Incidence of Bladder Cancer in Type 2 Diabetes Mellitus Patients: A Population-Based Cohort Study

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
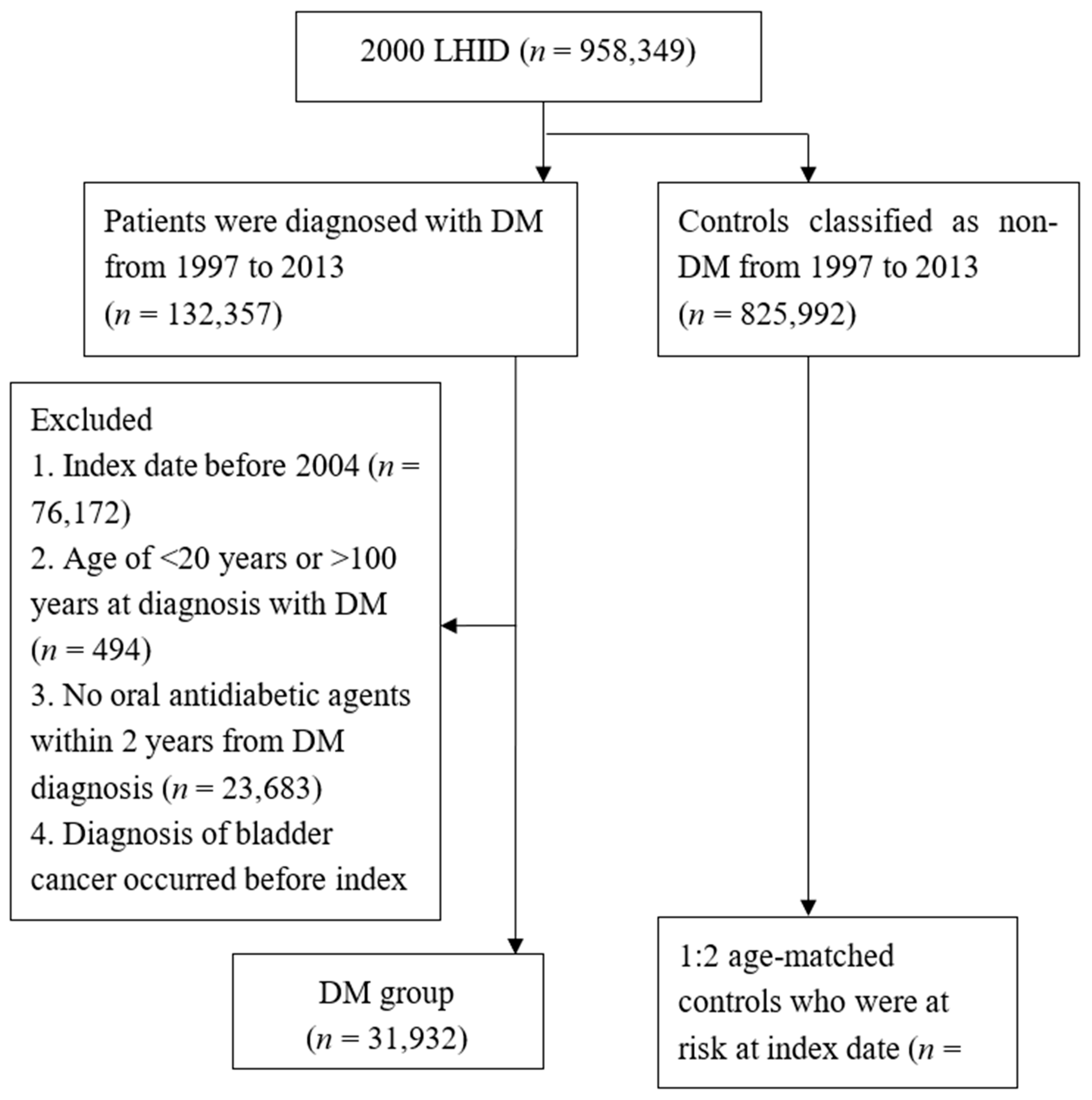
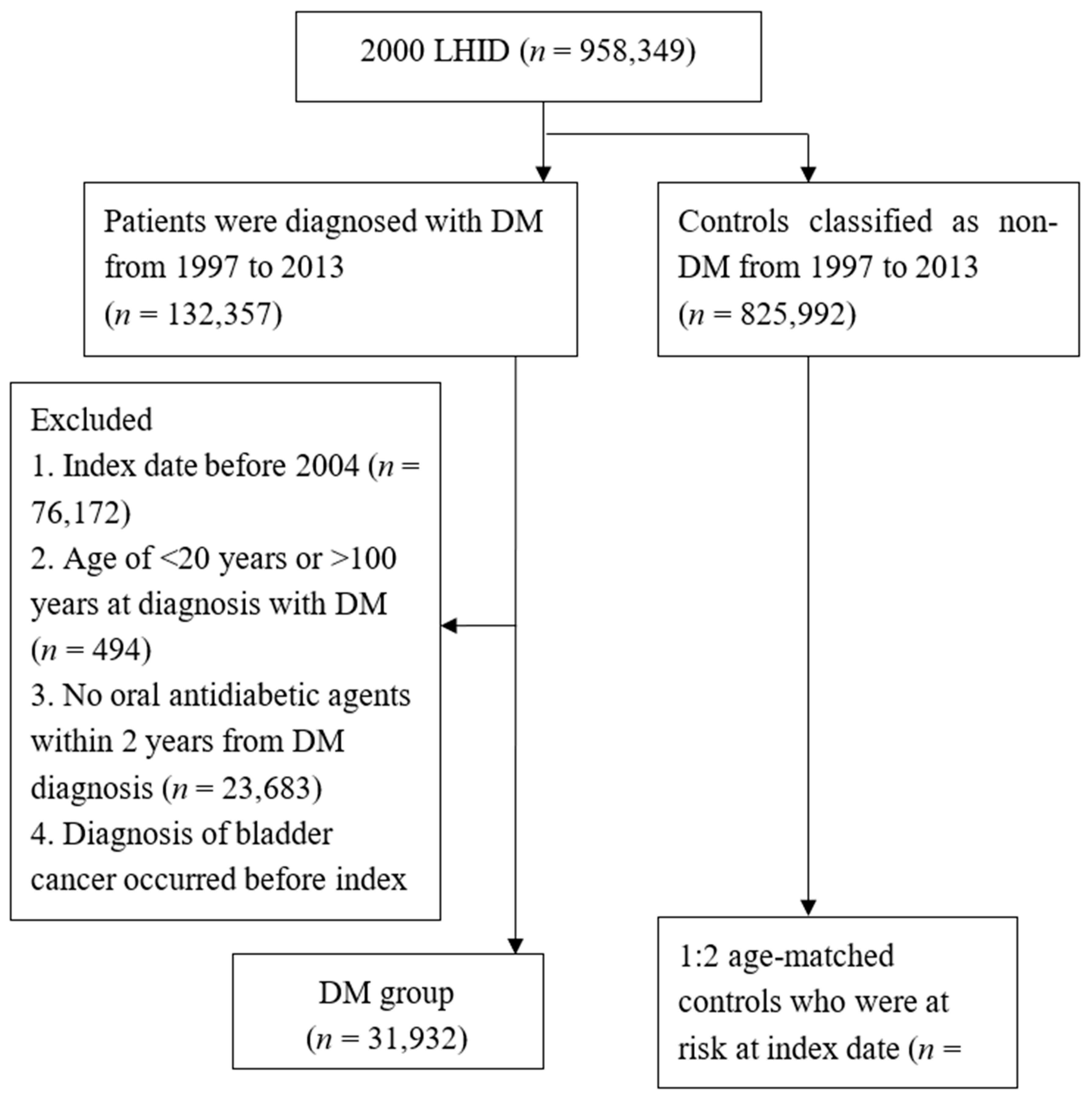
2.2. Patient Selection
2.3. End Points
2.4. Statistical Analysis
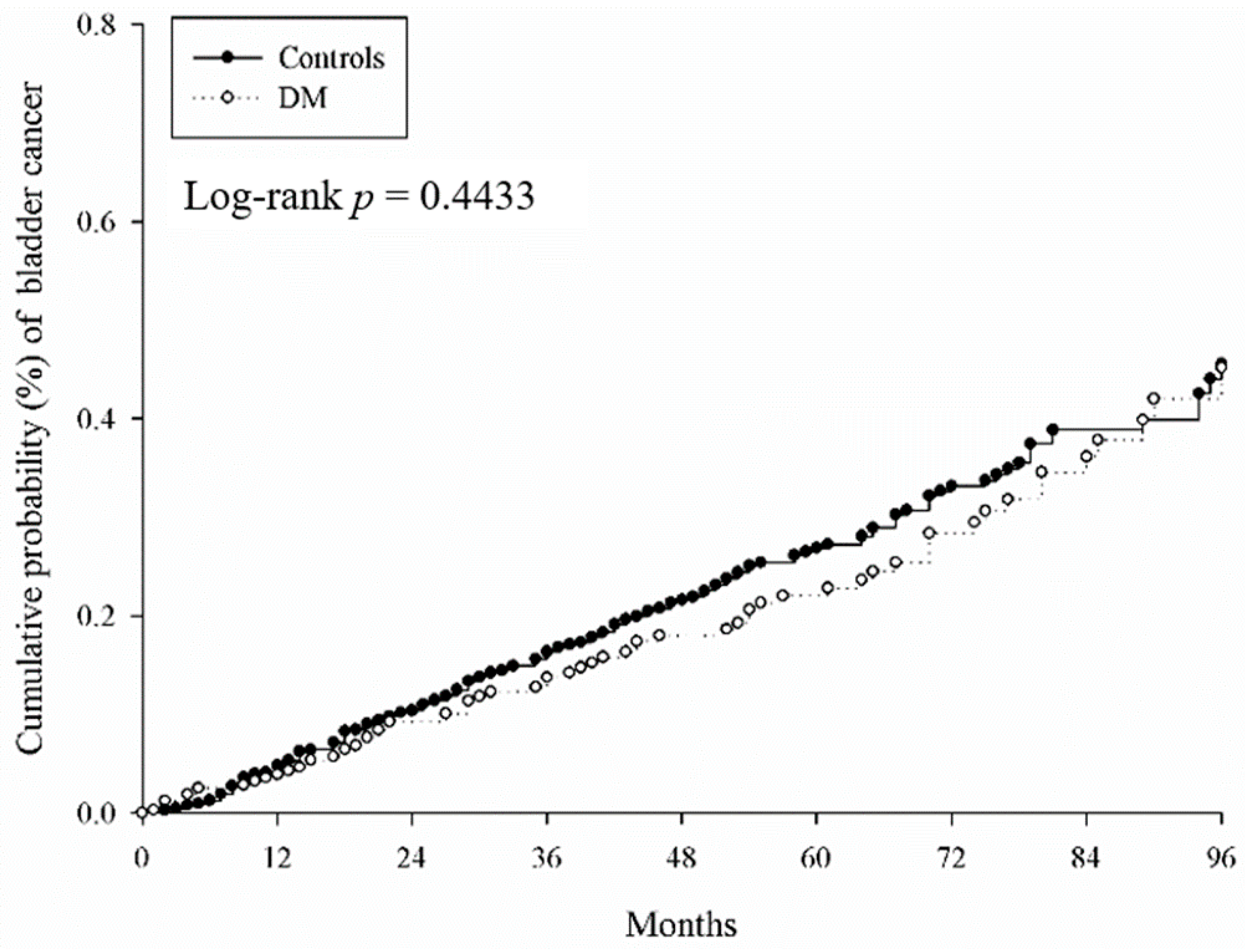
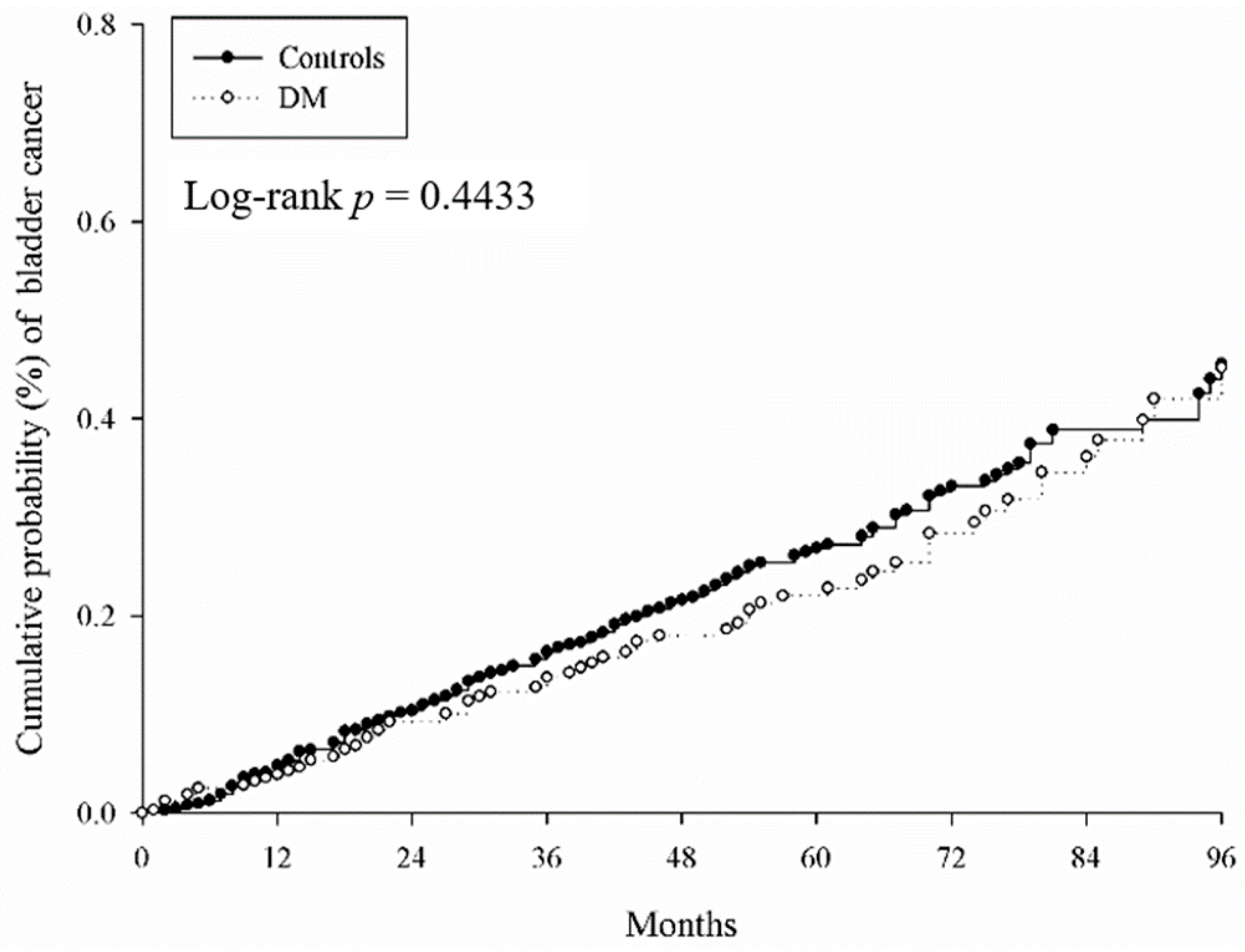
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- American Cancer Society. Available online: https://www.cancer.org/ (accessed on 20 April 2020).
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burger, M.; Catto, J.W.; Dalbagni, G.; Grossman, H.B.; Herr, H.; Karakiewicz, P.; Kassouf, W.; Kiemeney, L.A.; La Vecchia, C.; Shariat, S. Epidemiology and risk factors of urothelial bladder cancer. Eur. Urol. 2013, 63, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Taiwan Cancer Registry. Available online: http://tcr.cph.ntu.edu.tw (accessed on 20 April 2020).
- Pakzad, R.; Mohammadian-Hafshejani, A.; Mohammadian, M.; Pakzad, I.; Safiri, S.; Khazaei, S.; Salehiniya, H. Incidence and mortality of bladder cancer and their relationship with development in Asia. Asian Pac. J. Cancer Prev. 2015, 16, 7365–7374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arabsalmani, M.; Mohammadian-Hafshejani, A.; Ghoncheh, M.; Hadadian, F.; Towhidi, F.; Vafaee, K.; Salehiniya, H. Incidence and mortality of kidney cancers, and human development index in Asia; a matter of concern. J. Nephropathol. 2017, 6, 30. [Google Scholar] [CrossRef]
- Letašiová, S.; Medveďová, A.; Šovčíková, A.; Dušinská, M.; Volkovová, K.; Mosoiu, C.; Bartonová, A. Bladder cancer, a review of the environmental risk factors. Environ. Health 2012, 11, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.-L.; Dzeng, S.R.; Yang, M.-H.; Chiu, K.-H.; Shieh, G.-M.; Wai, C.M. Arsenic species in groundwaters of the blackfoot disease area, Taiwan. Environ. Sci. Technol. 1994, 28, 877–881. [Google Scholar] [CrossRef]
- Morgan, T.M.; Cookson, M.S.; Netto, G.J.; Epstein, J.I. Bladder cancer overview and staging. In The Urinary Tract; Springer: Berlin/Heidelberg, Germany, 2012; pp. 83–112. [Google Scholar]
- Alam, U.; Asghar, O.; Azmi, S.; Malik, R.A. General aspects of diabetes mellitus. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2014; Volume 126, pp. 211–222. [Google Scholar]
- Zaccardi, F.; Webb, D.R.; Yates, T.; Davies, M.J. Pathophysiology of type 1 and type 2 diabetes mellitus: A 90-year perspective. Postgrad. Med. J. 2016, 92, 63–69. [Google Scholar] [CrossRef]
- Roglic, G. WHO Global report on diabetes: A summary. Int. J. Noncommunicable Dis. 2016, 1, 3. [Google Scholar] [CrossRef]
- Kahn, B.B. Type 2 diabetes: When insulin secretion fails to compensate for insulin resistance. Cell 1998, 92, 593–596. [Google Scholar] [CrossRef] [Green Version]
- Smyth, T. Effective management of hypoglycaemia. Nurs. Stand. 2018, 33, 59–66. [Google Scholar] [CrossRef]
- International Diabetes Federation. Available online: https://www.idf.org (accessed on 26 April 2020).
- Fang, H.; Yao, B.; Yan, Y.; Xu, H.; Liu, Y.; Tang, H.; Zhou, J.; Cao, L.; Wang, W.; Zhang, J. Diabetes mellitus increases the risk of bladder cancer: An updated meta-analysis of observational studies. Diabetes Technol. Ther. 2013, 15, 914–922. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, Z.; Wang, X.; Shen, Z.; Lu, Y.; Zhong, S.; Xu, C. Risk of bladder cancer in patients with diabetes mellitus: An updated meta-analysis of 36 observational studies. BMC Cancer 2013, 13, 310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bao, C.; Yang, X.; Xu, W.; Luo, H.; Xu, Z.; Su, C.; Qi, X. Diabetes mellitus and incidence and mortality of kidney cancer: A meta-analysis. J. Diabetes Complicat. 2013, 27, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Huo, R.; Chen, X.; Yu, X. Diabetes mellitus and the risk of bladder cancer: A PRISMA-compliant meta-analysis of cohort studies. Medicine 2017, 96, e8588. [Google Scholar] [CrossRef] [PubMed]
- Ozer, K.; Horsanali, M.O.; Gorgel, S.N.; Ozbek, E. Diabetes is an important risk factor for metastasis in non-muscle-invasive bladder cancer. Asian Pac. J. Cancer Prev. 2016, 17, 105–108. [Google Scholar] [CrossRef] [Green Version]
- Zhang, F.; Yang, Y.; Skrip, L.; Hu, D.; Wang, Y.; Wong, C.; Qiu, J.; Lei, H. Diabetes mellitus and risk of prostate cancer: An updated meta-analysis based on 12 case–control and 25 cohort studies. Acta Diabetol. 2012, 49, 235–246. [Google Scholar] [CrossRef]
- Ogurtsova, K.; da Rocha Fernandes, J.; Huang, Y.; Linnenkamp, U.; Guariguata, L.; Cho, N.H.; Cavan, D.; Shaw, J.; Makaroff, L. IDF Diabetes Atlas: Global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res. Clin. Pract. 2017, 128, 40–50. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Z.; Zhang, X.; Shen, Z.; Zhong, S.; Wang, X.; Lu, Y.; Xu, C. Diabetes mellitus and risk of bladder cancer: A meta-analysis of cohort studies. PLoS ONE 2013, 8, e56662. [Google Scholar] [CrossRef] [Green Version]
- Mu, L.; Zhu, N.; Zhang, J.; Xing, F.; Li, D.; Wang, X. Type 2 diabetes, insulin treatment and prognosis of breast cancer. Diabetes Metab. Res. Rev. 2017, 33, e2823. [Google Scholar] [CrossRef]
- Scappaticcio, L.; Maiorino, M.I.; Bellastella, G.; Giugliano, D.; Esposito, K. Insights into the relationships between diabetes, prediabetes, and cancer. Endocrine 2017, 56, 231–239. [Google Scholar] [CrossRef]
- Pereira, L.X.; da Silva, L.C.A.; de Oliveira Feitosa, A.; Ferreira, R.J.S.; Duarte, A.K.F.; da Conceição, V.; de Sales Marques, C.; Rodrigues, A.K.B.F.; Koike, B.D.V.; de Queiroz, A.C. Correlation between renin-angiotensin system (RAS) related genes, type 2 diabetes, and cancer: Insights from metanalysis of transcriptomics data. Mol. Cell. Endocrinol. 2019, 493, 110455. [Google Scholar] [CrossRef] [PubMed]
- Freedman, N.D.; Silverman, D.T.; Hollenbeck, A.R.; Schatzkin, A.; Abnet, C.C. Association between smoking and risk of bladder cancer among men and women. JAMA 2011, 306, 737–745. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.; Jain, M.; Kapoor, R.; Muruganandham, K.; Srivastava, A.; Mandhani, A. Impact of age and gender on the clinicopathological characteristics of bladder cancer. Indian J. Urol. IJU J. Urol. Soc. India 2009, 25, 207. [Google Scholar]
- Nugent, R.A.; Fathima, S.F.; Feigl, A.B.; Chyung, D. The burden of chronic kidney disease on developing nations: A 21st century challenge in global health. Nephron Clin. Pract. 2011, 118, c269–c277. [Google Scholar] [CrossRef] [PubMed]
- Webster, A.C.; Nagler, E.V.; Morton, R.L.; Masson, P. Chronic kidney disease. Lancet 2017, 389, 1238–1252. [Google Scholar] [CrossRef]
- Hill, N.R.; Fatoba, S.T.; Oke, J.L.; Hirst, J.A.; O’Callaghan, C.A.; Lasserson, D.S.; Hobbs, F.R. Global prevalence of chronic kidney disease–a systematic review and meta-analysis. PLoS ONE 2016, 11, e0158765. [Google Scholar] [CrossRef]
- Tsai, M.-H.; Hsu, C.-Y.; Lin, M.-Y.; Yen, M.-F.; Chen, H.-H.; Chiu, Y.-H.; Hwang, S.-J. Incidence, prevalence, and duration of chronic kidney disease in Taiwan: Results from a community-based screening program of 106,094 individuals. Nephron 2018, 140, 175–184. [Google Scholar] [CrossRef]
- Wong, G.; Hayen, A.; Chapman, J.R.; Webster, A.C.; Wang, J.J.; Mitchell, P.; Craig, J.C. Association of CKD and cancer risk in older people. J. Am. Soc. Nephrol. 2009, 20, 1341–1350. [Google Scholar] [CrossRef] [Green Version]
- Levey, A.; Atkins, R.; Coresh, J.; Cohen, E.; Collins, A.; Eckardt, K.-U.; Nahas, M.; Jaber, B.; Jadoul, M.; Levin, A. Chronic kidney disease as a global public health problem: Approaches and initiatives–a position statement from Kidney Disease Improving Global Outcomes. Kidney Int. 2007, 72, 247–259. [Google Scholar] [CrossRef] [Green Version]
- Weng, P.-H.; Hung, K.-Y.; Huang, H.-L.; Chen, J.-H.; Sung, P.-K.; Huang, K.-C. Cancer-specific mortality in chronic kidney disease: Longitudinal follow-up of a large cohort. Clin. J. Am. Soc. Nephrol. 2011, 6, 1121–1128. [Google Scholar] [CrossRef] [Green Version]
- Rausch, S.; Hennenlotter, J.; Todenhöfer, T.; Aufderklamm, S.; Schwentner, C.; Sievert, K.-D.; Stenzl, A.; Gakis, G. Impaired estimated glomerular filtration rate is a significant predictor for non–muscle-invasive bladder cancer recurrence and progression—Introducing a novel prognostic model for bladder cancer recurrence. Urol. Oncol. Semin. Orig. Investig. 2014, 32, 1178–1183. [Google Scholar] [CrossRef] [PubMed]
- Krabbe, L.-M.; Lotan, Y.; Bagrodia, A.; Gayed, B.A.; Darwish, O.M.; Youssef, R.F.; Bolenz, C.; Sagalowsky, A.I.; Raj, G.V.; Shariat, S.F. Prospective comparison of molecular signatures in urothelial cancer of the bladder and the upper urinary tract—is there evidence for discordant biology? J. Urol. 2014, 191, 926–931. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.-J.; Lee, S.-Y.; Teh, B.T.; Chuang, C.-K.; Nortier, J. Upper tract urothelial carcinomas in patients with chronic kidney disease: Relationship with diagnostic challenge. BioMed Res. Int. 2014, 2014, 989458. [Google Scholar] [CrossRef]
- Miyazaki, J.; Nishiyama, H. Epidemiology of urothelial carcinoma. Int. J. Urol. 2017, 24, 730–734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grollman, A.P. Aristolochic acid nephropathy: Harbinger of a global iatrogenic disease. Environ. Mol. Mutagenesis 2013, 54, 1–7. [Google Scholar] [CrossRef]
- Rosenquist, T.A.; Grollman, A.P. Mutational signature of aristolochic acid: Clue to the recognition of a global disease. DNA Repair 2016, 44, 205–211. [Google Scholar] [CrossRef]
- Kang, C.-H.; Chen, C.-H.; Chiang, P.-H. Primary urothelial carcinoma of the upper urinary tract in dialysis patients with 5-year follow-up. Jpn. J. Clin. Oncol. 2010, 40, 241–246. [Google Scholar] [CrossRef] [Green Version]
- Evers, J.; Grotenhuis, A.J.; Aben, K.K.; Kiemeney, L.A.; Vrieling, A. No clear associations of adult BMI and diabetes mellitus with non-muscle invasive bladder cancer recurrence and progression. PLoS ONE 2020, 15, e0229384. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| Baseline Characteristics | Control n = 63,864 | DM n = 31,932 | ASD |
|---|---|---|---|
| Sex | 0 | ||
| Female | 27,562 (43.16%) | 13,781 (43.16%) | |
| Male | 36,302 (56.84%) | 18,151 (56.84%) | |
| Age (years old) | 0 | ||
| 20–39 | 6596 (10.33%) | 3259 (10.21%) | |
| 40–59 | 33,346 (52.21%) | 16,611 (52.02%) | |
| 60–79 | 20,783 (32.54%) | 10,503 (32.89%) | |
| 80–100 | 3139 (4.92%) | 1559 (4.88%) | |
| Urbanization | 0.129 | ||
| Urban | 38,494 (60.27%) | 18,432 (57.72%) | |
| Suburban | 18,815 (29.46%) | 9756 (30.55%) | |
| Rural | 6555 (10.26%) | 3744 (11.72%) | |
| Low income | 308 (0.48%) | 167 (0.52%) | 0.006 |
| Length of hospital stays † | 0.244 | ||
| 0 days | 58,542 (91.67%) | 28,015 (87.73%) | |
| 1–6 days | 2903 (4.55%) | 1884 (5.90%) | |
| ≥7 days | 2419 (3.79%) | 2033 (6.37%) | |
| Co-morbidity † | |||
| Hypertension | 13,878 (21.73%) | 13,369 (41.87%) | 0.443 |
| Ischemic heart diseases | 4047 (6.34%) | 3454 (10.82%) | 0.161 |
| Hyperlipidemia | 6126 (9.59%) | 5798 (18.16%) | 0.25 |
| Congestive heart failure | 1245 (1.95%) | 1327 (4.16%) | 0.129 |
| Peripheral vascular disease | 697 (1.09%) | 549 (1.72%) | 0.053 |
| Cerebrovascular disease | 2623 (4.11%) | 2112 (6.61%) | 0.111 |
| Dementia | 403 (0.63%) | 266 (0.83%) | 0.024 |
| Chronic pulmonary diseases | 5443 (8.52%) | 3653 (11.44%) | 0.097 |
| Glaucoma | 1027 (1.61%) | 632 (1.98%) | 0.028 |
| Cataract | 4505 (7.05%) | 2499 (7.83%) | 0.029 |
| Rheumatic disease | 580 (0.91%) | 285 (0.89%) | 0.002 |
| Peptic ulcer disease | 6000 (9.39%) | 3562 (11.15%) | 0.058 |
| Kidney disease | 1341 (2.10%) | 935 (2.93%) | 0.053 |
| Liver disease | 5161 (8.08%) | 4315 (13.51%) | 0.176 |
| Hemiplegia or paraplegia | 426 (0.67%) | 314 (0.98%) | 0.035 |
| Coagulation defects | 36 (0.06%) | 29 (0.09%) | 0.013 |
| Incidence | Control (n = 63,864) | DM (n = 31,932) |
|---|---|---|
| Follow-up person-months | 3,274,239 | 1,615,183 |
| New bladder cancer cases | 152 | 67 |
| Incidence (95% CI) * | 0.46 (0.40–0.54) | 0.41 (0.33–0.53) |
| Crude relative risk (95% CI) | Reference | 0.894 (0.670–1.191) |
| Period (Months) | Incidence Rate (95% CI) | aHR (95% CI) | |
|---|---|---|---|
| Control | DM | ||
| 0–36 | 0.48 (0.39–0.59) | 0.39 (0.28–0.55) | 0.786 (0.528–1.168) |
| 36–72 | 0.51 (0.39–0.66) | 0.45 (0.3–0.67) | 0.838 (0.507–1.387) |
| 72–96 | 0.53 (0.32–0.89) | 0.72 (0.39–1.35) | 1.219 (0.531–2.798) |
| p value for time varying test | 0.5541 | ||
| Variable | aHR (95% CI) |
|---|---|
| DM (reference: Control) | 0.842 (0.627–1.13) |
| Sex (reference: Female) | |
| Male | 1.849 (1.393–2.456) |
| Age, years old (reference: 40–59) | |
| 20–39 | 0.314 (0.114–0.864) |
| 60–79 | 2.844 (2.063–3.92) |
| 80–100 | 4.003 (2.393–6.697) |
| Urbanization (reference: Urban) | |
| Suburban | 1.157 (0.867–1.544) |
| Rural | 0.806 (0.51–1.273) |
| Low income | 0.889 (0.124–6.351) |
| Length of hospital stays † (reference: 0 day) | |
| 1–6 days | 1.139 (0.665–1.948) |
| ≥7 days | 1.83 (1.117–3) |
| Co–morbidity † | |
| Hypertension | 1.006 (0.735–1.375) |
| Ischemic heart diseases | 1.321 (0.894–1.952) |
| Hyperlipidemia | 1.231 (0.851–1.781) |
| Congestive heart failure | 0.573 (0.262–1.253) |
| Peripheral vascular disease | 1.301 (0.572–2.959) |
| Cerebrovascular disease | 1.01 (0.606–1.684) |
| Dementia | – |
| Chronic pulmonary diseases | 1.196 (0.823–1.739) |
| Glaucoma | 1.278 (0.64–2.553) |
| Cataract | 1.657 (1.151–2.384) |
| Rheumatic disease | 0.408 (0.057–2.92) |
| Peptic ulcer disease | 1.321 (0.916–1.905) |
| Kidney disease | 3.383 (2.146–5.332) |
| Liver disease | 0.841 (0.538–1.313) |
| Hemiplegia or paraplegia | 0.396 (0.054–2.882) |
| Coagulation defects | - |
| Sub-Group | Incidence * (95% CI) | aHR † (95% CI) | |
|---|---|---|---|
| Non-DM | DM | ||
| Sex | |||
| Female | 0.35 (0.27–0.47) | 0.32 (0.21–0.49) | 0.767 (0.462–1.273) |
| Male | 0.55 (0.45–0.67) | 0.49 (0.36–0.65) | 0.874 (0.608–1.255) |
| p for interaction | 0.8811 | ||
| Age | |||
| 20–39 | 0.09 (0.03–0.27) | 0.06 (0.01–0.41) | 0.133 (0.006–2.829) |
| 40–59 | 0.22 (0.16–0.30) | 0.30 (0.20–0.44) | 1.180 (0.704–1.976) |
| 60–79 | 0.87 (0.71–1.07) | 0.72 (0.52–0.99) | 0.794 (0.537–1.173) |
| 80–100 | 1.60 (1.03–2.48) | 0.53 (0.17–1.66) | 0.307 (0.089–1.063) |
| p for interaction | 0.1356 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pan, Y.; Lee, C.-Y.; Lee, L.-M.; Wen, Y.-C.; Huang, J.-Y.; Yang, S.-F.; Hsiao, C.-H. Incidence of Bladder Cancer in Type 2 Diabetes Mellitus Patients: A Population-Based Cohort Study. Medicina 2020, 56, 441. https://doi.org/10.3390/medicina56090441
Pan Y, Lee C-Y, Lee L-M, Wen Y-C, Huang J-Y, Yang S-F, Hsiao C-H. Incidence of Bladder Cancer in Type 2 Diabetes Mellitus Patients: A Population-Based Cohort Study. Medicina. 2020; 56(9):441. https://doi.org/10.3390/medicina56090441
Chicago/Turabian StylePan, Yueh, Chia-Yi Lee, Liang-Ming Lee, Yu-Ching Wen, Jing-Yang Huang, Shun-Fa Yang, and Chi-Hao Hsiao. 2020. "Incidence of Bladder Cancer in Type 2 Diabetes Mellitus Patients: A Population-Based Cohort Study" Medicina 56, no. 9: 441. https://doi.org/10.3390/medicina56090441
APA StylePan, Y., Lee, C.-Y., Lee, L.-M., Wen, Y.-C., Huang, J.-Y., Yang, S.-F., & Hsiao, C.-H. (2020). Incidence of Bladder Cancer in Type 2 Diabetes Mellitus Patients: A Population-Based Cohort Study. Medicina, 56(9), 441. https://doi.org/10.3390/medicina56090441