Low Serum Branched-chain Amino Acid and Insulin-Like Growth Factor-1 Levels Are Associated with Sarcopenia and Slow Gait Speed in Patients with Liver Cirrhosis

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Diagnosis of Sarcopenia and Slow Gait Speed
2.3. Clinical and Laboratory Assessments
2.4. Classification Based on Serum BCAA and IGF-1 Levels
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Comparison of Clinical Characteristics between Patients with and without Sarcopenia
3.3. Factors Associated with Sarcopenia in Patients with LC
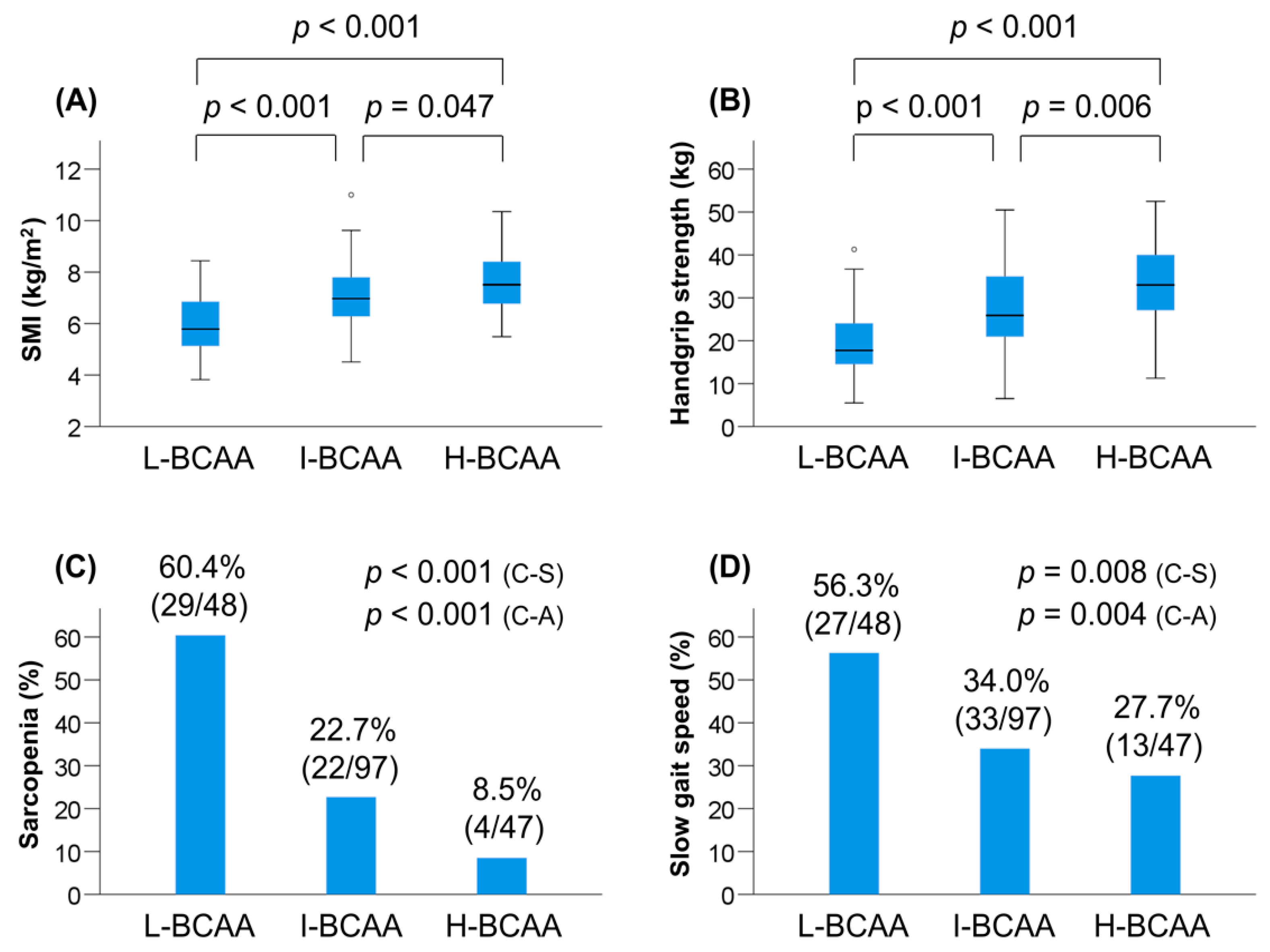
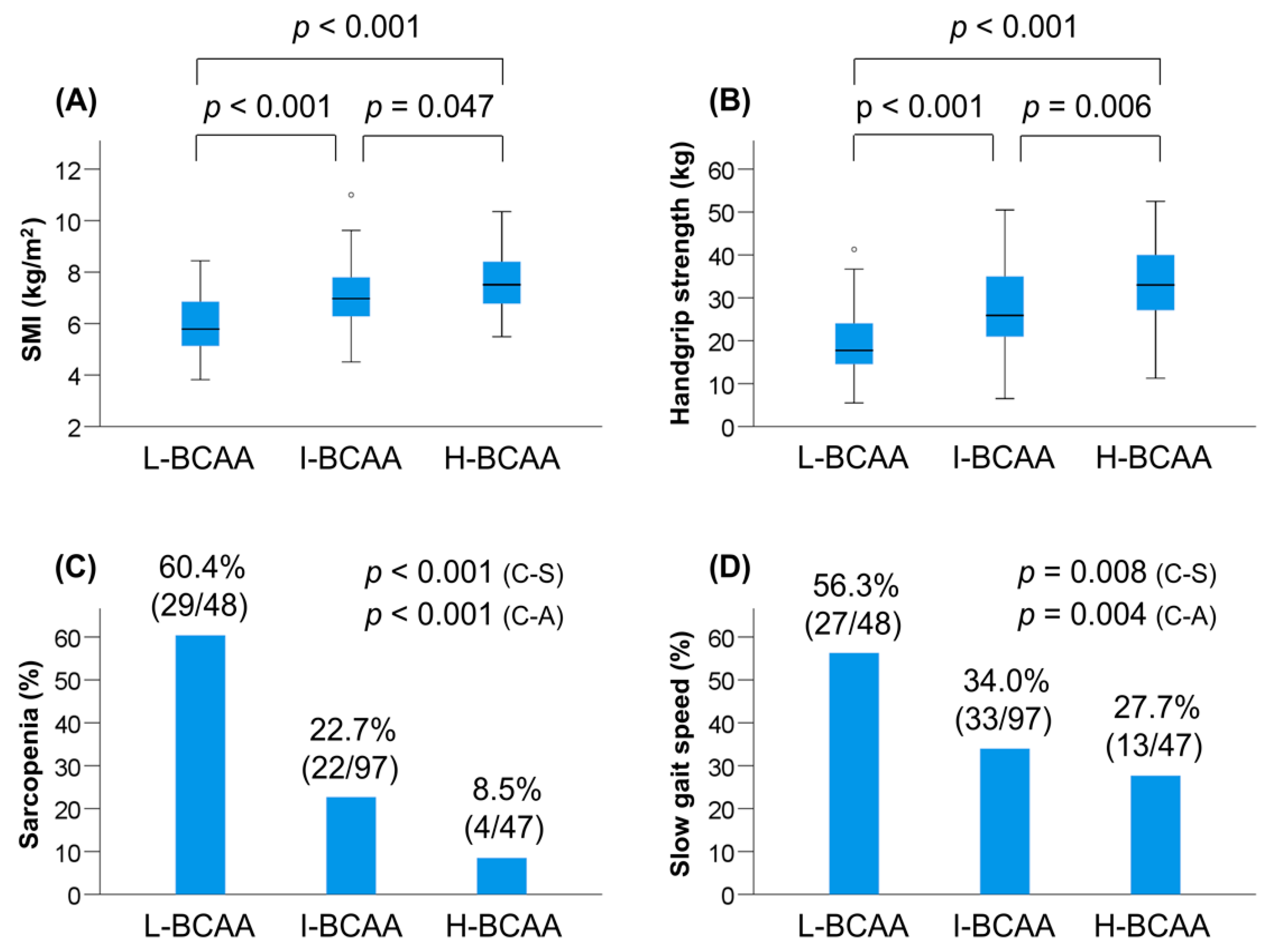
3.4. Clinical Characteristics of Patients Based on Serum BCAA Levels
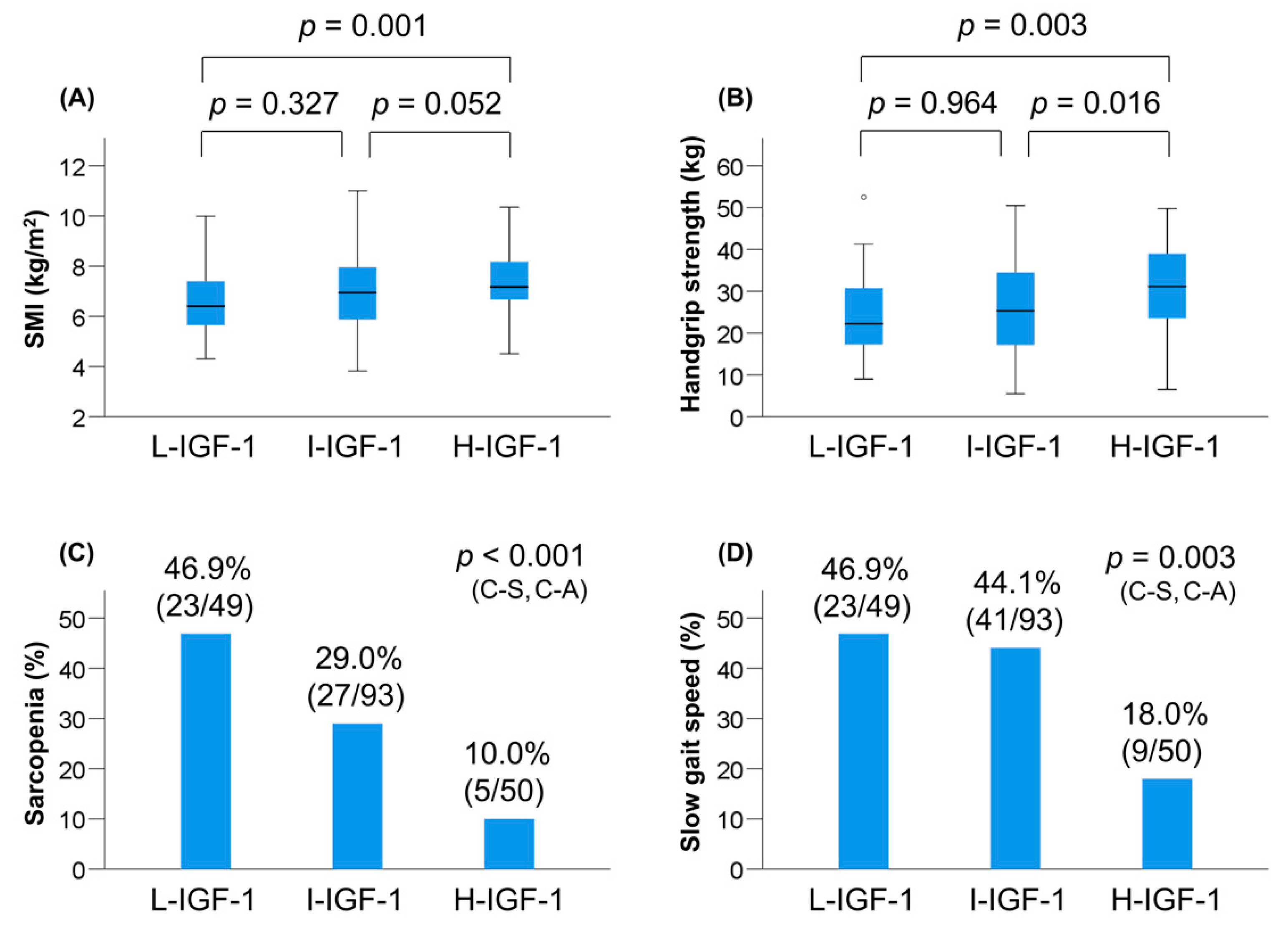
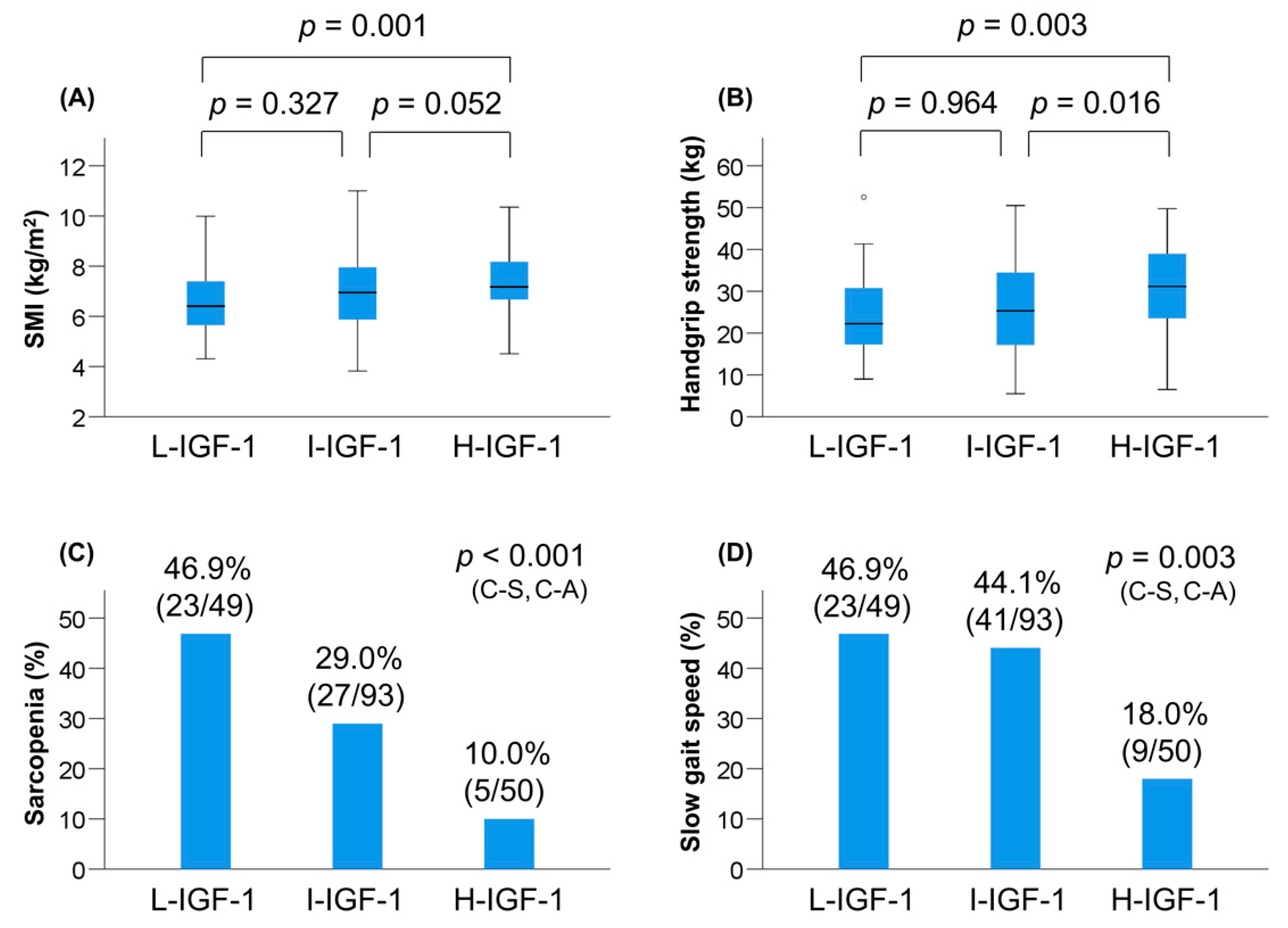
3.5. Clinical Characteristics of Patients Based on IGF-1 Levels
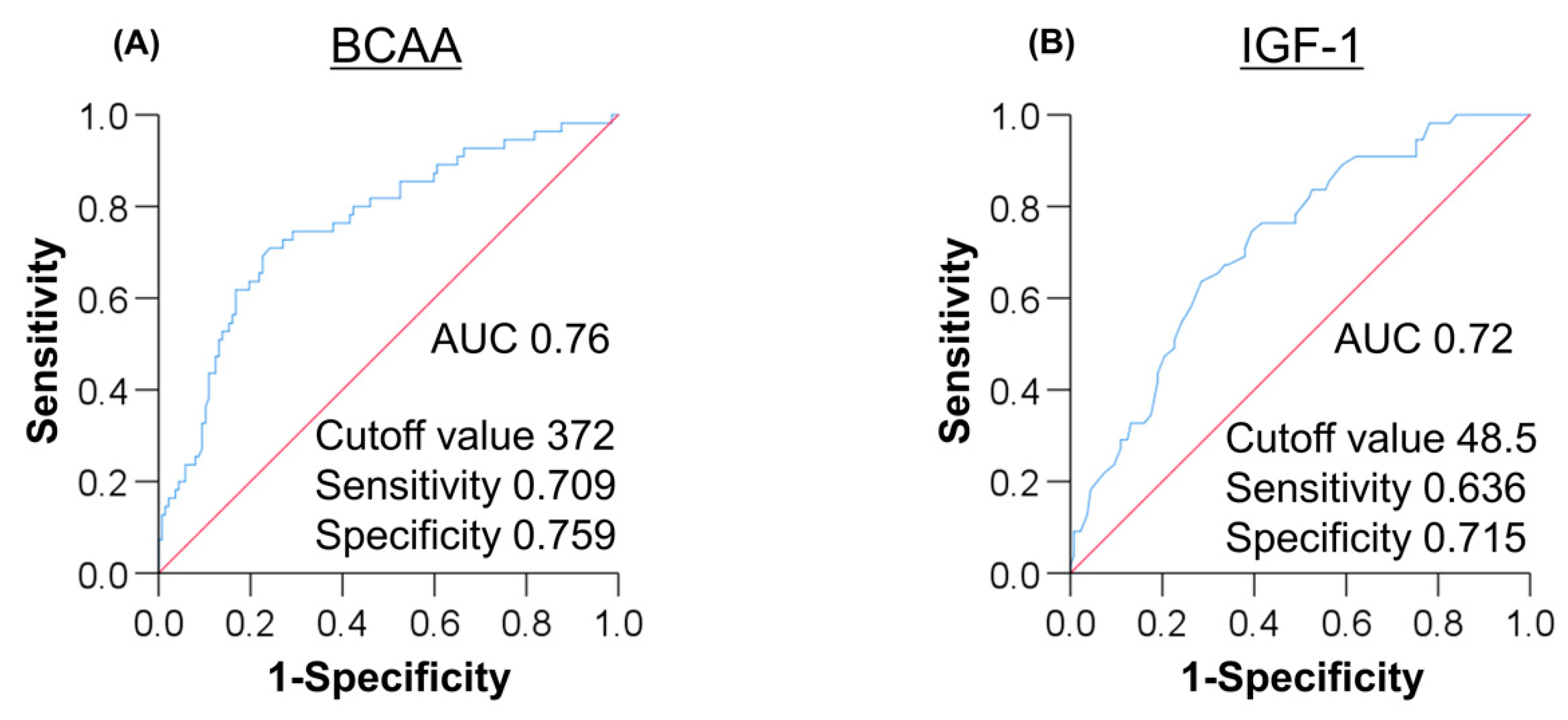
3.6. Optimal Cutoff Values of BCAA and IGF-1 for Predicting Sarcopenia
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Nishikawa, H.; Shiraki, M.; Hiramatsu, A.; Moriya, K.; Hino, K.; Nishiguchi, S. Japan Society of Hepatology guidelines for sarcopenia in liver disease (1st edition): Recommendation from the working group for creation of sarcopenia assessment criteria. Hepatol. Res. 2016, 46, 951–963. [Google Scholar] [CrossRef] [PubMed]
- Hanai, T.; Shiraki, M.; Nishimura, K.; Ohnishi, S.; Imai, K.; Suetsugu, A.; Takai, K.; Shimizu, M.; Moriwaki, H. Sarcopenia impairs prognosis of patients with liver cirrhosis. Nutrition 2015, 31, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Ohashi, K.; Ishikawa, T.; Hoshi, A.; Suzuki, M.; Mitobe, Y.; Yamada, E.; Abeywickrama, H.M.; Seki, N.; Koyama, C.; Aoki, H.; et al. Relationship between sarcopenia and both physical activity and lifestyle in patients with chronic liver disease. J. Clin. Med. Res. 2018, 10, 920–927. [Google Scholar] [CrossRef] [Green Version]
- Saeki, C.; Takano, K.; Oikawa, T.; Aoki, Y.; Kanai, T.; Takakura, K.; Nakano, M.; Torisu, Y.; Sasaki, N.; Abo, M.; et al. Comparative assessment of sarcopenia using the JSH, AWGS, and EWGSOP2 criteria and the relationship between sarcopenia, osteoporosis, and osteosarcopenia in patients with liver cirrhosis. BMC Musculoskelet Disord. 2019, 20, 615. [Google Scholar] [CrossRef] [Green Version]
- Nishikawa, H.; Enomoto, H.; Yoh, K.; Iwata, Y.; Sakai, Y.; Kishino, K.; Ikeda, N.; Takashima, T.; Aizawa, N.; Takata, R.; et al. Serum zinc concentration and sarcopenia: A close linkage in chronic liver diseases. J. Clin. Med. 2019, 8, 336. [Google Scholar] [CrossRef] [Green Version]
- Fozouni, L.; Wang, C.W.; Lai, J.C. Sex Differences in the Association Between Frailty and Sarcopenia in Patients with Cirrhosis. Clin. Transl. Gastroenterol. 2019, 10, e00102. [Google Scholar] [CrossRef]
- Traub, J.; Bergheim, I.; Eibisberger, M.; Stadlbauer, V. Sarcopenia and Liver Cirrhosis-Comparison of the European Working Group on Sarcopenia Criteria 2010 and 2019. Nutrients 2020, 12, 547. [Google Scholar] [CrossRef] [Green Version]
- Ebadi, M.; Bhanji, R.A.; Mazurak, V.C.; Montano-Loza, A.J. Sarcopenia in cirrhosis: From pathogenesis to interventions. J. Gastroenterol. 2019, 54, 845–859. [Google Scholar] [CrossRef] [Green Version]
- Sinclair, M.; Gow, P.J.; Grossmann, M.; Angus, P.W. Review article: Sarcopenia in cirrhosis-aetiology, implications and potential therapeutic interventions. Aliment. Pharmacol. Ther. 2016, 43, 765–777. [Google Scholar] [CrossRef] [Green Version]
- Tajiri, K.; Shimizu, Y. Branched-chain amino acids in liver diseases. Transl. Gastroenterol. Hepatol. 2018, 3, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katsanos, C.S.; Kobayashi, H.; Sheffield-Moore, M.; Aarsland, A.; Wolfe, R.R. A high proportion of leucine is required for optimal stimulation of the rate of muscle protein synthesis by essential amino acids in the elderly. Am. J. Physiol. Endocrinol. Metab. 2006, 291, E381–E387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moriwaki, H. Branched-chain amino acids as a protein- and energy-source in liver cirrhosis. Biochem. Biophys. Res. Commun. 2004, 313, 405–409. [Google Scholar] [CrossRef] [PubMed]
- Assy, N.; Pruzansky, Y.; Gaitini, D.; Shen Orr, Z.; Hochberg, Z.; Baruch, Y. Growth Hormone-Stimulated IGF-1 Generation in Cirrhosis Reflects Hepatocellular Dysfunction. J. Hepatol. 2008, 49, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Tsien, C.; Davuluri, G.; Singh, D.; Allawy, A.; Ten Have, G.A.; Thapaliya, S.; Schulze, J.M.; Barnes, D.; McCullough, A.J.; Engelen, M.P.; et al. Metabolic and molecular responses to leucine-enriched branched chain amino acid supplementation in the skeletal muscle of alcoholic cirrhosis. Hepatology 2015, 61, 2018–2029. [Google Scholar] [CrossRef] [PubMed]
- Ottestad, I.; Ulven, S.M.; Øyri, L.K.L.; Sandvei, K.S.; Gjevestad, G.O.; Bye, A.; Sheikh, N.A.; Biong, A.S.; Andersen, L.F.; Holven, K.B. Reduced plasma concentration of branched-chain amino acids in sarcopenic older subjects: A cross-sectional study. Br. J. Nutr. 2018, 120, 445–453. [Google Scholar] [CrossRef] [Green Version]
- Yamada, M.; Kimura, Y.; Ishiyama, D.; Nishio, N.; Tanaka, T.; Ohji, S.; Otobe, Y.; Koyama, S.; Sato, A.; Suzuki, M.; et al. Plasma Amino Acid Concentrations Are Associated with Muscle Function in Older Japanese Women. J. Nutr. Health Aging 2018, 22, 819–823. [Google Scholar] [CrossRef]
- Van Nieuwpoort, I.C.; Vlot, M.C.; Schaap, L.A.; Lips, P.; Drent, M.L. The Relationship Between Serum IGF-1, Handgrip Strength, Physical Performance and Falls in Elderly Men and Women. Eur. J. Endocrinol. 2018, 179, 73–84. [Google Scholar] [CrossRef] [Green Version]
- Doi, T.; Shimada, H.; Makizako, H.; Tsutsumimoto, K.; Hotta, R.; Nakakubo, S.; Suzuki, T. Insulin-Like Growth Factor-1 Related to Disability Among Older Adults. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 797–802. [Google Scholar] [CrossRef] [Green Version]
- Bian, A.; Ma, Y.; Zhou, X.; Guo, Y.; Wang, W.; Zhang, Y.; Wang, X. Association Between Sarcopenia and Levels of Growth Hormone and Insulin-Like Growth factor-1 in the Elderly. BMC Musculoskelet Disord. 2020, 21, 214. [Google Scholar] [CrossRef] [Green Version]
- García, P.S.; Cabbabe, A.; Kambadur, R.; Nicholas, G.; Csete, M. Brief-Reports: Elevated Myostatin Levels in Patients with Liver Disease: A Potential Contributor to Skeletal Muscle Wasting. Anesth. Analg. 2010, 111, 707–709. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, H.; Enomoto, H.; Ishii, A.; Iwata, Y.; Miyamoto, Y.; Ishii, N.; Yuri, Y.; Hasegawa, K.; Nakano, C.; Nishimura, T.; et al. Elevated Serum Myostatin Level Is Associated with Worse Survival in Patients with Liver Cirrhosis. J. Cachexia Sarcopenia Muscle 2017, 8, 915–925. [Google Scholar] [CrossRef] [PubMed]
- Drummond, M.J.; Rasmussen, B.B. Leucine-enriched nutrients and the regulation of mammalian target of rapamycin signaling and human skeletal muscle protein synthesis. Curr. Opin. Clin. Nutr. Metab. Care 2008, 11, 222–226. [Google Scholar] [CrossRef] [PubMed]
- Hiraoka, A.; Michitaka, K.; Kiguchi, D.; Izumoto, H.; Ueki, H.; Kaneto, M.; Kitahata, S.; Aibiki, T.; Okudaira, T.; Tomida, H.; et al. Efficacy of Branched-Chain Amino Acid Supplementation and Walking Exercise for Preventing Sarcopenia in Patients with Liver Cirrhosis. Eur. J. Gastroenterol. Hepatol. 2017, 29, 1416–1423. [Google Scholar] [CrossRef]
- Buckinx, F.; Landi, F.; Cesari, M.; Fielding, R.A.; Visser, M.; Engelke, K.; Maggi, S.; Dennison, E.; Al-Daghri, N.M.; Allepaerts, S.; et al. Pitfalls in the measurement of muscle mass: A need for a reference standard. J. Cahexia Sarcopenia Muscle 2018, 9, 269–278. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Variable | All Patients | Sarcopenia | Non-Sarcopenia | p Value |
|---|---|---|---|---|
| Patients, n (%) | 192 | 55 (28.6) | 137 (71.4) | |
| Age (years) | 69.0 (59.0–76.0) | 76.0 (71.0–80.0) | 65.0 (58.0–73.0) | <0.001 |
| Male, n (%) | 129 (67.2) | 32 (58.2) | 97 (70.8) | 0.092 |
| BMI (kg/m2) | 23.7 (21.1–26.1) | 21.0 (19.0–22.6) | 24.5 (22.5–26.6) | <0.001 |
| Etiology | ||||
| HBV/HCV/Alcohol/other, n | 18/66/63/45 | 3/30/12/10 | 15/36/51/35 | 0.003 |
| Child–Pugh A/B + C, n | 129/63 | 35/20 | 94/43 | 0.507 |
| Total bilirubin (mg/dL) | 0.9 (0.6–1.3) | 0.8 (0.5–1.4) | 0.9 (0.7–1.3) | 0.417 |
| Albumin (g/dL) | 3.8 (3.4–4.2) | 3.7 (3.1–4.2) | 3.9 (3.5–4.3) | 0.035 |
| Prothrombin time (%) | 81 (67–94) | 82 (68–100) | 81 (67–92) | 0.524 |
| IGF-1 (ng/mL) | 55 (41–73) | 45 (33–55) | 61 (47–77) | <0.001 |
| BCAA (µmol/L) | 399 (330–475) | 321 (293–397) | 425 (376–492) | <0.001 |
| BCAA supplementation, n (%) | 36 (18.8) | 11 (20.0) | 25 (18.2) | 0.779 |
| Zinc (µg/dL) | 63 (54–74) | 62 (48–73) | 65 (55–74) | 0.111 |
| SMI (kg/m2) | ||||
| ALL patients | 6.95 (5.98–7.87) | 5.65 (4.99–6.44) | 7.34 (6.59–8.22) | <0.001 |
| Male | 7.34 (6.79–8.25) | 6.32 (5.69–6.80) | 7.80 (7.14–8.46) | <0.001 |
| Female | 5.87 (5.21–6.48) | 5.09 (4.55–5.39) | 6.24 (5.89–6.74) | <0.001 |
| Handgrip strength (kg) | ||||
| ALL patients | 25.9 (18.3–35.3) | 17.3 (14.5–23.4) | 31.0 (23.3–37.2) | <0.001 |
| Male | 31.6 (25.0–37.5) | 22.1 (18.3–24.2) | 35.2 (30.1–40.0) | <0.001 |
| Female | 17.0 (14.2–21.9) | 14.6 (12.6–16.5) | 21.1 (15.3–23.4) | <0.001 |
| Gait speed (m/s) | 1.06 (0.86–1.26) | 0.80 (0.61–0.97) | 1.12 (1.02–1.34) | <0.001 |
| Slow gait speed, n (%) | 73 (38.0) | 44 (80.0) | 29 (21.2) | <0.001 |
| Variable | Univariate | Multivariate | ||
|---|---|---|---|---|
| OR (95%CI) | p Value | OR (95% CI) | p Value | |
| Age (years) | 1.079 (1.041–1.117) | <0.001 | 1.102 (1.053–1.153) | <0.001 |
| BMI (kg/m2) | 0.707 (0.622–0.803) | <0.001 | 0.760 (0.650–0.887) | 0.001 |
| Albumin (g/dL) | 0.470 (0.267–0.826) | 0.009 | ||
| IGF-1 (ng/mL) | 0.960 (0.942–0.978) | <0.001 | 0.962 (0.938–0.987) | 0.003 |
| BCAA (µmol/L) | 0.989 (0.985–0.993) | <0.001 | 0.989 (0.983–0.994) | <0.001 |
| Variable | L-BCAA | I-BCAA | H-BCAA | p Value |
|---|---|---|---|---|
| Patients, n (%) | 48 (25.0) | 97 (50.5) | 47 (24.5) | |
| Age (years) | 71.5 (53.0–76.0) | 69.0 (61.0–76.0) | 68.0 (59.0–77.0) | 0.938 |
| Male, n (%) | 20 (41.7) | 69 (71.1) | 40 (85.1) | <0.001 |
| BMI (kg/m2) | 22.2 (19.9–24.1) | 23.7 (21.1–26.3) | 24.8 (23.0–26.9) | 0.002 |
| Etiology | ||||
| HBV/HCV/Alcohol/other, n | 2/17/17/12 | 7/33/33/24 | 9/16/13/9 | 0.262 |
| Child–Pugh A/B + C, n | 20/28 | 70/27 | 39/8 | <0.001 |
| Total bilirubin (mg/dL) | 0.9 (0.6–1.8) | 0.8 (0.6–1.2) | 1.0 (0.7–1.3) | 0.459 |
| Albumin (g/dL) | 3.5 (3.2–4.2) | 3.8 (3.5–4.2) | 4.1 (3.7–4.4) | <0.001 |
| Prothrombin time (%) | 74 (56–88) | 80 (68–94) | 86 (76–98) | 0.012 |
| IGF-1 (ng/mL) | 47 (32–61) | 56 (46–74) | 63 (44–81) | 0.001 |
| BCAA supplementation, n (%) | 12 (25.0) | 18 (18.6) | 6 (12.8) | 0.311 |
| Zinc (µg/dL) | 58 (46–67) | 62 (54–74) | 70 (61–81) | <0.001 |
| SMI (kg/m2) | ||||
| ALL patients | 5.79 (5.11–6.88) | 6.97 (6.23–7.83) | 7.51 (6.70–8.43) | <0.001 |
| Male | 6.93 (6.26–7.96) | 7.16 (6.82–8.21) | 7.60 (7.03–8.52) | 0.059 |
| Female | 5.39 (4.72–5.88) | 5.99 (5.69–6.66) | 6.49 (6.11–7.15) | <0.001 |
| Handgrip strength (kg) | ||||
| ALL patients | 17.8 (14.5–24.1) | 25.9 (20.9–35.1) | 33.0 (27.1–40.5) | <0.001 |
| Male | 24.8 (18.4–35.2) | 30.7 (24.9–36.9) | 35.2 (28.8–40.6) | 0.004 |
| Female | 15.4 (14.1–18.0) | 18.1 (14.2–23.0) | 21.9 (17.9–26.0) | 0.058 |
| Sarcopenia, n (%) | 29 (60.4) | 22 (22.7) | 4 (8.5) | <0.001 |
| Gait speed (m/s) | 0.95 (0.64–1.13) | 1.09 (0.90–1.32) | 1.10 (0.99–1.29) | 0.001 |
| Slow gait speed, n (%) | 27 (56.3) | 33 (34.0) | 13 (27.7) | 0.008 |
| Variable | L-IGF-1 | I-IGF-1 | H-IGF-1 | p Value |
|---|---|---|---|---|
| Patients, n (%) | 49 (25.5) | 93 (48.4) | 50 (26.0) | |
| Age (years) | 70.0 (57.5–77.5) | 72.0 (63.0–76.0) | 65.0 (56.5–73.0) | 0.089 |
| Male, n (%) | 31 (63.3) | 62 (66.7) | 36 (72.0) | 0.644 |
| BMI (kg/m2) | 22.5 (20.3–25.7) | 23.6 (20.8–25.9) | 24.8 (22.5–26.8) | 0.036 |
| Etiology | ||||
| HBV/HCV/Alcohol/other, n | 3/21/18/7 | 6/33/27/27 | 9/12/18/11 | 0.066 |
| Child–Pugh A/B + C, n | 24/25 | 66/27 | 39/11 | 0.005 |
| Total bilirubin (mg/dL) | 1.1 (0.6–1.8) | 0.9 (0.6–1.3) | 0.8 (0.6–1.1) | 0.177 |
| Albumin (g/dL) | 3.6 (3.3–3.9) | 3.9 (3.4–4.3) | 4.1 (3.7–4.4) | 0.002 |
| Prothrombin time (%) | 66 (57–89) | 81 (69–94) | 88 (76–100) | <0.001 |
| BCAA (µmol/L) | 346 (311–425) | 402 (333–479) | 433 (390–493) | 0.001 |
| BCAA supplementation, n (%) | 9 (18.4) | 21 (22.6) | 6 (12.0) | 0.302 |
| Zinc (µg/dL) | 58 (49–70) | 65 (56–73) | 70 (56–78) | 0.026 |
| SMI (kg/m2) | ||||
| ALL patients | 6.41 (5.62–7.42) | 6.95 (5.86–7.98) | 7.18 (6.66–8.19) | 0.002 |
| Male | 7.02 (6.35–7.86) | 7.38 (6.91–8.36) | 7.61 (7.00–8.57) | 0.049 |
| Female | 5.39 (4.87–6.08) | 5.84 (5.22–6.11) | 6.60 (6.06–6.96) | 0.003 |
| Handgrip strength (kg) | ||||
| ALL patients | 22.2 (16.8–32.3) | 25.4 (17.1–34.8) | 31.2 (23.4–39.4) | 0.002 |
| Male | 29.8 (21.5–35.5) | 30.9 (25.2–37.0) | 35.1 (29.4–42.3) | 0.019 |
| Female | 15.0 (14.1–21.0) | 16.5 (14.0–21.9) | 22.9 (16.6–25.8) | 0.022 |
| Sarcopenia, n (%) | 23 (46.9) | 27 (29.0) | 5 (10.0) | <0.001 |
| Gait speed (m/s) | 1.00 (0.69–1.12) | 1.04 (0.80–1.21) | 1.17 (1.04–1.40) | <0.001 |
| Slow gait speed, n (%) | 23 (46.9) | 41 (44.1) | 9 (18.0) | 0.003 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saeki, C.; Kanai, T.; Nakano, M.; Oikawa, T.; Torisu, Y.; Saruta, M.; Tsubota, A. Low Serum Branched-chain Amino Acid and Insulin-Like Growth Factor-1 Levels Are Associated with Sarcopenia and Slow Gait Speed in Patients with Liver Cirrhosis. J. Clin. Med. 2020, 9, 3239. https://doi.org/10.3390/jcm9103239
Saeki C, Kanai T, Nakano M, Oikawa T, Torisu Y, Saruta M, Tsubota A. Low Serum Branched-chain Amino Acid and Insulin-Like Growth Factor-1 Levels Are Associated with Sarcopenia and Slow Gait Speed in Patients with Liver Cirrhosis. Journal of Clinical Medicine. 2020; 9(10):3239. https://doi.org/10.3390/jcm9103239
Chicago/Turabian StyleSaeki, Chisato, Tomoya Kanai, Masanori Nakano, Tsunekazu Oikawa, Yuichi Torisu, Masayuki Saruta, and Akihito Tsubota. 2020. "Low Serum Branched-chain Amino Acid and Insulin-Like Growth Factor-1 Levels Are Associated with Sarcopenia and Slow Gait Speed in Patients with Liver Cirrhosis" Journal of Clinical Medicine 9, no. 10: 3239. https://doi.org/10.3390/jcm9103239
APA StyleSaeki, C., Kanai, T., Nakano, M., Oikawa, T., Torisu, Y., Saruta, M., & Tsubota, A. (2020). Low Serum Branched-chain Amino Acid and Insulin-Like Growth Factor-1 Levels Are Associated with Sarcopenia and Slow Gait Speed in Patients with Liver Cirrhosis. Journal of Clinical Medicine, 9(10), 3239. https://doi.org/10.3390/jcm9103239