ± 72 | 88 (39, 137) |
| Transport | - | 147 ± 151 | 77 ± 44 | −70 (−167, 27) |
| - | Active transport | 74 ± 39 | 38 ± 29 | −36 (−62, −10) |
| - | Passive transport | 73 ± 124 | 39 ± 32 | −34 (−111, 43) |
| Quiet Time | - | 133 ± 84 | 128 ± 72 | −4 (−68, 59) |
| - | Reading | 99 ± 95 | 108 ± 70 | 9 (−61, 78) |
| - | Other | 33 ± 39 | 20 ± 20 | −13 (−37, 11) |
| Self-Care | - | 135 ± 32 | 127 ± 18 | −9 (−32, 15) |
| - | Eating | 78 ± 23 | 79 ± 11 | 1 (−69, 70) |
| - | Grooming | 57 ± 16 | 48 ± 11 | −9 (−22, 3) |
| Social | - | 100 ± 80 | 101 ± 62 | 1 (−69, 70) |
| - | Communications | 95 ± 74 | 80 ± 50 | −15 (−82, 53) |
| - | Socializing | 5 ± 11 | 21 ± 37 | 15 (−9, 40) |
| Chores | - | 28 ± 100 | 207 ± 112 | −1 (−101, 99) |
| - | Indoor chores | 206 ± 99 | 191 ± 114 | −15 (−114, 85) |
| - | Outdoor chores | 2 ± 6 | 1 ± 29 | 13 (−5, 32) |
| Screen Time | - | 135 ± 84 | 149 ± 106 | 14 (−75, 104) |
| - | Television | 127 ± 83 | 149 ± 108 | 22 (−67, 111) |
| Videogames | 8 ± 17 | 0 ± 0 | −8 (−18, 2) |
| Variable | Baseline † | Post-Intervention † | Mean Change Time (95% CI) |
|---|---|---|---|
| Daily Minutes | |||
| SB | 688 ± 80 | 650 ± 82 | −37 (−103, 27) |
| LPA | 207 ± 57 | 201 ± 51 | −6 (−50, 37) |
| MVPA | 53 ± 27 | 55 ± 31 | 2 (−21, 26) |
| Weekly Minutes | |||
| SB | 4822 ± 560 | 4512 ± 643 | −309 (−797, 179) |
| LPA | 1454 ± 404 | 1406 ± 358 | −47 (−357, 261) |
| MVPA | 374 ± 195 | 387 ± 218 | 12 (−154, 180) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Johnson, N.; Bradley, A.; Klawitter, L.; Johnson, J.; Johnson, L.; Tomkinson, G.R.; Hackney, K.J.; Stastny, S.; Ehlers, D.K.; McGrath, R. The Impact of a Telehealth Intervention on Activity Profiles in Older Adults during the COVID-19 Pandemic: A Pilot Study. Geriatrics 2021, 6, 68. https://doi.org/10.3390/geriatrics6030068
Johnson N, Bradley A, Klawitter L, Johnson J, Johnson L, Tomkinson GR, Hackney KJ, Stastny S, Ehlers DK, McGrath R. The Impact of a Telehealth Intervention on Activity Profiles in Older Adults during the COVID-19 Pandemic: A Pilot Study. Geriatrics. 2021; 6(3):68. https://doi.org/10.3390/geriatrics6030068
Chicago/Turabian StyleJohnson, Nathaniel, Adam Bradley, Lukus Klawitter, Jane Johnson, Lance Johnson, Grant R. Tomkinson, Kyle J. Hackney, Sherri Stastny, Diane K. Ehlers, and Ryan McGrath. 2021. "The Impact of a Telehealth Intervention on Activity Profiles in Older Adults during the COVID-19 Pandemic: A Pilot Study" Geriatrics 6, no. 3: 68. https://doi.org/10.3390/geriatrics6030068
APA StyleJohnson, N., Bradley, A., Klawitter, L., Johnson, J., Johnson, L., Tomkinson, G. R., Hackney, K. J., Stastny, S., Ehlers, D. K., & McGrath, R. (2021). The Impact of a Telehealth Intervention on Activity Profiles in Older Adults during the COVID-19 Pandemic: A Pilot Study. Geriatrics, 6(3), 68. https://doi.org/10.3390/geriatrics6030068