Melphalan, Etoposide, and Carboplatin Megatherapy with Autologous Stem Cell Transplantation in Children with Relapsing or Therapy-Resistant Extracranial Germ-Cell Tumors—A Retrospective Analysis

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Patient and Chemotherapy Characteristics
2.2. High-Dose Chemotherapy with Autologous Stem Cell Transplantation
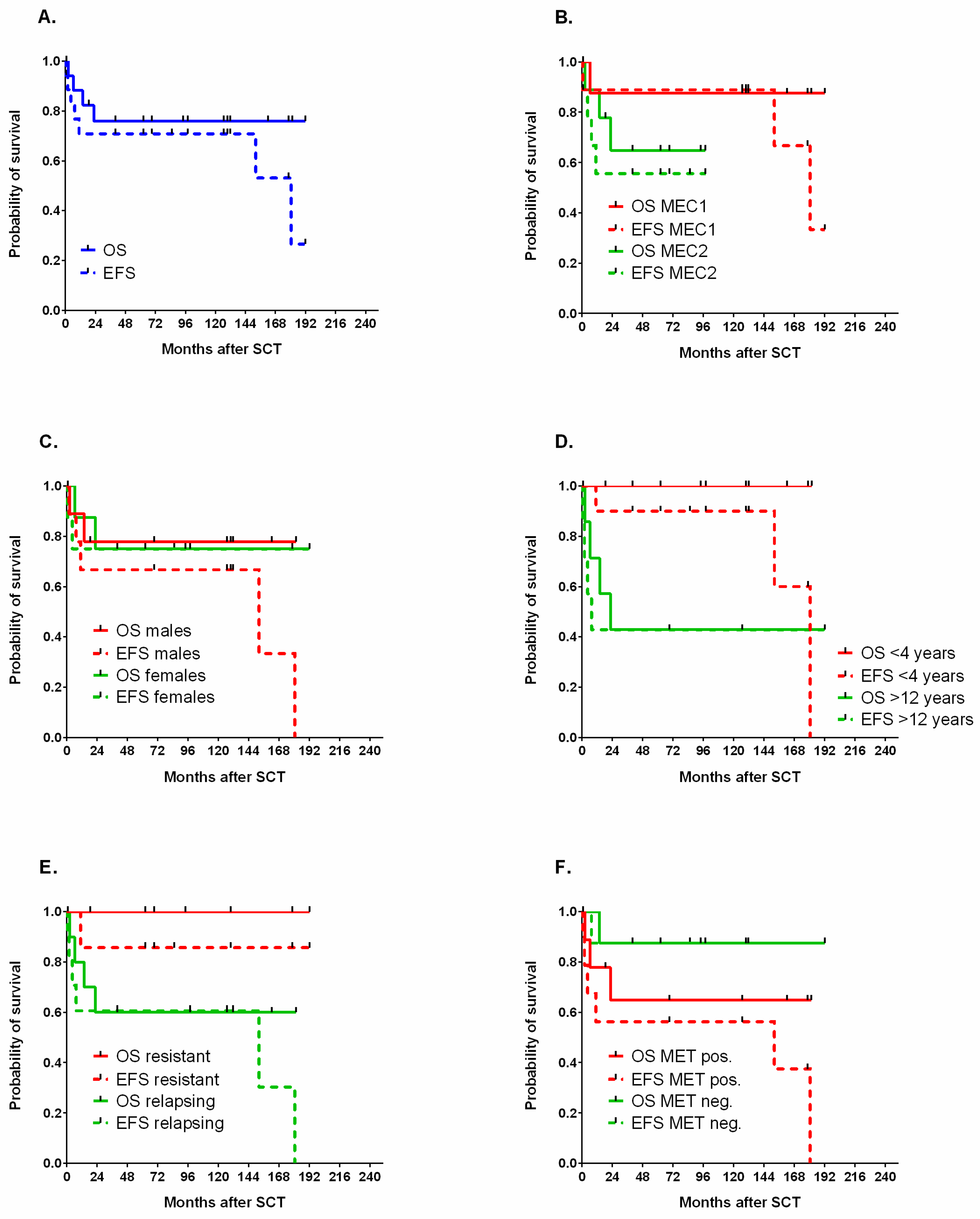
2.3. Survival Analysis
3. Discussion
4. Methods
4.1. Study Population
4.2. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lorch, A.; Mollevi, C.; Kramar, A.; Einhorn, L.H.; Necchi, A.; Massard, C.; Degiorgi, U.; Flechon, A.; Margolin, K.A.; Beyer, J.; et al. Conventional-dose versus high-dose chemotherapy in relapsed or refractory male germ-cell tumors: A retrospective study in 1,594 patients. J. Clin. Oncol. 2010, 28, 4513. [Google Scholar] [CrossRef]
- Feldman, D.R.; Sheinfeld, J.; Bajorin, D.F.; Fischer, P.; Turkula, S.; Ishill, N.; Patil, S.; Bains, M.; Reich, L.M.; Bosl, G.J.; et al. TI-CE High-Dose Chemotherapy for Patients With Previously Treated Germ Cell Tumors: Results and Prognostic Factor Analysis. J. Clin. Oncol. 2010, 28, 1706–1713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adra, N.; Abonour, R.; Althouse, S.K.; Albany, C.; Hanna, N.H.; Einhorn, L.H. High-Dose Chemotherapy and Autologous Peripheral-Blood Stem-Cell Transplantation for Relapsed Metastatic Germ Cell Tumors: The Indiana University Experience. J. Clin. Oncol. 2017, 35, 1096–1102. [Google Scholar] [CrossRef] [PubMed]
- Common Terminology Criteria for Adverse Events (CTCAE) v5.0. Available online: https://ctep.cancer.gov/protocolDevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_8.5x11.pdf (accessed on 6 November 2020).
- Popadiuk, S.; Korzon, M.; Chybicka, A.; Szmyd, K.; Balwierz, W.; Trelinska, J.; Kowalczyk, J.; Wisniewska-Slusarz, H.; Woźniak, W.; Bilska, K.; et al. Analysis of risk factor treatment failures in therapeutic programme for malignant germ cell tumours in children. Multicentre prospective study of Polish Pediatric Group for Solid Tumours 1998–2006. Med. Wieku Rozw. 2008, 11, 301–306. [Google Scholar]
- Popadiuk, S.; Korzon, M.; Szumera, M.; Chybicka, A.; Szmyd, K.; Dzierzega, M.; Kowalczyk, J.R.; Wiśniewska-Slusarz, H.; Trelińska, J.; Wozniak, W.; et al. Malignant germ cell tumours. Multicenter prospective trial in Polish Pediatric Group for Solid Tumours (years 1998–2000). Prz. Lek. 2004, 2, 29–32. [Google Scholar]
- De Corti, F.; Sarnacki, S.; Patte, C.; Mosseri, V.; Baranzelli, M.C.; Martelli, H.; Conter, C.; Frappaz, D.; Orbach, D. Prognosis of malignant sacrococcygeal germ cell tumours according to their natural history and surgical management. Surg. Oncol. 2012, 21, e31–e37. [Google Scholar] [CrossRef] [PubMed]
- Drozyńska, E.; Połczyńska, K.; Popadiuk, S.; Niedzwiecki, M.; Wiśniewski, J.; Balcerska, A.; Izycka-Swieszewska, E.; Bilska, K.; Balwierz, W.; Chełmecka, L.; et al. Characteristics of extracranial malignant germ cell tumours in two age groups of children (0–10 and 10–18 years). Multicentre experiences. Med. Wieku Rozw. 2011, 15, 16–24. Available online: http://www.ncbi.nlm.nih.gov/pubmed/21786508 (accessed on 16 December 2020).
- De Bénazé, G.D.; Pacquement, H.; Conter, C.F.; Patte, C.; Orbach, D.; Corradini, N.; Berger, C.; Sudour-Bonnange, H.; Vérité, C.; Martelli, H.; et al. Paediatric dysgerminoma: Results of three consecutive French germ cell tumours clinical studies (TGM-85/90/95) with late effects study. Eur. J. Cancer 2018, 91, 30–37. [Google Scholar] [CrossRef]
- Oing, C.; Seidel, C.; Von Amsberg, G.; Oechsle, K.; Bokemeyer, C. Pharmacotherapeutic treatment of germ cell tumors: Standard of care and recent developments. Expert Opin. Pharm. 2015, 17, 545–560. [Google Scholar] [CrossRef]
- Riaz, I.B.; Umar, M.; Zahid, U.; Husnain, M.; Iftikhar, A.; McBride, A.; Bilal, J.; Javed, A.; Akbar, S.; Singh, P.; et al. Role of one, two and three doses of high-dose chemotherapy with autologous transplantation in the treatment of high-risk or relapsed testicular cancer: A systematic review. Bone Marrow Transpl. 2018, 53, 1242–1254. [Google Scholar] [CrossRef] [Green Version]
- Nichols, C.R.; Tricot, G.; Williams, S.D.; Van Besien, K.; Loehrer, P.J.; Roth, B.J.; Akard, L.; Hoffman, R.; Goulet, R.; Wolff, S.N. Dose-intensive chemotherapy in refractory germ cell cancer--a phase I/II trial of high-dose carboplatin and etoposide with autologous bone marrow transplantation. J. Clin. Oncol. 1989, 7, 932–939. [Google Scholar] [CrossRef] [PubMed]
- Feldman, D.R.; Huddart, R.; Hall, E.; Beyer, J.; Powles, T. Is High Dose Therapy Superior to Conventional Dose Therapy as Initial Treatment for Relapsed Germ Cell Tumors? The TIGER Trial. J. Cancer 2011, 2, 374–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conter, C.F.; Orbach, D.; Cropet, C.; Baranzelli, M.C.; Martelli, H.; Thebaud, E.; Vérité, C.; Rome, A.; Fasola, S.; Corradini, N.; et al. Salvage therapy for refractory or recurrent pediatric germ cell tumors: The french SFCE experience. Pediatr. Blood Cancer 2014, 61, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Pico, J.-L.; Rosti, G.; Kramar, A.; Wandt, H.; Koza, V.; Salvioni, R.; Theodore, C.; Lelli, G.; Siegert, W.; Horwich, A.; et al. A randomised trial of high-dose chemotherapy in the salvage treatment of patients failing first-line platinum chemotherapy for advanced germ cell tumours. Ann. Oncol. 2005, 16, 1152–1159. [Google Scholar] [CrossRef]
- Finlay, J.L.; Goldman, S.; Wong, M.C.; Cairo, M.; Garvin, J.; August, C.; Cohen, B.H.; Stanley, P.; Zimmerman, R.A.; Bostrom, B.; et al. Pilot study of high-dose thiotepa and etoposide with autologous bone marrow rescue in children and young adults with recurrent CNS tumors. The Children’s Cancer Group. J. Clin. Oncol. 1996, 14, 2495–2503. [Google Scholar] [CrossRef]
- Pashankar, F.D.; Frazier, A.L.; Krailo, M.; Xia, C.; Pappo, A.S.; Malogolowkin, M.; A Olson, T.; Rodriguez-Galindo, C. Treatment of refractory germ cell tumors in children with paclitaxel, ifosfamide, and carboplatin: A report from the Children’s Oncology Group AGCT0521 study. Pediatr. Blood Cancer 2018, 65, e27111. [Google Scholar] [CrossRef]
- De Pasquale, M.D.; D’Angelo, P.; Crocoli, A.; Boldrini, R.; Conte, M.; Bisogno, G.; Spreafico, F.; Inserra, A.; Biasoni, D.; Dall’Igna, P.; et al. Salvage treatment for children with relapsed/refractory germ cell tumors: The Associazione Italiana Ematologia Oncologia Pediatrica (AIEOP) experience. Pediatr. Blood Cancer 2019, 67, e28125. [Google Scholar] [CrossRef]
- Nieto, Y.; Vaughan, W.P. Pharmacokinetics of high-dose chemotherapy. Bone Marrow Transpl. 2004, 33, 259–269. [Google Scholar] [CrossRef] [Green Version]
- Shaw, P.J.; E Nath, C.; Lazarus, H.M. Not too little, not too much—Just right! (Better ways to give high dose melphalan). Bone Marrow Transpl. 2014, 49, 1457–1465. [Google Scholar] [CrossRef] [Green Version]
- Tricot, G.; Alberts, D.S.; Johnson, C.; Roe, D.J.; Dorr, R.T.; Bracy, D.; Vesole, D.H.; Jagannath, S.; Meyers, R.; Barlogie, B. Safety of autotransplants with high-dose melphalan in renal failure: A pharmacokinetic and toxicity study. Clin. Cancer Res. 1996, 2, 947–952. [Google Scholar]
- Pinguet, F.; Martel, P.; Fabbro, M.; Petit, I.; Canal, P.; Culine, S.; Astre, C.; Bressolle, F. Pharmacokinetics of high-dose intravenous melphalan in patients undergoing peripheral blood hematopoietic progenitor-cell transplantation. Anticancer. Res. 1997, 17, 605–611. [Google Scholar] [PubMed]
- Park, J.R.; Kreissman, S.G.; London, W.B.; Naranjo, A.; Cohn, S.L.; Hogarty, M.D.; Tenney, S.C.; Haas-Kogan, D.; Shaw, P.J.; Kraveka, J.M.; et al. Effect of Tandem Autologous Stem Cell Transplant vs Single Transplant on Event-Free Survival in Patients With High-Risk Neuroblastoma. JAMA 2019, 322, 746–755. [Google Scholar] [CrossRef] [PubMed]
- Ladenstein, R.; Pötschger, U.; Pearson, A.D.J.; Brock, P.; Luksch, R.; Castel, V.; Yaniv, I.; Papadakis, V.; Laureys, G.; Malis, J.; et al. Busulfan and melphalan versus carboplatin, etoposide, and melphalan as high-dose chemotherapy for high-risk neuroblastoma (HR-NBL1/SIOPEN): An international, randomised, multi-arm, open-label, phase 3 trial. Lancet Oncol. 2017, 18, 500–514. [Google Scholar] [CrossRef]
- Desai, A.V.; Heneghan, M.B.; Li, Y.; Bunin, N.J.; A Grupp, S.; Bagatell, R.; E Seif, A. Toxicities of busulfan/melphalan versus carboplatin/etoposide/melphalan for high-dose chemotherapy with stem cell rescue for high-risk neuroblastoma. Bone Marrow Transpl. 2016, 51, 1204–1210. [Google Scholar] [CrossRef]
- Furtwaengler, R.; Kager, L.; Melchior, P.; Rübe, C.; Ebinger, M.; Nourkami, N.; Niggli, F.; Warmann, S.; Hubertus, J.; Amman, G.; et al. High-dose treatment for malignant rhabdoid tumor of the kidney: No evidence for improved survival-The Gesellschaft für Pädiatrische Onkologie und Hämatologie (GPOH) experience. Pediatr. Blood Cancer 2018, 65, e26746. [Google Scholar] [CrossRef]
- Choi, J.Y.; Kang, H.J.; Hong, K.T.; Hong, C.R.; Lee, Y.J.; Park, J.D.; Phi, J.H.; Kim, S.-K.; Wang, K.-C.; Kim, I.H.; et al. Tandem high-dose chemotherapy with topotecan–thiotepa–carboplatin and melphalan–etoposide–carboplatin regimens for pediatric high-risk brain tumors. Int. J. Clin. Oncol. 2019, 24, 1515–1525. [Google Scholar] [CrossRef]
- Hong, C.R.; Kang, H.J.; Kim, M.S.; Ju, H.Y.; Lee, J.W.; Kim, H.-S.; Park, S.-H.; Park, K.D.; Park, J.D.; Shin, H.Y.; et al. High-dose chemotherapy and autologous stem cell transplantation with melphalan, etoposide and carboplatin for high-risk osteosarcoma. Bone Marrow Transpl. 2015, 50, 1375–1378. [Google Scholar] [CrossRef] [Green Version]
- Kremens, B.; Gruhn, B.; Klingebiel, T.; Hasan, C.; Laws, H.-J.; Koscielniak, E.; Hero, B.; Selle, B.; Niemeyer, C.; Finckenstein, F.G.; et al. High-dose chemotherapy with autologous stem cell rescue in children with nephroblastoma. Bone Marrow Transpl. 2002, 30, 893–898. [Google Scholar] [CrossRef]
- Spreafico, F.; Bisogno, G.; Collini, P.; Jenkner, A.; Gandola, L.; D’Angelo, P.; Casazza, G.; Piva, L.; Luksch, R.; Perotti, D.; et al. Treatment of high-risk relapsed Wilms tumor with dose-intensive chemotherapy, marrow-ablative chemotherapy, and autologous hematopoietic stem cell support: Experience by the Italian association of pediatric hematology and oncology. Pediatr. Blood Cancer 2008, 51, 23–28. [Google Scholar] [CrossRef] [Green Version]
- Dallorso, S.; EBMT Paediatric Working Party; Dini, G.; Faraci, M.; Spreafico, F. SCT for Wilms’ tumour. Bone Marrow Transpl. 2008, 41, S128–S130. [Google Scholar] [CrossRef] [Green Version]
- Nieto, Y.; Tu, S.-M.; Bassett, R.; Jones, R.B.; Gulbis, A.M.; Tannir, N.; Kingham, A.; Ledesma, C.; Margolin, K.; Holmberg, L.; et al. Bevacizumab/high-dose chemotherapy with autologous stem-cell transplant for poor-risk relapsed or refractory germ-cell tumors. Ann. Oncol. 2015, 26, 2125–2132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jodele, S.; E Dandoy, C.; Myers, K.C.; Wallace, G.; Lane, A.; Teusink-Cross, A.; Weiss, B.; Davies, S.M. High-dose Carboplatin/Etoposide/Melphalan increases risk of thrombotic microangiopathy and organ injury after autologous stem cell transplantation in patients with neuroblastoma. Bone Marrow Transpl. 2018, 53, 1311–1318. [Google Scholar] [CrossRef] [PubMed]
- Göbel, U.; Wessalowski, R.; Calaminus, G.; Pape, H.; Bamberg, M.; Engert, J.; Waag, K.; Gadner, H.; Göbel, U. Treatment of Recurrent Malignant Sacrococcygeal Germ Cell Tumors: Analysis of 22 Patients Registered in the German Protocols MAKEI 83/86, 89, and 96. J. Clin. Oncol. 2001, 19, 1951–1960. [Google Scholar] [CrossRef] [PubMed]
- Wessalowski, R.; Schneider, D.T.; Mils, O.; Friemann, V.; Kyrillopoulou, O.; Schaper, J.; Matuschek, C.; Rothe, K.; Leuschner, I.; Willers, R.; et al. Regional deep hyperthermia for salvage treatment of children and adolescents with refractory or recurrent non-testicular malignant germ-cell tumours: An open-label, non-randomised, single-institution, phase 2 study. Lancet Oncol. 2013, 14, 843–852. [Google Scholar] [CrossRef]
- Fizazi, K.; Tjulandin, S.; Salvioni, R.; Germà-Lluch, J.R.; Bouzy, J.; Ragan, D.; Bokemeyer, C.; Gerl, A.; Fléchon, A.; De Bono, J.S.; et al. Viable Malignant Cells After Primary Chemotherapy for Disseminated Nonseminomatous Germ Cell Tumors: Prognostic Factors and Role of Postsurgery Chemotherapy—Results From an International Study Group. J. Clin. Oncol. 2001, 19, 2647–2657. [Google Scholar] [CrossRef] [PubMed]
- Fizazi, K.; Oldenburg, J.; Dunant, A.; Chen, I.; Salvioni, R.; Hartmann, J.T.; De Santis, M.; Daugaard, G.; Flechon, A.; De Giorgi, U.; et al. Assessing prognosis and optimizing treatment in patients with postchemotherapy viable nonseminomatous germ-cell tumors (NSGCT): Results of the sCR2 international study. Ann. Oncol. 2008, 19, 259–264. [Google Scholar] [CrossRef]
- Funt, S.A.; Patil, S.; Feldman, D.R.; Motzer, R.J.; Bajorin, D.F.; Sheinfeld, J.; Tickoo, S.K.; Reuter, V.E.; Bosl, G.J. Impact of Teratoma on the Cumulative Incidence of Disease-Related Death in Patients with Advanced Germ Cell Tumors. J. Clin. Oncol. 2019, 37, 2329–2337. [Google Scholar] [CrossRef]
- Maoz, A.; Matsuo, K.; Ciccone, M.A.; Matsuzaki, S.; Klar, M.; Roman, L.D.; Sood, A.K.; Gershenson, D.M. Molecular Pathways and Targeted Therapies for Malignant Ovarian Germ Cell Tumors and Sex Cord–Stromal Tumors: A Contemporary Review. Cancers 2020, 12, 1398. [Google Scholar] [CrossRef]
- Einhorn, L.H.; Brames, M.J.; Heinrich, M.C.; Corless, C.L.; Madani, A. Phase II Study of Imatinib Mesylate in Chemotherapy Refractory Germ Cell Tumors Expressing KIT. Am. J. Clin. Oncol. 2006, 29, 12–13. [Google Scholar] [CrossRef]
- Fankhauser, C.D.; Curioni-Fontecedro, A.; Allmann, V.; Beyer, J.; Tischler, V.; Sulser, T.; Moch, H.; Bode, P.K. Frequent PD-L1 expression in testicular germ cell tumors. Br. J. Cancer 2015, 113, 411–413. [Google Scholar] [CrossRef] [Green Version]
- Adra, N.; Einhorn, L.H.; Althouse, S.; Ammakkanavar, N.; Musapatika, D.; Albany, C.; Vaughn, D.; Hanna, N. Phase II trial of pembrolizumab in patients with platinum refractory germ-cell tumors: A Hoosier Cancer Research Network Study GU14-206. Ann. Oncol. 2018, 29, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Therasse, P.; Arbuck, S.G.; Eisenhauer, E.A.; Wanders, J.; Kaplan, R.S.; Rubinstein, L.; Verweij, J.; Van Glabbeke, M.; Van Oosterom, A.T.; Christian, M.C.; et al. New Guidelines to Evaluate the Response to Treatment in Solid Tumors. J. Natl. Cancer Inst. 2000, 92, 205–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Patient Number (UPN) | Sex | Histology | Localization | First-Line Chemotherapy | Second Line Chemotherapy | Third Line Chemotherapy | Surgery | Indication for HDCT | Metastatic Disease at HDCT |
|---|---|---|---|---|---|---|---|---|---|
| 1 | M | GCT | extragonadal (sacrococcygeal), bone metastases | 6 × VIP | 4 × ABK | after 4 VIP, viable tumor (teratoma with blastemic fields) remained | advanced disease, viable tumor after 4 VIP chemotherapy | yes | |
| 2 | F | GCT | extragonadal (sacrococcygeal) | 6 × VIP | 2 × ABK | 1. after 4 VIP, 2. after 6 VIP | relapsed disease with residual tumor | no | |
| 3 | F | YS | gonadal (ovary), pulmonary metastases | 4 × VBP | 4 × VIP | 2 × ABK | 3 times (resections and biopsies) | metastatic relapse | yes |
| 4 | F | YS | extragonadal (sacrococcygeal) | 5 × VIP | 3 × ABK | before chemotherapy | tumor rupture at surgery | no | |
| 5 | M | GCT | gonadal (testis), abdominal lymph nodes and pulmonary metastases | 4 × VIP | 6 × ABK | before chemotherapy | advanced disease | yes | |
| 6 | M | seminoma | gonadal (testis), abdominal lymph nodes, brain and pulmonary metastases | 6 × VIP | 4 × ABK | before HDCT | advanced metastatic disease | yes | |
| 7 | F | YS/IT | extragonadal (sacrococcygeal) | 5 × VIP | 4 × ABK | before chemotherapy and at relapse | relapse after VIP chemotherapy | no | |
| 8 | F | YS | extragonadal (sacrococcygeal), pulmonary metastases | 6 × VIP | 3 × ABK | 1. after VIP, 2. prior to HDCT (no viable cells) | relapse after VIP chemotherapy | no | |
| 9 | M | GCT | extragonadal (retroperitoneal) | 4 × VBP | 3 × VIP | 4 × ABK | prior to HDCT | relapse after VIP chemotherapy | no |
| 10 | M | IT | extragonadal (sacrococcygeal), pulmonary metastases | missing data | local tumor prior to HDCT | metastatic relapse | yes | ||
| 11 | M | GCT | gonadal (testis) | 6 × VIP | 7 × BEP | local tumor prior to HDCT | advanced disease with metastatic pulmonary relapse | yes | |
| 12 | M | YS/IT | extragonadal (mediastinal), pulmonary metastases | 6 × VIP | before chemotherapy | advanced disease with unresectable tumor | no | ||
| 13 | M | YS | extragonadal (mediastinal tumor with extradural component in spinal canal) | missing data | before chemotherapy | relapsed disease after VIP chemotherapy | no | ||
| 14 | M | IT | extragonadal (sacrococcygeal), pulmonary and peritoneal metastases | 1 × VBP | 6 × VIP | 3 × ABK | 1. at diagnosis, 2. in relapse after VIP (viable cells) | advanced, metastatic disease, viable tumor after VIP chemotherapy | yes |
| 15 | F | embryonal carcinoma | gonadal (ovary) | 4 × VIP | 2 × ABK | PVB, POG/CCG 8882 | before chemotherapy | metastatic peritoneal disease, multiple relapses | yes |
| 16 | M | IT | extragonadal (sacrococcygeal), pulmonary metastases | 1 × VBP | 5 × VIP | 5 × ABK | multiple resections; the last—after 3 ABK, tumorectomy and metastasectomy, viable cells remained | disseminated disease with multiple relapses, viable tumor after 3 ABK chemotherapy | yes |
| 17 | F | embryonal carcinoma | extragonadal (sacrococcygeal), hepatic and pulmonary metastases | 6 × VIP | ABK | HDCY | 1. before chemotherapy, 2. after VIP chemotherapy | disseminated disease, viable tumor after VIP chemotherapy | yes |
| 18 | F | dysgerminoma | gonadal (ovary), mediastinal and brain metastases | 6 × VIP | HDCY | 1. before chemotherapy, 2. primary resection after 5 VIP | advanced metastatic disease | yes | |
| Patient Number (UPN) | Age at HDCT in Months | Status at HDCT | AFP within 4 Weeks Prior to HDCT | HDCT Protocol | Graft Content 106 CD34 Cells/kg | Mucositis, Grade | FUO/Infections | Toxicities with Grades | Post-HDCT Surgery | Post-HDCT Status | Follow-Up Time (Months) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 39.0 | 1 PR | normal | MEC2 | 4.81 | 3 | FUO 3 | hepatic aminotransferase activity 2 | after 13 months, mature teratoma | alive, local relapse | 18.7 |
| 2 | 30.4 | 2 PR | n/a | MEC2 | 7.038 | 3 | FUO 3 | hepatic aminotransferase activity 2 | no | A&W | 40.0 |
| 3 | 184.7 | 2 PR | elevated | MEC2 | 4.83 | 3 | FUO 3 | hepatic aminotransferase activity 3 | twice—debulking | DOD | 22.7 |
| 4 | 41.7 | 1 PR | elevated | MEC2 | 7.86 | 3 | FUO 3 | hepatic aminotransferase activity 4, hepatic veno-occlusive disease 3 | no | A&W | 62.3 |
| 5 | 222.6 | 1 PR | normal | MEC2 | 11.1 | 3 | FUO 3 | no | A&W | 69.1 | |
| 6 | 212.9 | 3 PR | normal | MEC2 | 3.4 | 3 | FUO 3 | hepatic aminotransferase activity 1 | no | DOD | 2.4 |
| 7 | 28.6 | 1 CR | normal | MEC2 | 13.22 | 3 | FUO 3 | hepatic aminotransferase activity 2 | no | A&W | 94.1 |
| 8 | 26.6 | 2 CR | normal | MEC2 | 4.09 | 3 | FUO 3 | hepatic aminotransferase activity 1 | no | A&W | 97.8 |
| 9 | 209.2 | 2 PR | elevated | MEC2 | 4.48 | 3 | FUO 3, sepsis 3 | no | DOD | 13.9 | |
| 10 | 37.7 | 2 CR | normal | MEC1 | 3.52 | 3 | FUO 3, sepsis 3 | no | A&W | 0.8 | |
| 11 | 219.4 | 2 PR | normal | MEC1 | 3.93 | 3 | FUO 3, bacteremia 2 | hepatic aminotransferase activity 3, creatinine 3, hyponatremia 3, hyperkalemia 3, acute kidney injury 3 | no | A&W | 126.7 |
| 12 | 29.2 | 1 PR | normal | MEC1 | 3.12 | 3 | FUO 3 | hepatic aminotransferase activity 1 | no | A&W | 129.7 |
| 13 | 32.7 | 2 PR | elevated | MEC1 | 6.98 | 4 | FUO 3, sepsis 4 | mucosal and gastrointestinal bleeding 4 | no | A&W | 131.7 |
| 14 | 17.2 | 2 PR | normal | MEC1 | 5.11 | 3 | FUO 3 | hepatic aminotransferase activity 3 | no | GCT remission, second malignancy (osteosarcoma) | 162.2 |
| 15 | 176.8 | 2 PR | elevated | MEC1 | 1.25 | 4 | FUO 3, sepsis 3 | hepatic aminotransferase activity 2, creatinine 2, oliguria 2 | no | DOD | 6.3 |
| 16 | 26.3 | 3 CR | normal | MEC1 | 4.64 | 3 | FUO 3 | no | alive, local relapse | 181.5 | |
| 17 | 43.0 | 1 CR | normal | MEC1 | 2.84 | 3 | FUO 3 | no | A&W | 178.6 | |
| 18 | 147.3 | 1 PR | n/a | MEC1 | 2.4 | 3 | FUO 3 | yes, no malignancy | A&W | 192.0 |
| Category | Number of Patients | 5 Year OS | Log Rank p | 5 Year EFS | Log Rank p | |
|---|---|---|---|---|---|---|
| All patients | 18 | 76% | 70.80% | |||
| Type of HDCT | MEC1 | 9 | 87.50% | ns | 88.90% | ns |
| MEC2 | 9 | 64.80% | 55.60% | |||
| Sex | male | 10 | 77.80% | ns | 66.70% | ns |
| female | 8 | 75% | 75% | |||
| Age | <4 years | 11 | 100% | 0.007 | 90% | 0.02 |
| >12 years | 7 | 42.90% | 43% | |||
| Disease status at HDCT | 1 CR/PR | 7 | 100% | ns | 85.7% | ns |
| >1 CR/PR | 11 | 60% | 60.6% | |||
| Metastatic disease | yes | 10 | 64.80% | ns | 56.30% | ns |
| no | 8 | 87.50% | 87.50% | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ussowicz, M.; Mielcarek-Siedziuk, M.; Musiał, J.; Stachowiak, M.; Węcławek-Tompol, J.; Sęga-Pondel, D.; Frączkiewicz, J.; Trelińska, J.; Raciborska, A. Melphalan, Etoposide, and Carboplatin Megatherapy with Autologous Stem Cell Transplantation in Children with Relapsing or Therapy-Resistant Extracranial Germ-Cell Tumors—A Retrospective Analysis. Cancers 2020, 12, 3841. https://doi.org/10.3390/cancers12123841
Ussowicz M, Mielcarek-Siedziuk M, Musiał J, Stachowiak M, Węcławek-Tompol J, Sęga-Pondel D, Frączkiewicz J, Trelińska J, Raciborska A. Melphalan, Etoposide, and Carboplatin Megatherapy with Autologous Stem Cell Transplantation in Children with Relapsing or Therapy-Resistant Extracranial Germ-Cell Tumors—A Retrospective Analysis. Cancers. 2020; 12(12):3841. https://doi.org/10.3390/cancers12123841
Chicago/Turabian StyleUssowicz, Marek, Monika Mielcarek-Siedziuk, Jakub Musiał, Mateusz Stachowiak, Jadwiga Węcławek-Tompol, Dorota Sęga-Pondel, Jowita Frączkiewicz, Joanna Trelińska, and Anna Raciborska. 2020. "Melphalan, Etoposide, and Carboplatin Megatherapy with Autologous Stem Cell Transplantation in Children with Relapsing or Therapy-Resistant Extracranial Germ-Cell Tumors—A Retrospective Analysis" Cancers 12, no. 12: 3841. https://doi.org/10.3390/cancers12123841