
Conventional PCR Versus Next Generation Sequencing for Diagnosis of FLT3, IDH and NPM1 Mutations in Acute Myeloid Leukemia: Results of the PETHEMA PCR-LMA Study

 , , , , , , , , , , , , , , , ,
, , , , , , , , , , , , , , , ,  ,
,  , , ,
on behalf of the PETHEMA Groupadd
Show full author list
, , ,
on behalf of the PETHEMA Groupadd
Show full author list
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Platform and Reference Laboratorios
2.2. Patients
2.3. Molecular Studies
2.3.1. Single Gene Testing Methods
2.3.2. NGS Methodology
2.4. Study End-Points and Statistical Analyses
3. Results
3.1. Patient Baseline Characteristics
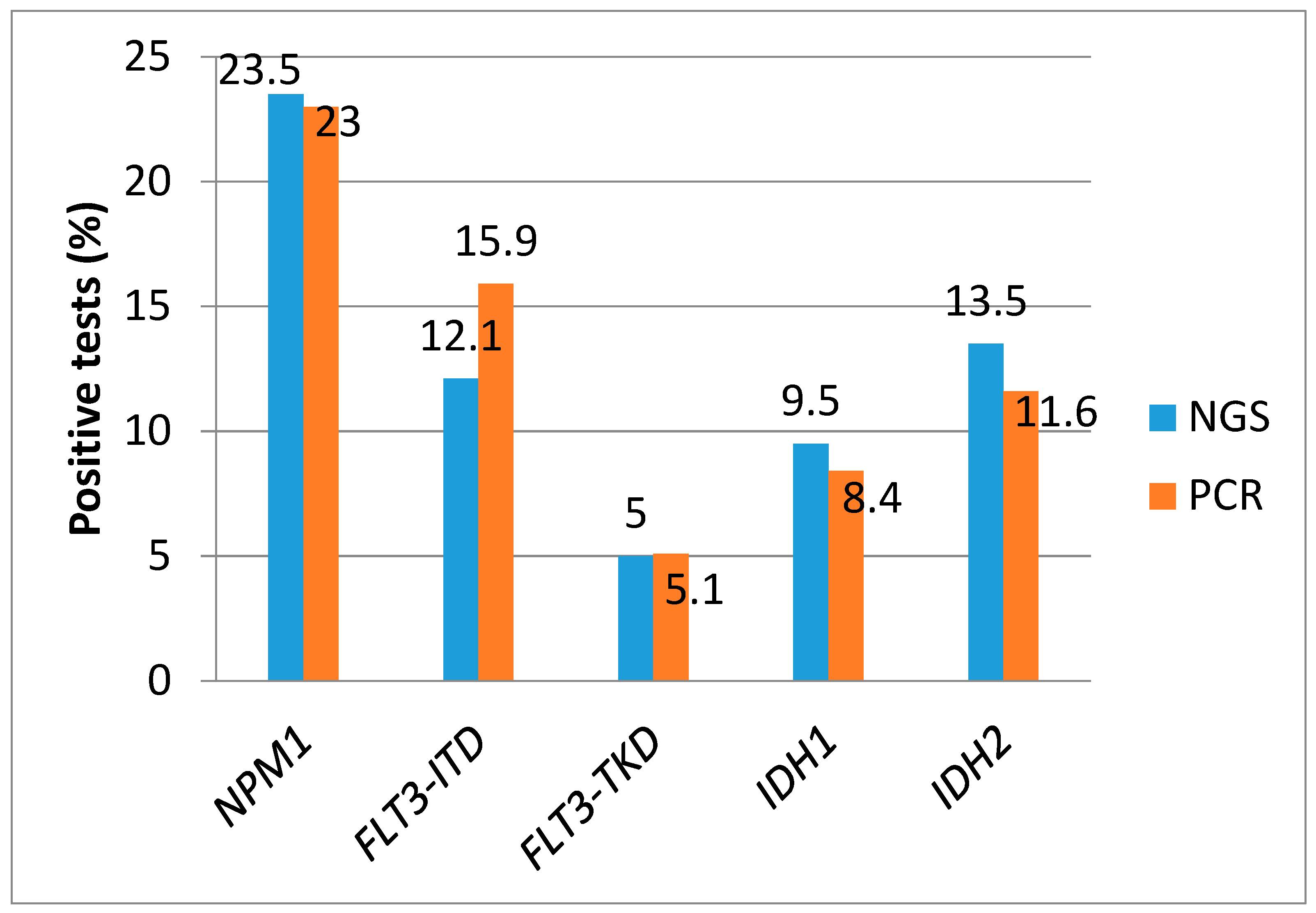
3.2. Frequency of NPM1, FLT3-ITD, FLT3-TKD, IDH1, and IDH2 Mutations by PCR
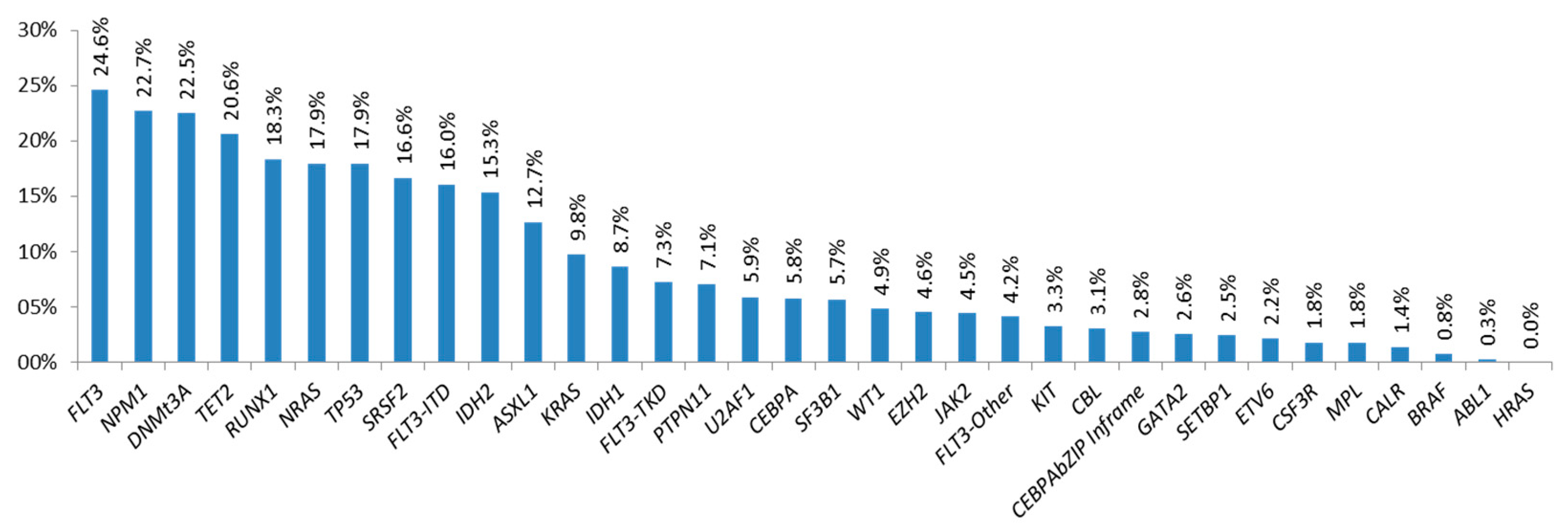
3.3. Frequency of Mutations Detected by NGS
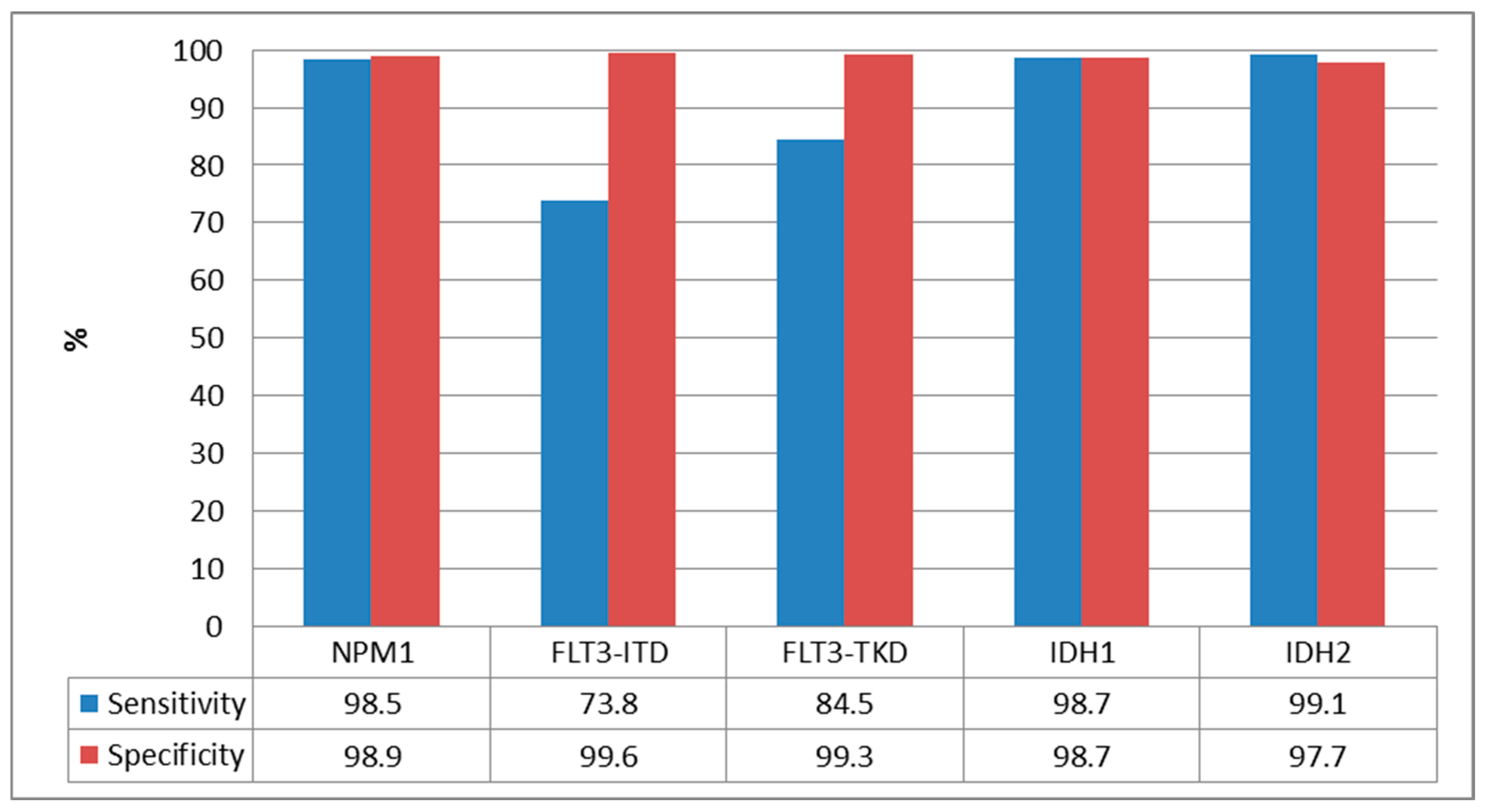
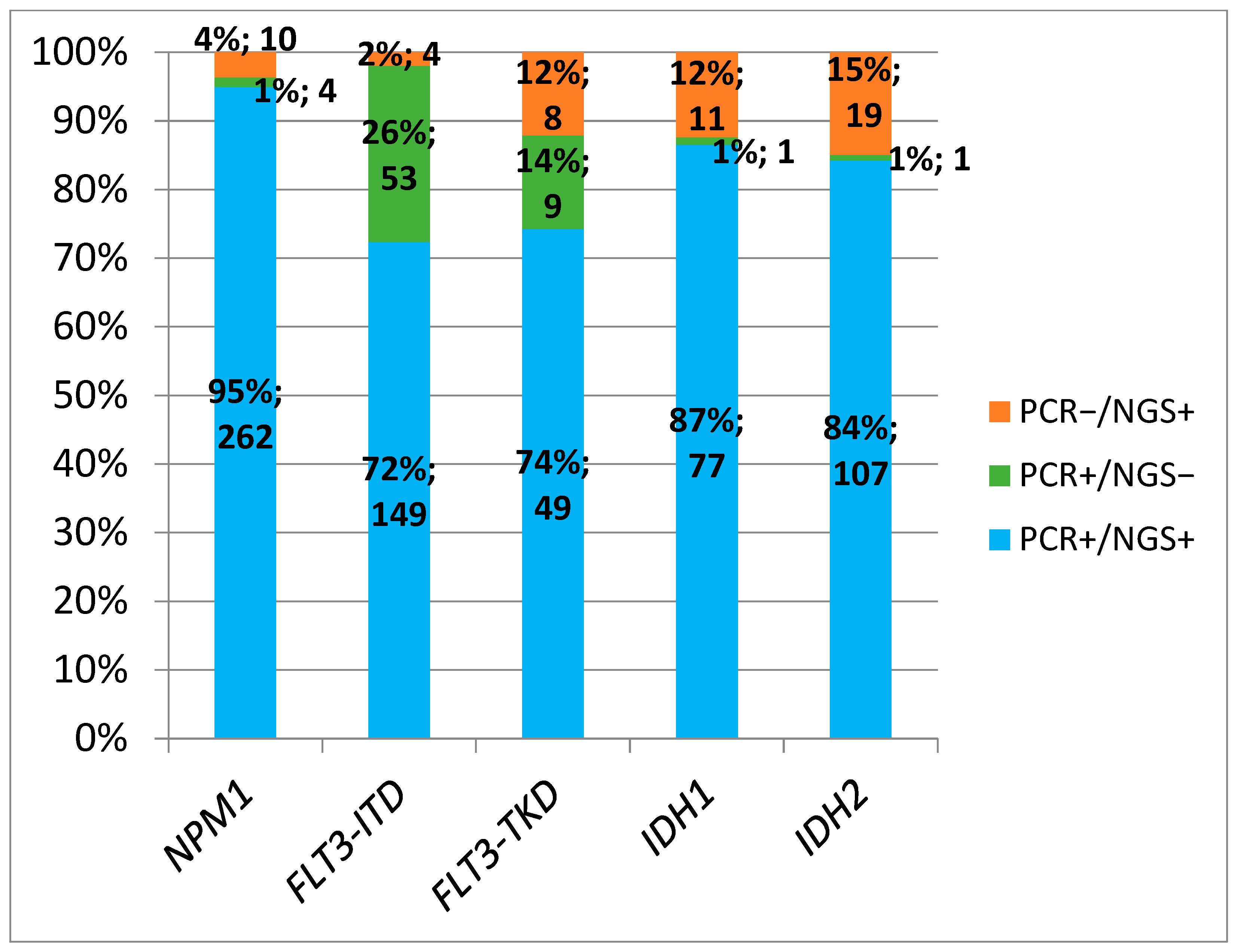
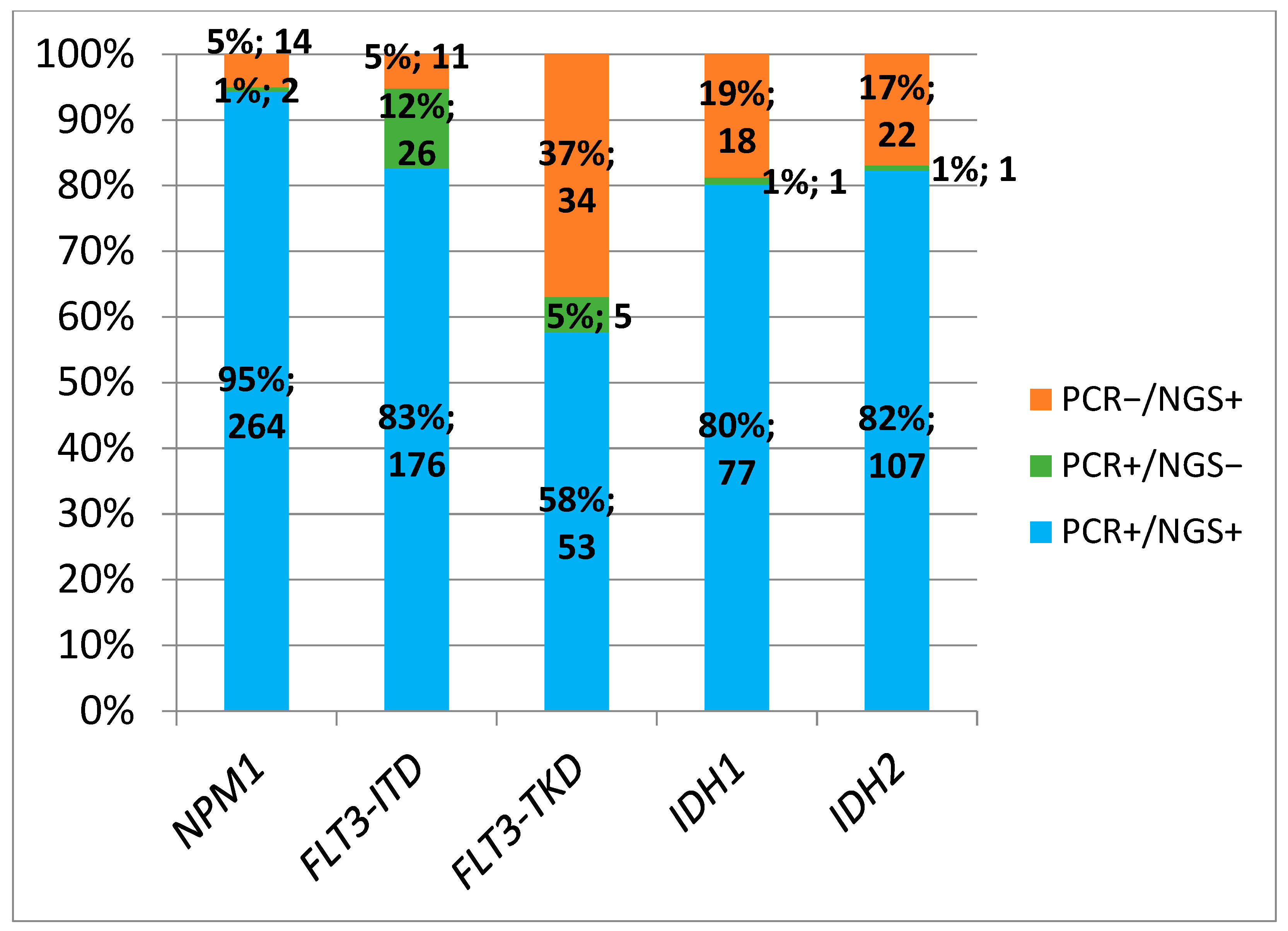
3.4. Comparison Between PCR and NGS
3.5. Comparative Between PCR and NGS at AML Diagnosis
3.6. Comparative Between PCR and NGS at R/R AML Episode
3.7. Turnaraound Time
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Döhner, H.; Wei, A.H.; Appelbaum, F.R.; Craddock, C.; DiNardo, C.D.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Godley, L.A.; Hasserjian, R.P.; et al. Diagnosis and Management of AML in Adults: 2022 Recommendations from an International Expert Panel on Behalf of the ELN. Blood 2022, 140, 1345–1377. [Google Scholar] [CrossRef] [PubMed]
- Arber, D.A.; Orazi, A.; Hasserjian, R.P.; Borowitz, M.J.; Calvo, K.R.; Kvasnicka, H.M.; Wang, S.A.; Bagg, A.; Barbui, T.; Branford, S.; et al. International Consensus Classification of Myeloid Neoplasms and Acute Leukemias: Integrating Morphologic, Clinical, and Genomic Data. Blood 2022, 140, 1200–1228. [Google Scholar] [CrossRef]
- Khoury, J.D.; Solary, E.; Abla, O.; Akkari, Y.; Alaggio, R.; Apperley, J.F.; Bejar, R.; Berti, E.; Busque, L.; Chan, J.K.C.; et al. The 5th Edition of the World Health Organization Classification of Haematolymphoid Tumours: Myeloid and Histiocytic/Dendritic Neoplasms. Leukemia 2022, 36, 1703–1719. [Google Scholar] [CrossRef]
- Döhner, H.; Estey, E.; Grimwade, D.; Amadori, S.; Appelbaum, F.R.; Büchner, T.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Larson, R.A.; et al. Diagnosis and Management of AML in Adults: 2017 ELN Recommendations from an International Expert Panel. Blood 2017, 129, 424–447. [Google Scholar] [CrossRef]
- Papaemmanuil, E.; Gerstung, M.; Bullinger, L.; Gaidzik, V.I.; Paschka, P.; Roberts, N.D.; Potter, N.E.; Heuser, M.; Thol, F.; Bolli, N.; et al. Genomic Classification and Prognosis in Acute Myeloid Leukemia. N. Engl. J. Med. 2016, 374, 2209–2221. [Google Scholar] [CrossRef] [PubMed]
- Tazi, Y.; Arango-Ossa, J.E.; Zhou, Y.; Bernard, E.; Thomas, I.; Gilkes, A.; Freeman, S.; Pradat, Y.; Johnson, S.J.; Hills, R.; et al. Unified Classification and Risk-Stratification in Acute Myeloid Leukemia. Nat. Commun. 2022, 13, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Bacher, U.; Shumilov, E.; Flach, J.; Porret, N.; Joncourt, R.; Wiedemann, G.; Fiedler, M.; Novak, U.; Amstutz, U.; Pabst, T. Challenges in the Introduction of next-Generation Sequencing (NGS) for Diagnostics of Myeloid Malignancies into Clinical Routine Use. Blood Cancer J. 2018, 8, 113. [Google Scholar] [CrossRef]
- Leisch, M.; Jansko, B.; Zaborsky, N.; Greil, R.; Pleyer, L. Next Generation Sequencing in AML-on the Way to Becoming a New Standard for Treatment Initiation And/or Modulation? Cancers 2019, 11, 252. [Google Scholar] [CrossRef]
- Jennings, L.J.; Arcila, M.E.; Corless, C.; Kamel-Reid, S.; Lubin, I.M.; Pfeifer, J.; Temple-Smolkin, R.L.; Voelkerding, K.V.; Nikiforova, M.N. Guidelines for Validation of Next-Generation Sequencing–Based Oncology Panels: A Joint Consensus Recommendation of the Association for Molecular Pathology and College of American Pathologists. J. Mol. Diagn. 2017, 19, 341–365. [Google Scholar] [CrossRef]
- Pollyea, D.A.; George, T.I.; Abedi, M.; Bejar, R.; Cogle, C.R.; Foucar, K.; Garcia-Manero, G.; Grinblatt, D.L.; Komrokji, R.S.; Maciejewski, J.P.; et al. Diagnostic and Molecular Testing Patterns in Patients with Newly Diagnosed Acute Myeloid Leukemia in the Connect® MDS/AML Disease Registry. eJHaem 2020, 1, 58–68. [Google Scholar] [CrossRef]
- Sargas, C.; Ayala, R.; Chillón, M.C.; Larráyoz, M.J.; Carrillo-Cruz, E.; Bilbao, C.; Yébenes-Ramírez, M.; Llop, M.; Rapado, I.; García-Sanz, R.; et al. Networking for Advanced Molecular Diagnosis in Acute Myeloid Leukemia Patients Is Possible: The PETHEMA NGS-AML Project. Haematologica 2021, 106, 3079–3089. [Google Scholar] [CrossRef]
- Gale, R.E.; Green, C.; Allen, C.; Mead, A.J.; Burnett, A.K.; Hills, R.K.; Linch, D.C. The Impact of FLT3 Internal Tandem Duplication Mutant Level, Number, Size, and Interaction with NPM1 Mutations in a Large Cohort of Young Adult Patients with Acute Myeloid Leukemia. Blood 2008, 111, 2776–2784. [Google Scholar] [CrossRef] [PubMed]
- Thiede, C.; Steudel, C.; Mohr, B.; Schaich, M.; Schäkel, U.; Platzbecker, U.; Wermke, M.; Bornhäuser, M.; Ritter, M.; Neubauer, A.; et al. Analysis of FLT3-Activating Mutations in 979 Patients with Acute Myelogenous Leukemia: Association with FAB Subtypes and Identification of Subgroups with Poor Prognosis. Blood 2002, 99, 4326–4335. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, Y.; Kiyoi, H.; Nakano, Y.; Suzuki, R.; Kodera, Y.; Miyawaki, S.; Asou, N.; Kuriyama, K.; Yagasaki, F.; Shimazaki, C.; et al. Activating Mutation of D835 within the Activation Loop of FLT3 in Human Hematologic Malignancies. Blood 2001, 97, 2434–2439. [Google Scholar] [CrossRef]
- Tefferi, A.; Lasho, T.L.; Abdel-Wahab, O.; Guglielmelli, P.; Patel, J.; Caramazza, D.; Pieri, L.; Finke, C.M.; Kilpivaara, O.; Wadleigh, M.; et al. IDH1 and IDH2 Mutation Studies in 1473 Patients with Chronic-, Fibrotic- or Blast-Phase Essential Thrombocythemia, Polycythemia Vera or Myelofibrosis. Leukemia 2010, 24, 1302–1309. [Google Scholar] [CrossRef] [PubMed]
- Sargas, C.; Ayala, R.; Larráyoz, M.J.; Chillón, M.C.; Carrillo-Cruz, E.; Bilbao-Sieyro, C.; Prados de la Torre, E.; Martínez-Cuadrón, D.; Rodríguez-Veiga, R.; Boluda, B.; et al. Molecular Landscape and Validation of New Genomic Classification in 2668 Adult AML Patients: Real Life Data from the PETHEMA Registry. Cancers 2023, 15, 438. [Google Scholar] [CrossRef]
- Labrador, J.; Martínez-Cuadrón, D.; Boluda, B.; Serrano, J.; Gil, C.; Pérez-Simón, J.A.; Bernal, T. Evolving Patterns and Clinical Outcome of Genetic Studies Performed at Diagnosis in Acute Myeloid Leukemia Patients: Real Life Data from the PETHEMA Registry. Cancer 2024, 130, 3436–3451. [Google Scholar] [CrossRef]
- Nagel, G.; Weber, D.; Fromm, E.; Erhardt, S.; Lübbert, M.; Fiedler, W.; Kindler, T.; Krauter, J.; Brossart, P.; Kündgen, A.; et al. Epidemiological, Genetic, and Clinical Characterization by Age of Newly Diagnosed Acute Myeloid Leukemia Based on an Academic Population-Based Registry Study (AMLSG BiO). Ann. Hematol. 2017, 96, 1993–2003. [Google Scholar] [CrossRef]
- Schlenk, R.F.; Paschka, P.; Krzykalla, J.; Weber, D.; Kapp-Schwoerer, S.; Gaidzik, V.I.; Leis, C.; Fiedler, W.; Kindler, T.; Schroeder, T.; et al. Gemtuzumab Ozogamicin in NPM1-Mutated Acute Myeloid Leukemia: Early Results from the Prospective Randomized AMLSG 09-09 Phase III Study. J. Clin. Oncol. 2020, 38, 623–632. [Google Scholar] [CrossRef]
- Petersdorf, S.H.; Kopecky, K.J.; Slovak, M.; Willman, C.; Nevill, T.; Brandwein, J.; Larson, R.A.; Erba, H.P.; Stiff, P.J.; Stuart, R.K.; et al. A Phase 3 Study of Gemtuzumab Ozogamicin during Induction and Postconsolidation Therapy in Younger Patients with Acute Myeloid Leukemia. Blood 2013, 121, 4854–4860. [Google Scholar] [CrossRef]
- Hills, R.K.; Castaigne, S.; Appelbaum, F.R.; Delaunay, J.; Petersdorf, S.; Othus, M.; Estey, E.H.; Dombret, H.; Chevret, S.; Ifrah, N.; et al. Addition of Gemtuzumab Ozogamicin to Induction Chemotherapy in Adult Patients with Acute Myeloid Leukaemia: A Meta-Analysis of Individual Patient Data from Randomised Controlled Trials. Lancet Oncol. 2014, 15, 986–996. [Google Scholar] [CrossRef]
- Stone, R.M.; Mandrekar, S.J.; Sanford, B.L.; Laumann, K.; Geyer, S.; Bloomfield, C.D.; Thiede, C.; Prior, T.W.; Döhner, K.; Marcucci, G.; et al. Midostaurin plus Chemotherapy for Acute Myeloid Leukemia with a FLT3 Mutation. N. Engl. J. Med. 2017, 377, 454–464. [Google Scholar] [CrossRef]
- Döhner, H.; Pratz, K.W.; DiNardo, C.D.; Wei, A.H.; Jonas, B.A.; Pullarkat, V.A.; Thirman, M.J.; Récher, C.; Schuh, A.C.; Babu, S.; et al. Genetic Risk Stratification and Outcomes among Treatment-Naive Patients with AML Treated with Venetoclax and Azacitidine. Blood 2024, 144, 2211–2222. [Google Scholar] [CrossRef] [PubMed]
- Megías-Vericat, J.E.; Ballesta-López, O.; Barragán, E.; Montesinos, P. IDH1-Mutated Relapsed or Refractory AML: Current Challenges and Future Prospects. Blood Lymphat. Cancer Targets Ther. 2019, 9, 19–32. [Google Scholar] [CrossRef] [PubMed]
- Zarnegar-Lumley, S.; Alonzo, T.A.; Gerbing, R.B.; Othus, M.; Sun, Z.; Ries, R.E.; Wang, J.; Leonti, A.; Kutny, M.A.; Ostronoff, F.; et al. Characteristics and Prognostic Impact of IDH Mutations in AML: A COG, SWOG, and ECOG Analysis. Blood Adv. 2023, 7, 5941–5953. [Google Scholar] [CrossRef]
- Paschka, P.; Schlenk, R.F.; Gaidzik, V.I.; Habdank, M.; Krönke, J.; Bullinger, L.; Späth, D.; Kayser, S.; Zucknick, M.; Götze, K.; et al. IDH1 and IDH2 Mutations Are Frequent Genetic Alterations in Acute Myeloid Leukemia and Confer Adverse Prognosis in Cytogenetically Normal Acute Myeloid Leukemia with NPM1 Mutation without FLT3 Internal Tandem Duplication. J. Clin. Oncol. 2010, 28, 3636–3643. [Google Scholar] [CrossRef] [PubMed]
- Perl, A.E.; Martinelli, G.; Cortes, J.E.; Neubauer, A.; Berman, E.; Paolini, S.; Montesinos, P.; Baer, M.R.; Larson, R.A.; Ustun, C.; et al. Gilteritinib or Chemotherapy for Relapsed or Refractory FLT3 -Mutated AML. N. Engl. J. Med. 2019, 381, 1728–1740. [Google Scholar] [CrossRef]
- Daver, N.; Schlenk, R.F.; Russell, N.H.; Levis, M.J. Targeting FLT3 Mutations in AML: Review of Current Knowledge and Evidence. Leukemia 2019, 33, 299–312. [Google Scholar] [CrossRef]
- Dumas, P.Y.; Raffoux, E.; Bérard, E.; Bertoli, S.; Hospital, M.A.; Heiblig, M.; Desbrosses, Y.; Bonmati, C.; Pautas, C.; Lambert, J.; et al. Gilteritinib Activity in Refractory or Relapsed FLT3-Mutated Acute Myeloid Leukemia Patients Previously Treated by Intensive Chemotherapy and Midostaurin: A Study from the French AML Intergroup ALFA/FILO. Leukemia 2023, 37, 91–101. [Google Scholar] [CrossRef]
- Haferlach, T. Advancing Leukemia Diagnostics: Role of next Generation Sequencing (Ngs) in Acute Myeloid Leukemia. Hematol. Rep. 2020, 12, 8957. [Google Scholar] [CrossRef]
- Mezei, Z.A.; Tornai, D.; Földesi, R.; Madar, L.; Sümegi, A.; Papp, M.; Antal-Szalmás, P. A DNA Pool of FLT3-ITD Positive DNA Samples Can Be Used Efficiently for Analytical Evaluation of NGS-Based FLT3-ITD Quantitation—Testing Several Different ITD Sequences and Rates, Simultaneously. J. Biotechnol. 2019, 303, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Schranz, K.; Hubmann, M.; Harin, E.; Vosberg, S.; Herold, T.; Metzeler, K.H.; Rothenberg-Thurley, M.; Janke, H.; Bräundl, K.; Ksienzyk, B.; et al. Clonal Heterogeneity of FLT3-ITD Detected by High-Throughput Amplicon Sequencing Correlates with Adverse Prognosis in Acute Myeloid Leukemia. Oncotarget 2018, 9, 30128–30145. [Google Scholar] [CrossRef] [PubMed]
- Alvarado, Y.; Kantarjian, H.M.; Luthra, R.; Ravandi, F.; Borthakur, G.; Garcia-Manero, G.; Konopleva, M.; Estrov, Z.; Andreeff, M.; Cortes, J.E. Treatment with FLT3 Inhibitor in Patients with FLT3-Mutated Acute Myeloid Leukemia Is Associated with Development of Secondary FLT3-Tyrosine Kinase Domain Mutations. Cancer 2014, 120, 2142–2149. [Google Scholar] [CrossRef] [PubMed]
- Grob, T.; Sanders, M.A.; Vonk, C.M.; Kavelaars, F.G.; Rijken, M.; Hanekamp, D.W.; Gradowska, P.L.; Cloos, J.; Fløisand, Y.; Van Marwijk Kooy, M.; et al. Prognostic Value of FLT3 -Internal Tandem Duplication Residual Disease in Acute Myeloid Leukemia. J. Clin. Oncol. 2023, 41, 756–765. [Google Scholar] [CrossRef]
- Wang, E.S.; Issa, G.C.; Erba, H.P.; Altman, J.K.; Montesinos, P.; DeBotton, S.; Walter, R.B.; Pettit, K.; Savona, M.R.; Shah, M.V.; et al. Ziftomenib in Relapsed or Refractory Acute Myeloid Leukaemia (KOMET-001): A Multicentre, Open-Label, Multi-Cohort, Phase 1 Trial. Lancet Oncol. 2024, 25, 1310–1324. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Median (Range) | Number (%) n = 1512 |
|---|---|---|
| Age at diagnosis | 65 (19–98) | |
| <60 years | 511 (34) | |
| 60–70 years | 428 (28) | |
| >70 years | 573 (38) | |
| Male sex | 860 (57) | |
| ECOG | 1 (0–4) | |
| 0–1 | 789 (79) | |
| ≥2 | 210 (21) | |
| WBC count (×109/L) | 8.6 (0.1–401) | |
| Hemoglobin (g/dL) | 8.9 (2–15.9) | |
| Platelet count (×109/L) | 54 (3–907) | |
| BM blast % | 54 (1–100) | |
| Cytogenetic risk MRC (n = 824) | ||
| Low | 68 (8) | |
| Intermediate | 485 (59) | |
| High | 271 (33) |
| Gene Mutation | PCR+ N(%) | PCR− N(%) | TOTAL | |
|---|---|---|---|---|
| NPM1 | NGS+ | 262 (98.5) | 10 (1.1) | 272 |
| NGS− | 4 (1.5) | 880 (98.9) | 884 | |
| TOTAL | 266 (100) | 890 (100) | 1156 | |
| FLT3-ITD | NGS+ | 149 (73.8) | 4 (0.04) | 153 |
| NGS− | 53 (26.2) | 1061 (99.6) | 1114 | |
| TOTAL | 202 (100) | 1065 (100) | 1267 | |
| FLT3-TKD | NGS+ | 49 (84.5) | 8 (0.07) | 57 |
| NGS− | 9 (15.5) | 1064 (99.3) | 1073 | |
| TOTAL | 58 (100) | 1072 (100) | 1130 | |
| IDH1 | NGS+ | 77 (98.7) | 11 (1.3) | 88 |
| NGS− | 1 (1.3) | 836 (98.7) | 837 | |
| TOTAL | 78 (100) | 847 (100) | 925 | |
| IDH2 | NGS+ | 107 (99.1) | 19 (2.3) | 126 |
| NGS− | 1 (0.9) | 804 (97.7) | 805 | |
| TOTAL | 108 (100) | 823 (100) | 931 |
| Gene Mutation | PCR+ N(%) | PCR− N(%) | TOTAL | |
|---|---|---|---|---|
| NPM1 | NGS+ | 264 (99.2) | 14 (1.6) | 278 |
| NGS− | 2 (0.8) | 876 (98.4) | 878 | |
| TOTAL | 266 (100) | 890 (100) | 1156 | |
| FLT3-ITD | NGS+ | 176 (87.1) | 11 (0.1) | 187 |
| NGS− | 26 (12.9) | 1054 (99) | 1080 | |
| TOTAL | 202 (100) | 1065 (100) | 1267 | |
| FLT3-TKD | NGS+ | 53 (91.4) | 34 (3.2) | 87 |
| NGS− | 5 (8.6) | 1038 (96.8) | 1043 | |
| TOTAL | 58 (100) | 1072 (100) | 1130 | |
| IDH1 | NGS+ | 77 (98.7) | 18 (2.1) | 95 |
| NGS− | 1 (1.3) | 829 (97.9) | 830 | |
| TOTAL | 78 (100) | 847 (100) | 925 | |
| IDH2 | NGS+ | 107 (99.1) | 22 (2.7) | 129 |
| NGS− | 1 (0.9) | 801 (97.3) | 802 | |
| TOTAL | 108 (100) | 823 (100) | 931 |
| Protein Change Detected | Number of Patients | VAF (%) Median (Range) |
|---|---|---|
| Asp835Tyr | 14 | 3.2 (1–44.29) |
| Asp835His | 6 | 2.1 (1.23–46.6) |
| Asp835Glu | 5 | 1.9 (1.13–4.68) |
| Ile836del | 5 | 3 (1.91–12.53) |
| Asp835Val | 2 | 21.43 (1.4–41.46) |
| Asp835Ile | 1 | 3.11 |
| Asp835del | 1 | 4.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boluda, B.; Rodriguez-Veiga, R.; Sargas, C.; Ayala, R.; Larráyoz, M.J.; Chillón, M.C.; Soria-Saldise, E.; Bilbao, C.; Prados de la Torre, E.; Navarro, I.; et al. Conventional PCR Versus Next Generation Sequencing for Diagnosis of FLT3, IDH and NPM1 Mutations in Acute Myeloid Leukemia: Results of the PETHEMA PCR-LMA Study. Cancers 2025, 17, 854. https://doi.org/10.3390/cancers17050854
Boluda B, Rodriguez-Veiga R, Sargas C, Ayala R, Larráyoz MJ, Chillón MC, Soria-Saldise E, Bilbao C, Prados de la Torre E, Navarro I, et al. Conventional PCR Versus Next Generation Sequencing for Diagnosis of FLT3, IDH and NPM1 Mutations in Acute Myeloid Leukemia: Results of the PETHEMA PCR-LMA Study. Cancers. 2025; 17(5):854. https://doi.org/10.3390/cancers17050854
Chicago/Turabian StyleBoluda, Blanca, Rebeca Rodriguez-Veiga, Claudia Sargas, Rosa Ayala, María J. Larráyoz, María Carmen Chillón, Elena Soria-Saldise, Cristina Bilbao, Esther Prados de la Torre, Irene Navarro, and et al. 2025. "Conventional PCR Versus Next Generation Sequencing for Diagnosis of FLT3, IDH and NPM1 Mutations in Acute Myeloid Leukemia: Results of the PETHEMA PCR-LMA Study" Cancers 17, no. 5: 854. https://doi.org/10.3390/cancers17050854
APA StyleBoluda, B., Rodriguez-Veiga, R., Sargas, C., Ayala, R., Larráyoz, M. J., Chillón, M. C., Soria-Saldise, E., Bilbao, C., Prados de la Torre, E., Navarro, I., Martinez-Cuadron, D., Gil, C., Bernal, T., Bergua, J., Algarra, L., Tormo, M., Martínez-Sanchez, P., Carrillo-Cruz, E., Serrano, J., ... Montesinos, P., on behalf of the PETHEMA Group. (2025). Conventional PCR Versus Next Generation Sequencing for Diagnosis of FLT3, IDH and NPM1 Mutations in Acute Myeloid Leukemia: Results of the PETHEMA PCR-LMA Study. Cancers, 17(5), 854. https://doi.org/10.3390/cancers17050854