Effect of Oral Probiotic Lactobacillus rhamnosus GR-1 and Lactobacillus reuteri RC-14 on the Vaginal Microbiota, Cytokines and Chemokines in Pregnant Women

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
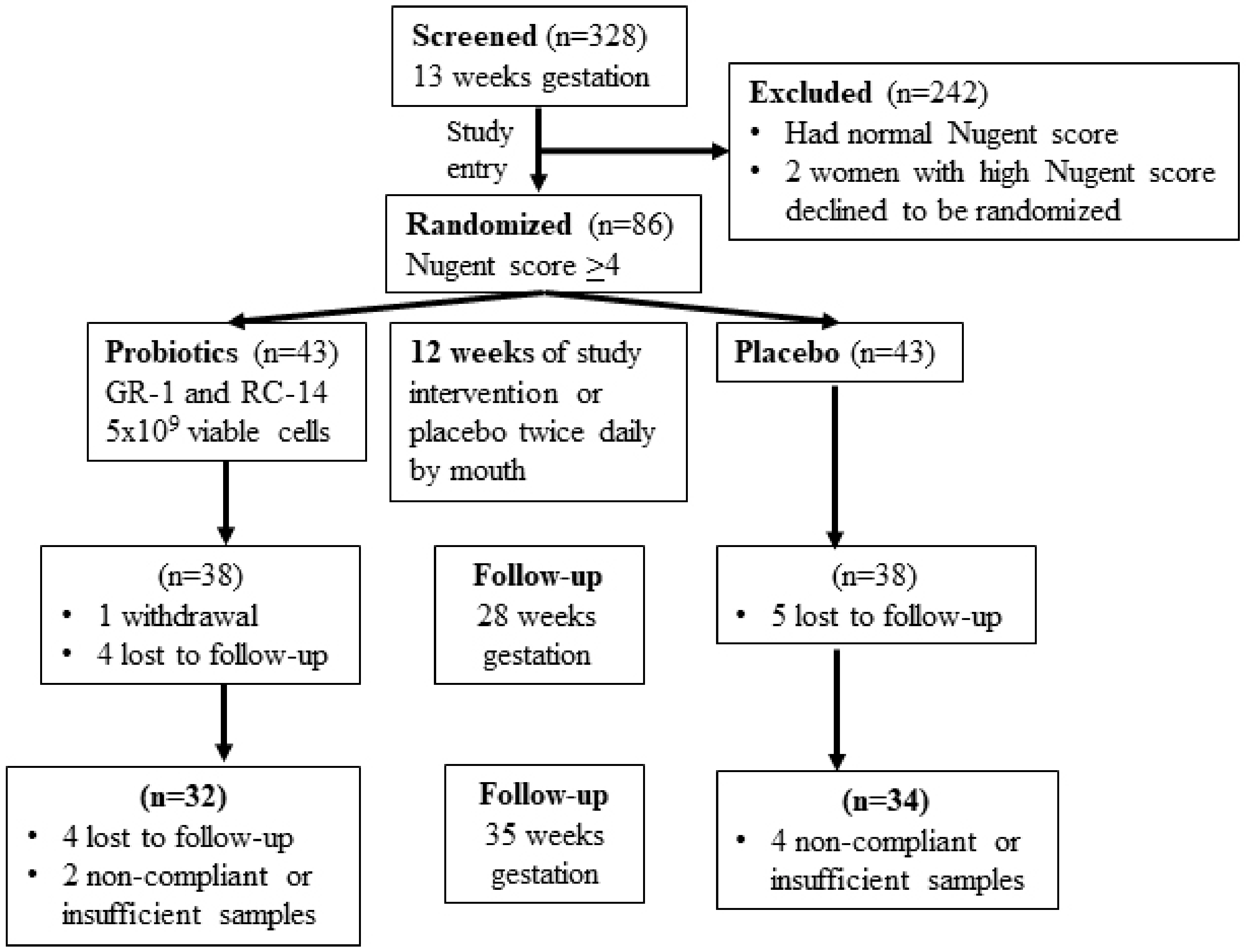
2.1. Study Participants
2.2. Study Groups and Randomization
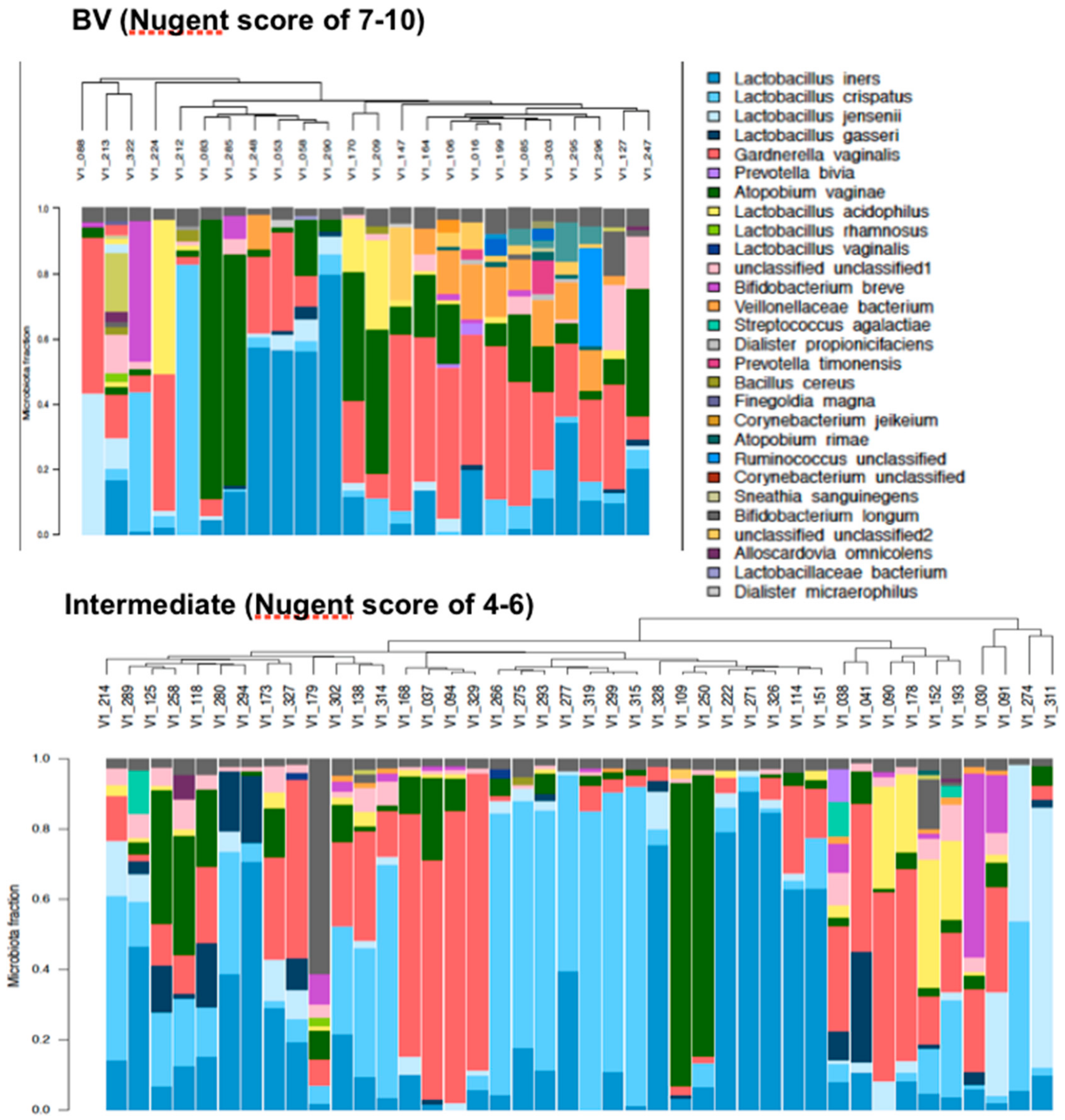
2.3. Nugent Score
2.4. Probiotic Strains
2.5. DNA Isolation and Polymerase Chain Reaction (PCR) Amplification of V6 Region of 16S rDNA
2.6. Sequencing
2.7. Protein Extraction and Cytokine/Chemokine Multiplex Assay
2.8. Statistical Analyses
3. Results
3.1. Pre-Randomization Characteristics
3.2. Pregnancy Outcomes
3.3. Compliance
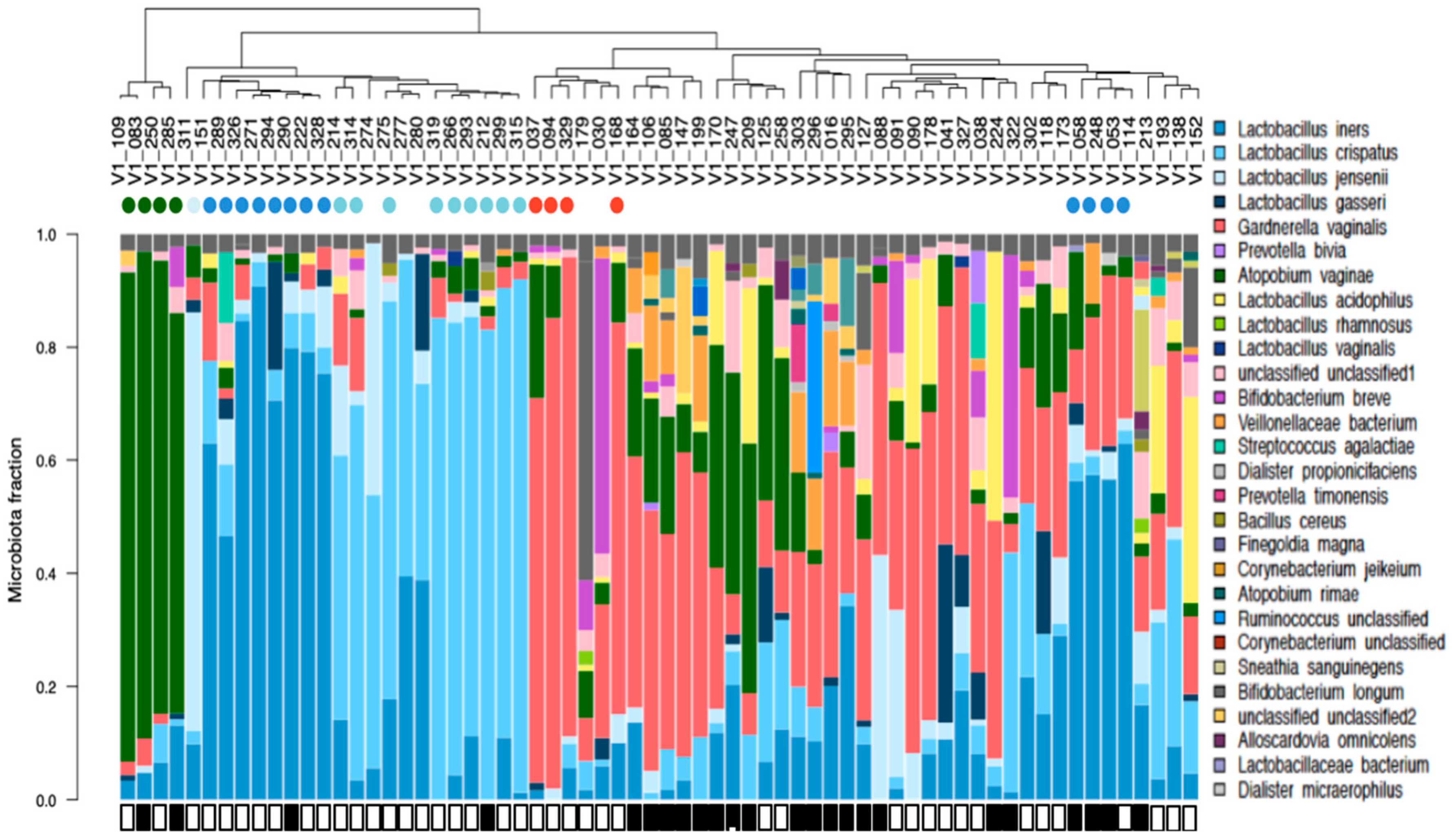
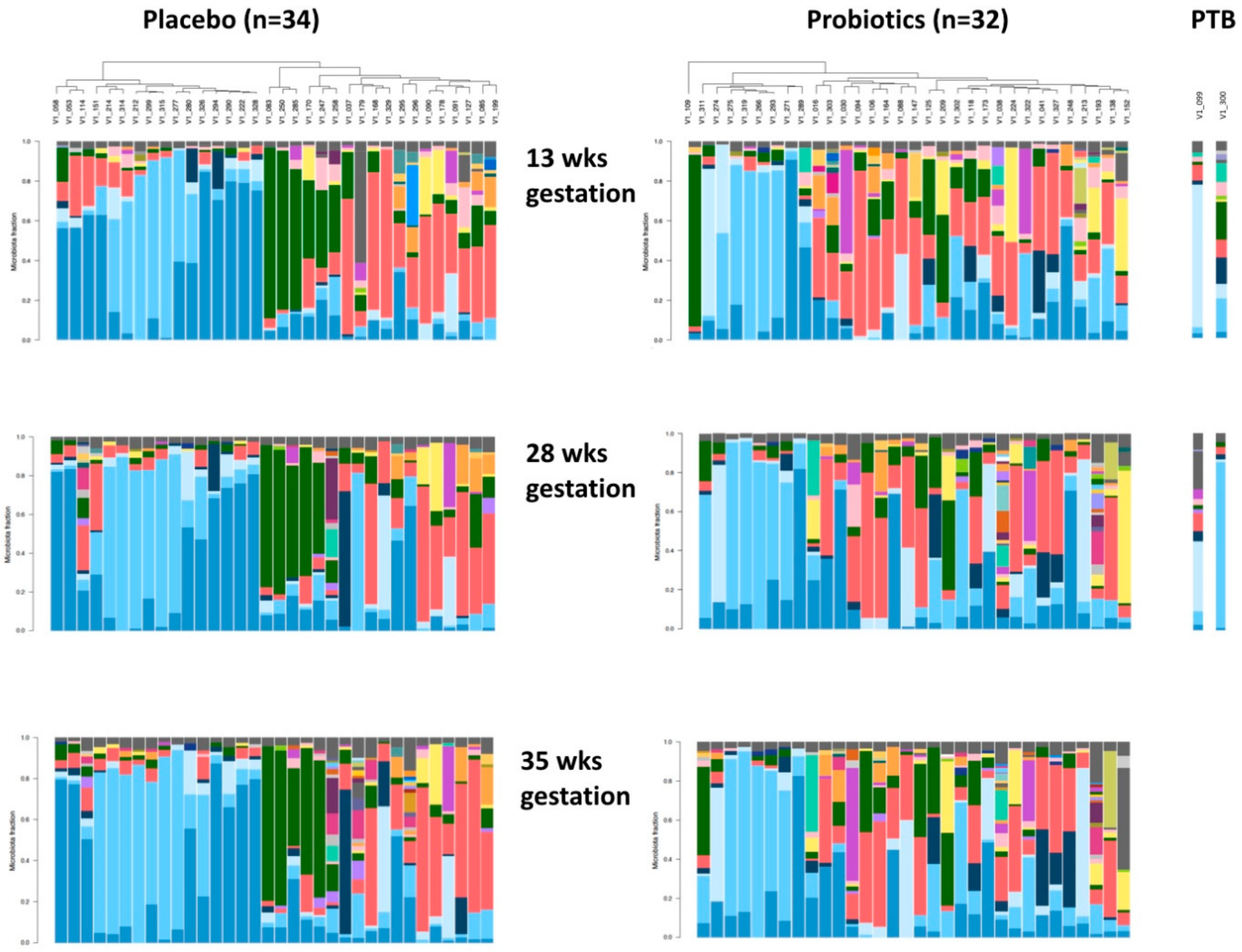
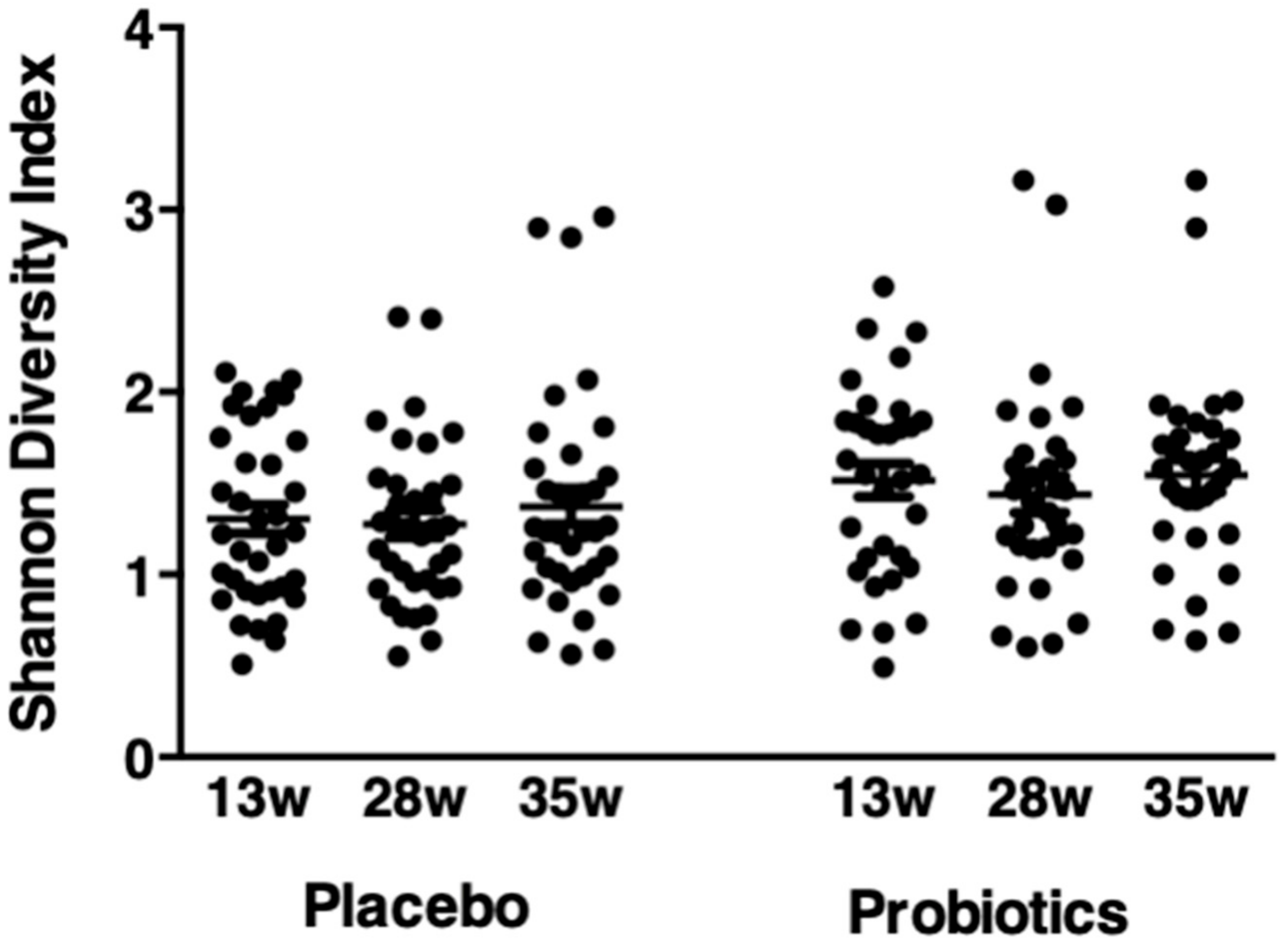
3.4. Vaginal Microbiota
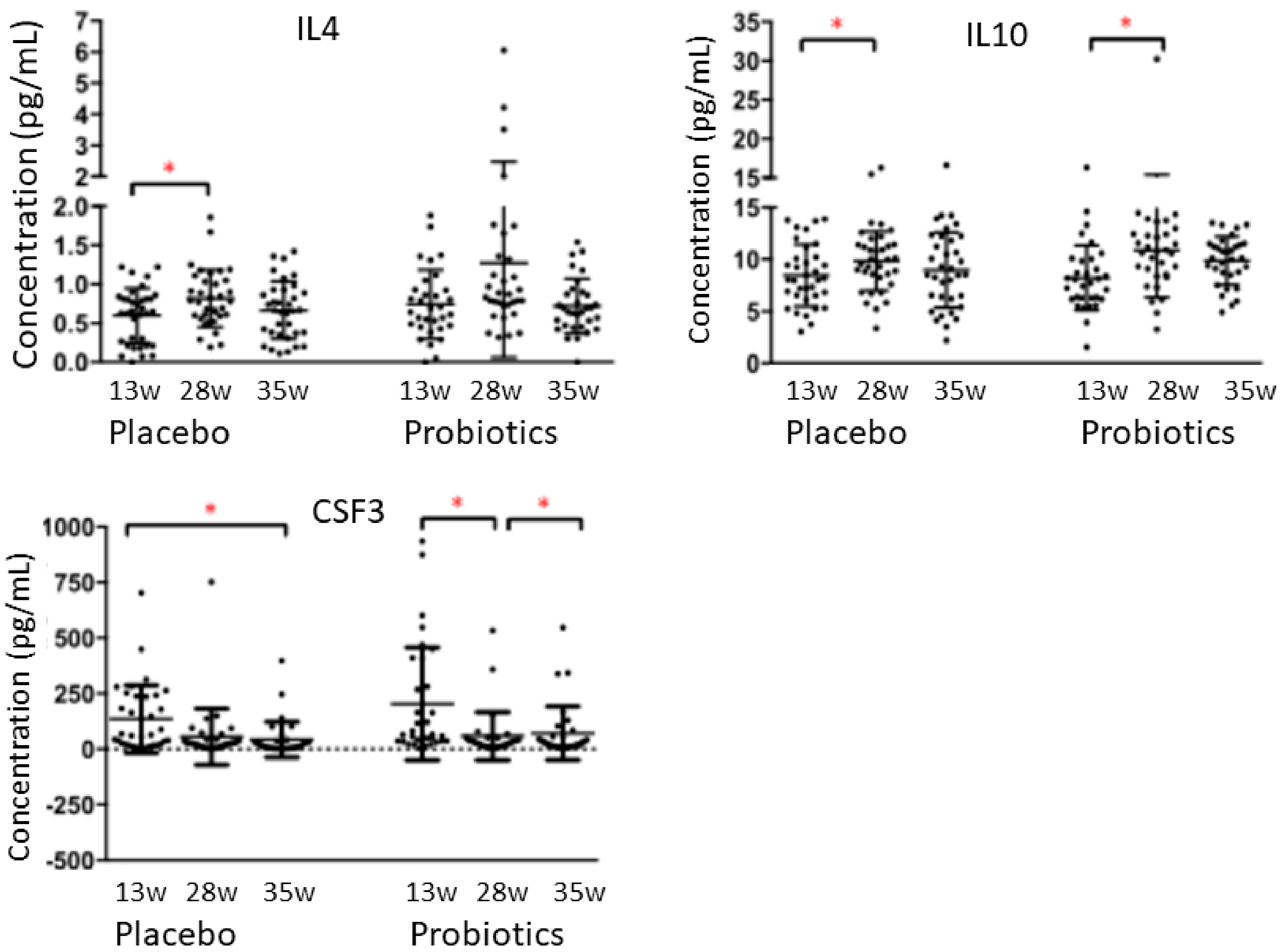
3.5. Cytokines/Chemokines
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Reid, G.; Bocking, A. The potential for probiotics to prevent bacterial vaginosis and preterm labor. Am. J. Obstet. Gynecol. 2003, 189, 1202–1208. [Google Scholar] [CrossRef]
- Donders, G.G.; Van Calsteren, K.; Bellen, G.; Reybrouck, R.; Van den Bosch, T.; Riphagen, I.; Van Lierde, S. Predictive value for preterm birth of abnormal vaginal biota, bacterial vaginosis and aerobic vaginitis during the first trimester of pregnancy. Br. J. Obstet. Gynecol. 2009, 116, 1315–1324. [Google Scholar] [CrossRef] [PubMed]
- Donati, L.; Di Vico, A.; Nucci, M.; Quagliozzi, L.; Spagnuolo, T.; Labianca, A.; Bracaglia, M.; Ianniello, F.; Caruso, A.; Paradisi, G. Vaginal microbial flora and outcome of pregnancy. Arch. Gynecol. Obstet. 2010, 281, 589–600. [Google Scholar] [CrossRef]
- McMillan, A.; Rulisa, S.; Sumarah, M.; Macklaim, J.M.; Renaud, J.; Bisanz, J.E.; Gloor, G.B.; Reid, G. A multi-platform metabolomics approach identifies highly specific biomarkers of bacterial diversity in the vagina of pregnant and non-pregnant women. Sci. Rep. 2015, 21, 14174. [Google Scholar] [CrossRef] [PubMed]
- Keelan, J.A.; Blumenstein, M.; Helliwell, R.J.; Sato, T.A.; Marvin, K.W.; Mitchell, M.D. Cytokines, prostaglandins and parturition--A review. Placenta 2003, 24, S33–S46. [Google Scholar] [CrossRef] [PubMed]
- Challis, J.R.; Lockwood, C.J.; Myatt, L.; Norman, J.E.; Strauss, J.F., 3rd; Petraglia, F. Inflammation and pregnancy. Reprod. Sci. 2009, 16, 206–215. [Google Scholar] [CrossRef]
- Balkus, J.; Agnew, K.; Lawler, R.; Mitchell, C.; Hitti, J. Effects of pregnancy and bacterial vaginosis on proinflammatory cytokine and secretory leukocyte protease inhibitor concentrations in vaginal secretions. J. Pregnancy 2010, 2010, 385981. [Google Scholar] [CrossRef]
- Holst, R.M.; Hagberg, H.; Wennerholm, U.B.; Skogstrand, K.; Thorsen, P.; Jacobsson, B. Prediction of microbial invasion of the amniotic cavity in women with preterm labor: Analysis of multiple proteins in amniotic and cervical fluids. Br. J. Obstet. Gynecol. 2011, 118, 240–249. [Google Scholar] [CrossRef]
- Nugent, R.P.; Krohn, M.A.; Hillier, S.L. Reliability of diagnosing bacterial vaginosis is improved by a standardized method of gram stain interpretation. J. Clin. Microbiol. 1991, 29, 297–301. [Google Scholar] [CrossRef]
- Gloor, G.B.; Hummelen, R.; Macklaim, J.M.; Dickson, R.J.; Fernandes, A.D.; MacPhee, R.; Reid, G. Microbiome profiling by illumina sequencing of combinatorial sequence-tagged PCR products. PLoS ONE 2010, 5, e15406. [Google Scholar] [CrossRef]
- Hummelen, R.; Fernandes, A.D.; Macklaim, J.M.; Dickson, R.J.; Changalucha, J.; Gloor, G.B.; Reid, G. Deep sequencing of the vaginal microbiota of women with HIV. PLoS ONE 2010, 5, e12078. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, S.; Hoffman, N.G.; Morgan, M.T.; Matsen, F.A.; Fiedler, T.L.; Hall, R.W.; Ross, F.J.; McCoy, C.O.; Bumgarner, R.; Marrazzo, J.M.; et al. Bacterial communities in women with bacterial vaginosis: High resolution phylogenetic analyses reveal relationships of microbiota to clinical criteria. PLoS ONE 2012, 7, e37818. [Google Scholar] [CrossRef] [PubMed]
- Romero, R.; Hassan, S.S.; Gajer, P.; Tarca, A.L.; Fadrosh, D.W.; Nikita, L.; Galuppi, M.; Lamont, R.F.; Chaemsaithong, P.; Miranda, J.; et al. The composition and stability of the vaginal microbiota of normal pregnant women is different from that of non-pregnant women. Microbiome 2014, 2, 4. [Google Scholar] [CrossRef] [PubMed]
- Romero, R.; Hassan, S.S.; Gajer, P.; Tarca, A.L.; Fadrosh, D.W.; Bieda, J.; Chaemsaithong, P.; Miranda, J.; Chaiworapongsa, T.; Ravel, J. The vaginal microbiota of pregnant women who subsequently have spontaneous preterm labor and delivery and those with a normal delivery at term. Microbiome 2014, 2, 18. [Google Scholar] [CrossRef]
- Aagaard, K.; Riehle, K.; Ma, J.; Segata, N.; Mistretta, T.A.; Coarfa, C.; Raza, S.; Rosenbaum, S.; Van den Veyver, I.; Milosavljevic, A.; et al. A metagenomic approach to characterization of the vaginal microbiome signature in pregnancy. PLoS ONE 2012, 7, e36466. [Google Scholar] [CrossRef]
- Chaban, B.; Links, M.G.; Jayaprakash, T.P.; Wagner, E.C.; Bourque, D.K.; Lohn, Z.; Albert, A.Y.; van Schalkwyk, J.; Reid, G.; Hemmingsenk, S.M.; et al. Characterization of the vaginal microbiota of healthy Canadian women through the menstrual cycle. Microbiome 2014, 2, 23. [Google Scholar] [CrossRef]
- Verstraelen, H.; Vilchez-Vargas, R.; Desimpel, F.; Jauregui, R.; Vankeirsbilck, N.; Weyers, S.; Verhelst, R.; De Sutter, P.; Pieper, D.H.; Van De Wiele, T. Characterisation of the human uterine microbiome in non-pregnant women through deep sequencing of the V1-2 region of the 16S rRNA gene. PeerJ 2016, 4, e1602. [Google Scholar] [CrossRef]
- FAO/WHO. Joint FAO/WHO expert consultation on evaluation of health and nutritional properties of probiotics in food. 2001. Available online: http://www.fao.org/3/a-a0512e.pdf (accessed on 28 January 2020).
- Homayouni, A.; Bastani, P.; Ziyadi, S.; Mohammad-Alizadeh-Charandabi, S.; Ghalibaf, M.; Mortazavian, A.M.; Mehrabany, E.V. Effects of probiotics on the recurrence of bacterial vaginosis: A review. J. Low. Genit. Tract Dis. 2014, 18, 79–86. [Google Scholar] [CrossRef]
- Macklaim, J.M.; Clemente, J.C.; Knight, R.; Gloor, G.B.; Reid, G. Changes in vaginal microbiota following antimicrobial and probiotic therapy. Microb. Ecol. Health Dis. 2015, 26, 27799. [Google Scholar] [CrossRef]
- Reid, G. Probiotic agents to protect the urogenital tract against infection. Am. J. Clin. Nutr. 2001, 73, 437S–443S. [Google Scholar] [CrossRef]
- Reid, G.; Brigidi, P.; Burton, J.P.; Contractor, N.; Duncan, S.; Fargier, E.; Hill, C.; Lebeer, S.; Martín, R.; McBain, A.J.; et al. Microbes central to human reproduction. Am. J. Reprod. Immunol. 2015, 73, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Walsh, C.J.; Guinane, C.M.; O’Toole, P.W.; Cotter, P.D. Beneficial modulation of the gut microbiota. FEBS Lett. 2014, 588, 4120–4130. [Google Scholar] [CrossRef]
- Reid, G.; Charbonneau, D.; Kochanowski, B.; Beuerman, D.; Poehner, R.; Bruce, A.W. Oral use of Lactobacillus rhamnosus GR-1 and L. fermentum RC-14 significantly alters vaginal flora: Randomized, placebo-controlled trial in 64 healthy women. FEMS Immunol. Med. Microbiol. 2003, 35, 131–134. [Google Scholar] [CrossRef]
- Yeganegi, M.; Watson, C.S.; Martins, A.; Kim, S.O.; Reid, G.; Challis, J.R.; Bocking, A.D. Effect of Lactobacillus rhamnosus GR-1 supernatant and fetal sex on lipopolysaccharide-induced cytokine and prostaglandin-regulating enzymes in human placental trophoblast cells: Implications for treatment of bacterial vaginosis and prevention of preterm labor. Am. J. Obstet. Gynecol. 2009, 200, e1–e8. [Google Scholar]
- Yeganegi, M.; Leung, C.G.; Martins, A.; Kim, S.O.; Reid, G.; Challis, J.R.; Bocking, A.D. Lactobacillus rhamnosus GR-1 stimulates colony-stimulating factor 3 (granulocyte) (CSF3) output in placental trophoblast cells in a fetal sex-dependent manner. Biol. Reprod. 2011, 84, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Yang, S.; Kim, S.O.; Reid, G.; Challis, J.R.; Bocking, A.D. Lipopolysaccharide-induced profiles of cytokine, chemokine, and growth factors produced by human decidual cells are altered by Lactobacillus rhamnosus GR-1 supernatant. Reprod. Sci. 2014, 21, 939–947. [Google Scholar] [CrossRef]
- Kim, S.O.; Sheikh, H.I.; Ha, S.D.; Martins, A.; Reid, G. G-CSF-mediated inhibition of JNK is a key mechanism for Lactobacillus rhamnosus-induced suppression of TNF production in macrophages. Cell. Microbiol. 2006, 8, 1958–1971. [Google Scholar] [CrossRef]
- Yang, S.; Li, W.; Challis, J.R.; Reid, G.; Kim, S.O.; Bocking, A.D. Probiotic Lactobacillus rhamnosus GR-1 supernatant prevents lipopolysaccharide-induced preterm birth and reduces inflammation in pregnant CD-1 mice. Am. J. Obstet. Gynecol. 2014, 211, e1–e44. [Google Scholar] [CrossRef]
- Aitchison, J. The Statistical Analysis of Compositional Data; Chapman and Hall: London, UK, 1986. [Google Scholar]
- Gloor, G.B.; Wu, J.R.; Pawlowsky-Glahn, V.; Egozcue, J.J. It’s all relative: Analyzing microbiome data as compositions. Ann. Epidemiol. 2016, 26, 322–329. [Google Scholar] [CrossRef]
- Gloor, G.B.; Macklaim, J.M.; Vu, M.; Fernandes, A.D. Compositional uncertainty should not be ignored in high-throughput sequencing data analysis. Aus. J. Stat. 2016, 45, 73–87. [Google Scholar] [CrossRef]
- Fernandes, A.D.; Macklaim, J.M.; Linn, T.G.; Reid, G.; Gloor, G.B. ANOVA- like differential expression analysis for mixed population RNA-seq. PLoS ONE 2013, 8, e67019. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, A.D.; Reid, J.N.; Macklaim, J.M.; McMurrough, T.M.; Edgell, D.R.; Gloor, G.B. Unifying the analysis of high-throughput sequencing datasets: Characterizing RNA-seq, 16S rRNA gene sequencing and selective growth experiments by compositional data analysis. Microbiome 2014, 2, 15. [Google Scholar] [CrossRef] [PubMed]
- Magurran, A.E. Measuring Biological Diversity; Wiley-Blackwell: Malden, MA, USA, 2004. [Google Scholar]
- Kramer, M.S.; Platt, R.W.; Wen, S.W.; Joseph, K.S.; Allen, A.; Abrahamowicz, M.; Blondel, B.; Bréart, G. Fetal/Infant Health Study Group of the Canadian Perinatal Surveillance System. A new and improved population-based Canadian reference for birth weight for gestational age. Pediatrics 2001, 108, e35. [Google Scholar] [CrossRef] [PubMed]
- Krauss-Silva, L.; Moreira, M.E.; Alves, M.B.; Braga, A.; Camacho, K.G.; Batista, M.R.; Almada-Horta, A.; Rebello, M.R.; Guerra, F. A randomised controlled trial of probiotics for the prevention of spontaneous preterm delivery associated with bacterial vaginosis: Preliminary results. Trials 2011, 12, 239. [Google Scholar] [CrossRef]
- Menard, J.P.; Fenollar, F.; Henry, M.; Bretelle, F.; Raoult, D. Molecular quantification of Gardnerella vaginalis and Atopobium vaginae loads to predict bacterial vaginosis. Clin. Infect. Dis. 2008, 47, 33–43. [Google Scholar] [CrossRef]
- Antonio, M.A.; Meyn, L.A.; Murray, P.J.; Busse, B.; Hillier, S.L. Vaginal colonization by probiotic Lactobacillus crispatus CTV-05 is decreased by sexual activity and endogenous lactobacilli. J. Infect. Dis. 2009, 199, 1506–1513. [Google Scholar] [CrossRef]
- Gille, C.; Böer, B.; Marschal, M.; Urschitz, M.S.; Heinecke, V.; Hund, V.; Speidel, S.; Tarnow, I.; Mylonas, I.; Franz, A.; et al. Effect of probiotics on vaginal health in pregnancy. EFFPRO, a randomized controlled trial. Am. J. Obstet. Gynecol. 2016, 215, 608.e1–608.e7. [Google Scholar] [CrossRef]
- Ravel, J.; Gajer, P.; Abdo, Z.; Schneider, G.M.; Koenig, S.S.; McCulle, S.L.; Karlebach, S.; Gorle, R.; Russell, J.; Tacket, C.O.; et al. Vaginal microbiome of reproductive-age women. Proc. Natl. Acad. Sci. USA 2011, 108, 4680–4687. [Google Scholar] [CrossRef]
- Reid, G. Cervico-vaginal microbiomes—Threats and possibilities. Trends Endocronol. Metabol. 2016, 27, 446–454. [Google Scholar] [CrossRef]
- Pramanick, R.; Mayadeo, N.; Warke, H.; Begum, S.; Aich, P.; Aranha, C. Vaginal microbiota of asymptomatic bacterial vaginosis and vulvovaginal candidiasis: Are they different from normal microbiota? Microb. Pathog. 2019, 134, 103599. [Google Scholar] [CrossRef]
- Walsh, A.M.; Crispie, F.; Kilcawley, K.; O’Sullivan, O.; O’Sullivan, M.G.; Claesson, M.J.; Cotter, P.D. Microbial succession and flavor production in the fermented dairy beverage Kefir. mSystems 2016, 1, e00052-16. [Google Scholar] [CrossRef] [PubMed]
- Park, D.H. Effects of carbon dioxide on metabolite production and bacterial communities during kimchi fermentation. Biosci. Biotechnol. Biochem. 2018, 82, 1234–1242. [Google Scholar] [CrossRef] [PubMed]
- Milani, C.; Alessandri, G.; Mancabelli, L.; Lugli, G.A.; Longhi, G.; Anzalone, R.; Viappiani, A.; Duranti, S.; Turroni, F.; Ossiprandi, M.C.; et al. Bifidobacterial distribution across Italian cheeses produced from raw milk. Microorganisms 2019, 7, 599. [Google Scholar] [CrossRef]
- Menezes, L.A.A.; Sardaro, M.L.S.; Duarte, R.T.D.; Mazzon, R.R.; Neviani, E.; Gatti, M.; De Dea Lindner, J. Sourdough bacterial dynamics revealed by metagenomic analysis in Brazil. Food Microbiol. 2020, 85, 103302. [Google Scholar] [CrossRef] [PubMed]
- Ling, Z.; Kong, J.; Liu, F.; Zhu, H.; Chen, X.; Wang, Y.; Li, L.; Nelson, K.E.; Xia, Y.; Xiang, C. Molecular analysis of the diversity of vaginal microbiota associated with bacterial vaginosis. BMC Genomics 2010, 11, 488. [Google Scholar] [CrossRef] [PubMed]
- Costa de Freitas, A.; Chaban, B.; Bocking, A.; Money, D.M.; Hill, J.E.; the VOGUE Study team. Characterization of the vaginal microbiome in pregnancy. Genome 2014, 57, 373. [Google Scholar]
- Fettweis, J.M.; Serrano, M.G.; Brooks, J.P.; Edwards, D.J.; Girerd, P.H.; Parikh, H.I.; Huang, B.; Arodz, T.J.; Edupuganti, L.; Glascock, A.L.; et al. The vaginal microbiome and preterm birth. Nat. Med. 2019, 25, 1012–1021. [Google Scholar] [CrossRef]
- Gardiner, G.E.; Heinemann, C.; Bruce, A.W.; Beuerman, D.; Reid, G. Persistence of Lactobacillus fermentum RC-14 and Lactobacillus rhamnosus GR-1 but not L. rhamnosus GG in the human vagina as demonstrated by randomly amplified polymorphic DNA. Clin. Diagn. Lab. Immunol. 2003, 9, 92–96. [Google Scholar] [CrossRef]
- Verdenelli, M.C.; Cecchini, C.; Coman, M.M.; Silvi, S.; Orpianesi, C.; Coata, G.; Cresci, A.; Di Renzo, G.C. Impact of probiotic SYNBIO® administered by vaginal suppositories in promoting vaginal health of apparently healthy women. Curr. Microbiol. 2016, 73, 483–490. [Google Scholar] [CrossRef]
- Nenadic, D.B.; Pavlovic, M.D. Cervical fluid cytokines in pregnant women: Relation to vaginal wet mount findings and polymorphonuclear leukocyte counts. Eur. J. Obstet. Gynecol. Reprod. Biol. 2008, 140, 165–170. [Google Scholar] [CrossRef]
- Chandiramani, M.; Seed, P.T.; Orsi, N.M.; Ekbote, U.V.; Bennett, P.R.; Shennan, A.H.; Tribe, R.M. Limited relationship between cervico-vaginal fluid cytokine profiles and cervical shortening in women at high risk of spontaneous preterm birth. PLoS ONE 2012, 7, e52412. [Google Scholar] [CrossRef] [PubMed]
- Whitcomb, B.W.; Schisterman, E.F.; Luo, X.; Chegini, N. Maternal serum granulocyte colony-stimulating factor levels and spontaneous preterm birth. J. Womens Health (Larchmt) 2009, 18, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Dugoua, J.J.; Machado, M.; Zhu, X.; Chen, X.; Koren, G.; Einarson, T.R. Probiotic safety in pregnancy: A systematic review and meta-analysis of randomized controlled trials of Lactobacillus, Bifidobacterium, and Saccharomyces spp. J. Obstet. Gynaecol. Can. 2009, 31, 542–552. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristic | Probiotic Group n = 43 (%) | Placebo Group n = 43 (%) |
|---|---|---|
| Maternal Age (years) | 33.8 ± 4.2 | 34.4 ± 3.3 |
| Pre-pregnancy Body Mass Index | 22.5 ± 3.2 | 22.4 ± 3.1 |
| Week of vaginal swab collection | 13.2 ± 1.1 | 13.3 ± 1.1 |
| Ethnicity * | ||
| Caucasian | 18 (56.3) | 22 (64.8) |
| South Asian | 2 (6.2) | 3 (8.8) |
| East Asian | 6 (18.8) | 7 (20.6) |
| Black | 2 (6.2) | 0 |
| Hispanic | 2 (6.2) | 2 (6.2) |
| Mixed | 1 (3.1) | 0 |
| Other | 1 (3.1) | 0 |
| Mode of conception | ||
| Natural | 40 (93) | 40 (93) |
| Assisted | 3 (7) | 3 (7) |
| Ovulation induction | 1 | 1 |
| IVF | 0 | 1 |
| Intracystoplasmic sperm injection | 0 | 1 |
| Donor sperm | 1 | 0 |
| IUI | 1 | 0 |
| Pre-existing medical conditions | 17 (39.5) | 27 (62.8) |
| Depression/anxiety disorder | 1 | 9 |
| Endocrine disorders | 5 | 3 |
| Hematological | 1 | 3 |
| Musculoskeletal | 2 | 3 |
| Gastrointestinal | 0 | 3 |
| Cardiovascular | 2 | 0 |
| Genitourinary/Urinary/Gynecological | 4 | 1 |
| Respiratory | 0 | 4 |
| Others | 2 | 1 |
| Previous surgeries in past 10 years | 16 (37.2) | 34 (79) |
| Obstetrical/gynecological | 12 | 23 |
| Others | 4 | 11 |
| Current medications | 16 (37.2) | 22 (51.2) |
| Anti-nauseants | 1 | 3 |
| Vitamin D | 1 | 1 |
| Antidepressants | 2 | 4 |
| Natural supplements | 5 | 2 |
| Thyroid medications | 4 | 1 |
| Analgesics | 0 | 1 |
| Iron supplements | 1 | 3 |
| Gastrointestinal medications | 2 | 1 |
| Asthma medications | 0 | 5 |
| Others | 0 | 1 |
| Fermented food ingested during pregnancy | 35 (81.4) | 41 (95.4) |
| Natural supplement | 2 (4.7) | 2 (4.7) |
| Labour and Delivery Characteristics | Probiotic Group n = 41 (%) | Placebo Group n = 43 (%) |
|---|---|---|
| Antibiotics during pregnancy * | 6 (14.6) | 5 (11.6) |
| Antibiotics during labor and delivery | 19 (46.3) | 16 (37.2) |
| Induction of labor | 8 (19.5) | 9 (20.9) |
| Mode of Delivery | ||
| Vaginal | 33 (80.5) | 34 (79.1) |
| Spontaneous | 28/33 (84.9) | 28/34 (82.4) |
| Assisted | 5/33 (15.2) | 6/34 (17.7) |
| C-section | 8 (19.5) | 9 (20.9) |
| Emergency | 6/8 (75.0) | 2/9 (22.2) |
| Elective | 2/8 (25.0) | 7/9 (77.8) |
| Gestational age at delivery (weeks) | 39.1 ± 1.4 | 39.4 ± 0.9 |
| Birth weight (g) | 3340 ± 433.7 | 3351 ± 463.5 |
| IUGR (<3rd percentile) | 0 | 1 (2.3) |
| Preterm birth (<37 weeks of gestation) | 2 (4.9) | 0 |
| Apgar score <7 at 5 minutes | 1 (2.4) | 0 |
| Fetal Sex | ||
| Male | 19 (46.3) | 24 (55.8) |
| Female | 22 (53.7) | 19 (44.2) |
| Cord blood pH | 7.26 ± 0.07 | 7.26 ± 0.08 |
| Placebo Group | Probiotic Group | ||||||
|---|---|---|---|---|---|---|---|
| Species | 13 Weeks | 28 Weeks | 35 Weeks | 13 Weeks | 28 Weeks | 35 Weeks | p-Value |
| Lactobacillus iners | 10.7 ± 2.7 a’ | 10.5 ± 2.5 a’ | 10.1 ± 2.5 b’ | 9.8 ± 2.1 a | 9.8 ± 2.5 a | 9.5 ± 2.4 a | 0.006 |
| Gardnerella vaginalis | 10.3 ± 2.4 a’ | 10.0 ± 2.2 a’ | 9.3 ± 2.4 b’ | 10.5 ± 2.4 a | 9.9 ± 2.4 b | 9.6 ± 2.5 b | <0.002 |
| Atopobium vaginae | 9.4 ± 2.2 a’ | 9.3 ± 2.2 a’ | 8.8 ± 2.2 b’ | 9.0 ± 2.3 a | 8.6 ± 2.4 b | 8.7 ± 2.4 a,b | 0.002 |
| Lactobacillus acidophilus | 6.6 ± 2.6 a’ | 5.7 ± 2.7 b’ | 5.3 ± 2.7 c’ | 6.8 ± 2.5 a | 6.4 ± 2.4 a | 6.4 ± 2.4 a | <0.006 |
| Atopobium rimae | 2.8 ± 2.2 a’ | 2.3 ± 2.3 a’ | 1.6 ± 2.3 b’ | 2.5 ± 2.3 a | 1.9 ± 2.0 b | 1.7 ± 2.6 b | <0.002 |
| Bacillus cereus | 2.8 ± 2.5 a’ | 1.6 ± 2.4 b’c’ | 1.9 ± 2.2 c’ | 2.5 ± 2.9 a | 1.5 ± 2.9 b | 1.7 ± 2.9 b | <0.001 |
| Lactobacillaceae bacterium | 1.6 ± 3.2 a’ | −0.7 ± 1.4 b’ | −1.3 ± 1.5 c’ | −0.2 ± 2.5 a | −1.2 ± 1.6 b | −1.4 ± 1.2 b | <0.008 |
| Escherichia coli | 1.2 ± 1.8 a’ | −0.7 ± 1.7 b’ | −0.2 ± 2.1 b’ | 1.3 ± 2.5 a | −0.4 ± 2.1 b | 0.0 ± 1.9 b | <0.002 |
| Desulfotomaculum halophilum | 1.4 ± 2.6 a’ | 0.4 ± 2.6 b’ | −0.8 ± 2.4 c’ | 0.5 ± 2.5 a | −0.9 ± 2.1 b | −1.1 ± 2.3 b | <0.002 |
| Streptococcus thermophiles | −0.3 ± 2.3 a’ | −2.4 ± 1.3 b’ | −2.4 ± 1.6 b’ | 0.2 ± 2.3 a | −1.7 ± 1.6 a | −2.3 ± 1.6 a | <0.006 |
| Erythrobacter flavus | −1.7 ± 2.4 a’ | −3.0 ± 1.1 b’ | −3.1 ± 1.4 b’ | −1.4 ± 2.6 a | −2.6 ± 1.7 b | −2.9 ± 1.6 b | <0.006 |
| Prevotella denticola | −2.5 ± 0.8 a’ | −2.8 ± 1.8 a’ | −3.4 ± 1.0 b’ | −2.2 ± 1.0 a | −2.7 ± 1.2 a,b | −3.1 ± 1.1 b | <0.003 |
| Placebo Group | Probiotic Group | ||||||
|---|---|---|---|---|---|---|---|
| Species | 13 Weeks | 28 Weeks | 35 Weeks | 13 Weeks | 28 Weeks | 35 Weeks | p-Value |
| Corynebacterium pseudogenitalium | −0.9 ± 1.5 a’ | 0.4 ± 1.6 b’ | 1.0 ± 1.8 c’ | −1.1 ± 1.8 a | 1.0 ± 2.4 b | 1.0 ± 1.7 b | <0.002 |
| Facklamia hominis | −1.6 ± 1.0 a’ | −1.4 ± 1.4 a’ | −0.8 ± 1.8 b’ | −1.8 ± 1.1 a | −0.9 ± 1.6 b | −1.0 ± 1.6 b | <0.004 |
| Corynebacterium amycolatum | −1.9 ± 0.9 a’ | −1.1 ± 1.5 b’ | −0.5 ± 1.8 c’ | −1.6 ± 1.0 a | −0.7 ± 1.7 b | −0.3 ± 1.1 b | <0.008 |
| Clostridiales coagulans | −1.8 ± 0.9 a’ | −1.0 ± 1.7 b’ | −0.3 ± 2.0 c’ | −1.9 ± 1.0 a | −1.3 ± 1.8 b | −1.3 ± 1.7 b | <0.003 |
| Varibaculum cambriense | −1.7 ± 1.0 a’ | −0.4 ± 1.8 b’ | 0.0 ± 1.7 b’ | −1.6 ± 1.3 a | −0.7 ± 1.5 b | −0.5 ± 1.8 b | <0.005 |
| Campylobacter ureolyticus | −2.0 ± 0.9 a’ | −1.8 ± 1.7 b’ | −1.1 ± 1.5 b’ | −1.6 ± 1.6 a | −1.6 ± 1.6 a | −1.4 ± 2.1 b | <0.004 |
| Corynebacterium coyleae | −2.2 ± 1.4 a’ | −1.1 ± 2.4 b’ | −1.4 ± 2.4 b’ | −2.1 ± 1.1 a | −1.7 ± 1.6 b | −1.7 ± 1.5 b | <0.002 |
| Prevotella disiens | −0.9 ± 1.5 a’ | 0.4 ± 1.6 b’ | 1.0 ± 1.8 b’ | −1.1 ± 1.8 a | 1.0 ± 2.4 a | 1.0 ± 1.7 a | <0.003 |
| Cryptobacterium curtum | −1.6 ± 1.0 a’ | −1.4 ± 1.4 a’ | −0.8 ± 1.8 b’ | −1.8 ± 1.1 a | −0.9 ± 1.6 a | −1.0 ± 1.6 b | <0.005 |
| Placebo Group (n = 33) | Probiotic Group (n = 31) | |||||
|---|---|---|---|---|---|---|
| 13 Weeks | 28 Weeks | 35 Weeks | 13 Weeks | 28 Weeks | 35 Weeks | |
| IL·1J3 | 121.3 ± 186.6 a’ | 80.7 ± 171.6 a’ | 72.2 ± 166.8 a’ | 199.7 ± 404.2 a | 66.4 ± 143.3 a | 82.3 ± 113.2 a |
| IL-2 | 0.6 ± 0.7 a’ | 0.6 ± 0.6 a’ | 0.4 ± 0.5 a’ | 0.4 ± 0.6 a | 1.2 ± 2.8 a | 0.6 ± 0.6 a |
| IL-4 | 0.6 ± 0.4 a’ | 0.8 ± 0.4 b’ | 0.7 ± 0.4 a’,b’ | 0.8 ± 0.4 a | 1.3 ± 1.2 a | 0.7 ± 0.4 a |
| IL-5 | 0.3 ± 0.3 a’ | 0.4 ± 0.5 a’ | 0.4 ± 0.3 a’ | 0.6 ± 1.2 a | 1.1 ± 2.1 a | 0.5 ± 0.3 a |
| IL-6 | 15.1 ± 30.5 a’ | 4.1 ± 5.6 a’ | 3.4 ± 5.0 a’ | 36.0 ± 71.1 a | 6.3 ± 10.7 a | 5.3 ± 8.0 a |
| IL-7 | 56.0 ± 121.4 a’ | 34.6 ± 33.7 a’ | 29.9 ± 37.1 a’ | 55.4 ± 117.5 a | 90.4 ± 269.4 a | 29.3 ± 36.2 a |
| IL-8 | 1453.9 ± 2230.1 a’ | 1155.8 ± 2716.0 a’ | 604.4 ± 985.1 a’ | 2068.0 ± 4658.2 a | 418.2 ± 442.6 a | 855.0 ± 1258.5 a |
| IL-9 | 7.9 ± 16.2 a’ | 4.6 ± 4.1 a’ | 4.5 ± 6.7 a’ | 6.4 ± 12.1 a | 16.5 ± 57.3 a | 3.8 ± 3.8 a |
| IL-10 | 8.4 ± 2.9 a’ | 10.0 ± 2.7 b’ | 9.0 ± 3.6 a’,b’ | 8.4 ± 3.2 a | 11.0 ± 4.6 b | 9.9 ± 2.4 a,b |
| IL-12p70 | 57.8 ± 89.8 a’ | 55.0 ± 47.0 a’ | 44.6 ± 38.1 a’ | 50.3 ± 72.7 a | 90.0 ± 217.5 a | 41.4 ± 22.1 a |
| IL-13 | 4.7 ± 8.8 a’ | 3.4 ± 2.1 a’ | 3.3 ± 3.0 a’ | 5.1 ± 9.8 a | 9.7 ± 27.8 a | 3.1 ± 2.8 a |
| IL-15 | 1.0 ± 1.1 a’ | 1.3 ± 1.5 a’ | 0.8 ± 0.9 a’ | 1.0 ± 1.0 a | 1.6 ± 1.6 a | 0.8 ± 0.9 a |
| IL-17 | 4.3 ± 2.7 a’ | 5.0 ± 2.6 a’ | 3.7 ± 1.8 a’ | 4.3 ± 2.6 a | 7.7 ± 7.1 a | 3.8 ± 1.8 a |
| CCL2 | 10.7 ± 17.4 a’ | 8.4 ± 4.3 a’ | 6.8 ± 4.6 a’ | 10.6 ± 13.3 a | 11.6 ± 10.2 a | 9.5 ± 8.5 a |
| CCL3 | 1.9 ± 1.5 a’ | 1.5 ± 1.0 a’ | 1.6 ± 1.8 a’ | 3.7 ± 6.1 a | 1.7 ± 1.4 a | 1.6 ± 0.9 a |
| CCL4 | 9.1 ± 9.5 a’ | 5.6 ± 8.8 a’ | 5.0 ± 13.4 a’ | 21.1 ± 48.8 a | 3.8 ± 3.3 a | 6.3 ± 7.6 a |
| CCL5 | 32.8 ± 134.4 a’ | 3.8 ± 1.5 a’. | 2.9 ± 1.4 a’ | 10.0 ± 33.8 a | 4.4 ± 3.1 a | 3.3 ± 1.5 a |
| CCL11 | 11.2 ± 19.4 a’ | 14.6 ± 36.7 a’ | 7.2 ± 9.6 a’ | 6.6 ± 11.8 a | 24.8 ± 78.1 a | 11.0 ± 12.7 a |
| CSF2 | 15.1 ± 13.2 a’ | 12.1 ± 7.0 a’ | 9.4 ± 7.1 a’ | 13.0 ± 12.0 a | 21.9 ± 45.6 a | 9.2 ± 6.4 a |
| CSF3 | 131.9 ± 156.2 ’ | 58.1 ± 129.8 a’,b’ | 44.2 ± 81.1 b’ | 204.6 ± 253.5 a | 60.5 ± 109.5 b | 73.4 ± 122.0 a |
| CXCL10 | 1346.5 ± 3779.0 a’ | 639.9 ± 762.5 a’ | 309.7 ± 354.0 a’ | 512.7 ± 1064.9 a | 682.6 ± 1371.7 a | 581.2 ± 866.2 a |
| TNF-a | 31.4 ± 55.3 a’ | 33.1 ± 41.7 a’ | 24.7 ± 30.2 a’ | 31.6 ± 30.6 a | 56.8 ± 84.7 a | 31.6 ± 27.9 a |
| IFN-Y | 49.0 ± 45.9 a’ | 73.5 ± 46.4 a’ | 62.0 ± 55.1 a’ | 80.4 ± 68.4 a | 127.4 ± 110.9 a | 67.3 ± 54.4 a |
| PDGF-bb | 74.4 ± 133.1 a’ | 45.6 ± 60.0 a’ | 33.2 ± 41.6 a’ | 64.7 ± 136.2 a | 90.8 ± 249.4 a | 31.6 ± 34.5 a |
| bFGF | 5.1 ± 7.0 a’ | 4.2 ± 2.5 a’ | 3.6 ± 2.5 a’ | 4.4 ± 3.0 a | 6.9 ± 12.5 a | 3.4 ± 1.3 a |
| VEGF | 2982.6 ± 4491.4 a’ | 3666.5 ± 4247.7 a’ | 3541.9 ± 4860.3 a’ | 3883.9 ± 8847.3 a | 2856.4 ± 2362.8 a | 2623.1 ± 2070.7 a |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, S.; Reid, G.; Challis, J.R.G.; Gloor, G.B.; Asztalos, E.; Money, D.; Seney, S.; Bocking, A.D. Effect of Oral Probiotic Lactobacillus rhamnosus GR-1 and Lactobacillus reuteri RC-14 on the Vaginal Microbiota, Cytokines and Chemokines in Pregnant Women. Nutrients 2020, 12, 368. https://doi.org/10.3390/nu12020368
Yang S, Reid G, Challis JRG, Gloor GB, Asztalos E, Money D, Seney S, Bocking AD. Effect of Oral Probiotic Lactobacillus rhamnosus GR-1 and Lactobacillus reuteri RC-14 on the Vaginal Microbiota, Cytokines and Chemokines in Pregnant Women. Nutrients. 2020; 12(2):368. https://doi.org/10.3390/nu12020368
Chicago/Turabian StyleYang, Siwen, Gregor Reid, John R.G. Challis, Gregory B. Gloor, Elizabeth Asztalos, Deborah Money, Shannon Seney, and Alan D. Bocking. 2020. "Effect of Oral Probiotic Lactobacillus rhamnosus GR-1 and Lactobacillus reuteri RC-14 on the Vaginal Microbiota, Cytokines and Chemokines in Pregnant Women" Nutrients 12, no. 2: 368. https://doi.org/10.3390/nu12020368
APA StyleYang, S., Reid, G., Challis, J. R. G., Gloor, G. B., Asztalos, E., Money, D., Seney, S., & Bocking, A. D. (2020). Effect of Oral Probiotic Lactobacillus rhamnosus GR-1 and Lactobacillus reuteri RC-14 on the Vaginal Microbiota, Cytokines and Chemokines in Pregnant Women. Nutrients, 12(2), 368. https://doi.org/10.3390/nu12020368