
Sport and Dental Traumatology: Surgical Solutions and Prevention





Abstract
1. Introduction
2. Dental Trauma and Injuries
2.1. Traumatic Dental Injuries (TDI)
2.2. Prevalence
2.2.1. Prevalence Contact Sports
2.2.2. Prevalence Combat Sports
2.3. Epidemiology
2.4. Teeth Involved
2.5. Etiology
3. Treatment Options
3.1. Tooth Avulsion
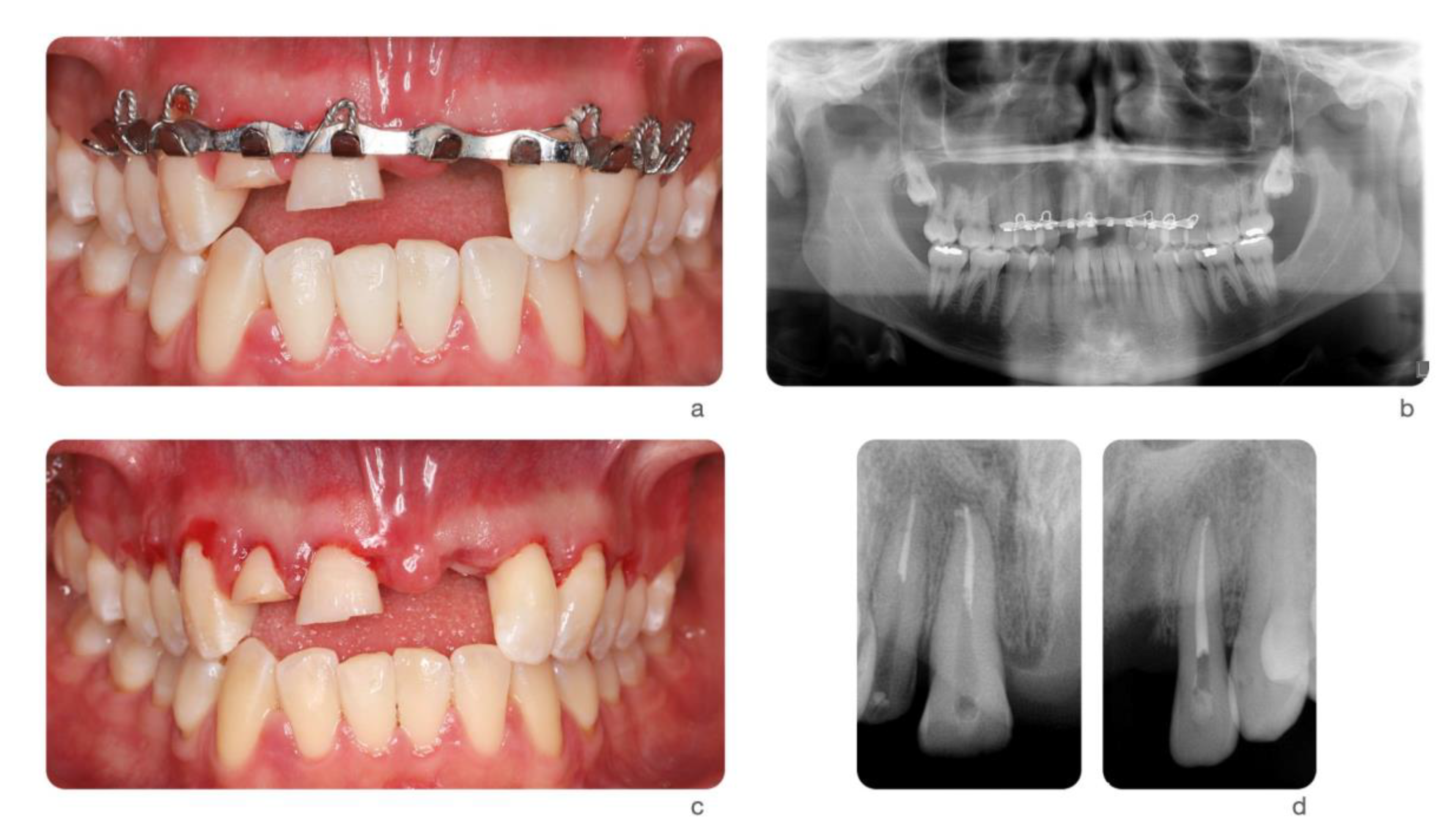
- If the tooth has already been replanted, the injured area should be cleaned with water, saline or chlorhexidine. After, the correct position of the replanted tooth should be verified clinically and radiographically. The tooth should be left in place, except if the tooth was positioned in the wrong position. In that case, it should be corrected with slight finger pressure. Local anesthesia should be administered, if necessary, and preferably with no vasoconstrictor to presence the vascularity. If the teeth were replanted in the wrong socket or rotated, the tooth should be repositioned up to 48 h after the traumatic incident. The tooth should be stabilized for 2 weeks using a passive flexible splint such as wire of a diameter up to 0.4 mm or nylon fishing line. The composite and bonding agents should leave a hygienic space, with some distance from from the gingival tissues and interproximal areas. In cases of associated alveolar fracture, a more rigid splint is indicated and should be left in place for about 4 weeks. Finally, gingival lacerations, if present, should be sutured and systemic antibiotics should be prescribed [29].
- In the other two scenarios, the root surface should be rinsed with saline or osmolality-balanced media to remove gross debris by gently agitating it in the storage medium. the socket should be irrigated with sterile saline. If there is a fracture of the socket wall, the fractured fragment should be repositioned into its original position. The removal of the coagulum with a saline stream may allow better repositioning of the tooth. the tooth should be slowly replanted with slight digital pressure [29].
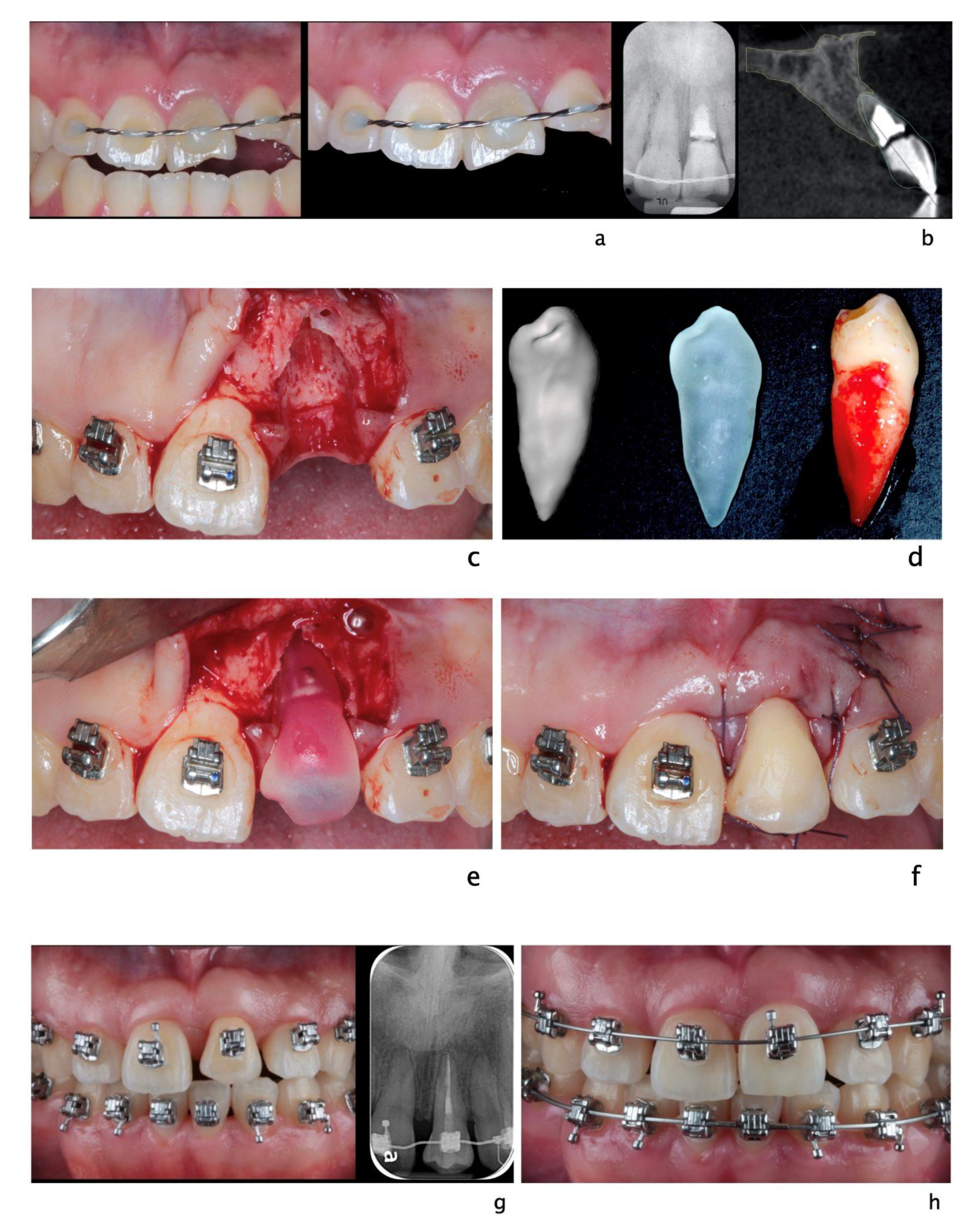
3.2. Auto-Transplantation
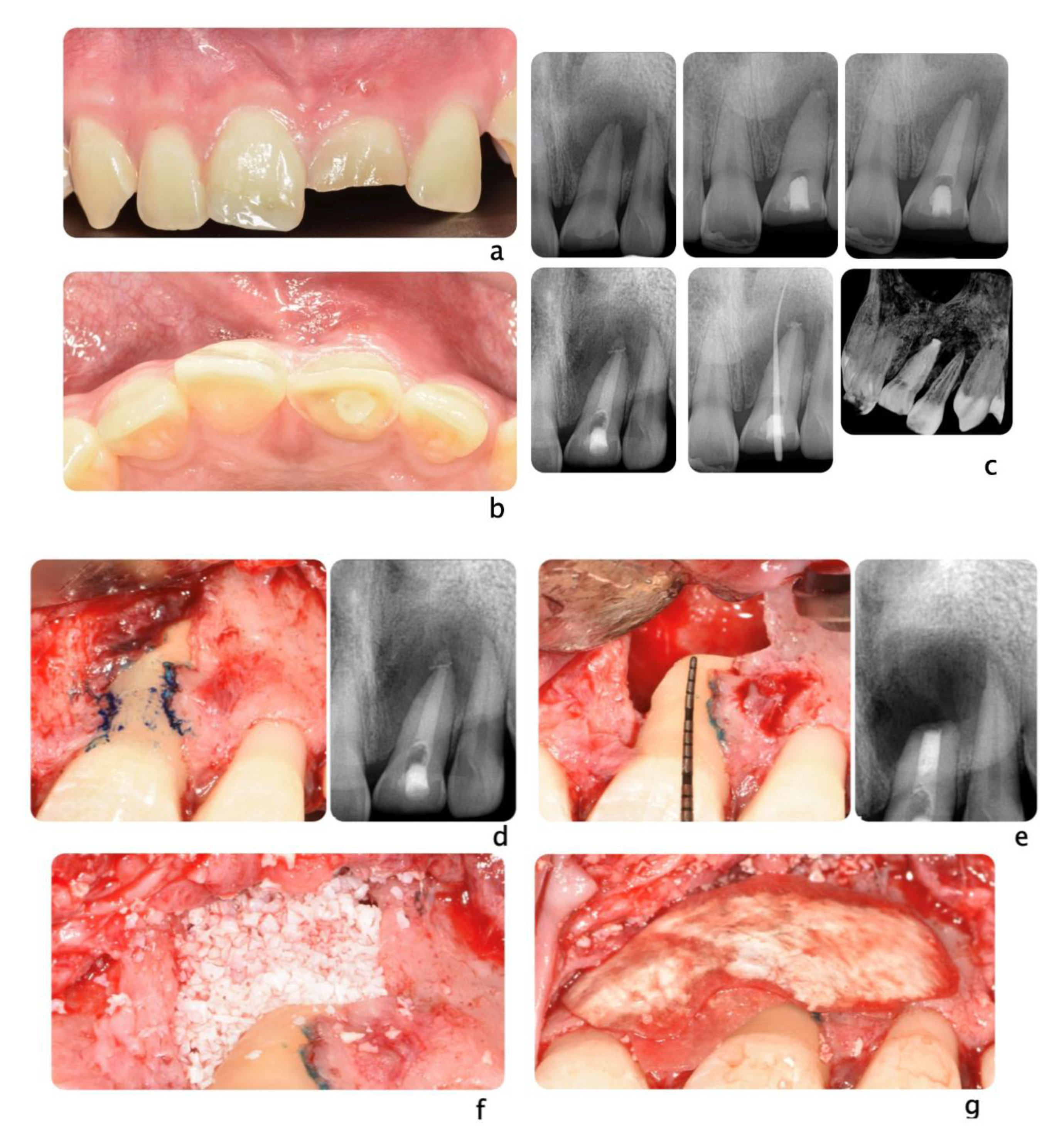
3.3. Soft and Hard Tissue Reconstruction
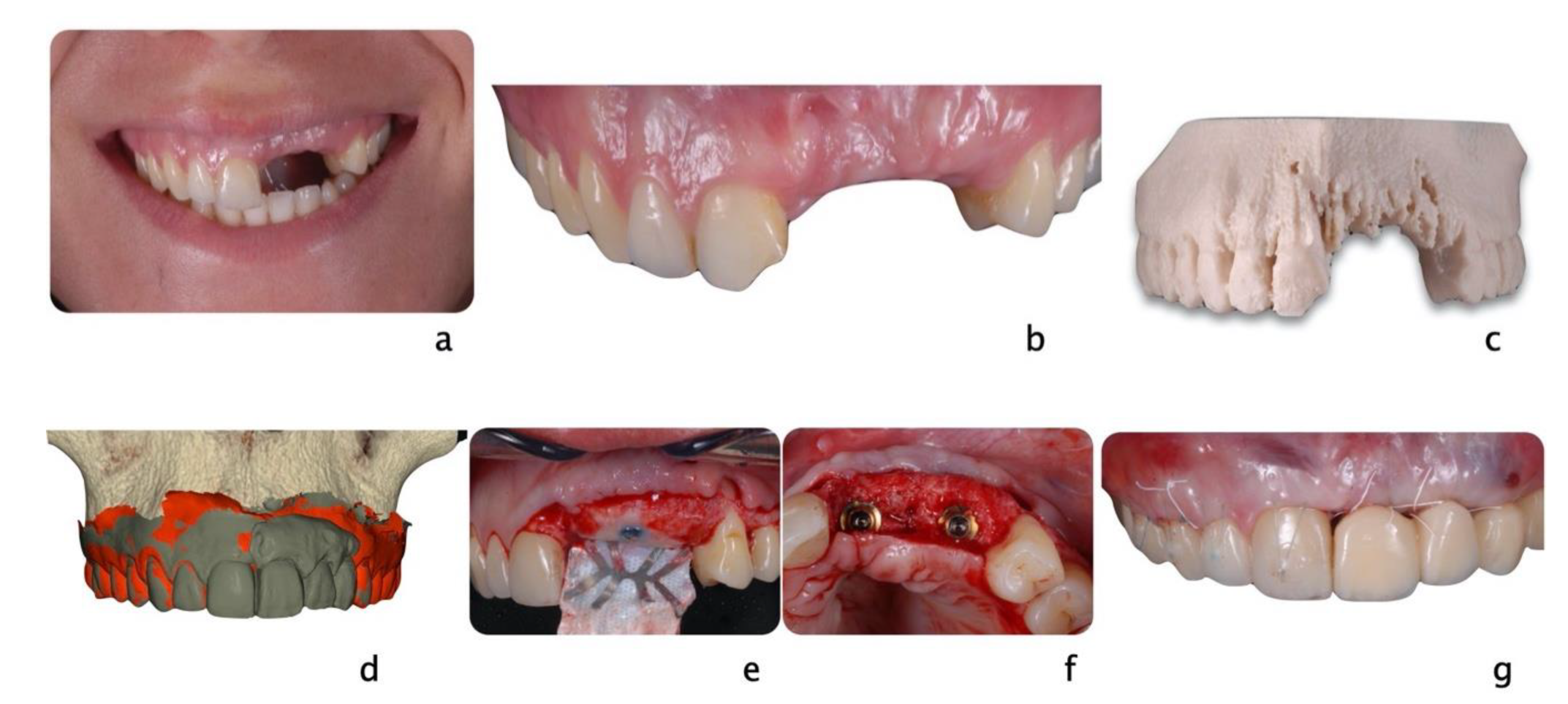
3.4. Dental Implants
- Type 1, immediate placement, no later than 24 h after tooth extraction.
- Type 2, early placement, typically 4 to 8 weeks after tooth extraction with only healed soft tissue at extraction site.
- Type 3, early placement, typically 12 to 16 weeks after tooth extraction with healed soft tissue and significant healing of alveolar bone at extraction site.
- Type 4, late placement, after 6 months with complete healing at extraction site.
3.5. Other Treatment Options
4. Prevention
Appliances to Prevent Dental Injuries
5. Discussion
6. Conclusions
- The timing or tooth replantation after a traumas is crucial. All avulsed permanent and mature teeth eventually develop pulp necrosis. When the tooth is immature and presents an open apex, further root development can be achieved.
- The advances of dental CBCT and 3D printing allow the surgeon to successfully plan and execute tooth auto transplantations. The use of printed replica significantly decreased the surgical time and increased to more than 95% the survival rates.
- The soft and hard tissue deficiencies following trauma should be re-evaluated after initial healing and stabilization. The defects then can be treated as clinical scenario requiring standard soft and hard tissue regeneration.
- If the injured is an adult, tooth/teeth loss, tooth/teeth anxylosis and auto transplantation failure may be treated with dental implants to restore the missing tooth/teeth;
- The diffusion of injuries among adolescents calls for individualized treatment based on growth and time that separates the traumatic event to final restorations. Mini-implants could be used as an interim or final restoration to replace avulsed teeth.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Injuries and Violence: The Facts 2014; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Petersson, E.E.; Andersson, L.; Sörensen, S. Traumatic Oral Vs Non-Oral Injuries. Swed. Dent. J. 1997, 21, 55–68. [Google Scholar]
- Hayter, J.P.; Ward, A.J.; Smith, E.J. Maxillofacial Trauma in Severely Injured Patients. Br. J. Oral Maxillofac. Surg. 1991, 29, 370–373. [Google Scholar] [CrossRef]
- Piccininni, P.; Clough, A.; Padilla, R.; Piccininni, G. Dental and Orofacial Injuries. Clin. Sports Med. 2017, 36, 369–405. [Google Scholar] [CrossRef] [PubMed]
- Borssén, E.; Källestål, C.; Holm, A.-K. Treatment time of traumatic dental injuries in a cohort of 16-year-olds in northern Sweden. Acta Odontologica Scandinavica 2002, 60, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Keçeci, A.D.; Eroglu, E.; Baydar, M.L. Dental trauma incidence and mouthguard use in elite athletes in Turkey. Dent. Traumatol. 2005, 21, 76–79. [Google Scholar] [CrossRef]
- Polmann, H.; Melo, G.; Conti Réus, J.; Domingos, F.L.; de Souza, B.D.M.; Padilha, A.C.; Duque, T.M.; Porporatti, A.L.; Flores-Mir, C.; De Luca Canto, G. Prevalence of Dentofacial Injuries among Combat Sports Practitioners: A Systematic Review and Meta-Analysis. Dent. Traumatol. 2020, 36, 124–140. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, L.M.; Neto, J.C.L.; Lima, T.F.; Magno, M.B.; Santiago, B.M.; Cavalcanti, Y.W.; de Almeida, L.D.F.D. The Use of Mouthguards and Prevalence of Dento-Alveolar Trauma among Athletes: A Systematic Review and Meta-Analysis. Dent. Traumatol. 2019, 35, 54–72. [Google Scholar] [CrossRef]
- Cavalleri, G.; Zerman, N. Traumatic crown fractures in permanent incisors with immature roots: A follow-up study. Dent. Traumatol. 1995, 11, 294–296. [Google Scholar] [CrossRef] [PubMed]
- Kumamoto, D.; Maeda, Y. Global Trends and Epidemiology of Sports Injuries. J. Pediatr. Dent. Care 2005, 11, 15–25. [Google Scholar]
- Reehal, P. Facial Injury in Sport. Curr. Sports Med. Rep. 2010, 9, 27–34. [Google Scholar] [CrossRef]
- Cortes, M.I.D.S.; Marcenes, W.; Sheiham, A. Impact of traumatic injuries to the permanent teeth on the oral health-related quality of life in 12-14-year-old children. Community Dent. Oral Epidemiol. 2002, 30, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, B.R.; Heckler, F.R. Sports-Related Facial Injuries. Clin. Sports Med. 1997, 16, 543–562. [Google Scholar] [CrossRef]
- Andreasen, J.O.; Andreasen, F.M.; Andersson, L. Textbook and Color. Atlas of Traumatic Injuries to the Teeth; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Levin, L.; Day, P.F.; Hicks, L.; O’Connell, A.; Fouad, A.F.; Bourguignon, C.; Abbott, P.V. International Association of Dental Traumatology Guidelines for the Management of Traumatic Dental Injuries: General Introduction. Dent. Traumatol. 2020, 36, 309–313. [Google Scholar] [CrossRef]
- Bourguignon, C.; Cohenca, N.; Lauridsen, E.; Flores, M.T.; O’Connell, A.C.; Day, P.F.; Tsilingaridis, G.; Abbott, P.V.; Fouad, A.F.; Hicks, L.; et al. International Association of Dental Traumatology Guidelines for the Management of Traumatic Dental Injuries: 1. Fractures and Luxations. Dent. Traumatol. 2020, 36, 314–330. [Google Scholar] [CrossRef]
- Oliveira Werlich, M.; Honnef, L.R.; Silva Bett, J.V.; Domingos, F.L.; Pauletto, P.; Dulcineia Mendes de Souza, B.; Duque, T.M.; Curi Hallal, A.L.; De Luca Canto, G. Prevalence of Dentofacial Injuries in Contact Sports Players: A Systematic Review and Meta-Analysis. Dent. Traumatol. 2020, 36, 477–488. [Google Scholar] [CrossRef] [PubMed]
- Association, American Dental. Using Mouthguards to Reduce the Incidence and Severity of Sports-Related Oral Injuries. J. Am. Dent. Assoc. 2006, 137, 1712–1720. [Google Scholar] [CrossRef]
- For the Dental Patient. The Importance of Using Mouthguards. Tips for Keeping Your Smile Safe. J. Am. Dent. Assoc. 2004, 135, 1061. [Google Scholar] [CrossRef]
- NFHS. Position Statement and Recommendations for Mouthguard Use in Sport; National Federation of State High School Associations: Indianapolis, IN, USA, 2018. [Google Scholar]
- Schneider, S.; Seither, B.; Tönges, S.; Schmitt, H. Sports Injuries: Population Based Representative Data on Incidence, Diagnosis, Sequelae, and High Risk Groups. Br. J. Sports Med. 2006, 40, 334–339. [Google Scholar] [CrossRef] [PubMed]
- Zaleckiene, V.; Peciuliene, V.; Brukiene, V.; Drukteinis, S. Traumatic Dental Injuries: Etiology, Prevalence and Possible Outcomes. Stomatologija 2014, 16, 7–14. [Google Scholar]
- Navabazam, A.; Farahani, S.S. Prevalence of Traumatic Injuries to Maxillary Permanent Teeth in 9- to 14-Year-Old School Children in Yazd, Iran. Dent. Traumatol. 2010, 26, 154–157. [Google Scholar] [CrossRef]
- Traebert, J.; Bittencourt, D.D.; Peres, K.G.; Peres, M.A.; De Lacerda, J.T.; Marcenes, W. Aetiology and Rates of Treatment of Traumatic Dental Injuries among 12-Year-Old School Children in a Town in Southern Brazil. Dent. Traumatol. 2006, 22, 173–178. [Google Scholar] [CrossRef]
- Scott, N.; Hughes, J.; Forbes-Haley, C.; East, C.; Holmes, S.; Wilson, E.; Ball, S.; Hammond, D.; Drake, D.; Hutchison, I.; et al. Management of Facial Injuries in Elite and Professional Sports—A Consensus Report. Br. J. Oral Maxillofac. Surg. 2020, 58, e254–e259. [Google Scholar] [CrossRef] [PubMed]
- Trope, M. Clinical Management of the Avulsed Tooth: Present Strategies and Future Directions. Dent. Traumatol. 2002, 18, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, J.O.; Borum, M.K.; Jacobsen, H.L.; Andreasen, F.M. Replantation of 400 avulsed permanent incisors. 4. Factors related to periodontal ligament healing. Dent. Traumatol. 1995, 11, 76–89. [Google Scholar] [CrossRef] [PubMed]
- Kinirons, M.J.; Gregg, T.A.; Welbury, R.R.; Cole, B.O.I. Variations in the Presenting and Treatment Features in Reimplanted Permanent Incisors in Children and Their Effect on the Prevalence of Root Resorption. Br. Dent. J. 2000, 189, 263–266. [Google Scholar] [CrossRef] [PubMed]
- Fouad, A.F.; Abbott, P.V.; Tsilingaridis, G.; Cohenca, N.; Lauridsen, E.; Bourguignon, C.; O’Connell, A.; Flores, M.T.; Day, P.F.; Hicks, L.; et al. International Association of Dental Traumatology Guidelines for the Management of Traumatic Dental Injuries: 2. Avulsion of Permanent Teeth. Dent. Traumatol. 2020, 36, 331–342. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Zuckerman, O.; Fuss, Z.; Ashkenazi, M. New Emphasis in the Treatment of Dental Trauma: Avulsion and Luxation. Dent. Traumatol. 2007, 23, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Schröder, U.; Granath, L.E. Early Reaction of Intact Human Teeth to Calcium Hydroxide Following Experimental Pulpotomy and Its Significance to the Development of Hard Tissue Barrier. Odont Revy 1971, 22, 379–395. [Google Scholar]
- Moule, A.J.; Moule, C.A. The Endodontic Management of Traumatized Permanent Anterior Teeth: A Review. Aust. Dent. J. 2007, 52 (Suppl. 1), S122–S137. [Google Scholar] [CrossRef]
- Slagsvold, O.; Bjercke, B. Indications for Autotransplantation in Cases of Missing Premolars. Am. J. Orthod. 1978, 74, 241–257. [Google Scholar] [CrossRef]
- Machado, L.A.; Do Nascimento, R.R.; Ferreira DM, T.P.; Mattos, C.T.; Vilella, O.V. Long-Term Prognosis of Tooth Autotransplantation: A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Surg. 2016, 45, 610–617. [Google Scholar] [CrossRef]
- Akhlef, Y.; Schwartz, O.; Andreasen, J.O.; Jensen, S.S. Autotransplantation of Teeth to the Anterior Maxilla: A Systematic Review of Survival and Success, Aesthetic Presentation and Patient-Reported Outcome. Dent. Traumatol. 2018, 34, 20–27. [Google Scholar] [CrossRef]
- Atala-Acevedo, C.; Abarca, J.; Martínez-Zapata, M.J.; Díaz, J.; Olate, S.; Zaror, C. Success Rate of Autotransplantation of Teeth With an Open Apex: Systematic Review and Meta-Analysis. J. Oral Maxillofac. Surg. 2017, 75, 35–50. [Google Scholar] [CrossRef]
- Chung, W.-C.; Tu, Y.-K.; Lin, Y.-H.; Lu, H.-K. Outcomes of autotransplanted teeth with complete root formation: A systematic review and meta-analysis. J. Clin. Periodontol. 2014, 41, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Verweij, J.; Jongkees, F.; Moin, D.A.; Wismeijer, D.; Van Merkesteyn, J. Autotransplantation of teeth using computer-aided rapid prototyping of a three-dimensional replica of the donor tooth: A systematic literature review. Int. J. Oral Maxillofac. Surg. 2017, 46, 1466–1474. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.L.; Wong, T.L.T.; Wong, M.C.M.; Lang, N.P. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin. Oral Implant. Res. 2011, 23, 1–21. [Google Scholar] [CrossRef]
- Elnayef, B.; Porta, C.; Del Amo, F.S.-L.; Mordini, L.; Gargallo-Albiol, J.; Hernández-Alfaro, F. The Fate of Lateral Ridge Augmentation: A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Implant. 2018, 33, 622–635. [Google Scholar] [CrossRef] [PubMed]
- Mordini, L.; Hur, Y.; Ogata, Y.; Finkelman, M.; Cavani, F.; Steffensen, B. Volumetric Changes Following Lateral Guided Bone Regeneration. Int. J. Oral Maxillofac. Implant. 2020, 35, e77–e85. [Google Scholar] [CrossRef] [PubMed]
- Elnayef, B.; Monje, A.; Gargallo-Albiol, J.; Galindo-Moreno, P.; Wang, H.L.; Hernandez-Alfaro, F. Vertical Ridge Augmentation in the Atrophic Mandible: A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Implant. 2017, 32, 291–312. [Google Scholar] [CrossRef]
- Yu, C.Y.; Abbott, P.V. Responses of the pulp, periradicular and soft tissues following trauma to the permanent teeth. Aust. Dent. J. 2016, 61 (Suppl. S1), 39–58. [Google Scholar] [CrossRef] [PubMed]
- Barootchi, S.; Tavelli, L.; Dds, G.Z.; Giannobile, W.V.; Wang, H. Gingival phenotype modification therapies on natural teeth: A network meta-analysis. J. Periodontol. 2020, 91, 1386–1399. [Google Scholar] [CrossRef]
- Hämmerle, C.H.F.; Chen, S.T.; Wilson, T.G. Consensus statements and recommended clinical procedures regarding the placement of implants in extraction sockets. Int. J. Oral Maxillofac. Implant. 2004, 19 (Suppl. S2004), 26–28. [Google Scholar]
- Bassir, S.H.; El Kholy, K.; Chen, C.-Y.; Lee, K.H.; Intini, G. Outcome of early dental implant placement versus other dental implant placement protocols: A systematic review and meta-analysis. J. Periodontol. 2018, 90, 493–506. [Google Scholar] [CrossRef]
- Chen, S.T.; Wilson, T.G.; Hämmerle, C.H.F. Immediate or early placement of implants following tooth extraction: Review of biologic basis, clinical procedures, and outcomes. Int. J. Oral Maxillofac. Implant. 2004, 19, 12–25. [Google Scholar]
- Morton, D.; Chen, S.T.; Martin, W.C.; Levine, R.A.; Buser, D. Consensus Statements and Recommended Clinical Procedures Regarding Optimizing Esthetic Outcomes in Implant Dentistry. Int. J. Oral Maxillofac. Implant. 2014, 29, 216–220. [Google Scholar] [CrossRef]
- Bohner, L.; Hanisch, M.; Kleinheinz, J.; Jung, S. Dental implants in growing patients: A systematic review. Br. J. Oral Maxillofac. Surg. 2019, 57, 397–406. [Google Scholar] [CrossRef]
- Bernard, J.P.; Schatz, J.P.; Christou, P.; Belser, U.; Kiliaridis, S. Long-Term Vertical Changes of the Anterior Maxillary Teeth Adjacent to Single Implants in Young and Mature Adults. A Retrospective Study. J. Clin. Periodontol. 2004, 31, 1024–1028. [Google Scholar] [CrossRef] [PubMed]
- Thilander, B.; Ödman, J.; Lekholm, U. Orthodontic Aspects of the Use of Oral Implants in Adolescents: A 10-Year Follow-up Study. Eur. J. Orthod. 2001, 23, 715–731. [Google Scholar] [CrossRef]
- Schwartz-Arad, D.; Bichacho, N. Effect of Age on Single Implant Submersion Rate in the Central Maxillary Incisor Region: A Long-Term Retrospective Study. Clin. Implant. Dent. Relat. Res. 2013, 17, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Fudalej, P.; Kokich, V.G.; Leroux, B. Determining the Cessation of Vertical Growth of the Craniofacial Structures to Facilitate Placement of Single-Tooth Implants. Am. J. Orthod. Dentofacial Orthop. 2007, 131, S59–S67. [Google Scholar] [CrossRef] [PubMed]
- Jensen, S.S. Timing of Implant Placement after Traumatic Dental Injury. J. Endod. 2019, 45, S52–S56. [Google Scholar] [CrossRef]
- Verma, D.; Peltomäki, T.; Jäger, A. Reliability of growth prediction with hand-wrist radiographs. Eur. J. Orthod. 2009, 31, 438–442. [Google Scholar] [CrossRef]
- Flores-Mir, C.; Nebbe, B.; Major, P.W. Use of Skeletal Maturation Based on Hand-Wrist Radiographic Analysis as a Predictor of Facial Growth: A Systematic Review. Angle Orthod. 2004, 74, 118–124. [Google Scholar] [PubMed]
- Giannetti, L.; Apponi, R.; Diago, A.M.D.; Mintrone, F. Rehabilitation of a patient with mini-implants after avulsion of the upper incisors: A 13-year follow up. Dent. Traumatol. 2021, 37, 354–359. [Google Scholar] [CrossRef] [PubMed]
- Murri dello Diago, A.; Apponi, R.; Colombini, V.; Mordini, L.; Ideo, F. Complex Implant-Prosthetic Rehabilitation Following Sports Trauma with 14 Years of Follow-Up: Case Report. Dent. J. 2021, 9, 6. [Google Scholar] [CrossRef] [PubMed]
- Giannetti, L.; Murri Dello Diago, A.; Vecci, F.; Consolo, U. Mini-Implants in Growing Patients: A Case Report. Pediatr. Dent. 2010, 32, 239–244. [Google Scholar] [PubMed]
- Jung, R.E.; Al-Nawas, B.; Araujo, M.; Avila-Ortiz, G.; Barter, S.; Brodala, N.; Chappuis, V.; Chen, B.; De Souza, A.; Almeida, R.F.; et al. Group 1 Iti Consensus Report: The Influence of Implant Length and Design and Medications on Clinical and Patient-Reported Outcomes. Clin. Oral Implants Res. 2018, 29 (Suppl. S16), 69–77. [Google Scholar] [CrossRef]
- Bidra, A.S.; Almas, K. Mini implants for definitive prosthodontic treatment: A systematic review. J. Prosthet. Dent. 2013, 109, 156–164. [Google Scholar] [CrossRef]
- Garon, M.W.; Merkle, A.; Wright, J.T. Mouth protectors and oral trauma: A study of adolescent football players. J. Am. Dent. Assoc. 1986, 112, 663–665. [Google Scholar] [CrossRef]
- Bergman, L.; Milardović Ortolan, S.; Žarković, D.; Viskić, J.; Jokić, D.; Mehulić, K. Prevalence of Dental Trauma and Use of Mouthguards in Professional Handball Players. Dent. Traumatol. 2017, 33, 199–204. [Google Scholar] [CrossRef]
- Tuna, E.B.; Ozel, E. Factors Affecting Sports-Related Orofacial Injuries and the Importance of Mouthguards. Sports Med. 2014, 44, 777–783. [Google Scholar] [CrossRef]
- Reed, R.V. Origin and early history of the dental mouthpiece. Br. Dent. J. 1994, 176, 478–480. [Google Scholar] [CrossRef] [PubMed]
- Biasca, N.; Wirth, S.; Tegner, Y. The avoidability of head and neck injuries in ice hockey: An historical review. Br. J. Sports Med. 2002, 36, 410–427. [Google Scholar] [CrossRef]
- Knapik, J.J.; Hoedebecke, B.L.; Rogers, G.G.; Sharp, M.A.; Marshall, S.W. Effectiveness of Mouthguards for the Prevention of Orofacial Injuries and Concussions in Sports: Systematic Review and Meta-Analysis. Sports Med. 2019, 49, 1217–1232. [Google Scholar] [CrossRef]
- Labella, C.R.; Smith, B.W.; Sigurdsson, A. Effect of Mouthguards on Dental Injuries and Concussions in College Basketball. Med. Sci. Sports Exerc. 2002, 34, 41–44. [Google Scholar] [CrossRef]
- Blignaut, J.B.; Carstens, I.L.; Lombard, C.J. Injuries sustained in rugby by wearers and non-wearers of mouthguards. Br. J. Sports Med. 1987, 21, 5–7. [Google Scholar] [CrossRef] [PubMed]
- Guerard, S.; Barou, J.-L.; Petit, J.; Poisson, P. Characterization of mouthguards: Impact performance. Dent. Traumatol. 2017, 33, 281–287. [Google Scholar] [CrossRef]
- Newsome, P.R.H.; Tran, D.C.; Cooke, M.S. The role of the mouthguard in the prevention of sports-related dental injuries: A review. Int. J. Paediatr. Dent. 2001, 11, 396–404. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, A.; Takahashi, T.; Kurokawa, K.; Mitsuyama, A.; Hayashi, K.; Ishigami, T.; Shahrin, S.; Chowdhury, R.; Churei, H.; Ueno, T. Effects of Mouthguards on Electromyographic Activity of Masticatory Muscles. Int. J. Sports Dent. 2016, 9, 27–37. [Google Scholar]
- Spinas, E.; Mameli, A.; Giannetti, L. Traumatic Dental Injuries Resulting from Sports Activities; Immediate Treatment and Five Years Follow-Up: An Observational Study. Open Dent. J. 2018, 12, 1–10. [Google Scholar] [CrossRef]
- McClelland, C.; Kinirons, M.; Geary, L. A preliminary study of patient comfort associated with customised mouthguards. Br. J. Sports Med. 1999, 33, 186–189. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, J.D.; Nakamura, W.S.; Maeda, Y.; Takeda, T.; Leesungbok, R.; Lazarchik, D.; Dorney, B.; Gonda, T.; Nakajima, K.; Yasui, T.; et al. Mouthguards and Their Use in Sports: Report of the 1st International Sports Dentistry Workshop, 2016. Dent. Traumatol. 2017, 33, 421–426. [Google Scholar] [CrossRef]
- Gómez-Gimeno, À.; Zamora-Olave, C.; Cordobés-Navarro, M.; Willaert, E.; Martinez-Gomis, J. Satisfaction with shortening the palatal extension of a mouthguard for water polo players: A randomized crossover study. Dent. Traumatol. 2019, 35, 135–141. [Google Scholar] [CrossRef]
- Zamora-Olave, C.; Willaert, E.; Parera, L.; Riera-Puñet, N.; Martinez-Gomis, J. Experience with Mouthguards and Prevalence of Orofacial Injuries among Field Hockey Players in Catalonia. Dent. Traumatol. 2020, 36, 285–290. [Google Scholar] [CrossRef] [PubMed]
- Spinas, E.; Aresu, M.; Giannetti, L. Use of Mouth Guard in Basketball: Observational Study of a Group of Teenagers with and without Motivational Reinforcement. Eur. J. Paediatr. Dent. 2014, 15, 392–396. [Google Scholar] [PubMed]
- Spinas, E.; Giannetti, L.; Mameli, A.; Re, D. Dental Injuries in Young Athletes, a Five-Year Follow-up Study. Eur. J. Paediatr. Dent. 2018, 19, 187–193. [Google Scholar] [PubMed]
- Bastian, N.E.; Heaton, L.J.; Capote, R.T.; Wan, Q.; Riedy, C.A.; Ramsay, D.S. Mouthguards During Orthodontic Treatment: Perspectives of Orthodontists and a Survey of Orthodontic Patients Playing School-Sponsored Basketball and football. Am. J. Orthod. Dentofac. Orthop. 2020, 157, 516–525. [Google Scholar] [CrossRef]
- American Dental Association. Orofacial Protectors; ADA: New York, NY, USA, 2016; p. 181. [Google Scholar]
- Bister, D. The SAC classification in implant dentistry (2009). Eur. J. Orthod. 2009, 31, 564. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TDI | Definition | |
|---|---|---|
| Uncomplicated crown fractures | Enamel infraction | An incomplete fracture (crack or crazing) of the enamel, without loss of tooth structure |
| Enamel fracture | A coronal fracture involving enamel only, with loss of tooth structure | |
| Enamel/dentin fracture | A fracture confined to enamel and dentin without pulp exposure | |
| Complicated crown fractures | Enamel/dentin fracture with pulp exposure | A fracture confined to enamel and dentin with pulp exposure |
| Crown/root fracture | UNCOMPLICATED (WITHOUT PULP EXPOSURE) A fracture involving enamel, dentin, and cementum (note: crown-root fractures typically extend below the gingival margin) COMPLICATED (WITH PULP EXPOSURE) A fracture involving enamel, dentin, cementum, and the pulp (note: crown-root fractures typically extend below the gingival margin) | |
| Root fractures | A fracture of the root involving dentin, pulp and cementum. The fracture may be horizontal, oblique or a combination of both | |
| Alveolar fracture | The fracture involves the alveolar bone and may extend to adjacent bones | |
| Concussion | An injury to the tooth-supporting structures without abnormal loosening or displacement of the tooth, but with marked reaction to percussion | |
| Subluxation | An injury to the tooth-supporting structures with abnormal loosening, but without displacement of the tooth | |
| Luxation | Extrusion | Displacement of the tooth out of its socket in an incisal/axial direction |
| Lateral luxation | Displacement of the tooth in any lateral direction, usually associated with a fracture or compression of the alveolar socket wall or facial cortical bone | |
| Intrusion | Displacement of the tooth in an apical direction into the alveolar bone | |
| Avulsion | Complete displacement of the tooth out of its socket | |
| Cause | N Subjects | Prevalence | 95% CI | N Studies |
|---|---|---|---|---|
| Primary and permanent teeth | ||||
| Sports | 13,534 | 12.5% | 8.2%–17.7% | 21 |
| Physical activity | 10,481 | 19.45% | 12.6%–27.3% | 15 |
| Permanent teeth | ||||
| Sports | 4811 | 12.9% | 8.3%–18.3% | 14 |
| Physical activity | 2948 | 20.8% | 14.0%–28.6% | 8 |
| Primary teeth | ||||
| Sports | 1281 | 5.8% | 3.2%–9.2% | 6 |
| Physical activity | 1755 | 11.6% | 2.8%–25.4% | 9 |
| PERMANENT DENTITION | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Follow-Up Regimens | Treatment | ||||||||||||
| Avulsion | TDI | 1 W | 2 W | 4 W | 6–8 W | 3 M | 4 M | 6 M | 1 Y | Yearly (at Least 5 y) | Tooth replanted at the site of injury or before the patient’s arrival at the dental clinic |
| Extra-oral dry time > 60 min |
| Common treatment for mature and immature teeth |
|
|
| ||||||||||
| Avulsion (immature tooth) | S R | R | R | R | R | R | R | Initiate RCT within 2 weeks after replantation | |||||
| Avulsion (mature tooth) | S R | R | R | R | R | R | Pulp revascularization, which can lead to further root development, is the goal when replanting immature teeth in children. The risk of external root resorption should be weighed against the chances of revascularization. If spontaneous revascularization does not occur, apexification, pulp revitalization/ revascularization, or root canal treatment should be initiated as soon as pulp necrosis and infection is identified | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mordini, L.; Lee, P.; Lazaro, R.; Biagi, R.; Giannetti, L. Sport and Dental Traumatology: Surgical Solutions and Prevention. Dent. J. 2021, 9, 33. https://doi.org/10.3390/dj9030033
Mordini L, Lee P, Lazaro R, Biagi R, Giannetti L. Sport and Dental Traumatology: Surgical Solutions and Prevention. Dentistry Journal. 2021; 9(3):33. https://doi.org/10.3390/dj9030033
Chicago/Turabian StyleMordini, Lorenzo, Po Lee, Ricardo Lazaro, Roberto Biagi, and Luca Giannetti. 2021. "Sport and Dental Traumatology: Surgical Solutions and Prevention" Dentistry Journal 9, no. 3: 33. https://doi.org/10.3390/dj9030033
APA StyleMordini, L., Lee, P., Lazaro, R., Biagi, R., & Giannetti, L. (2021). Sport and Dental Traumatology: Surgical Solutions and Prevention. Dentistry Journal, 9(3), 33. https://doi.org/10.3390/dj9030033