
Internal Quality Control in Medical Laboratories: Westgard and the Others


Abstract
1. ISO 15189 and Internal Quality Control on Examination Results (IQC)
2. Alternatives to IQC: Calibration Materials?
3. Alternatives to IQC: Patients’ Results
4. Alternatives to IQC: Repeated Examinations
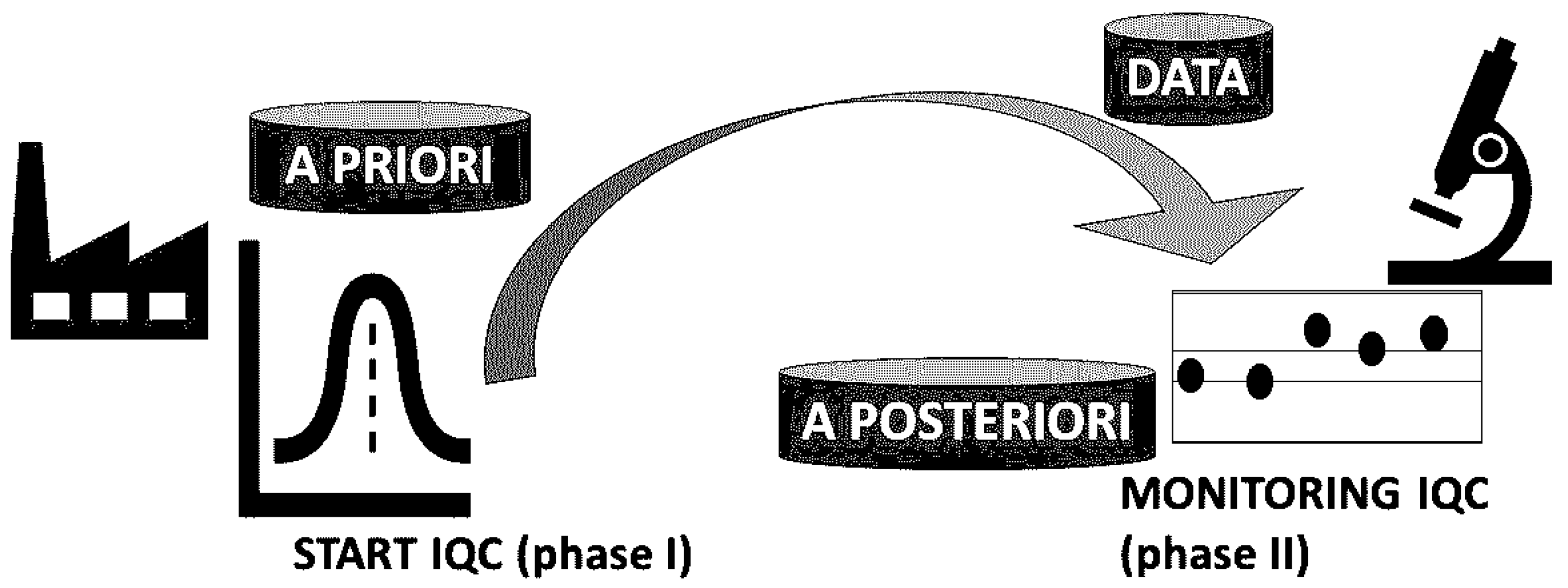
5. Alternatives to IQC: The “Bayesian” Approach
6. SIPMeL Q19 Recommendations for IQC According to ISO 15189: Final Thoughts
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ISO | International Organization for Standardization |
| SIPMeL | Italian Society of Clinical Pathology and Laboratory Medicine |
| IQC | Internal Quality Control |
| MA | Moving Average |
| RPT-QC | Quality Control with Repeat Testing on Patient Samples |
| CASCO | ISO Committee for Conformity Assessment |
| MU | Measurement Uncertainty |
| IFCC | International Federation of Clinical Chemistry and Laboratory Medicine |
| TF-GLQ | Task Force on Global Lab Quality |
| CLSI | Clinical and Laboratory Standards Institute |
| EWMA | Exponentially Weighted Moving Average |
| POCT | Point-of-Care Testing |
| NGS | Next-Generation Sequencing |
References
- ISO 15189:2022; Medical Laboratories—Requirements for Quality and Competence. ISO: Geneva, Switzerland, 2022.
- Q19 Recommendations for ISO 15189 Accreditation of Medical Laboratory: Examination Processes, Validity of Examination Results. 3 April 2024. Document Approved by the National Council on 27 February 2024. Available online: https://www.sipmel.it/it/lineeguida/approvate/121264 (accessed on 2 May 2025).
- Linko, S.; Boursier, G.; Bernabeu-Andreu, F.; Dzneladze, N.; Vanstapel, F.; Brguljan, P.; Tosheska-Trajkovska, K.; Mehay, H.; Panteghini, M.; Brugnoni, D.; et al. EN ISO 15189 revision: EFLM Committee Accreditation and ISO/CEN standards (C: A/ISO) analysis and general remarks on the changes. Clin. Chem. Lab. Med. 2025, 63, 1084–1098. [Google Scholar] [CrossRef] [PubMed]
- Pradella, M. New ISO standards for medical biology laboratories, prescriptions and deviations. Ann. Biol. Clin. 2022, 80, 451–453. [Google Scholar] [CrossRef]
- ISO/TS 20914:2019; Medical Laboratories—Practical Guidance for the Estimation of Measurement Uncertainty. ISO: Geneva, Switzerland, 2019.
- Pradella, M. Le raccomandazioni SIPMeL per l’accreditamento ISO del monitoraggio di validità dei risultati degli esami CQI per ISO 15189. Riv. Ital. Med. Lab. 2024, 20, 209–219. [Google Scholar] [CrossRef]
- Giannoli, J.M.; Vassault, A.; Carobene, A.; Liaudet, A.P.; Blasutig, I.M.; Dabla, P.K.; Lin, J.; Thomas, A.; Tesser Poloni, J.A.; Meng, Q.H.; et al. Ensuring internal quality control practices in medical Laboratories: IFCC recommendations for practical applications based on ISO 15189:2022. Clin. Chim. Acta 2025, 571, 120240. [Google Scholar] [CrossRef] [PubMed]
- Pradella, M. Divergences between IFCC recommendations for Internal Quality Control and ISO standards. Clin. Chim. Acta 2025, 120334. [Google Scholar] [CrossRef]
- Çubukçu, H.C.; Thelen, M.; Plebani, M.; Panteghini, M. IFCC recommendations for internal quality control practice: A missed opportunity. Clin. Chem. Lab. Med. 2025; Online ahead of print. [Google Scholar] [CrossRef]
- Panteghini, M. An improved implementation of metrological traceability concepts is needed to benefit from standardization of laboratory results. Clin. Chem. Lab. Med. 2025, 63, 270–278. [Google Scholar] [CrossRef]
- ISO 17511:2020; In Vitro Diagnostic Medical Devices—Requirements for Establishing Metrological Traceability of Values Assigned to Calibrators, Trueness Control Materials and Human Samples. ISO: Geneva, Switzerland, 2020.
- ISO 21151:2020; In Vitro Diagnostic Medical Devices—Requirements for International Harmonisation Protocols Establishing Metrological Traceability of Values Assigned to Calibrators and Human Samples. ISO: Geneva, Switzerland, 2020.
- Braga, F.; Pasqualetti, S.; Aloisio, E.; Panteghini, M. The internal quality control in the traceability era. Clin. Chem. Lab. Med. 2021, 59, 291–300. [Google Scholar] [CrossRef]
- Westgard, J.; Bayat, H.; Westgard, S. How to evaluate fixed clinical QC limits vs. riskbased SQC strategies. Clin. Chem. Lab. Med. 2022, 60, e199–e201. [Google Scholar] [CrossRef]
- Pradella, M. Controllo di qualità interno: Statistica avversaria della metrologia? Riv. Ital. Med. Lab. 2021, 17, 130–132. [Google Scholar] [CrossRef]
- CLSI EP15:2014; User Verification of Precision and Estimation of Bias. CLSI: Malvern, PA, USA, 2014.
- CLSI EP32 ED2:2024; Metrological Traceability in Laboratory Medicine. CLSI: Malvern, PA, USA, 2024.
- CLSI C24:2016; Statistical Quality Control for Quantitative Measurement Procedures: Principles and Definitions. CLSI: Malvern, PA, USA, 2016.
- van Andel, E.; Henricks, L.M.; Giliams, A.P.M.; Noordervliet, R.M.; Mensink, W.J.; Filippo, D.; van Rossum, H.H.; Cobbaert, C.M.; Gillis, J.M.E.P.; Schenk, P.W.; et al. Moving average quality control of routine chemistry and hematology parameters—A toolbox for implementation. Clin. Chem. Lab. Med. 2022, 60, 1719–1728. [Google Scholar] [CrossRef]
- van Rossum, H.H.; van den Broek, D. Design and implementation of quality control plans that integrate moving average and internal quality control: Incorporating the best of both worlds. Clin. Chem. Lab. Med. 2019, 57, 1329–1338. [Google Scholar] [CrossRef] [PubMed]
- van Rossum, H.H. Technical quality assurance and quality control for medical laboratories: A review and proposal of a new concept to obtain integrated and validated QA/QC plans. Crit. Rev. Clin. Lab. Sci. 2022, 59, 586–600. [Google Scholar] [CrossRef]
- Cembrowski, G.S. Use of patient data for quality control. Clin. Lab. Med. 1986, 6, 715–733. [Google Scholar] [CrossRef]
- Çubukçu, H.C. QC Constellation. Clin. Chem. Lab. Med. 2024, 62, 2185–2197. [Google Scholar] [CrossRef]
- Carson, P.K.; Yeh, A.B. Exponentially weighted moving average (EWMA) control charts for monitoring an analytical process. Ind. Eng. Chem. Res. 2008, 47, 405–411. [Google Scholar] [CrossRef]
- Çubukçu, H.C. The weighting factor of exponentially weighted moving average chart. Turk. J. Biochem. 2020, 45, 639–641. [Google Scholar] [CrossRef]
- Topcu, D.I.; Çubukçu, H.C. Optimization of patient based real-time quality control based on the Youden index. Clin. Chim. Acta 2022, 534, 50–56. [Google Scholar] [CrossRef]
- Cembrowski, G.S.; Xu, Q.; Cervinski, M.A. Average of Patient Deltas: Patient-Based Quality Control Utilizing the Mean Within-Patient Analyte Variation. Clin. Chem. 2021, 67, 1019–1029. [Google Scholar] [CrossRef] [PubMed]
- Bietenbeck, A.; Cervinski, M.A.; Katayev, A.; Loh, T.P.; van Rossum, H.H.; Badrick, T. Understanding Patient-Based Real-Time Quality Control Using Simulation Modeling. Clin. Chem. 2020, 66, 1072–1083. [Google Scholar] [CrossRef]
- Flatland, B.; Freeman, K.P. Repeat patient testing quality control (RPT-QC): Background and theory. Vet. Clin. Pathol. 2024, 53 (Suppl. 1), 24–30. [Google Scholar] [CrossRef]
- Westgard, J.O. Basic QC Practices, 4th ed.; Training in Statistical Quality Control for Medical Laboratories; Westgard QC: Madison, WI, USA, 2016. [Google Scholar]
- Daly, S.; Graham, P.A.; Freeman, K.P. Repeat patient testing-quality control with canine samples shows promise as an alternative to commercial quality control material for a network of four Sysmex XT-2000iV hematology analyzers. Vet. Clin. Pathol. 2024, 53 (Suppl. 1), 39–47. [Google Scholar] [CrossRef] [PubMed]
- Westgard, S.; Daly, S.; Freeman, K.; Flatlan, B. Repeat Patient QC: A new approach for patient-based control. Webinar, 14 December 2023. [Google Scholar]
- Tsiamyrtzis, P.; Sobas, F.; Négrier, C. Use of prior manufacturer specifications with Bayesian logic eludes preliminary phase issues in quality control: An example in a hemostasis laboratory. Blood Coagul. Fibrinolysis 2015, 26, 590–596. [Google Scholar] [CrossRef]
- Jousselme, E.; Meijer, P.; Sobas, F.; Tsiamyrtzis, P. Complementarity between Bayesian Internal Quality Control results management and External Quality Assessment bivariate z-score analysis: Application to a concrete case study. Ann. Biol. Clin. 2025, 82, 645–650. [Google Scholar] [CrossRef] [PubMed]
- ISO 15198:2004; Clinical Laboratory Medicine—In Vitro Diagnostic Medical Devices—Validation of User Quality Control Procedures by the Manufacturer. ISO: Geneva, Switzerland, 2004.
- Pradella, M. Produttore di diagnostici e laboratorio medico alleati per il controllo di qualità dei risultati: Ritardi e novità. Riv. Ital. Med. Lab. 2020, 16, 73–77. [Google Scholar] [CrossRef]
- Pradella, M. Alliance of IVD manufacturer and medical laboratory for quality control of results. Adv. Lab. Med. 2021, 2, 137–140. [Google Scholar] [CrossRef]
- Reilly-Stitt, C.; Jennings, I.; Kitchen, S.; Walker, I.D. Internal Quality Control in Hemostasis Assays. Semin. Thromb. Hemost. 2024, 50, 1084–1090. [Google Scholar] [CrossRef] [PubMed]
- CLSI POCT07:2010; Quality Management: Approaches to Reducing Errors at the Point of Care. CLSI: Malvern, PA, USA, 2010.
- CLSI POCT08:2010; Quality Practices in Noninstrumented Point-of-Care Testing: An Instructional Manual and Resources for Health Care Workers. CLSI: Malvern, PA, USA, 2010.
- CLSI POCT14:2020; Point-of-Care Coagulation Testing and Anticoagulation Monitoring. CLSI: Malvern, PA, USA, 2010.
- van Rossum, H.H.; Giannoli, J.-M. and Badrick, T. Patient Moving Average for Continuous Real-Time QC; Real-World Application Illustrated. Int. J. Lab. Hematol. 2025, 47, 570–573. [Google Scholar] [CrossRef]
- Cembrowski, G. Whither Hematology Moving Averages? Int. J. Lab. Hematol. 2025, 47, 555–556. [Google Scholar] [CrossRef]

{kind=link}
| IQC Alternative | ISO 15189 and SIPMeL Q19 Conformity |
|---|---|
| Traceability material (with manufacturer) | No |
| Patient results (moving averages) | Yes |
| Repeated patient examinations | Yes |
| Bayesian approach (with manufacturer) | Yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pradella, M. Internal Quality Control in Medical Laboratories: Westgard and the Others. Laboratories 2025, 2, 15. https://doi.org/10.3390/laboratories2030015
Pradella M. Internal Quality Control in Medical Laboratories: Westgard and the Others. Laboratories. 2025; 2(3):15. https://doi.org/10.3390/laboratories2030015
Chicago/Turabian StylePradella, Marco. 2025. "Internal Quality Control in Medical Laboratories: Westgard and the Others" Laboratories 2, no. 3: 15. https://doi.org/10.3390/laboratories2030015
APA StylePradella, M. (2025). Internal Quality Control in Medical Laboratories: Westgard and the Others. Laboratories, 2(3), 15. https://doi.org/10.3390/laboratories2030015