First Quantification of Calcium Intake from Calcium-Dense Dairy Products in Dutch Fracture Patients (The Delft Cohort Study)

Abstract
:1. Introduction
2. Experimental Section
Patients and Methods
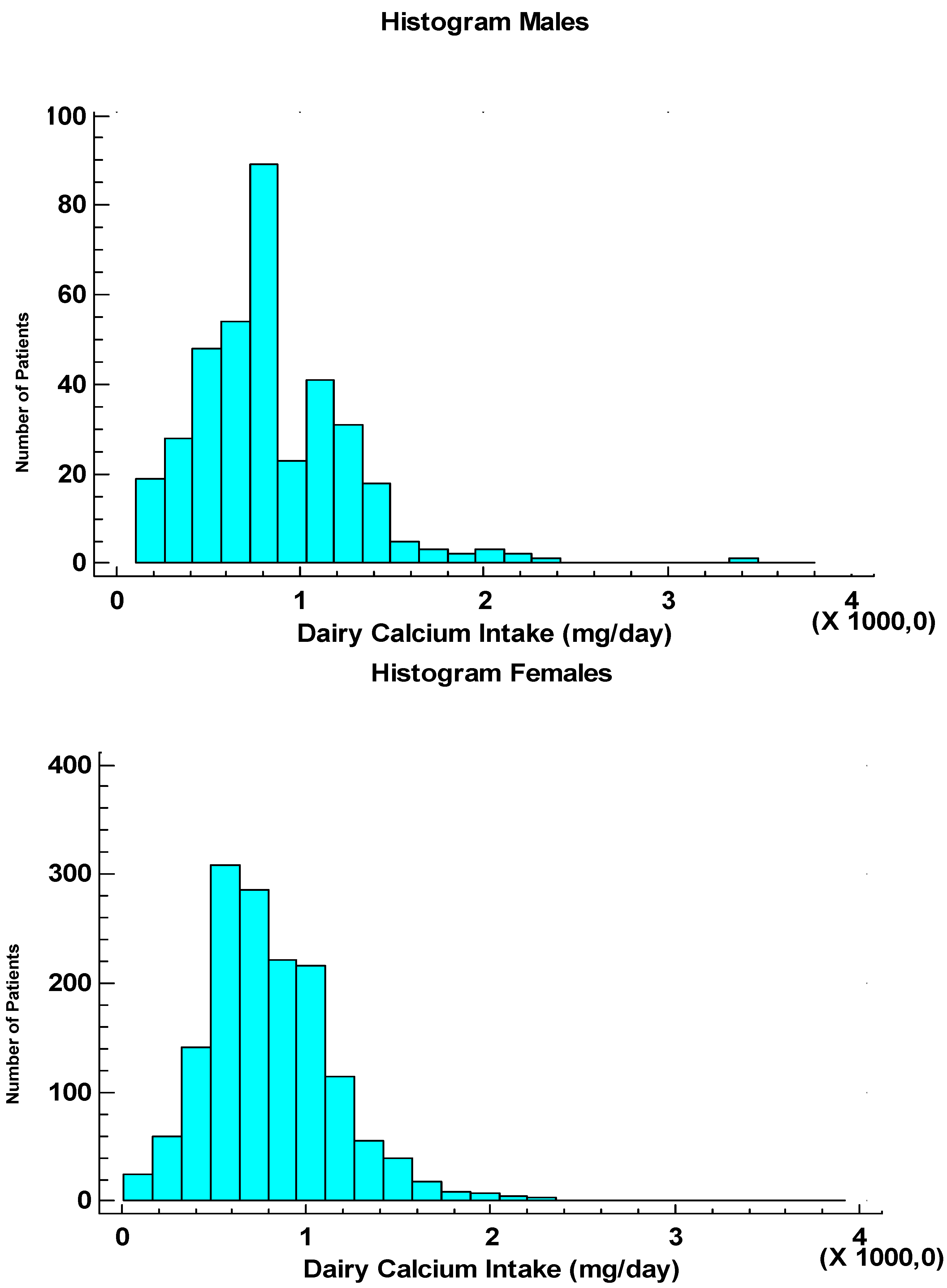
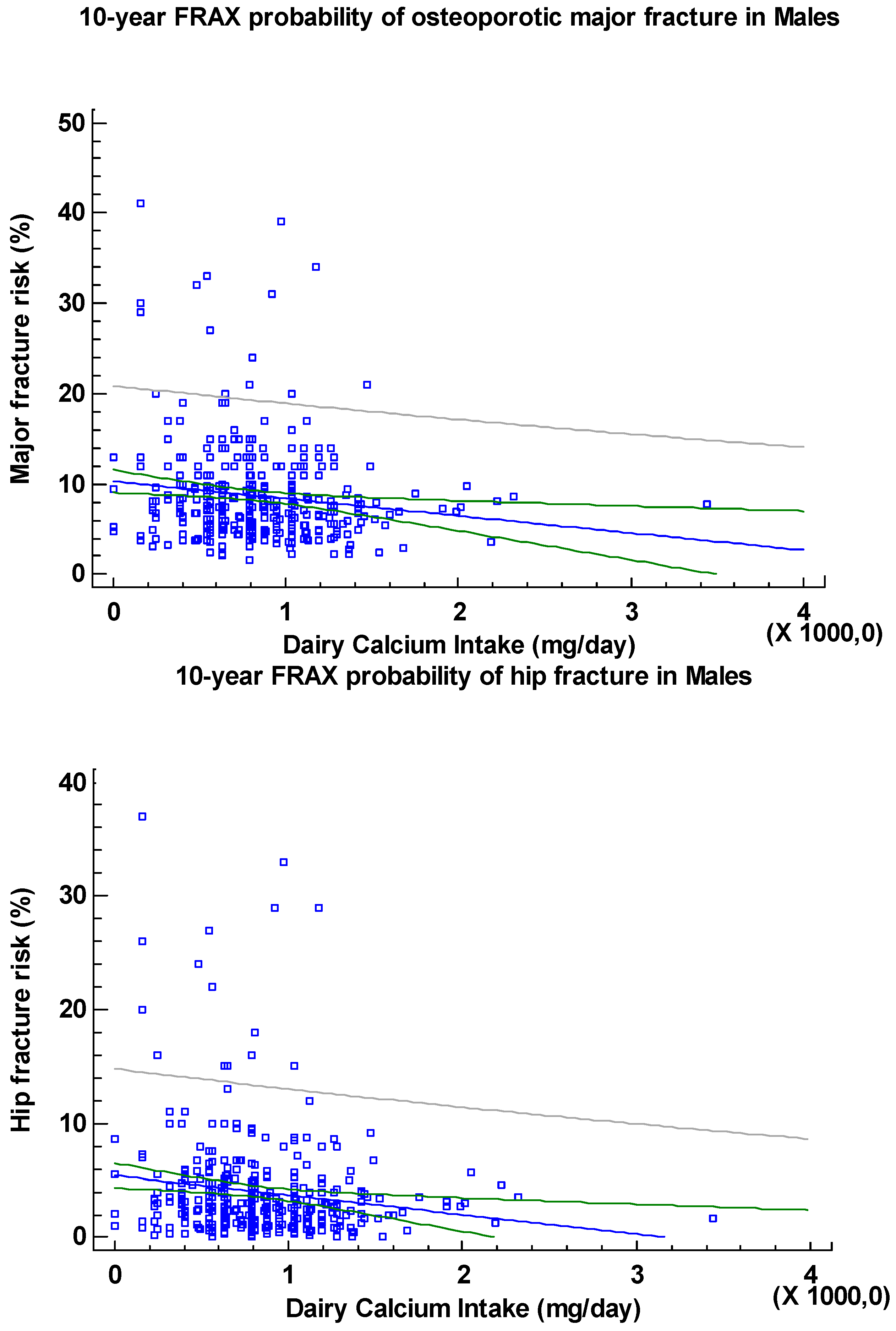
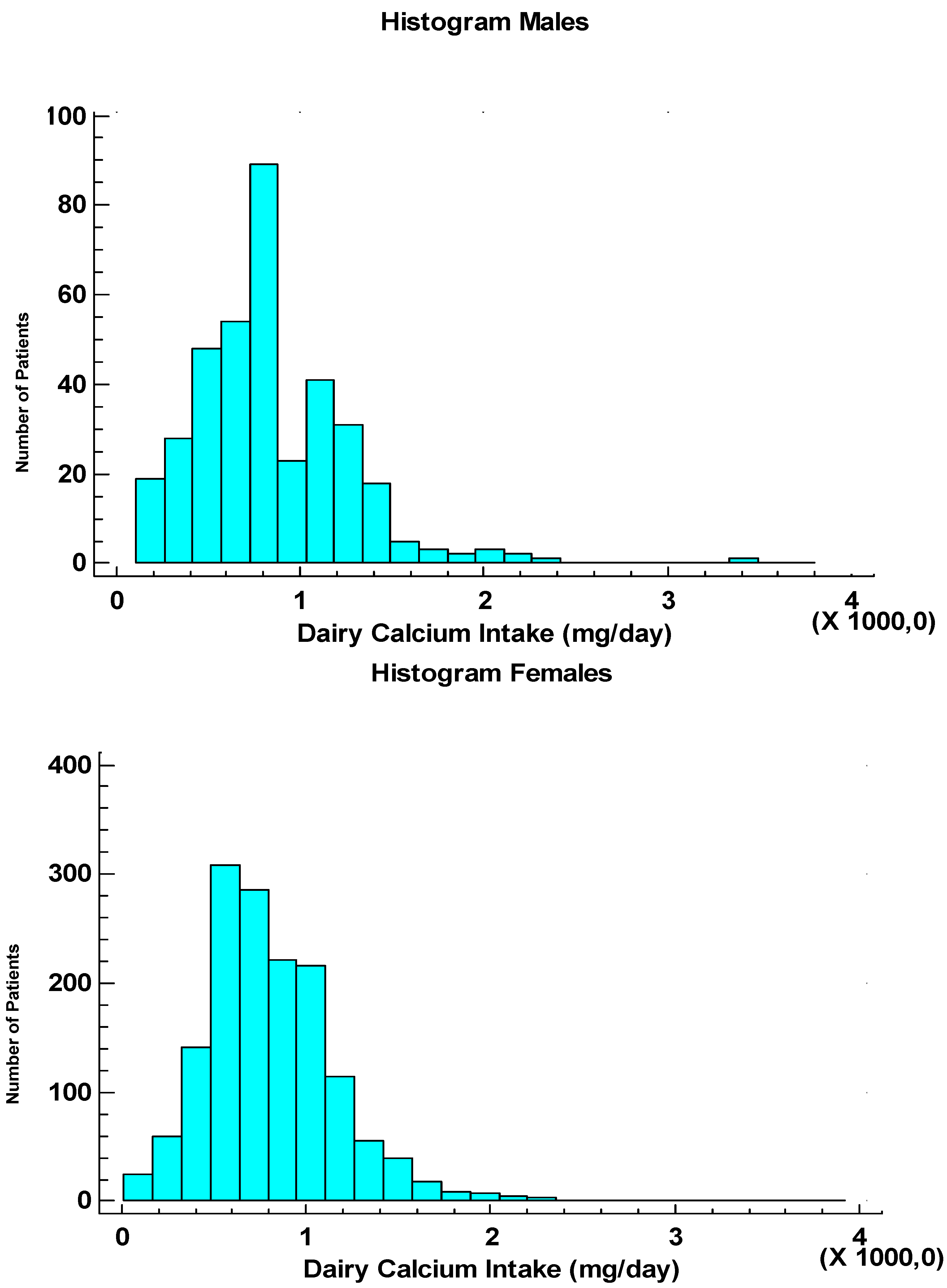
3. Results

{kind=link}
{kind=link}
| Sex | Numbers | Age | % Osteoporosis (T-Score < −2.5 SD) | FRAX, % (for Major Fracture) | FRAX, % (for Hip Fracture) |
|---|---|---|---|---|---|
| Women | 1526 | 66 (50–96) | 13.6 | 11.0 (2.4–90.0) | 2.6 (0.0–73.0) |
| Men | 372 | 65 (50–90) | 6.2 | 7.5 (1.6–41.0) | 2.7 (0.1–37.0) |
| Variables | Data | |
|---|---|---|
| Sex | ||
| Women | 0 | |
| Men | 1 | |
| Age Decades | ||
| 50–59 years | 1 | |
| 60–69 years | 2 | |
| 70–79 years | 3 | |
| 80–89 years | 4 | |
| 90–100 years | 5 | |
| Age at Menopause | age (years), women only | |
| Population Density | ||
| category 1 | 21–250 inhabitants/km2 | |
| category 2 | 250–500 inhabitants/km2 | |
| category 3 | 500–1000 inhabitants/km2 | |
| category 4 | 1000–2500 inhabitants/km2 | |
| category 5 | 2500–5967 inhabitants/km2 | |
| Dairy Calcium Intake | ||
| per serving milk | 270 mg calcium | |
| per serving yoghourt | 240 mg calcium | |
| per serving cheese | 160 mg calcium | |
| Currently Smoking | ||
| No | 0 | |
| Yes | 1 | |
| Alcohol | ||
| ≥3 servings per day | 1 | |
| ≤2 servings per day | 0 | |
| Current use of corticosteroids | ||
| No | 0 | |
| Yes | 1 | |
| Rheumatoid arthritis | ||
| No | 0 | |
| Yes | 1 | |
| Previous fracture | ||
| No | 0 | |
| Yes | 1 | |
| Hip fracture mother | ||
| No | 0 | |
| Yes | 1 | |
| Current use of calcium prescribed or as OTC | Excluded | |
| Current use of any drug against osteoporosis # | Excluded | |
| Length | cm | |
| Weight | kg | |
| BMI | Body Mass Index: Weight/(Length × Length) | |
| BMD | Bone Mineral Density test, BMD-at-the-femoral neck (T-score) | |
| FRAX | 10-year probability of major osteoporotic fracture | |
| FRAX Hip | 10-year probability of hip fracture | |
| Secondary causes for osteoporosis known to the patient | ||
| No | 0 | |
| Yes | 1 | |
| Age (years) | Women W (N = 1526) | Men M (N = 372) | Ratio of Genders W/M |
|---|---|---|---|
| 50–59 | 399 (26.1) | 113 (30.4) | 3.5 |
| 60–69 | 528 (34.6) | 125 (33.6) | 4.2 |
| 70–79 | 428 (28.0) | 96 (25.8) | 4.5 |
| 80–89 | 161 (10.6) | 37 (10.0) | 4.4 |
| 90–100 | 10 (0.7) | 1 (0.2) | 10.0. |
| Age (years) | Women (N = 1526) | Servings/Day |
| 50–59 | 399 (26.1) | 3 (0–9) |
| 60–69 | 528 (34.6) | 3 (0–15) |
| 70–79 | 428 (28.0) | 3 (0–13) |
| 80–89 | 161 (10.6) | 3 (0–8) |
| 90–100 | 10 (0.7) | 3 (2–4) |
| Age (years) | Men (N = 372) | Servings/Day |
| 50–59 | 113 (30.4) | 3 (0–15) |
| 60–69 | 125 (33.6) | 3 (0–9) |
| 70–79 | 96 (25.8) | 3 (0–8) |
| 80–89 | 37 (10.0) | 3 (1–5) |
| 90–100 | 1 (0.2) | 1 |
| Population Density Category (Inhabitants per km2) | Women (N = 1526) | Servings/day |
| 2 (250–500) | 98 (6.4) | 3 (1–10) |
| 3 (500–1000) | 5 (0.3) | 4 (3–5) |
| 4 (1000–2500) | 565 (37.0) | 3 (0–9) |
| 5 (2500–5976) | 858 (56.3) | 3 (0–15) |
| Population Density Category (Inhabitants per km2) | Men (N = 372) | Servings/day |
| 2 (250–500) | 19 (5.1) | 3 (1–6) |
| 3 (500–1000) | 2 (0.5) | 4 (3–5) |
| 4 (1000–2500) | 156 (41.9) | 3 (0–15) |
| 5 (2500–5976) | 195 (52.5) | 3 (0–9) |
| Dairy Calcium Intake (mg/day) | Women (N = 1451) | ||
| DXA T–Score (SD) | |||
| ≥−1 | −1.0 to −2.5 | ≤−2.5 | |
| <500 | 42 (2.9) | 141 (9.7) | 49 (3.4) |
| 500–1000 | 182 (12.5) | 445 (30.7) | 152 (10.5) |
| 1000–1500 | 87 (6.0) | 228 (15.7) | 59 (4.1) |
| 1500–2000 | 12 (0.8) | 34 (2.3) | 6 (0.4) |
| ≥2000 | 4 (0.3) | 7 (0.5) | 3 (0.2) |
| Dairy Calcium Intake (mg/day) | Men (N = 349) | ||
| DXA T–Score (SD) | |||
| ≥−1 | −1.0 to −2.5 | ≤−2.5 | |
| <500 | 12 (3.4) | 37 (10.6) | 9 (2.6) |
| 500–1000 | 53 (15.2) | 118 (33.8) | 14 (4.0) |
| 1000–1500 | 21 (6.0) | 62 (17.8) | 6 (1.7) |
| 1500–2000 | 2 (0.6) | 9 (2.6) | 0 (0.0) |
| ≥2000 | 0 (0.0) | 6 (1.7) | 0 (0.0) |

Comparison between the Current Dutch Cohort and a Cohort from the U.S.
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Cho, K.; Cederholm, T.; Lökk, J. Calcium intake in elderly patients with hip fractures. Food Nutr. Res. 2008, 52. [Google Scholar] [CrossRef]
- Fulgoni, V.L., III; Huth, P.J.; DiRienzo, D.B.; Miller, G.D. Determination of the optimal number of dairy servings to ensure a low prevalence of inadequate calcium intake in Americans. J. Am. Coll. Nutr. 2004, 2, 651–659. [Google Scholar]
- Beasley, J.M.; LaCroix, A.Z.; Neuhouser, M.L.; Huang, Y.; Tinker, L.; Woods, N.; Michael, Y.; Curb, J.D.; Prentice, R.L. Protein intake and incident frailty in the women’s health initiative observational study. J. Am. Geriatr. Soc. 2010, 58, 1063–1071. [Google Scholar] [CrossRef]
- National Institute for Public Health and the Environment RIVM. NEVO-Tabel: Nederlands Voedingsstoffenbestand 2006/Stichting Nederlands Voedingsstoffenbestand. Den Haag: Voedingscentrum, 2006. Available online: http://www.rivm.nl/Onderwerpen/Onderwerpen/N/Nederlands_Voedingsstoffenbestand/Publicaties (accessed on 10 March 2012).
- Dutch Dairy Board. Kerncijfers Belangrijkste Zuivellanden 2010. Available online: http://www.prodzuivel.nl/pz/productschap/publicaties/Kerncijfers/Kerncijfers_belangrijkste_zuivellanden.htm (accessed on 10 March 2012).
- National Institute for Public Health and the Environment RIVM. Dutch National Food Consumption Survey 2007–2010: Diet of Children and Adults Aged 7 to 69 Years. Available online: http://www.rivm.nl/Bibliotheek/Wetenschappelijk/Rapporten/2011/oktober/Dutch_National_Food_Consumption_Survey_2007_2010_Diet_of_children_and_adults_aged_7_to_69_years (accessed on 10 March 2012).
- Dutch Institute for Healthcare Improvement CBO. Richtlijn Osteoporose en Fractuurpreventie. Available online: www.diliguide.nl/document/1015/file/pdf/ (accessed on 19 December 2011).
- McLellan, A.R.; Gallacher, S.J.; Fraser, M.; McQuillian, C. The fracture liaison service: Success of program for the evaluation and management of patients with osteoporotic fracture. Osteoporos. Int. 2003, 14, 1028–1034. [Google Scholar] [CrossRef]
- Hegeman, J.H.; Oskam, J.; van der Palen, J.; Ten Duis, H.J.; Vierhout, P.A. The distal radial fracture in elderly women and the bone mineral density of the lumbar spine and hip. J. Hand Surg. Br. 2004, 29, 473–476. [Google Scholar]
- Kanis, J.A.; Johnell, O.; Oden, A.; Johansson, H.; McCloskey, E. Frax and the assessment of fracture probability in men and women from the UK. Osteoporos. Int. 2004, 19, 385–397. [Google Scholar]
- Lalmohamed, A.; Welsing, P.M.J.; Lems, W.F.; Jacobs, J.W.G.; Kanis, J.A.; Johansson, H.; de Boer, A.; de Vries, F. The Calibration of FRAX® 3.1 to the Dutch population with data on the epidemiology of hip fractures. Osteoporos. Int. 2012, 23, 861–899. [Google Scholar]
- Genant, H.K.; Wu, C.Y.; van Kuijk, C.; Nevitt, M.C. Vertebral fracture assessment using a semiquantitive technique. J. Bone Miner. Res. 1993, 8, 1137–1148. [Google Scholar]
- Dutch National Atlas of Public Health. Bevolkingsdichtheid per Gemeente. Available online: http://www.zorgatlas.nl/beinvloedende-factoren/demografie/groei-en-spreiding/bevolkingsdichtheid-per-gemeente#breadcrumb 2010 (accessed on 14 January 2012).
- Heaney, R.P. Calcium, dairy products and osteoporosis. J. Am. Coll. Nutr. 2000, 19, S83–S99. [Google Scholar] [CrossRef]
- National Osteoporosis Foundation. Clinician’s Guide to Prevention and Treatment of Osteoporosis; National Osteoporosis Foundation: Washington, DC, USA, 2014. [Google Scholar]
- Zhong, Y.; Okoro, C.A.; Balluz, L.S. Association of Total calcium and dietary protein intakes with fractures risk in postmenopausal women: The 1999–2002 National Health and Nutrition Examination Survey (NHANES). Nutrition 2009, 25, 647–654. [Google Scholar] [CrossRef]
- Prentice, A. Diet, Nutrition and the Prevention of Osteoporosis. Public Health Nutr. 2004, 7, 227–243. [Google Scholar] [CrossRef]
- Tang, B.M.; Eslick, G.D.; Nowson, C.; Smith, C.; Bensoussan, A. Use of calcium or calcium in combination with vitamin D supplementation to prevent fractures and bone loss in people aged 50 years or older: A meta-analysis. Lancet 2007, 370, 657–666. [Google Scholar] [CrossRef]
- Heaney, R.P. Dairy and bone health. J. Am. Coll. Nutr. 2009, 28, S82–S90. [Google Scholar] [CrossRef]
- Surdykowski, A.K.; Kenny, A.M.; Insogna, K.L.; Kerstetter, J.E. Optimizing bone health in older adults: The importance of dietary protein. Aging Health 2010, 6, 345–357. [Google Scholar] [CrossRef]
- Warensjö, E.; Byberg, L.; Melhus, H.; Gedeborg, R.; Mallmin, H.; Wolk, A.; Michaëlsson, K. Dietary calcium intake and risk of fracture and osteoporosis: Prospective longitudinal cohort study. BMJ 2011, 342, d1473. [Google Scholar] [CrossRef]
- Bischoff-Ferrari, H.A.; Dawson-Hughes, B.; Baron, J.A.; Burckhardt, P.; Li, R.; Spiegelman, D.; Specker, B.; Orav, J.E.; Wong, J.B.; Staehelin, H.B.; et al. Calcium intake and hip fractures in men and women: A meta-analysis of prospective cohort studies and randomised controlled trails. Am. J. Clin. Nutr. 2007, 86, 1780–1790. [Google Scholar]
- Bischoff-Ferrari, H.A.; Dawson-Hughes, B.; Baron, J.A.; Kanis, J.A.; Orav, E.J.; Staehelin, H.B.; Kiel, D.P.; Burckhardt, P.; Henschkowski, J.; Spiegelman, D.; et al. Milk intake and risk of hip fracture in men and women: A meta analysis of prospective cohort studies. J. Bone Miner. Res. 2011, 26, 833–839. [Google Scholar] [CrossRef]
- Wilt, T.J.; Shaukat, A.; Shamliyan, T.; Taylor, B.C.; MacDonald, R.; Tacklind, J.; Rutks, I.; Schwarzenberg, S.J.; Kane, R.L.; Levitt, M. Lactose Intolerance and Health; Minnesota Evidence-based Practice Center: Minneapolis, MN, USA, 2010. [Google Scholar]
- Feskanich, D.; Willett, W.C.; Colditz, G.A. Calcium, Vitamin D, milk consumption, and hip fractures: A prospective study among postmenopausal women. Am. J. Clin. Nutr. 2003, 77, 504–511. [Google Scholar]
- Cheng, S.Y.; Levy, A.R.; Lefaivre, K.A.; Guy, P.; Kuramoto, L.; Sobolev, B. Geographic trends in incidence of hip fractures: A comprehensive literature review. Osteoporos. Int. 2011, 22, 2575–2586. [Google Scholar] [CrossRef]
- Feskanich, D.; Bischoff-Ferrari, H.A.; Frazier, A.L.; Willett, W.C. Milk consumption during teenage years and risk of hip fractures in older adults. MA Pediatr. 2014, 168, 54–60. [Google Scholar]
- Swallow, D.M. Genetics of lactase persistence and lactose intolerance. Annu. Rev. Genet. 2003, 37, 197–219. [Google Scholar] [CrossRef]
- Scrimshaw, N.S.; Murray, E.B. The acceptability of milk and milk products in populations with a high prevalence of lactose intolerance. Am. J. Clin. Nutr. 1988, 48, 1079–1159. [Google Scholar]
- Suarez, F.L.; Adshead, J.; Furne, J.K.; Levitt, M.D. Lactose maldigestion is not an impediment to the intake of 1500 mg calcium daily as dairy products. Am. J. Clin. Nutr. 1998, 68, 1118–1122. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Van den Berg, P.; Van Haard, P.M.M.; Van den Bergh, J.P.W.; Niesten, D.D.; Van der Elst, M.; Schweitzer, D.H. First Quantification of Calcium Intake from Calcium-Dense Dairy Products in Dutch Fracture Patients (The Delft Cohort Study). Nutrients 2014, 6, 2404-2418. https://doi.org/10.3390/nu6062404
Van den Berg P, Van Haard PMM, Van den Bergh JPW, Niesten DD, Van der Elst M, Schweitzer DH. First Quantification of Calcium Intake from Calcium-Dense Dairy Products in Dutch Fracture Patients (The Delft Cohort Study). Nutrients. 2014; 6(6):2404-2418. https://doi.org/10.3390/nu6062404
Chicago/Turabian StyleVan den Berg, Peter, Paul M. M. Van Haard, Joop P. W. Van den Bergh, Dieu Donné Niesten, Maarten Van der Elst, and Dave H. Schweitzer. 2014. "First Quantification of Calcium Intake from Calcium-Dense Dairy Products in Dutch Fracture Patients (The Delft Cohort Study)" Nutrients 6, no. 6: 2404-2418. https://doi.org/10.3390/nu6062404
APA StyleVan den Berg, P., Van Haard, P. M. M., Van den Bergh, J. P. W., Niesten, D. D., Van der Elst, M., & Schweitzer, D. H. (2014). First Quantification of Calcium Intake from Calcium-Dense Dairy Products in Dutch Fracture Patients (The Delft Cohort Study). Nutrients, 6(6), 2404-2418. https://doi.org/10.3390/nu6062404