1. Introduction
The incidence and prevalence of non-healing umbilical ulcers in infants are challenging to determine due to their rarity and multiple underlying etiologies.
One of the most common causes is umbilical granuloma, which arises after delayed cord separation and appears as a small, pedunculated nodule at the umbilicus. Umbilical granulomas show an annual incidence ranging from 3.8% to 7.3%, and a median of 6.3% [
1]. Congenital etiologies such as patent urachus or omphalomesenteric duct remnants are reported far less frequently. Patent omphalomesenteric duct, a communication between the ileum and umbilicus, often presents with drainage of enteric contents and prolapse of the ileum. Similarly, a patent urachus causes urine leakage from the umbilicus due to an abnormal connection between the bladder and umbilicus. The prevalence of urachal anomalies in the pediatric population is around 1.03%, while omphalomesenteric duct remnants occur in approximately 2% of newborns, with complete patency observed in less than 0.1% [
2]. Other causes include neonatal omphalitis, an infection characterized by purulent discharge, which is rare in developed countries, with an incidence of about 0.7% [
3]. Identifying the precise etiology is key to the effective management and healing of umbilical ulcers in infants.
In our case, the underlying cause of the non-healing umbilical ulcer was initially identified as an infected urachal remnant, a congenital anomaly in which the embryological connection between the bladder and umbilicus persists. After surgical excision of the urachal remnant and proper closure of the wound, the ulcer reopened, despite seemingly adequate surgical management.
The recurrence of the wound, without clear explanation at that time, prompted further investigation, eventually leading us to consider less common congenital anomalies and immune deficiencies. Genetic testing revealed an autosomal dominant defect of
RAC2 gene.
RAC2 is a GTPase protein that regulates multiple aspects of neutrophil biology, including oxidase activity, chemotaxis, and granule release [
4]. In this case, a deeper understanding of neutrophil biology and its role in wound healing is crucial, especially in the context of
RAC2 deficiency [
5]. Neutrophils are among the first immune cells to arrive at the site of injury, where they play a key role in initiating the inflammatory response. They perform essential functions in host defense, such as endothelial interaction, chemotaxis, and phagocytosis, which are critical for clearing pathogens and initiating the tissue repair process. Neutrophils interact with the endothelium through a series of steps: selectin-initiated capture, integrin-mediated adhesion, and chemotaxis-driven diapedesis into the injured tissue. Once in the tissue, neutrophils deal with bacterial invasion by engulfing and destroying pathogens through oxidative bursts and the release of antimicrobial granules [
6]. In the context of wound healing, the
RAC2 mutation impairs neutrophil migration to the wound site and hinders its ability to carry out essential microbial killing functions. This leads to persistent infections, failure to properly clear pathogens, and prolonged inflammation, which in turn impairs the normal healing cascade. Without adequate neutrophil function, the body struggles to initiate the repair process, and wounds remain open and susceptible to further infection.
2. Case Presentation
A 5-month-old female infant presented to the pediatric ward of our hospital with recurrent bacterial infections and a non-healing ulcer at the umbilical site following urachal remnant removal surgery performed at another hospital. Her medical history at admission in our center included a delayed umbilical cord separation (reported to be at 4 weeks) with multiple surgical site infections. During the admission to the Pediatric department, E. cloacae strain was detected by microbiological swab on the umbilical wound, which was treated with Cotrimoxazole and Ciprofloxacin, based on an antibiogram of the pathogen. In the following month, the local conditions of the umbilical wound never improved after conservative treatment, including advanced dressings (hydrofiber with silver ions), and so the pediatricians asked for a Plastic Surgery consultation. Multiple subsequent microbiological isolates were detected, including Stenotrophomonas maltophila, E. faecalis, ESBL Klebsiella, ESBL E. coli, and VRE Enterococcus faecium. Regular infectious disease consultations were performed, and new systemic antibiotic therapies were prescribed, including IV Tigecycline and Linezolid, which apparently eradicated the local infection. At the time of our evaluation, the patient presented a 3 × 4 cm non-healing ulcer with fibrinous wound bed and perilesional erythema. The complete blood count (CBC) was within normal limits, except for a trend toward leukocytosis, consistent with the umbilical wound. Suspecting an infection associated with the incomplete removal of the urachal remnant, we decided, after consulting with pediatricians and pediatric surgeons, to proceed with a surgical intervention to manage the local conditions.
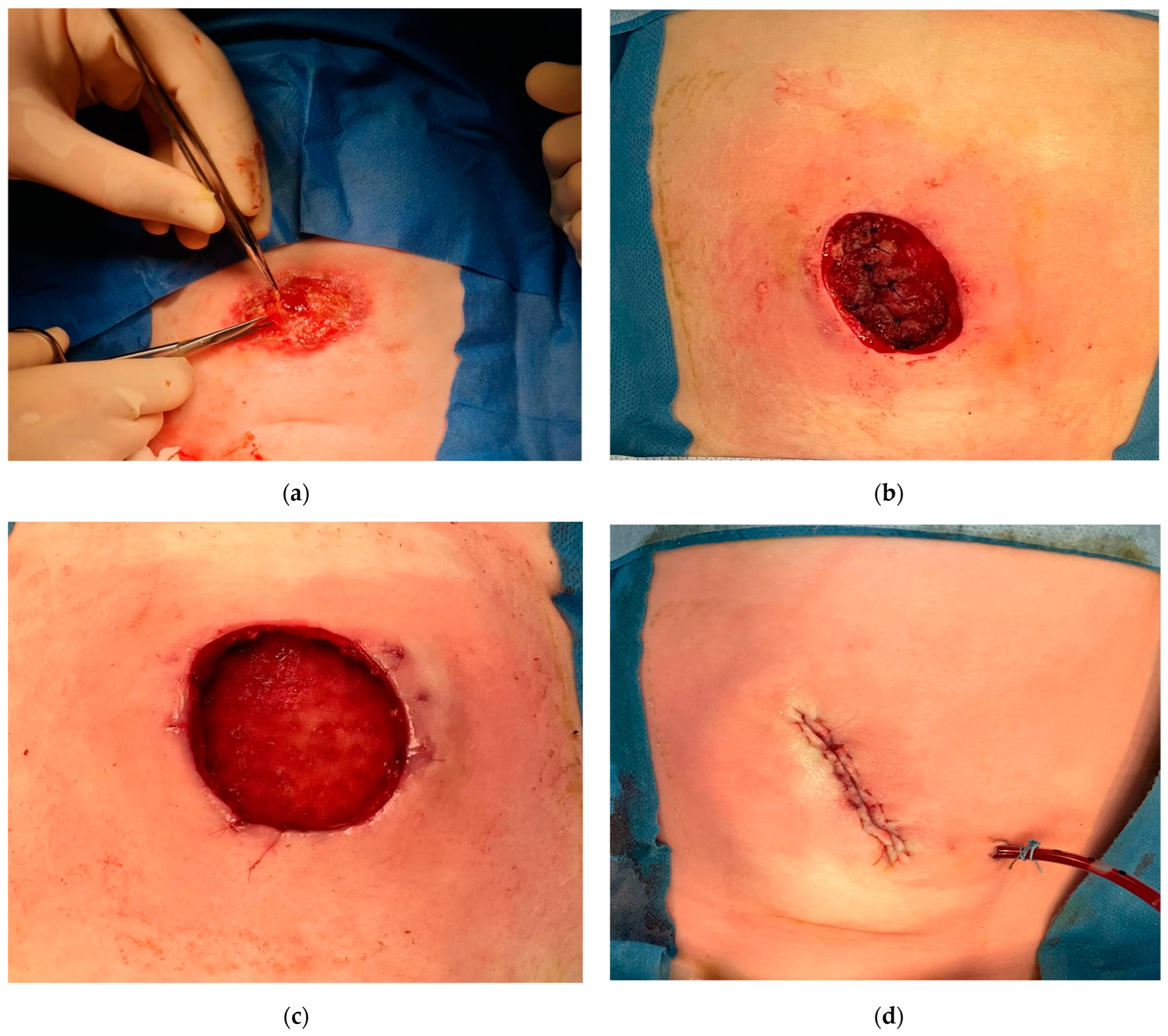
The initial treatment provided surgical wound exploration and debridement. During the procedure, the presence of an orifice communicating with the abdominal cavity and the upper bladder dome was noted, with the presence of a urachal remnant. The residual urachus was removed and thorough debridement was performed, followed by reinforcement of the damaged abdominal wall with a porcine dermis-derived collagen matrix and local flap closure (
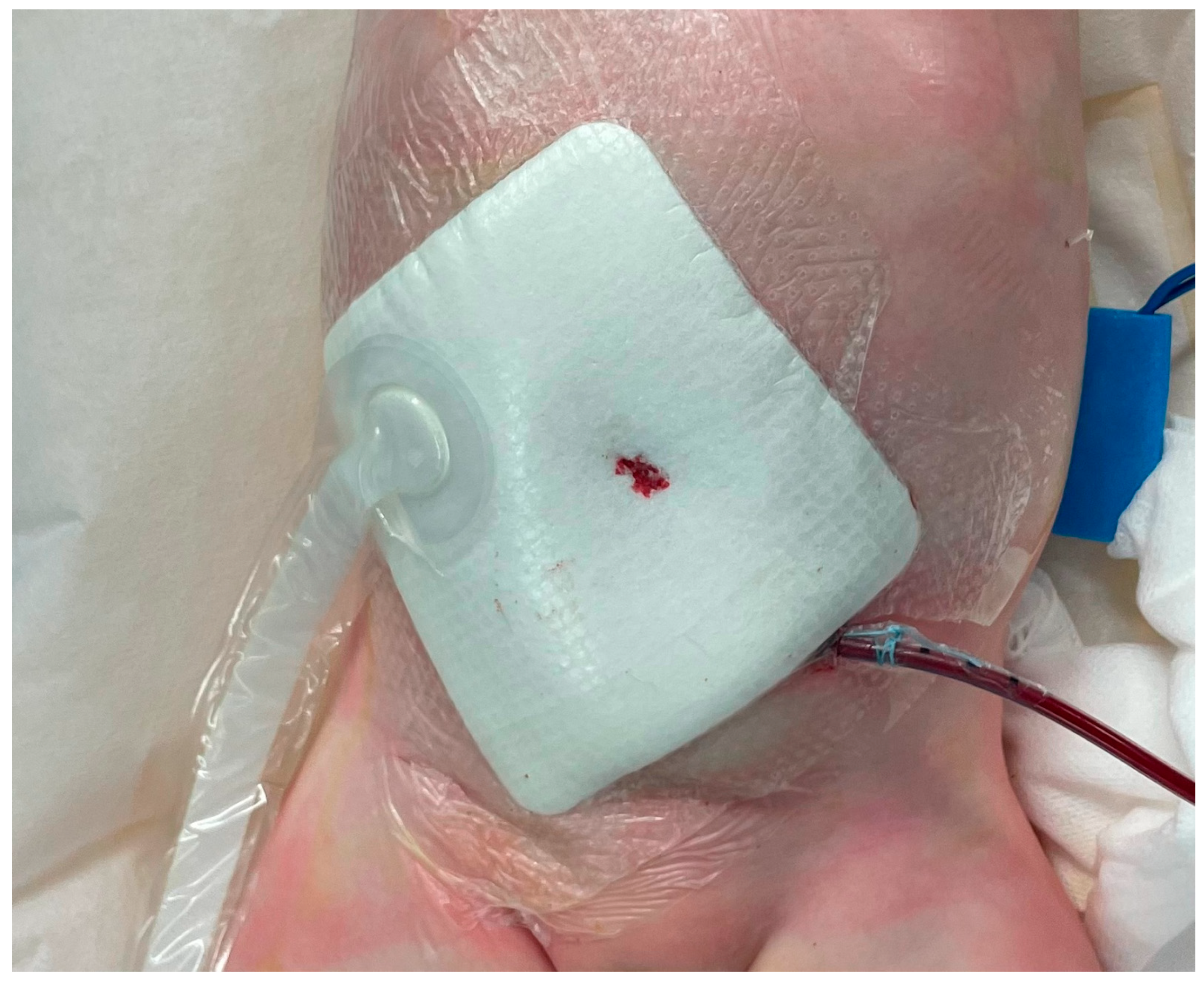
Figure 1). Additional incisional negative pressure therapy was applied to help control the wound exudate and maintain a clean microenvironment (
Figure 2). However, the ulcer failed to heal, with dehiscence occurring 10 days postoperatively.
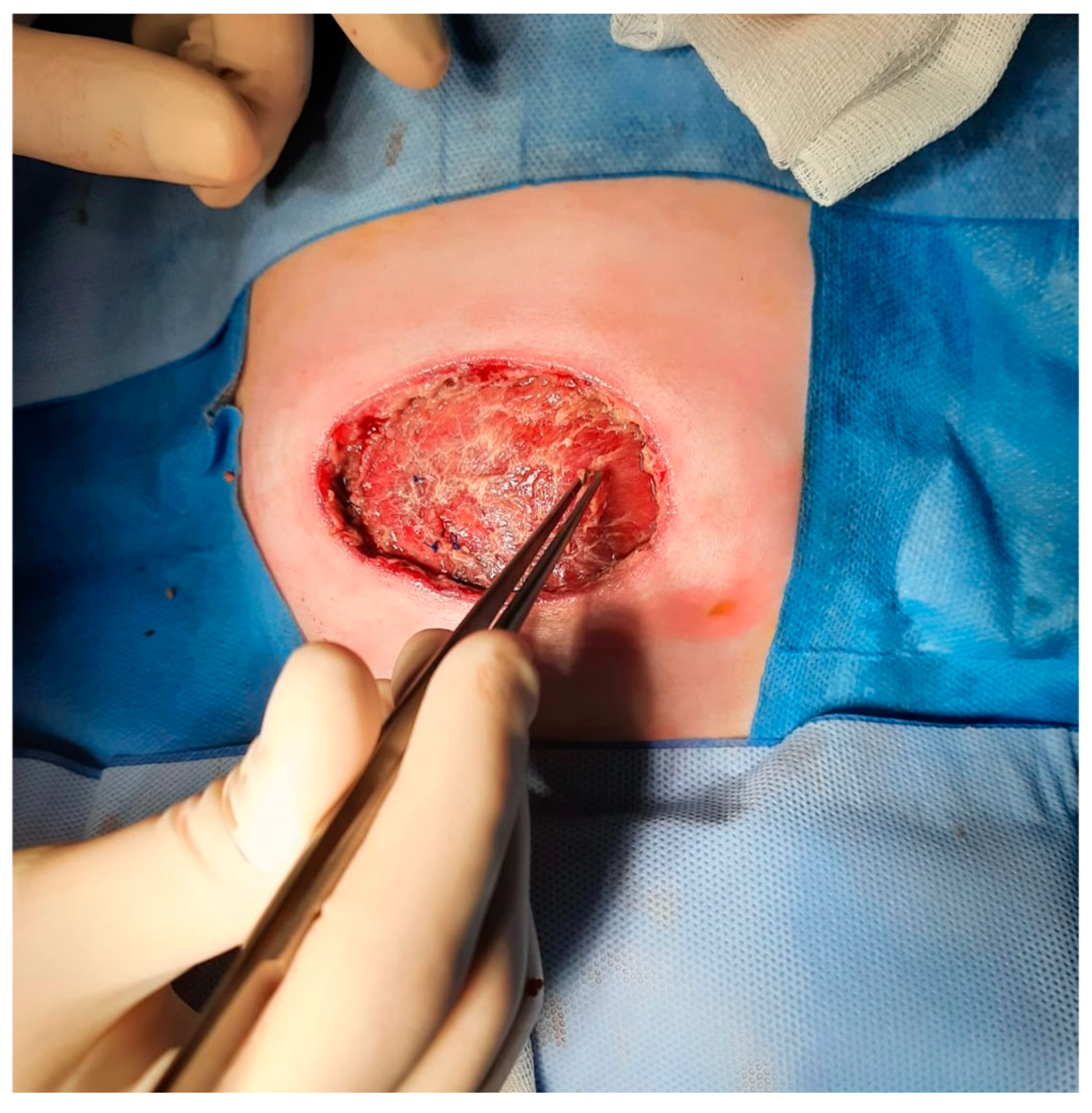
We performed microbiological analysis of the wound and concurrently executed further debridement and applied traditional negative pressure therapy whilst waiting for new microbiological laboratory results (
Figure 3). The tests showed positivity for
S. Epidermidis. Interesting to note was the absence of pus in the infected areas, despite microbiological analysis proving a concurrent infection.
The suspicion of congenital immunodeficiency in this case arose primarily due to the combination of clinical signs: recurrent bacterial infections, a non-healing umbilical postoperative ulcer, and the absence of pus. A genetic and immunologic workup was then conducted. After a new multidisciplinary evaluation while awaiting genetic analysis and considering the poorly controlled infective conditions, the patient was treated with serial wound debridement and negative pressure therapy.
The immunological analysis revealed CD4+ lymphopenia with a representative T naïve cohort, IgG in range, undetectable IgA, while leukocyte adhesion molecules were in the range of normality. The genetic tests led to the final diagnosis of a heterozygous autosomal dominant point mutation in the RAC2 gene. The test results were ready approximately one month after admission.
RAC2 deficiency, which impairs neutrophil function, accounted for the recurrent infections and poor wound healing observed in the patient. Oncohaematologists proposed hematopoietic stem cell transplant (HSCT) as curative treatment, but the procedure was ruled out until the wound was healed to reduce the high infectious risk involved in such a procedure. Following the diagnosis, the oncohaematologists proceeded with granulocyte transfusion (buffy coat from non-familiar donor) three times a week to support the immune system. The antibiotic therapy was targeted based on the pathogens identified on the wound during the whole hospital stay. The wound was surgically debrided and covered with an innovative bovine collagen type I dermal template selected for its immunomodulatory properties.
Despite this strategy, the treatment was unsuccessful, as the surgical site developed a recurrency of infection with a new strain of
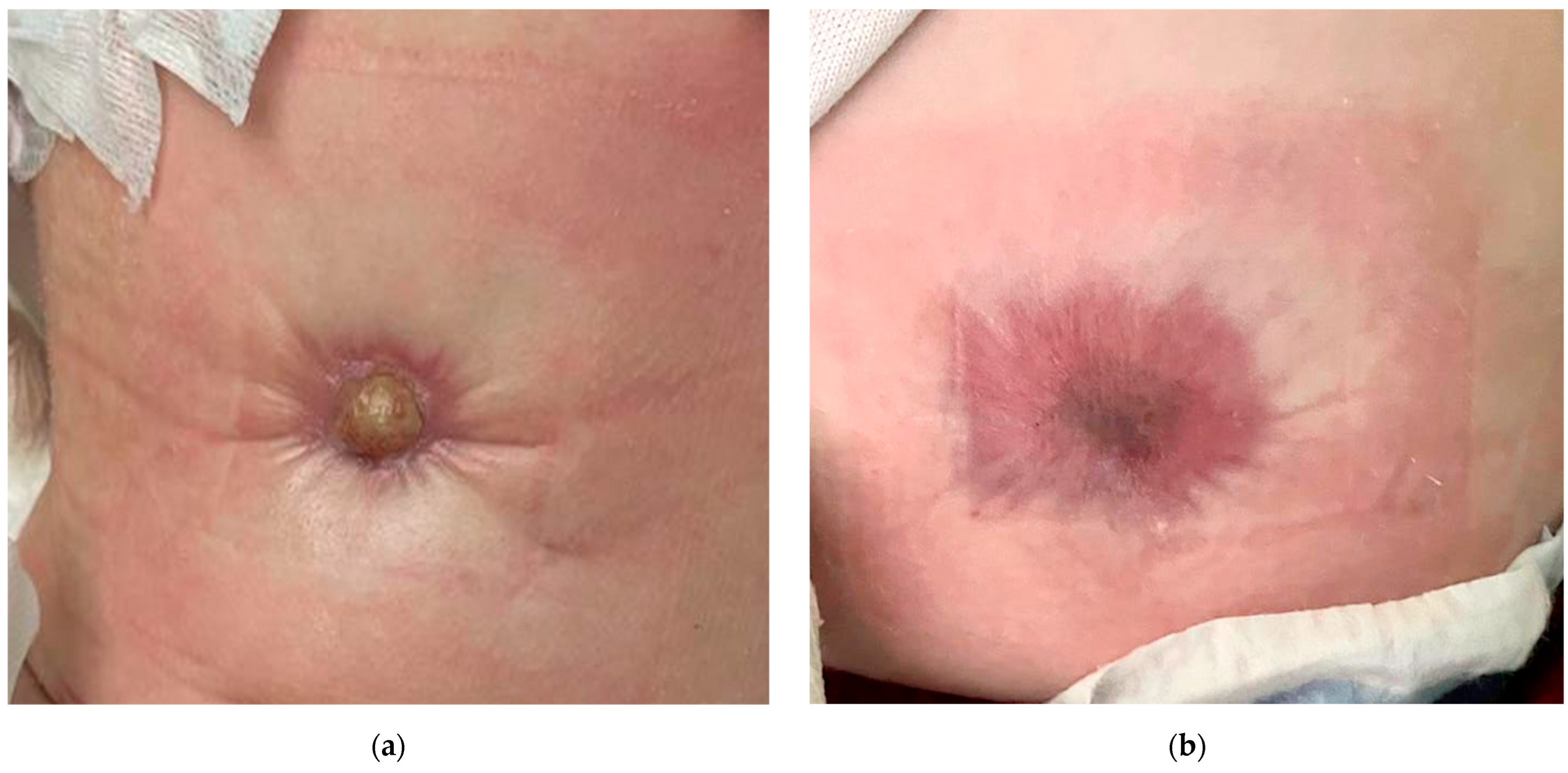
S. epidermidis (ampicillin-resistant, teicoplanin-resistant, gentamycin-resistant, levofloxacin-resistant, and ampicillin/sulbactam-resistant). To enhance the healing process, the patient underwent another cycle of negative pressure therapy combined with eight sessions of hyperbaric oxygen therapy. Following confirmation that the wound bed tested negative in microbiological swabs at the one-month follow-up, an additional surgical debridement was performed. The wound was then covered with a dermal matrix, as illustrated in
Figure 4 and
Figure 5.
Thirty days after the application of the new dermal matrix, the wound bed was apparently ready for split thickness split graft, which was harvested from the left inguinal area. Despite interventions, the wound only partially healed, and the central portion of the ulcer remained open, as shown in
Figure 6. In the following days, the patient developed progressively worsening thrombocytopenia, with a minimum platelet count of 12,000 × 10
9/L. This condition was successfully treated with intravenous immunoglobulin infusions, administered at a dose of 1 g twice daily for 3 days. A last attempt at closure was performed with a novel dermal inductor (a decellularized skin matrix derived from fish skin) suited for chronic ulcers (see
Figure 7).
The wound did not heal again, prompting a radical shift in the treatment strategy. Given the impossibility to surgically close the wound with several different products of tissue engineering and with autologous solutions, we considered it inappropriate to proceed with further surgical treatments and a new multidisciplinary meeting was convened. We decided to proceed with HSCT despite the open wound.
The HSCT was performed as shown in
Table 1.
During the hospital stay prior to the hematopoietic stem cell transplant (HSCT), the child experienced a febrile episode on day −9, just a few hours after the infusion of Rituximab. Laboratory tests revealed elevated inflammatory markers, with C-reactive protein (CRP) peaking at 39.14 mg/L on day −8. Blood cultures remained consistently negative throughout. On day −7, a new microbiological swab from a wound isolated Enterococcus faecalis, which was resistant to gentamicin and kanamycin. Targeted antibiotic therapy was initiated with amikacin, daptomycin, and piperacillin/tazobactam, and it was progressively tapered until complete discontinuation on day +27.
After the HSCT, the wound finally began healing spontaneously with only the aid of antiseptic silver dressings and daily wound care, achieving complete closure within a month without further surgical interventions (
Figure 8).
3. Discussion
This case highlights the challenges of treating chronic, non-healing wounds in a patient with
RAC2 deficiency, a congenital immunodeficiency impairing neutrophil function. This condition leads to recurrent infections, poor wound healing, and immune dysregulation. Despite admission to a specialized pediatric center, delays in immunological and genetic testing prolonged the therapeutic process. Initial management followed standard pediatric wound protocols due to the lack of a confirmed diagnosis. During the first surgery, a breach communicating with the upper dome of the bladder was identified even after the previous urachal remnant removal procedure. An acellular dermal matrix was applied for abdominal wall reinforcement to minimize infection risk and prevent further communication [
7,
8].
Although incisional negative pressure wound therapy (iNPWT) was used to control, exudate, and promote a clean wound environment, it did not prevent dehiscence or recurring infections. Conservative management, including hyperbaric therapy and NPWT, helped to limit systemic infection but failed to fully eliminate local bacterial recurrence [
9,
10].
The subsequent treatment approach included surgical debridement and the application of dermal substitutes to establish a viable wound bed. Dermal matrices, a standard tool in the reconstructive ladder, have proven to be effective even in pediatric cases. We chose a bovine collagen type I matrix due to its known ability to positively interact with the immune system and encourage a favorable macrophage response [
11,
12,
13]. In terms of surgical management, we prioritized less invasive procedures, utilizing dermal substitutes and matrices to promote wound healing while minimizing surgical burden. However, despite ongoing microbiological management and repeated debridements, multiple attempts with different dermal matrices did not achieve stable wound closure.
The delay in diagnosis underscored the difficulty in handling such cases, where the underlying genetic cause has remained unclear for an extended period. During this time, surgical intervention aimed to achieve the most effective and safe coverage for the defect. More invasive surgical options, such as local flaps, could have resulted in further complications, including infection or dehiscence, particularly in the context of the patient’s compromised immune status.
Once
RAC2 deficiency was confirmed, a multidisciplinary approach became critical, with a focus on wound management while preparing for hematopoietic stem cell transplantation (HSCT), which was recognized as the only curative option [
13,
14]. It must be stated that in every case of immunodeficiency, the decision-making process for a transplant is multifaceted and involves numerous considerations beyond the primary reason for the transplant. Factors such as the patient’s overall health and functional status, the presence of other medical conditions, and the severity of the disease play significant roles in determining the appropriateness and timing of the transplantation. Each of these variables must be carefully evaluated to assess both the potential benefits and risks of the procedure, ensuring the best possible outcome for the patient [
15]. The decision to postpone hematopoietic stem cell transplantation (HSCT), despite the illness’s progression, was based on the high infection risk associated with performing the procedure while the wound remained open [
16]. HSCT requires intense immunosuppression to facilitate donor cell engraftment, placing the patient at increased susceptibility to infections. An open wound could serve as a direct entryway for pathogens, markedly heightening the risk of life-threatening infections during this critical period. Infections are a leading cause of mortality among HSCT recipients, particularly in pediatric patients whose immune systems are still developing [
17]. Infection-related complications, whether bacterial, fungal, or viral, can not only heighten the risk of graft failure but also complicate the overall recovery process [
18].
In the case reported by Accetta et al. [
19], several differences in clinical course and management likely explain the contrasting outcomes. A critical factor is the timing of the diagnosis and intervention. Their neonatal screening detected low T-cell receptor excision circles (TRECs), immediately raising suspicion of an underlying immunodeficiency [
18]. This patient was evaluated at just two weeks of age, well before any severe infections or complications arose. Early detection allowed for timely interventions, including granulocyte transfusions and surgical debridement for omphalitis, leading to appropriate wound healing. The patient stabilized early, allowing for hematopoietic stem cell transplantation (HSCT) at 3.5 months without further complications.
In our case, the diagnosis of RAC2 deficiency was delayed; it was confirmed approximately a month after the initial presentation. This delay extended the clinical course, as recurrent infections interfered with post-surgical wound healing. Despite multiple debridement attempts and conservative treatments, the wound remained open, leading to the decision to proceed with hematopoietic stem cell transplantation (HSCT) before achieving complete wound closure. This case emphasizes the complexities of managing RAC2-related immunodeficiency when both immune impairment and secondary infections impede wound healing.
In Accetta’s case, the patient’s wound healed sufficiently after initial debridement for omphalitis, allowing HSCT to be scheduled post-healing. In contrast, our patient experienced persistent wound dehiscence and infections, which compromised surgical recovery and initially delayed HSCT. The main factors contributing to the differing outcomes between the cases appear to be the timing of diagnosis, effectiveness of infection control, and wound condition before transplantation. These differences allowed Accetta’s patient to undergo HSCT post-surgery, whereas in our case, the procedure had to be postponed.
The case presented by Kurkchubasche et al. offers further insight into managing neutrophil dysfunction related to the
RAC2 mutation [
20]. While these cases share similarities, particularly in presenting non-healing wounds and recurrent infections, the clinical responses to granulocyte infusions were notably different. In Kurkchubasche’s case, the patient had persistent perirectal and umbilical wounds that did not respond to antibiotics or surgical debridement. The turning point came with daily granulocyte transfusions over eight days, leading to complete healing of the umbilical wound and a significant improvement in the perirectal wound. This allowed the patient to stabilize for a bone marrow transplant with a matched sibling donor, ultimately resolving their symptoms in the long term. In contrast, despite granulocyte transfusions and appropriate surgical and antibiotic treatments, our patient’s wound failed to heal, possibly due to more severe immunological impairment or infections involving multi-resistant pathogens.
4. Conclusions
This case highlights essential considerations in managing patients with
RAC2 deficiency, especially the value of early genetic testing, ideally before symptoms like recurrent infections and impaired wound healing become apparent. Here, the
RAC2 mutation was only identified after a month and multiple surgical interventions, suggesting that earlier testing could have altered the therapeutic approach from the outset. A more timely diagnosis, potentially achievable through neonatal screening with the T-cell receptor excision circles (TRECs) assay, could have allowed for a more customized therapeutic approach from the beginning [
21].
The successful management of this case relied on a multidisciplinary team, including surgeons, pediatric oncologists, and infectious disease specialists. However, the team reflected on the possibility that adjusting the timing of the interventions, potentially with fewer surgeries for wound closure, might have led to a better outcome.
The timing of the hematopoietic stem cell transplantation (HSCT) was a pivotal factor in the treatment. The oncology–hematology team decided to delay HSCT until infection control and wound closure were achieved to minimize the risk of post-transplant infection related to the necessary immunosuppression. However, in hindsight, an earlier HSCT may have been advantageous, even with an open wound, given the rigorous infection control measures in place. The authors now believe that in patients with RAC2 mutations, the risks of delaying HSCT could outweigh the infection risks, provided that comprehensive perioperative management is implemented, including aggressive prophylactic antibiotics, antifungals, hyperbaric therapy, and strict sterile techniques.
This case highlights the need for increased awareness of RAC2-related immunodeficiencies, especially in patients exhibiting unusual wound healing and recurrent infections. Early diagnosis and intervention are vital to prevent fatal outcomes. Additionally, in cases with severe immunodeficiency and open wounds, early HSCT consideration is recommended, as successful wound healing heavily depends on immune function. The rapid wound healing observed after HSCT in this case supports this approach, emphasizing the essential role of immune competence in the success of surgical interventions for patients with RAC2 deficiency.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}