PTCY-Based Haploidentical Donor Transplantation versus HLA-Matched Related and Unrelated Donor Transplantations in Patients with Refractory or Relapsed Lymphoma—A Matched-Pair Analysis

Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Definition
2.3. Supportive Care
2.4. Statistical Methods
3. Results
3.1. Patients and Transplant Characteristics
3.2. Engraftment
3.3. Treatment-Related Toxicities and Infections
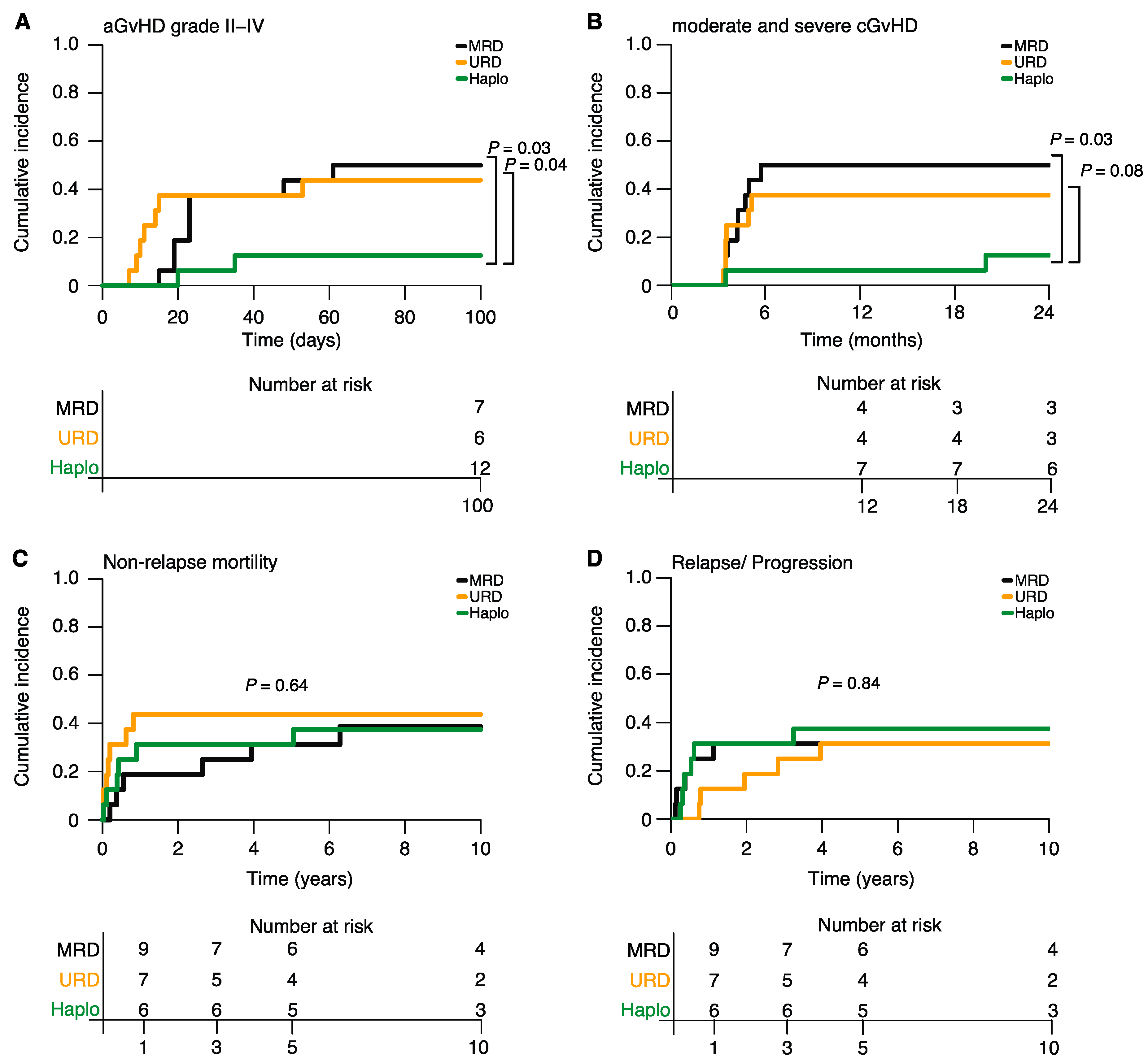
3.4. GvHD, Relapse and NRM
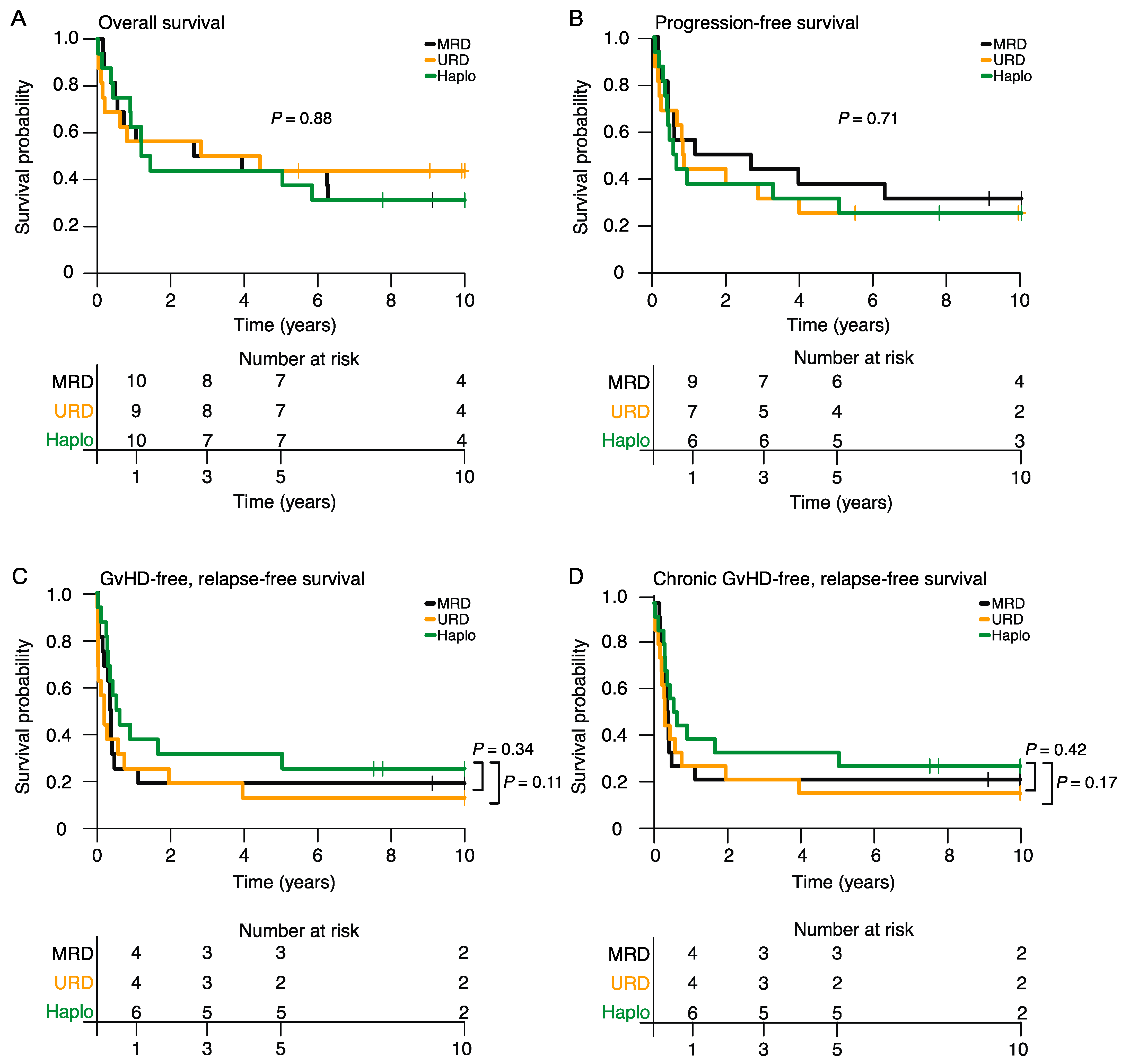
3.5. Outcome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dickinson, M.J.; Carlo-Stella, C.; Morschhauser, F.; Bachy, E.; Corradini, P.; Iacoboni, G.; Khan, C.; Wróbel, T.; Offner, F.; Trněný, M.; et al. Glofitamab for Relapsed or Refractory Diffuse Large B-Cell Lymphoma. N. Engl. J. Med. 2022, 387, 2220–2231. [Google Scholar] [CrossRef]
- Chong, E.A.; Ruella, M.; Schuster, S.J. Five-Year Outcomes for Refractory B-Cell Lymphomas with CAR T-Cell Therapy. N. Engl. J. Med. 2021, 384, 673–674. [Google Scholar] [CrossRef]
- Westin, J.R.; Oluwole, O.O.; Kersten, M.J.; Miklos, D.B.; Perales, M.A.; Ghobadi, A.; Rapoport, A.P.; Sureda, A.; Jacobson, C.A.; Farooq, U.; et al. Survival with Axicabtagene Ciloleucel in Large B-Cell Lymphoma. N. Engl. J. Med. 2023, 389, 148–157. [Google Scholar] [CrossRef]
- van Kampen, R.J.; Canals, C.; Schouten, H.C.; Nagler, A.; Thomson, K.J.; Vernant, J.P.; Buzyn, A.; Boogaerts, M.A.; Luan, J.J.; Maury, S.; et al. Allogeneic stem-cell transplantation as salvage therapy for patients with diffuse large B-cell non-Hodgkin’s lymphoma relapsing after an autologous stem-cell transplantation: An analysis of the European Group for Blood and Marrow Transplantation Registry. J. Clin. Oncol. 2011, 29, 1342–1348. [Google Scholar] [CrossRef] [PubMed]
- Kyriakou, C.; Canals, C.; Finke, J.; Kobbe, G.; Harousseau, J.L.; Kolb, H.J.; Novitzky, N.; Goldstone, A.H.; Sureda, A.; Schmitz, N. Allogeneic stem cell transplantation is able to induce long-term remissions in angioimmunoblastic T-cell lymphoma: A retrospective study from the lymphoma working party of the European group for blood and marrow transplantation. J. Clin. Oncol. 2009, 27, 3951–3958. [Google Scholar] [CrossRef]
- Fenske, T.S.; Hamadani, M.; Cohen, J.B.; Costa, L.J.; Kahl, B.S.; Evens, A.M.; Hamlin, P.A.; Lazarus, H.M.; Petersdorf, E.; Bredeson, C. Allogeneic Hematopoietic Cell Transplantation as Curative Therapy for Patients with Non-Hodgkin Lymphoma: Increasingly Successful Application to Older Patients. Biol. Blood Marrow Transplant. 2016, 22, 1543–1551. [Google Scholar] [CrossRef] [PubMed]
- Gopal, A.K.; Guthrie, K.A.; Rajendran, J.; Pagel, J.M.; Oliveira, G.; Maloney, D.G.; Matesan, M.C.; Storb, R.F.; Press, O.W. (9)(0)Y-Ibritumomab tiuxetan, fludarabine, and TBI-based nonmyeloablative allogeneic transplantation conditioning for patients with persistent high-risk B-cell lymphoma. Blood 2011, 118, 1132–1139. [Google Scholar] [CrossRef] [PubMed]
- Zoellner, A.K.; Fritsch, S.; Prevalsek, D.; Engel, N.; Hubmann, M.; Reibke, R.; Rieger, C.T.; Hellmuth, J.C.; Haas, M.; Mumm, F.; et al. Sequential therapy combining clofarabine and T-cell-replete HLA-haploidentical haematopoietic SCT is feasible and shows efficacy in the treatment of refractory or relapsed aggressive lymphoma. Bone Marrow Transplant. 2015, 50, 679–684. [Google Scholar] [CrossRef] [PubMed]
- Avivi, I.; Canals, C.; Vernant, J.P.; Wulf, G.; Nagler, A.; Hermine, O.; Petersen, E.; Yakoub-Agha, I.; Craddock, C.; Schattenberg, A.; et al. Matched unrelated donor allogeneic transplantation provides comparable long-term outcome to HLA-identical sibling transplantation in relapsed diffuse large B-cell lymphoma. Bone Marrow Transplant. 2014, 49, 671–678. [Google Scholar] [CrossRef][Green Version]
- Berning, P.; Schmitz, N.; Ngoya, M.; Finel, H.; Boumendil, A.; Wang, F.; Huang, X.J.; Hermine, O.; Philippe, L.; Couronné, L.; et al. Allogeneic hematopoietic stem cell transplantation for NK/T-cell lymphoma: An international collaborative analysis. Leukemia 2023, 37, 1511–1520. [Google Scholar] [CrossRef]
- Passweg, J.R.; Baldomero, H.; Basak, G.W.; Chabannon, C.; Corbacioglu, S.; Duarte, R.; Kuball, J.; Lankester, A.; Montoto, S.; de Latour, R.P.; et al. The EBMT activity survey report 2017: A focus on allogeneic HCT for nonmalignant indications and on the use of non-HCT cell therapies. Bone Marrow Transplant. 2019, 54, 1575–1585. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, S.; Dreger, P.; Hermine, O.; Kyriakou, C.; Montoto, S.; Robinson, S.; Schmitz, N.; Schouten, H.C.; Sureda, A.; Tanase, A. Haploidentical stem cell transplantation for patients with lymphoma: A position statement from the Lymphoma Working Party-European Society for Blood and Marrow Transplantation. Bone Marrow Transplant. 2019, 55, 317–324. [Google Scholar] [CrossRef] [PubMed]
- McCurdy, S.R.; Kanakry, J.A.; Showel, M.M.; Tsai, H.L.; Bolanos-Meade, J.; Rosner, G.L.; Kanakry, C.G.; Perica, K.; Symons, H.J.; Brodsky, R.A.; et al. Risk-stratified outcomes of nonmyeloablative HLA-haploidentical BMT with high-dose posttransplantation cyclophosphamide. Blood 2015, 125, 3024–3031. [Google Scholar] [CrossRef] [PubMed]
- Passweg, J.R.; Baldomero, H.; Bader, P.; Bonini, C.; Duarte, R.F.; Dufour, C.; Gennery, A.; Kroger, N.; Kuball, J.; Lanza, F.; et al. Use of haploidentical stem cell transplantation continues to increase: The 2015 European Society for Blood and Marrow Transplant activity survey report. Bone Marrow Transplant. 2017, 52, 811–817. [Google Scholar] [CrossRef] [PubMed]
- Solomon, S.R.; Sizemore, C.A.; Sanacore, M.; Zhang, X.; Brown, S.; Holland, H.K.; Morris, L.E.; Bashey, A. Haploidentical transplantation using T cell replete peripheral blood stem cells and myeloablative conditioning in patients with high-risk hematologic malignancies who lack conventional donors is well tolerated and produces excellent relapse-free survival: Results of a prospective phase II trial. Biol Blood Marrow Transplant. 2012, 18, 1859–1866. [Google Scholar] [CrossRef]
- Raiola, A.M.; Dominietto, A.; Ghiso, A.; Di Grazia, C.; Lamparelli, T.; Gualandi, F.; Bregante, S.; Van Lint, M.T.; Geroldi, S.; Luchetti, S.; et al. Unmanipulated haploidentical bone marrow transplantation and posttransplantation cyclophosphamide for hematologic malignancies after myeloablative conditioning. Biol Blood Marrow Transplant. 2013, 19, 117–122. [Google Scholar] [CrossRef]
- Luznik, L.; O’Donnell, P.V.; Symons, H.J.; Chen, A.R.; Leffell, M.S.; Zahurak, M.; Gooley, T.A.; Piantadosi, S.; Kaup, M.; Ambinder, R.F.; et al. HLA-haploidentical bone marrow transplantation for hematologic malignancies using nonmyeloablative conditioning and high-dose, posttransplantation cyclophosphamide. Biol Blood Marrow Transplant. 2008, 14, 641–650. [Google Scholar] [CrossRef]
- Ciurea, S.O.; Bayraktar, U.D. “No donor”? Consider a haploidentical transplant. Blood Rev. 2015, 29, 63–70. [Google Scholar] [CrossRef]
- Kanate, A.S.; Mussetti, A.; Kharfan-Dabaja, M.A.; Ahn, K.W.; DiGilio, A.; Beitinjaneh, A.; Chhabra, S.; Fenske, T.S.; Freytes, C.; Gale, R.P.; et al. Reduced-intensity transplantation for lymphomas using haploidentical related donors vs. HLA-matched unrelated donors. Blood 2016, 127, 938–947. [Google Scholar] [CrossRef]
- Kanakry, J.A.; Kasamon, Y.L.; Gocke, C.D.; Tsai, H.L.; Davis-Sproul, J.; Ghosh, N.; Symons, H.; Bolanos-Meade, J.; Gladstone, D.E.; Swinnen, L.J.; et al. Outcomes of related donor HLA-identical or HLA-haploidentical allogeneic blood or marrow transplantation for peripheral T cell lymphoma. Biol. Blood Marrow Transplant. J. Am. Soc. Blood Marrow Transplant. 2013, 19, 602–606. [Google Scholar] [CrossRef]
- Dietrich, S.; Finel, H.; Martinez, C.; Tischer, J.; Blaise, D.; Chevallier, P.; Castagna, L.; Milpied, N.; Bacigalupo, A.; Corradini, P.; et al. Post-transplant cyclophosphamide-based haplo-identical transplantation as alternative to matched sibling or unrelated donor transplantation for non-Hodgkin lymphoma: A registry study by the European society for blood and marrow transplantation. Leukemia 2016, 30, 2086–2089. [Google Scholar] [CrossRef] [PubMed]
- Dulery, R.; Menard, A.L.; Chantepie, S.; El Cheikh, J.; Francois, S.; Delage, J.; Giannotti, F.; Ruggeri, A.; Brissot, E.; Battipaglia, G.; et al. Sequential Conditioning with Thiotepa in T-Cell Replete Hematopoietic Stem Cell Transplantation for the Treatment of Refractory Hematological Malignancies: Comparison with Matched Related, Haplo-Mismatched and Unrelated Donors. Biol. Blood Marrow Transplant. 2018, 30, 2086–2089. [Google Scholar] [CrossRef]
- Dreger, P.; Sureda, A.; Ahn, K.W.; Eapen, M.; Litovich, C.; Finel, H.; Boumendil, A.; Gopal, A.; Herrera, A.F.; Schmid, C.; et al. PTCy-based haploidentical vs. matched related or unrelated donor reduced-intensity conditioning transplant for DLBCL. Blood Adv. 2019, 3, 360–369. [Google Scholar] [CrossRef] [PubMed]
- Meybodi, M.A.; Cao, W.; Luznik, L.; Bashey, A.; Zhang, X.; Romee, R.; Saber, W.; Hamadani, M.; Weisdorf, D.J.; Chu, H.; et al. HLA-haploidentical vs. matched-sibling hematopoietic cell transplantation: A systematic review and meta-analysis. Blood Adv. 2019, 3, 2581–2585. [Google Scholar] [CrossRef] [PubMed]
- Fraccaroli, A.; Prevalsek, D.; Fritsch, S.; Haebe, S.; Bucklein, V.; Schulz, C.; Hubmann, M.; Stemmler, H.J.; Ledderose, G.; Hausmann, A.; et al. Sequential HLA-haploidentical transplantation utilizing post-transplantation cyclophosphamide for GvHD prophylaxis in high-risk and relapsed/refractory AML/MDS. Am. J. Hematol. 2018, 93, 1524–1531. [Google Scholar] [CrossRef]
- Doppelhammer, M.; Fraccaroli, A.; Prevalsek, D.; Bücklein, V.; Häbe, S.; Schulz, C.; Hubmann, M.; Hausmann, A.; Claus, R.; Rank, A.; et al. Comparable outcome after haploidentical and HLA-matched allogeneic stem cell transplantation for high-risk acute myeloid leukemia following sequential conditioning-a matched pair analysis. Ann. Hematol. 2019, 98, 753–762. [Google Scholar] [CrossRef]
- Armand, P.; Kim, H.T.; Logan, B.R.; Wang, Z.; Alyea, E.P.; Kalaycio, M.E.; Maziarz, R.T.; Antin, J.H.; Soiffer, R.J.; Weisdorf, D.J.; et al. Validation and refinement of the Disease Risk Index for allogeneic stem cell transplantation. Blood 2014, 123, 3664–3671. [Google Scholar] [CrossRef]
- Bacigalupo, A.; Ballen, K.; Rizzo, D.; Giralt, S.; Lazarus, H.; Ho, V.; Apperley, J.; Slavin, S.; Pasquini, M.; Sandmaier, B.M.; et al. Defining the intensity of conditioning regimens: Working definitions. Biol. Blood Marrow Transplant. 2009, 15, 1628–1633. [Google Scholar] [CrossRef]
- Center for International Blood and Marrow Transplant Research. CIBMTR Forms Manual: 100 Days Post-HSCT Data Form 2100. 2014. Available online: http://www.cibmtr.org/DataManagement/TrainingReference/Manuals/DataManagement/Documents (accessed on 15 September 2023).
- Przepiorka, D.; Weisdorf, D.; Martin, P.; Klingemann, H.G.; Beatty, P.; Hows, J.; Thomas, E.D. 1994 Consensus Conference on Acute GVHD Grading. Bone Marrow Transplant. 1995, 15, 825–828. [Google Scholar]
- Filipovich, A.H.; Weisdorf, D.; Pavletic, S.; Socie, G.; Wingard, J.R.; Lee, S.J.; Martin, P.; Chien, J.; Przepiorka, D.; Couriel, D.; et al. National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I. Diagnosis and staging working group report. Biol. Blood Marrow Transplant. J. Am. Soc. Blood Marrow Transplant. 2005, 11, 945–956. [Google Scholar] [CrossRef]
- Tischer, J.; Engel, N.; Fritsch, S.; Prevalsek, D.; Hubmann, M.; Schulz, C.; Zoellner, A.K.; Bucklein, V.; Reibke, R.; Mumm, F.; et al. Virus infection in HLA-haploidentical hematopoietic stem cell transplantation: Incidence in the context of immune recovery in two different transplantation settings. Ann. Hematol. 2015, 94, 1677–1688. [Google Scholar] [CrossRef] [PubMed]
- McCurdy, S.R.; Kasamon, Y.L.; Kanakry, C.G.; Bolanos-Meade, J.; Tsai, H.L.; Showel, M.M.; Kanakry, J.A.; Symons, H.J.; Gojo, I.; Smith, B.D.; et al. Comparable composite endpoints after HLA-matched and HLA-haploidentical transplantation with post-transplantation cyclophosphamide. Haematologica 2017, 102, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Saini, N.Y.; Saliba, R.M.; Rondon, G.; Maadani, F.; Popat, U.; Hosing, C.M.; Oran, B.; Bashir, Q.; Olson, A.; Nieto, Y.; et al. Impact of Donor Type and Melphalan Dose on Allogeneic Transplantation Outcomes for Patients with Lymphoma. Biol. Blood Marrow Transplant. 2019, 25, 1340–1346. [Google Scholar] [CrossRef] [PubMed]
- Abramson, H.N. Monoclonal Antibodies for the Treatment of Multiple Myeloma: An Update. Int. J. Mol. Sci. 2018, 19, 3924. [Google Scholar] [CrossRef]
- Mariotti, J.; Bramanti, S.; Santoro, A.; Castagna, L. Haploidentical Stem Cell Transplantation in Lymphomas-Expectations and Pitfalls. J. Clin. Med. 2020, 9, 3589. [Google Scholar] [CrossRef]
- Luznik, L.; Fuchs, E.J. High-dose, post-transplantation cyclophosphamide to promote graft-host tolerance after allogeneic hematopoietic stem cell transplantation. Immunol. Res. 2010, 47, 65–77. [Google Scholar] [CrossRef]
- Kanakry, J.A.; Gocke, C.D.; Bolanos-Meade, J.; Gladstone, D.E.; Swinnen, L.J.; Blackford, A.L.; Fuchs, E.J.; Huff, C.A.; Borrello, I.; Matsui, W.H.; et al. Phase II Study of Nonmyeloablative Allogeneic Bone Marrow Transplantation for B Cell Lymphoma with Post-Transplantation Rituximab and Donor Selection Based First on Non-HLA Factors. Biol. Blood Marrow Transplant. 2015, 21, 2115–2122. [Google Scholar] [CrossRef][Green Version]
- Gooptu, M.; Romee, R.; St Martin, A.; Arora, M.; Al Malki, M.; Antin, J.H.; Bredeson, C.N.; Brunstein, C.G.; Chhabra, S.; Fuchs, E.J.; et al. HLA-haploidentical vs. matched unrelated donor transplants with posttransplant cyclophosphamide-based prophylaxis. Blood 2021, 138, 273–282. [Google Scholar] [CrossRef]
- Mussetti, A.; Kanate, A.S.; Wang, T.; He, M.; Hamadani, M.; Finel, H., Sr.; Boumendil, A., Sr.; Glass, B.; Castagna, L.; Dominietto, A.; et al. Haploidentical Versus Matched Unrelated Donor Transplants Using Post-Transplantation Cyclophosphamide for Lymphomas. Transplant. Cell Ther. 2023, 29, 184.e181–184.e189. [Google Scholar] [CrossRef]
- Bashey, A.; Zhang, M.J.; McCurdy, S.R.; St Martin, A.; Argall, T.; Anasetti, C.; Ciurea, S.O.; Fasan, O.; Gaballa, S.; Hamadani, M.; et al. Mobilized Peripheral Blood Stem Cells Versus Unstimulated Bone Marrow As a Graft Source for T-Cell-Replete Haploidentical Donor Transplantation Using Post-Transplant Cyclophosphamide. J. Clin. Oncol. 2017, 35, 3002–3009. [Google Scholar] [CrossRef]
- Cappell, K.M.; Sherry, R.M.; Yang, J.C.; Goff, S.L.; Vanasse, D.A.; McIntyre, L.; Rosenberg, S.A.; Kochenderfer, J.N. Long-Term Follow-Up of Anti-CD19 Chimeric Antigen Receptor T-Cell Therapy. J. Clin. Oncol. 2020, 38, 3805–3815. [Google Scholar] [CrossRef] [PubMed]
- Locke, F.L.; Ghobadi, A.; Jacobson, C.A.; Miklos, D.B.; Lekakis, L.J.; Oluwole, O.O.; Lin, Y.; Braunschweig, I.; Hill, B.T.; Timmerman, J.M.; et al. Long-term safety and activity of axicabtagene ciloleucel in refractory large B-cell lymphoma (ZUMA-1): A single-arm, multicentre, phase 1-2 trial. Lancet. Oncol. 2019, 20, 31–42. [Google Scholar] [CrossRef] [PubMed]
- Locke, F.L.; Miklos, D.B.; Jacobson, C.A.; Perales, M.A.; Kersten, M.J.; Oluwole, O.O.; Ghobadi, A.; Rapoport, A.P.; McGuirk, J.; Pagel, J.M.; et al. Axicabtagene Ciloleucel as Second-Line Therapy for Large B-Cell Lymphoma. N. Engl. J. Med. 2022, 386, 640–654. [Google Scholar] [CrossRef] [PubMed]
- Dreger, P.; Fenske, T.S.; Montoto, S.; Pasquini, M.C.; Sureda, A.; Hamadani, M. Cellular Immunotherapy for Refractory Diffuse Large B Cell Lymphoma in the Chimeric Antigen Receptor-Engineered T Cell Era: Still a Role for Allogeneic Transplantation? Biol. Blood Marrow Transplant. 2020, 26, e77–e85. [Google Scholar] [CrossRef]
- Epperla, N.; Kumar, A.; Abutalib, S.A.; Awan, F.T.; Chen, Y.B.; Gopal, A.K.; Holter-Chakrabarty, J.; Kekre, N.; Lee, C.J.; Lekakis, L.; et al. ASTCT Clinical Practice Recommendations for Transplantation and Cellular Therapies in Diffuse Large B Cell Lymphoma. Transplant. Cell Ther. 2023, 29, 548–555. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| MRD (1) | URD (2) | Haplo (3) | p Value | |||
|---|---|---|---|---|---|---|
| 1 vs. 3 | 2 vs. 3 | Overall | ||||
| Patients | 16 (100) | 16 (100) | 16 (100) | |||
| Patient age *, median (range), year | 53 (42–62) | 51 (44–67) | 52 (45–66) | 0.98 | 0.57 | 0.76 |
| Patient sex | ||||||
| Female | 4 (25) | 8 (50) | 5 (31) | >0.99 | 0.47 | 0.31 |
| KPS ≥ 80 * | 16 (100) | 16 (100) | 16 (100) | >0.99 | >0.99 | >0.99 |
| ECOG 0-I * | 16 (100) | 16 (100) | 16 (100) | >0.99 | >0.99 | >0.99 |
| Lymphoma classification * | >0.99 | >0.99 | >0.99 | |||
| Indolent | 2 (12.5) | 2 (12.5) | 2 (12.5) | |||
| Aggressive | 14 (87.5) | 14 (87.5) | 14 (87.5) | |||
| Histology | 0.79 | 0.88 | 0.83 | |||
| Indolent B-NHL | 2 (12.5) | 2 (12.5) | 2 (12.5) | |||
| Aggressive T-NHL | 4 (25) | 2 (12.5) | 2 (12.5) | |||
| MCL | 6 (37.5) | 4 (25) | 6 (37.5) | |||
| DLBCL | 4 (25) | 8 (50) | 6 (37.5) | |||
| Status prior HSCT initiation * | >0.99 | >0.99 | >0.99 | |||
| CR | 2 (12.5) | 2 (12.5) | 2 (12.5) | |||
| Active | 14 (87.5) | 14 (87.5) | 14 (87.5) | |||
| Prior therapy regimens | 0.34 | 0.71 | 0.44 | |||
| Median (range) | 4 (3–7) | 4 (2–7) | 5 (2–7) | |||
| Prior auto-HSCT | 11 (69) | 10 (62.5) | 9 (56) | |||
| Modified DRI score | 0.85 | 0.55 | 0.66 | |||
| Low | 3 (19) | 2 (12.5) | 2 (13) | |||
| Intermediate | 4 (25) | 7 (44) | 4 (25) | |||
| High | 6 (37) | 2 (12.5) | 5 (31) | |||
| Very high | 3 (19) | 5 (31) | 5 (31) | |||
| HCT score | ||||||
| ≥3 | 10 (62.5) | 7 (44) | 8 (50) | 0.48 | 0.72 | 0.56 |
| Median follow-up, year | 10.4 | 10.2 | 10.5 |
| MRD (1) | URD (2) | Haplo (3) | p Value | |||
|---|---|---|---|---|---|---|
| 1 vs. 3 | 2 vs. 3 | Overall | ||||
| Patients | 16 (100) | 16 (100) | 16 (100) | |||
| Donor age, median (range), year | 48 (23–63) | 28 (20–58) | 27 (19–68) | 0.009 | 0.86 | 0.002 |
| Donor sex | ||||||
| Female | 6 (37.5) | 4 (25) | 12 (75) | 0.03 | 0.005 | 0.12 |
| D-R sex match | ||||||
| Female—Male | 5 (31) | 2 (13) | 8 (50) | 0.28 | 0.02 | 0.07 |
| Donor kindship | n.a. | n.a. | n.a. | |||
| Sibling | 16 (100) | n.a. | 4 (25) | |||
| Children | n.a. | n.a. | 10 (63) | |||
| Parents | n.a. | n.a. | 1 (6) | |||
| Cousins | n.a. | n.a. | 1 (6) | |||
| ABO incompatibility | 0.92 | 0.52 | 0.85 | |||
| Major | 1(6) | 1(6) | 1 (6) | |||
| Minor | 5 (31) | 7 (44) | 4 (25) | |||
| None | 10 (63) | 8 (50) | 11 (69) | |||
| Stem cell source | <0.001 | <0.001 | <0.001 | |||
| Bone marrow | 1 (6) | 0 | 11 (69) | |||
| Peripheral blood | 15 (94) | 16 (100) | 5 (31) | |||
| Average graft cell dose (range) | ||||||
| NC × 108/kg BW | 2.0 | 0 | 3.2 (1.7–4.4) | n.a. | n.a. | n.a. |
| CD34+ × 106/kg BW | 8.7 (3.3–14.5) | 9.1 (4.7–14) | 6.8 (2.9–14.3) | 0.34 | 0.2 | 0.39 |
| CMV R-D sero-status | 0.42 | 0.77 | 0.78 | |||
| Negative/negative | 5 (31) | 8 (50) | 8 (50) | |||
| Negative/positive | 2 (13) | 1 (6) | 0 | |||
| Positive/negative | 4 (25) | 3 (19) | 4 (25) | |||
| Positive/positive | 5 (31) | 4 (25) | 4 (25) | |||
| Conditioning regimen | 0.04 | 0.001 | <0.001 | |||
| Flu/CY/TBI | 5 (31) | 7 (44) | 0 | |||
| Flu/CY ± others | 6 (38) | 5 (31) | 0 | |||
| Flu/Mel ± others | 0 | 3 (19) | 16 (100) | |||
| TBI ± others | 5 (31) | 0 | 0 | |||
| Others | 0 | 1 (6) | 0 | |||
| GvHD prophylaxis | <0.001 | <0.001 | <0.001 | |||
| PTCY | 0 | 0 | 16 (100) | |||
| CNI—MMF ± others | 13 (81) | 15 (94) | 16 (100) | |||
| CNI—MTX ± others | 1 (6) | 0 | 0 | |||
| Sirolimus—MMF | 2 (13) | 1 (6) | 0 | |||
| Median year of transplantation | 2006 | 2008 | 2012 | |||
| MRD (1) | URD (2) | Haplo (3) | p Value | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Grade | I–II | III–IV | I–II | III–IV | I–II | III–IV | 1 vs. 3 | 2 vs. 3 | Overall |
| GI tract | |||||||||
| Mucositis | 7 (44) | 2 (13) | 6 (38) | 2 (13) | 8 (50) | 4 (25) | 0.46 | 0.32 | 0.62 |
| Nausea/vomiting | 14 (88) | 1 (6) | 12 (75) | 1 (6) | 12 (75) | 0 | 0.23 | 0.56 | 0.56 |
| Diarrhea | 12 (75) | 4 (25) | 11 (69) | 3 (19) | 12 (75) | 2 (13) | 0.26 | 0.89 | 0.61 |
| Liver | |||||||||
| Hyperbilirubinemia | 3 (19) | 2 (13) | 4 (25) | 3 (19) | 8 (50) | 1 (6) | 0.17 | 0.28 | 0.32 |
| Transient elevation of transaminases | 2 (13) | 1 (6) | 4 (25) | 2 (13) | 6 (38) | 3 (19) | 0.09 | 0.57 | 0.31 |
| Ascites | 1 (6) | 0 | 1 (6) | 0 | 2 (13) | 0 | 0.54 | 0.54 | 0.76 |
| VOD | 0 | 0 | 0 | 0 | 0 | 0 | >0.99 | >0.99 | >0.99 |
| Lung | |||||||||
| Dyspnea | 2 (13) | 3 (19) | 1 (6) | 6 (38) | 1 (6) | 1 (6) | 0.43 | 0.1 | 0.25 |
| Urogenital tract | |||||||||
| Creatinine elevation | 3 (19) | 2 (13) | 6 (38) | 1 (6) | 7 (44) | 3 (19) | 0.20 | 0.43 | 0.39 |
| Hemorrhagic cystitis | 1 (6) | 0 | 2 (13) | 0 | 6 (38) | 0 | 0.03 | 0.1 | 0.06 |
| Skin | |||||||||
| Hand–foot syndrome | 1 (6) | 0 | 0 | 0 | 0 | 0 | 0.31 | >0.99 | 0.36 |
| Rash | 1 (6) | 1 (6) | 0 | 0 | 0 | 0 | 0.34 | >0.99 | 0.38 |
| TAM | 0 | 0 | 2 (13) | 0 | 1 (6) | 0 | 0.38 | >0.99 | 0.34 |
| Cardiovascular system | |||||||||
| Arrhythmia | 0 | 3 (19) | 2 (13) | 3 (19) | 1 (6) | 1 (6) | 0.36 | 0.43 | 0.48 |
| CNS | |||||||||
| Headache | 6 (38) | 0 | 5 (31) | 0 | 0 | 0 | 0.01 | 0.02 | 0.03 |
| Confusion | 4 (25) | 2 (13) | 3 (19) | 2 (13) | 2 (13) | 1 (6) | 0.50 | 0.71 | 0.83 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haebe, S.; Fraccaroli, A.; Stauffer, E.; Prevalsek, D.; Zoellner, A.K.; Drolle, H.; Stemmler, H.-J.; Dreyling, M.; von Bergwelt-Baildon, M.; Tischer, J. PTCY-Based Haploidentical Donor Transplantation versus HLA-Matched Related and Unrelated Donor Transplantations in Patients with Refractory or Relapsed Lymphoma—A Matched-Pair Analysis. Cancers 2023, 15, 5246. https://doi.org/10.3390/cancers15215246
Haebe S, Fraccaroli A, Stauffer E, Prevalsek D, Zoellner AK, Drolle H, Stemmler H-J, Dreyling M, von Bergwelt-Baildon M, Tischer J. PTCY-Based Haploidentical Donor Transplantation versus HLA-Matched Related and Unrelated Donor Transplantations in Patients with Refractory or Relapsed Lymphoma—A Matched-Pair Analysis. Cancers. 2023; 15(21):5246. https://doi.org/10.3390/cancers15215246
Chicago/Turabian StyleHaebe, Sarah, Alessia Fraccaroli, Elena Stauffer, Dusan Prevalsek, Anna K. Zoellner, Heidrun Drolle, Hans-Joachim Stemmler, Martin Dreyling, Michael von Bergwelt-Baildon, and Johanna Tischer. 2023. "PTCY-Based Haploidentical Donor Transplantation versus HLA-Matched Related and Unrelated Donor Transplantations in Patients with Refractory or Relapsed Lymphoma—A Matched-Pair Analysis" Cancers 15, no. 21: 5246. https://doi.org/10.3390/cancers15215246
APA StyleHaebe, S., Fraccaroli, A., Stauffer, E., Prevalsek, D., Zoellner, A. K., Drolle, H., Stemmler, H.-J., Dreyling, M., von Bergwelt-Baildon, M., & Tischer, J. (2023). PTCY-Based Haploidentical Donor Transplantation versus HLA-Matched Related and Unrelated Donor Transplantations in Patients with Refractory or Relapsed Lymphoma—A Matched-Pair Analysis. Cancers, 15(21), 5246. https://doi.org/10.3390/cancers15215246